Contents
- What is cancer immunotherapy
- Immunotherapy side effects
- How Immunotherapy is given
- Your immune system
- Types of cancer immunotherapy
- Immunotherapy vs Chemotherapy
- Immunotherapy for bladder cancer
- Immunotherapy for breast cancer
- Immunotherapy for colon cancer
- Immunotherapy for lung cancer
- Immunotherapy for melanoma
- Immunotherapy for pancreatic cancer
- Immunotherapy for prostate cancer
What is cancer immunotherapy
Cancer immunotherapy is treatment that uses your immune system to fight cancer. Immunotherapy for cancer works by helping certain parts of your immune system to recognize and attack cancer cells. Some types of immunotherapy are also called targeted treatments or biological therapies (biotherapies). You might have immunotherapy on its own or with other cancer treatments.
Immunotherapy is a treatment for some types of cancer, for example melanoma that has spread. Immunotherapy uses natural body substances, or drugs made from natural body substances, to treat cancer.
Cancer immunotherapies are helpful in cancer treatment because cancer cells are different from normal cells. And the immune system can recognize and kill abnormal cells.
Cancer immunotherapy can be done in a couple of ways:
- Stimulating your own immune system to work harder or smarter to attack cancer cells
- Giving you immune system components, such as man-made immune system proteins
In the last few decades immunotherapy has become an important part of treating some types of cancer. Newer types of immune treatments are now being studied, and they’ll impact how doctors treat cancer in the future.
Immunotherapy includes treatments that work in different ways. Some boost your body’s immune system in a very general way. Others help train the immune system to attack cancer cells specifically.
Immunotherapy works better for some types of cancer than for others. Immunotherapy is used by itself for some of these cancers, but for others it seems to work better when used with other types of treatment.
Scientists can produce, in the laboratory, different chemicals that are part of the immune response. So, they can make different types of immunotherapy such as:
- monoclonal antibodies (MABs), which recognize and attack certain proteins on the surface of cancer cells
- vaccines to help the immune system to recognize and attack cancer
- cytokines to help to boost the immune system
- adoptive cell transfer to change the genes in a person’s white blood cells
Immunotherapy side effects
Immunotherapy can cause side effects, which affect people in different ways. The side effects you may have and how they make you feel will depend on how healthy you are before treatment, your type of cancer, how advanced it is, the type of therapy you are getting, and the dose. Doctors and nurses cannot know for certain how you will feel during treatment.
The most common side effects are skin reactions at the needle site. These side effects include:
- Pain
- Swelling
- Soreness
- Redness
- Itchiness
- Rash
You may have flu-like symptoms, which include:
- Fever
- Chills
- Weakness
- Dizziness
- Nausea or vomiting
- Muscle or joint aches
- Fatigue
- Headache
- Trouble breathing
- Low or high blood pressure
Other side effects might include:
- Swelling and weight gain from retaining fluid
- Heart palpitations
- Sinus congestion
- Diarrhea
- Risk of infection
Immunotherapies may also cause severe or even fatal allergic reactions. However, these reactions are rare.
Potentially serious side effects of specific immunotherapies include:
Immune Checkpoint Inhibitors
Organ-damaging immune-mediated reactions involving the digestive system, liver, skin, nervous system, and heart and in the hormone-producing glands. These reactions can cause immune-mediated pneumonitis, colitis, hepatitis, nephritis and renal (kidney) dysfunction, myocarditis (inflammation of the heart muscle), and hypothyroidism and hyperthyroidism.
Immune Cell Therapy
- Cytokine release syndrome (CAR T-cell therapy)
- Capillary leak syndrome (TIL therapy)
Therapeutic Antibodies and Other Immune System Molecules
- Cytokine release syndrome (blinatumomab)
- Infusion reactions, capillary leak syndrome, and loss of visual acuity (denileukin diftitox)
Therapeutic Vaccines
- Flu-like symptoms
- Severe allergic reaction
- Stroke (Sipuleucel-T)
- Tumor lysis syndrome, herpes virus infection (T-VEC)
Immune System Modulators
- Flu-like symptoms, severe allergic reaction, lowered blood counts, changes in blood chemistry, organ damage (cytokines)
- Flu-like symptoms, severe allergic reaction, urinary side effects (BCG)
- Severe birth defects if taken during pregnancy, blood clots/venous embolism, neuropathy (thalidomide, lenalidomide, pomalidomide)
- Skin reactions (imiquimod)
How Immunotherapy is given
Different forms of immunotherapy may be given in different ways. These include:
Intravenous (IV)
The immunotherapy goes directly into a vein.
Oral
The immunotherapy comes in pills or capsules that you swallow.
Topical
The immunotherapy comes in a cream that you rub onto your skin. This type of immunotherapy can be used for very early skin cancer.
Intravesical
The immunotherapy goes directly into the bladder.
Your immune system
Your immune system is a collection of organs, special cells, and substances that help protect you from infections caused by bacteria, viruses, fungi or parasites, illnesses and some other diseases. Immune cells and the substances they make travel through your body to protect it from germs that cause infections. Your immune system also help protect you from the development of cancer in some ways.
Your immune system includes the lymph glands, spleen and white blood cells. Normally, it can spot and destroy faulty cells in the body, stopping cancer developing. But a cancer might develop when:
- your immune system recognizes cancer cells but it is not strong enough to kill the cancer cells
- the cancer cells produce signals that stop your immune system from attacking it
- the cancer cells hide or escape from your immune system
Your immune system is important to cancer patients in many ways because:
- cancer can weaken your immune system
- cancer treatments may weaken your immune system
- your immune system may help to fight cancer
Your immune system keeps track of all of the substances normally found in your body. Any new substance that the immune system doesn’t recognize raises an alarm, causing the immune system to attack it. For example, germs contain substances such as certain proteins that are not normally found in the human body. The immune system sees these as “foreign” and attacks them. The immune response can destroy anything containing the foreign substance, such as germs or cancer cells.
Your immune system has a tougher time targeting cancer cells, though. This is because cancer starts when cells become altered and start to grow out of control. The immune system doesn’t always recognize cancer cells as foreign.
Clearly there are limits on the immune system’s ability to fight cancer on its own, because many people with healthy immune systems still develop cancer. Sometimes the immune system doesn’t see the cancer cells as foreign because the cells aren’t different enough from normal cells. Sometimes the immune system recognizes the cancer cells, but the response might not be strong enough to destroy the cancer. Cancer cells themselves can also give off substances that keep the immune system in check.
To overcome this, researchers have found ways to help the immune system recognize cancer cells and strengthen its response so that it will destroy them.
Cancer and treatments may weaken immunity
Cancer can weaken your immune system by spreading into the bone marrow. The bone marrow makes blood cells that help to fight infection. This happens most often in leukaemia or lymphoma, but it can happen with other cancers too. The cancer can stop the bone marrow from making so many blood cells.
Certain cancer treatments can temporarily weaken your immune system. This is because they can cause a drop in the number of white blood cells made in the bone marrow. Cancer treatments that are more likely to weaken the immune system are:
- chemotherapy
- targeted cancer drugs
- radiotherapy
- high dose of steroids
Your immune system can help to fight cancer
Some cells of the immune system can recognize cancer cells as abnormal and kill them. Unfortunately, this may not be enough to get rid of a cancer altogether. But some new treatments aim to use the immune system to fight cancer.
There are 2 main parts of the immune system:
- the protection you have from birth (in built immune protection)
- the protection you develop after having certain diseases (acquired immunity)
In built immune protection
This is also called innate immunity. These mechanisms are always ready and prepared to defend your body from infection. They can act immediately (or very quickly). This in built protection comes from:
- a barrier formed by the skin around the body
- the inner linings of the gut and lungs, which produce mucus and trap invading bacteria
- hairs that move the mucus and trapped bacteria out of the lungs
- stomach acid, which kills bacteria
- helpful bacteria growing in the bowel, which prevent other bacteria from taking over
- urine flow, which flushes bacteria out of the bladder and urethra
- white blood cells called neutrophils, which can find and kill bacteria
Different things can overcome and damage these natural protection mechanisms. For example:
- something may break the skin barrier, such as having a drip in your arm or a wound from surgery
- a catheter into your bladder can become a route for bacteria to get inside the bladder and cause infection
- antacid medicines for heartburn may neutralize the stomach acid that kills bacteria
Certain cancer treatments can also overcome these protection mechanisms. Chemotherapy can temporarily reduce the number of neutrophils in the body, making it harder for you to fight infections. Radiotherapy to the lung can damage the hairs and mucus producing cells that help to remove bacteria.
Neutrophils
These white blood cells are very important for fighting infection. They can:
- move to areas of infection in the body
- stick to the invading bacteria, viruses or fungi
- swallow up the bacteria, viruses or fungi and kill them with chemicals
Your normal neutrophil count is between 2,000 and 7,500 per cubic millimeter of blood. When you don’t have enough neutrophils in your blood, doctors may say that you are neutropenic.
Chemotherapy, targeted cancer drugs and some radiotherapy treatments can lower the neutrophil count. So, you may be more likely to get bacterial or fungal infections after these treatments.
It is important for you to know the following when having cancer treatment:
- infections can become serious very quickly in people with low neutrophil counts
- antibiotics could save your life, so if you get a fever or feel ill, phone your cancer center or go to hospital straight away
- you may need to take antibiotics to help prevent severe infection if your blood counts are low
You are more likely to become ill from bugs you carry around with you, than from catching someone else’s. This means that you usually don’t have to avoid contact with your family, friends or children after treatment.
You can ask your doctor or nurse what precautions you should take against infection.
Acquired immunity
This is immune protection that the body learns after having certain diseases. The body learns to recognize each different kind of bacteria, fungus or virus it meets for the first time. So, the next time the same bug invades the body, the immune system is ready for it and able to fight it off more easily. This is why you usually only get some infectious diseases, such as measles or chicken pox, once.
Vaccination works by using this type of immunity. A vaccine contains a small amount of protein from a disease. This is not harmful, but it allows the immune system to recognize the disease if it meets it again. The immune response can then stop you getting the disease.
Some vaccines use small amounts of the live bacteria or virus. These are live attenuated vaccines. It means that scientists have changed the virus or bacteria so that it stimulates the immune system to make antibodies. A live vaccine won’t cause an infection.
Other types of vaccine use killed bacteria or viruses, or parts of proteins produced by bacteria and viruses.
B cells and T cells
Lymphocytes are a type of white blood cells involved in the acquired immune response. There are 2 main types of lymphocytes:
- B cells (B lymphocytes)
- T cells (T lymphocytes)
The bone marrow produces all blood cells, including B and T lymphocytes. Like the other blood cells, they have to fully mature before they can help in the immune response.
B cells mature in the bone marrow. But T cells mature in the thymus gland. Once they are fully mature, the B and T cells travel to the spleen and lymph nodes ready to fight infection.
What B cells do
B cells react against invading bacteria or viruses by making proteins called antibodies. The antibody made is different for each different type of germ (bug). The antibody locks onto the surface of the invading bacteria or virus. The invader is then marked with the antibody so that the body knows it is dangerous and needs to be killed. Antibodies can also detect and kill damaged cells.
The B cells are part of the memory of the immune system. The next time the same germ tries to invade, the B cells that make the right antibody are ready for it. They are able to make their antibody very quickly.
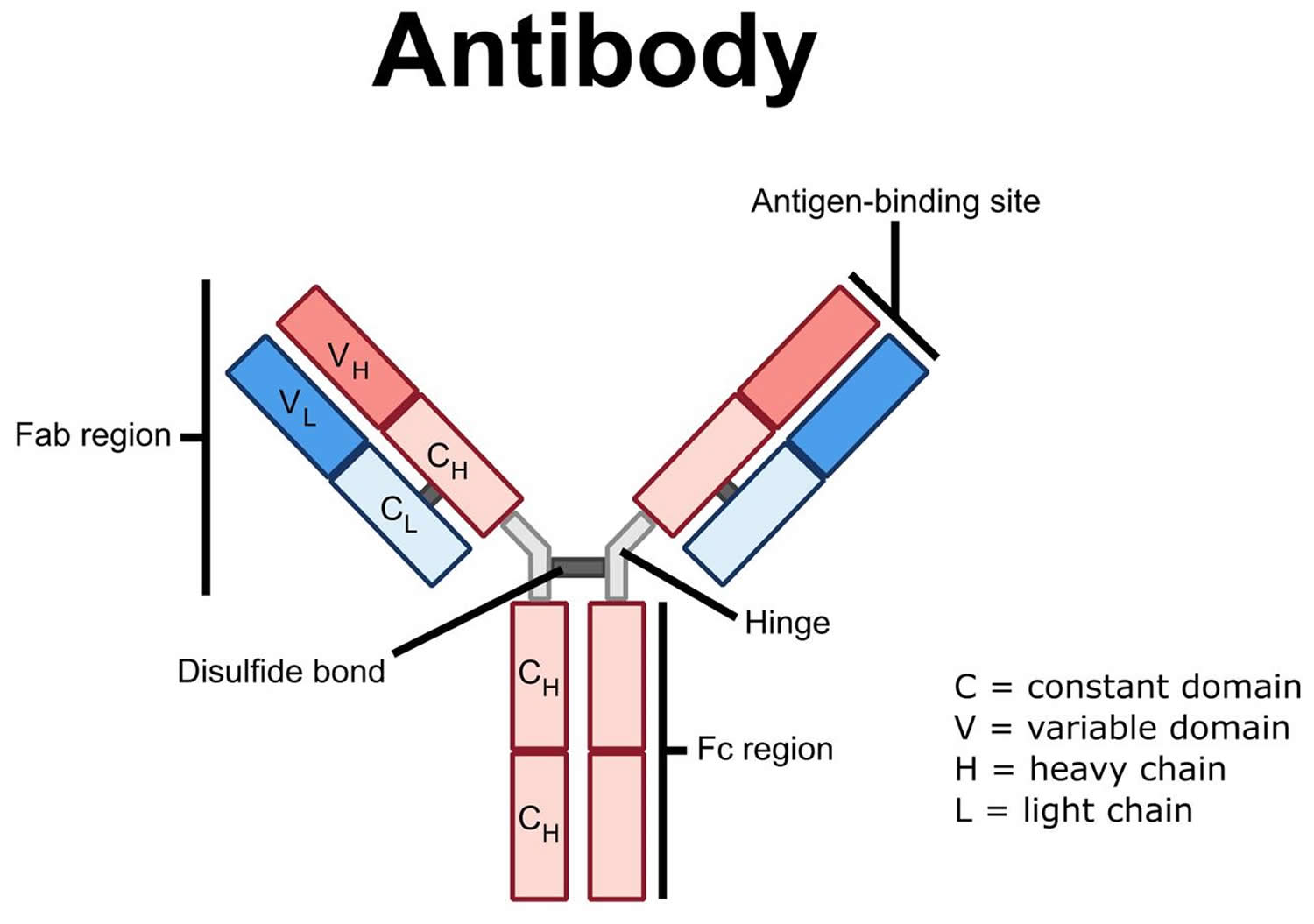
How antibodies work
Antibodies have 2 ends. One end sticks to proteins on the outside of white blood cells. The other end sticks to the germ or damaged cell and helps to kill it. The end of the antibody that sticks to the white blood cell is always the same. Scientists call this the constant end (constant domain).
The end of the antibody that recognizes germs and damaged cells varies, depending on the cell it needs to recognize. So it is called the variable end (constant domain). Each B cell makes antibodies with a different variable end from other B cells.
Cancer cells are not normal cells. So some antibodies with variable ends recognize cancer cells and stick to them.
Figure 1. Antibody
What T cells do
There are different kinds of T cells called:
- helper T cells
- killer T cells
The helper T cells stimulate the B cells to make antibodies and help killer cells develop.
Killer T cells kill the body’s own cells that have been invaded by the viruses or bacteria. This prevents the germ from reproducing in the cell and then infecting other cells.
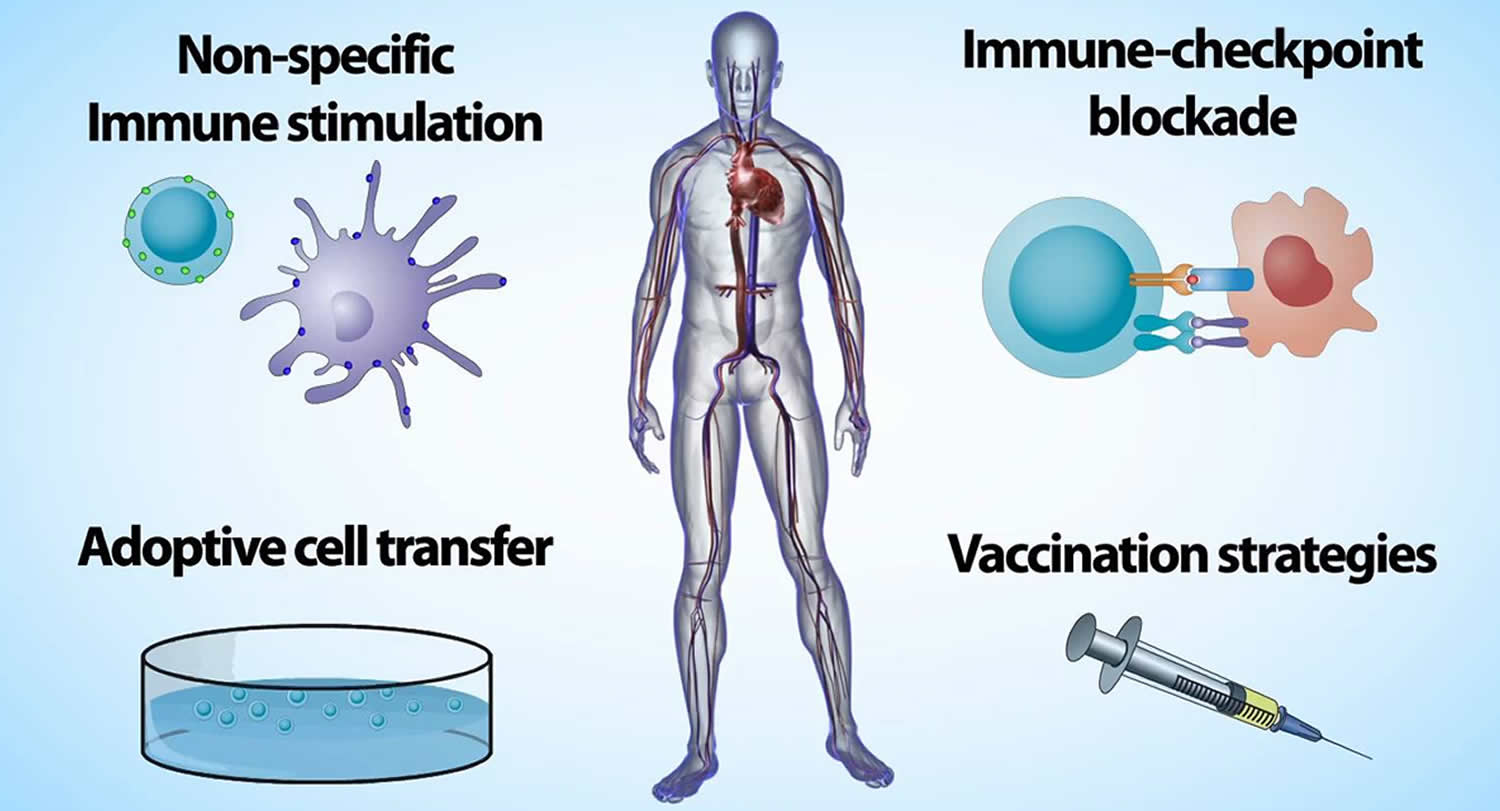
Types of cancer immunotherapy
The main types of immunotherapy now being used to treat cancer include:
- Monoclonal antibodies (MAb): These are man-made versions of immune system proteins. Antibodies can be very useful in treating cancer because they can be designed to attack a very specific part of a cancer cell.
- Immune checkpoint inhibitors: These drugs basically take the ‘brakes’ off the immune system, which helps it recognize and attack cancer cells.
- Cancer vaccines: Vaccines are substances put into the body to start an immune response against certain diseases. We usually think of them as being given to healthy people to help prevent infections. But some vaccines can help prevent or treat cancer.
- Adoptive cell transfer, which is a treatment that attempts to boost the natural ability of your T cells to fight cancer. In this treatment, T cells are taken from your tumor. Then those that are most active against your cancer are grown in large batches in the lab. The process of growing your T cells in the lab can take 2 to 8 weeks. During this time, you may have treatments such as chemotherapy and radiation therapy to reduce your immune cells. After these treatments, the T cells that were grown in the lab will be given back to you via a needle in your vein. For more information about a specific type of adoptive cell transfer see CAR T-Cell Therapies: Chimeric antigen receptor (CAR) T-cell therapy and Tumor-infiltrating lymphocytes (or TILs).
- Other, non-specific immunotherapies: These treatments boost the immune system in a general way, but this can still help the immune system attack cancer cells.
Immunotherapy drugs are now used to treat many different types of cancer. For more information about immunotherapy as a treatment for a specific cancer, please see our information on that type of cancer.
Many newer types of immunotherapy are now being studied for use against cancer.
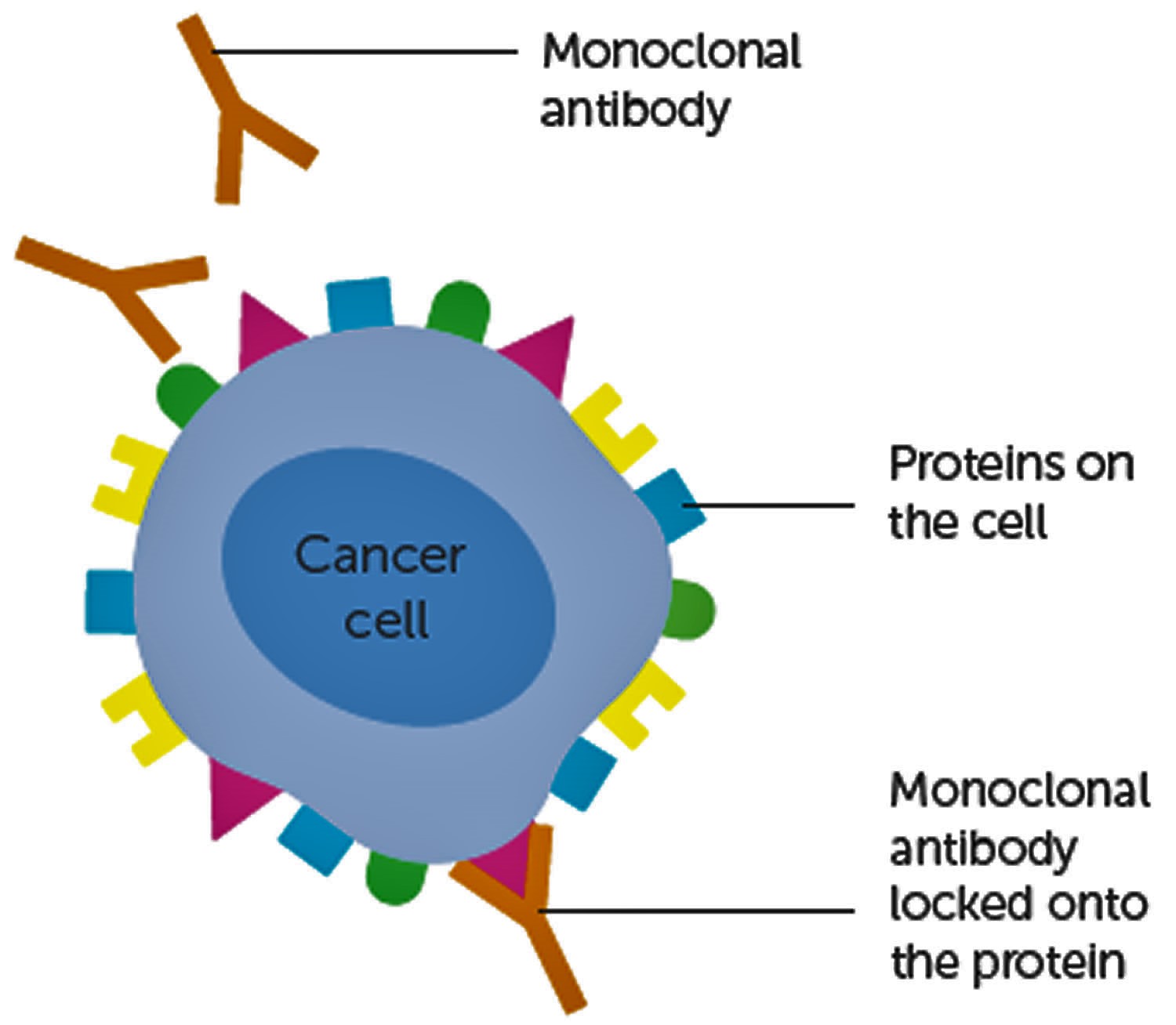
Monoclonal antibodies to treat cancer
One way the immune system attacks foreign substances in the body is by making large numbers of antibodies. An antibody is a protein that sticks to a specific protein called an antigen. Antibodies circulate throughout the body until they find and attach to the antigen. Once attached, they can recruit other parts of the immune system to destroy the cells containing the antigen.
Researchers can design antibodies that specifically target a certain antigen, such as one found on cancer cells. They can then make many copies of that antibody in the lab. These are known as monoclonal antibodies (mAbs).
Monoclonal antibodies are used to treat many diseases, including some types of cancer. To make a monoclonal antibody, researchers first have to identify the right antigen to attack. For cancer, this is not always easy, and so far mAbs have proven to be more useful against some cancers than others.
Over the past couple of decades, the US Food and Drug Administration (FDA) has approved more than a dozen monoclonal antibodies to treat certain cancers. As researchers have found more antigens linked to cancer, they have been able to make monoclonal antibodies (mAbs) against more and more cancers. Clinical trials of newer monoclonal antibodies are now being done on many types of cancer.
Figure 2. How monoclonal antibodies treat cancer
Types of monoclonal antibodies
Different types of monoclonal antibodies are used in cancer treatment.
Naked monoclonal antibodies
Naked monoclonal antibodies (mAbs) are antibodies that work by themselves. There is no drug or radioactive material attached to them. These are the most common type of monoclonal antibodies used to treat cancer.
Most naked monoclonal antibodies attach to antigens on cancer cells, but some work by binding to antigens on other, non-cancerous cells, or even free-floating proteins.
Naked monoclonal antibodies can work in different ways.
- Some boost a person’s immune response against cancer cells by attaching to them and acting as a marker for the body’s immune system to destroy them. An example is alemtuzumab (Campath®), which is used to treat some patients with chronic lymphocytic leukemia (CLL). Alemtuzumab binds to the CD52 antigen, which is found on cells called lymphocytes (which include the leukemia cells). Once attached, the antibody attracts immune cells to destroy these cells.
- Some naked monoclonal antibodies boost the immune response by targeting immune system checkpoints. (See Immune checkpoint inhibitors to treat cancer.)
- Other naked monoclonal antibodies work mainly by attaching to and blocking antigens on cancer cells (or other nearby cells) that help cancer cells grow or spread. For example, trastuzumab (Herceptin®) is an antibody against the HER2 protein. Breast and stomach cancer cells sometimes have large amounts of this protein on their surface. When HER2 is activated, it helps these cells grow. Trastuzumab binds to these proteins and stops them from becoming active.
Conjugated monoclonal antibodies
Monoclonal antibodies (mAbs) joined to a chemotherapy drug or to a radioactive particle are called conjugated monoclonal antibodies. The monoclonal antibodies is used as a homing device to take one of these substances directly to the cancer cells. The monoclonal antibodies circulates throughout the body until it can find and hook onto the target antigen. It then delivers the toxic substance where it is needed most. This lessens the damage to normal cells in other parts of the body.
Conjugated monoclonal antibodies are also sometimes referred to as tagged, labeled, or loaded antibodies.
Radiolabeled antibodies: Radiolabeled antibodies have small radioactive particles attached to them. Ibritumomab tiuxetan (Zevalin®) is an example of a radiolabeled monoclonal antibodies. This is an antibody against the CD20 antigen, which is found on lymphocytes called B cells. The antibody delivers radioactivity directly to cancerous B cells and can be used to treat some types of non-Hodgkin lymphoma.
Treatment with this type of antibody is sometimes known as radioimmunotherapy.
Chemolabeled antibodies: These monoclonal antibodies have powerful chemotherapy (or other) drugs attached to them. They are also known as antibody-drug conjugates. (The drug is often too powerful to be used on its own – it would cause too many side effects if not attached to an antibody.)
Chemolabeled antibodies used to treat cancer include:
- Brentuximab vedotin (Adcetris®), an antibody that targets the CD30 antigen (found on lymphocytes), attached to a chemo drug called MMAE. This drug is used to treat Hodgkin lymphoma and anaplastic large cell lymphoma.
- Ado-trastuzumab emtansine (Kadcyla®, also called TDM-1), an antibody that targets the HER2 protein, attached to a chemo drug called DM1. It’s used to treat some breast cancer patients whose cancer cells have too much HER2.
A related drug known as denileukin diftitox (Ontak®) is an immune system protein known as interleukin-2 (IL-2) attached to a toxin from the germ that causes diphtheria. Although it’s not an antibody, IL-2 normally attaches to certain cells in the body that contain the CD25 antigen, which makes it useful for delivering the toxin to these cells. Denileukin diftitox is used to treat lymphoma of the skin (also known as cutaneous T-cell lymphoma). It’s also being studied for use against a number of other cancers.
Bispecific monoclonal antibodies
These drugs are made up of parts of 2 different mAbs, meaning they can attach to 2 different proteins at the same time. An example is blinatumomab (Blincyto), which is used to treat some types of acute lymphocytic leukemia (ALL). One part of blinatumomab attaches to the CD19 protein, which is found on some leukemia and lymphoma cells. Another part attaches to CD3, a protein found on immune cells called T cells. By binding to both of these proteins, this drug brings the cancer cells and immune cells together, which is thought to cause the immune system to attack the cancer cells.
Monoclonal antibodies side effects
Monoclonal antibodies are given intravenously (injected into a vein). The antibodies themselves are proteins, so giving them can sometimes cause something like an allergic reaction. This is more common while the drug is first being given. Possible side effects can include:
- Fever
- Chills
- Weakness
- Headache
- Nausea
- Vomiting
- Diarrhea
- Low blood pressure
- Rashes
Compared with chemotherapy drugs, naked monoclonal antibodies (mAbs) tend to have fewer serious side effects. But they can still cause problems in some people. Some monoclonal antibodies (mAbs) can have side effects that are related to the antigens they target. For example:
- Bevacizumab (Avastin®) is an mAb that targets a protein called VEGF that affects tumor blood vessel growth. It can cause side effects such as high blood pressure, bleeding, poor wound healing, blood clots, and kidney damage.
- Cetuximab (Erbitux®) is an antibody that targets a cell protein called EGFR, which is found on normal skin cells (as well as some types of cancer cells). This drug can cause serious rashes in some people.
Conjugated antibodies can be more powerful than naked monoclonal antibodies, but they can also cause more side effects. The side effects depend on which type of substance they’re attached to.
Immune checkpoint inhibitors to treat cancer
An important part of your immune system is its ability to tell between normal cells in the body and those it sees as “foreign.” This lets the immune system attack the foreign cells while leaving the normal cells alone. To do this, it uses “checkpoints” – molecules on certain immune cells that need to be activated (or inactivated) to start an immune response.
Cancer cells sometimes find ways to use these checkpoints to avoid being attacked by the immune system. But drugs called checkpoint inhibitors block proteins that stop the immune system attacking cancer cells. Checkpoint inhibitors are also described as a type of monoclonal antibody (mAb) or targeted treatment.
Checkpoint inhibitors block different proteins, including PD-1 and PD-L1 (programmed death ligand 1). So you might also hear some of these drugs called PD-1 inhibitors or PD-L1 inhibitors. Checkpoint inhibitors are used to treat cancers such as melanoma skin cancer and lung cancer. Researchers are also looking at them in clinical trials for other types of cancer.
How checkpoint inhibitors work
Our immune system protects us from disease, killing bacteria and viruses. One main type of immune cell that does this is called a T cell.
T cells have proteins on them that turn on an immune response and other proteins that turn it off. These are called checkpoints.
Some checkpoint proteins help tell T cells to become active, for example when an infection is present. But if T cells are active for too long, or react to things they shouldn’t, they can start to destroy healthy cells and tissues. So other checkpoints help tell T cells to switch off.
Some cancer cells make high levels of proteins. These can switch off T cells, when they should really be attacking the cancer cells. So the cancer cells are pushing a stop button on the immune system. And the T cells can no longer recognize and kill cancer cells.
Drugs that block checkpoint proteins are called checkpoint inhibitors. They stop the proteins on the cancer cells from pushing the stop button. This turns the immune system back on and the T cells are able to find and attack the cancer cells.
Types of checkpoint inhibitors
These drugs block different checkpoint proteins including:
- CTLA-4 (cytotoxic T lymphocyte associated protein 4)
- PD-1 (programmed cell death protein 1)
- PD-L1 (programmed death ligand 1)
CTLA-4 and PD-1 are found on T cells. PD-L1 are on cancer cells.
Drugs that target PD-1 or PD-L1
PD-1 (programmed cell death protein 1) is a checkpoint protein on immune cells called T cells. It normally acts as a type of “off switch” that helps keep the T cells from attacking other cells in the body. It does this when it attaches to PD-L1 (programmed death ligand 1), a protein on some normal (and cancer) cells. When PD-1 binds to PD-L1, it basically tells the T cell to leave the other cell alone. Some cancer cells have large amounts of PD-L1, which helps them evade immune attack.
Monoclonal antibodies that target either PD-1 or PD-L1 can block this binding and boost the immune response against cancer cells. These drugs have shown a great deal of promise in treating certain cancers.
PD-1 inhibitors: Examples of drugs that target PD-1 (programmed cell death protein 1) include:
- Pembrolizumab (Keytruda)
- Nivolumab (Opdivo)
Nivolumab and pembrolizumab are treatments for some people with:
- melanoma skin cancer
- Hodgkin lymphoma
- non small cell lung cancer
- head and neck cancers
- cancer of the urinary tract (urothelial cancer) – kidney cancer and bladder cancer
The urinary tract includes the:
- center of the kidney (renal pelvis)
- tubes that take urine from the kidneys to the bladder (ureters)
- bladder
- tube that drains urine from the bladder and out of the body (urethra)
They are also being studied for use against many other types of cancer.
PD-L1 inhibitors: Examples of drugs that target PD-L1 (programmed death ligand 1) include:
- Atezolizumab (Tecentriq) (also known as MPDL3280A)
- Avelumab (Bavencio)
- Durvalumab (Imfinzi)
These drugs have also been shown to be helpful in treating different types of cancer, including bladder cancer, non-small cell lung cancer, and Merkel cell skin cancer (Merkel cell carcinoma). They are also being studied for use against other types of cancer.
Atezolizumab is a treatment for some people with lung cancer and urothelial cancers. It is also used in clinical trials for other cancers including breast cancer.
One concern with all of these drugs is that they can allow the immune system to attack some normal organs in the body, which can lead to serious side effects in some people. Common side effects of these drugs can include fatigue, cough, nausea, loss of appetite, skin rash, and itching. Less often they can cause more serious problems in the lungs, intestines, liver, kidneys, hormone-making glands, or other organs.
Many other drugs that target either PD-1 or PD-L1 are now being tested in clinical trials as well, both alone and combined with other drugs.
Drugs that target CTLA-4
CTLA-4 (cytotoxic T lymphocyte associated protein 4) is another protein on some T cells that acts as a type of “off switch” to keep the immune system in check.
Ipilimumab (Yervoy) is a monoclonal antibody that attaches to CTLA-4 (cytotoxic T lymphocyte associated protein 4) and stops it from working. This can boost the body’s immune response against cancer cells.
Ipilimumab (Yervoy) is used as a treatment for advanced melanoma of the skin. It is also being studied for use against other cancers.
Because ipilimumab affects the immune system, it can sometimes cause serious or even life-threatening side effects. In fact, compared to drugs that target PD-1 (programmed cell death protein 1) or PD-L1 (programmed death ligand 1), serious side effects seem to be more likely with ipilimumab.
When might you have immune checkpoint inhibitors drugs?
Ask your doctor if these immune checkpoint inhibitors drugs are suitable for you. Whether you can have this treatment depends on your type of cancer. It might also depend on:
- the stage of your cancer
- whether you have already had certain treatments
To find out if you can have pembrolizumab (Keytruda) for non small cell lung cancer, you need to have your cancer cells tested. To have this PD-1 inhibitor for lung cancer, you need to have large amounts of the PD-L1 protein on your cancer cells. This is called PL-L1 positive cancer.
This testing does not apply to all checkpoint inhibitors. Your doctor or specialist nurse can tell you if this applies to you.
You might be offered checkpoint inhibitors as part of a clinical trial. Or you could ask your doctor whether there are any trials that you could take part in.
How you have immune checkpoint inhibitors treatment
You usually have these drugs as a treatment through a drip into your bloodstream.
Immune checkpoint inhibitors side effects
These drugs boost all the immune cells, not just the ones that target cancer. So the overactive T cells can cause possible side effects. These might include:
- tiredness (fatigue)
- feeling or being sick
- dry, itchy skin, skin rash
- loss of appetite
- diarrhea
- breathlessness and a dry cough, caused by inflammation of the lungs
These drugs can also disrupt the normal working of the liver, kidneys and hormone making glands (such as the thyroid). You have regular blood tests to check for this.
Some of these side effects can be serious. Your medical team will talk through the possible side effects so you know what to look out for. Tell your doctor or nurse if you have any side effects so they can treat them as soon as possible.
Side effects, such as diarrhea, can be serious. And you are also likely to have worse side effects if you have ipilimumab (Yervoy) and nivolumab (Opdivo) together. You might have these 2 drugs if you have advanced melanoma.
Cancer vaccines
You probably know about vaccines given to healthy people to help prevent infections, such as measles and chicken pox. These vaccines use weakened or killed germs like viruses or bacteria to start an immune response in the body. Getting the immune system ready to defend against these germs helps keep people from getting infections.
Most cancer vaccines work the same way, cancer vaccines stimulate your immune system into action to attack cancer cells. The immune system makes antibodies that can recognize and attack the harmless versions of the disease. Once the body has made these antibodies it can recognize the disease if you come into contact with it again. The goal is to help treat cancer or to help keep it from coming back after other treatments. But there are also some vaccines that may actually help prevent certain cancers.
Vaccines to prevent cancer
Many people might not realize it, but some cancers are caused by viruses. Vaccines that help protect against infections with these viruses might also help prevent some of these cancers.
- Some strains of the human papilloma virus (HPV) have been linked to cervical, anal, throat, and some other cancers. Vaccines against HPV may help protect against some of these cancers.
- People who have chronic (long-term) infections with the hepatitis B virus (HBV) are at higher risk for liver cancer. Getting the vaccine to help prevent HBV infection may therefore lower some people’s risk of getting liver cancer.
These are traditional vaccines that target the viruses that can cause certain cancers. They may help protect against some cancers, but they don’t target cancer cells directly.
These types of vaccines are only useful for cancers known to be caused by infections. But most cancers, such as colorectal, lung, prostate, and breast cancers, are not thought to be caused by infections. Doctors are not yet sure if it’s possible to make vaccines to prevent these other cancers. Some researchers are now trying, but this research is still in very early stages. Even if such vaccines prove to be possible, it will be many years before they become available.
Vaccines to treat cancer
Cancer treatment vaccines are different from the vaccines that work against viruses. These vaccines try to get the immune system to mount an attack against cancer cells in the body. Instead of preventing disease, they are meant to get the immune system to attack a disease that already exists.
Some cancer treatment vaccines are made up of cancer cells, parts of cells, or pure antigens. Sometimes a patient’s own immune cells are removed and exposed to these substances in the lab to create the vaccine. Once the vaccine is ready, it’s injected into the body to increase the immune response against cancer cells.
Vaccines are often combined with other substances or cells called adjuvants that help boost the immune response even further.
Cancer vaccines cause the immune system to attack cells with one or more specific antigens. Because the immune system has special cells for memory, it’s hoped that the vaccine might continue to work long after it’s given.
Cancer vaccines might help to:
- stop further growth of a cancer
- prevent a cancer from coming back
- destroy any cancer cells left behind after other treatments
Sipuleucel-T (Provenge®)
This is the only vaccine approved in the US to treat cancer so far. It’s used to treat advanced prostate cancer that is no longer being helped by hormone therapy.
For this vaccine, immune system cells are removed from the patient’s blood and sent to a lab. There they are exposed to chemicals that turn them into special immune cells called dendritic cells. They are also exposed to a protein called prostatic acid phosphatase (PAP), which should produce an immune response against prostate cancer cells.
The dendritic cells are then given back to the patient by infusion into a vein (IV). This process is repeated twice more, 2 weeks apart, so that the patient gets 3 doses of cells. Back in the body, the dendritic cells help other immune system cells attack the prostate cancer.
Although the vaccine doesn’t cure prostate cancer, it has been shown to help extend patients’ lives by several months on average. Studies to see if this vaccine can help men with less advanced prostate cancer are now being done.
Side effects are usually mild and can include fever, chills, fatigue, back and joint pain, nausea, and headache. A few men may have more severe symptoms, including problems breathing and high blood pressure.
Other vaccines
Scientists are studying many different types of cancer vaccines and how they work in different ways. More research is needed before they have a full picture of how well this type of treatment works and which cancers it may treat.
Many different types of cancer vaccines have shown some promise in clinical trials, but they are not yet approved in the United States to treat cancer.
The following types of cancer vaccines are most commonly under investigation throughout the world:
- Antigen vaccines
These vaccines are made from special proteins (antigens) in cancer cells. They aim to stimulate your immune system to attack the cancer. Scientists have worked out the genetic codes of many cancer cell proteins, so they can make them in the lab in large quantities.
- Whole cell vaccines
A whole cell vaccine uses the whole cancer cell, not just a specific cell protein (antigen), to make the vaccine. Scientists make the vaccine from your own cancer cells, another person’s cancer cells or cancer cells that were grown in the laboratory.
- Dendritic cell vaccines
Dendritic cells help the immune system recognize and attack abnormal cells, such as cancer cells. To make the vaccine, scientists grow dendritic cells alongside cancer cells in the lab. The vaccine then stimulates your immune system to attack the cancer.
- DNA vaccines
These vaccines are made with bits of DNA from cancer cells. They can be injected into the body to make the cells of the immune system better at responding to and destroying cancer cells.
- Anti idiotype vaccines
This vaccine stimulates the body to make antibodies against cancer cells.
Tumor-infiltrating lymphocytes
This approach uses T cells that are naturally found in a patient’s tumor, called tumor-infiltrating lymphocytes (TILs). TILs that best recognize the patient’s tumor cells in laboratory tests are selected, and these cells are grown to large numbers in the laboratory. The cells are then activated by treatment with immune system signaling proteins called cytokines and infused into the patient’s bloodstream.
The idea behind this approach is that the TILs have already shown the ability to target tumor cells, but there may not be enough of them in the tumor microenvironment to kill the tumor or to overcome the immune suppressive signals that the tumor is releasing. Introducing massive amounts of activated TILs can help to overcome these barriers.
CAR T-cell therapy
Chimeric antigen receptor (CAR) T-cell therapy is still quite new and researchers are looking into how well it works as a treatment for cancer. You might have it as part of a clinical trial.
To understand CAR T-cell therapy more, it helps to understand what T cells do.
White blood cells called lymphocytes play an important part in fighting infection and diseases, including cancer. There are different types of lymphocytes. T cells are one type.
T cells move around the body to find and destroy defective cells. When you come into contact with a new infection or disease, the body makes T cells to fight that specific infection or disease. It then keeps some in reserve so that if you come across the infection again your body can recognise it and attack it immediately.
T cells are good at fighting infection. But it can be difficult for them to tell the difference between a cancer cell and a normal cell. So the cancer cells can hide away and not be recognised.
Your immune system has many different kinds of cells that work together to destroy foreign substances. First, the immune system has to recognize that these substances do not belong in the body. It does this by finding proteins on the surface of those cells, called antigens. Some immune cells, like T-cells, have their own proteins (called receptors) that attach to foreign antigens and help trigger other parts of the immune system to destroy the foreign substance. The relationship between antigens and immune receptors is like a lock and key. Just as every lock can only be opened with the right key, each foreign antigen has a unique immune receptor that is able to bind to it. Cancer cells also have antigens, but the immune system has a tougher time knowing cancer cells are foreign. If your immune cells do not have the right receptor (protein) to find a cancer cell’s antigen, they cannot attach to it and help destroy the cancer cell.
Scientists are trying to find ways to get T cells to recognise cancer cells. One possible way to do this might be CAR T-cell therapy.
What happens with CAR T-cell therapy
With this treatment, you have a sample of T cells taken from your blood. Your medical team do this through a process called apheresis or leukapheresis.
First you have a tube put into a vein in each arm. One tube removes the blood and passes it into an apheresis machine. The machine separates the different parts of the blood. For CAR T-cell therapy, the machine takes out your T cells. The rest of your blood cells and normal blood fluid go back into your body through the tube in your other arm.
In the lab, scientists change the T cells. You might hear this called genetically engineering the T cell by adding the specific chimeric antigen receptor (CAR). The T cell is now a CAR T-cell. CAR stands for chimeric antigen receptor. These CAR T-cells are designed to recognise and target a specific protein on the cancer cells.
These changed T cells grow and multiply in the lab. It can take a few weeks to finish making CAR T-cells because a very large number of CAR T-cells are needed for this therapy. Once there are enough CAR T-cells, they will be given back to the patient into your bloodstream to launch a precise attack against the cancer cells. The aim is for the CAR T-cells to then recognise and attack the cancer cells.
The changes they make in the lab mean that they can stay in your body for long periods of time, recognising and attacking the specific cancer cells. Researchers are still looking into how long they might stay in the body.
Which cancer types are currently treated with CAR T-cell therapy
Currently, there are three CAR T-cell therapies approved for use in the United States. Tisagenlecleucel (Kymriah™) is for advanced or recurrent acute lymphoblastic leukemia (ALL) in children and young adults. Axicabtagene ciloleucel (Yescarta™) is approved for patients with certain types of B-cell non-Hodgkin lymphoma who have not responded to or who have relapsed after at least two other kinds of treatment. The other two are for certain types of advanced or recurrent large B-cell lymphoma. This type of lymphoma is one of several types of non-Hodgkin’s lymphoma. This technique has shown very encouraging results in clinical trials against these cancers. In many patients the cancer could not be found after treatment, although it’s not yet clear if these therapies will result in a long-term cure. In some patients the CAR T-cells seem to go away after the cancer has been in remission for a while and researchers are studying whether those patients have a higher risk of their cancer coming back. Researchers are also studying long-term side effects of this kind of treatment. Other CAR T-cell therapies to treat different types of cancer are being studied and are currently only available in clinical trials.
Researchers have produced CAR T-cells for these cancers to target a protein on the surface of the cell called CD19. This protein is on the surface of nearly all B cells.
There are trials looking at CAR T-cell therapy for different types of cancer, including:
- leukemia
- myeloma – a cancer of the plasma cells in the bone marrow
- neuroblastoma – a rare cancer that develops from particular types of nerve cells called neuroblasts, it mostly affects children under the age of 5 years old.
Side effects of CAR T-cell therapy
Some people have had serious side effects from this treatment, especially as the CAR T-cells multiply in the body to fight the cancer. Serious side effects can include very high fevers and dangerously low blood pressure in the days after it’s given.
This is a new treatment, so doctors might not know about all the possible side effects yet. Two known side effects include:
- cytokine-release syndrome
- no B cells or fewer B cells after treatment with CAR T-cells that target CD19
Cytokine release syndrome
Cytokines are group of proteins in the body that play an important part in boosting the immune system. CAR T-cell therapy stimulates the immune system to make large amounts of cytokines. It causes symptoms such as:
- fever (high temperature)
- dizziness due to low blood pressure
- difficulty breathing
This syndrome might happen in the first week of treatment. You can have treatment to reverse the syndrome.
Fewer B cells in some types of CAR T-cell therapy
In treatment for some leukemias, CAR T-cells are designed to recognise a protein called CD 19. CD 19 is found on the surface of most B cells. B cells are a type of white blood cell and, like T cells, they play an important part in fighting infection.
CAR T-cell therapy that targets the CD 19 protein also destroys the B cells. It kills normal B cells as well as cancerous B cells. This either reduces the number of B cells or destroys them all. This makes it difficult for you to fight infections.
You might need treatment for this side effect. This treatment is called immunoglobulin therapy. It contains antibodies to help you fight infection.
Research is still trying to find out if this is a temporary or long term side effect.
Cytokines
Cytokines are a group of proteins in the body that play an important part in boosting your immune system. Interferon and interleukin are types of cytokines found in the body. Scientists have developed man made versions of these to treat cancer.
The man made version of interleukin is called aldesleukin.
Cytokines are injected, either under the skin, into a muscle, or into a vein.
How interferon and aldesleukin work
Interferon and aldesleukin work in several ways, including:
interfering with the way cancer cells grow and multiply
stimulating the immune system and encouraging killer T cells and other cells to attack cancer cells
encouraging cancer cells to produce chemicals that attract immune system cells to them
Interferon
Interferon is also called interferon alfa or Intron A.
Doctors use interferon for several different types of cancer including:
kidney cancer (renal cell cancer)
melanoma
multiple myeloma
some types of leukaemia
You are more likely to have interferon as an injection just under the skin (subcutaneously). Or you might have it into the bloodstream through a drip (infusion).
How often you have it depends on which type of cancer you are having treatment for. Most people have interferon 3 times a week. Or you might have it as a daily injection.
Interleukins
Interleukins are a group of cytokines that act as chemical signals between white blood cells.
Interleukin-2 (IL-2) helps immune system cells grow and divide more quickly. Interleukin-2 (IL-2) activates certain white blood cells in the body called lymphocytes, which fight diseases and infections. A man-made version of Interleukin 2 (IL-2) called Aldesleukin or Proleukin is approved to treat advanced kidney cancer and metastatic melanoma.
Interleukin-2 (IL-2) can be used as a single drug treatment for these cancers, or it can be combined with chemotherapy or with other cytokines such as interferon-alfa. Using interleukin-2 (IL-2) with these treatments might help make them more effective against some cancers, but the side effects of the combined treatment are also increased.
Side effects of interleukin-2 (IL-2) can include flu-like symptoms such as chills, fever, fatigue, and confusion. Most people gain weight. Some have nausea, vomiting, or diarrhea. Many people develop low blood pressure, which can be treated with other medicines. Rare but potentially serious side effects include an abnormal heartbeat, chest pain, and other heart problems. Because of these possible side effects, if interleukin-2 (IL-2) is given in high doses, it must be done in a hospital.
Other interleukins, such as IL-7, IL-12, and IL-21, are now being studied for use against cancer too, both as adjuvants and as stand-alone agents.
Aldesleukin
Aldesleukin (IL-2, Proleukin or interleukin 2) is a man made protein. It is very similar to a protein produced by the body called interleukin-2. Interleukin-2 is part of the immune system.
Doctors use it most often to treat kidney cancer. It is also in clinical trials for some other types of cancer.
You are most likely to have it as an injection just under the skin (subcutaneously). But you may have it into a vein, either as an injection or through a drip.
How often you have this drug depends on which cancer you are being treated for.
Aldesleukin works in a number of ways. It:
- works directly on cancer cells by interfering with how the cells grow and multiply
- stimulates the immune system by encouraging the growth of killer T cells and other cells that attack cancer cells
- encourages cancer cells to send out chemicals that attract immune system cells
How you have it
You usually have adesleukin as an injection just under the skin. You can also have it into your bloodstream.
You have blood tests before starting treatment and during your treatment. They check your levels of blood cells and other substances in the blood. They also check how well your liver and kidneys are working.
- Injection just under the skin
You usually have injections under the skin (subcutaneous injection) into the stomach, thigh or top of your arm.
You might have stinging or a dull ache for a short time after this type of injection but they don’t usually hurt much. The skin in the area may go red and itchy for a while.
You usually have a daily injection under the skin for 5 days then 2 days rest. You have it like this for 4 weeks and then have a week without treatment. Then this 5 week cycle is repeated. The number of cycles of treatment you need depends on how well your cancer responds.
- Drugs into your bloodstream
You have the treatment through a drip into your arm. A nurse puts a small tube (a cannula) into one of your veins and connects the drip to it.
You might need a central line. This is a long plastic tube that gives the drugs into a large vein, either in your chest or through a vein in your arm. It stays in while you’re having treatment, which may be for a few months.
You might have aldesleukin into a vein over several days. This means you will need to stay in hospital. The team caring for you can keep a close eye on how you are coping with it.
Aldesleukin side effects
Each of these effects happens in more than 1 in 10 people (10%). You might have one or more of them.
- Increased risk of infection: Signs of an infection include headaches, aching muscles, a cough, a sore throat, pain passing urine, or feeling cold and shivery.
- Breathlessness and looking pale: Cancer treatment can cause the level of red blood cells to fall (anemia). This makes you breathless and look pale.
- Bruising and bleeding. This is due to a drop in the number of platelets that help clot your blood. If your platelets get very low you may have lots of tiny red spots or bruises on your arms or legs called petechiae. You might notice you:
- bruise more easily
- have nosebleeds
- have bleeding gums when you brush your teeth
- Tiredness (fatigue): You might feel very tired during your treatment.
- Flu like symptoms: You may have headaches, muscle aches (myalgia), a high temperature and shivering.
- Confusion, depression or sleepiness: You might have some mood changes while having this drug.
- Fluid leaking out of small blood vessels: Fluid may leak out of the small blood vessels in your body (vascular leak syndrome) if you have aldesleukin through a drip.
- Inflammation of the lung tissue: This drug can cause inflammation of the lungs (pneumonitis).
- Skin rash: A rash can also be itchy. Tell your doctor or nurse if you have a skin rash. They can prescribe medicine to stop the itching and soothe your skin.
- Feeling or being sick
- Diarrhea
- Loss of appetite
- Difficulty sleeping
- Anxiety: You might feel more worried or panicky than usual.
- Sore mouth: Your mouth might get sore.
- Pain at the injection site
- Low blood pressure.
Interferons
Interferons are chemicals that help the body resist virus infections and cancers. The types of interferon (IFN) are named after the first 3 letters of the Greek alphabet:
- IFN-alfa
- IFN-beta
- IFN-gamma
Only interferon-alfa is used to treat cancer. It boosts the ability of certain immune cells to attack cancer cells. It may also slow the growth of cancer cells directly, as well as the blood vessels that tumors need to grow.
Interferon-alfa can be used to treat these cancers:
- Hairy cell leukemia
- Chronic myelogenous leukemia (CML)
- Follicular non-Hodgkin lymphoma
- Cutaneous (skin) T-cell lymphoma
- Kidney cancer
- Melanoma
- Kaposi sarcoma
Side effects of interferons can include:
- Flu-like symptoms (chills, fever, headache, fatigue, loss of appetite, nausea, vomiting)
- Low white blood cell counts (which increase the risk of infection)
- Skin rashes
- Thinning hair
These side effects can be severe and can make treatment with interferon hard for many people to tolerate. Most side effects don’t last long after the treatment stops, but fatigue can last longer. Other rare long-term effects include damage to nerves, including those in the brain and spinal cord.
Other drugs that boost the immune system
Some other drugs boost the immune system in a non-specific way, similar to cytokines. But unlike cytokines, these drugs are not naturally found in the body.
Thalidomide, lenalidomide, and pomalidomide
Thalidomide (Thalomid®), lenalidomide (Revlimid®), and pomalidomide (Pomalyst®) are known as immunomodulating drugs (or IMiDs). They are thought to work in a general way by boosting the immune system, although it’s not exactly clear how they do this. These drugs are used to treat multiple myeloma and some other cancers.
The drugs can cause side effects such as drowsiness, fatigue, constipation, low blood cell counts, and neuropathy (painful nerve damage). There is also an increased risk of serious blood clots (that start in the leg and can travel to the lungs). These tend to be more likely with thalidomide than with the other drugs.
These drugs can also cause severe birth defects if taken during pregnancy.
Bacille Calmette-Guérin
Bacille Calmette-Guérin (BCG) is a germ that doesn’t cause serious disease in humans, but it does infect human tissues and helps activate the immune system. This makes BCG useful as a form of cancer immunotherapy. BCG was one of the earliest immunotherapies used against cancer and is still being used today.
BCG is used to treat early stage bladder cancer. It is a liquid put into the bladder through a catheter. BCG attracts the body’s immune system cells to the bladder, where they can attack the bladder cancer cells. Treatment with BCG can cause symptoms that are like having the flu, such as fever, chills, and fatigue. It can also cause a burning feeling in the bladder.
BCG can also be used to treat some melanoma skin cancers by injecting it directly into the tumors.
Imiquimod
Imiquimod (Zyclara®) is a drug that is applied to the skin as a cream. It stimulates a local immune response against skin cancer cells. It is used to treat some very early stage skin cancers (or pre-cancers), especially if they are in sensitive areas such as on the face.
The cream is applied anywhere from once a day to twice a week for several months. Some people have serious skin reactions to this drug.
Immunotherapy vs Chemotherapy
Chemotherapy also called chemo is a cancer treatment where powerful chemicals, medicines or drugs is used to kill fast-growing cancer cells in your body. Chemotherapy is most often used to treat cancer, since cancer cells grow and multiply much more quickly than most cells in the body. Surgery and radiation therapy remove, kill, or damage cancer cells in a certain area, but chemotherapy can work throughout the whole body. This means chemotherapy can kill cancer cells that have spread (metastasized) to parts of the body far away from the original (primary) tumor.
Chemotherapy may be used to:
- Keep the cancer from spreading
- Make the cancer grow slower
- Kill cancer cells that may have spread to other parts of the body (metastasized)
- Make side effects from cancer better, like pain or blockages
- Cure cancer
There are many different types of chemotherapy medication, but they all work in a similar way. Chemotherapy stop cancer cells reproducing by targeting cells at different phases of the process of forming new cells, called the cell cycle, which prevents them from growing and spreading in the body. Chemotherapy drugs can be used alone or in combination to treat a wide variety of cancers.
Though chemotherapy is an effective way to treat many types of cancer, chemotherapy treatment also carries a risk of side effects. Some chemotherapy side effects are mild and treatable, while others can cause serious complications.
Sometimes chemotherapy is the only treatment you need. More often, chemotherapy is used with surgery or radiation therapy or both. Here’s why:
- Chemotherapy may be used to shrink a tumor before surgery or radiation therapy. Chemotherapy used in this way is called neoadjuvant chemotherapy.
- Chemotherapy may be used after surgery or radiation therapy to help kill any remaining cancer cells. Chemotherapy used in this way is called adjuvant chemotherapy.
- Chemotherapy may be used with other treatments if your cancer comes back.
When chemotherapy is used
Chemotherapy may be used if cancer has spread or there’s a risk it will.
Chemotherapy can be used to:
- try to cure the cancer completely (curative chemotherapy)
- make other treatments more effective – for example, it can be combined with radiotherapy (chemoradiation) or used before surgery (neo-adjuvant chemotherapy)
- reduce the risk of the cancer coming back after radiotherapy or surgery (adjuvant chemotherapy)
- relieve symptoms if a cure isn’t possible (palliative chemotherapy)
The effectiveness of chemotherapy varies significantly. Ask your doctors about the chances of treatment being successful for you.
Goals of chemotherapy
If your doctor has recommended chemotherapy to treat your cancer, it’s important to understand the goals of chemotherapy treatment when making treatment decisions. There are three main goals for chemotherapy (chemo) in cancer treatment:
- Cure
- Control
- Palliation
Cure
If possible, chemotherapy is used to cure cancer, meaning that the cancer is destroyed – it goes away and doesn’t come back.
Most doctors don’t use the word “cure” except as a possibility or intention. So, when giving treatment that has a chance of curing a person’s cancer, the doctor may describe it as treatment with curative intent.
There are no guarantees, and though cure may be the goal, it doesn’t always work out that way. It often takes many years to know if a person’s cancer is really cured.
Control
If cure is not possible, the goal may be to control the disease. Chemo is used to shrink tumors and/or stop the cancer from growing and spreading. This can help the person with cancer feel better and live longer.
In many cases, the cancer doesn’t completely go away, but is controlled and managed as a chronic disease, much like heart disease or diabetes. In other cases, the cancer may even seem to have gone away for a while, but it’s expected to come back. Then chemo can be given again.
Palliation
Chemo can also be used to ease symptoms caused by the cancer. This is called palliative chemotherapy or palliation.
When the cancer is at an advanced stage, meaning it’s not under control and has spread from where it started to other parts of the body, the goal may be to improve the quality of life or help the person feel better. For instance, chemo may be used to help shrink a tumor that’s causing pain or pressure.
It’s important to know that any treatment that’s used to reduce symptoms or improve comfort is called palliative care. For example, anti-nausea treatments or pain medicines are palliative, and can be used at all stages of treatment. It can be confusing when chemo is used as a palliative treatment, because it’s most often used to try to cure or control the cancer. But when it’s used with the goal of comfort, chemo becomes palliative care.
Chemotherapy types
Chemotherapy can be given in several ways. Your doctors will recommend the best type for you.
The most common types are:
- chemotherapy given into a vein (intravenous chemotherapy) – this is usually done in hospital and involves medicine being given through a tube in a vein in your hand, arm or chest
- chemotherapy tablets (oral chemotherapy) – this usually involves taking a course of medication at home, with regular check-ups in hospital
You may be treated with one type of chemotherapy medicine or a combination of different types.
You’ll usually have several treatment sessions, which will typically be spread over the course of a few months.
How chemotherapy kills cancer cells
Chemotherapy circulates throughout your body in the bloodstream. So it can treat cancer cells almost anywhere in the body. This is known as systemic treatment.
Chemotherapy kills cells that are in the process of splitting into 2 new cells.
Body tissues are made of billions of individual cells. Once we are fully grown, most of the body’s cells don’t divide and multiply much. They only divide if they need to repair damage.
When cells divide, they split into 2 identical new cells. So where there was 1 cell, there are now 2. Then these divide to make 4, then 8 and so on.
In cancer, the cells keep on dividing until there is a mass of cells. This mass of cells becomes a lump, called a tumor.
Because cancer cells divide much more often than most normal cells, chemotherapy is much more likely to kill them.
Some drugs kill dividing cells by damaging the part of the cell’s control center that makes it divide. Other drugs interrupt the chemical processes involved in cell division.
The effects on dividing cells
Chemotherapy damages cells as they divide.
In the center of each living cell is a dark blob, called the nucleus. The nucleus is the control center of the cell. It contains chromosomes, which are made up of genes.
These genes have to be copied exactly each time a cell divides into 2 to make new cells.
Chemotherapy damages the genes inside the nucleus of cells.
Some drugs damage cells at the point of splitting. Some damage the cells while they’re making copies of all their genes before they split. Chemotherapy is much less likely to damage cells that are at rest, such as most normal cells.
You might have a combination of different chemotherapy drugs. This will include drugs that damage cells at different stages in the process of cell division. This means there’s more chance of killing more cells.
Why chemotherapy causes side effects
The fact that chemotherapy drugs kill dividing cells helps to explain why chemotherapy causes side effects. It affects healthy body tissues where the cells are constantly growing and dividing, such as:
- your hair, which is always growing
- your bone marrow, which is constantly producing blood cells
- your skin and the lining of your digestive system, which are constantly renewing themselves
Because these tissues have dividing cells, chemotherapy can damage them. But normal cells can replace or repair the healthy cells that are damaged by chemotherapy.
So the damage to healthy cells doesn’t usually last. Most side effects disappear once your treatment is over. Some side effects such as sickness or diarrhea might only happen during the days you are actually having the drugs.
Immunotherapy for bladder cancer
Bladder cancer begins when cells in the urinary bladder start to grow uncontrollably. As more cancer cells develop, they can form a tumor and spread to other areas of the body.
Depending on the stage of the bladder cancer and other factors, treatment options for people with bladder cancer can include:
- Surgery
- Intravesical therapy
- Chemotherapy
- Radiation therapy
- Immunotherapy
Immunotherapy for Bladder Cancer
Intravesical BCG (for some early-stage bladder cancers)
Bacille Calmette-Guérin (BCG) is a type of bacteria related to the one that causes tuberculosis (TB). While BCG doesn’t usually cause a person to get sick, it can help trigger an immune response. Bacille Calmette-Guérin (BCG) can be put directly into the bladder (as a liquid) through a catheter. This activates immune system cells in the bladder, which in turn can attack bladder cancer cells.
For some early-stage cancers, Bacille Calmette-Guérin (BCG) can be used after transurethral resection of bladder tumor to help keep the cancer from coming back. Treatment is usually started a few weeks after a transurethral resection of bladder tumor and is given once a week for 6 weeks. Sometimes long-term maintenance BCG therapy is given.
Treatment with Bacille Calmette-Guérin (BCG) can cause symptoms that feel like having the flu, such as fever, chills, and fatigue. Bacille Calmette-Guérin (BCG) can also cause a burning feeling in the bladder. Rarely, BCG can spread through the body, leading to a serious infection. One sign of this can be a high fever that isn’t helped by aspirin or similar medicines. If this happens, call your doctor right away.
Immune checkpoint inhibitors (for advanced bladder cancers)
An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoints” – molecules on immune cells that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. But newer drugs that target these checkpoints hold a lot of promise as cancer treatments.
Atezolizumab (Tecentriq), durvalumab (Imfinzi), and avelumab (Bavencio) are drugs that target PD-L1, a protein on cells (including some cancer cells) that helps keep the immune system from attacking them. By blocking PD-L1, these drugs boost the immune response against the cancer cells. This can shrink some tumors or slow their growth.
Nivolumab (Opdivo) and pembrolizumab (Keytruda) target PD-1, another protein that normally helps keep the immune system in check. Blocking PD-1 can help the immune system attack the cancer cells.
Any of these drugs can be used in people with advanced bladder that starts growing again after chemotherapy. Atezolizumab and pembrolizumab can also be used in people who can’t get the chemo drug cisplatin for some reason.
These drugs are given as intravenous (IV) infusions, typically every 2 or 3 weeks.
Possible side effects
Common side effects of these drugs include fatigue, nausea, loss of appetite, fever, urinary tract infections, rash, diarrhea, and constipation.
Less often, more serious side effects can occur. These drugs work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, or other organs.
It’s very important to report any new side effects to your health care team promptly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
Immunotherapy for breast cancer
Most women with breast cancer will have some type of surgery to remove the tumor. Depending on the type of breast cancer and how advanced it is, you might need other types of treatment as well, either before or after surgery, or sometimes both.
Your treatment plan will depend on other factors as well, including your overall health and personal preferences.
There are several ways to treat breast cancer, depending on its type and stage.
Local treatments: Some treatments are local, meaning they treat the tumor without affecting the rest of the body. Types of local therapy used for breast cancer include:
- Surgery
- Radiation therapy
Systemic treatments: Drugs used to treat breast cancer are considered systemic therapies because they can reach cancer cells almost anywhere in the body. They can be given by mouth or put directly into the bloodstream. Depending on the type of breast cancer, different types of drug treatment might be used, including:
- Chemotherapy
- Hormone therapy
- Targeted therapy
Many women get more than one type of treatment for their cancer.
Targeted therapy for HER2-positive breast cancer
For about 1 in 5 women with breast cancer, the cancer cells have too much of a growth-promoting protein known as HER2/neu (or just HER2) on their surface. These cancers, known as HER2-positive breast cancers, tend to grow and spread more aggressively. A number of drugs have been developed that target this protein:
- Trastuzumab (Herceptin): This is a monoclonal antibody, which is a man-made version of a very specific immune system protein. It is often given along with chemo, but it might also be used alone (especially if chemo alone has already been tried). Trastuzumab can be used to treat both early- and late-stage breast cancer. When started before or after surgery to treat early breast cancer, this drug is usually given for a total of 6 months to a year. For advanced breast cancer, treatment is often given for as long as the drug is helpful. This drug is given into a vein (IV).
- Pertuzumab (Perjeta): This monoclonal antibody can be given with trastuzumab and chemo, either before surgery to treat early-stage breast cancer, or to treat advanced breast cancer. This drug is given into a vein (IV).
- Ado-trastuzumab emtansine (Kadcyla, also known as TDM-1): This is a monoclonal antibody attached to a chemotherapy drug. It is used by itself to treat advanced breast cancer in women who have already been treated with trastuzumab and chemo. This drug is also given in a vein (IV).
- Lapatinib (Tykerb): This is a kinase inhibitor. It is a pill taken daily. Lapatinib is used to treat advanced breast cancer, and might be used along with certain chemotherapy drugs, trastuzumab, or hormone therapy drugs.
- Neratinib (Nerlynx): This is another kinase inhibitor. It is a pill that is taken daily. Neratinib is used to treat early-stage breast cancer after a woman has completed one year of trastuzumab and is usually given for one year. Some clinical trials show that it may also be effective in advanced breast cancer, as well.
Side effects of targeted therapy for HER2-positive breast cancer
The side effects of these drugs are often mild, but some can be serious. Discuss what you can expect with your doctor.
Some women develop heart damage during or after treatment with trastuzumab, pertuzumab, or ado-trastuzumab emtansine. This can lead to congestive heart failure. For most (but not all) women, this effect lasts a short time and gets better when the drug is stopped. The risk of heart problems is higher when these drugs are given with certain chemo drugs that also can cause heart damage, such as doxorubicin (Adriamycin) and epirubicin (Ellence). Because these drugs can cause heart damage, doctors often check your heart function (with an echocardiogram or a MUGA scan) before treatment, and again while you are taking the drug. Let your doctor know if you develop symptoms such as shortness of breath, leg swelling, and severe fatigue.
Lapatinib and neratinib can cause severe diarrhea, so it’s very important to let your health care team know about any changes in bowel habits as soon as they happen. Lapatinib can also cause hand-foot syndrome, in which the hands and feet become sore and red, and may blister and peel. Pertuzumab can also cause diarrhea.
If you are pregnant, you should not take these drugs. They can harm and even cause death to the fetus. If you could become pregnant, talk to your doctor about using effective birth control while taking these drugs.
Targeted therapy for hormone receptor-positive breast cancer
About 2 of 3 breast cancers are hormone receptor-positive (ER-positive or PR-positive). For women with these cancers, treatment with hormone therapy is often helpful. Certain targeted therapy drugs can make hormone therapy even more effective, although these targeted drugs might also add to the side effects.
CDK4/6 inhibitors
Palbociclib (Ibrance), ribociclib (Kisqali), and abemaciclib (Verzenio) are drugs that block proteins in the cell called cyclin-dependent kinases (CDKs), particularly CDK4 and CDK6. Blocking these proteins in hormone receptor-positive breast cancer cells helps stop the cells from dividing. This can slow cancer growth.
These drugs are approved for women who have gone through menopause and have advanced hormone receptor-positive, HER2-negative breast cancer. They are used along with certain hormone therapy drugs such as fulvestrant or an aromatase inhibitor (such as letrozole). These drugs are taken as pills, typically once or twice a day.
Abemaciclib can also be used by itself in women who have previously been treated with hormone therapy and chemotherapy.
Side effects of these drugs tend to be mild. The most common side effects are low blood cell counts and fatigue. Nausea and vomiting, mouth sores, hair loss, diarrhea, and headache are less common side effects. Very low white blood cell counts can increase the risk of serious infection.
Everolimus (Afinitor)
Everolimus is used for women who have gone through menopause and have advanced hormone receptor-positive, HER2-negative breast cancer. It is used along with the aromatase inhibitor exemestane (Aromasin) for women whose cancers have grown while being treated with either letrozole or anastrozole (or if the cancer started growing shortly after treatment with these drugs was stopped).
This targeted therapy drug blocks mTOR, a protein in cells that normally helps them grow and divide. Everolimus may also stop tumors from developing new blood vessels, which can help limit their growth. In treating breast cancer, this drug seems to help hormone therapy drugs work better. Everolimus is a pill that is taken once a day.
Common side effects of everolimus include mouth sores, diarrhea, nausea, feeling weak or tired, low blood counts, shortness of breath, and cough. Everolimus can also increase blood lipids (cholesterol and triglycerides) and blood sugars, so your doctor will check your blood work periodically while you are taking this drug. It can also increase your risk of serious infections, so your doctor will watch you closely for infection.
Everolimus is also being studied for use in earlier-stage breast cancer, with other hormone therapy drugs, and in combination with other treatments.
Targeted therapy for women with BRCA gene mutations
Olaparib (Lynparza) is a type of drug known as a PARP inhibitor. PARP proteins normally help repair damaged DNA inside cells. The BRCA genes (BRCA1 and BRCA2) also help repair DNA (in a slightly different way), but mutations in one of those genes can stop this from happening. PARP inhibitors work by blocking the PARP proteins. Because tumor cells with a mutated BRCA gene already have trouble repairing damaged DNA, blocking the PARP proteins often leads to the death of these cells.
Olaparib can be used to treat metastatic, HER2-negative breast cancer in women with a BRCA mutation who have already gotten chemotherapy (and hormone therapy if the cancer is hormone receptor-positive). Only a small portion of women with breast cancer have a mutated BRCA gene. If you are not known to have a BRCA mutation, your doctor will test your blood to be sure you have one before starting treatment with this drug.
This drug comes in pills that are taken once a day.
Side effects can include nausea, vomiting, diarrhea, fatigue, loss of appetite, taste changes, low red blood cell counts (anemia), belly pain, and muscle and joint pain. Rarely, some people treated with a PARP inhibitor have developed a blood cancer, such as myelodysplastic syndrome or acute myeloid leukemia (AML).
Immunotherapy for colon cancer
Treatment for colon cancer is based largely on the stage (extent) of the cancer, but other factors can also be important.
People with colon cancers that have not spread to distant sites usually have surgery as the main or first treatment. Chemotherapy may also be used after surgery (called adjuvant treatment). Most adjuvant treatment is given for about 6 months.
Stage IV colon cancers have spread from the colon to distant organs and tissues. Colon cancer most often spreads to the liver, but it can also spread to other places like the lungs, brain, peritoneum (the lining of the abdominal cavity), or to distant lymph nodes. If the cancer has spread too much to try to cure it with surgery, chemotherapy is the main treatment. Most people with stage IV cancer will get chemotherapy and/or targeted therapies to control the cancer. If one of these regimens is no longer working, another may be tried. For people with certain gene changes in their cancer cells, another option after initial chemotherapy might be treatment with an immunotherapy drugs such as pembrolizumab (Keytruda) and nivolumab (Opdivo).
Immune checkpoint inhibitors
An important part of the immune system is its ability to keep itself from attacking the body’s normal cells. To do this, it uses “checkpoint” proteins on immune cells, which act like switches that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to keep the immune system from attacking them. But drugs that target these checkpoints hold a lot of promise as cancer treatments.
Pembrolizumab (Keytruda) and Nivolumab (Opdivo) are drugs that target PD-1 (programmed cell death protein 1). PD-1 is a protein found on immune system cells called T cells. It normally helps keep these cells from attacking “good” cells in the body.
Pembrolizumab and nivolumab block the cancer cells’ ability to attach to PD-1, so, the immune system can then “see” the cells as “bad.” This boosts the immune response against the cancer cells and can shrink some tumors or slow their growth.
These drugs can be used for people whose colorectal cancer cells have tested positive for specific gene changes, such as a high level of microsatellite instability (MSI-H), or changes in one of the mismatch repair (MMR) genes. The drugs are used for people whose cancer is still growing after treatment with chemotherapy. They might also be used to treat people whose cancer can’t be removed with surgery, has come back (recurred) after treatment, or has spread to other parts of the body (metastasized).
Pembrolizumab (Keytruda) is given as an intravenous (IV) infusion. Treatment takes about 30 minutes and is given every 3 weeks.
Nivolumab (Opdivo) is given as an (IV infusion) that takes 1 hour. It’s given every 2 weeks.
Possible side effects
Side effects can include:
- Fatigue
- Fever
- Cough
- Shortness of breath
- Itching
- Skin rash
- Nausea
- Loss of appetite
- Diarrhea
- Constipation
- Muscle and/or joint pain
Other, more serious side effects occur less often. Checkpoint inhibitors work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, or other organs.
It’s very important to tell your cancer care team about new side effects right away. Let them know about any changes you notice. If serious side effects do occur, treatment may need to be stopped and you may get high doses of steroids to suppress your immune system.
Immunotherapy for lung cancer
If you’ve been diagnosed with non-small cell lung cancer, your cancer care team will discuss your treatment options with you.
Depending on the stage of the cancer and other factors, treatment options for people with non-small cell lung cancer can include:
- Surgery
- Radiofrequency ablation
- Radiation therapy
- Chemotherapy
- Targeted therapies
- Immunotherapy
Palliative treatments can also be used to help with symptoms.
In many cases, more than one of type of treatment is used.
Immunotherapy for Non-Small Cell Lung Cancer
Immune checkpoint inhibitors
An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoints” – molecules on immune cells that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. But newer drugs that target these checkpoints hold a lot of promise as cancer treatments.
- Nivolumab (Opdivo) and pembrolizumab (Keytruda) target PD-1, a protein on immune system cells called T cells that normally helps keep these cells from attacking other cells in the body. By blocking PD-1, these drugs boost the immune response against cancer cells. This can shrink some tumors or slow their growth.
- Atezolizumab (Tecentriq) targets PD-L1, a protein related to PD-1 that is found on some tumor cells and immune cells. Blocking this protein can also help boost the immune response against cancer cells.
Nivolumab, pembrolizumab and atezolizumab can be used in people with certain types of non-small cell lung cancer whose cancer starts growing again after chemotherapy or other drug treatments. Pembrolizumab can also be used as the first treatment in some people, either along with or instead of chemo.
- Durvalumab (Imfinzi) also targets the PD-L1 protein. This drug is used a little differently than the other immunotherapy drugs. It is used in people with certain types of non-small cell lung cancer whose cancer has not gotten worse after they have already received chemotherapy along with radiation (chemoradiation). The goal of treatment with this drug is to keep the cancer from getting worse for as long as possible.
These immunotherapy drugs are given as an intravenous (IV) infusion every 2 or 3 weeks.
Possible side effects
Side effects of these drugs can include fatigue, cough, nausea, itching, skin rash, loss of appetite, constipation, joint pain, and diarrhea.
Other, more serious side effects occur less often. These drugs work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, or other organs.
It’s very important to report any new side effects to your health care team promptly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
Immunotherapy for melanoma
Once melanoma has been diagnosed and staged, your cancer care team will discuss your treatment options with you. Based on the stage of the melanoma cancer and other factors, your treatment options might include:
- Surgery
- Immunotherapy
- Targeted therapy
- Chemotherapy
- Radiation therapy
Early-stage melanomas can often be treated with surgery alone, but more advanced cancers often require other treatments. Sometimes more than one type of treatment is used.
Immune checkpoint inhibitors for melanoma skin cancer
These newer drugs have shown a lot of promise in treating advanced melanomas. An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoints”, which are proteins on immune cells that need to be turned on (or off) to start an immune response. Melanoma cells sometimes use these checkpoints to avoid being attacked by the immune system. But these drugs target the checkpoint proteins, helping to restore the immune response against melanoma cells.
PD-1 inhibitors
Pembrolizumab (Keytruda) and nivolumab (Opdivo) are drugs that target PD-1, a protein on immune system cells called T cells that normally help keep these cells from attacking other cells in the body. By blocking PD-1, these drugs boost the immune response against melanoma cells. This can often shrink tumors and help people live longer (although it’s not yet clear if these drugs can cure melanoma).
These drugs are given as an intravenous (IV) infusion every 2 or 3 weeks.
Side effects of these drugs can include fatigue, cough, nausea, itching, skin rash, decreased appetite, constipation, joint pain, and diarrhea.
Other, more serious side effects occur less often. These drugs work by basically removing the brakes from the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands, kidneys, or other organs.
It’s very important to report any new side effects to your health care team promptly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of corticosteroids to suppress your immune system.
CTLA-4 inhibitor
Ipilimumab (Yervoy) is another drug that boosts the immune response, but it has a different target. It blocks CTLA-4, another protein on T cells that normally helps keep them in check.
This drug is given as an intravenous (IV) infusion, usually once every 3 weeks for 4 treatments. In patients with melanomas that can’t be removed by surgery or that have spread to other parts of the body, this drug has been shown to help people live longer, although it’s not clear if it can cure the melanoma.
The most common side effects from this drug include fatigue, diarrhea, skin rash, and itching.
Serious side effects seem to happen more often with this drug than with the PD-1 inhibitors. Like the PD-1 inhibitors, this drug can cause the immune system to attack other parts of the body, which can lead to serious problems in the intestines, liver, hormone-making glands, nerves, skin, eyes, or other organs. In some people these side effects can be life threatening.
It’s very important to report any new side effects during or after treatment to your health care team promptly. If serious side effects do occur, you may need to stop treatment and take high doses of corticosteroids to suppress your immune system.
Cytokines (interferon-alfa and interleukin-2)
Cytokines are proteins in the body that boost the immune system in a general way. Man-made versions of cytokines, such as interferon-alfa and interleukin-2 (IL-2), are sometimes used in patients with melanoma. They are given as intravenous (IV) infusions, at least at first. Some patients or caregivers may be able to learn how to give injections under the skin at home.
For advanced melanomas: Both interferon-alfa and IL-2 can shrink advanced melanomas in about 10% to 20% of patients when used alone. These drugs may also be given along with chemotherapy drugs (known as biochemotherapy) for stage IV melanoma.
Side effects can include flu-like symptoms such as fever, chills, aches, severe tiredness, drowsiness, and low blood cell counts. Interleukin-2, particularly in high doses, can cause fluid to build up in the body so that the person swells up and can feel quite sick. Because of this and other possible serious side effects, high-dose IL-2 is given only in the hospital, in centers that have experience with this type of treatment.
After surgery for some earlier-stage melanomas: Thicker melanomas are more likely than thinner melanomas to come back in another part of the body after surgery, even if all of the cancer is thought to have been removed. Interferon-alfa can sometimes be used as an added (adjuvant) therapy after surgery to try to prevent this. This may delay the recurrence of melanoma, but it’s not yet clear if it improves survival.
High doses must be used for the interferon to be effective, but many patients can’t take the side effects of high-dose therapy. These can include fever, chills, aches, depression, feeling very tired, and effects on the heart and liver. Patients getting this drug need to be watched closely by a doctor who is experienced with this treatment.
When deciding whether to use adjuvant interferon therapy, patients and their doctors need to take into account the potential benefits and side effects of this treatment.
Oncolytic virus therapy
Viruses are a type of germ that can infect and kill cells. Some viruses can be altered in the lab so that they infect and kill mainly cancer cells. These are known as oncolytic viruses. Along with killing the cells directly, the viruses can also alert the immune system to attack the cancer cells.
Talimogene laherparepvec (Imlygic), also known as T-VEC, is an oncolytic virus that can be used to treat melanomas in the skin or lymph nodes that can’t be removed with surgery. The virus is injected directly into the tumors, typically every 2 weeks. This treatment can sometimes shrink these tumors, but it hasn’t been shown to shrink tumors in other parts of the body. It’s also not clear if this treatment can help people live longer. Side effects can include flu-like symptoms and pain at the injection site.
Bacille Calmette-Guerin (BCG) vaccine
BCG is a germ related to the one that causes tuberculosis. BCG doesn’t cause serious disease in humans, but it does activate the immune system. The BCG vaccine is sometimes used to help treat stage III melanomas by injecting it directly into tumors.
Imiquimod cream
Imiquimod (Zyclara) is a drug that is put on the skin as a cream. It stimulates a local immune response against skin cancer cells. For very early (stage 0) melanomas in sensitive areas on the face, some doctors may use imiquimod if surgery might be disfiguring. It can also be used for some melanomas that have spread along the skin. Still, not all doctors agree it should be used for melanoma.
The cream is usually applied 2 to 5 times a week for around 3 months. Some people have serious skin reactions to this drug. Imiquimod is not used for more advanced melanomas.
Immunotherapy for pancreatic cancer
If you’ve been diagnosed with pancreatic cancer, your cancer care team will discuss your treatment options with you.
Depending on the type and stage of the cancer and other factors, treatment options for people with pancreatic cancer can include:
- Surgery
- Ablation or embolization treatments
- Radiation therapy
- Chemotherapy and other drugs
Pain control is also an important part of treatment for many patients.
Sometimes, the best option might include more than one type of treatment.
The cell surface molecule CD40 is a member of the tumor necrosis factor receptor superfamily and is broadly expressed by immune cells, in particular B cells, dendritic cells and monocytes, as well as other normal cells and some malignant cells 1. CD40 agonist antibodies (αCD40) promote antigen-presenting cell maturation and enhance macrophage tumoricidal activity 2 Beatty et al. 3 reported on a small cohort of pancreatic ductal adenocarcinoma patients treated with gemcitabine chemotherapy plus anti-CD40 agonist antibodies and observed tumor regressions in a CD40-dependent mechanism by targeting tumor stroma. More recent studies suggested that CD40 agonists can mediate both T-cell-independent and T-cell-dependent immune mechanisms of tumor regression in pancreatic cancer. An early clinical trial testing agonist CD40 monoclonal antibody in combination of gemcitabine was well-tolerated and associated with increased antitumor activity in patients with pancreatic ductal adenocarcinoma 4.
Immunotherapy for prostate cancer
Depending on each case, treatment options for men with prostate cancer might include:
- Watchful waiting or active surveillance
- Surgery
- Radiation therapy
- Cryotherapy (cryosurgery)
- Hormone therapy
- Chemotherapy
- Vaccine treatment
- Bone-directed treatment
These treatments are generally used one at a time, although in some cases they may be combined.
Cancer vaccine treatment for prostate cancer
Sipuleucel-T (Provenge) is a cancer vaccine. Unlike traditional vaccines, which boost the body’s immune system to help prevent infections, this vaccine boosts the immune system to help it attack prostate cancer cells.
The vaccine is used to treat advanced prostate cancer that’s no longer responding to hormone therapy but is causing few or no symptoms.
This vaccine is made specifically for each man. To make it, white blood cells (cells of the immune system) are removed from your blood over a few hours while you are hooked up to a special machine. The cells are then sent to a lab, where they are exposed to a protein from prostate cancer cells called prostatic acid phosphatase (PAP). The cells are then sent back to the doctor’s office or hospital, where they are given back to you by infusion into a vein (IV). This process is repeated 2 more times, 2 weeks apart, so that you get 3 doses of cells. The cells help your other immune system cells attack the prostate cancer.
The vaccine hasn’t been shown to stop prostate cancer from growing, but it seems to help men live an average of several months longer. As with hormone therapy and chemotherapy, this type of treatment has not been shown to cure prostate cancer.
Studies are now being done to see if this vaccine can help men with less advanced prostate cancer.
Possible side effects of vaccine treatment
Side effects from the vaccine tend to be milder than those from hormone therapy or chemotherapy. Common side effects can include fever, chills, fatigue, back and joint pain, nausea, and headache. These most often start during the cell infusions and last no more than a couple of days. A few men may have more severe symptoms, including problems breathing and high blood pressure, which usually get better after treatment.
- Prospect of targeting the CD40 pathway for cancer therapy. Vonderheide RH. Clin Cancer Res. 2007 Feb 15; 13(4):1083-8. http://clincancerres.aacrjournals.org/content/13/4/1083.long[↩]
- Molecular mechanism and function of CD40/CD40L engagement in the immune system. Elgueta R, Benson MJ, de Vries VC, Wasiuk A, Guo Y, Noelle RJ. Immunol Rev. 2009 May; 229(1):152-72. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3826168/[↩]
- Vonderheide R.H., Bajor D.L., Winograd R., Evans R.A., Bayne L.J., Beatty G.L. CD40 Agonists Alter Tumor Stroma and Show Efficacy Against Pancreatic Carcinoma in Mice and Humans. Science. 2011;331:1612–1616 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3406187/[↩]
- Beatty G.L., Torigian D.A., Chiorean E.G., Saboury B., Brothers A., Alavi A., Troxel A.B., Sun W., Teitelbaum U.R., Vonderheide R.H., et al. A phase I study of an agonist CD40 monoclonal antibody (CP-870,893) in combination with gemcitabine in patients with advanced pancreatic ductal adenocarcinoma. Clin. Cancer Res. 2013;19:6286–6295. doi: 10.1158/1078-0432.CCR-13-1320 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3834036/[↩]





{kind=link}