Contents
- What is bronchiolitis
- Anatomy of the Respiratory System in Children
- Bronchiolitis causes
- What is respiratory syncytial virus (RSV)?
- What causes respiratory syncytial virus (RSV)?
- Who is affected by respiratory syncytial virus (RSV)?
- Why is respiratory syncytial virus (RSV) a concern?
- What are the symptoms of respiratory syncytial virus (RSV)?
- How is respiratory syncytial virus (RSV) diagnosed?
- What is the treatment for respiratory syncytial virus (RSV)?
- How can respiratory syncytial virus (RSV) be prevented?
- What is respiratory syncytial virus (RSV)?
- Bronchiolitis prevention
- Bronchiolitis symptoms
- Bronchiolitis complications
- Bronchiolitis diagnosis
- Bronchiolitis treatment
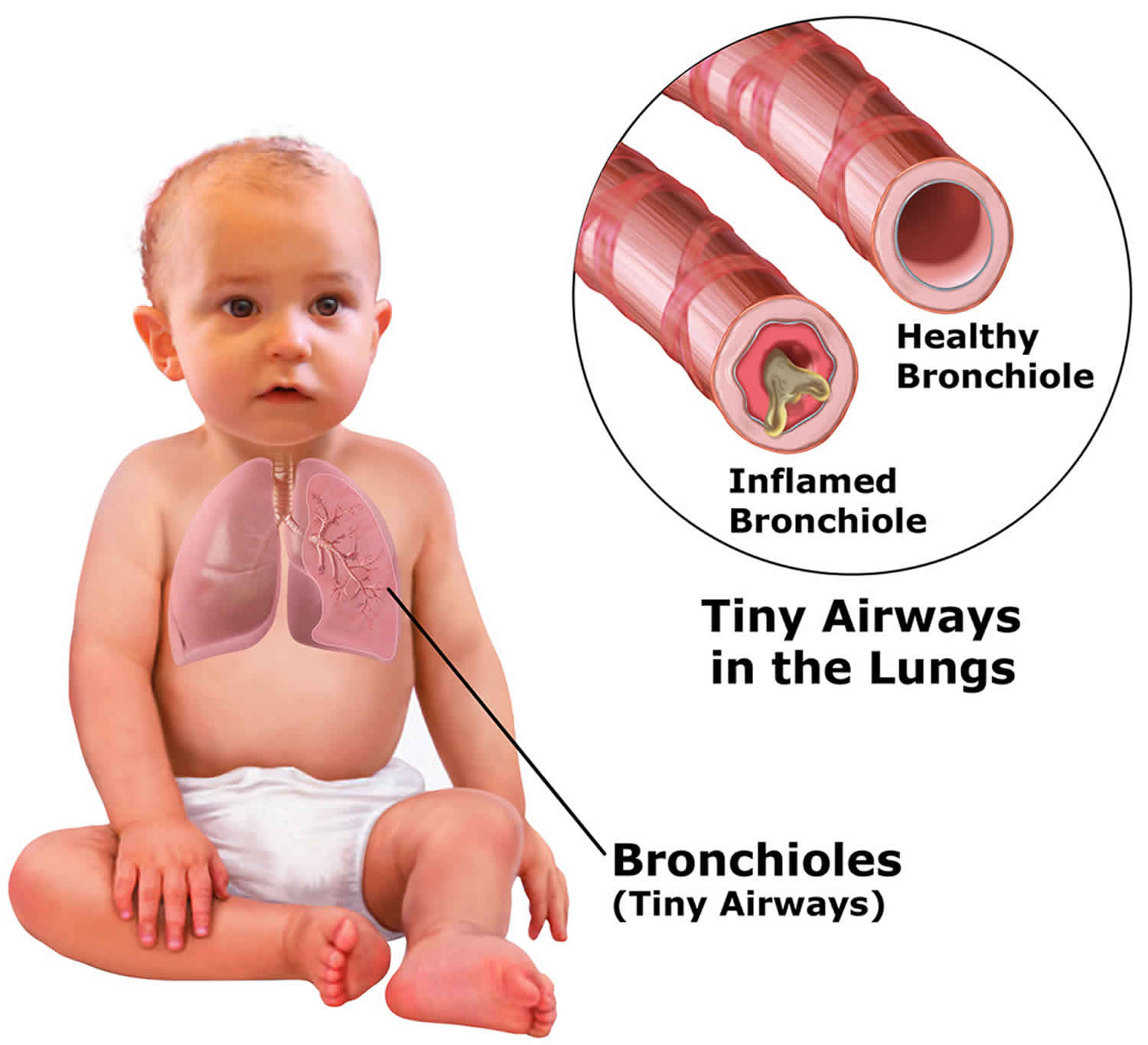
What is bronchiolitis
Bronchiolitis is a viral chest infection often caused by the respiratory syncytial virus (RSV) that can affect your child’s ability to breathe freely. Bronchiolitis is caused by inflammation in the very small airways that deliver air to the lungs called the bronchioles. Bronchiolitis usually affects babies and young children under 12 months of age and can be more severe in babies that were born prematurely. As the very small airways (bronchioles) become inflamed, they swell and become clogged with fluid and mucus, making it hard for your baby to breathe and obtain enough oxygen.
Although bronchiolitis is often a mild illness, some babies are at risk for severe bronchiolitis — including those who were born prematurely, have a chronic heart or lung disease, or have a weakened immune system due to illness or medicines. Those infants need to be treated in a hospital.
Kids who have had bronchiolitis might be more likely to develop asthma later in life. It’s not yet clear whether the illness causes or triggers asthma, or whether kids who eventually develop asthma were just more prone to developing bronchiolitis as infants. Experts continue to study the relationship between bronchiolitis and the later development of asthma.
Bronchiolitis:
- most often affects infants and young children because their noses and small airways can become blocked more easily than those of older kids or adults
- typically happens during the first 2 years of life, most commonly at about 3 to 6 months of age
- is more common in males, premature babies, children who have not been breastfed, and those who live in crowded conditions
The respiratory syncytial virus (RSV) is spread in small droplets produced by talking, coughing or sneezing and also by contact with objects that carry the virus.
The best ways to prevent the spread of bronchiolitis are to:
- keep your sick baby away from other children
- wash your hands frequently
Your child might have bronchiolitis if they appear to have a cold and a runny nose that progresses to a wheeze and cough after a day or two. Their breathing might become fast and labored, making it hard for them to eat and drink.
The symptoms are usually worst on the second or third day of infection. Your child will be mostly better within 7 to 10 days, but the cough might take a couple more weeks to go away completely.
There are steps you can take to help your baby recover from mild bronchiolitis.
Your baby needs to rest and take in small amounts of fluids frequently so they don’t get too tired when feeding and don’t become dehydrated. Infants with bronchiolitis need lots of fluids. Commonly, the breathing difficulties associated with viral bronchiolitis affect the child’s ability to feed, especially in infants younger than 6 months. To meet the increased need for fluids, it’s often best to give infants small amounts more often, as this is usually better tolerated.
It is important that a child with the condition does not become dehydrated. This can be checked by monitoring the number of feeds the child is taking and the number of wet nappies.
It is important to make sure that your home is free of cigarette smoke as it makes the symptoms worse.
Other things you can do to help your child’s breathing and make them more comfortable are to humidify the air, keep them upright and make sure they are not exposed to cigarette smoke.
Because bronchiolitis is usually caused by a virus, antibiotics won’t help. Similarly, medicines such as salbutamol (e.g. Ventolin), steroids and antihistamines are not usually effective.
Professional treatment
Fortunately, most cases of bronchiolitis are mild and don’t need specific professional treatment. Antibiotics aren’t useful because bronchiolitis is caused by a viral infection, and antibiotics are only effective against bacterial infections. Medicine may sometimes be given to help open a child’s airways.
Infants who have trouble breathing, are dehydrated, or appear fatigued should be checked by a doctor. Those who are moderately or severely ill may need to be hospitalized, watched closely, and given fluids and humidified oxygen. Rarely, in very severe cases, some babies are placed on respirators to help them breathe until they start to get better.
You should take your child to see your doctor if you notice them:
- wheezing or having difficulty breathing, especially if this is accompanied by chest retractions (pulling in of the chest wall)
- breathing very fast or has irregular breathing
- eating less than half the usual amount for at least two feeds
- having a dry nappy for 12 hours or more (dehydrated)
- is coughing and distressed
- has difficulty feeding or drinking and has fewer wet nappies than usual
- is changing color in the face when he coughs.
- is tired or more sleepy than usual.
Also arrange to see a doctor if:
- the symptoms worsen quickly
- your baby is less than 12 weeks of age
- your baby was born with a medical condition that affects their heart and lungs
Dial your local emergency services number and ask for an ambulance if your child is:
- having a lot of difficulty breathing or is exhausted from trying to breathe
- pale and sweaty or their skin is blue around the lips or fingernails
- breathing very rapidly
- having trouble feeding
- very tired, cannot be woken or goes back to sleep soon after being woken
Anatomy of the Respiratory System in Children
The respiratory system is made up of the organs involved in the interchanges of gases and consists of the:
- Nose
- Mouth
- Throat (pharynx)
- Voice box (larynx)
- Windpipe (trachea)
- Airways (bronchi)
- Lungs
The upper respiratory tract includes the following:
- Nose
- Nasal cavity
- Sinuses
The lower respiratory tract includes the following:
- Voice box (larynx)
- Windpipe (trachea)
- Lungs
- Airways (bronchi and bronchioles)
- Air sacs (alveoli)
The lungs take in oxygen, which the body’s cells need to live and carry out their normal functions. They also get rid of carbon dioxide, a waste product of the cells.
The lungs are a pair of cone-shaped organs made up of spongy, pinkish-gray tissue. They take up most of the space in the chest, or the thorax (the part of the body between the base of the neck and diaphragm). The lungs are enveloped in a membrane called the pleura and separated from each other by the mediastinum: This area contains the following:
- Heart and its large vessels
- Trachea (windpipe)
- Esophagus
- Thymus gland
- Lymph nodes
The right lung has 3 lobes. The left lung has 2 lobes. When you breathe, the air:
- Enters the body through the nose or the mouth.
- Travels down the throat through the larynx (voice box) and trachea (windpipe).
- Goes into the lungs through tubes called main-stem bronchi:
- One main-stem bronchus leads to the right lung and one to the left lung
- In the lungs, the main-stem bronchi divide into smaller bronchi
- Then into even smaller tubes called bronchioles
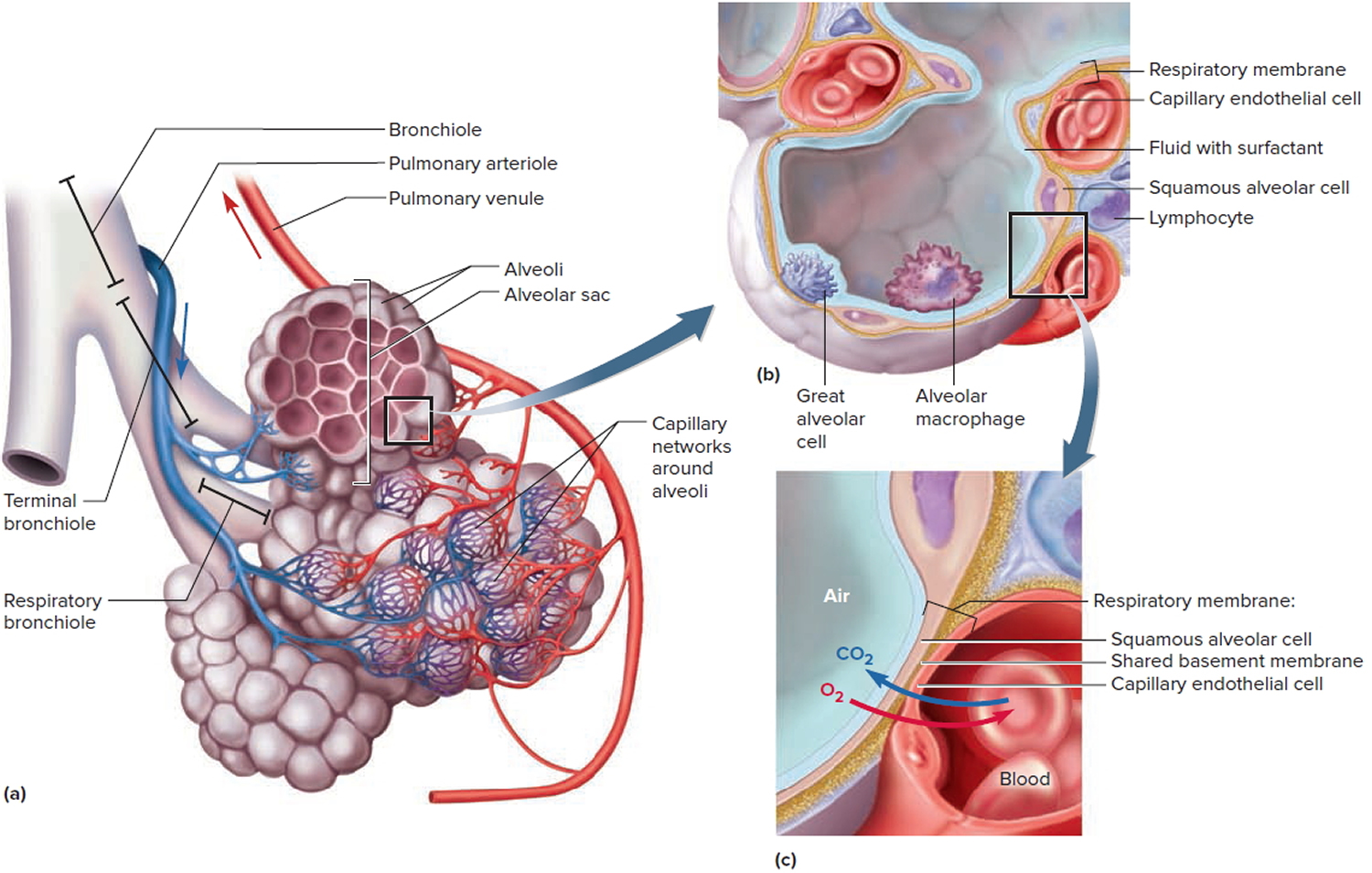
- Bronchioles end in tiny air sacs called alveoli
Figure 1. Anatomy of the Respiratory System in Children
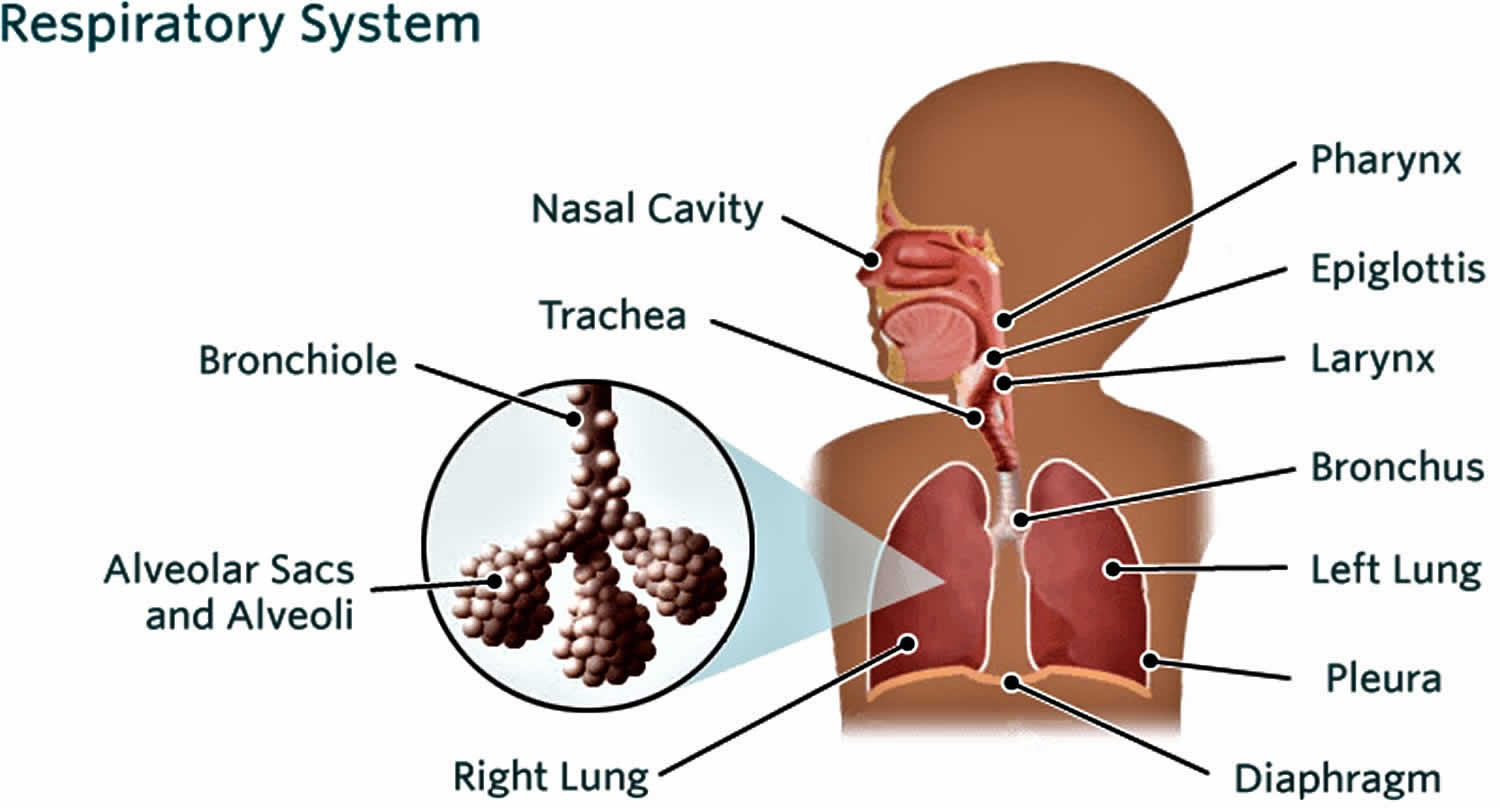
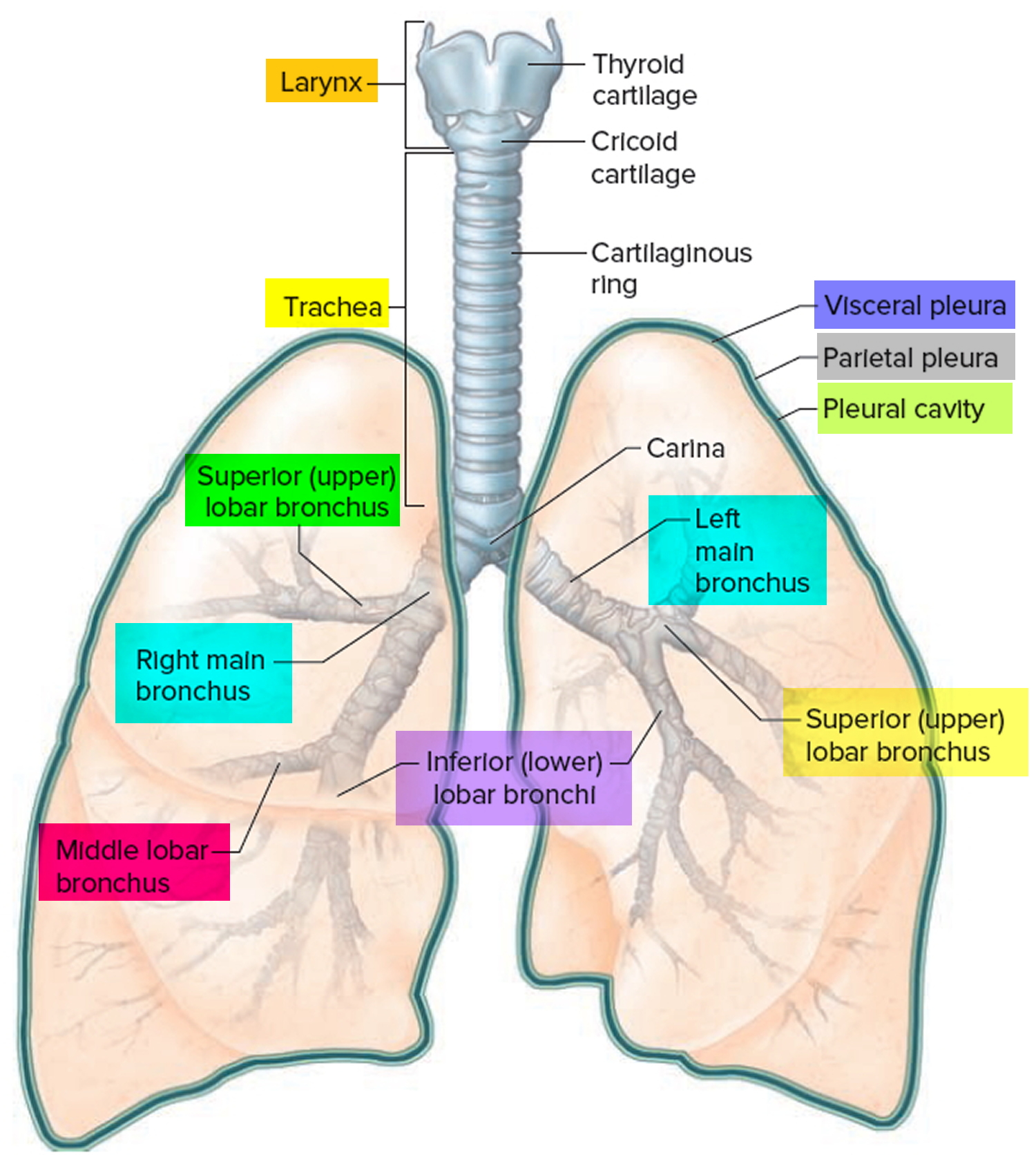
Figure 2. Pulmonary Alveoli (microscopic view)
Is bronchiolitis contagious?
Yes. Bronchiolitis is an infectious disease. The infections that cause bronchiolitis are contagious. The virus can spread in tiny drops of fluid from an infected person’s nose and mouth, which may become airborne via sneezes, coughs, or laughs, and also can end up on things the person has touched, such as used tissues or toys.
Infants in childcare centers have a higher risk of getting an infection that may lead to bronchiolitis because they’re in close contact with lots of other young children.
Avoid contact with other babies in the first few days. Keep your child home from child care or other places where there may be young children. Older children and adults can catch the virus that causes bronchiolitis, but it is most common in young children and babies.
What is bronchiolitis incubation period?
The incubation period (the time between infection and the onset of symptoms) ranges from several days to a week, depending on the infection causing the bronchiolitis.
How long does a bronchiolitis last?
Most infants with viral bronchiolitis recover completely within 7 to 12 days. However, a small number may have symptoms (most commonly a cough and have wheezing) that persist for 3 or 4 weeks.
Viral bronchiolitis illness generally reaches its peak on the second or third day after coughing begins, causing breathing difficulty before slowly getting better.
If your child was premature or has a weakened immune system or other serious health problem, such as a heart or lung condition, then bronchiolitis may be more severe.
Should my child with bronchiolitis be in hospital?
Usually, viral bronchiolitis is a mild illness that can be managed at home. However, occasionally it can be more severe and hospital admission is necessary. See the section above “When to seek medical help”.
A child will need to be treated in hospital if their fluid intake is inadequate and they are becoming dehydrated, or if they are having difficulty breathing. Hospital admission is more likely in very young children and in children with other medical conditions such as cystic fibrosis or a heart defect.
In hospital, children with viral bronchiolitis will usually be given fluids either intravenously (through a drip) or through a nasogastric tube (a tube that’s inserted through the nose and goes to the stomach). They will also be given oxygen if necessary and assistance with their breathing in severe cases. The antiviral medicine ribavirin (Virazide) may also be given in severe cases but can have serious side effects and is not always effective.
Are tests needed to diagnose bronchiolitis?
A chest X-ray is not recommended as it has been proven that it does not help with the management in infants presenting with bronchiolitis. Blood tests are generally not helpful.
Are there any medications that may help bronchiolitis in infants?
Medicines do not usually help babies with bronchiolitis.
- Antibiotics are not given because bronchiolitis is caused by a virus and antibiotics do not cure viruses.
- VentolinTM, AtroventTM or other puffers are not prescribed as these have been proven not to help as the wheezing is not related to asthma.
- Steroids such as PredmixTM or cortisone based medicines also do not help.
Will bronchiolitis happen again?
Maybe. It is possible to have bronchiolitis again, but most babies will only have it once.
Children exposed to second hand smoke are more likely to develop a range of illnesses including bronchiolitis, compared to children living in smoke-free environments.
If you do smoke, you can choose not to smoke in front of children, particularly in enclosed areas such as the car and home. Ask others to do the same.
What is bronchiolitis obliterans?
Bronchiolitis obliterans also known as obliterative bronchiolitis, is a manifestation of chronic allograft rejection, that is, rejection following lung transplantation from another human being. It develops in nearly 50 percent of all patients who receive a lung transplant from an unrelated donor.
Bronchiolitis obliterans or obliterative bronchiolitis is a severe inflammatory response provoked by lung transplantation from an unrelated donor. The inflammatory response causes a large number of lymphocytes (a type of white blood cell that fights infection) to come into the graft tissue (transplanted tissue), resulting in fibrosis (increase in fibrous tissue) and progressive narrowing of the airway. This can cause airway obstruction and is a major cause of death in patients after receiving lung transplantation.
Bronchiolitis obliterans is the major obstacle to prolonged survival following lung transplatation. Survival following lung transplantation is significantly poorer as compared to transplatation of other organs.
Although bronchiolitis obliterans is rare within the first year after lung transplantation, it becomes common beyond the first year. Bronchiolitis obliterans happens to a total of 50 to 80% of patients in a period of 5 years following lung tranplantation.
Risk factors for bronchiolitis obliterans
Patients with acute allograft rejection (rejection to the foreign organ shortly after tranplantation), especially those with multiple or severe episodes, are at a significantly increased risk of developing bronchiolitis obliterans.
Other risk factors include mismatching of HLA (the major histocompatibility complex in humans), pneumonia caused by a virus called cytomegalovirus (CMV) and injury to the airways or transplanted tissue.
A new study shows that exposure to a chemical called diacetyl, a component of artificial butter flavouring, can be harmful to the nose and airways of mice. Scientists at the National Institute of Environmental Health Sciences, part of the National Institutes of Health, conducted the study because diacetyl has been implicated in causing bronchiolitis obliterans in humans. Obliterative bronchiolitis has been detected recently in workers who inhale significant concentrations of the flavoring in microwave popcorn packaging plants. When laboratory mice inhaled diacetyl vapors for three months, they developed lymphocytic bronchiolitis – a potential precursor of bronchiolitis obliterans. None of the mice, however, were diagnosed with bronchiolitis obliterans.
Progression of obliterative bronchiolitis
The time frame from lung transplantation to the start of symptoms of bronchiolitis obliterans is variable, ranging from 3 months to more than 9 years after transplantation.
Once obliterative bronchiolitis develops, the lung function typically declines progressively. Generally, progressive obstruction to airflow results in exercise limitation, repetitive lung infections, and, eventually, death due to poor lung function.
The course of bronchiolitis obliterans, however, varies between individuals. Some patients experience rapid loss of lung function and die in a few months. Others progress slowly, followed by prolonged stability.
Obliterative bronchiolitis has been graded into 5 categories based on the FEV1, which is the volume of air that can be forced out in one second after taking a deep breath.
The five categories are BOS 0, BOS 0p, BOS 1, BOS 2, and BOS 3, with declining lung function as the grade goes higher.
How is bronchiolitis obliterans diagnosed?
The doctor will perform a lung function test measuring the FEV1, which is the volume of air that can be forced out in one second after taking a deep breath.
Some other tests like bronchoalveolar lavage (lung washings) and culture may be carried out in some centres.
Bronchiolitis obliterans prognosis
The death rate at 3 years after the start of bronchiolitis obliterans is more than 50%.
The survival rate at 5 years after the start of the disease is only 30 to 50%.
Patients who develop bronchiolitis obliterans within the first 3 years after transplatation have a poorer outcome. A majority of these patients have a greater decline in lung function, greater need for oxygen and a higher rate of transplant failure (requiring retransplantation) or death.
How is bronchiolitis obliterans treated?
- Treat specific complications
- Treat/prevent episode of acute rejection (rejection shortly after transplantation)
- Oxygen supplement
- Drugs to dilate (widen) the airways to relieve symptoms from airway obstruction
Some other treatment options may be considered:
- Increased immunosuppression (to suppress the inflammatory response)
- Drugs like tacrolimus, mycophenolate mofetil, cytolytic therapy
A second transplantation of the lung may be considered in some cases, if possible.
A recent study demonstrated in experimental mice that inhalation of safe and controlled doses of carbon monoxide for several weeks after transplant surgery prevented the development of bronchiolitis obliterans. This might be a useful treatment option in the future but further research is still needed. Since carbon monoxide is a poisonous gas, care must be taken in terms of dosage in any future therapy to prevent toxicity.
Bronchiolitis vs Pneumonia
Pneumonia is swelling due to infection of the tissue in one or both lungs. Many germs, such as bacteria, viruses, and fungi, can cause pneumonia. You can also get pneumonia by inhaling a liquid or chemical. People most at risk are older than 65 or younger than 2 years of age, or already have health problems.
At the end of the breathing tubes in your lungs are clusters of tiny air sacs. If you have pneumonia, these tiny sacs become inflamed and fill up with fluid.
Symptoms of pneumonia vary from mild to severe. See your doctor promptly if you
- Have a high fever
- Have shaking chills
- Have a cough with phlegm that doesn’t improve or gets worse
- Develop shortness of breath with normal daily activities
- Have chest pain when you breathe or cough
- Feel suddenly worse after a cold or the flu
Your doctor will use your medical history, a physical exam, and lab tests to diagnose pneumonia. Treatment depends on what kind you have. If bacteria are the cause, antibiotics should help. If you have viral pneumonia, your doctor may prescribe an antiviral medicine to treat it.
Preventing pneumonia is always better than treating it. Vaccines are available to prevent pneumococcal pneumonia and the flu. Other preventive measures include washing your hands frequently and not smoking.
Bronchiolitis vs Bronchitis
Bronchitis is an inflammation of the bronchial tubes, the larger airways that carry air to your lungs that connect the trachea (windpipe) to the lungs. Bronchitis causes a cough that often brings up mucus. Bronchitis can also cause shortness of breath, wheezing, a low fever, and chest tightness. There are two main types of bronchitis: acute and chronic.
Most cases of acute bronchitis get better within several days. But your cough can last for several weeks after the infection is gone.
The same viruses that cause colds and the flu often cause acute bronchitis. These viruses spread through the air when people cough, or though physical contact (for example, on unwashed hands). Being exposed to tobacco smoke, air pollution, dusts, vapors, and fumes can also cause acute bronchitis. Less often, bacteria can also cause acute bronchitis.
To diagnose acute bronchitis, your health care provider will ask about your symptoms and listen to your breathing. You may also have other tests.
Treatments include rest, fluids, and aspirin (for adults) or acetaminophen to treat fever. A humidifier or steam can also help. You may need inhaled medicine to open your airways if you are wheezing. Antibiotics won’t help if the cause is viral. You may get antibiotics if the cause is bacterial.
Bronchiolitis causes
Bronchiolitis can be caused by many different viruses, but it’s most often caused by a virus called respiratory syncytial virus (RSV). The respiratory syncytial virus (RSV) spreads through sneezing, coughing or personal contact.
Respiratory syncytial virus (RSV) infections are responsible for more than half of all cases of bronchiolitis. Other viruses associated with bronchiolitis include rhinovirus (the common cold virus), influenza (flu), human metapneumovirus, adenovirus, coronavirus, and parainfluenza.
Childcare attendance and exposure to cigarette smoke also can increase a child’s risk for bronchiolitis.
What is respiratory syncytial virus (RSV)?
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis (inflammation of the small airways in the lungs) and pneumonia in babies. It is an illness that often occurs in yearly outbreaks in communities, school classrooms, and day care centers. In the United States, RSV is more common in winter and spring months.
What causes respiratory syncytial virus (RSV)?
Respiratory syncytial virus (RSV) is spread from respiratory secretions through close contact with infected people or contact with contaminated surfaces or objects. Infection can occur when infectious material contacts mucous membranes of the eyes, mouth, or nose, and possibly through the inhalation of droplets generated by a sneeze or cough. The incubation period (time from exposure to symptoms) is about four to six days.
Who is affected by respiratory syncytial virus (RSV)?
RSV can affect a person of any age, although it is most common in babies between 2 and 8 months old. Most babies have been infected at least once by the time they are 2 years old. Babies can also be reinfected with the virus. Recurrence throughout life is common. Babies born prematurely or with chronic lung disease are at increased risk of developing more severe illness.
Why is respiratory syncytial virus (RSV) a concern?
In babies born prematurely, or who have certain heart, lung, and neuromuscular diseases, infection with the virus can lead to severe respiratory illness and pneumonia, and may become life-threatening. RSV in infancy may be related to development of asthma later in childhood.
What are the symptoms of respiratory syncytial virus (RSV)?
The early phase of RSV in infants and young children is often mild, somewhat like a cold. In children younger than 3, the disease may progress into the lower airways and cause coughing and wheezing. In some, the infection progresses to a severe respiratory disease requiring hospitalization to help the child breathe.
The following are the most common symptoms of RSV. However, each baby may experience symptoms differently. Symptoms may include:
- Runny nose
- Fever
- Cough
- Apnea (short periods without breathing)
- Listlessness
- Poor feeding
- Wheezing
- Retractions (pulling in) of the chest wall
- Rapid breathing; turning blue around the lips
The symptoms of RSV may resemble other conditions or medical problems. Always consult your baby’s doctor for a diagnosis.
How is respiratory syncytial virus (RSV) diagnosed?
Diagnosis is sometimes difficult because the symptoms of RSV can resemble other infections. Illness in other family members, other babies in the hospital nursery, or the time of year may provide clues. In addition to a complete medical history and physical examination of your child, a test (nasal swab or nasal wash) of the baby’s respiratory secretions may show the presence of a virus.
What is the treatment for respiratory syncytial virus (RSV)?
Specific treatment for RSV will be determined by your baby’s doctor based on:
- Your baby’s age, overall health, and medical history
- The extent of the condition
- Your baby’s tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
There are no medications used to treat the virus itself. Care of a baby with RSV involves treating the effects of the virus on the respiratory system. Because a virus causes the illness, antibiotics are not useful. Treatment may include:
- Supplemental oxygen
- Intravenous fluids (to prevent dehydration)
- Tube feedings (if the baby has difficulty sucking)
- Bronchodilator medications (to open the airways)
- Antiviral medications (for very sick or high-risk babies)
How can respiratory syncytial virus (RSV) be prevented?
The CDC and the American Academy of Pediatrics recommend that babies at high risk for RSV receive the medication palivizumab (Synagis) to protect them against the serious complications of the illness. High-risk babies include those born prematurely and those with heart, lung, or neuromuscular diseases. Palivizumab is a monoclonal antibody that is usually given monthly during the RSV “season” from late fall through spring.
Palivizumab is not a vaccine and does not prevent the virus. But it does lessen the severity of the illness and may help shorten the hospital stay.
In addition, contacts with your baby should wash their hands with warm soapy water prior to holding your baby. Keep your baby away from tobacco smoke as well as crowded areas like malls. Vaccinate your children each year against influenza starting at age 6 months.
Bronchiolitis prevention
The best way to prevent the spread of viruses that can cause bronchiolitis is frequent hand washing by parents, caregivers and your child. Also wash or wipe toys and surfaces regularly. It may help to keep infants away from others who have colds or coughs. Avoid taking young babies into crowded places, especially confined areas such as shopping centers, and avoid close contact with people who have cold symptoms. Babies who are exposed to cigarette smoke are more likely to develop severe bronchiolitis compared with those from smoke-free homes. So it’s important to protect children from secondhand smoke.
There’s no bronchiolitis vaccine available yet, but a medication can be given to ease the severity of the disease. It’s recommended only for infants at high risk of severe disease, such as those born very prematurely or those with chronic lung or heart disease. The medicine, which contains antibodies to RSV, is given as an injection monthly during peak RSV season.
Preventing bronchiolitis in high-risk children
Children with a high risk of developing severe bronchiolitis may be able to have monthly antibody injections during the winter (November to March).
Children considered to be at high risk include those:
- born very prematurely
- born with a heart or lung condition
- with an immune deficiency (weakened immune system)
The injections may help limit the severity of bronchiolitis if your child becomes infected. But they can be expensive.
Speak to your doctor if you think your child has an increased risk of developing severe bronchiolitis.
Bronchiolitis symptoms
When bronchiolitis starts, bronchiolitis symptoms look a bit like a cold. They include a runny nose and sneezing, a mild cough and sometimes a fever.
As bronchiolitis develops, your child’s breathing might become fast and laboured and her cough might get more severe.
You might notice signs that your child is working hard to breathe – for example, his ribs moving in and out more than usual, and his nostrils flaring. You might also hear a high-pitched whistling sound called a ‘wheeze’ when your child breathes out. In severe cases, your child’s lips might look blue.
Your child might be hard to feed and she might get quite upset.
Bronchiolitis is usually at its worst on the second or third day, but it can last for up to 10 days. As your baby improves, the wheezing and the fast breathing settles. The cough can last longer.
Bronchiolitis is most common in babies and young children.
Bronchiolitis has similar symptoms to asthma, but it’s a different condition and needs different treatment.
The first symptoms of bronchiolitis are usually the same as those of a common cold:
- stuff nose and congestion
- runny nose
- cough
- fever
These symptoms last a day or two and are followed by worsening of the cough and wheezing (high-pitched whistling noises when exhaling).
Sometimes, more severe respiratory difficulties gradually develop. Signs to watch for include:
- fast, shallow breathing
- a rapid heartbeat
- retractions — when the areas below the ribs, between the ribs, and in the neck sink in as a child inhales
- flaring of the nostrils
- irritability, with difficulty sleeping and signs of fatigue (tiredness) or lethargy
- vomiting after coughing
- poor appetite or not feeding well, causing decreased peeing and fewer wet diapers
Less commonly, babies (especially preemies) may have episodes where they briefly stop breathing (called apnea) before developing other symptoms.
In severe cases, symptoms may worsen quickly. A child with severe bronchiolitis may get very tired from the work of breathing and have poor air movement in and out of the lungs due to the clogging of the small airways. The skin can turn blue (called cyanosis), which is especially noticeable in the lips and fingernails.
Beware of dehydration
Sometimes these symptoms can lead to dehydration. Your baby may be coughing so much and having such difficulty breathing that it is hard for them to drink. Children can quickly become dehydrated if they do not get enough to drink. Offer small amounts of fluids regularly so that your child does not get too tired when feeding and is less likely to become dehydrated.
Bronchiolitis complications
If your child develops complications from bronchiolitis, it’s likely that they’ll need hospital treatment.
Potential complications of bronchiolitis include:
- cyanosis (a blue tinge to the skin caused by a lack of oxygen)
- dehydration (when the normal water content of the body is reduced)
- fatigue (extreme tiredness and a lack of energy)
- severe respiratory failure (an inability to breathe unaided)
In rare cases, bronchiolitis can be accompanied by a bacterial lung infection called pneumonia. Pneumonia will need to be treated separately.
Contact your doctor immediately if any of these complications occur.
In some cases (for example, if your child is having severe breathing difficulties) you’ll need to dial your local emergency services number and ask for an ambulance so your child can be taken to hospital.
Who’s at risk of complications?
Although serious complications are rare, around 45,000 children with bronchiolitis are admitted to hospital each year for further monitoring or treatment.
If your child was born with a health problem, such as a heart or lung condition, there’s an increased risk of complications from bronchiolitis.
Their symptoms may be more severe and come on very rapidly.
The infection may also make any symptoms of your child’s underlying health problem worse.
Long-term effects of bronchiolitis
Bronchiolitis doesn’t usually cause long-term breathing problems, but it can damage the cells in your child’s airways.
This damage can last for 3 to 4 months in some children, causing persistent wheezing and coughing.
Respiratory conditions in later life
There may be a link between bronchiolitis and developing respiratory conditions such as asthma in later life. But the link isn’t fully understood.
It’s not clear whether having bronchiolitis as an infant increases your risk of developing asthma later in life, or whether there are environmental or genetic (inherited) factors that cause both bronchiolitis and asthma.
If your child has repeated bouts of bronchiolitis, their risk of developing asthma later in life may be increased.
Bronchiolitis diagnosis
See your doctor if your child has symptoms of bronchiolitis. A diagnosis is usually based on the symptoms and an examination of your child’s breathing.
Your doctor may ask if your child has had a runny nose, cough or high temperature and for how long. This will help confirm whether they have the symptoms of bronchiolitis.
They’ll listen to your child’s breathing using a stethoscope to check for any crackling or high-pitched wheezing as your child breathes in and out.
If your child hasn’t been feeding very well or has been vomiting, your doctor may also look for signs of dehydration.
These include:
- a dipped fontanelle (the soft spot on the top of the head) in babies
- a dry mouth and skin
- drowsiness
- producing little or no urine
Your doctor may recommend that your child is admitted to hospital if they aren’t feeding properly and are dehydrated, or they’re having problems breathing.
Further tests
Further tests for bronchiolitis aren’t usually necessary. But as some conditions cause similar symptoms to bronchiolitis, such as cystic fibrosis and asthma, tests may be needed.
If it isn’t clear what’s causing your child’s symptoms, or your child has signs of severe bronchiolitis, your doctor may recommend further tests in hospital to help confirm the diagnosis.
These tests might include:
- a mucus sample test (where a sample of mucus from your child’s nose will be tested to identify the virus causing their bronchiolitis)
- urine or blood tests
- a pulse oximeter test (where a small electronic device is clipped to your child’s finger or toe to measure the oxygen in their blood)
Bronchiolitis treatment
If your child’s bronchiolitis is mild, you’ll be able to manage it at home:
- If your breastfed child is younger than six months, offer extra breastfeeds.
- If your formula-fed child is younger than six months, offer him his usual amount of formula. You might need to feed him smaller amounts more frequently if he’s unwell.
- If your child is older than six months, keep breastfeeding or bottle-feeding. You can also offer your child clear fluids, like water. If your child isn’t hungry while she has a fever, that’s OK.
- Give your child paracetamol according to directions if he has a fever.
- Ensure that your child gets as much rest as possible.
- Make sure your child is in a smoke-free environment. Also avoid contact with other babies and children in the first few days, because bronchiolitis is an infectious disease.
You child doesn’t need antibiotics, because bronchiolitis is caused by a virus, and antibiotics don’t cure viruses.
If your child’s bronchiolitis is more serious, she might need to go to hospital. This is usually because she isn’t feeding properly, has become dehydrated, or needs oxygen. Your doctor will tell you whether your child needs to go to hospital.
Your child might need fluids via a nose tube or a drip into a vein in his arm. Sometimes your child might be given asthma medication like Ventolin®. This might help some children breathe more easily by opening up their airways, but it’s generally not effective in children younger than six months of age.
The medicine palivizumab (Synagis) – a monoclonal antibody against RSV – may help decrease the likelihood of bronchiolitis in babies who are at high risk of having a severe illness.
Home remedy
Most babies with bronchiolitis can be managed at home.
- Do not smoke in the home or around your baby. This is especially important around babies with any breathing problems.
- Encourage your baby to rest.
- Give shorter breast feeds/formula/water more frequently. This way your baby does not get too tired when feeding. If your child does not get enough fluids they can get dehydrated.
- You can give Paracetamol (e.g., acetaminophen) if your baby has a temperature and is unsettled.
- Avoid contact with other babies in the first few days, as bronchiolitis is an infectious disease.
- Hand washing helps with the prevention of spread of the virus.
If your baby is distressed and having trouble feeding they may need to be admitted to hospital.
The best treatment for most kids is time to recover and plenty of fluids. Making sure a child drinks enough fluids can be tricky, though, because infants with bronchiolitis may not feel like drinking. They should be offered fluids in small amounts often.
Indoor air, especially during winter, can dry out airways and make the mucus stickier. Some parents use a cool-mist vaporizer or humidifier in the child’s room to help loosen mucus in the airway and relieve cough and congestion. If you use one, clean it daily with household bleach to prevent mold build-up. Avoid hot-water and steam humidifiers, which can be hazardous and can cause scalding.
To clear nasal congestion, try a bulb syringe and saline (saltwater) nose drops. This can be especially helpful just before feeding and sleeping. Sometimes, keeping a child in a slightly upright position may help ease labored breathing.
Acetaminophen can be given to reduce fever and make your child more comfortable. Be sure to give the appropriate dose based on your child’s weight.
Keep your child upright
Keeping your child upright may make their breathing easier and may be useful when they’re trying to feed.
If your child has a nap in an upright position, make sure their head doesn’t fall forward by supporting it with something, such as a rolled-up blanket.





{kind=link}