Contents
What is a bronchoscopy
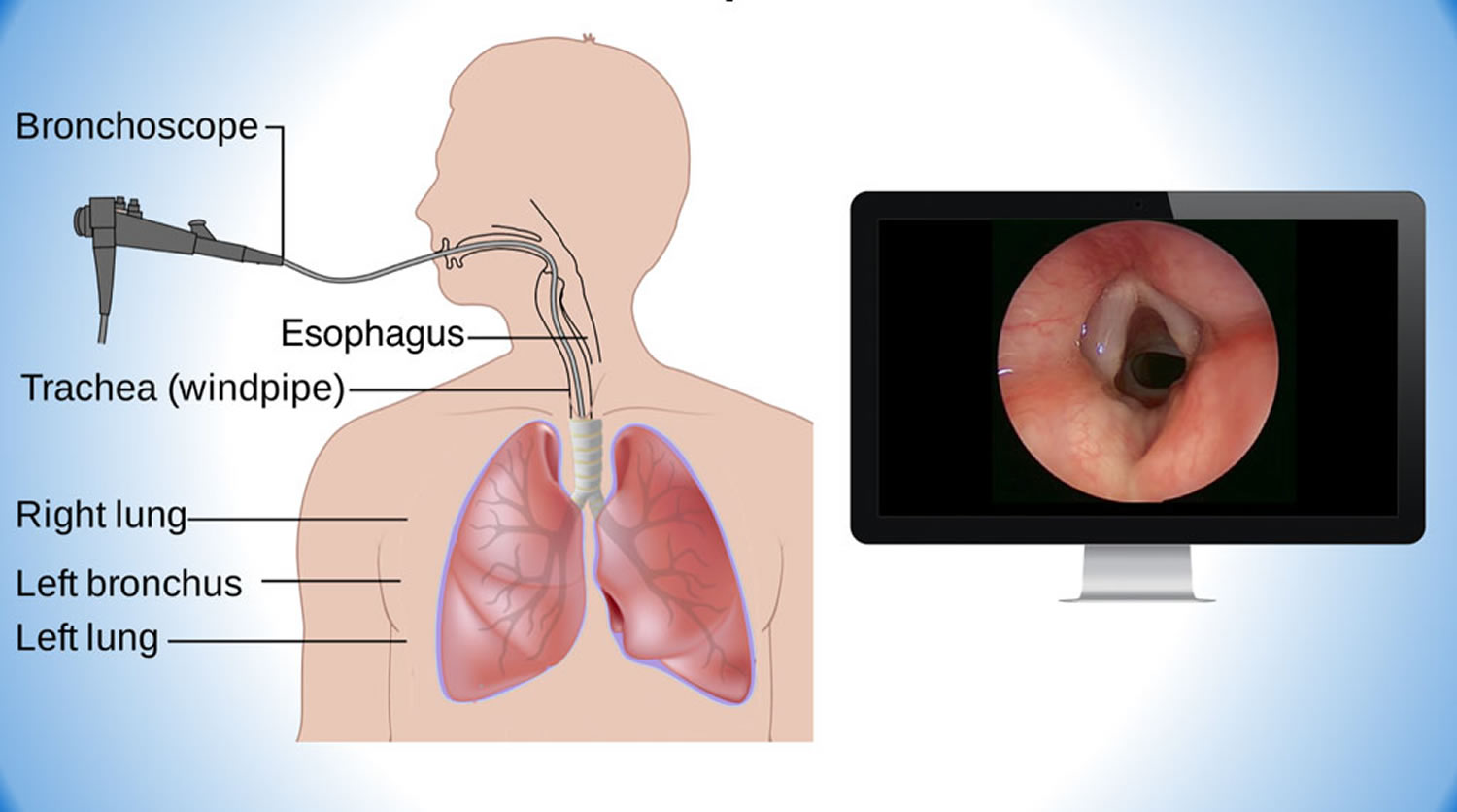
Bronchoscopy is a medical procedure that lets doctors look at your lungs and the interior of the airways. Bronchoscopy is usually performed by a doctor who specializes in lung disorders (a pulmonologist). During bronchoscopy, a thin tube attached to a camera called a bronchoscope, is passed through your nose or mouth, down your throat and into your lungs. The bronchoscope allows the doctor to see your airways and take photographs or videos of the trachea, main stem bronchi, and some of the small bronchi. The bronchoscope also allows doctors to take a sample of the tissue there, which is known as a biopsy. In children, bronchoscopy procedure may be used to remove foreign objects that have been inhaled. In adults, the bronchoscopy procedure is most often used to take samples of (biopsy) suspicious lesions and for culturing specific areas in the lung.
Bronchoscopy is most commonly performed using a flexible bronchoscope. However, in certain situations, such as if there’s a lot of bleeding in your lungs or a large object is stuck in your airway, a rigid bronchoscope may be needed.
Common reasons for needing bronchoscopy are persistent cough, infection and something unusual seen on a chest X-ray or other test.
Bronchoscopy can also be used to obtain samples of mucus or tissue, or to remove foreign bodies or other blockages from the airways or lungs.
A bronchoscopy is normally performed under mild sedation, so you are awake but feel relaxed and drowsy during the procedure.
Before the procedure, your doctor will give you a local anaesthetic so that you do not feel pain. This is usually a spray or a gargle. You might also be given an injection to make you drowsy.
It might be slightly uncomfortable to have the tube inserted. It will probably be in your airways for 20 minutes or less. You will be able to breathe.
After the bronchoscopy, you will spend some time in recovery waiting for the anaesthetic and sedative to wear off.
For a few days, you might feel an irritation in your throat. But it should go away.
How long does a bronchoscopy take?
The entire bronchoscopy procedure, including prep and recovery time, typically takes about four hours. Bronchoscopy itself usually lasts about 30 to 60 minutes.
Are bronchoscopies safe?
For most people a bronchoscopy is a safe procedure, but like with any medical test there are some risks, such as:
- bleeding
- infection
- difficulty breathing afterwards
In rare cases, you can get a collapsed lung. If this happens, it can be treated immediately by your doctor.
What is a bronchoscopy used to diagnose
Bronchoscopy is usually done to find the cause of a lung problem. For example, your doctor might refer you for bronchoscopy because you have a persistent cough or an abnormal chest X-ray or computerized tomography (CT) scan result.
Your doctor may ask you to undergo a bronchoscopy to help diagnose or investigate:
- An imaging test showed abnormal changes of your lung, such as a growth or tumor, changes or scarring of lung tissue, or collapse of one area of your lung.
- Lung disease, with symptoms such as wheezing, chronic cough, or shortness of breath
- A tumor
- Fever
- To biopsy lymph nodes near your lungs.
- To explain shortness of breath or low oxygen levels
- To see why you are coughing up blood.
- To see if there is a foreign object in your airway.
- You have a cough that has lasted more than 3 months without any clear cause.
- You have an infection in your lungs and major airways (bronchi) that cannot be diagnosed any other way or need a certain type of diagnosis.
- You inhaled a toxic gas or chemical.
- To see if a lung rejection after a lung transplant is occurring.
You may also have a bronchoscopy to treat a lung or airway problem. For example, it may be done to:
- Remove fluid or mucus plugs from your airways
- Remove a foreign object from your airways
- Widen (dilate) an airway that is blocked or narrowed
- Drain an abscess
- Treat cancer using a number of different techniques
- Wash out an airway
In people with lung cancer, a bronchoscope with a built-in ultrasound probe may be used to check the lymph nodes in the chest. This is called endobronchial ultrasound (EBUS) and helps doctors determine the appropriate treatment. EBUS bronchoscopy may be used for other types of cancer to determine if the cancer has spread.
Bronchoscopy can also treat some medical problems. It can be used to remove obstructions or tumors from the air passages or lungs, or to place a small tube to hold open an airway (stent). In these instances, special devices may be passed through the bronchoscope, such as a laser or electrocautery probe for controlling bleeding.
Human lung anatomy
Right lung
The right lung has three lobes and two fissures. Normally, the lobes are freely movable against each other because they are separated, almost to the hilum, by invaginations of visceral pleura. These invaginations form the fissures:
- The oblique fissure separates the inferior lobe (lower lobe) from the superior lobe and the middle lobe of the right lung.
- The horizontal fissure separates the superior lobe (upper lobe) from the middle lobe.
The approximate position of the oblique fissure on a patient, in quiet respiration, can be marked by a curved line on the thoracic wall that begins roughly at the spinous process of the vertebra TIV level of the spine, crosses the fifth interspace laterally, and then follows the contour of rib VI anteriorly.
The horizontal fissure follows the fourth intercostal space from the sternum until it meets the oblique fissure as it crosses rib V.
The orientations of the oblique and horizontal fissures determine where clinicians should listen for lung sounds from each lobe. The largest surface of the superior lobe is in contact with the upper part of the anterolateral wall and the apex of this lobe proj ects into the root of the neck. The surface of the middle lobe lies mainly adjacent to the lower anterior and lateral wall. The costal surface of the inferior lobe is in contact with the posterior and inferior walls.
The medial surface of the right lung lies adjacent to a number of important structures in the mediastinum and the root of the neck. These include the:
- heart,
- inferior vena cava,
- superior vena cava,
- azygos vein, and
- esophagus.
The right subclavian artery and vein arch over and are related to the superior lobe of the right lung as they pass over the dome of the cervical pleura and into the axilla.
Left lung
The left Iung is smaller than the right lung and has two lobes separated by an oblique fissure. The oblique fissure of the left lung is slightly more oblique than the corresponding fissure of the right lung. During quiet respiration, the approximate position of the left oblique fissure can be marked by a curved line on the thoracic wall that begins between the spinous processes of vertebrae T III and T IV, crosses the fifth interspace laterally, and follows the contour of rib VI anteriorly.
As with the right lung, the orientation of the oblique fissure determines where to listen for lung sounds from each lobe. The largest surface of the superior lobe is in contact with the upper part of the anterolateral wall, and the apex of this lobe proj ects into the root of the neck. The costal surface of the inferior lobe is in contact with the posterior and inferior walls.
The inferior portion o f the medial surface of the left lung, unlike the right lung, is notched because of the heart’s projection into the left pleural cavity from the middle mediastinum. From the anterior border of the lower part of the superior lobe a tongue-like extension (the lingula of the left lung) projects over the heart bulge.
The medial surface of the left lung lies adjacent to a number of important structures in the mediastinum and root of the neck. These include the:
- heart,
- aortic arch,
- thoracic aorta, and
- esophagus.
The left subclavian artery and vein arch over and are related to the superior lobe of the left lung as they pass over the dome of the cervical pleura and into the axilla.
Bronchial tree
The trachea is a flexible tube that extends from vertebral level C VI (cervical spine C6) in the lower neck to vertebral level T IV /V (thoracic spine T4-T5) in the
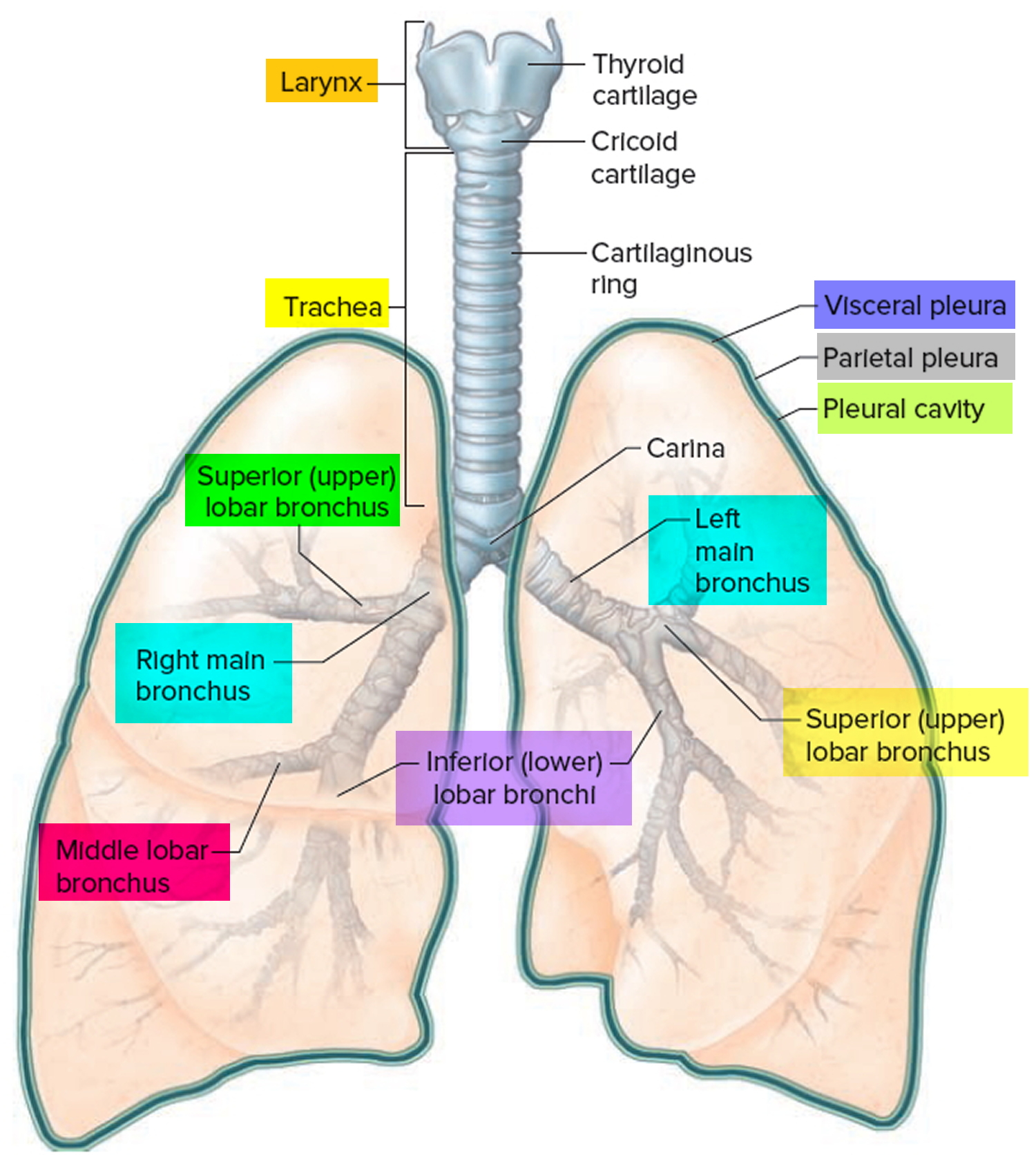
mediastinum where it bifurcates into a right and a left main bronchus. The trachea is held open by C-shaped transverse cartilage rings embedded in its wall the open part of the C facing posteriorly. The lowest tracheal ring has a hook-shaped structure, the carina, that projects backwards in the midline between the origins of the two main bronchi. The posterior wall of the trachea is composed mainly of smooth muscle. Each main bronchus enters the root of a lung and passes through the hilum into the lung itself. The right main bronchus is wider and takes a more vertical course through the root and hilum than the left main bronchus. Therefore, inhaled foreign bodies tend to lodge more frequently on the right side than on the left.
The bronchial tree consists of branched airways leading from the trachea to the microscopic air sacs in the lungs (Figure 3, 5 and 6). Its branches begin with the right and left main (primary) bronchi, which arise from the trachea at the level of the fifth thoracic vertebra. Each bronchus enters its respective lung. A short distance from its origin, each main bronchus divides into lobar (secondary) bronchi. The lobar bronchi branch into segmental (tertiary) bronchi, which supply bronchopulmonary segments. Within each bronchopulmonary segment, the segmental bronchi give rise to multiple generations of divisions of increasingly finer tubes and, ultimately, to bronchioles , which further subdivide to terminal bronchioles, respiratory bronchioles, and finally to very thin tubes called alveolar ducts. These ducts lead to thin-walled outpouchings called alveolar sacs. Alveolar sacs lead to smaller, microscopic air sacs called alveoli (singular, alveolus), which lie within capillary networks (Figure 6). The alveoli are the sites of gas exchange between the inhaled air and the bloodstream.
The structure of a bronchus is similar to that of the trachea, but the tubes that branch from it have less cartilage in their walls, and the bronchioles lack cartilage. As the cartilage diminishes, a layer of smooth muscle surrounding the tube becomes more prominent. This muscular layer persists even in the smallest bronchioles, but only a few muscle cells are associated with the alveolar ducts.
The absence of cartilage in the bronchioles allows their diameters to change in response to contraction of the smooth muscle in their walls, similar to what happens with arterioles of the cardiovascular system. Part of the “fight-or-flight” response, triggered by the sympathetic nervous system, is bronchodilation, in which the smooth muscle relaxes and the airways become wider and allow more airflow. The opposite, bronchoconstriction, occurs when the smooth muscle contracts and it becomes difficult to move air in and out of the lungs. Bronchoconstriction can occur with allergies. Asthma is an extreme example of bronchoconstriction.
The mucous membranes of the bronchial tree continue to filter the incoming air, and the many branches of the tree distribute the air to alveoli throughout the lungs. The alveoli, in turn, provide a large surface area of thin simple squamous epithelial cells through which gases are easily exchanged. Oxygen diffuses from the alveoli into the blood in nearby capillaries, and carbon dioxide diffuses from the blood into the alveoli.
Figure 2. Bronchial tree of the lungs
Bronchopulmonary segments
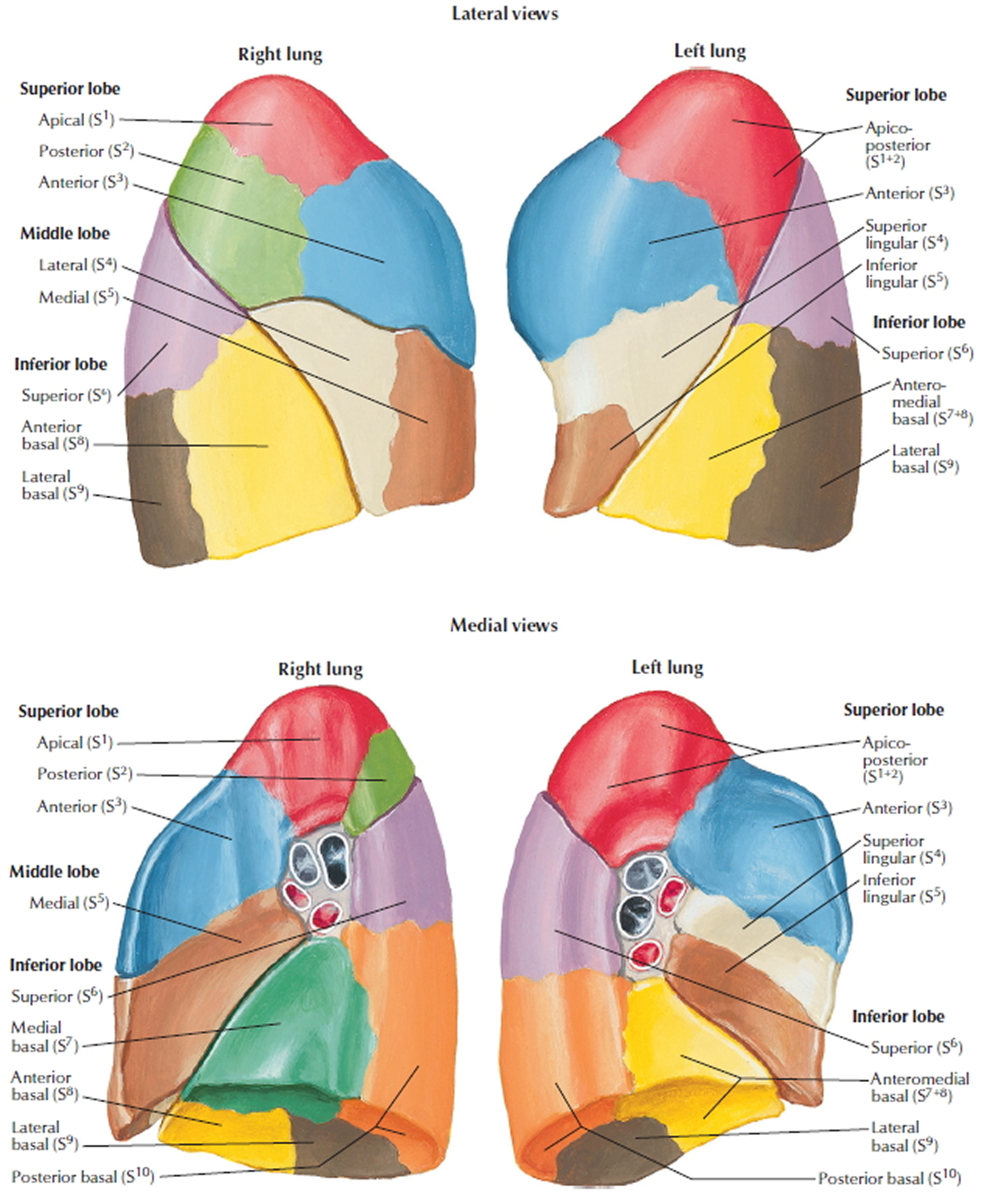
A bronchopulmonary segment is the area of lung supplied by a segmental bronchus and its accompanying pulmonary artery branch. Tributaries of the pulmonary vein tend to pass intersegmentally between and around the margins of segments. Each bronchopulmonary segment is shaped like an irregular cone, with the apex at the origin of the segmental bronchus and the base projected peripherally onto the surface of the lung.
A bronchopulmonary segment is the smallest functionally independent region of a lung and the smallest area of lung that can be isolated and removed without affecting adjacent regions.
There are ten bronchopulmonary segments in each lung; some of them fuse in the left lung.
Figure 3. Bronchopulmonary segments
Lung Alveoli
Each human lung is a spongy mass composed of 150 million little sacs, the alveoli. These provide about 70 m2, per lung, of gas-exchange surface—about equal to the floor area of a handball court or a room about 8.4 m (25 ft) square.
An alveolus is a pouch about 0.2 to 0.5 mm in diameter. Thin, broad cells called squamous (type I) alveolar cells cover about 95% of the alveolar surface area. Their thinness allows for rapid gas diffusion between the air and blood. The other 5% is covered by round to cuboidal great (type II) alveolar cells. Even though they cover less surface area, these considerably outnumber the squamous alveolar cells.
Great (type II) alveolar cells have two functions:
- They repair the alveolar epithelium when the squamous cells are damaged; and
- They secrete pulmonary surfactant, a mixture of phospholipids and protein that coats the alveoli and smallest bronchioles and prevents the bronchioles from collapsing when one exhales.
The most numerous of all cells in the lung are alveolar macrophages (dust cells), which wander the lumens of the alveoli and the connective tissue between them. These cells keep the alveoli free of debris by phagocytizing dust particles that escape entrapment by mucus in the higher parts of the respiratory tract. In lungs that are infected or bleeding, the macrophages also phagocytize bacteria and loose blood cells. As many as 100 million alveolar macrophages perish each day as they ride up the mucociliary escalator to be swallowed and digested, thus ridding the lungs of their load of debris.
Each alveolus is surrounded by a web of blood capillaries supplied by small branches of the pulmonary artery. The barrier between the alveolar air and blood, called the respiratory membrane, consists only of the squamous alveolar cell, the squamous endothelial cell of the capillary, and their shared basement membrane. These have a total thickness of only 0.5 μm, just 1/15 the diameter of a single red blood cell.
It is very important to prevent fluid from accumulating in the alveoli, because gases diffuse too slowly through liquid to sufficiently aerate the blood. Except for a thin film of moisture on the alveolar wall, the alveoli are kept dry by the absorption of excess liquid by the blood capillaries. The mean blood pressure in these capillaries is only 10 mm Hg compared to 30 mm Hg at the arterial end of the average capillary elsewhere. This low blood pressure is greatly overridden by the oncotic pressure that retains fluid in the capillaries, so the osmotic uptake of water overrides filtration and keeps the alveoli free of fluid. The lungs also have a more extensive lymphatic drainage than any other organ in the body. The low capillary blood pressure also prevents rupture of the delicate respiratory membrane.
Figure 4. Lungs alveoli
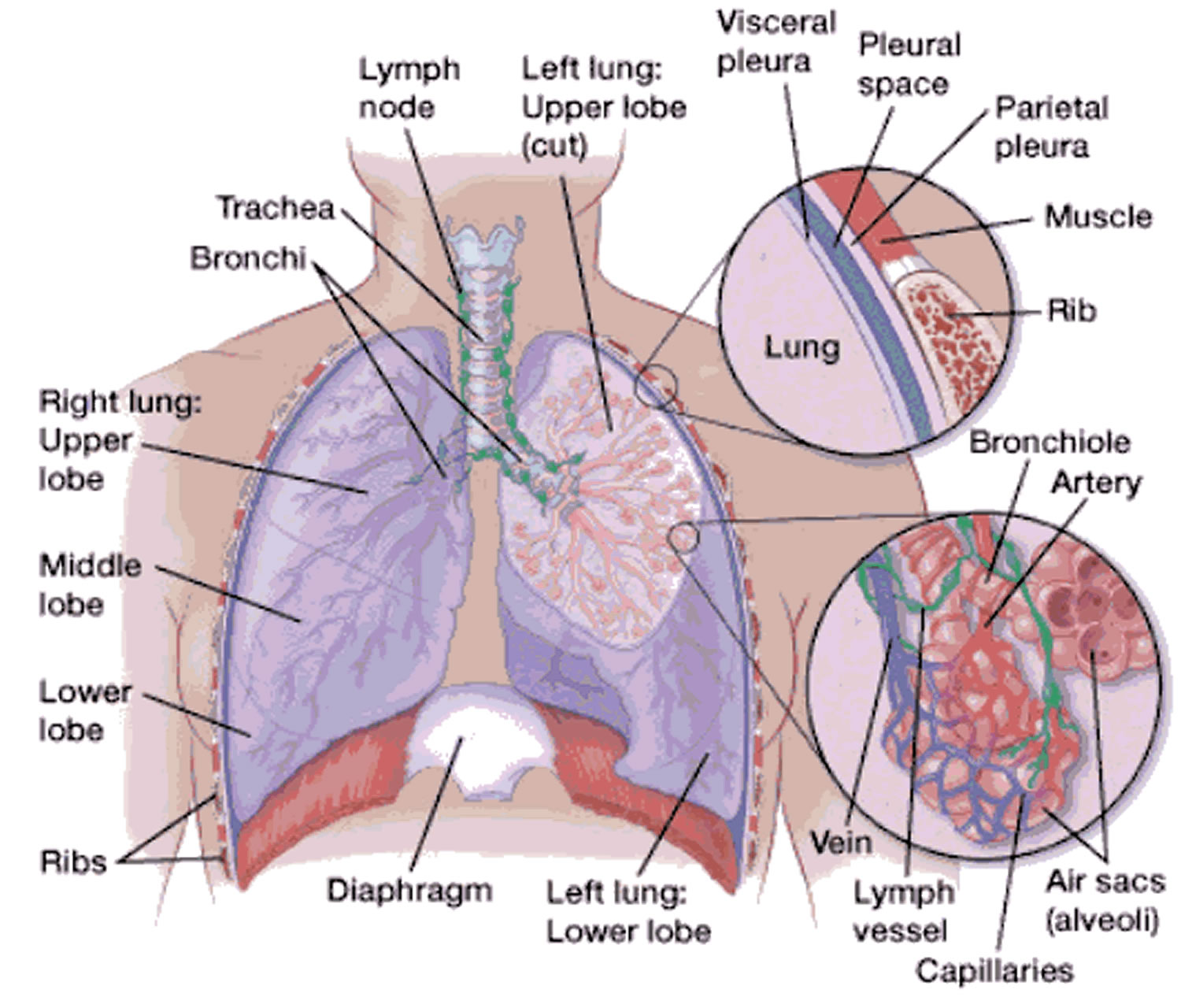 Figure 5. Pulmonary Alveoli (microscopic view)
Figure 5. Pulmonary Alveoli (microscopic view)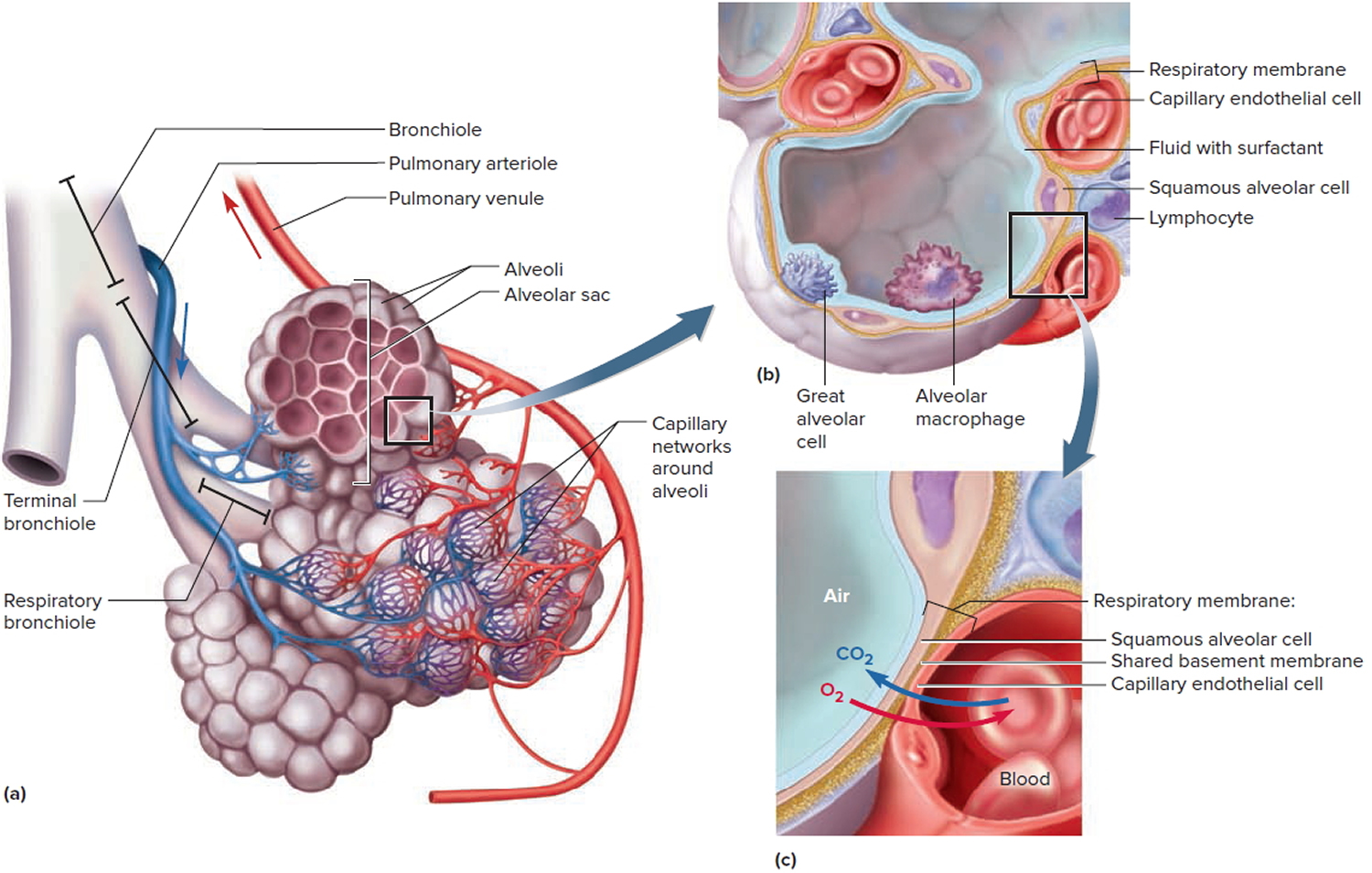
Note: (a) Clusters of alveoli and their blood supply. (b) Structure of an alveolus. (c) Structure of the respiratory membrane.
Bronchoscopy procedure
Bronchoscopy is usually done in a procedure room in a clinic or in a hospital operating room. The entire procedure, including prep and recovery time, typically takes about four hours. Bronchoscopy itself usually lasts about 30 to 60 minutes.
If you are a diabetic who takes insulin, special arrangements may need to be made.
It is wise to arrange for someone to accompany you home after the bronchoscopy procedure because the sedation you may be given for the bronchoscopy could make it unsafe for you to drive or to travel alone on public transport. It is also advisable to arrange for someone to stay with you to keep an eye on you overnight. Please do not bring valuables or wear jewellery to the procedure as this can interfere with x-rays that may be needed.
How you prepare for bronchoscopy
Preparation for bronchoscopy usually involves the following steps:
- Food and medications
You may be asked to stop taking blood-thinning medications (including aspirin, clopidogrel [Plavix] and warfarin [Coumadin, Jantoven]) several days before your bronchoscopy.
You’ll also be asked not to eat or drink for 6 to 12 hours before the bronchoscopy procedure.
- Clothing and personal items
On the day of the procedure, you’ll be asked to put on a gown and take out any dentures, partial dentures or bridges. You may also be asked to remove any dentures, hearing aids, contact lenses or glasses.
- Other precautions
If you’ll be going home after the procedure, you’ll need a friend or family member to take you home. You won’t be able to drive because of the lingering effects of the medications used during the procedure. It’s also a good idea to have someone stay with you for the rest of the day.
During the bronchoscopy procedure
You’ll be asked to sit or lie back on a table or a bed with your arms at your sides. You’ll be connected to a monitor so that the health care team can track your heart rate, blood pressure and oxygen level during the procedure.
A numbing medication will be sprayed in your throat and possibly your nose. This medication, called an anesthetic, this numbs the nose and throat, reducing any discomfort during the bronchoscopy but often makes you cough a little to begin with. It helps to lessen gagging and coughing as the bronchoscope is placed into your throat. The medicine may taste unpleasant but that will go away. You may also be given an injection which dries up the saliva in the mouth.
You may also be given a sedative injection through a vein (intravenously) to help you relax. You’ll feel sleepy, but you’ll still be awake. Sometimes, instead of sedation you may be advised to have a full general anaesthetic.
During bronchoscopy, a thin tube called a bronchoscope is placed in your nose or mouth. The bronchoscope has a light and a very small camera at its tip that displays pictures on a monitor.
The bronchoscope is advanced slowly down the back of your throat, through the vocal cords and into the airways. It may feel uncomfortable, but it shouldn’t hurt. Your health care team will try to make you as comfortable as possible.
When taking samples (biopsy), an x-ray machine is sometimes used to place the bronchoscope in the correct area of the lung. Sometimes, the doctor uses ultrasound to assist in the procedure.
Usually, salty water is washed into the airway and sucked back to retrieve germs or cells (bronchoscopy with collection of bronchoalveolar lavage (BAL) fluid). Immunocompromised hosts with respiratory illnesses often undergo bronchoscopy with BAL (bronchoalveolar lavage) 1. A small brush like a bottle brush and needles or forceps may also be used to collect specimens of the lung or lymph glands in the chest. Sometimes, other more specialized tests are undertaken which will be explained by your doctor. In that case, your doctor may ask you if you have pain in the chest, back or shoulders. In general, you shouldn’t feel pain.
Figure 6. Bronchoscopy procedure (flexible bronchoscopy)
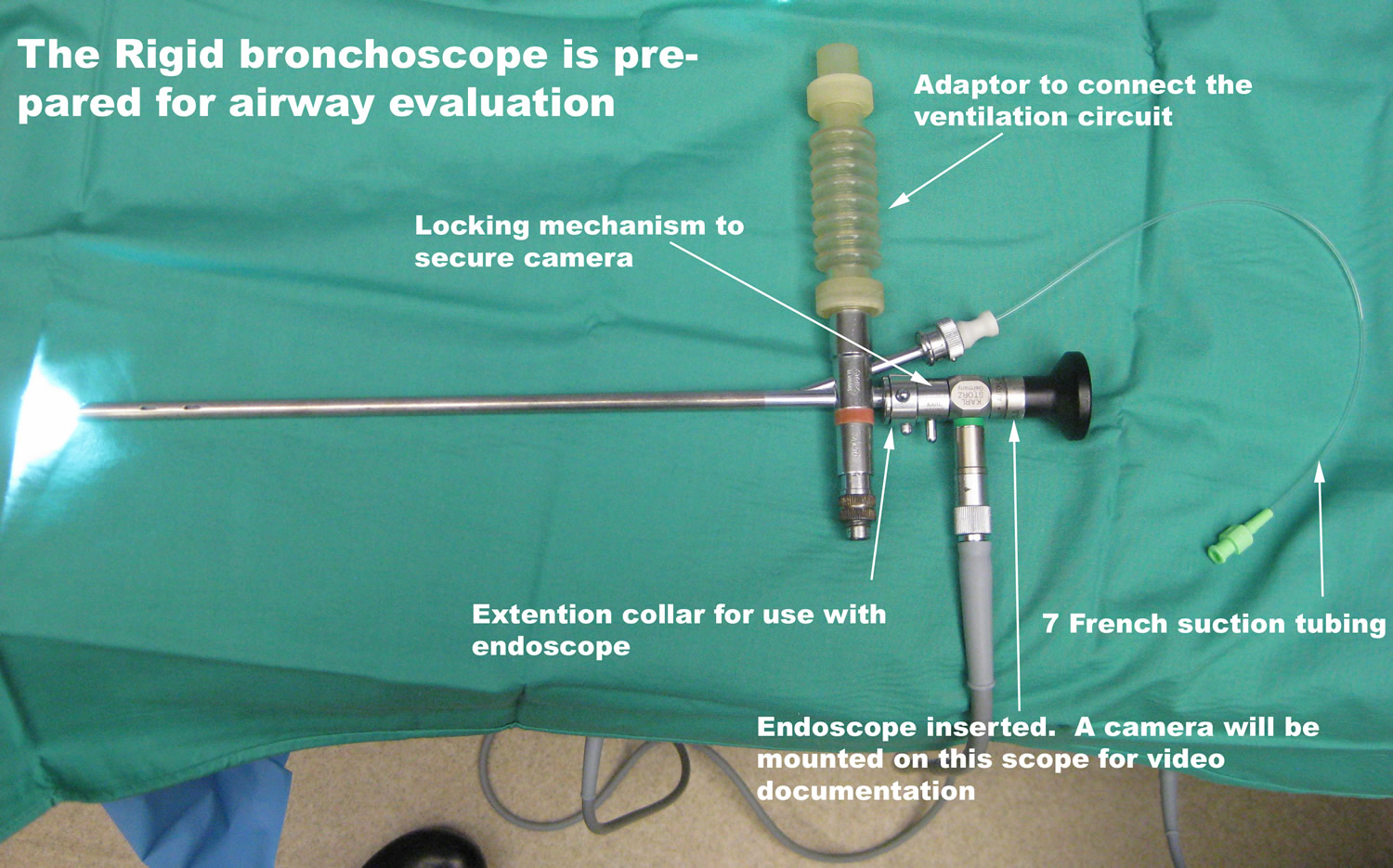
Rigid bronchoscopy
In adults, the primary indications for using the rigid bronchoscopy are central airway obstruction secondary to neoplastic and nonneoplastic pathologies, massive hemoptysis, mucus plugging, and blood clot removal, as well as foreign bodies 2. There has been an expanding interest in the management of central airway obstruction by pulmonologists and this has led to a renewed interest in rigid bronchoscopy 3. More than just treating cancer-related central airway obstruction mechanically, rigid bronchoscopy also makes possible a number of therapies such as laser/photoresection, endobronchial stents, balloon dilation, electrocautery, use of the argon beam, and cryotherapy 4. The wide channel of the rigid bronchoscope lends itself to easier removal of foreign bodies from the airway and debulking of masses, easier control of hemorrhage during therapeutic interventions in the trachea and mainstem bronchi, as well as easier dilation of proximal airways, and easier deployment of stents and other airway implantables, all while allowing for relative ease of ventilation 5.
Unlike fiberoptic flexible bronchoscopy, rigid bronchoscopy is performed in the operating room under general anesthesia. Performing rigid bronchoscopy under general anesthesia adds the potential complication of pulmonologist and anesthesiologist sharing the airway but also adds a degree of safety by allowing the pulmonologist to focus on airway intervention, while the anesthesiologist prevents and manages mechanical and systemic complications as they arise 6. Here the anesthesiologists, with the bronchoscope operator, need to navigate the multiple approaches to airway management, such as apneic oxygenation, spontaneous ventilation (assisted or otherwise), controlled mechanical ventilation, high frequency, and manual jet ventilation 3. Relative contraindications to rigid bronchoscopy include uncontrolled coagulopathy, oxygenation, and ventilator demands that are at the clinical extremes, especially in the hands of an inexperienced operator 7. The type and rate of complications of rigid bronchoscopy are similar to those of flexible fiberoptic bronchoscopy and can likewise be divided into mechanical and systemic complications. Complications in either category can potentially result in death.
Figure 7. Rigid bronchoscopy

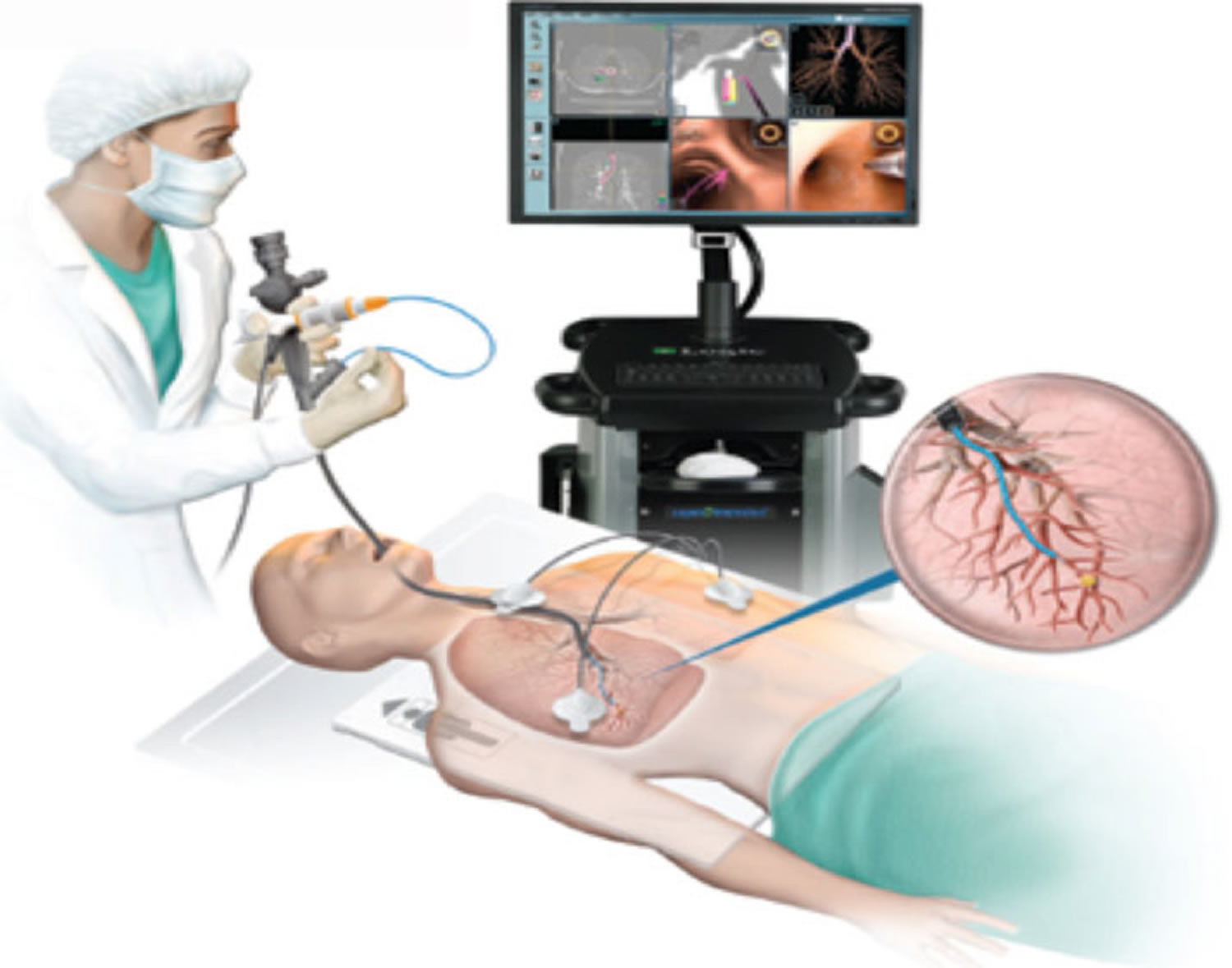
Electromagnetic navigational bronchoscopy has emerged as a diagnostic tool to improve on the yield of current conventional techniques. Electromagnetic navigational bronchoscopy combines conventional and virtual bronchoscopy to enable the guidance of bronchoscopic instruments to target areas within the peripheral lung parenchyma 8. These areas are frequently beyond the reach of standard fiberoptic bronchoscopy.
In essence, electromagnetic navigational bronchoscopy consists of:
- (I) a low-dose electromagnetic field created around the patient;
- (II) software that creates a three-dimensional (3D) virtual bronchial tree;
- (III) a sensor device with navigational capacity that can be located within the magnetic field;
- (IV) an interface to display the position of the sensor within the field and input desired target location;
- (V) an extended working channel that enables accurate placement of ancillary bronchoscopic tools, such as brush, biopsy forceps etc. into the target lesion.
Electromagnetic navigational bronchoscopy is divided into two phases. Firstly a planning phase where thin-slice protocol CT is performed prior to the procedure. The images are analyzed by the software and this produces a virtual road map of the bronchial tree in preparation for the second phase, i.e., the navigational phase.
The locatable guide (LG) is continuously sensed in real time by the magnetic field as it is navigated to the point of interest within the bronchial tree. The reconstructed virtual anatomy helps direct the scope via a suggested route for navigation. The software constantly displays the distance from the lesion. The process of matching the CT images to the patient’s real life anatomy (CT to body divergence) is called registration accuracy; this is measured as an Average Fiducial Target Registration Error and should be less than 5 millimeters (mm). An Average Fiducial Target Registration Error greater than 5 mm signifies unacceptable discrepancy and will lead to reduced navigational accuracy 9. Once sufficient data is available to match the patient’s anatomy to the CT images, the locatable guide is advanced on the pre-planned pathway. The progress and location of the locatable guide is displayed in six simultaneous views as chosen by the operator. Finally, when the target site is reached the extended working channel is locked, the locatable guide is removed and a variety of ancillary tools can be passed through the extended working channel to obtain samples—for example needle aspiration, brush biopsy, and forceps.
Electromagnetic navigational bronchoscopy types
Currently there are two distinct systems that use electromagnetic navigational bronchoscopy. Both systems are based on the same basic principal and consist of an initial planning phase with few minor variations. The i-Logic (Covidien, Mansfield, MA, USA) system generates the magnetic field via a board that is placed underneath the patient and the sensors are maneuverable. The i-Logic locatable guide is available in various angles that is mounted on the extended working channel . The second commercially available system, the SPiNDrive (Veran Medical Technologies, Inc., St Louis, MO, USA) utilizes a magnetic field over the patient. The sensor system is built into the various instruments that are mounted on the extended working channel , thus allowing direct navigation of the biopsy instrument. In addition, this system has a sensor pad that allows additional imaging enhancements to compensate for respiratory movement, which in theory, at least, allows for better bronchoscopic navigation.
Current evidence
In a small retrospective chart review electromagnetic navigational bronchoscopy led to a diagnosis in 77% of lesions where standard bronchoscopic biopsies were unsuccessful. In this study, nearly half (49%) of the lesions were identified as malignant, mostly non-small cell lung cancer 10. In a larger retrospective study of 248 patients, the i-Logic system had a comparatively lower diagnostic yield of 55.7% for peripheral lesions (mean size 2.1±1.4 cm standard deviation and 70% for lymph nodes that were 1.8±0.9 cm 11.
An open-label, prospective, single-group, controlled clinical study with 15 patients demonstrated a 69% diagnostic yield. In this study the majority of these lesions were diagnosed as non-small cell lung cancer 12. The average size of the lesions was 3.35±1.10 cm 13. Similar results were replicated in a larger study (89 patients) by Eberhardt et al 14. This study reported a 67% diagnostic accuracy using electromagnetic navigational bronchoscopy. They also noted a significantly higher yield in diagnosing lesions in the right middle lobe, 88% 14. These results were independent of the size of lesion. Consistent with the previous studies Seijo et al. 15 showed a similar diagnostic yield of 67% in 34 of 51 patients with indeterminate pulmonary lesions. This study had a smaller median size of the nodules at 2.5±1.0 cm, a median distance from the pleural surface of 11 mm and a positive bronchus sign in 74% patients. A higher diagnostic accuracy was seen in lesions with a positive bronchus sign, 79% versus 31% respectively. The sensitivity and specificity of electromagnetic navigational bronchoscopy for malignancy in this study were 71% and 100% respectively 15. Gildea et al. 16, obtained a higher diagnostic accuracy compared to the preceding studies. The diagnostic accuracy was reported at 80.3% overall. However, it should be highlighted that only 57.0% of these lesions were less than 2 cm in diameter and the mean distance to the center of targeted peripheral lesions was 0.9 cm. The diagnostic yield was not significantly affected by lesion size or Average Fiducial Target Registration Error (AFTRE) . A final diagnosis of malignancy was obtained in 74% of cases via electromagnetic navigational bronchoscopy, with the most common diagnosis being non-small cell lung cancer 16. electromagnetic navigational bronchoscopy produced a diagnosis in 25 (62.5%) out of 40 cases. The diagnostic yield of electromagnetic navigational bronchoscopy was significantly greater when data registration accuracy was less than 4 mm (77.2% and 44.4% respectively). The mean lung lesion diameter was 23.5±1.5 mm and depth from the visceral-costal pleura was 14.9±2.0 mm 9.
A recent meta-analysis of 15 trials with a total of 1,033 nodules found a definitive diagnosis was obtained in 64.9% procedures. The sensitivity to detect cancer was 71.1%, with a negative predictive value of 52.1% 17.
Other routinely used techniques such as standard flexible bronchoscopy have a much lower diagnostic yield when compared to electromagnetic navigational bronchoscopy (15% vs. 54%) when sampling peripheral lung lesions less than 2 cm. However the yield of bronchoscopy improves the closer the lesion is to the hilum 13.
The electromagnetic navigational bronchoscopy has been compared to other technologies in a large randomized controlled trial. This study had three arms comparing electromagnetic navigational bronchoscopy, radial probe-endobronchial ultrasound (RP-EBUS), and a combined electromagnetic navigational bronchoscopy and radial probe-endobronchial ultrasound arm. A total of 120 patients were recruited, of which 118 had a definitive histological diagnosis and were included in the final analysis. The diagnostic yield of the combined procedure (88%) was greater than EBUS (69%) or electromagnetic navigational bronchoscopy alone (59%). Of importance, the combined procedures yield was independent of lesion size or lobar distribution 18. In another series by the same authors, the diagnostic yield was much higher (93% vs. 48%) when the lesion could be identified by radial probe-endobronchial ultrasound after navigation to the area with electromagnetic navigational bronchoscopy 19. A similar study evaluated electromagnetic navigational bronchoscopy and peripheral EBUS (pEBUS) alone and in combination. The average diameter of the lesions was 27 mm with an average distance of 20 mm from the pleural surface. The combination of peripheral EBUS and electromagnetic navigational bronchoscopy identified lesions in 93% (56/60) cases compared to 75% (45/60) cases with peripheral EBUS alone. The overall diagnostic yield was 50%, however, in this study the diagnostic yield did not significantly improve with addition of electromagnetic navigational bronchoscopy over peripheral EBUS alone (26/60 vs. 30/60). This low diagnostic rate is unusual given the high success rate in identification of the lesions, 93% 20. These results suggest that combining traditional techniques with electromagnetic navigational bronchoscopy may overcome some of the limitations of the technologies and therefore may allow pulmonologists to achieve a more accurate diagnosis.
Other potential applications of electromagnetic navigational bronchoscopy
This technology may have several other applications including the placement of fiducial markers, guidance for trans-tracheal and trans-bronchial biopsy and bronchoscopic pleural dye marking for localization of lesions pre-surgery. The placement of brachytherapy catheters and markers for radiotherapy has become increasingly useful in the management and the treatment of inoperable lung cancer. This allows for precise delivery of treatment with minimization of side effects to the surrounding healthy lung parenchyma. This role of electromagnetic navigational bronchoscopy was validated in a case series which demonstrated that eight of the nine patients (89%) had successful deployment of fiducial markers, and importantly seven markers were located directly within the tumor. Of a total of 39 placed markers, 35 of these remained in place at 10 days 21 . In another study with 43 patients, 39 cases had the markers in or on the lesion at the time of surgery (90.6%). The mean displacement was 1.67 cm and the mean tumor size 2.78 cm 22.
In another study with 234 markers placed, it was demonstrated that electromagnetic navigational bronchoscopy guided placement of coil spring fiducial markers had better retention rates, with lower complication rates compared to linear fiducial markers 23. Similar safety and efficacy results with the deployment of brachytherapy catheters into inoperable lung cancer via electromagnetic navigational bronchoscopy has also been demonstrated 24. electromagnetic navigational bronchoscopy has also used to place pleural dye markers to allow lesion location at the time of minimal invasive surgery. Krimsky et al. 25 showed that 81% of the patients had visible dye marker at the time of surgical wedge resection and there were no cases requiring conversion to an open procedure. This reduced the conversion rates from a typical 50% with conventional thoracoscopies and reduced the procedural time 26.
The overall safety of electromagnetic navigational bronchoscopy is superior to conventional techniques for the evaluation of the indeterminate pulmonary lesions. A variety of complications have been reported; however the majority of these are minor including hypoxemia or bleeding. To date, no deaths have been reported in the literature. In a large retrospective study, the overall complication rate was 3.20%, with 1.27% of the total 266 patients developing a pneumothorax, making this the commonest complication of electromagnetic navigational bronchoscopy 27. In a large meta-analysis with a total of 1,033 IPN, pneumothorax was seen in 3.6% cases, of which 1.6% required chest tube placement 28. This data has been validated by numerous studies with a reported incidence of pneumothorax ranging from 0–10% 27.
The safety of electromagnetic navigational bronchoscopy has been demonstrated in patients with implantable defibrillators and pacemakers. No cases of fatal arrhythmia or disruption in pacemaker function has been reported 29.
The use of electromagnetic navigational bronchoscopy to place fiducial markers is associated with a lower complication rate compared to trans-cutaneous implantation of these devices 30. Thus electromagnetic navigational bronchoscopy seems to be well tolerated when compared to other traditional methods. The biggest advantage of electromagnetic navigational bronchoscopy over trans thoracic needle aspiration is its superior safety profile. Because the pleural is not breached with transbronchial biopsy, the pneumothorax rates are considerably lower than trans thoracic needle aspiration ranging between 0% to 10% 31.
Factors influencing outcomes of electromagnetic navigational bronchoscopy
The navigation phase during electromagnetic navigational bronchoscopy is deemed successful in 90% of cases, yet the overall diagnostic yield remains significantly lower at 70% 11. There are numerous factors that affect this, as discussed below.
A higher CT-body divergence results in a higher AFTRE obviously results in poor virtual visualization of the airway and poor navigation. This reduces the diagnostic yield and leads to higher complication rates. Recently a new i-Logic software update has reduced the need for manual adjustments resulting in automation and a higher registration accuracy. This eliminates the need to mark numerous pre-defined points for alignment of the CT images with the real time anatomy. However no efficacy data is available for this to date.
User technique and patient sedation also play a role in the outcome of electromagnetic navigational bronchoscopy. No conclusive data is available regarding the optimal sedation method. There is no statistically significant differences in diagnostic yield reported in two studies performed by Eberhardt et al. These studies compared conscious sedation to general anesthesia and reported diagnostic accuracies of 67% vs. 76%, P=0.28 and 64% vs. 70% respectively 32. Another study showed that inhalational anesthesia could also be used for electromagnetic navigational bronchoscopy 33. However these results do not demonstrate superiority of one anaesthetic method over another and therefore the choice of anaesthetic method is determined by patient co-morbidities, operator experience and anaesthetist availability.
However the main factor affecting the outcome are the characteristics of the lesion itself. Lesions located in the right upper or middle lobes have higher diagnostic yield 27. Traditionally these lobes are difficult to examine with conventional bronchoscopy. The presence of a bronchus sign favorably impacts the diagnostic yield. The yield was shown to double from 30% to 60% when a positive sign was present for peripheral pulmonary nodules 30). In a single center study with 51 patients the overall diagnostic yield was 67% in 34 procedures. However sub-analysis demonstrated that the electromagnetic navigational bronchoscopy was diagnostic in 79% (30/38) patients with a bronchus sign on CT imaging but only in 4/13 (31%) without an identifiable bronchus sign 31.
As mentioned above, numerous studies of varying sizes have shown that the combination of electromagnetic navigational bronchoscopy with other modalities like fluoroscopy or radial probe-endobronchial ultrasound increase the diagnostic yield as compared to either method alone. A combined procedure raised the diagnostic yield by 29% 34. However despite the increase in diagnosis, this has not been statistically significant in all studies 35 .
The location of the nodule is also an important factor in the outcome. It has been shown that the further the lesion is to the periphery, the lower the yield. Central, intermediate, and peripheral lesions were associated with diagnostic yields 82%, 61%, and 53%, respectively. This difference was statistically significant. The diagnostic yield of bronchoscopy was 14% (2 of 14) when lesions were less than 2 cm and peripherally located, as compared to 31% (5 of 16) when lesions were greater than 2 cm and intermediately located 36. The use of filtered cigarettes has resulted in an increased incidence of peripheral opacities 37. Peripheral lesion less than 2 cm have a lower diagnostic yield compared to lesions greater than 2 cm 38. In a pooled study with similar predetermined cut off sizes, lesions less than 2 cm were associated with a lower diagnostic yield when compared to lesions greater than 2 cm (56.3% vs. 77.7%) 39. However another study showed that the location of the lesions had no further independent effect on the yield of bronchoscopy if the lesions were greater than 2 cm in size. The yield was 28% when the diameter was less than 2 cm compared to 64% if the diameter was greater than or equal to 2.0 cm 40. Best results were seen when lesions were greater than 5 cm from the hilum (67% positive yield) 41. The choice of ancillary tools may also affect the performance and accuracy of electromagnetic navigational bronchoscopy. When compared to forceps biopsy, catheter aspiration had a higher success rate (22/40 vs. 36/40). In this study 75.5% of the samples were diagnostic. However, in lesions not seen with ultrasound, suction catheter was diagnostic in 100% compared to only 33% with forceps biopsy 33. Even with standard bronchoscopy a needle brush (a cytology brush with a needle tip) had a higher diagnostic yield than transbronchial needle aspirate, regular cytology brush or transbronchial forceps biopsy 42.
After the bronchoscopy procedure
You’ll be monitored for several hours after bronchoscopy. Your mouth and throat will probably be numb for 1-2 hours. You won’t be allowed to eat or drink until the numbness wears off. This helps keep food and liquids from entering your airways and lungs.
You will be kept under nursing supervision during this time. Sometimes, after special biopsies of the lung tissue, you may be advised to have an x-ray. If you are being tested for tuberculosis, you may be required to wear a mask or stay in the recovery room with a nurse after the bronchoscopy procedure.
Because of the sedative you receive, you must check with your doctor about how long you should wait before driving, using machinery, using public transport, going back to work, signing legal documents etc.
When your mouth and throat are no longer numb and you’re able to swallow and cough normally again, you can have something to drink. Start with sips of water. When you can swallow normally, you may eat soft foods, such as soup and applesauce. Add other foods as you feel comfortable.
You may have a mild sore throat, hoarseness, cough or muscle aches. This is normal. Warm water gargles and throat lozenges can help lessen the discomfort. Just be sure all the numbness is gone before you try sucking on lozenges or gargling.
A slight fever and cough is not uncommon for 1-2 days. If you get any more serious side-effects, please let your doctor know. If biopsies were taken during the bronchoscopy procedure, it is common to experience a slight red color to your sputum, however if, post bronchoscopy procedure, you cough up blood and the amount is larger than a quarter coin, please let your doctor know.
Call your doctor right away if you:
- Fever of 100.4 °F (38 °C) or higher
- Have a fever that lasts more than a few days
- Have increasing chest pain
- Have trouble breathing
- Cough up more than a few tablespoons of blood
- Redness or swelling of the IV site
- Blood or other fluid leaking from the IV site
- Severe hoarseness
- Trouble breathing
Bronchoscopy results
It often takes a few days for all the specimens/samples to be checked in the laboratory so your doctor may not be able to give you an accurate diagnosis on the day of the bronchoscopy. Results of tests for tuberculosis can take up to 6 weeks or more. Your doctor will usually discuss the bronchoscopy results with you one to three days after the procedure. Your doctor will use the results to decide how to treat any lung problems that were found. It’s also possible that you may need other tests.
If a biopsy was taken during the bronchoscopy, it will need to be reviewed by a pathologist. Because the tissue samples need special preparation, some results take longer than others to return. Some biopsy specimens will need to be sent for genetic testing, which might take two weeks or more.
Normal Results
Normal results mean normal cells and fluids are found. No foreign substances or blockages are seen.
What Abnormal Results Mean
Many disorders can be diagnosed with bronchoscopy, including:
- Infections from bacteria, viruses, fungi, parasites, or tuberculosis.
- Lung damage related to allergic-type reactions.
- Lung disorders in which the deep lung tissues become inflamed due to the immune system response, and then damaged. For example, changes from sarcoidosis or rheumatoid arthritis may be found.
- Lung cancer, or cancer in the area between the lungs.
- Narrowing (stenosis) of the trachea or bronchi.
- Acute rejection after a lung transplant.
Bronchoscopy risks
Complications from bronchoscopy are uncommon and usually minor, although they may rarely be severe. Complications may be related to the procedure itself or to the sedative or numbing medicine.
- Bleeding. Bleeding is more likely if airways are inflamed or damaged by disease, or if a biopsy was taken. Usually, bleeding is minor and stops without treatment.
- Collapsed lung. In rare cases, an airway may be injured during bronchoscopy. If the lung is punctured, air can collect in the space around the lungs, which can cause one or both lungs to collapse. Usually this problem is easily treated, but it may require admission to the hospital.
- Fever. Fever is relatively common after bronchoscopy but is not always a sign of infection. Treatment is generally not needed.
Main bronchoscopy complications are:
- Bleeding from biopsy sites
- Infection
There is also a small risk of:
- Abnormal heart rhythms
- Breathing difficulties
- Fever
- Heart attack, in people with existing heart disease
- Low blood oxygen
- Collapsed lung
- Sore throat
Risks when general anesthesia is used include:
- Muscle pain
- Change in blood pressure
- Slower heart rate
- Nausea and vomiting
Table 1. Complications of fiberoptic bronchoscopy
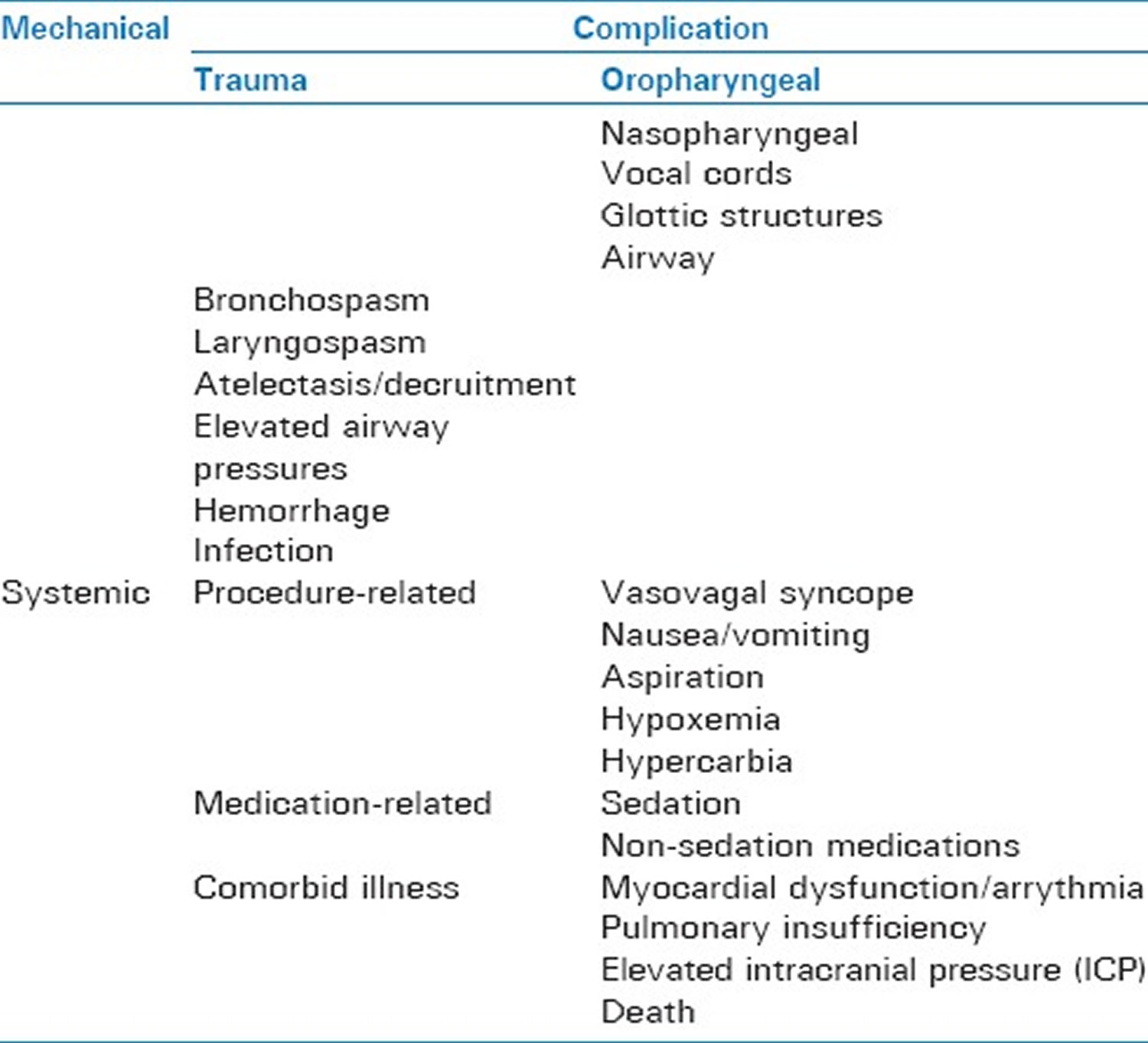
Table 2. Complications of rigid bronchoscopy
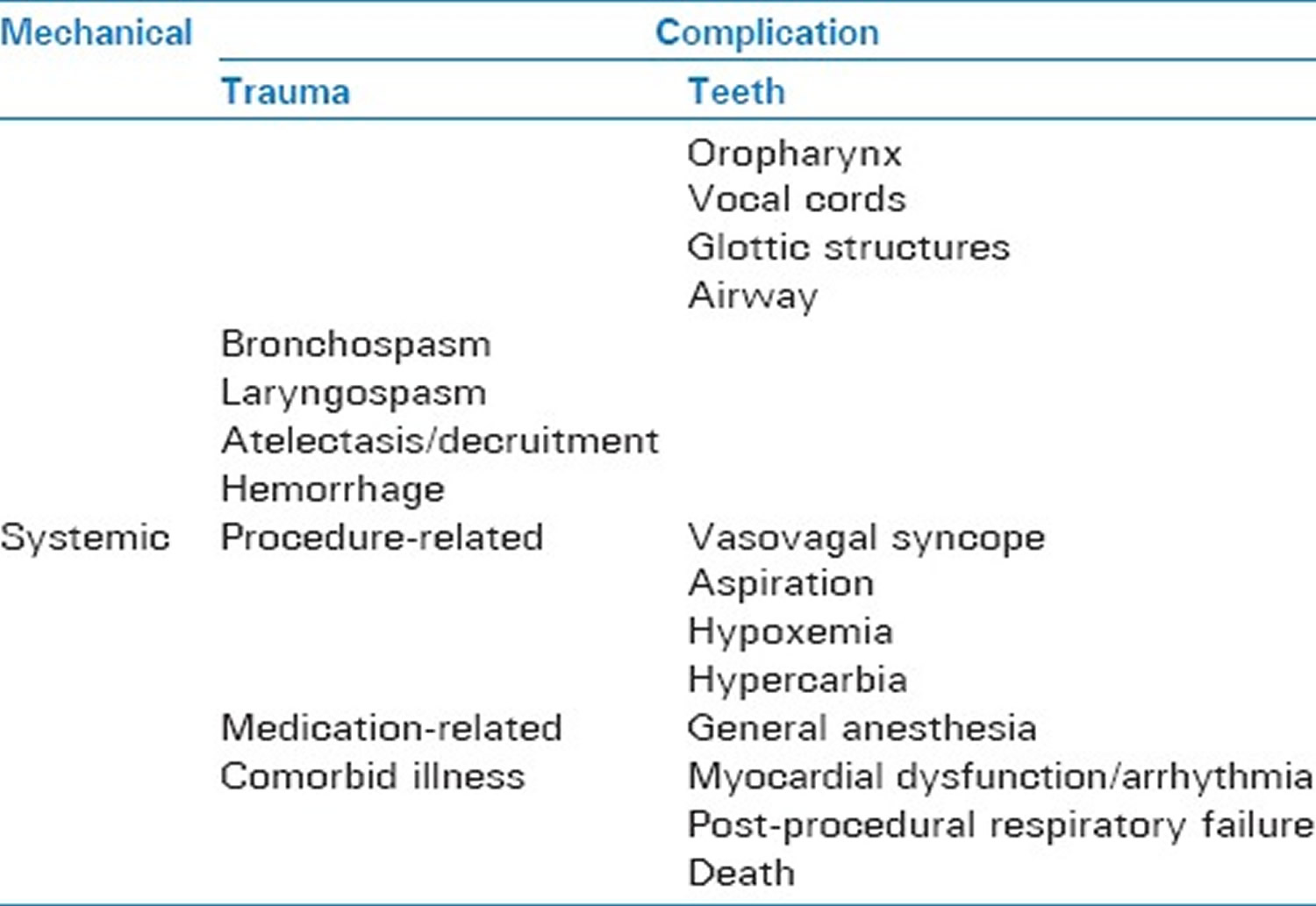
The most common mechanical complications of rigid bronchoscopy are trauma to the teeth, oropharynx, vocal cords or other glottic structures, laryngospasm, pneumothorax, and hemorrhage, and death 44. Systemic complications include vasovagal syncope, hypoxemia, hypercarbia, medication effects of general anesthesia, arrhythmia, post-procedural respiratory failure, and death 44.
It should be noted that there are relatively few prospective studies providing quantifiable complication rates during and after rigid bronchoscopy, so the true rate of complications resulting from the procedure is difficult to pinpoint and will vary by operator experience and institution 43. However, advances in equipment, monitoring, and anesthetic drugs have increased the overall margin of safety for rigid bronchoscopy. One retrospective study 44 reviewed 775 cases of rigid bronchoscopy in a university hospital between 1992 and 1999 and found that 86.7% of cases occurred without any of the above listed complications. In this study 103/775 (13.3%) of cases had complications, which included bleeding (6.6%), respiratory failure (5.3%), cough (0.6%), death (0.4%), and arrhythmia (0.3%) 44. A lesion at or near the carina had the highest correlation with procedural complications 44. Furthermore, rigid bronchoscopy seems to be safe to use in neurosurgery patients with space-occupying lesions 45.
One underreported complication during rigid bronchoscopy with laser is airway fire. With advances in technology, laser can now be used through flexible fiberoptic bronchoscopes, rigid bronchoscopes, during esophagoscopy, and during suspension microlaryngoscopy. Due to this variety of applications, most reports of the incidence of airway fire are not specific to rigid bronchoscopy. In order to ensure the highest margin of safety in preventing airway fire, good communication must exist between the anesthesiologist and proceduralist, and the concentration of inhaled oxygen when the laser is in use should be < 40% 5. Standard precautions should be adhered to during laser airway procedures, especially when flammable objects (stents and endotracheal tubes) are also present in the airway.
Another notable retrospective study 46 compared the complication rate of flexible fiberoptic bronchoscopy under topical anesthesia with the complication rate of rigid bronchoscopy under general anesthesia. Lukomsky et al. 46, reviewed 3,449 rigid bronchoscopy procedures and complications associated with rigid bronchoscopy occurred in 173 of 3,449 cases (5%); four rigid bronchoscope cases were complicated by pneumothorax and six cases were complicated by death (four due to hypoxia) resulting in a fatality rate of 0.17% 46.
- Azadeh N, Sakata KK, Saeed A, et al. Comparison of Respiratory Pathogen Detection in Upper versus Lower Respiratory Tract Samples Using the BioFire FilmArray Respiratory Panel in the Immunocompromised Host. Canadian Respiratory Journal. 2018;2018:2685723. doi:10.1155/2018/2685723. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5907482/[↩]
- Petrella F, Borri A, Casiraghi M, Cavaliere S, Donghi S, Galetta D, et al. Operative rigid bronchoscopy: Indications, basic techniques and results. Multimed Man Cardiothorac Surg 2014. https://www.ncbi.nlm.nih.gov/pubmed/25133397[↩]
- Pathak V, Welsby I, Mahmood K, Wahidi M, MacIntyre N, Shofer S. Ventilation and anesthetic approaches for rigid bronchoscopy. Ann Am Thorac Soc. 2014;11:628–34. https://www.ncbi.nlm.nih.gov/pubmed/24635585[↩][↩]
- Ayers ML, Beamis JF., Jr Rigid bronchoscopy in the twenty-first century. Clin Chest Med. 2001;22:355–64. https://www.ncbi.nlm.nih.gov/pubmed/11444118[↩]
- Goudra BG, Singh PM, Borle A, Farid N, Harris K. Anesthesia for advanced bronchoscopic procedures: State-of-the-art review. Lung. 2015 https://www.ncbi.nlm.nih.gov/pubmed/25921014[↩][↩]
- Dincq AS, Gourdin M, Collard E, Ocak S, D’Odemont JP, Dahlqvist C, et al. Anesthesia for adult rigid bronchoscopy. Acta Anaesthesiol Belg. 2014;65:95–103. https://www.ncbi.nlm.nih.gov/pubmed/25470890[↩]
- Nicastri DG, Weiser TS. Rigid bronchoscopy: Indications and techniques. Oper Tech Thorac Cardiovasc Surg. 2012;17:44–51.[↩]
- Goud A, Dahagam C, Breen DP, Sarkar S. Role of electromagnetic navigational bronchoscopy in pulmonary nodule management. Journal of Thoracic Disease. 2016;8(Suppl 6):S501-S508. doi:10.21037/jtd.2016.02.73. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4990667/[↩]
- Makris D, Scherpereel A, Leroy S, et al. Electromagnetic navigation diagnostic bronchoscopy for small peripheral lung lesions. Eur Respir J 2007;29:1187-92. 10.1183/09031936.00165306 https://www.ncbi.nlm.nih.gov/pubmed/17360724[↩][↩]
- Mahajan AK, Patel S, Hogarth DK, et al. Electromagnetic navigational bronchoscopy: an effective and safe approach to diagnose peripheral lung lesions unreachable by conventional bronchoscopy in high-risk patients. J Bronchology Interv Pulmonol 2011;18:133-7. 10.1097/LBR.0b013e318216cee6 https://www.ncbi.nlm.nih.gov/pubmed/23169081[↩]
- Wilson DS, Bartlett RJ. Improved Diagnostic Yield of Bronchoscopy in a Community Practice: Combination of Electromagnetic Navigation System and Rapid On-site Evaluation. J Bronchol 2007;14:227-32. 10.1097/LBR.0b013e31815a7b00[↩][↩]
- Schreiber G, McCrory DC. Performance characteristics of different modalities for diagnosis of suspected lung cancer: summary of published evidence. Chest 2003;123:115S-128S. 10.1378/chest.123.1_suppl.115S https://www.ncbi.nlm.nih.gov/pubmed/12527571[↩]
- Schwarz Y, Greif J, Becker HD, et al. Real-time electromagnetic navigation bronchoscopy to peripheral lung lesions using overlaid CT images: the first human study. Chest 2006;129:988-94. 10.1378/chest.129.4.988 https://www.ncbi.nlm.nih.gov/pubmed/16608948[↩][↩]
- Eberhardt R, Anantham D, Herth F, et al. Electromagnetic navigation diagnostic bronchoscopy in peripheral lung lesions. Chest 2007;131:1800-5. 10.1378/chest.06-3016 https://www.ncbi.nlm.nih.gov/pubmed/17400670[↩][↩]
- Seijo LM, de Torres JP, Lozano MD, et al. Diagnostic yield of electromagnetic navigation bronchoscopy is highly dependent on the presence of a Bronchus sign on CT imaging: results from a prospective study. Chest 2010;138:1316-21. 10.1378/chest.09-2708 https://www.ncbi.nlm.nih.gov/pubmed/20435658[↩][↩]
- Gildea TR, Mazzone PJ, Karnak D, et al. Electromagnetic navigation diagnostic bronchoscopy: a prospective study. Am J Respir Crit Care Med 2006;174:982-9. 10.1164/rccm.200603-344OC https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2648102/[↩][↩]
- Gex G, Pralong JA, Combescure C, et al. Diagnostic yield and safety of electromagnetic navigation bronchoscopy for lung nodules: a systematic review and meta-analysis. Respiration 2014;87:165-76. 10.1159/000355710 https://www.ncbi.nlm.nih.gov/pubmed/24401166[↩]
- Eberhardt R, Anantham D, Ernst A, et al. Multimodality bronchoscopic diagnosis of peripheral lung lesions: a randomized controlled trial. Am J Respir Crit Care Med 2007;176:36-41. 10.1164/rccm.200612-1866OC https://www.ncbi.nlm.nih.gov/pubmed/17379850[↩]
- Eberhardt R, Morgan RK, Ernst A, et al. Comparison of suction catheter versus forceps biopsy for sampling of solitary pulmonary nodules guided by electromagnetic navigational bronchoscopy. Respiration 2010;79:54-60. 10.1159/000232394 https://www.ncbi.nlm.nih.gov/pubmed/19648733[↩]
- Chee A, Stather DR, Maceachern P, et al. Diagnostic utility of peripheral endobronchial ultrasound with electromagnetic navigation bronchoscopy in peripheral lung nodules. Respirology 2013;18:784-9. 10.1111/resp.12085 https://www.ncbi.nlm.nih.gov/pubmed/23521707[↩]
- Anantham D, Feller-Kopman D, Shanmugham LN, et al. Electromagnetic navigation bronchoscopy-guided fiducial placement for robotic stereotactic radiosurgery of lung tumors: a feasibility study. Chest 2007;132:930-5. 10.1378/chest.07-0522[↩]
- Harley DP, Krimsky WS, Sarkar S, et al. Fiducial marker placement using endobronchial ultrasound and navigational bronchoscopy for stereotactic radiosurgery: an alternative strategy. Ann Thorac Surg 2010;89:368-73; discussion 373-4. 10.1016/j.athoracsur.2009.09.048[↩]
- Schroeder C, Hejal R, Linden PA. Coil spring fiducial markers placed safely using navigation bronchoscopy in inoperable patients allows accurate delivery of CyberKnife stereotactic radiosurgery. J Thorac Cardiovasc Surg 2010;140:1137-42. 10.1016/j.jtcvs.2010.07.085[↩]
- Becker HD, Harms W, Debus J, et al. Brachytherapy of inoperable peripheral lung cancer guided by electromagnetic navigation and endobrochial ultrasound: feasibility study and confirmation by long-term results at two centers. Chest 2009;136:2S 10.1378/chest.136.4_MeetingAbstracts.2S-f[↩]
- Krimsky WS, Minnich DJ, Cattaneo SM, et al. Thoracoscopic detection of occult indeterminate pulmonary nodules using bronchoscopic pleural dye marking. J Community Hosp Intern Med Perspect 2014;4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3937566/[↩]
- Suzuki K, Nagai K, Yoshida J, et al. Video-assisted thoracoscopic surgery for small indeterminate pulmonary nodules: indications for preoperative marking. Chest 1999;115:563-8. 10.1378/chest.115.2.563[↩]
- Mahajan AK, Patel S, Hogarth DK, et al. Electromagnetic navigational bronchoscopy: an effective and safe approach to diagnose peripheral lung lesions unreachable by conventional bronchoscopy in high-risk patients. J Bronchology Interv Pulmonol 2011;18:133-7. 10.1097/LBR.0b013e318216cee6[↩][↩][↩]
- Gex G, Pralong JA, Combescure C, et al. Diagnostic yield and safety of electromagnetic navigation bronchoscopy for lung nodules: a systematic review and meta-analysis. Respiration 2014;87:165-76. 10.1159/000355710[↩]
- Khan AY, Berkowitz D, Krimsky WS, et al. Safety of pacemakers and defibrillators in electromagnetic navigation bronchoscopy. Chest 2013;143:75-81. 10.1378/chest.12-0689[↩]
- Kupelian PA, Forbes A, Willoughby TR, et al. Implantation and stability of metallic fiducials within pulmonary lesions. Int J Radiat Oncol Biol Phys 2007;69:777-85. 10.1016/j.ijrobp.2007.03.040[↩][↩]
- Seijo LM, de Torres JP, Lozano MD, et al. Diagnostic yield of electromagnetic navigation bronchoscopy is highly dependent on the presence of a Bronchus sign on CT imaging: results from a prospective study. Chest 2010;138:1316-21. 10.1378/chest.09-2708[↩][↩]
- Eberhardt R, Anantham D, Herth F, et al. Electromagnetic navigation diagnostic bronchoscopy in peripheral lung lesions. Chest 2007;131:1800-5. 10.1378/chest.06-3016[↩]
- Eberhardt R, Morgan RK, Ernst A, et al. Comparison of suction catheter versus forceps biopsy for sampling of solitary pulmonary nodules guided by electromagnetic navigational bronchoscopy. Respiration 2010;79:54-60. 10.1159/000232394[↩][↩]
- Eberhardt R, Anantham D, Ernst A, et al. Multimodality bronchoscopic diagnosis of peripheral lung lesions: a randomized controlled trial. Am J Respir Crit Care Med 2007;176:36-41. 10.1164/rccm.200612-1866OC[↩]
- Chee A, Stather DR, Maceachern P, et al. Diagnostic utility of peripheral endobronchial ultrasound with electromagnetic navigation bronchoscopy in peripheral lung nodules. Respirology 2013;18:784-9. 10.1111/resp.12085[↩]
- Baaklini WA, Reinoso MA, Gorin AB, et al. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest 2000;117:1049-54. 10.1378/chest.117.4.1049[↩]
- Wynder EL, Muscat JE. The changing epidemiology of smoking and lung cancer histology. Environ Health Perspect 1995;103 Suppl 8:143-8. 10.1289/ehp.95103s8143[↩]
- Wang Memoli JS, Nietert PJ, Silvestri GA. Meta-analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest 2012;142:385-93. 10.1378/chest.11-1764[↩]
- Steinfort DP, Khor YH, Manser RL, et al. Radial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: systematic review and meta-analysis. Eur Respir J 2011;37:902-10. 10.1183/09031936.00075310[↩]
- Radke JR, Conway WA, Eyler WR, et al. Diagnostic accuracy in peripheral lung lesions. Factors predicting success with flexible fiberoptic bronchoscopy. Chest 1979;76:176-9. 10.1378/chest.76.2.176[↩]
- Cortese DA, McDougall JC. Biopsy and brushing of peripheral lung cancer with fluoroscopic guidance. Chest 1979;75:141-5. 10.1378/chest.75.2.141[↩]
- Wang KP, Britt EJ. Needle brush in the diagnosis of lung mass or nodule through flexible bronchoscopy. Chest 1991;100:1148-50. 10.1378/chest.100.4.1148[↩]
- Stahl DL, Richard KM, Papadimos TJ. Complications of bronchoscopy: A concise synopsis. International Journal of Critical Illness and Injury Science. 2015;5(3):189-195. doi:10.4103/2229-5151.164995. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4613418/[↩][↩][↩]
- Drummond M, Magalhaes A, Hespanhol V, Marques A. Rigid bronchoscopy: Complications in a university hospital. J Bronchol. 2003;10:177–81.[↩][↩][↩][↩][↩]
- Grosu HB, Morice RC, Sarkiss M, Bashoura L, Eapen GA, Jimenez CA, et al. Safety of flexible bronchoscopy, rigid bronchoscopy, and endobronchial ultrasound-guided transbronchial needle aspiration in patients with malignant space-occupying brain lesions. Chest. 2015;147:1621–8. https://www.ncbi.nlm.nih.gov/pubmed/25393333[↩]
- Lukomsky GI, Ovchinnikov AA, Bilal A. Complications of bronchoscopy: Comparison of rigid bronchoscopy under general anesthesia and flexible fiberoptic bronchoscopy under topical anesthesia. Chest. 1981;79:316–21. https://www.ncbi.nlm.nih.gov/pubmed/7471862[↩][↩][↩]





{kind=link}