Contents
What is colpocleisis
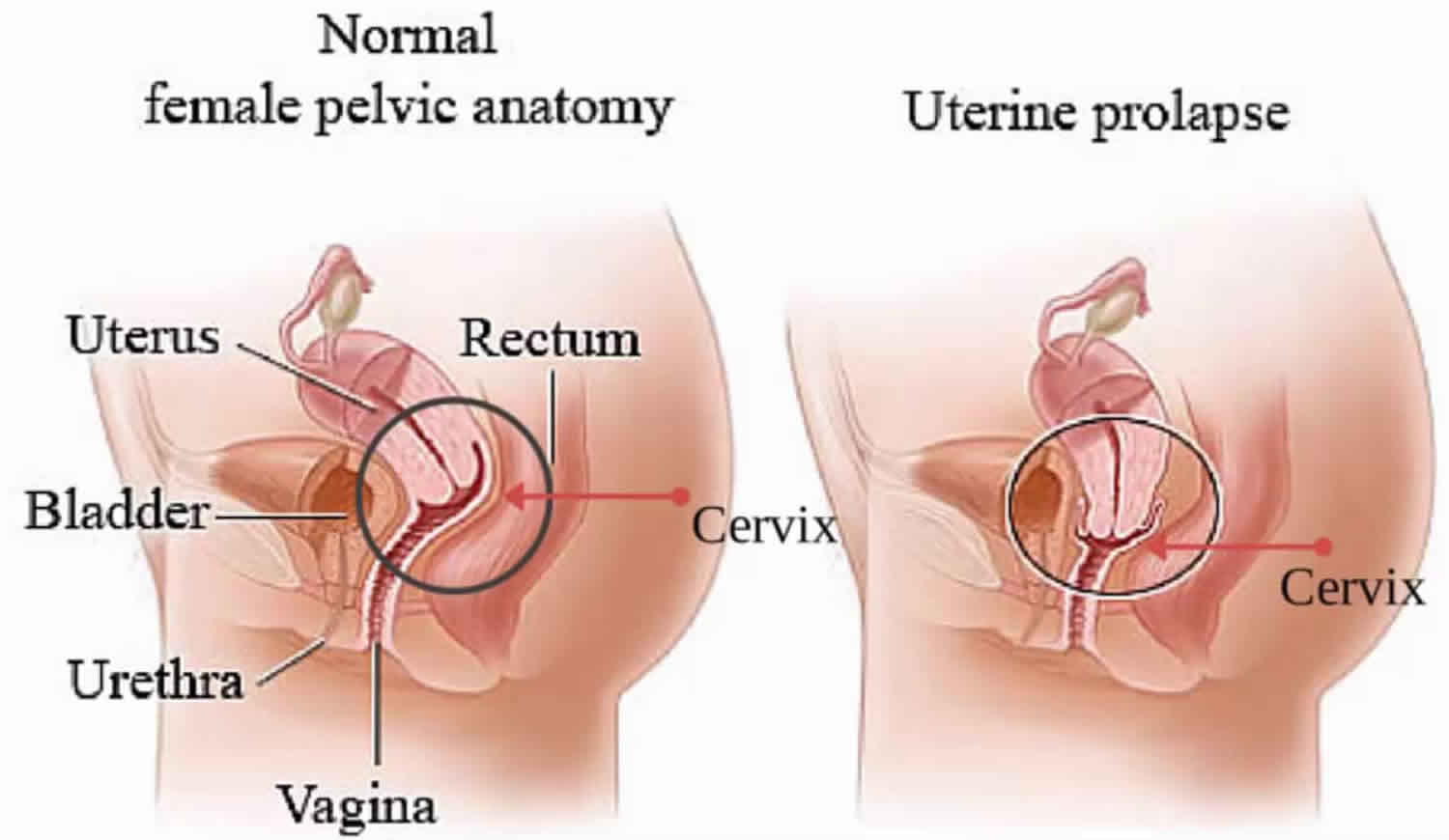
Colpocleisis is vaginal obliteration or closure of the vagina surgery for treatment of severe uterine or vaginal vault prolapse (advanced pelvic organ prolapse) in women who no longer desires sexual intercourse or whose other chronic health problems make a longer surgical procedure more dangerous 1. Colpocleisis is done for an older woman whose uterus has moved from its natural position to press uncomfortably into the vagina (uterine prolapse). LeFort colpocleisis procedure may also be done if an older woman’s vagina severely sags or drops into the vaginal canal (vaginal vault prolapse). In this surgery, the vagina is sewn shut. Colpocleisis surgery treats prolapse by narrowing and shortening the vagina. It works well and carries a low risk, but it is not a good choice for women who want to be able to have vaginal intercourse 2. Colpocleisis remains one of the most durable and least invasive surgical procedures for pelvic organ prolapse, with success rates of 98% to 100% reported 3. Recent studies continue to confirm high success rates and improved body image, with low morbidity and mortality 4.
Pelvic organ prolapse affects millions of women in the United States, with more than 300,000 surgeries performed annually to address conditions of the pelvic floor 5. The lifetime risk of having surgery for prolapse or incontinence by age 80-85 is 11-19%, with 30% of women requiring additional prolapse procedures 6. With the rapid rise in the elderly population, the number of surgeries performed yearly is projected to increase dramatically.
Colpocleisis is done by removing the entire vaginal lining except for 2.5 cm (1 in.) to 4 cm (1.5 in.). The vagina is then sewn shut. If the uterus is still present, a small opening is left in the vagina to allow fluids to drain from the uterus.
Because colpocleisis is a relatively brief surgical procedure, it may be done when a woman has one or more severe long-term (chronic) medical conditions, such as asthma or heart disease, that make a longer procedure more of a risk.
All colpocleisis procedures involve removal of the vaginal epithelium. The 2 most common types are partial and total colpocleisis. Partial colpocleisis (LeFort) involves surgical creation of a longitudinal vaginal septum by apposition of denuded anterior and posterior vaginal walls. LeFort colpocleisis is the only obliterative option if the uterus is to be preserved; however, it is also appropriate in cases of posthysterectomy prolapse. In LeFort’s publication, he describes a partial colpocleisis technique that left the uterus in situ, after which a perineorrhaphy was performed 8 days postoperatively 7. His technique was based on the premise that apposition of the vaginal walls could prevent uterine prolapse and that a widened genital hiatus may lead to unsuccessful outcomes. His theory holds true today; this obliterative procedure is associated with high rates of satisfaction 8.
Both partial and total colpocleisis are commonly combined with levator plication and perineorrhaphy 9.
LeFort colpocleisis (partial colpocleisis), in comparison with complete colpocleisis, offers several advantages 10. The most obvious advantage is the avoidance of recurrent prolapse in sexually nonactive, older patients. Historically, colpocleisis has been reported to produce stress incontinence, which may be avoided by partial colpocleisis. Careful attention to avoiding anterior wall adhesions by leaving anterior and posterior vaginal walls separated and a very small, nonfunctional vagina will prevent scarring with fixation at the bladder neck, which in most instances will result in stress incontinence. To leave a functional vagina in an elderly women, not active for many years and with no plans for sexual activity, will leave the patient with the possibility of recurrent prolapse. Partial colpocleisis, a relatively short procedure with minimal blood loss and with careful attention to the avoidance of scarring between the anterior and posterior walls, will obviate the reported stress incontinence following complete colpocleisis. A retrospective study by Song et al 11 of 35 women who underwent LeFort colpocleisis found that at median 5-year follow-up, 33 patients (94.3%) reported satisfaction with the surgery, with two patients, one of whom suffered postoperative overactive bladder syndrome and another of whom had vaginal hematoma, characterizing themselves as “neither satisfied nor dissatisfied.” Using the Chinese version of the Pelvic Floor Distress Inventory-short form 20, the investigators also found significant improvement in pelvic symptoms (from a preoperative score of 60.5 to a postoperative score of 14.1).
Currently, there are no standard guidelines for colpocleisis. Among the wide variation that exists in clinical practice are LeFort versus total colpocleisis, routine preoperative endometrial evaluation, and concomitant procedures such as hysterectomy and procedures for urinary incontinence.
The primary disadvantage to colpocleisis procedures is loss of the ability to have vaginal intercourse. In addition, the colpocleisis procedure precludes the ability to evaluate the cervix or uterus for pathologic changes. Evaluating candidates for cervical or uterine abnormalities prior to surgery is therefore important. This entails reviewing previous pap smears and cervical biopsies and asking targeted questions regarding patients with postmenopausal bleeding who may require endometrial biopsy or ultrasound to evaluate endometrial thickness.
With regards to sexual activity, a study of older adults on their sexuality reported that the prevalence of sexual activity decreased with age. Sexual activity amongst women ages 57 to 64 was 62% and decreased to 17% in women ages 75 to 85 12. As the number of women older than age 60 years seeking care for pelvic floor disorders is projected to increase at least 45% over the next few decades, many patients may forego preservation of vaginal function for a minimally invasive approach with long-lasting outcomes 13.
Advantages to this approach include shorter operative time, decreased morbidity, decreased blood loss, faster recovery, and high anatomic success rates. A retrospective cohort study of women (mean age 80) who had advanced prolapse reported comparable satisfaction after colpocleisis versus reconstructive surgery 13. In another study, women with mean age of 79 reported significant improvement in pelvic symptoms and related bother after having colpocleisis performed. Ninety five percent of those patients reported that they were either “very satisfied” or “satisfied” with the outcome of their surgery 14.
In a more recent multicenter study by Crisp et al 15, colpocleisis as a definitive surgical intervention resulted in a positive impact on bowel, bladder, and prolapse symptoms. A high rate of satisfaction and low levels of regret were reported 15. In another study of 310 women, the largest case series to date, Zebede et al 16 reported a 98.1% anatomic success with a 92.9% patient satisfaction. The complication rate was low (15.2%) and the mortality rate was 1.3%; this suggests that colpocleisis is a low-risk, effective procedure.
Colpocleisis technique
Colpocleisis involves the removal of vaginal epithelium and subsequent imbrication of the vaginal muscularis in anterior-to-posterior apposition, thereby creating a tissue septum of support. Variations in technique are based on the size and amount of epithelium removed.
LeFort’s original description called for the creation of 2 trapezoids of the anterior and posterior vaginal epithelium with subsequent imbrication creating a tissue platform. The remaining lateral vaginal epithelium is contiguous with the cervix and creates 2 lateral tunnels, permitting postoperative drainage as well as a channel for any postmenopausal bleeding remote from surgery.
During dissection of the anterior vaginal epithelium, care is taken not to dissect beyond the urethrovesical junction because this can lead to inadvertent cystotomy. This is also performed in an effort not to cause downward traction at the bladder neck because this can potentially increase the risk of stress incontinence postoperatively.
Hematoma formation is the most common culprit in the breakdown or failure of colpocleisis. Hemostasis is therefore maintained throughout the procedure via use of Bovie cautery and the application of pressure to areas of bleeding. In addition, as bleeding often occurs at the leading edges of the trapezoids, the anterior and posterior segments are brought together with full-thickness purchase of tissue.
Colpocleisis contraindications
Although colpocleisis surgery is minimally invasive, patients with severe cardiopulmonary risk factors leading to increased anesthetic risk may not be able to undergo this surgery. Colpocleisis surgery is contraindicated in patients with cervical and uterine pathology requiring extensive surgical resection and staging of disease. The ideal patient would therefore have negative pap smears and no history of postmenopausal bleeding with uterine pathology.
Colpocleisis procedure
General, regional, or local anesthesia may be used for colpocleisis surgery. Prophylactic broad spectrum antibiotics should be given in accordance with the most recent guidelines. Patients with cardiovascular risk factors should receive beta blockade during the perioperative time frame. Patients should also be stratified in accordance to thromboembolic risk. Compression stockings and/or pharmacologic prophylaxis should be used to prevent clot formation 17. Being mindful when placing the patient in dorsal lithotomy is important because inappropriate patient positioning can result in nerve injury.
LeFort colpocleisis procedure
First, the anterior and posterior compartments are inspected for any areas of irritation or ulcerations because they may need to be addressed prior to the start of the procedure. If a uterus is in place, your surgeon starts by performing cervical dilation and uterine curettage to rule out any intrauterine pathology.
Next, your surgeon will delineate equivalent trapezoids posteriorly and anteriorly with a marker (watch YouTube videos above). The epithelium inside each trapezoid is then infiltrated with 1% lidocaine with epinephrine to aid in dissection.
A scalpel blade is used to incise the epithelial outlines previously made. On the anterior wall, the epithelium is then carefully dissected off the underlying muscularis bluntly and sharply with Metzenbaum scissors. Hemostasis is maintained with Bovie cautery. The same is performed on the posterior wall.
The leading edges of the anterior and posterior rectangles are brought together with 2.0 Vicryl sutures in a running, non-locking fashion, taking full thickness with each pass of the needle. The muscularis layer is approximated in an anterior to posterior fashion using interrupted 2.0 Vicryl suture.
Simultaneously, interrupted sutures are placed laterally for the creation of the tunnels. Imbrication is performed until the most proximal edges of the anterior and posterior trapezoids are approximated. By doing this, the viscera is placed back into the pelvis. The 2 epithelial edges are then brought together with a series of interrupted 2.0 Vicryl sutures.
Next, a high perineoplasty is performed. A diamond-shaped flap of the perineal/vulvar mucosa is identified. After infiltration with 1% lidocaine with epinephrine, the triangle is then excised with a scalpel. The perineal body is then reconstructed side to side with use of 1.0 Vicryl suture followed by skin closure with 2.0 Vicryl suture. Typically, after the perineorrhaphy, the genital hiatus should allow passage of one finger.
To complete the surgery, a cystoscopy is performed to ensure no ureteral kinking, cystotomy, or urethral or bladder pathology. Five- to ten minutes before cystoscopy, 5 mL of indigo carmine is given intravenously. A 70° scope is introduced into the bladder and a systematic surveillance is performed. Ureteral function is reassured by the peristalsis and efflux of indigo carmine-tinged urine from the ureteric orifices bilaterally. Lastly, a rectal examination is performed to detect the presence of suture within the rectum.
Mid-Urethral Sling
Concomitant mid-urethral sling and colpocleisis appears to be quite effective. A small case series of 38 women demonstrated that colpocleisis with concomitant mid-urethral sling improves urinary symptoms without causing significant urinary retention 18.
In a retrospective study, the complications and outcomes of 30 women undergoing colpocleisis and sling without general anesthesia was reviewed. With a follow-up of 19.1 months, no intraoperative complications were reported; however, 1 postoperative myocardial infarction and 3 women requiring reoperation for prolapse were reported. The cure rate for stress incontinence was reported at 94% 19.
In another retrospective study, 210 women underwent colpocleisis, of which 161 had concurrent suburethral sling. Placement of the sling resulted in 92.5% stress continent rate and 91% resolution of voiding dysfunction postoperatively 20. Collectively, these studies suggest that placement of a sling at the time of colpocleisis results in high rates of continence with minimal voiding dysfunction postoperatively. Currently, research in the concomitant use of prophylactic anti-incontinent procedure in those undergoing vaginal prolapse surgeries is ongoing. Note that if a continent procedure is to be performed at the same time of colpocleisis, it may be performed once half of the vaginal canal has been obliterated.
Hysterectomy
Concomitant hysterectomy is often performed at the time of pelvic organ prolapse surgery. However, a retrospective study of 92 women who underwent colpocleisis with concomitant hysterectomy showed significant increase in operative duration and transfusion rates compared to no hysterectomy 12. Those recommending hysterectomy at the time of colpocleisis reason that colpocleisis precludes future evaluation of the cervix or uterus. Hysterectomy also obviates the possibility of future pyometra, which is a rare complication. The surgical outcomes with or without hysterectomy is equivalent. Hysterectomy may be strongly considered, however, in cases of increased cervical or uterine cancer risk.
Colpocleisis surgery recovery
You may stay in the hospital from 1 to 2 days. Prior to your hospital discharge, a voiding trial is performed. For patients with preoperative urinary retention, the authors use a suprapubic catheter. Those going home with a catheter are given nitrofurantoin or ciprofloxacin to prevent infection and are seen in the office within 5-6 days for catheter removal and subsequent bladder challenge. Pain control is usually accomplished with intravenous and oral medications, with a rare need for patient-controlled analgesia. Patients are discharged home with ibuprofen and acetaminophen with hydrocodone.
A follow-up postoperative visit is scheduled at 2 weeks. At this time, uterine pathology is reviewed if the patient had concomitant cervical dilation and curettage. A postvoid residual is also assessed to evaluate for urinary retention. Patients then have subsequent visits at 6 weeks, 3 months, and 1 year, and as needed thereafter.
You will probably be able to return to your normal activities in about 4 weeks, but this can vary widely. Avoid strenuous activity for the first 2 weeks, and increase your activity level gradually.
Colpocleisis complications
Complications of colpocleisis surgery are uncommon. The main point of colpocleisis is speed and simplicity. Colpocleisis procedure is usually best for women who have chronic health conditions, because a more extensive or complicated surgery could be dangerous.
Clinicians should consider the frequent association of advanced pelvic organ prolapse with urinary retention and urinary incontinence 12. This evaluation is important because 13-65% of continent women who undergo surgical correction for prolapse are reported to experience stress incontinence postoperatively 6. Some have postulated that advance prolapse can cause kinking of the urethra leading to obstruction; therefore, anatomic correction may relieve such kinking, resulting in stress incontinence.
To investigate for incontinence or retention, a cough stress test or cystometry may be used. In the case of urinary retention, a simple postvoid residual test can be performed. If postvoid residual is less than 100 mL, then the patient does not have urinary retention. If postvoid residual is greater than 200 mL, the patient has retention and will likely benefit from prolapse surgery because 90% of women with elevated postvoid residual volumes experience resolution after prolapse correction 8. Additionally, multichannel urodynamic testing prior to surgery may prove helpful in unveiling voiding dysfunction or incontinence.
- Jones K, Wang G, Romano R, St Marie P, Harmanli O. Colpocleisis: A Survey of Current Practice Patterns. Female Pelvic Med Reconstr Surg. 2017;23(4):276–280. doi:10.1097/SPV.0000000000000372 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6488017[↩]
- Kuncharapu, I., Majeroni, B. A., & Johnson, D. W. (2010). Pelvic organ prolapse. American Family Physician, 81, 1111-1117.[↩]
- Zebede A, Smith AL, Plowright LN, et al. Obliterative LeFort colpocleisis in a large group of elderly women. Obstet Gynecol 2013; 121(2 pt 1):279–284.[↩]
- Mueller MG, Ellimootil C, Abernethy MG, et al. Colpocleisis: a safe, minimally invasive option for pelvic organ prolapse. Female Pelvic Med Reconstr Surg 2015;21(1):30–33[↩]
- Colpocleisis. https://emedicine.medscape.com/article/2047195-overview[↩]
- Kenton K, Brubaker L, Falk S. Pelvic organ prolapse in women: Surgical repair of the apical prolapse (uterine or vaginal vault prolapse). UpToDate 2011.[↩][↩]
- FitzGerald MP, Richter HE, Siddique S, Thompson P, Zyczynski H. Colpocleisis: a review. Int Urogynecol J Pelvic Floor Dysfunct. 2006 May. 17(3):261-71.[↩]
- Neimark M, Davila GW, Kopka S. LeFort Colpocleisis. J Pelvic Med Surg 2003; 9:83[↩][↩]
- Fitzgerald MP, Richter HE, Siddique S, et al. Colpocleisis: a review. Int Urogynecol J Pelvic Floor Dysfunct 2006;17(3):261–271[↩]
- Partial colpocleisis. Am J Obstet Gynecol. 1986 Jun;154(6):1200-5. https://www.ajog.org/article/0002-9378(86)90699-X/pdf[↩]
- Song X, Zhu L, Ding J, Xu T, Lang J. Long-term follow-up after LeFort colpocleisis: patient satisfaction, regret rate, and pelvic symptoms. Menopause. 2016 Jun. 23 (6):621-5.[↩]
- Hullfish KL, Bovbjerg VE, Steers WD. Colpocleisis for pelvic organ prolapse: patient goals, quality of life, and satisfaction. Obstet Gynecol. 2007 Aug. 110(2 Pt 1):341-5.[↩][↩][↩]
- Abbasy S, Kenton K. Obliterative procedures for pelvic organ prolapse. Clin Obstet Gynecol. 2010 Mar. 53(1):86-98.[↩][↩]
- Murphy M, Sternschuss G, Haff R, van Raalte H, Saltz S, Lucente V. Quality of life and surgical satisfaction after vaginal reconstructive vs obliterative surgery for the treatment of advanced pelvic organ prolapse. Am J Obstet Gynecol. 2008 May. 198(5):573.e1-7.[↩]
- Crisp CC, Book NM, Smith AL, Cunkelman JA, Mishan V, Treszezamsky AD, et al. Body image, regret, and satisfaction following colpocleisis. Am J Obstet Gynecol. 2013 Nov. 209(5):473.e1-7.[↩][↩]
- Zebede, Salomon MD; Smith, Aimee L. MD; Plowright, Leon N. MD; Hegde, Aparna MD; Aguilar, Vivian C. MD; Davila, et al. Obliterative LeFort Colpocleisis in a Large Group of Elderly Women. Obstet Gynecol. Feb 2013. 121:279-284.[↩]
- Moore RD, Miklos JR. Colpocleisis and tension-free vaginal tape sling for severe uterine and vaginal prolapse and stress urinary incontinence under local anesthesia. J Am Assoc Gynecol Laparosc. 2003 May. 10(2):276-80[↩]
- FitzGerald MP, Brubaker L. Colpocleisis and urinary incontinence. Am J Obstet Gynecol. 2003 Nov. 189(5):1241-4.[↩]
- Abbasy S, Lowenstein L, Pham T, Mueller ER, Kenton K, Brubaker L. Urinary retention is uncommon after colpocleisis with concomitant mid-urethral sling. Int Urogynecol J Pelvic Floor Dysfunct. 2009 Feb. 20(2):213-6.[↩]
- Moore RD, Miklos JR. Colpocleisis and tension-free vaginal tape sling for severe uterine and vaginal prolapse and stress urinary incontinence under local anesthesia. J Am Assoc Gynecol Laparosc. 2003 May. 10(2):276-80.[↩]





{kind=link}