
Contents
What is cradle cap
Cradle cap also known as pityriasis capitis, is the common name for seborrheic dermatitis or infantile seborrheic dermatitis affecting the scalp of newborns 1, 2, 3. Cradle cap is a common, harmless skin condition that causes yellow scales or white scaly patches on your baby’s scalp, but it can be distressing for parents 4. The scales are greasy or flaky, and a rash may surround them. Cradle cap doesn’t usually itch or cause discomfort to your baby. Cradle cap has no negative effects on your baby’s health and doesn’t affect their eating or sleeping. Do not pick at the scales as this can cause an infection. Cradle cap is not contagious and is not caused by poor hygiene or an allergy. Cradle cap is very common and affects most babies at one point or another. Cradle cap is not a contagious condition, nor does it occur because of poor hygiene. Cradle cap usually appears in babies in the first two months and clears up without treatment within weeks to a few months and goes away before your baby’s first birthday. A few babies develop cradle cap at 1 or 2 years of age. Simple, at-home care like gently shampooing your baby’s scalp may help speed things along. Regular baby shampoo works just fine to lather up your baby’s scalp. Just make sure the shampoo is mild and unscented. Don’t use shampoos made for adults or designed to treat dandruff as these aren’t meant for a baby’s delicate skin. If you’d like, you can try a specially-made shampoo for this condition. You’ll find these at the store with “cradle cap” on the label. You can also ask your pediatrician or skin doctor to recommend a shampoo formulated to help with cradle cap. Additionally, adult dandruff shampoos that contain salicylic acid aren’t recommended for use in babies either because that ingredient can be absorbed through the skin.
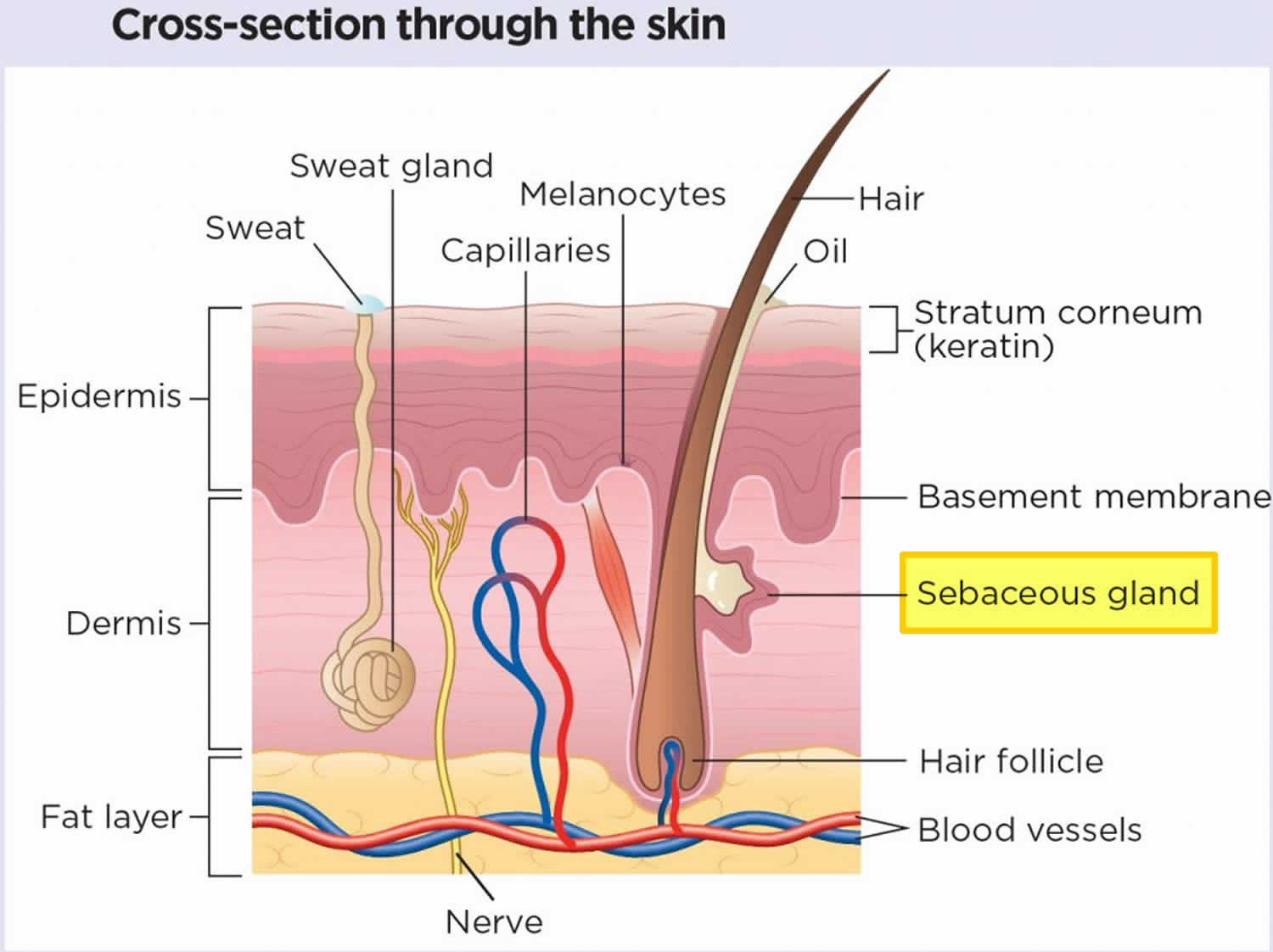
Seborrheic dermatitis also called seborrhoeic dermatitis or seborrheic eczema is a common, longterm (chronic) or relapsing form of dermatitis (inflammatory skin condition) or chronic form of eczema that mainly affects the sebaceous gland (oil-producing) rich regions of your body, including your scalp, face, eyebrows, eyelids, ears and trunk 5, 6, 7, 8. Seborrheic dermatitis appears as itchy red patches, greasy scales with white or yellow crusty or powdery flakes on your scalp and other parts of your body, but its not contagious. Seborrheic dermatitis can occur with or without redness. Its presence doesn’t mean the skin is unclean or infected. “Seborrheic” refers to the “sebaceous glands” while “dermatitis” means “inflammatory skin condition”. Sebaceous glands are microscopic oil glands found in your hair follicles that secrete sebum. Sebum is an oily substance that protects your skin from drying out (see Figure 1). There are infantile and adult forms of seborrheic dermatitis. Seborrheic dermatitis on the scalp of teenagers or adults is called “dandruff” or “pityriasis capitis” and “cradle cap” when seborrheic dermatitis is on a baby’s scalp 9, 10. Dandruff presents as diffuse bran-like scaly patches within hair-bearing areas of the scalp without underlying redness. Dandruff may be asymptomatic or mildly itchy. Cradle cap (pityriasis capitis) is the common term for seborrheic dermatitis on the scalp of infants. Cradle cap is seen most commonly in infants aged between 3 weeks and 12 months with peak prevalence at 3 months of age 11.
Cradle cap is a very common skin disorder affecting the oil-rich parts of the skin, including the face, ears, and scalp, and it is often seen in babies up to 3 months of age. The skin becomes flaky and inflamed, and a yellowish scale can accumulate. If the scale is picked off, the skin underneath will look pink or red. Cradle cap itself is not serious, but the affected areas can become infected if not treated properly. The cause of cradle cap is related to overgrowth of normal skin yeast including Malassezia (Pityrosporum) species and Candida. Any baby can develop cradle cap.
Cradle cap begins as a flaky scalp; it may then progressively worsen to a yellow scale layered on pink or red skin. The hair may become matted down in the scale. Babies may be itchy and may scratch at their heads or more commonly, rub their heads or faces on surfaces. If the cradle cap becomes infected, it will ooze, scab, become increasingly red, or the baby might develop a fever.
Cradle cap is easily treated; start by trying to gently remove some of the scale and flakiness by giving the baby a warm bath with gentle baby shampoo. If this is not sufficient, try loosening the scale before bath time by applying a bland oil, such as mineral oil or baby oil, massaging it in and carefully combing with a soft toothbrush or cradle crap comb and shampooing it out at bath time. Emollients are ingredients in skin care products that soothe dryness or irritation. Occlusive emollients form a thick and greasy coating on your baby’s skin and don’t dissolve in water. Examples of occlusive emollients include petroleum jelly, mineral oil, lanolin and liquid paraffin. The emollient may prove more effective if remaining in contact with the skin for a prolonged period of time, overnight if necessary, to break up the scale. Avoid olive oil, which may not be good for your baby’s skin, and peanut oil, in case of allergies. The oil will help soften the scale making it easier for removal. Once the scale is removed, parents should continue daily shampooing of their infant’s affected areas to prevent recurrence.
Finally, you may try a shampoo designed for dandruff in adults, such as one with salicylic acid or selenium sulfide, although you should discuss this with your baby’s doctor before attempting it if the baby is younger than 3 months.
Your baby’s doctor may recommend a stronger antifungal shampoo or an antifungal cream. If the area is infected, he/she will prescribe antibiotics. If the area is very inflamed, your doctor may prescribe a steroid cream.
Figure 1. Skin anatomy
Cradle cap is benign and self-limiting. Cradle cap usually resolves without intervention over the course of weeks to several months. If disease persists beyond 12 months, the diagnosis should be reconsidered.
You should see your child’s doctor if the cradle cap does not improve with the self-care measures described above. Be sure to call the doctor if the cradle cap looks red, oozes, has excessive crusting, it spreads to the face or body or if the baby has fever coupled with the previously described symptoms.
Other scalp conditions that may resemble cradle cap are:
- Atopic dermatitis
- Impetigo
- Tinea capitis
- Contact irritant dermatitis
- Psoriasis.
Cradle cap vs. seborrheic dermatitis
Seborrheic dermatitis is the medical term for itchy red patches and greasy scales that can affect you at any age (in adults, you know it as “dandruff”). Cradle cap is a form of seborrheic dermatitis that’s limited to your baby’s scalp and occurs soon after birth. You might hear people call it infantile seborrheic dermatitis.
Some babies can develop seborrheic dermatitis in other areas besides their scalp (like their face or bottom). If that happens, your pediatrician can offer additional guidance on clearing up your baby’s condition.
What does cradle cap look like?
Classically with cradle cap, there is a non-inflammatory eruption of greasy yellow scales on the scalp. The vertex and frontal areas are most commonly affected. Cradle cap is usually not itchy and infants are otherwise generally well.
Cradle cap is easy to recognise by the large, greasy, yellow or brown scales on your baby’s scalp.
The scales flake and may make the affected skin look red. Sometimes the hair will come away with the flakes, but it will grow back.
It usually occurs on the scalp but can also affect the face, ears, neck, nappy area and armpits, and behind the knees.
Figure 2. Cradle cap baby – the baby may have anywhere from fine, white scaling to greasy, thick hyperkeratosis of the scalp.

Figure 3. Cradle cap baby – greasy, yellow scaly patches that sometimes appear on the scalps of young babies

Figure 4. Seborrheic dermatitis newborn

Who gets cradle cap?
Cradle cap is extremely common in early infancy with an estimated prevalence of 9.5–10%. Cradle cap is seen most commonly in infants aged between 3 weeks and 12 months with peak prevalence at 3 months of age 12. Foley et al. 12 reported a prevalence of 10.4% in boys and 9.5% in girls, suggesting no gender predilection. Furthermore, cradle cap peaks at three months of age with a prevalence of 70%, then decrease steadily as the infant approaches one year of life. Cradle cap affects about 7% of children between during the second year of life, and most cases are characterized as mild, with a further decrease in prevalence through the fourth year of life 12
Is cradle cap contagious?
Cradle cap isn’t contagious. You don’t need to worry about your baby spreading the rash to others. You can send your baby to daycare or let them have play dates with other babies.
Cradle cap causes
The exact cause why babies get cradle cap is not known. Scientists believe cradle cap is likely due to a combination of factors. It may be related to hyperactivity of sebaceous glands responsive to residual circulating maternal androgens 13. For example, sebaceous glands in your baby’s scalp may produce too much sebum (an oil-like substance) possibly due to hormones they receive from their birthing mother. Overproduction of sebum causes the dead skin cells (scale) to remain stuck to the scalp instead of undergoing normal peeling or shedding. Evidence from research indicates that human sebocytes (fat-producing cells) respond to androgen stimulation, and their increased activity worsens the severity of cradle cap 14. Furthermore, the increase in frequency of seborrheic dermatitis during infancy and adolescence supports a hormonal influence on the condition 1.
Malassezia (Pityrosporum) yeast that naturally lives on your baby’s skin has also been implicated in many cases of cradle cap although its exact role is not clear 15, 13. Malassezia yeast breaks down sebum (an oil-like substance), consuming the saturated fatty acids, and subsequently leaves the unsaturated fatty acids behind. Malassezia globosa and Malassezia restricta have been found in over 80% of all age cases in an outpatient dermatology setting 16. The fact that cradle cap responds to antifungal medication strongly supports the role of yeast as a causal factor 14. This theory is further supported by the observed reduction in the number of Malassezia (Pityrosporum) yeast cells during treatment, which correlates with clinical improvement 17. Recurrence of cradle cap is observed following a rebound in the number of Malassezia yeast cells to pretreatment levels 18. However, Malassezia yeast is also seen in a large quantity of normal patients, suggesting an independent susceptibility to the yeast.
Studies have shown that infants with cradle crap commonly have a family member with either atopic dermatitis and/or asthma 19.
Cradle cap isn’t contagious, and it’s not caused by poor hygiene.
Cradle cap prevention
Shampooing your baby’s hair every few days can help prevent cradle cap. Gentle, daily use of baby shampoo should be tried initially. If this fails or the crust is particularly thick, a vegetable or other mineral oil overnight and a mild tar shampoo in the morning is usually effective. A soft infant brush or comb may be helpful to remove any adherent crust. If these home care tips don’t work, talk with your baby’s doctor about products that might help, such as a low-potency hydrocortisone cream or a shampoo with 2% antifungal ketoconazole medicine. Ketoconazole 2% cream is shown to be an effective choice with a clinical cure rate of 79%. Occasionally, a mild topical steroid may be needed.
The following home care tips may help you control the build up fo scales of cradle cap:
- Soften the scales with baby oil first, followed by gentle brushing with a soft brush to loosen scales, and then wash off with baby shampoo. Soak the crusts overnight with white petroleum jelly, plain mineral oil or baby oil, and shampoo in the morning. Gently rub your baby’s scalp with your fingers or a washcloth to loosen the scales. Don’t scratch.
- Wash your baby’s hair once a day with baby shampoo. Loosen the scales with a small, soft-bristled brush or fine-toothed comb before rinsing off the shampoo.
- If the scales don’t loosen easily, rub petroleum jelly or a few drops of mineral oil onto your baby’s scalp. Let it soak into the scales for a few minutes, or hours if needed. Then brush and shampoo the hair as usual. Be sure to rinse well. If you leave in the oil, the cradle cap may get worse.
- When the scales are gone, wash your baby’s hair two or three times a week with a mild shampoo to prevent scale buildup.
You can buy special shampoo for cradle cap from a pharmacy. Always read the instruction leaflet to check it’s safe to use on your child.
Avoid getting the shampoo in your baby’s eyes. If you’re unsure about using it, speak to a pharmacist for advice.
If these methods don’t work, speak to your pharmacist about using a greasy emollient (e.g., white petrolatum, mineral oil, baby oil) or soap substitute, such as emulsifying ointment.
There is usually no need to see your doctor if your baby has cradle cap. However, you may want to ask them for advice if there is swelling to the scalp or if the cradle cap spreads to other parts of the body.
Cradle cap signs and symptoms
Cradle cap refers only to the scaly rash on a baby’s scalp. The vertex and frontal areas are most commonly affected. When you look at your baby’s scalp, you’ll see yellow or white patches of scales that resemble fish scales. When you touch the scales, they may feel fragile and flaky. Or, they may feel waxy and greasy. This scaly skin doesn’t cause your baby any pain or discomfort. Most babies don’t even seem to notice it and are otherwise generally well with uninterrupted feeding and sleep 20.
Cradle cap classically presents as greasy, non-inflammatory plaques with overlying yellowish scale, on the vertex and frontal regions of the scalp. Similar scales also may be present on the ears, eyelids, nose and groin.
These greasy, non-inflammatory plaques with overlying yellowish scale stick to your baby’s head and may:
- Look crusted.
- Flake off.
- Be surrounded by a red or pink rash (if your baby has light skin tones).
- Be surrounded by a rash that’s lighter or darker than your baby’s normal skin color (if your baby has darker skin tones).
Some babies have seborrheic dermatitis that extends beyond their scalp, including parts of their face. If this happens, you may notice a rash:
- On your baby’s forehead.
- On their eyebrows.
- In the folds of their neck or arms.
- Behind their ears.
- On their bottom (diaper rash).
If you notice these signs, tell your pediatrician. They’ll check your baby and see if they need special moisturizers or medicated creams.
Cradle cap complications
Bacterial co-infection could be a possible, but rarely seen complication, likely due to repeated scratching if irritated.
Cradle cap diagnosis
Your baby’s doctor can diagnose cradle cap simply by looking at your baby’s scalp. The rash and scales, along with their location on your baby’s head, are easy clues to identifying the condition. Your baby doesn’t need any lab tests or biopsies.
On physical exam, notable findings include accumulation of greasy yellow scale on the vertex and forehead of the scalp. The face may also be involved, presenting as erythematous scaly plaques on the forehead, eyebrows/eyelids, nasolabial folds, cheeks, and post-auricular areas. Nonetheless, other areas may be affected such as the umbilical area, diaper zone, and skin fold areas. The areas affected away from the scalp tend to have less scale with more redness. In rare cases, cradle cap can present as an erythrodermic eruption (intense and usually widespread reddening of the skin due to inflammatory skin disease). In this situation, immunodeficiencies and vitamin deficiencies should be considered by the clinician.
Cradle cap differential diagnosis
Other scalp conditions that may resemble cradle cap are:
- Atopic dermatitis. Atopic dermatitis presents with moderate to severe itch that interferes with sleeping and feeding in the baby, as well as reddish, scaly and sometimes crusted lesions that are poorly demarcated on the cheek, scalp and extensor surfaces.
- Impetigo. Impetigo starts out as small fluid-filled sacs or blisters with a thin, fragile roof.
- Tinea capitis. Tinea capitis presents similarly although with possible hair loss, the presence of lymphadenopathy and confirmed with KOH examination.
- Contact irritant dermatitis
- Psoriasis. Psoriasis is uncommon in this age group, but would present as sharply defined, bright red, silvery scale papules that coalesce into plaques.
- Langerhans cell histiocytosis. Langerhans cell histiocytosis should be considered in refractory cases of infantile seborrhoeic dermatitis that present with ulceration and erosion along with brownish-red to purpuric nodules in similar areas, ultimately confirmed by biopsy.
Cradle cap treatment
If your baby only has cradle cap, without rashes elsewhere on their body, they likely don’t need medical treatment. Cradle cap should go away on its own within a few months. The initial approach, especially in mild and localized cradle cap, should be conservative, involving either application of gentle emollient or repeated shampooing, followed by careful removal of scales using a soft toothbrush or comb.
How you can help get rid of cradle cap:
- Soften the skin. Before you wash your baby’s scalp, apply an emollient to their skin. Good options are plain mineral oil, petroleum jelly and baby oil. Avoid olive oil, which may not be good for your baby’s skin, and peanut oil, in case of allergies. Gently massage the emollient into your baby’s scalp and leave it on for several hours (or even overnight) before shampooing.
- Lather up. Wash your baby’s scalp every other day with a mild, fragrance-free shampoo. Gently massage their scalp using your fingertips or a soft washcloth. Don’t scrub hard or use anything scratchy against your baby’s skin (like your fingernails). You may choose to use a soft brush to help remove the scales.
- Don’t pick at the scales. You may be tempted to scratch or pick at the scales to pry them loose. But don’t do this! Picking at the scales creates areas of raw skin and may increase your baby’s risk of an infection.
More extensive or resistant cradle cap (cradle cap that does not improve after conservative measures) may be treated with a low-potency topical steroid cream (e.g., hydrocortisone 1%) or azole antifungal cream (e.g., ketoconazole 2%) for 1–2 weeks. Topical steroid may be preferred if there is a significant inflammatory component 21, 22.
In intertriginous areas (skinfold areas), ketoconazole 2% cream is the preferred treatment option. Wannanukul et al. 23 reported no superiority between ketoconazole 2% and hydrocortisone 1% for infantile seborrheic dermatitis, suggesting the primary mechanism to be emollient care. Nonetheless, the efficacy between 2% ketoconazole cream and 1% hydrocortisone cream showed no statistical significance in the better treatment option 24. Selenium sulfide, zinc pyrithione, and salicylic acid are used in adults with seborrheic dermatitis, yet the efficacy and safety are not known in the infant population.
Cradle cap prognosis
Cradle cap is benign and self-limiting. Any baby can develop cradle cap. Cradle cap is not contagious and does not occur because of poor hygiene. It usually resolves without any treatment over the course of weeks to several months. If cradle cap persists beyond 12 months, the diagnosis should be reconsidered.
It’s a good idea to call your pediatrician if you notice one or more of the following issues:
- The cradle cap isn’t improving after a few months.
- Your baby has a rash on areas other than their scalp.
- The skin on your baby’s scalp feels hot to the touch.
- Fluid or blood is leaking from the crusted skin.
- The skin on your baby’s scalp smells bad.
- The area of the rash and scales looks swollen or very red.
These signs could mean your baby:
- May benefit from prescription creams or shampoos.
- Has seborrheic dermatitis that’s not just limited to their scalp. This may need treatment, such as a medicated cream.
- Has another condition like atopic dermatitis or scabies that needs treatment.
- Nobles T, Harberger S, Krishnamurthy K. Cradle Cap. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531463[↩][↩]
- Victoire A, Magin P, Coughlan J, van Driel ML. Interventions for infantile seborrhoeic dermatitis (including cradle cap). Cochrane Database Syst Rev. 2019 Mar 4;3(3):CD011380. doi: 10.1002/14651858.CD011380.pub2[↩]
- Elish D, Silverberg NB. Infantile seborrheic dermatitis. Cutis. 2006 May;77(5):297-300.[↩]
- Micali G, Pulvirenti N, Dall’Oglio F, Tedeschi A, Quattrocchi E, Lacarrubba F. Treatment of cradle cap in infants with a new cosmetic non-steroidal gel cream: Clinical, laboratory, and instrumental evaluation. J Cosmet Dermatol. 2021 Apr;20 Suppl 1(Suppl 1):14-17. doi: 10.1111/jocd.14095[↩]
- Woolhiser E, Keime N, Patel A, Weber I, Adelman M, Dellavalle RP. Nutrition, Obesity, and Seborrheic Dermatitis: Systematic Review. JMIR Dermatol. 2024 Aug 5;7:e50143. doi: 10.2196/50143[↩]
- Heath CR, Usatine RP. Seborrheic dermatitis. J Fam Pract. 2021 Nov;70(9):E3-E4. doi: 10.12788/jfp.0315[↩]
- Okokon EO, Verbeek JH, Ruotsalainen JH, Ojo OA, Bakhoya VN. Topical antifungals for seborrhoeic dermatitis. Cochrane Database Syst Rev. 2015 May 2;(5):CD008138. doi: 10.1002/14651858.CD008138.pub3[↩]
- Gupta A, Bluhm R. Seborrheic dermatitis. J Eur Acad Dermatol Venereol. 2004;18(1):13–26. doi: 10.1111/j.1468-3083.2004.00693.x.693[↩]
- Seborrheic Dermatitis. https://my.clevelandclinic.org/health/diseases/14403-seborrheic-dermatitis[↩]
- Seborrhoeic dermatitis. https://dermnetnz.org/topics/seborrhoeic-dermatitis[↩]
- Foley P, Zuo Y, Plunkett A, Merlin K, Marks R. The frequency of common skin conditions in preschool-aged children in Australia: seborrheic dermatitis and pityriasis capitis (cradle cap). Arch Dermatol. 2003 Mar;139(3):318-22. doi: 10.1001/archderm.139.3.318[↩]
- Foley P, Zuo Y, Plunkett A, Merlin K, Marks R. The frequency of common skin conditions in preschool-aged children in Australia: seborrheic dermatitis and pityriasis capitis (cradle cap). Arch Dermatol. 2003 Mar;139(3):318-22. https://jamanetwork.com/journals/jamadermatology/fullarticle/479236[↩][↩][↩]
- Ro BI, Dawson TL. The role of sebaceous gland activity and scalp microfloral metabolism in the etiology of seborrheic dermatitis and dandruff. J Investig Dermatol Symp Proc. 2005 Dec;10(3):194-7. doi: 10.1111/j.1087-0024.2005.10104.x[↩][↩]
- Antifungal agents: mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Ghannoum MA, Rice LB. Clin Microbiol Rev. 1999 Oct; 12(4):501-17.[↩][↩]
- Kim GK. Seborrheic Dermatitis and Malassezia species: How Are They Related? Del Rosso JQ, ed. The Journal of Clinical and Aesthetic Dermatology. 2009;2(11):14-17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2923939/[↩]
- Zhang H, Ran Y, Xie Z, Zhang R. Identification of Malassezia species in patients with seborrheic dermatitis in China. Mycopathologia. 2013 Feb;175(1-2):83-9. doi: 10.1007/s11046-012-9606-z[↩]
- Bergrant IM, Faegemann J, Voog E, Lowhagen GB. Pytirosporum ovale and seborrhoeic dermatitis in HIV-seropositive and HIV-seronegative men. Quantitative cultures and serological studies. Journal of the European Academy of Dermatology & Venereology. 1996;6(2):147–51. DOI: 10.1111/j.1468-3083.1996.tb00158.x[↩]
- Higgins JPT, Green S. Cochrane Handbook for Systematic reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration 2011. www.cochrane-handbook.org. The Cochrane Collaboration[↩]
- Johansson C, Tengvall Linder M, Aalberse RC, Scheynius A. Elevated levels of IgG and IgG4 to Malassezia allergens in atopic eczema patients with IgE reactivity to Malassezia. Int Arch Allergy Immunol. 2004 Oct;135(2):93-100. doi: 10.1159/000080651[↩]
- Palamaras I, Kyriakis KP, Stavrianeas NG. Seborrheic dermatitis: lifetime detection rates. J Eur Acad Dermatol Venereol. 2012 Apr;26(4):524-6. doi: 10.1111/j.1468-3083.2011.04079.x[↩]
- Okokon EO, Verbeek JH, Ruotsalainen JH, Ojo OA, Bakhoya VN. Topical antifungals for seborrhoeic dermatitis. The Cochrane Database of Systematic Reviews. 2015;(4):CD008138. doi:10.1002/14651858.CD008138.pub2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4448221/[↩]
- Wananukul S, Chatproedprai S, Charutragulchai W. Randomized, double-blind, split-side comparison study of moisturizer containing licochalcone vs. 1% hydrocortisone in the treatment of infantile seborrhoeic dermatitis. J Eur Acad Dermatol Venereol. 2012 Jul;26(7):894-7. doi: 10.1111/j.1468-3083.2011.04187.x[↩]
- Wannanukul S, Chiabunkana J. Comparative study of 2% ketoconazole cream and 1% hydrocortisone cream in the treatment of infantile seborrheic dermatitis. J Med Assoc Thai. 2004 Sep;87 Suppl 2:S68-71.[↩]
- Taieb A, Legrain V, Palmier C, Lejean S, Six M, Maleville J. Topical ketoconazole for infantile seborrhoeic dermatitis. Dermatologica. 1990;181(1):26-32. doi: 10.1159/000247855[↩]





{kind=link}