Contents
What is a corneal ulcer
A corneal ulcer is an open sore on the cornea. An ‘ulcer’ is a shallow crater, a bit like a crater on the surface of the moon. The ulcer forms as part of your body’s reaction to a mild bacterial infection. Some bacteria are trapped in the eyelids, and some are naturally present on the surface of your eyes. The bacteria may invade the surface of the cornea, and your body’s immune system reacts to the bacteria to make the ulcer. When your body ‘overreacts’ an ulcer forms. A corneal ulcer is often caused by an infection, but severe dry eye or other eye disorders can cause it too. Corneal ulcers are characterized by corneal epithelial defects with underlying inflammation, and soon necrosis of the corneal stroma develops. Corneal ulcers tend to heal with scar tissue, resulting in opacification of the cornea and decreased visual acuity. Uveitis, corneal perforation with iris prolapse, pus in the anterior chamber (hypopyon), panophthalmitis, and destruction of the eye may occur without treatment and, on occasion, even with the best available treatment, particularly if treatment is delayed. More severe symptoms and complications tend to occur with deeper ulcers.
People at risk for corneal ulcers include:
- contact lens wearers
- people who have or have had cold sores, chicken pox or shingles
- people who use steroid eye drops
- people with dry eye
- people with eyelid disorders that prevent proper functioning of the eyelid
- people who injure or burn their cornea
If you wear contact lenses, safe handling, storage and cleaning of your lenses are key steps to reduce your risk of a corneal ulcer. It is important to learn how to take care of your contact lenses (see corneal ulcer prevention below).
Will a corneal ulcer heal itself?
No. A corneal ulcer is an open sore on the cornea and a corneal ulcer is often caused by an infection (bacteria, fungi, viruses, or Acanthamoeba) that requires proper treatment by your doctor or eye specialist (ophthalmologist). See your doctor or ophthalmologist immediately if you think you have a corneal ulcer or have any eye symptoms that concern you. Corneal ulcers can badly and permanently damage your vision and even cause blindness if they are not treated.
Corneal ulcers tend to heal with scar tissue, resulting in opacification of the cornea and decreased visual acuity. Uveitis, corneal perforation with iris prolapse, pus in the anterior chamber (hypopyon), panophthalmitis, and destruction of the eye may occur without treatment and, on occasion, even with the best available treatment, particularly if treatment is delayed. More severe symptoms and complications tend to occur with deeper ulcers.
What is corneal ulcer healing time?
The healing time for corneal ulcers varies. Corneal ulcers caused by Acanthamoeba (also most commonly due to exposure to contaminated water while wearing contact lenses) and fungi (most commonly due to trauma with vegetable material) are slow to develop or heal but progressive, whereas those caused by Pseudomonas aeruginosa (seen most frequently in contact lens wearers) develop rapidly, causing deep and extensive corneal necrosis. Wearing contact lenses while sleeping or wearing inadequately disinfected contact lenses can cause corneal ulcers.
What is the cornea?
The cornea is the eye’s outermost layer. It is the clear, dome shaped surface that covers the front of the eye. The cornea plays an important role in focusing your vision.
What are the parts of the cornea?
Although the cornea may look clear and seem to lack substance, it is a highly organized tissue. Unlike most tissues in the body, the cornea contains no blood vessels to nourish or protect it against infection. Instead, the cornea receives its nourishment from tears and the aqueous humor (a fluid in the front part of the eye that lies behind the cornea).
The tissues of the cornea are arranged in three basic layers, with two thinner layers, or membranes, between them. Each of these five layers has an important function. These layers are (Figure 2):
Epithelium
The epithelium is the cornea’s outermost layer. Its primary functions are to:
- block the passage into the eye of foreign material, such as dust, water, and bacteria; and
- provide a smooth surface to absorb oxygen and nutrients from tears, which are then distributed to the other layers of the cornea.
The epithelium is filled with thousands of tiny nerve endings, which is why your eye may hurt when it is rubbed or scratched. The part of the epithelium that epithelial cells anchor and organize themselves to is called the basement membrane.
Bowman’s membrane
The next layer behind the basement membrane of the epithelium is a transparent film of tissue called Bowman’s layer, composed of protein fibers called collagen. If injured, Bowman’s layer can form a scar as it heals. If these scars are large and centrally located, they may cause vision loss.
Stroma
Behind Bowman’s layer is the stroma, which is the thickest layer of the cornea. It is composed primarily of water and collagen. Collagen gives the cornea its strength, elasticity, and form. The unique shape, arrangement, and spacing of collagen proteins are essential in producing the cornea’s light-conducting transparency.
Descemet’s Membrane
Behind the stroma is Descemet’s membrane, a thin but strong film of tissue that serves as a protective barrier against infection and injuries. Descemet’s membrane is composed of collagen fibers that are different from those of the stroma, and are made by cells in the endothelial layer of the cornea (see above). Descemet’s membrane repairs itself easily after injury.
Endothelium
The endothelium is the thin, innermost layer of the cornea. Endothelial cells are important in keeping the cornea clear. Normally, fluid leaks slowly from inside the eye into the stroma. The endothelium’s primary task is to pump this excess fluid out of the stroma. Without this pumping action, the stroma would swell with water and become thick and opaque.
In a healthy eye, a perfect balance is maintained between the fluid moving into the cornea and the fluid pumping out of the cornea. Unlike the cells in Descemet’s membrane, endothelial cells that have been destroyed by disease or trauma are not repaired or replaced by the body.
What does the cornea do?
The cornea acts as a barrier against dirt, germs, and other particles that can harm the eye. The cornea shares this protective task with the eyelids and eye sockets, tears, and the sclera (white part of the eye). The cornea also plays a key role in vision by helping focus the light that comes into the eye. The cornea is responsible for 65-75 percent of the eye’s total focusing power.
The cornea and lens of the eye are built to focus light on the retina, which is the light-sensitive tissue at the back of the eye. When light strikes the cornea, it bends—or refracts—the incoming light onto the lens. The lens refocuses that light onto the retina, which starts the translation of light into vision. The retina converts light into electrical impulses that travel through the optic nerve to the brain, which interprets them as images.
The refractive process the eye uses is similar to the way a camera takes a picture. The cornea and lens in the eye act as the camera lens. The retina is like the film (in older cameras), or the image sensor (in digital cameras). If the image is not focused properly, the retina makes a blurry image.
The cornea also serves as a filter that screens out damaging ultraviolet (UV) light from the sun. Without this protection, the lens and the retina would be exposed to injury from UV rays.
Figure 1. Eye anatomy
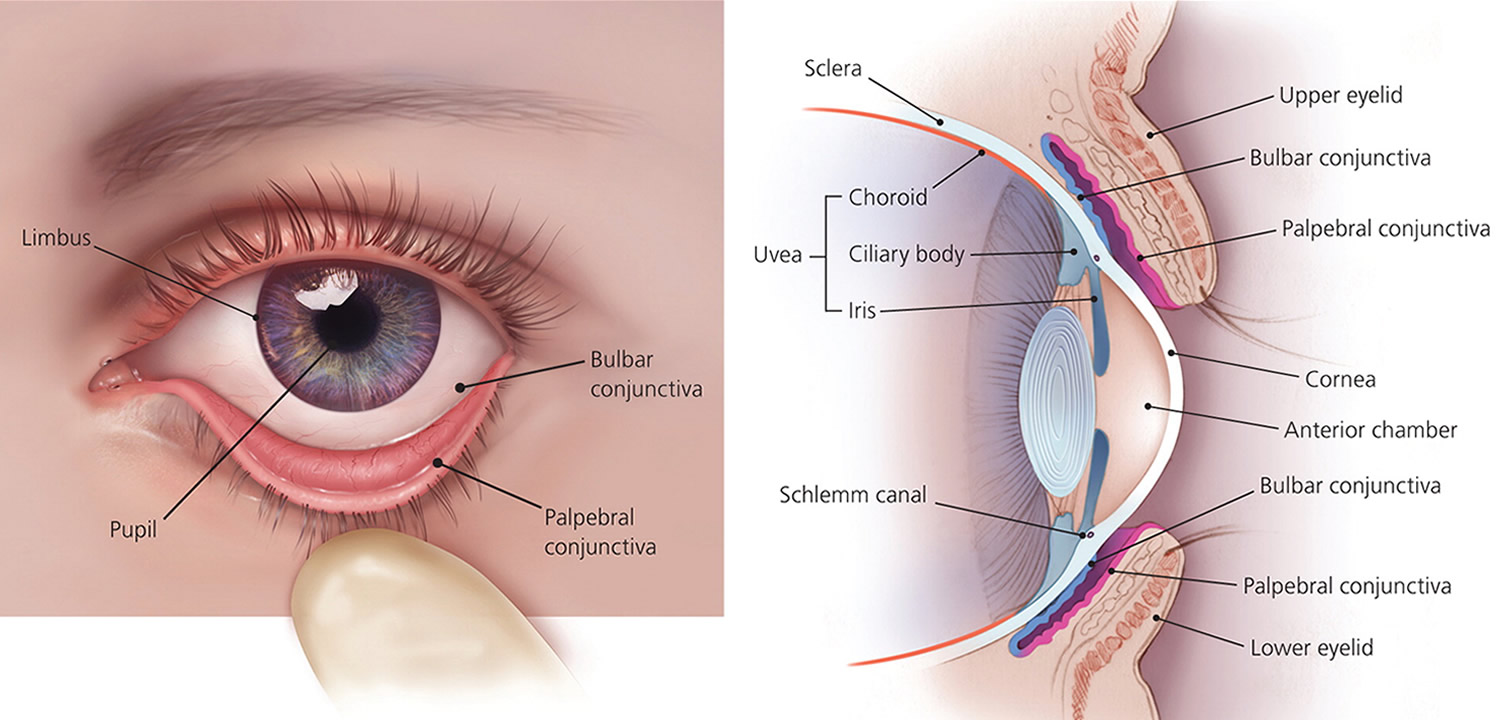 Figure 2. Structures of the cornea
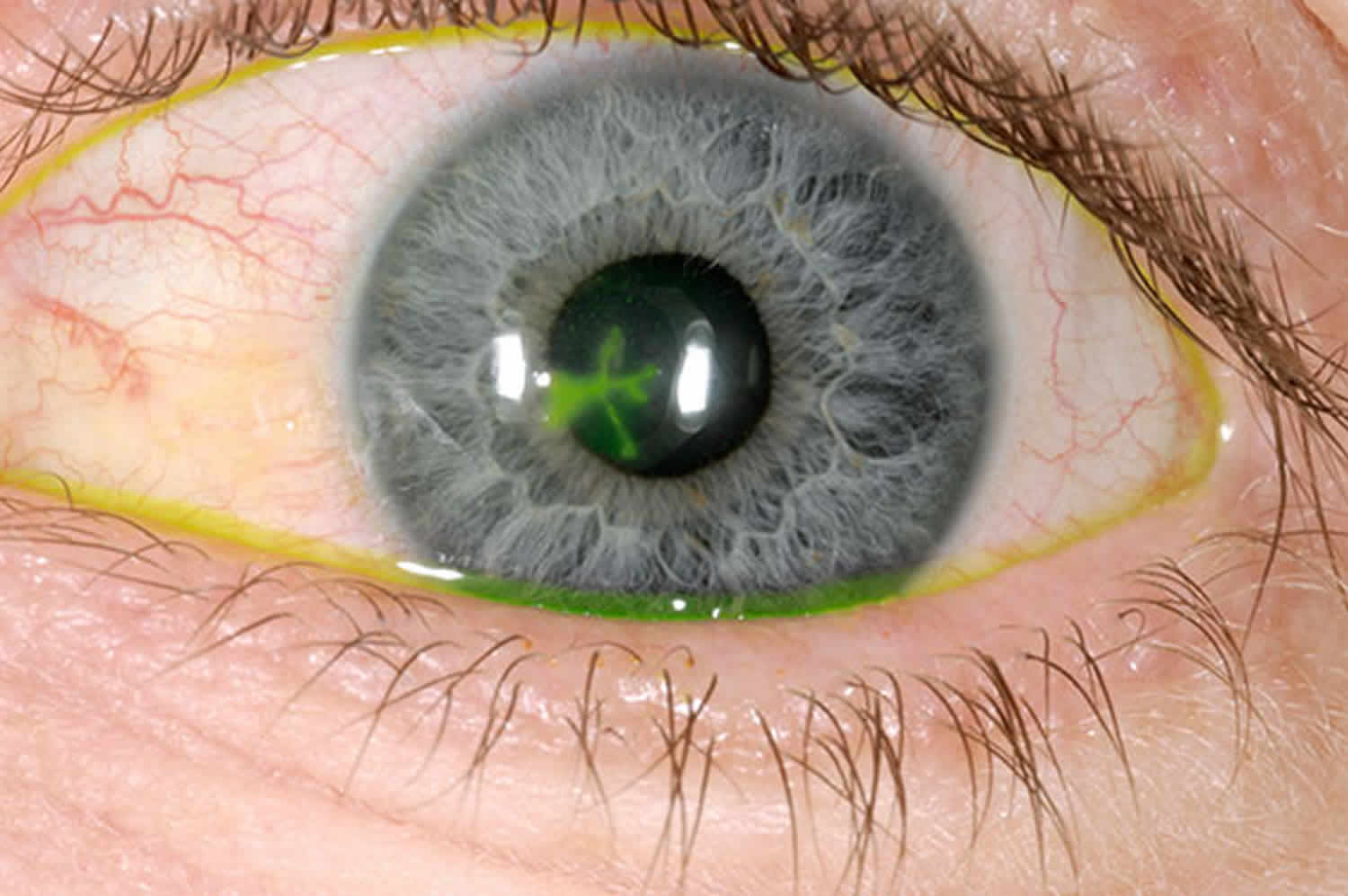
Figure 2. Structures of the cornea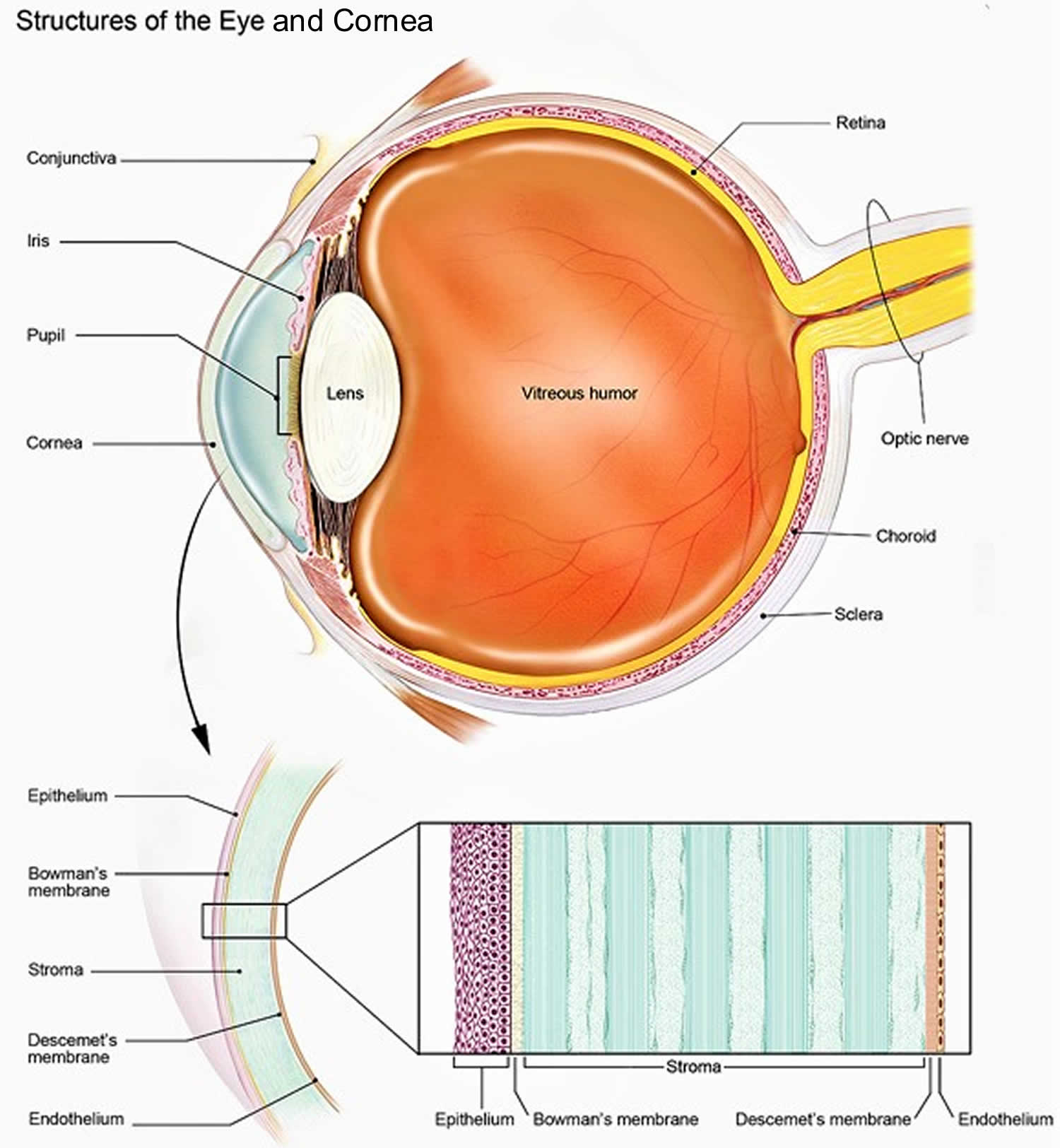 Figure 3. Corneal ulcer
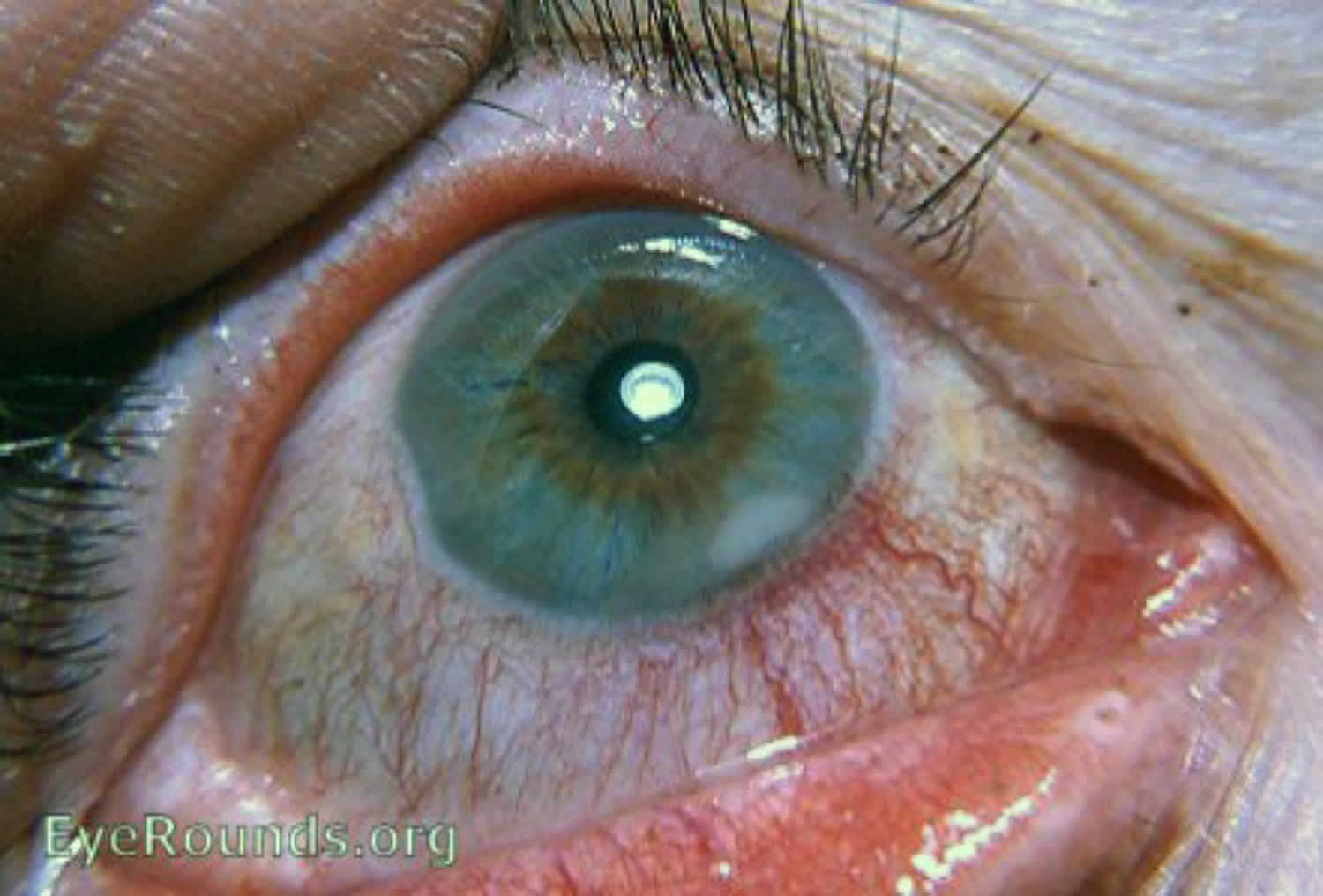
Figure 3. Corneal ulcer

What is marginal corneal ulcer
Marginal corneal ulcers can be infectious or non-infectious and infectious ulcers are usually caused by bacteria. Marginal corneal ulcer is characterized by the appearance of small, gray-white circumlimbal lesions. These infiltrative lesions are separated from the limbus by about 1 mm of clear cornea and they may have overlying epithelial defects. The non-infectious marginal keratitis is an immune system response to corneal damage.
Sterile marginal infiltrates
The process begins when antigen is introduced to the corneal surface and inflammatory mediators are released to the corneal periphery. Corneal infiltrates are usually oval in shape. Most lesions are found in the 4 or 5 o’clock position and the 7 or 8 o’clock position in the peripheral cornea 1.
Marginal corneal ulcer presence could be related to any of the following:
- Contact lens wear
- Bacterial by-products from untreated blepharitis (e.g., longstanding staphylococcal blepharitis)
- Autoimmune disease
- Other toxic stimuli
Structural damage to the eye:
- Localized vasodilation at the limbus secondary to the release of pro-inflammatory cytokines from the cornea
- White blood cells (neutrophils) are recruited into the cornea from the dilated limbal blood vessels
- Marginal infiltrates form from the collection of white blood cells
- The neutrophils release proteases that damage the corneal epithelium
- The resulting micro-ulcer produces overlying corneal staining with vital dyes
- A healed marginal ulcer may leave a scar in the corneal stroma
In one study of 200 cases of ulcers at the margin of the cornea, 180 cases represented simple catarrhal ulcers and infiltrates 2. Catarrhal is simply referring to mucous membranes in nature, and its use in this instance is related to the cause of the marginal corneal ulcer, i.e. the inflammatory response and lack of direct bacterial infection 3. One hundred and fifty-six of these cases were associated with chronic catarrhal conjunctivitis and 133 were associated with coagulase positive staphylococci isolated from the conjunctiva or lid margins. Additionally, concurrent blepharitis was an almost constant feature with these infiltrates and ulcerations 4. There are case reports of patients presenting with both folliculitis and marginal keratitis, indicating that these may be associated systemic conditions. The authors 5 of one case report speculate that there could be a common underlying process, namely an abnormal inflammatory response to bacterial stimuli, with staphylococcal aureus being the prime example of antigenic presentation.
Marginal corneal ulcer treatment
- Topical corticosteroids are recommended as the treatment of choice; a weak topical steroid should be instilled at least 4 times a day for 1-2 weeks 6.
- Addition of a topical antibiotic can be considered especially in cases where there is epithelial breakdown 7.
- Treatment should also include usual blepharitis treatment in order to reduce bacterial antigens and reduce the recurrence of marginal keratitis and ulceration 8.
- Eyelid hygiene
- Warm compresses
- Topical Antibiotics
- Oral Macrolide or Tetracyline antibiotic
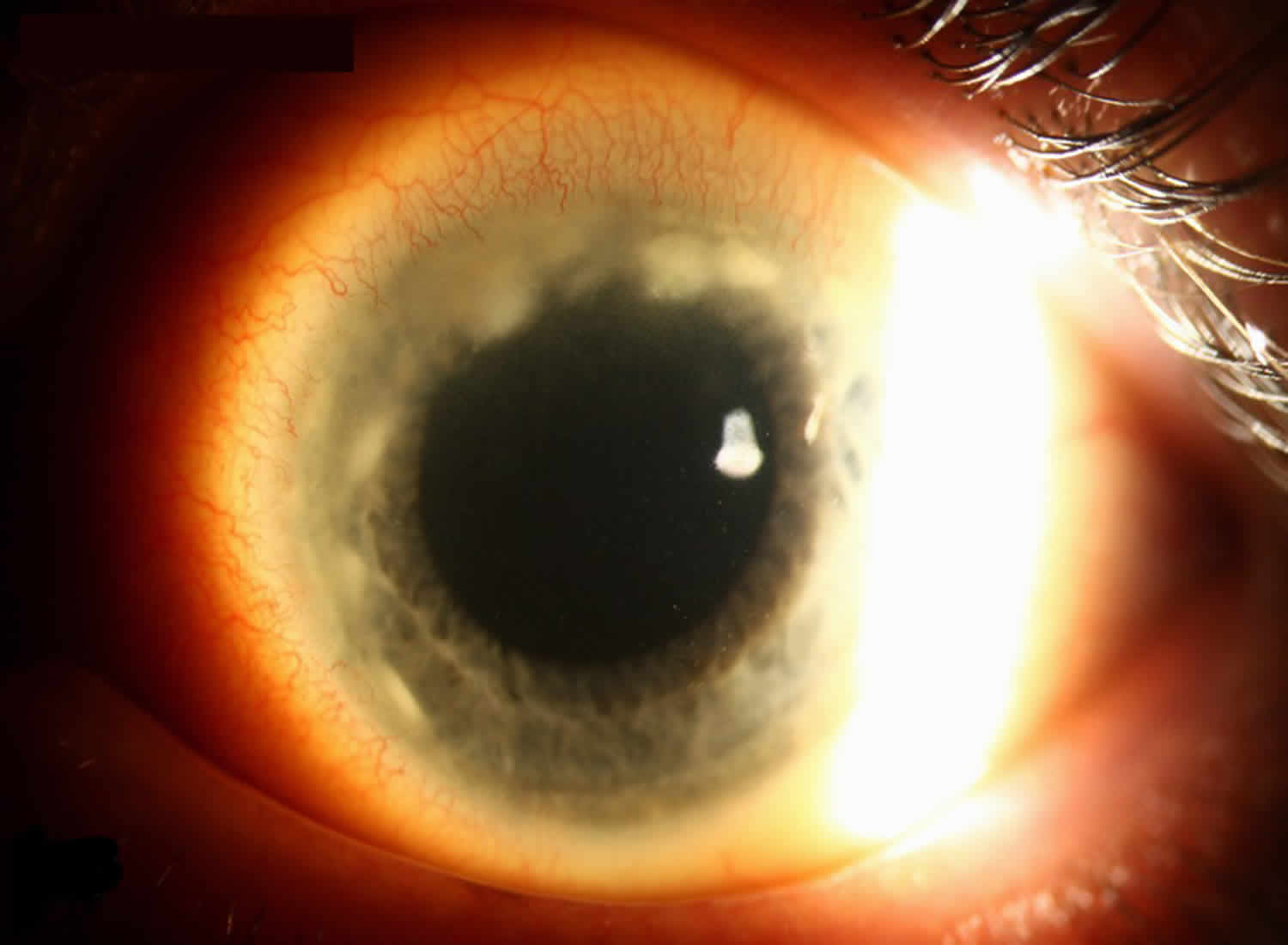
Figure 4. Marginal corneal ulcer
Marginal corneal ulcer causes
Staph aureus is thought to be the primary inciting agent and is commonly present in the lid margins of eyes affected by marginal corneal ulcers. In one study of marginal corneal ulcers, Staphylococcus aureus was isolated from 29% of either lids or conjunctiva of those patients with corneal ulcers compared to 11% of controls 9. In this same study, actual ulcer scrapings showed only degenerate epithelial cells, absence of cellular infiltration, and no organisms, suggesting a sterile ulcer 9. In another study of 180 marginal ulcers, 133 had either conjunctival, lid, or ulcer scrapings with evidence of coagulase positive Staphylococcus aureus 7. It has been theorized that marginal keratitis and ulceration are the result of enhanced cell mediated immunity (delayed type hypersensitivity) at the limbus to cell wall antigens and exotoxins of Staphylococcus aureus from the eyelids 8. The peripheral cornea is susceptible to immunologic reactions because of its proximity to limbal vasculature and conjunctival lymphoid tissue 8. Antigen-antibody complexes are thought to be deposited in the peripheral cornea; antigen provided from the eyelids and tear film and antibody provided from limbal blood vessels 6. One study immunized rabbits against Staphylococcus aureus and then applied viable Staphylococcus aureus topically to the rabbits’ eyes. Of 26 rabbit eyes, 8 developed elevated nodular lesions of the cornea and 8 developed peripheral corneal infiltrates running parallel to the limbus and separated from it by a lucid interval 10. After cessation of topical S. aureus, corneal infiltrates gradually resolved during the next 2-3 weeks. Gram stains were taken of corneal lesions in this study and showed no gram positive cocci, supporting the pathophysiology of a sterile inflammatory response rather than direct infection by Staphylococcus aureus 10. The group of immunized rabbits was compared to rabbits who were not immunized but still had S. Aureus topically applied to the eye. The unimmunized rabbits developed conjunctival hyperemia but did not develop corneal infiltrates, suggesting that an enhanced cell mediated immune response was responsible for development of infiltrates 10. There are also human studies that examined the theory of hypersensitivity as well. In one such study, skin testing for delayed hypersensitivity to Staphylococcus aureus was performed on all subjects. The authors explained that the cell wall of Staphylococcus aureus contains protein A, which specifically binds to the Fc receptor of an antibody molecule and forms immune complexes. These immune complexes act as antigen to produce a delayed hypersensitivity response 11. The study found that 8/11 subjects with blepharitis and history of marginal keratitis were in the group that demonstrated enhanced delayed hypersensitivity reaction to the protein injected in the skin test, further supporting the theory that delayed hypersensitivity contributes to the pathogenesis of this disease 11.
Marginal corneal ulcer signs and symptoms
Patients often present with symptoms of pain, photophobia, and foreign body sensation 9. The slit lamp exam most commonly shows peripheral curvilinear infiltrates in the superficial cornea (subepithelial/anterior stroma) at 10, 2, 4, or 8’oclock, where the eyelids cross the corneal periphery (Figure 5). Ulcerations are located in the marginal zone and separated from the limbus by a clear corneal zone. Flourescein staining often shows epithelial defects that are smaller than the infiltrate area 6. One study looked at 84 patients with marginal ulcers and described the appearance as single or multiple infiltrates, which subsequently coalesced with overlying epithelial breakdown of the corneal epithelium. Again, in all cases, the ulceration was separated from the limbus by clear cornea 9. These ulcers are also characterized by circumferential progression of associated marginal infiltrates, which was seen in our patient 7. In one study, the cases of marginal ulcers associated with chronic staphylococcal conjunctivitis also had a highly characteristic epithelial keratitis with puncate erosions on the lower half of cornea 4. Associated findings include dilated limbal vessels, conjunctival reaction, and occasionally lid erythema and edema with reactive ptosis 8. Often, there are signs of staphylococcal blepharitis, meibomitis, and acne rosacea. These signs include hard scales on the lashes, collarettes, dilated vessels on lid margins, poliosis, or madarosis 12.
Marginal corneal ulcer symptoms
- Pain
- Photophobia
- Foreign body sensation
- Eye redness
- Blurry vision
Signs of marginal corneal ulcer
- Unilateral or bilateral peripheral curvilinear infiltrates in superficial cornea where lids cross the corneal periphery
- Loss of corneal epithelium; ulcerations in the marginal zone separated from the limbus by a clear corneal zone
- Circumferential progression of associated marginal infiltrates with associated limbal hyperemia and conjunctivitis
- Ulcers can be associated with keratitis, which presents with small flat punctate lesions in the cornea epithelium.
- Staphylococcal blepharitis, meibomitis, acne rosacea is often also present
Figure 5. Marginal keratitis
Footnote: The corneal infiltrates seen in these photograph are active as evident by the hyperemia adjacent to the corresponding limbal area and the slit-lamp findings of an active keratitis.
[Source 13 ]Marginal corneal ulcer treatment
The treatment of corneal marginal ulcer focuses on addressing the two main components of the disease; the sterile corneal inflammatory reaction and the bacterial overgrowth on the eyelids. With regards to the corneal inflammatory disease, topical corticosteroids are recommended as the first-line treatment of choice 13. A weak topical steroid should be instilled at least 4 times a day for 1-2 weeks 6. Low dose prednisolone (0.12%) or a stronger concentration (1%) can be used, with the former being primarily anti-inflammatory and the latter with possible immunosuppressive effects as well 14. Some sources recommend the addition of a topical antibiotic for prophylactic and/or therapeutic benefit, especially in cases where there is epithelial breakdown 7. If there is any question about the cause of the infiltrate/ulcer, treatment should be initiated with antibiotic alone or in combination with steroid 8. A study comparing prednisolone drops, neomycin, and no treatment showed that the prednisolone treatment was significantly more effective than no treatment, but there was no significant difference between no treatment and neomycin 9. This further supports the theory that the lesions are a sterile inflammatory response that responds well to local anti-inflammatory therapy 13.
It is also important to reduce the antigenic burden by treating the bacterial lid disease. This treatment involves the usual blepharitis regimen, which commonly includes warm compresses and improved lid hygiene with frequent eyelid scrubs 8. Topical and/or systemic antibiotics are often added in acute presentation, with the oral antibiotic usually being a macrolide or a tetracycline 7. Tetracyclines have been shown to decrease the lipolytic activity of staphylococcus organisms, which is presumed to be one of the ways the bacteria alters meibomian gland secretions and causes chronic inflammation 15. Long-term blepharitis treatment has been shown to be effective in reducing the recurrence of marginal keratitis and ulceration 8. One study showed pure staphylococcal marginal ulcers usually responded promptly to treatment of the associated conjunctivitis and blepharitis 4. Regardless of the specific regimen a patient is placed on, prompt therapy addressing both the keratitis and blepharitis components will lead to a swift recovery, and steroids should be used once infectious sources have been ruled out.
Corneal ulcer causes
A corneal ulcer usually occurs after corneal trauma or with an irregular ocular surface, which allows bacteria, fungus, or parasites to enter the cornea and cause an infection with inflammation.
Corneal ulcers are most commonly caused by an infection with bacteria, viruses, fungi, or a parasite.
Corneal ulcers are usually caused by the following types of infections:
- Bacterial infections. These are common in contact lens wearers, especially in people using extended-wear lenses.
- Viral infections. The virus that causes cold sores (the herpes simplex virus [HSV]) may cause recurring attacks. Herpes simplex keratitis is a serious viral infection. It may cause repeated attacks that are triggered by stress, exposure to sunlight, or any condition that lowers the immune response. Also, the virus that causes chicken pox and shingles (the varicella virus) can cause corneal ulcers.
- Fungal infections. Improper use of contact lenses or steroid eye drops can lead to fungal infections, which in turn can cause corneal ulcers. Also, a corneal injury that results in plant material getting into the eye can lead to fungal keratitis. Fungal keratitis may also occur in people with a suppressed immune system.
- Parasitic (Acanthamoeba) infections. Acanthamoeba are microscopic, single-celled amoeba that can cause human infection. They are the most common amoebae in fresh water and soil. When Acanthamoeba enters the eye it can cause a bad infection, particularly for contact lens users. Acanthamoeba keratitis occurs in contact lens users. It is more likely to happen in people who make their own homemade cleaning solutions.
Corneal ulcers or infections may also be caused by:
- Abrasions or burns to the cornea caused by injury to the eye. Cornea scratches, scrapes and cuts can become infected by bacteria and lead to corneal ulcers. These injuries can happen from fingernail scratches, paper cuts, makeup brushes and tree branches. Burns caused by corrosive chemicals found in the workplace and at home can cause corneal ulcers.
- Contact lenses (most commonly when worn during sleep and/or inadequately disinfected). Wearing contact lenses, such as soft contacts that are left in overnight, may cause a corneal ulcer.
- Dry eye syndrome.
- Dry eyes, primary
- Dry eyes, secondary (e.g.,, neurotrophic keratitis)
- Bell’s palsy and other eyelid abnormalities that prevent proper eyelid function. If the eyelid does not close all the way, such as with Bell palsy, the cornea can dry out, and an ulcer can develop.
- Chronic blepharitis
- Entropion
- Incomplete eye closure (eg, due to inadequate eye closure [lagophthalmos], peripheral facial nerve palsy, eyelid defects after trauma, or exophthalmos)
- Trichiasis
- Foreign bodies in the eye
- Severe allergic eye disease
- Various inflammatory disorders
- Nontraumatic corneal abnormalities:
- Bullous keratopathy (ie, ruptured bullae)
- Mucous membrane pemphigoid (causing trichiasis and persistent corneal epithelial defects because of corneal epithelial stem cell failure)
- Herpes simplex keratitis with secondary bacterial superinfection
- Trachoma (with secondary trichiasis)
- Nutritional deficiencies:
- Protein undernutrition
- Vitamin A deficiency
Risk factors for corneal ulcer
Trauma from a foreign body (including contact lenses), severe dry eyes, or eyelid disease can predispose patients to corneal infections. Contact lens overuse or poor contact lens hygiene also puts a patient at higher risk for such infections due to the bacteria and other organisms that can grow on the contact lenses, cases, and in re-used contact lens solution.
Corneal ulcer prevention
Things you can do to prevent corneal ulcer include:
- Wash your hands well when handling your contact lenses.
- Avoid wearing contact lenses overnight. Also, it is important to care for your contact lenses correctly.
- Get prompt treatment for an eye infection to prevent ulcers from forming.
- Use the correct protective eyewear when doing any work or play that can lead to eye injury.
How to take care of contact lenses
Millions of people choose to wear contact lenses. However, contact lenses are not for everyone. You might not be able to wear contact lenses for the following reasons:
- You get a lot of eye infections.
- You have severe allergies or dry eyes that are hard to treat.
- You work or live where it is very dusty.
- You are not able to properly care for your contact lenses.
Your cornea and tear film must be healthy for you to be comfortable and see clearly with contact lenses.
To safely wear contact lenses, you must be committed to caring for them properly and replacing them when needed. Talk with your ophthalmologist or other eye care professional to discuss your vision needs and expectations. They can help you decide if contacts are a good option for you.
Contact lenses that are old or that do not fit well can scratch your eye. They can also cause blood vessels to grow into your cornea, a dangerous condition that threatens your vision.
Eye drops can cause problems with your contact lenses. It is best to avoid using any kind of eye drop when wearing contacts. However, you can use wetting drops as recommended by your eye doctor.
Remove your contact lenses and call your eye doctor right away if your eyes are very red, painful, watery or sensitive to light. Do the same if you have blurry vision or notice discharge (ooze or pus) coming from your eye. These can be symptoms of serious eye problems.
Take proper care of your contact lens
You must clean and disinfect any contact lens you remove from your eye before you put the lens back in. There are many types of cleansing systems. The choice depends on the type of lens you use, if you have allergies or if your eyes tend to form protein deposits. Ask your eye doctor what kind of cleaning solutions you should use.
Take special care to clean and store your lenses correctly to avoid dangerous eye infections.
Here is what you should do:
- Follow the schedule your eye doctor gives you for wearing and replacing your lenses. You should not wear daily wear lenses while you sleep.
- Remove contact lenses before taking a shower, using a hot tub, swimming, or doing anything where water gets in your eyes.
- Before touching your contact lenses, wash your hands with soap and water and dry them with a lint-free towel.
- Never put contacts in your mouth to wet them. Saliva (spit) is not a sterile solution.
- Do not rinse or store contacts in water (tap or sterile water). Also, never use a homemade saline solution.
- Do not use saline solution or rewetting drops to disinfect your lenses. They are not disinfectants.
- Follow directions from your doctor and from the lens cleaning solution manufacturer to clean and store your lenses.
- No matter what type of lens cleaning solution you buy, use a “rub and rinse” cleaning method. Rub your contact lenses with clean fingers, then rinse the lenses with solution before soaking them. Use this method even if the solution you are using is a “no-rub” type.
- Use new solution each time you clean and disinfect your contact lenses. Never reuse or “top off” with old solution. Also, do not pour contact lens solution into a different bottle. The solution will no longer be sterile.
- Make sure the tip of the solution bottle does not touch any surface. Keep the bottle tightly closed when you are not using it.
- Rinse your contact lens case with sterile contact lens solution (not tap water). Then leave the empty case open to air dry.
- Keep your contact lens case clean. Replace the case at least every 3 months, or right away if it gets cracked or damaged.
- If you store your lenses in the case for a long time, check the contact lens instructions or the lens solution directions to see if you should re-disinfect them before wearing them. Never wear your contact lenses if they have been stored for 30 days or longer without re-disinfecting.
- Contact lenses can warp over time, and your cornea can change shape. To make sure your lenses fit properly and the prescription is right for you, see your eye doctor regularly.
Corneal ulcer symptoms
Symptoms of infection or corneal ulcers include:
- Blurry or hazy vision
- Eye that appears red or bloodshot
- Itching and discharge
- Sensitivity to light (photophobia)
- Very painful and watery eyes
- White patch on the cornea that you may or may not be able to see when looking in the mirror
- The feeling of having something in your eye
- Pus or other discharge
- Swelling of the eyelids
- Tearing
See your ophthalmologist immediately if you think you have a corneal ulcer or have any eye symptoms that concern you. Corneal ulcers can badly and permanently damage your vision and even cause blindness if they are not treated.
Corneal ulcer possible complications
Untreated corneal ulcers and infections may lead to:
- Loss of the eye (rare)
- Severe vision loss
- Scars on the cornea
Corneal ulcer prognosis
Many people recover completely and have only a minor change in vision. However, a corneal ulcer or infection can cause long-term damage and affect vision.
Corneal ulcer diagnosis
Your ophthalmologist will use a special dye called fluorescein to light up any damage to your cornea. They will then examine your cornea using a special microscope called a slit lamp. The slit-lamp exam will allow your ophthalmologist to see the damage to your cornea and determine if you have a corneal ulcer.
If your ophthalmologist thinks that an infection has caused your corneal ulcer, they may take a tiny tissue sample. Examination of this sample helps identify and properly treat the infection.
Your ophthalmologist will do the following tests:
- Exam of scrapings from the ulcer
- Fluorescein stain of the cornea
- Keratometry (measuring the curve of the cornea)
- Pupillary reflex response
- Refraction test
- Slit-lamp examination
- Tests for dry eye
- Visual acuity
Blood tests to check for inflammatory disorders may also be needed.
Corneal ulcer treatment
Treatment for corneal ulcers and infections depends on the cause. Treatment should be started as soon as possible to prevent scarring of the cornea. Antibiotic, antifungal or antiviral eye drops are the treatments of choice. Sometimes your ophthalmologist will prescribe antifungal tablets. In other cases, they will treat you with an injection of medication near the eye.
If the exact cause is not known, you may be given antibiotic drops that work against many kinds of bacteria. Treatment usually involves frequent (e.g., every 1 to 2 hours around the clock) application of topical antimicrobials.
Once the exact cause is known, you may be given drops that treat bacteria, herpes, other viruses, or a fungus. In the case of suspected fungal or parasitic infection, a patient may receive special antibiotics specifically targeted at these organisms.
Your ophthalmologist may prescribe steroid or anti-inflammatory eye drops after your infection has improved or is gone. Corticosteroid eye drops should reduce swelling and help prevent scarring. Steroid eye drop use is controversial for corneal ulcer. You should only use them under close supervision by your ophthalmologist. It is possible that steroid eye drops may worsen an infection.
Your ophthalmologist may prescribe pain medication to take by mouth to reduce pain.
If your symptoms suddenly change or get worse during treatment, then let your ophthalmologist know right away.
Symptoms to look for include:
- pain and redness of the eye
- tearing and discharge from the eye
- blurry vision
After the infection is resolved, residual corneal scarring or thinning can occur, and occasionally corneal transplantation may be recommended to restore vision. Early treatment may help reduce the risk of complications. Frequent visits to an eye care professional may be necessary for several months to eliminate the problem.
Your doctor may also recommend that you:
- Avoid eye makeup
- DO NOT wear contact lenses at all, or do not wear them at night
- Take pain medicines
- Wear protective glasses
Corneal ulcer treatment guidelines
Treatment for corneal ulcers and infections depends on the cause. Treatment should be started as soon as possible to prevent scarring of the cornea.
If the exact cause is not known, you may be given antibiotic drops that work against many kinds of bacteria. Treatment usually involves frequent (e.g., every 1 to 2 hours around the clock) application of topical antimicrobials.
Treatment for corneal ulcers, regardless of cause, begins with moxifloxacin 0.5% or gatifloxacin 0.3 to 0.5% for small ulcers and fortified (higher than stock concentration) antibiotic drops, such as tobramycin 15 mg/mL and cefazolin 50 mg/mL, for more significant ulcers, particularly those that are near the center of the cornea. Frequent dosing (eg, q 15 min for 4 doses, followed by q 1 h around the clock) is necessary initially. Patching is contraindicated because it creates a stagnant, warm environment that favors bacterial growth and prevents the administration of topical drugs.
Herpes simplex is treated with trifluridine 1% drops q 2 h while the patient is awake to a total of 9 times/day, ganciclovir 0.15% gel 5 times/day, valacyclovir 1000 mg po bid, or acyclovir 400 mg po 5 times/day (or tid for recurrent herpes simplex keratitis) for about 14 days.
Fungal infections are treated with topical antifungal drops [eg, natamycin 5%, amphotericin B 0.15%, and sometimes voriconazole 1% (which is less effective)], initially q 1 h during the day and q 2 h overnight. Deep infections may require addition of oral voriconazole 400 mg bid for 2 doses then 200 mg bid, ketoconazole 400 mg once/day, fluconazole 400 mg once then 200 mg once/day, or itraconazole 400 mg once then 200 mg once/day.
If Acanthamoeba is identified, therapy can include topical propamidine 0.1%, neomycin 0.175%, and polyhexamethylene biguanide 0.02% or chlorhexidine 0.02% supplemented with miconazole 1%, clotrimazole 1%, or oral ketoconazole 400 mg once/day or itraconazole 400 mg once then 200 mg once/day. The drops are used q 1 to 2 h until clinical improvement is evident, then gradually reduced to 4 times/day and continued for a number of months until all inflammation has resolved. Polyhexamethylene biguanide and chlorhexidine are not commercially available as ocular agents but can be prepared by a compounding pharmacy.
For all ulcers, treatment may also include a cycloplegic, such as atropine 1% or scopolamine 0.25% 1 drop tid, to decrease the ache of a corneal ulcer and to reduce the formation of posterior synechiae. In severe cases, debridement of the infected epithelium or even penetrating keratoplasty may be required. Patients who are poorly compliant or who have large, central, or refractory ulcers may need to be hospitalized. Very selective patients can be treated adjunctively with a corticosteroid drop (eg, prednisolone acetate 1% qid for 1 wk then tapered over 2 to 3 wk). The final appearance of the scar and final visual acuity are not improved with topical corticosteroids. Topical corticosteroids do decrease the pain and photophobia, and speed the increase in visual acuity, significantly. Because there is a very small risk of the ulcer worsening, adding topical corticosteroids is only indicated when a patient needs to get back to normal functioning (e.g., work, driving etc.) as soon as possible. Such treatment should only be prescribed by ophthalmologists and should be restricted to patients in whom clinical and microbiologic evidence indicates a favorable response to antimicrobial treatment and who can be closely followed.
Surgical treatment
A corneal transplant can replace your damaged cornea with a healthy donor cornea to restore vision. When the infection is gone and the ulcer is healed after treatment with medication, sometimes a significant scar remains. In this case, a transplant may be done to improve vision. And if corneal ulcers cannot be treated with medication, you may also need corneal transplant surgery to keep your vision.
Corneal ulcer treatment at home
There is NO corneal ulcer home treatment.
See your ophthalmologist immediately if you think you have a corneal ulcer or have any eye symptoms that concern you. Corneal ulcers can badly and permanently damage your vision and even cause blindness if they are not treated. Antibiotic, antifungal or antiviral eye drops are the treatments of choice. Sometimes your ophthalmologist will prescribe antifungal tablets. In other cases, they will treat you with an injection of medication near the eye.
Infectious keratitis (caused by bacteria, Acanthamoeba, herpes simplex virus (HSV), and herpes zoster ophthalmicus) necessitates ophthalmologic referral. Recurrent herpes simplex virus (HSV) keratitis increases risk of visual loss from corneal damage 16, and herpes zoster ophthalmicus can cause chronic ocular inflammation, vision loss, and disabling pain 17.
- Marginal Corneal Ulcer. https://decisionmakerplus.net/dg-post/h16-043-marginal-corneal-ulcer[↩]
- Thygeson P. Complications of staphylococcic blepharitis. Am J Ophthalmol 1969;68(3):446-449[↩]
- Corneal Marginal Ulcer: Marginal keratitis with ulceration in a 45 year-old male. https://webeye.ophth.uiowa.edu/eyeforum/cases/249-corneal-marginal-ulcer.htm[↩]
- Thygeson P. Marginal corneal infiltrates and ulcers. Trans Am Acad Ophthalmol Otolaryngol 1947;51:198-209.[↩][↩][↩]
- Sivakumaran S, Meyer P, Burrows NP. Dissecting folliculitis of the scalp with marginal keratitis. Clin Exp Dermatol 2001;26(6):490-492.[↩]
- Kanski JJ. Cornea. Signs in Ophthalmology: Causes and Differential Diagnosis: Elsevier; 2010; chapter 5; p. 101-140.[↩][↩][↩][↩]
- Boto-de-los-Bueis A, del Hierro Zarzuelo A, García Perea A, de Pablos M, Pastora N, Noval S. Staphylococcus aureus Blepharitis Associated with Multiple Corneal Stromal Microabscess, Stromal Edema, and Uveitis. Ocul Immunol Inflamm 2015;23(2):180-183.[↩][↩][↩][↩][↩]
- Kaufman SCaR, Allison E. Peripheral Corneal Disease. CORNEA, Fundamentals, Diagnosis, and Management: Elsevier; 2017; chapter 19; p. 232-240.[↩][↩][↩][↩][↩][↩][↩]
- Chignell AH, Easty DL, Chesterton JR, Thomsitt J. Marginal ulceration of the cornea. Br J Ophthalmol 1970;54(7):433-440.[↩][↩][↩][↩][↩]
- Mondino BJ, Kowalski R, Ratajczak HV, Petes J, Cutler SB, Bronw SI. Rabbit model of phlyctenulosis and catarrhal infiltrates. Arch Ophthalmol 1981;99(5):891-895.[↩][↩][↩]
- Ficker L, Seal D, Wright P. Staphylococcal infection and the limbus: study of the cell-mediated immune response. Eye (Lond) 1989;3 ( Pt 2):190-193.[↩][↩]
- Srinivasan M, Mascarenhas J, Prashanth CN. Distinguishing infective versus noninfective keratitis. Indian J Ophthalmol 2008;56(3):203-207.[↩]
- Stiff AH, Ricca AM, Goins KM. Corneal Marginal Ulcer: Marginal keratitis with ulceration in a 45 year-old male. EyeRounds.org. posted March 14, 2017; Available from: http://EyeRounds.org/cases/249-corneal-marginal-ulcer.htm[↩][↩][↩]
- Smolin G, Okumoto M. Staphylococcal blepharitis. Arch Ophthalmol 1977;95(5):812-816.[↩]
- Dougherty JM, McCulley JP, Silvany RE, Meyer DR. The role of tetracycline in chronic blepharitis. Inhibition of lipase production in staphylococci. Invest Ophthalmol Vis Sci 1991;32(11):2970-2975.[↩]
- Kaye S, Choudhary A. Herpes simplex keratitis. Prog Retin Eye Res. 2006;25(4):355–380.[↩]
- Catron T, Hern HG. Herpes zoster ophthalmicus. West J Emerg Med. 2008;9(3):174–176.[↩]





{kind=link}