COVID-19 vaccine
As of November 19, 2025, COVID-19 vaccination is recommended by the U.S. Centers for Disease Control and Prevention (CDC) for people ages 6 months and older based on individual-based decision-making or shared clinical decision-making 1. This includes people who have received a COVID-19 vaccine, people who have had COVID-19, and people with long COVID 1. COVID-19 also known as coronavirus disease 2019 is a disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) 2. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spreads mainly from person to person, even from someone who is infected but has no symptoms. When people with COVID-19 cough, sneeze, breathe, sing or talk, their breath may contain the COVID-19 virus. The coronavirus carried by the breath of a person with the infection can land directly on the face of a nearby person, after a sneeze or cough, for example. The droplets or particles could also be breathed in by other people if they are close together or in areas with low airflow.
The main risk factors for COVID-19 are 3:
- Living with someone who has COVID-19.
- Spending time in places with poor airflow and a higher number of people when COVID-19 virus is spreading.
- Spending more than 30 minutes in close contact with someone who has COVID-19.
Many factors affect your risk of catching the virus that causes COVID-19. How long you are in contact with the virus, whether the space has good airflow and the activities you’re doing in the space all affect the risk. Also, your risk may change based on whether you or others wear masks, whether someone has COVID-19 symptoms, and how close you are to others. Close contact includes sitting next to and talking to other people, for example, or sharing a car or bedroom.
It seems to be rare for people to catch the COVID-19 virus from an infected surface. While the virus is shed in waste, called stool, COVID-19 infection from places such as public bathrooms is not common.
COVID-19 most often causes respiratory symptoms that can feel much like a cold, the flu, or pneumonia. COVID-19 may attack more than your lungs and respiratory system. Other parts of your body may also be affected by the disease. Most people with COVID-19 have mild illness or no symptoms 3, 4. But for older adults and people with certain medical conditions and having a weakened or suppressed immune system, COVID-19 can lead to the need for care in the hospital or death 5, 6, 3.
COVID-19 vaccination is recommended for the prevention of COVID-19 disease and its complications as follows 7:
- Adults ages 65 years and older: COVID-19 vaccination is based on individual-based decision-making also known as shared clinical decision-making.
- People ages 6 months–64 years: COVID-19 vaccination is based on individual-based decision-making also known as shared clinical decision-making with an emphasis that the risk-benefit of vaccination is most favorable for individuals who are at an increased risk for severe COVID-19 disease and lowest for individuals who are not at an increased risk, according to the CDC list of COVID-19 risk factors below 8.
Evidence used to inform the list of underlying medical conditions that increase a person’s risk of severe illness from COVID-19 is presented in alphabetical order by study design section. Conditions are categorized as higher risk, suggestive higher risk, and mixed evidence 8.
Higher Risk
Higher risk is defined as an underlying medical condition or risk factor that has a published meta-analysis or systematic review or underwent the CDC systematic review process 8. The meta-analysis or systematic review demonstrates a conclusive increase in risk for at least one severe COVID-19 outcome in people with these medical conditions or risk factors 8:
- Asthma
- Blood cancers
- Cerebrovascular disease
- Chronic kidney disease (people receiving dialysis)
- Chronic lung diseases limited to:
- Bronchiectasis
- Chronic obstructive pulmonary disease (COPD)
- Interstitial lung disease
- Pulmonary embolism
- Pulmonary hypertension
- Chronic liver diseases limited to:
- Cirrhosis
- Non-alcoholic fatty liver disease
- Alcoholic liver disease
- Autoimmune hepatitis
- Cystic fibrosis
- Diabetes mellitus type 1
- Diabetes mellitus type 2
- Down syndrome. Down syndrome is linked to a higher risk of needing care in the hospital. The risk of death from severe COVID-19 also is higher than typical for people with Down syndrome.
- Heart conditions such as heart failure, coronary artery disease, or cardiomyopathies
- HIV (Human immunodeficiency virus)
- Mental health conditions limited to:
- Mood disorders, including depression
- Schizophrenia spectrum disorders
- Neurologic conditions limited to dementia and Parkinson’s Disease
- Obesity (BMI >30 kg/m² or >95th percentile in children)
- Physical inactivity
- Primary immunodeficiencies
- Smoking, current and former
- Solid organ or blood stem cell transplantation
- Tuberculosis
- Use of corticosteroids or other immunosuppressive medications
Additionally, some people may be at increased risk for COVID-19 infection including healthcare workers and residents and employees in long-term care facilities and other
residential congregate settings.
COVID-19 symptoms may appear 2 to 14 days after exposure to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The following list does not include all possible symptoms of COVID-19. Symptoms may change with new COVID-19 variants and can vary depending on vaccination status. Possible symptoms include:
- Fever or chills
- Dry cough
- Shortness of breath or difficulty breathing
- Sore throat
- Congestion or runny nose
- New loss of taste or smell
- Fatigue or extreme tiredness
- Muscle or body aches
- Headache
- Nausea or vomiting
- Diarrhea
People may have only a few symptoms or none at all. People who have no symptoms but test positive for COVID-19 are called asymptomatic. For example, many children who test positive don’t have symptoms of COVID-19 illness. People who go on to have symptoms are considered presymptomatic. People in both groups can still spread the COVID-19 virus to others.
Some people may have symptoms that get worse about 5 to 7 days after symptoms start.
Most people with COVID-19 have mild to moderate symptoms. But COVID-19 can cause serious medical complications and lead to death. Older adults and people who already have medical conditions are at greater risk of serious illness.
COVID-19 may be a mild, moderate, severe or critical illness.
- In broad terms, mild COVID-19 doesn’t affect the ability of the lungs to get oxygen to the body.
- In moderate COVID-19 illness, the lungs work properly but there are signs that the infection is deep in the lungs.
- Severe COVID-19 means that the lungs don’t work correctly, and the person needs oxygen and other medical help in the hospital.
- Critical COVID-19 illness means the lungs and breathing system, called the respiratory system, have failed and there is damage throughout the body.
Rarely, people who catch this coronavirus can develop a group of symptoms linked to inflamed organs or tissues. This illness is called multisystem inflammatory syndrome (MIS). When children have this illness, it is called multisystem inflammatory syndrome in children (MIS-C). In adults, the name is multisystem inflammatory syndrome in adults (MIS-A).
Complications of severe COVID-19 illness can include:
- Acute respiratory distress syndrome (ARDS), which is when the body’s organs do not get enough oxygen.
- New heart issues or shock caused by the infection or heart conditions.
- Overreaction of the immune system, called the inflammatory response.
- Blood clots.
- Damage to brain function, called encephalopathy.
- Kidney injury.
COVID-19 illness also may worsen medical conditions a person already have.
In the United States, at-home COVID-19 tests are available. The U.S. Food and Drug Administration (FDA) approves or authorizes the tests 9, 10, 11, 12. On the FDA website, you can find a list of the tests that are validated and their expiration dates. You also can check with your healthcare professional before buying a test if you have any concerns.
When taking a test at home, carefully read the directions that come with the test. Follow the instructions exactly to get as accurate a result as possible.
Here are some guidelines for when to take a COVID-19 test:
- If you have COVID-19 symptoms, test for the illness right away.
- If you were exposed to the COVID-19 virus but don’t have symptoms, wait at least five days after exposure and then test.
- If you have symptoms and tested positive for COVID-19 within the last 30 days, you can test again. But if you were recently exposed to the coronavirus and don’t have symptoms, you don’t need to test.
Also, testing before an event or contact with people at high risk of serious illness helps prevent the spread of the virus that causes COVID-19.
COVID-19 tests use a sample taken from your nose or throat, or a sample of saliva.
Two types of tests can help diagnose COVID-19.
- Molecular tests. These tests look for genetic material from the COVID-19 virus. Polymerase chain reaction (PCR) tests are molecular tests. You also may see this type of test referred to as a nucleic acid amplification test (NAAT). Polymerase chain reaction (PCR) tests are more accurate than the other type of COVID-19 test, called an antigen test. PCR tests may be done at home. But they are much more likely to be done by a doctor and processed in a lab.
- Antigen tests. These tests look for viral proteins called antigens. Antigen tests also may be called Rapid COVID-19 tests or At-Home COVID-19 tests. These tests are useful if you need a quick result. Antigen tests are reliable and accurate, but they are less accurate than polymerase chain reaction (PCR) tests. This is especially true if you don’t have symptoms. If you take an antigen test and the result shows that you do not have COVID-19, called a negative result, take another antigen test after 48 hours to get the most accurate result.
If you have a positive result with a COVID-19 polymerase chain reaction (PCR) or antigen test, you almost certainly have COVID-19. Another test isn’t needed.
If you get a negative polymerase chain reaction (PCR) test result, you most likely do not have COVID-19.
If you have a negative antigen test result, the FDA recommends that you repeat an antigen test two days after the first test. Whether or not you have symptoms, repeating the test helps get the correct diagnosis.
If you test positive, see your doctor immediately to find out what options are available for you.
Many people with COVID-19 recover with rest, plenty of fluids and care that manages symptoms. Medicine you can get without a prescription can help, such as:
- Fever reducers, such as ibuprofen (Advil, Motrin IB, others) or acetaminophen (Tylenol, others).
- Pain relievers, such as ibuprofen (Advil, Motrin IB, others) or acetaminophen (Tylenol, others).
- Cough syrup or medicine.
If you are at high risk of serious COVID-19 illness, your doctor may suggest medicine to prevent mild illness from getting worse. These medicines can include nirmatrelvir-ritonavir (Paxlovid), remdesivir (Veklury) or molnupiravir (Lagevrio). Nirmatrelvir-ritonavir and molnupiravir are taken by mouth as pills. Remdesivir is given through an IV.
If you’re very ill, you may need to be treated in the hospital.
People who are in the hospital for COVID-19 treatment receive care based on their immune system response and the need for oxygen support.
Added oxygen may be given through a tube in the nose. Some people may need to have a tube placed in their airways to push air into the lungs. That’s called mechanical ventilation. In very severe situations, a machine called extracorporeal membrane oxygenation (ECMO) can be used to mimic the function of the heart and lungs.
Medicines for severe COVID-19 may be remdesivir, baricitinib (Olumiant) or tocilizumab (Actemra), or a corticosteroid such as dexamethasone.
Baricitinib is a pill. Tocilizumab is given through an IV. Dexamethasone may be given either as a pill or through an IV.
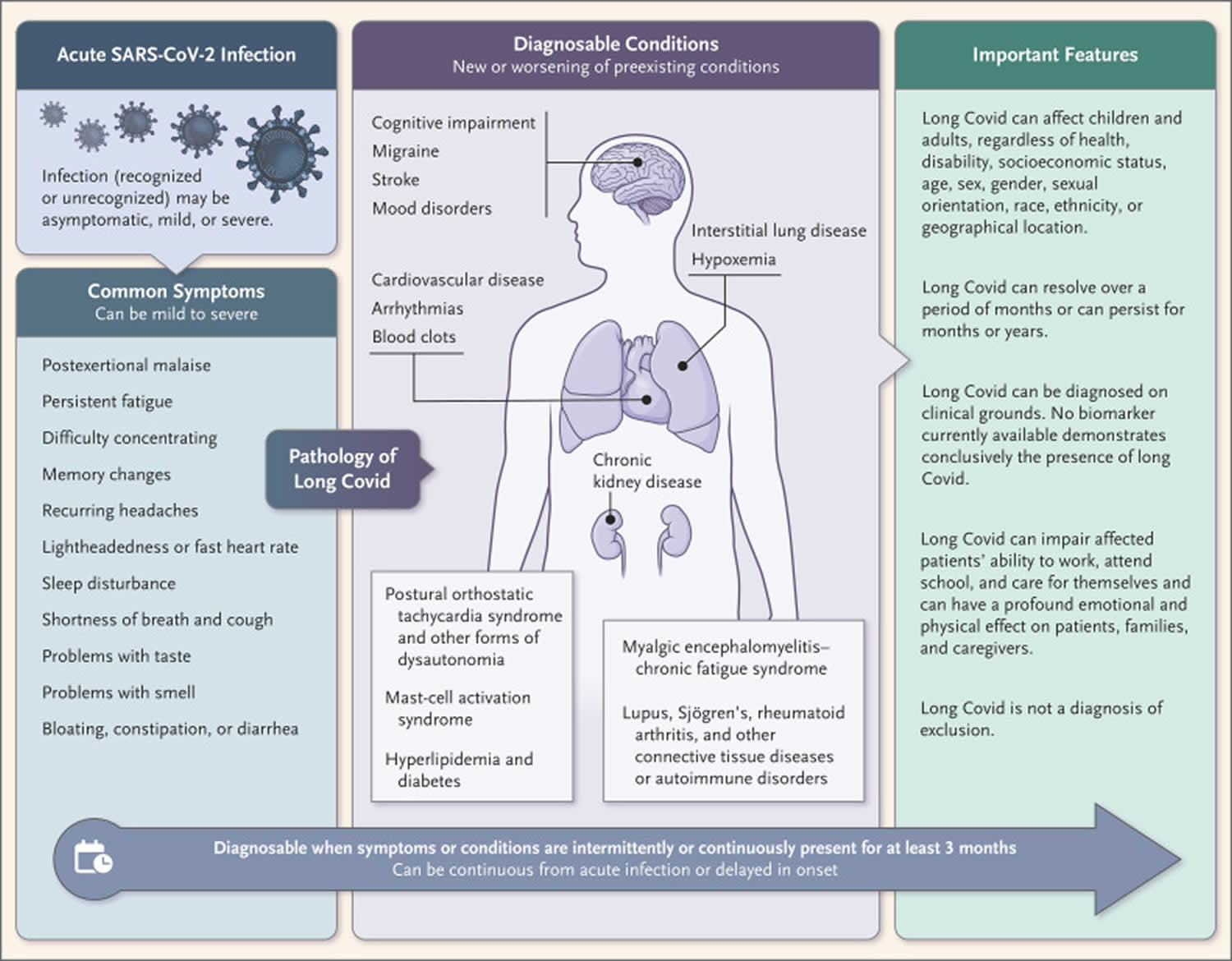
What is long COVID?
Long COVID, also known as Post-COVID Conditions (PCC), Post-Acute COVID, or Chronic COVID, is a term used to describe a chronic condition that occurs after COVID-19 infection and is present for at least 3 months that affects one or more organ systems 13, 14, 15, 16, 17. However, the actual definition for Long COVID is dependent on which continent you live in. The United States Centers for Disease Control and Prevention (CDC) defines “Long COVID” as symptoms lasting longer than 28 days from COVID diagnosis, while the United Kingdom National Institute for Health and Care Excellence (NICE) and the World Health Organization (WHO) require symptoms to be present at least 12 weeks after infection diagnosis 18, 19, 20. Symptoms can last weeks, months, or even years 21. Long COVID has been reported in at least 10% of patients recovering from COVID-19 infections and possibly up to 50% to 70% of hospitalized cases 22. Long COVID is seen in all levels of disease severity, from asymptomatic to critically ill, but the likelihood of Long COVID is highly correlated with the severity of symptoms. More than 200 symptoms have been associated with Long COVID, with the most commonly reported clinical symptoms being malaise, shortness of breath, fatigue, brain fogginess, autonomic dysfunction, headache, persistent loss of smell or taste, cough, depression, low-grade fevers, palpitations, dizziness, muscle pain, and joint pains16, 22. Most patients appear to recover from their initial acute COVID-19 illness within 4 weeks, and many patients continue to recover between 4 and 12 weeks.
Long COVID is associated with:
- Development of new or recurrent symptoms and conditions after the symptoms of initial acute COVID-19 illness have resolved.
- Symptoms that can emerge, persist, resolve, and reemerge over varying lengths of time.
- A spectrum of physical, social, and psychological consequences.
- Functional limitations that can affect patient wellness and quality of life and may cause disability.
Many theories exist regarding the cause of Long COVID, and the cause is likely multifactorial.
Possible causes of Long COVID include:
- Organ damage resulting from acute phase infection
- Complications from a dysregulated inflammatory state
- Microvascular dysfunction
- Ongoing viral activity associated with an intra-host viral reservoir
- Autoimmunity
- Inadequate antibody response
The leading possibilities for long COVID include ongoing viral infection, immune system dysregulation, small blood clots, imbalance of microorganisms most commonly the gut, systemic fibrosis, autoimmunity, persistent central nervous system infection, and autonomic dysfunction 22, 21, 23, 23, 24, 25.
Signs and symptoms are considered Long COVID if they begin or continue at least 4 weeks after the infection. Experts believe the immune system in some people overreacts to the virus that causes COVID-19. The immune system attacks the virus, but it also attacks healthy nerves, blood vessels, and organs. It is not yet known how long symptoms could continue. Anyone who had COVID-19 can develop long COVID, even if symptoms were mild or never developed at all.
Signs and symptoms may happen sometimes or all the time. Some may get better and then return or worsen later. Some may be worse with physical or mental activities. You may have any of the following:
General symptoms
- Tiredness or fatigue that interferes with daily life. Fatigue (feeling mentally and physically tired), trouble being as physically active as before, or trouble sleeping
- Symptoms that get worse after physical or mental effort
- Fever
Respiratory and heart symptoms
- Difficulty breathing or shortness of breath
- Coughing
- Chest pain
- Fast-beating or pounding heart (also known as heart palpitations)
Neurological symptoms
- Difficulty thinking or concentrating sometimes referred to as “brain fog”
- Headaches
- Sleep problems
- Dizziness when you stand up (lightheadedness)
- Pins-and-needles feelings
- Change in smell or taste
- Depression or anxiety
Digestive symptoms
- Diarrhea
- Stomach pain
- Constipation
Other symptoms
- Joint or muscle pain
- Rash
- Changes in menstrual cycles
People with Long COVID can have a wide variety of symptoms that can range from mild to severe and may be similar to symptoms from other illnesses. Symptoms can last weeks, months, or years after COVID-19 illness and can emerge, persist, resolve, and reemerge over different lengths of time. Long COVID may not affect everyone the same way.
Some people, especially those who had severe COVID-19, may experience multi-organ effects or autoimmune conditions lasting weeks, months, or even years after COVID-19 illness 26, 27. Multi-organ effects can involve many body systems, including the heart, lungs, kidneys, skin, and brain 28. Symptoms for many of these multi-organ complications are similar to commonly reported Long COVID symptoms. As a result of these effects, people who have had COVID-19 may be more likely to develop new or worsening of health conditions such as:
- Diabetes
- Heart conditions
- Blood clots
- Neurological conditions
Some people with Long COVID experience symptoms similar to those reported by people who suffer from other poorly understood chronic illnesses that may occur after other infections, such as Myalgic Encephalomyelitis or Chronic Fatigue Syndrome 29. People with Myalgic Encephalomyelitis or Chronic Fatigue Syndrome and other infection-associated illnesses can have difficulty:
- Recognizing and identifying symptoms of their illness
- Being believed by family, friends and healthcare providers
- Getting a diagnosis
- Managing their symptoms or conditions
Some people with Long COVID have symptoms that are hard to explain or difficult to manage. There is no laboratory test that can determine if your unexplained symptoms are due to Long COVID. A positive SARS-CoV-2 test is not required for a Long COVID diagnosis. People with these unexplained symptoms may sometimes even be misunderstood or experience stigma. This can result in a delay in diagnosis and receiving the appropriate care or treatment.
Your doctor considers a diagnosis of Long COVID based on:
- Your health history
- If you had a diagnosis of COVID-19 by a positive test, symptoms, or exposure
- A health examination
Clinical evaluations and results of routine blood tests, chest X-rays, and electrocardiograms may be normal in someone with Long COVID. Long COVID treatment is focused on managing symptoms, reducing their impact on daily activities, and improving your quality of life. People experiencing Long COVID should seek care from a doctor to create a personal medical management plan and improve their symptoms and quality of life.
Figure 1. Long COVID
COVID-19 vaccine types
Two types of COVID-19 vaccines currently recommended for use in the United States are the messenger RNA (mRNA) vaccines [Spikevax vaccine (Moderna), Mnexspike vaccine (Moderna) and Comirnaty vaccine (Pfizer-BioNTech)] and a protein subunit vaccine (Novavax vaccine sold under the brand names Nuvaxovid).
Messenger RNA (mRNA) vaccine
An mRNA vaccine gives cells instructions for how to make the S protein found on the surface of the COVID-19 virus. The vaccine shot sends the mRNA into your muscle. Your muscle cells may take in the mRNA and make the S protein. Or the mRNA may be picked up by an immune cell. Either the mRNA or the S protein alerts your body to the risk of the COVID-19 virus. Then your body begins to create a response to prevent you from getting sick from COVID-19 infection.
mRNA vaccines recommended for use in the United States 7:
- Moderna COVID-19 Vaccines: Spikevax (approved for ages 6 months and older) and Mnexspike (approved for ages 12 years and older). These vaccines are hereafter referred to collectively as Moderna COVID-19 Vaccine unless the specific vaccine name is relevant.
- Pfizer-BioNTech COVID-19 Vaccine: Comirnaty (approved for ages 5 years and older). Comirnaty vaccine is hereafter referred to as Pfizer-BioNTech COVID-19 Vaccine. There is currently NO FDA-approved or FDA-authorized Pfizer-BioNTech COVID-19 vaccine for ages 6 months to 4 years.
Vector vaccine
In vector vaccine, material from the virus that causes COVID-19 is placed in a modified version of a different virus. This different virus is called a viral vector. The viral vector gives cells instructions to make copies of the COVID-19 virus S protein. Once the cells display the S proteins on their surfaces, your immune system responds by creating antibodies and defensive white blood cells. If infection with the virus that causes COVID-19 happens later, the antibodies help clear out the virus.
Viral vector vaccines can’t cause infection with the COVID-19 virus or the viral vector virus. The Johnson & Johnson COVID-19 vaccine is a vector vaccine that’s no longer used in the United States.
Protein subunit vaccine
Subunit vaccines include only the parts of a virus that best stimulate the immune system. This type of COVID-19 vaccine has harmless S proteins in it. Once the immune system recognizes the S proteins, it creates antibodies and defensive white blood cells. If infection with the COVID-19 virus happens later, the antibodies help clear out the virus.
The Novavax COVID-19 vaccine is a protein subunit vaccine for use in the United States 7.
- Novavax COVID-19 Vaccine sold under the brand names Nuvaxovid (approved for ages 12 years and older). This vaccine is hereafter referred to as Novavax COVID-19 Vaccine.
COVID-19 vaccines available in the United States
The 2025-2026 COVID-19 vaccines available in the United States include Spikevax vaccine (Moderna), Mnexspike vaccine (Moderna), Comirnaty vaccine (Pfizer-BioNTech) and Novavax vaccines. These COVID-19 vaccines are all approved for people age 65 and older. Each vaccine is also approved for younger people with a health condition that raises the risk of serious COVID-19 illness.
The 2025–2026 formulations for COVID-19 vaccines in the United States are based on the Omicron JN.1-lineage of SARS-CoV-2, as follows 7:
- Spikevax vaccine (Moderna), Mnexspike vaccine (Moderna) and Comirnaty vaccine (Pfizer-BioNTech): LP.8.1 strain
- Novavax vaccine: JN.1 strain
The Spikevax, Mnexspike and Comirnaty COVID-19 vaccines for 2025-2026 focus on building protection against the LP.8.1 virus strain. The Novavax COVID-19 vaccine helps build protection against the JN.1 strain.
Moderna COVID-19 vaccine 2025-2026 formulas
- Spikevax. Spikevax vaccine is approved for people age 6 months to 64 years with a risk of serious COVID-19 illness and all people age 65 and older.
- Mnexspike. Mnexspike vaccine is approved for people age 12 to 64 years with a risk of serious COVID-19 illness and all people age 65 and older.
Pfizer BioNTech COVID-19 vaccine 2025-2026 formula
- Comirnaty. Comirnaty vaccine is approved for people age 5 to 64 years with a risk of serious COVID-19 illness and all people age 65 and older.
Novavax COVID-19 vaccine 2025-2026 formula
- Novavax COVID-19 vaccine (sold under the brand names Nuvaxovid). Novavax vaccine is approved for people age 12 to 64 years with a risk of serious COVID-19 illness and all people age 65 and older.
COVID-19 vaccination schedule
Age groups for approved use of 2025–2026 COVID-19 vaccines:
- For children ages 6 months to 4 years, only Spikevax COVID-19 vaccine is approved for use 30. Pfizer-BioNTech COVID-19 vaccine is NO longer authorized for this age group 30.
- Novavax COVID-19 vaccine (Nuvaxovid), approved for people ages 12 years and older, is administered as a single dose for initial vaccination 30.
- Mnexspike COVID-19 vaccine is approved for people ages 12 years and older 30.
- Comirnaty COVID-19 vaccine is approved for people ages 5 years and older 7.
Children ages 6 to 23 months
Spikevax vaccine is the only COVID-19 vaccine approved for children ages 6 to 23 months 30.
Children ages 6 to 23 months previously vaccinated with Pfizer-BioNTech COVID-19 vaccine should receive dose(s) of the 2025–2026 Spikevax vaccine 30.
Table 1. 2025–2026 COVID-19 vaccination schedule, November 4, 2025
| COVID-19 vaccination history before 2025–2026 vaccine* | Number of 2025–2026 doses indicated | Recommended 2025–2026 vaccine† and interval between doses |
|---|---|---|
| Unvaccinated: Administer initial series with 2025–2026 vaccine | ||
| Unvaccinated | 2 | 2025–2026 Dose 1 (Moderna): Day 0 2025–2026 Dose 2 (Moderna): 4–8 weeks after 2025–2026 Dose 1‡ |
| Initiated but did not complete the initial series before 2025–2026 vaccine: Complete initial series with 2025–2026 vaccine | ||
| 1 dose Moderna | 1 | 2025–2026 Dose 1 (Moderna): 4–8 weeks after last dose‡ |
| 1 dose Pfizer-BioNTech (Comirnaty vaccine) | 2 | 2025–2026 Dose 1 (Moderna): 3–8 weeks after last dose‡ 2025–2026 Dose 2 (Moderna): At least 4 weeks after 2025–2026 Dose 1 |
| 2 doses Pfizer-BioNTech (Comirnaty vaccine) | 1 | 2025–2026 Dose 1 (Moderna): At least 8 weeks after last dose |
| Completed the initial series before 2025–2026 vaccine: Administer 1 dose of 2025–2026 vaccine | ||
| 2 or more doses Moderna or 3 or more doses Pfizer-BioNTech (Comirnaty vaccine) | 1 | 2025–2026 Dose 1 (Moderna): At least 8 weeks after last dose |
Footnotes:
* COVID-19 vaccination history refers to all doses of COVID-19 vaccine from any manufacturer received before the availability of the 2025–2026 COVID-19 vaccines.
† Dosage for Spikevax vaccine: 0.25 mL/25 ug.
‡ An 8-week interval between the first and second COVID-19 vaccine doses (i.e., extended interval) might reduce the rare risk of myocarditis and pericarditis associated with COVID-19 vaccines.
Children ages 2 to 4 years
Spikevax vaccine is the only COVID-19 vaccine approved for children ages 2 to 4 years 30.
Spikevax vaccine is now administered to children ages 2 to 4 years as a single dose regardless of COVID-19 vaccination history 30.
See Table 2 footnote* for guidance on children who transition from age 23 months to 2 years during initial vaccination with 2025–2026 vaccine.
Table 2. Children ages 2 to 4 years COVID-19 vaccine schedule, November 4, 2025
| COVID-19 vaccination history before 2025–2026 vaccine† | Number of 2025–2026 doses indicated | Recommended 2025–2026 vaccine‡ and interval between doses |
|---|---|---|
| Unvaccinated: Administer initial vaccination with 2025–2026 vaccine | ||
| Unvaccinated | 1 | 2025–2026 Dose 1 Spikevax vaccine: Day 0 |
| Previously vaccinated before 2025–2026 vaccine: Administer 1 dose of 2025–2026 vaccine | ||
| 1 or more doses mRNA (Spikevax vaccine or Comirnaty vaccine) vaccine | 1 | 2025–2026 Dose 1 Spikevax vaccine: At least 8 weeks after last dose |
Footnotes:
* Children who transition from age 23 months to age 2 years during the initial vaccination with 2025–2026 vaccine (i.e., after they received Dose 1 but before Dose 2) should receive 1 dose of Spikevax vaccine 4–8 weeks after Dose 1.
† COVID-19 vaccination history refers to all doses of COVID-19 vaccine from any manufacturer received before the availability of the 2025–2026 COVID-19 vaccines.
‡ Dosage for Spikevax vaccine: 0.25 mL/25 ug.
Children ages 5 to 11 years
Spikevax vaccine and Comirnaty vaccine are approved for use in children ages 5 to 11 years 30.
Table 3. Children ages 5 to 11 years COVID-19 vaccine schedule, November 4, 2025
| COVID-19 vaccination history before 2025–2026 vaccine* | Number of 2025–2026 doses indicated | Recommended 2025–2026 vaccine† and interval between doses |
|---|---|---|
| Unvaccinated: Administer 1 dose of 2025–2026 vaccine | ||
| Unvaccinated | 1 | 2025–2026 Dose 1 (Spikevax vaccine or Comirnaty vaccine): Day 0 |
| Previously vaccinated before 2025–2026 vaccine: Administer 1 dose of 2025–2026 vaccine | ||
| 1 or more doses mRNA (Spikevax vaccine or Comirnaty vaccine) vaccine | 1 | 2025–2026 Dose 1 (Spikevax vaccine or Comirnaty vaccine): At least 8 weeks after last dose |
Footnotes:
* COVID-19 vaccination history refers to all doses of COVID-19 vaccine from any manufacturer received before the availability of the 2025–2026 COVID-19 vaccines.
† Dosage for Spikevax vaccine: 0.25 mL/25 ug; dosage for Comirnaty vaccine: 0.3 mL/10 ug.
People ages 12 to 64 years
Mnexspike, Spikevax, Novavax and Comirnaty COVID-19 vaccines are approved for people ages 12 to 64 years 30.
Novavax vaccine is administered as a single dose for initial vaccination 30.
Table 4. People ages 12 to 64 years COVID-19 vaccine schedule, November 4, 2025
| COVID-19 vaccination history before 2025–2026 vaccine* | Number of 2025–2026 doses indicated | Recommended 2025–2026 vaccine† and interval between doses |
|---|---|---|
| Unvaccinated: Administer 1 dose of 2025–2026 vaccine | ||
| Unvaccinated | 1 | 2025–2026 Dose 1 (Mnexspike, Spikevax, Novavax or Comirnaty COVID-19 vaccine): Day 0 |
| Previously vaccinated before 2025–2026 vaccine: Administer 1 dose of 2025–2026 vaccine | ||
| 1 or more doses any COVID-19 vaccine (Mnexspike, Spikevax, Novavax or Comirnaty vaccine) | 1 | 2025–2026 Dose 1 (Spikevax, Novavax, or Comirnaty vaccine): At least 8 weeks after last dose; (Mnexspike vaccine): At least 3 months after last dose‡ |
Footnotes:
* COVID-19 vaccination history refers to all doses of COVID-19 vaccine from any manufacturer received before the availability of the 2025–2026 COVID-19 vaccines.
† Dosage for Mnexspike vaccine: 0.2 mL/10 ug; dosage for Spikevax vaccine: 0.5 mL/50 ug; dosage for Novavax vaccine: 0.5 mL/5 ug rS protein and 50 ug Matrix-M adjuvant; dosage for Comirnaty vaccine: 0.3 mL/30 ug.
‡ The recommended interval for Mnexspike vaccine is 3 months after the last dose; however, a dose administered at least 2 months after the last dose should not be repeated.
People ages 65 years and older
Mnexspike, Spikevax, Novavax, and Comirnaty COVID-19 vaccines are approved for people ages 65 years and older 30.
Table 5. People ages 65 years and older COVID-19 vaccine schedule, November 4, 2025
| COVID-19 vaccination history before 2025–2026 vaccine* | Number of 2025–2026 doses indicated | Recommended 2025–2026 vaccine† and interval between doses |
|---|---|---|
| Unvaccinated: Administer 2 doses of 2025–2026 vaccine | ||
| Unvaccinated | 2 | 2025–2026 Dose 1 (Mnexspike, Spikevax, Novavax or Comirnaty COVID-19 vaccine): Day 0 2025–2026 Dose 2 (Spikevax vaccine, Novavax vaccine, or Comirnaty vaccine): 6 months (minimum interval 2 months) after 2025–2026 Dose 1; Mnexspike vaccine: 6 months (minimum interval 3 months)‡ after 2025–2026 Dose 1 |
| Previously vaccinated before 2025–2026 vaccine: Administer 2 doses of 2025–2026 vaccine | ||
| 1 or more doses any COVID-19 vaccine (Mnexspike, Spikevax, Novavax or Comirnaty COVID-19 vaccine) | 2 | 2025–2026 Dose 1 (Spikevax vaccine, Novavax vaccine, or Comirnaty vaccine): At least 8 weeks after last dose; Mnexspike vaccine: At least 3 months after last dose‡ 2025–2026 Dose 2 (Spikevax vaccine, Novavax vaccine, or Comirnaty vaccine): 6 months (minimum interval 2 months) after 2025–2026 Dose 1; Mnexspike vaccine: 6 months (minimum interval 3 months)‡ after 2025–2026 Dose 1 |
Footnotes:
* COVID-19 vaccination history refers to all doses of COVID-19 vaccine from any manufacturer received before the availability of the 2025–2026 COVID-19 vaccines.
† Dosage for Mnexspike vaccine 0.2 mL/10 ug; dosage for Spikevax vaccine: 0.5 mL/50 ug; dosage for Novavax vaccine: 0.5 mL/5 ug rS protein and 50 ug Matrix-M adjuvant; dosage for Comirnaty vaccine: 0.3 mL/30 ug.
‡ The recommended interval for Mnexspike vaccine is 3 months after the last dose; however, a dose administered at least 2 months after the last dose should not be repeated.
COVID-19 vaccine contraindications and precautions
Contraindications to vaccination are conditions that increase the risk for a serious adverse reaction 31. Vaccines should not be administered when a contraindication is present 31. Consultation with an allergist-immunologist is encouraged to provide expert evaluation of the original allergic reaction, and depending on the outcome of the evaluation, reassess if administration of additional doses of the same vaccine type may be possible 32.
People with a contraindication to one COVID-19 vaccine type (Table 6) may receive the alternative COVID-19 vaccine type in the usual vaccination setting 32. People with an allergy-related precaution to one COVID-19 vaccine type (Table 6) may receive the alternative COVID-19 vaccine type in the usual vaccination setting. Vaccination with the same COVID-19 vaccine type may be considered on an individual basis; the same vaccine type should be administered in an appropriate setting and under the supervision of a healthcare provider experienced in the management of severe allergic reactions. Additionally, if the same vaccine type is administered, an observation period of 30 minutes post-vaccination to monitor for allergic reactions and referral to an allergist-immunologist should be considered.
Healthcare professionals and health departments may request a consultation from CDC’s Clinical Immunization Safety Assessment Project for a complex COVID-19 vaccine safety question not readily addressed by CDC guidance.
Table 6. Contraindications and precautions to COVID-19 vaccination
| Medical condition or history | Guidance | Recommended action |
|---|---|---|
| History of a severe allergic reaction* (e.g., anaphylaxis†) after a previous dose or to a component of the COVID-19 vaccine‡ | Contraindication | Do not vaccinate with the same COVID-19 vaccine type.§ May administer the alternate COVID-19 vaccine type.§ See Considerations for people with a history of allergies and allergic reactions for additional information. |
| History of a diagnosed non-severe allergy* to a component of the COVID-19 vaccine‡ | Precaution | May administer the alternate COVID-19 vaccine type.§ For additional information, see Considerations for people with a history of allergies and allergic reactions. |
| History of a non-severe, immediate (onset less than 4 hours) allergic reaction* after administration of a previous dose of one COVID-19 vaccine type§ | Precaution | |
| Moderate or severe acute illness, with or without fever | Precaution | Defer vaccination until the illness has improved. |
| History of MIS-C or MIS-A | Precaution | See COVID-19 vaccination and MIS-C and MIS-A. |
| History of myocarditis or pericarditis within 3 weeks after a dose of any COVID-19 vaccine | Precaution | A subsequent dose of any COVID-19 vaccine should generally be avoided. See COVID-19 vaccination and myocarditis and pericarditis. |
Footnotes:
* For definitions of allergic reactions in Table 6 consult Interim Considerations: Preparing for the Potential Management of Anaphylaxis after COVID-19 Vaccination.
† Anaphylactic reactions have been rarely reported following receipt of COVID-19 vaccines, estimated incidence: 5 per million doses of mRNA COVID-19 vaccines administered 33. For more information on the assessment and potential management of anaphylaxis, see Interim Considerations: Preparing for the Potential Management of Anaphylaxis after COVID-19 Vaccination.
‡ See package inserts for a full list of vaccine ingredients. mRNA COVID-19 vaccines contain polyethylene glycol (PEG).
§ The mRNA COVID-19 vaccines (Mnexspike vaccine, Spikevax vaccine and Comirnaty vaccine) are one type of COVID-19 vaccine and the protein subunit vaccine (Novavax vaccine) is another type of COVID-19 vaccine.
Abbreviations: MIS-C = multisystem inflammatory syndrome in children; MIS-A = multisystem inflammatory syndrome in adults
[Source 32 ]COVID-19 vaccine booster
The U.S. Centers for Disease Control and Prevention (CDC) recommends the 2025-2026 COVID-19 vaccine for people ages 6 months and older based on individual-based decision making 1. This includes people who have received a COVID-19 vaccine, people who have had COVID-19, and people with long COVID 1.
Getting the 2025–2026 COVID-19 vaccine is especially important if you 1:
- Never received a COVID-19 vaccine
- Are ages 65 years and older
- Are at high risk for severe COVID-19
- Are living in a long-term care facility
- Are pregnant, breastfeeding, trying to get pregnant, or might become pregnant in the future.
- Want to lower your risk of getting Long COVID
Available COVID-19 vaccines
Two types of COVID-19 vaccines currently recommended for use in the United States are the messenger RNA (mRNA) vaccines [Spikevax vaccine (Moderna), Mnexspike vaccine (Moderna) and Comirnaty vaccine (Pfizer-BioNTech)] and a protein subunit vaccine (Novavax vaccine sold under the brand names Nuvaxovid).
- 2025–2026 Spikevax COVID-19 Vaccine: Anyone ages 6 months and older
- 2025–2026 Mnexspike COVID-19 Vaccine: Anyone ages 12 years and older
- 2025–2026 Comirnaty COVID-19 Vaccine: Anyone ages 5 years and older
- 2025–2026 Novavax COVID-19 Vaccine (Nuvaxovid): Anyone ages 12 years and older
See COVID-19 vaccination schedule above.
COVID-19 vaccine side effects
COVID-19 vaccines, like any medical product, can have side effects 34. Side effects reported after COVID-19 vaccination vary from person to person. Most common side effects are usually mild, such as soreness in the area where the shot was given. Everyone who gets a COVID-19 vaccine may be monitored onsite for at least 15 minutes after vaccination (people who experience or have experienced non-severe allergic reactions to COVID-19 vaccines may be monitored for 30 minutes).
mRNA vaccines (Spikevax, Mnexspike and Comirnaty vaccines) 34:
- Pain, soreness, redness at injection site
- Fatigue
- Headache
- Muscle pain
- Joint pain
- Chills
- Fever
- Nausea/vomiting (Moderna)
- In infants and toddlers, common symptoms include irritability or crying, decreased appetite, and sleepiness.
Protein subunit vaccine (Novavax vaccine) 34:
- Pain, soreness, redness, swelling at injection site
- Fatigue
- Headache
- Muscle pain
- Joint pain
- Chills
- Fever
- Nausea/vomiting
Severe allergic reactions
Severe allergic reactions following vaccination are rare but can be life threatening. Signs and symptoms of a severe allergic reaction can include:
- Anaphylaxis, a life-threatening reaction that needs to be treated with epinephrine (EpiPen) and that may require hospitalization. Symptoms include difficulty breathing, coughing, or wheezing.
- Low blood pressure or rapid heartbeat
- Swelling of the lips, tongue, or throat
- A widespread skin rash that can itch, be red, or cause raised bumps (hives). Can also include general swelling of parts of the body (like the face, arms, or legs).
- A rash in places like inside your mouth or nose. This requires hospitalization.
If you had a severe allergic reaction after receiving a particular type of COVID-19 vaccine (either mRNA or Novavax), you should not get another dose of that type of vaccine. You will likely be able to receive the alternate vaccine type. Your doctor may refer you to an allergy and immunology specialist for additional care or advice.
In rare cases, people have experienced serious health events after COVID-19 vaccination. An adverse event (any side effect or health problem after vaccination that is concerning to you, even if you are not sure if the vaccine caused the event) can be caused by the vaccine or be a coincidental event that is not related to the vaccine, such as an unrelated fever, that happened following vaccination.
Myocarditis and Pericarditis
Myocarditis is inflammation of the heart muscle. Pericarditis is inflammation of the outer lining of the heart. Cases of myocarditis and pericarditis have rarely been observed following COVID-19 vaccines used in the United States 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50. Cases have occurred most frequently in adolescent and young adult males within 7 days after receiving the second dose of an mRNA COVID-19 vaccine (Moderna and Pfizer-BioNTech); however, cases have also been observed in females and after other doses 36, 35. Data also suggest an increased risk of myocarditis and pericarditis following Novavax vaccination 36, 35. Vaccine recipients, especially males ages 12–39 years, should be made aware of the rare risk of myocarditis and pericarditis following COVID-19 vaccination.
Guillain-Barré Syndrome
Guillain-Barré syndrome is a rare autoimmune disorder where the immune system attacks the peripheral nerves, causing symptoms like tingling, weakness, and sometimes paralysis. Guillain-Barré syndrome often begins after a viral or bacterial infection, and while the cause is unknown, it can lead to a life-threatening condition if breathing muscles are affected. Based on data from the Vaccine Safety Datalink, the rate of Guillain-Barré syndrome within the first 21 days after receiving the Johnson & Johnson or Janssen COVID-19 vaccine was found to be 21 times higher than after receiving the Pfizer-BioNTech or Moderna (mRNA) COVID-19 vaccines 34. After the first 42 days, the rate of Guillain-Barré syndrome was 11 times higher after receiving the Johnson & Johnson or Janssen COVID-19 vaccine. Research found no increased risk of Guillain-Barré syndrome after receiving the Pfizer-BioNTech or Moderna vaccines 34. Similar to the data findings, CDC found higher than expected rates of Guillain-Barré syndrome reported to Vaccine Adverse Event Reporting System (VAERS) after receiving the Johnson & Johnson or Janssen COVID-19 vaccine but not after receiving the Pfizer-BioNTech or Moderna COVID-19 vaccines 34. Based on the findings from this data, the Advisory Committee on Immunization Practices (ACIP) recommended using mRNA COVID-19 vaccines instead of the Johnson & Johnson or Janssen COVID-19 vaccine, which is no longer available in the United States as of May 2023 34.
Thrombosis with thrombocytopenia syndrome
Thrombosis with thrombocytopenia syndrome (TTS) is a rare and serious condition that involves blood clots (thrombosis) and a low platelet count (thrombocytopenia) blood cells that help with clotting. Symptoms can include unusual blood clots in places like the brain or gut, accompanied by a low platelet count. Thrombosis with thrombocytopenia syndrome is a rare condition that has been seen in very few cases after getting the Johnson & Johnson or Janssen COVID-19 vaccine 34. Thrombosis with thrombocytopenia syndrome occurred in about 4 people per one million doses, with higher rates among women ages 30-49 years (9 to 10 cases per million). After reviewing data reports, a link between the Johnson & Johnson or Janssen COVID-19 vaccine and thrombosis with thrombocytopenia syndrome was found. This finding led to the Advisory Committee on Immunization Practices (ACIP) recommendation to use mRNA COVID-19 vaccines instead of the Johnson & Johnson or Janssen COVID-19 vaccine, which is no longer available in the United States 51, 52, 53, 54.
Death
There have been 55 cases of death after COVID-19 vaccination reported and a causal relationship has been excluded in 17 cases 55. In the remaining cases, the causal link between the vaccine and the death was not specified (8) or considered possible (15), probable (1), or very probable/demonstrated (14). The causes of deaths among these cases were: vaccine-induced immune thrombotic thrombocytopenia (VITT) (32), myocarditis (3), ADEM (1), myocardial infarction (1), and rhabdomyolysis (1). In such cases, the demonstration of a causal relationship is not obvious, and more studies, especially with post-mortem investigations, are needed to deepen understanding of the possible pathophysiological mechanisms of fatal vaccine side effects. A Finnish nationwide study between December 2020 and December 2021 found COVID-19 vaccination was suspected to play a part in 76 death 56. In Australia between 1 December 2021 and 31 December 2022, the TGA (Australian’s FDA) reports identified 14 reports where the cause of death was linked to COVID-19 vaccination from 976 reports received and reviewed of death in people who have been vaccinated with a COVID-19 vaccine 57.
COVID vaccine near me
You can find vaccination locations near you from your health department or pharmacies (https://www.vaccines.gov/en/). Check your local pharmacy’s website to see if vaccination appointments are available. Some pharmacies may offer vaccines to those who walk in without making an appointment ahead of time. Ask your doctor, pharmacist, or community health center, or visit their website. Contact your state health department. In many states, you may also dial 211 to connect to essential community services.
- Staying Up to Date with COVID-19 Vaccines. https://www.cdc.gov/covid/vaccines/stay-up-to-date.html[↩][↩][↩][↩][↩]
- About COVID-19. https://www.cdc.gov/covid/about/index.html[↩]
- Coronavirus disease 2019 (COVID-19). https://www.mayoclinic.org/diseases-conditions/coronavirus/symptoms-causes/syc-20479963[↩][↩][↩]
- Symptoms of COVID-19. https://www.cdc.gov/covid/signs-symptoms/index.html[↩]
- Sanyaolu A, Okorie C, Marinkovic A, Patidar R, Younis K, Desai P, Hosein Z, Padda I, Mangat J, Altaf M. Comorbidity and its Impact on Patients with COVID-19. SN Compr Clin Med. 2020;2(8):1069-1076. doi: 10.1007/s42399-020-00363-4[↩]
- Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, Jin HJ, Tan KS, Wang DY, Yan Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Mil Med Res. 2020 Mar 13;7(1):11. doi: 10.1186/s40779-020-00240-0[↩]
- Interim Clinical Considerations for Use of COVID-19 Vaccines in the United States, November 4, 2025. https://www.cdc.gov/covid/downloads/hcp/interim-clinical-considerations.pdf[↩][↩][↩][↩][↩]
- Underlying Conditions and the Higher Risk for Severe COVID-19. https://www.cdc.gov/covid/hcp/clinical-care/underlying-conditions.html[↩][↩][↩][↩]
- Coronavirus (COVID-19) Update: FDA Authorizes First COVID-19 Test for Self-Testing at Home. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-covid-19-test-self-testing-home[↩]
- FAQs on Testing for SARS-CoV-2. https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/faqs-testing-sars-cov-2[↩]
- At-Home COVID-19 Diagnostic Tests: Frequently Asked Questions. https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/home-covid-19-diagnostic-tests-frequently-asked-questions[↩]
- COVID-19 Test Basics. https://www.fda.gov/consumers/consumer-updates/covid-19-test-basics[↩]
- Long COVID Basics. https://www.cdc.gov/long-covid/about[↩]
- Clinical Overview of Long COVID. https://www.cdc.gov/long-covid/hcp/clinical-overview/index.html[↩]
- Ely EW, Brown LM, Fineberg HV; National Academies of Sciences, Engineering, and Medicine Committee on Examining the Working Definition for Long Covid. Long Covid Defined. N Engl J Med. 2024 Nov 7;391(18):1746-1753. doi: 10.1056/NEJMsb2408466[↩][↩]
- O’Mahoney LL, Routen A, Gillies C, et al. The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: A systematic review and meta-analysis. EClinicalMedicine. 2022 Dec 1;55:101762. doi: 10.1016/j.eclinm.2022.101762. Erratum in: EClinicalMedicine. 2023 May;59:101959. doi: 10.1016/j.eclinm.2023.101959[↩][↩]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Global Health; Board on Health Sciences Policy; Committee on Examining the Working Definition for Long COVID; Goldowitz I, Worku T, Brown L, et al., editors. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences. Washington (DC): National Academies Press (US); 2024 Jul 9. 2, Defining Long COVID. Available from: https://www.ncbi.nlm.nih.gov/books/NBK605682[↩]
- Chippa V, Aleem A, Anjum F. Postacute Coronavirus (COVID-19) Syndrome. [Updated 2024 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570608[↩]
- COVID-19 rapid guideline: managing the long-term effects of COVID-19. https://www.nice.org.uk/guidance/ng188/chapter/identification#case-definition[↩]
- Venkatesan P. NICE guideline on long COVID. Lancet Respir Med. 2021 Feb;9(2):129. doi: 10.1016/S2213-2600(21)00031-X[↩]
- Bonilla H, Peluso MJ, Rodgers K, et al. Therapeutic trials for long COVID-19: A call to action from the interventions taskforce of the RECOVER initiative. Front Immunol. 2023 Mar 9;14:1129459. doi: 10.3389/fimmu.2023.1129459[↩][↩]
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023 Mar;21(3):133-146. doi: 10.1038/s41579-022-00846-2. Epub 2023 Jan 13. Erratum in: Nat Rev Microbiol. 2023 Jun;21(6):408. doi: 10.1038/s41579-023-00896-0[↩][↩][↩]
- Raman B, Bluemke DA, Lüscher TF, Neubauer S. Long COVID: post-acute sequelae of COVID-19 with a cardiovascular focus. Eur Heart J. 2022 Mar 14;43(11):1157-1172. doi: 10.1093/eurheartj/ehac031[↩][↩]
- Yong SJ. Long COVID or post-COVID-19 syndrome: putative pathophysiology, risk factors, and treatments. Infect Dis (Lond). 2021 Oct;53(10):737-754. doi: 10.1080/23744235.2021.1924397[↩]
- Song WJ, Hui CKM, Hull JH, Birring SS, McGarvey L, Mazzone SB, Chung KF. Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses. Lancet Respir Med. 2021 May;9(5):533-544. doi: 10.1016/S2213-2600(21)00125-9[↩]
- Davis, H.E., McCorkell, L., Vogel, J.M. et al. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 21, 133–146 (2023). doi: 10.1038/s41579-022-00846-2[↩]
- Iqbal P, Ata F, Chaudhry H, et al. Post-COVID-19-associated multiorgan complications or “long COVID” with literature review and management strategy discussion: A meta-analysis. Health Sci Rep. 2023 Apr 14;6(4):e1211. doi: 10.1002/hsr2.1211[↩]
- National Academies of Sciences, Engineering, and Medicine. 2024. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences. Washington, DC: The National Academies Press. https://www.nationalacademies.org/read/27768[↩]
- Wood MS, Halmer N, Bertolli J, et al. (2024) Impact of COVID-19 on myalgic encephalomyelitis/chronic fatigue syndrome-like illness prevalence: A cross-sectional survey. PLoS ONE 19(9): e0309810. https://doi.org/10.1371/journal.pone.0309810[↩]
- 2025–2026 COVID-19 Vaccination Guidance. https://www.cdc.gov/covid/hcp/vaccine-considerations/routine-guidance.html[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Contraindications and Precautions. https://www.cdc.gov/vaccines/hcp/imz-best-practices/contraindications-precautions.html[↩][↩]
- Contraindications and Precautions. https://www.cdc.gov/covid/hcp/vaccine-considerations/safety-considerations.html[↩][↩][↩]
- Klein NP, Lewis N, Goddard K, et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA. 2021;326(14):1390–1399. doi:10.1001/jama.2021.15072[↩]
- Coronavirus Disease 2019 (COVID-19) Vaccine Safety. https://www.cdc.gov/vaccine-safety/vaccines/covid-19.html#cdc_generic_section_5-common-side-effects[↩][↩][↩][↩][↩][↩][↩][↩]
- Coronavirus Disease 2019 (COVID-19) Vaccine Safety. https://www.cdc.gov/vaccine-safety/vaccines/covid-19.html[↩][↩][↩]
- Safety Considerations for COVID-19 Vaccines. https://www.cdc.gov/covid/hcp/vaccine-considerations/safety-considerations.html[↩][↩][↩]
- Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices — United States, June 2021. https://www.cdc.gov/mmwr/volumes/70/wr/mm7027e2.htm[↩]
- Hause AM, Marquez P, Zhang B, et al. COVID-19 mRNA Vaccine Safety Among Children Aged 6 Months–5 Years — United States, June 18, 2022–August 21, 2022. MMWR Morb Mortal Wkly Rep 2022;71:1115–1120. DOI: http://dx.doi.org/10.15585/mmwr.mm7135a3[↩]
- Fleming-Dutra KE, Wallace M, Moulia DL, et al. Interim Recommendations of the Advisory Committee on Immunization Practices for Use of Moderna and Pfizer-BioNTech COVID-19 Vaccines in Children Aged 6 Months–5 Years — United States, June 2022. MMWR Morb Mortal Wkly Rep 2022;71:859–868. DOI: http://dx.doi.org/10.15585/mmwr.mm7126e2[↩]
- Hause AM, Baggs J, Marquez P, et al. COVID-19 Vaccine Safety in Children Aged 5–11 Years — United States, November 3–December 19, 2021. MMWR Morb Mortal Wkly Rep 2021;70:1755–1760. DOI: http://dx.doi.org/10.15585/mmwr.mm705152a1[↩]
- Walter, E. B., Talaat, K. R., Sabharwal, C., Gurtman, A., Lockhart, S., Paulsen, G. C., Barnett, E. D., Muñoz, F. M., Maldonado, Y., Pahud, B. A., Domachowske, J. B., Simões, E. A. F., Sarwar, U. N., Kitchin, N., Cunliffe, L., Rojo, P., Kuchar, E., Rämet, M., Munjal, I., Perez, J. L., … C4591007 Clinical Trial Group (2022). Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. The New England journal of medicine, 386(1), 35–46. https://doi.org/10.1056/NEJMoa2116298[↩]
- Woodworth KR, Moulia D, Collins JP, et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine in Children Aged 5–11 Years — United States, November 2021. MMWR Morb Mortal Wkly Rep 2021;70:1579–1583. DOI: http://dx.doi.org/10.15585/mmwr.mm7045e1[↩]
- Hause AM, Baggs J, Marquez P, et al. Safety Monitoring of COVID-19 Vaccine Booster Doses Among Persons Aged 12–17 Years — United States, December 9, 2021–February 20, 2022. MMWR Morb Mortal Wkly Rep 2022;71:347–351. DOI: http://dx.doi.org/10.15585/mmwr.mm7109e2[↩]
- Oster, M. E., Shay, D. K., Su, J. R., Gee, J., Creech, C. B., Broder, K. R., Edwards, K., Soslow, J. H., Dendy, J. M., Schlaudecker, E., Lang, S. M., Barnett, E. D., Ruberg, F. L., Smith, M. J., Campbell, M. J., Lopes, R. D., Sperling, L. S., Baumblatt, J. A., Thompson, D. L., Marquez, P. L., … Shimabukuro, T. T. (2022). Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA, 327(4), 331–340. https://doi.org/10.1001/jama.2021.24110[↩]
- Dooling K, Gargano JW, Moulia D, et al. Use of Pfizer-BioNTech COVID-19 Vaccine in Persons Aged ≥16 Years: Recommendations of the Advisory Committee on Immunization Practices — United States, September 2021. MMWR Morb Mortal Wkly Rep 2021;70:1344–1348. DOI: http://dx.doi.org/10.15585/mmwr.mm7038e2[↩]
- Gargano JW, Wallace M, Hadler SC, et al. Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices — United States, June 2021. MMWR Morb Mortal Wkly Rep 2021;70:977–982. DOI: http://dx.doi.org/10.15585/mmwr.mm7027e2[↩]
- Oliver, S. E., Wallace, M., See, I., et al. Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine: Updated Interim Recommendations from the Advisory Committee on Immunization Practices – United States, December 2021. MMWR. Morbidity and mortality weekly report, 71(3), 90–95. https://doi.org/10.15585/mmwr.mm7103a4[↩]
- Shimabukuro, T., & Nair, N. (2021). Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine. JAMA, 325(8), 780–781. https://doi.org/10.1001/jama.2021.0600[↩]
- Shimabukuro TT, Cole M, Su JR. Reports of Anaphylaxis After Receipt of mRNA COVID-19 Vaccines in the US—December 14, 2020-January 18, 2021. JAMA. 2021;325(11):1101–1102. doi:10.1001/jama.2021.1967[↩]
- Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Moderna COVID-19 Vaccine — United States, December 21, 2020–January 10, 2021. MMWR Morb Mortal Wkly Rep 2021;70:125–129. DOI: http://dx.doi.org/10.15585/mmwr.mm7004e1[↩]
- Kracalik, I., Oster, M. E., Broder, K. R., et al. Myocarditis Outcomes After mRNA COVID-19 Vaccination Investigators and the CDC COVID-19 Response Team (2022). Outcomes at least 90 days since onset of myocarditis after mRNA COVID-19 vaccination in adolescents and young adults in the USA: a follow-up surveillance study. The Lancet. Child & adolescent health, 6(11), 788–798. https://doi.org/10.1016/S2352-4642(22)00244-9[↩]
- Goddard, K., Lewis, N., Fireman, B., Weintraub, E., Shimabukuro, T., Zerbo, O., Boyce, T. G., Oster, M. E., Hanson, K. E., Donahue, J. G., Ross, P., Naleway, A., Nelson, J. C., Lewin, B., Glanz, J. M., Williams, J. T. B., Kharbanda, E. O., Katherine Yih, W., & Klein, N. P. (2022). Risk of myocarditis and pericarditis following BNT162b2 and mRNA-1273 COVID-19 vaccination. Vaccine, 40(35), 5153–5159. https://doi.org/10.1016/j.vaccine.2022.07.007[↩]
- Weintraub ES, Oster ME, Klein NP. Myocarditis or Pericarditis Following mRNA COVID-19 Vaccination. JAMA Netw Open. 2022;5(6):e2218512. doi:10.1001/jamanetworkopen.2022.18512[↩]
- Isaac See, Allison Lale, Paige Marquez, et al. Case Series of Thrombosis With Thrombocytopenia Syndrome After COVID-19 Vaccination—United States, December 2020 to August 2021. Ann Intern Med.2022;175:513-522. doi:10.7326/M21-4502[↩]
- Maiese A, Baronti A, Manetti AC, Di Paolo M, Turillazzi E, Frati P, Fineschi V. Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated? Vaccines (Basel). 2022 Feb 16;10(2):308. doi: 10.3390/vaccines10020308[↩]
- COVID-19 vaccination as a rare potential etiology for cause of death after medicolegal autopsy. A Finnish nationwide study. Vaccine: X Volume 24, June 2025, 100645, ISSN 2590-1362. https://doi.org/10.1016/j.jvacx.2025.100645[↩]
- https://www.tga.gov.au/sites/default/files/2024-03/FOI%204205.PDF[↩]

{kind=link}