Contents
- What is Embryonal Carcinoma
- Testis anatomy
- Embryonal carcinoma causes
- Embryonal carcinoma prevention
- Embryonal carcinoma symptoms
- Embryonal carcinoma diagnosis
- Staging embryonal carcinoma of testis
- Embryonal carcinoma treatment
- Embryonal carcinoma prognosis
What is Embryonal Carcinoma
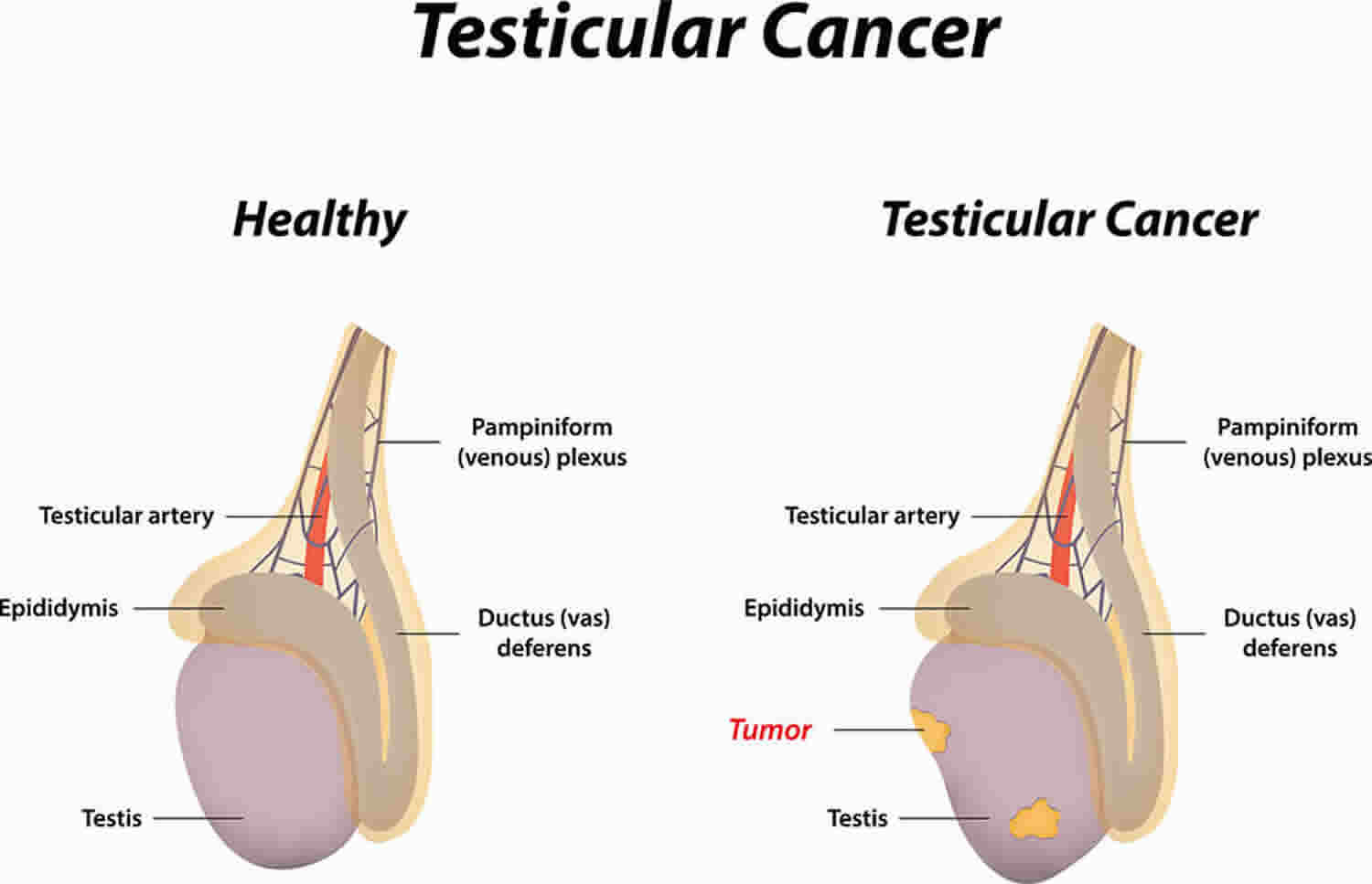
Embryonal carcinoma, also called nonseminomatous germ cell tumor, is a relatively aggressive (fast-growing) type of testicular cancer that originates from abnormal germ cells (cells that typically “germinate” into fully mature sperm), that often occurs in young to middle-aged men (men between their late teens and early 30s), and tends to grow rapidly and spread outside the testicle 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Germ cells within the testicles produce immature sperm that travel through a network of tubules (seminiferous tubules) and larger tubes into the epididymis (a long coiled tube next to the testicles) where the sperm mature and are stored (see Figure 3 below). Embryonal carcinomas are found in about 40% of testicular tumors, but pure embryonal carcinomas occur only 3% to 4% of the time. When seen under a microscope, embryonal carcinoma can look like tissues of very early embryos (fetus). This type of non-seminoma tends to grow rapidly and spread outside the testicle. Approximately 66% of patients with embryonal carcinoma are found to have metastasis at the time of diagnosis 5. Embryonal carcinomas tend to have an aggressive course due to their early tendency to invade other parts of the body 3, 7. Early diagnosis and treatment are, therefore, critical for a positive outcome 3.
Embryonal carcinoma is classified as a nonseminoma germ cell tumor, meaning it’s a type of testicular cancer that doesn’t fall under the seminoma category.
Embryonal carcinomas form when germ cells (cells that typically “germinate” into fully mature sperm) multiply out of control. Eventually, the cells form a mass, or tumor. These tumors tend to grow fast and spread beyond your testicle. Scientists don’t know why these cells start behaving abnormally in the first place. But they believe the abnormal germ cells form early, during embryonic development.
Embryonal carcinoma can increase blood levels of a tumor marker protein called alpha-fetoprotein (AFP), as well as human chorionic gonadotropin (hCG).
The most common treatments for embryonal carcinoma include surgery to remove the cancer and chemotherapy. Your treatment plan depends on lots of factors. These include your cancer stage, overall health and treatment preferences. Specific treatments include:
- Radical inguinal orchiectomy: Your doctor will remove the affected testicle. Your doctor will seal nearby blood vessels and lymph tissue to prevent the possibility of the cancer spreading.
- Retroperitoneal lymph node dissection (RPLND): Your doctor may remove the lymph nodes in the back of your abdomen (retroperitoneal lymph node) if embryonal carcinoma has spread there or if there’s a chance of spread.
- Chemotherapy: Embryonal carcinoma usually responds well to chemotherapy. Chemotherapy treatment uses drugs to kill cancer cells. You may need chemotherapy after surgery to kill any remaining cancer cells. Sometimes, with advanced-stage embryonal carcinoma, doctors prescribe chemo before surgery.
While aggressive, embryonal carcinoma prognosis (outlook) is good if treated early before the cancer has spread. The biggest indicator of your prognosis (outlook) is the tumor stage. According to a recent study tracking embryonal carcinoma survival rates, over 98% of people treated for Stage 1 cancer were alive five years later. Around 80% with Stage 3 embryonal carcinoma were alive five years later.
Even if you respond well to treatment, your doctor will continue to monitor you in case the cancer returns. With embryonal carcinoma, there’s a 20% chance of recurrence if the cancer’s only in your testicle. The likelihood of recurrence increases to over 50% if the cancer is in your scrotum or lymph nodes.
How common is embryonal carcinoma?
Testicular cancer in all its forms, including germ cell tumors like embryonal carcinoma, is rare. Of all testicular cancer diagnoses, only 2% of germ cell tumors are pure embryonal carcinomas. But around 85% of all testicular mixed germ cell tumors contain embryonal carcinoma elements. Mixed germ cell tumors contain a mixture of non-seminoma tumor types.
In extremely rare cases, embryonal carcinoma can start in other organs, like your ovaries. Embryonal carcinoma that forms in the ovaries is a rare ovarian germ cell tumor. No matter where embryonal carcinoma starts, these tumors tend to grow and spread fast.
What are germ cell tumors?
Germ cell tumors develop in germ cells. Germ cells are cells in your body that develop into sperms in males and eggs in females. Germ cell tumors most often develop in the ovary or testicle because this is where most germ cells are. However, germ cells can sometimes be left behind in other parts of your body from when you developed in the womb. So germ cell tumors can develop anywhere in your body where there are germ cells.
Doctors use different names to describe the different types of germ cell tumors (GCTs). The name describes:
- whereabouts in the body it started – such as ovarian or testicular
- what the tumor looks like under the microscope
Some tumors are non cancerous (benign). And some are cancerous (malignant):
- Benign germ cell tumors include mature teratomas.
- Malignant germ cell tumors are split into 2 main groups:
- Seminoma germ cell tumors (in females these are called dysgerminomas). Seminomas are sometimes called pure seminomas. They only contain one type of cell. Some germ cell tumor contain both seminoma cells and non seminoma cells. Doctors usually class and treat these as non seminoma tumors.
- Non-seminoma germ cell tumors (in females these are called non dysgerminomas). Some non-seminomas develop from just one type of cell. And some develop from a mixture of cell types. So, for example, a tumor can contain a mix of some teratoma cells and some embryonal carcinoma cells.
- Malignant non-seminoma tumors include:
- immature teratomas
- yolk sac tumors
- choriocarcinomas
- embryonal carcinomas
- Malignant non-seminoma tumors include:
Germ cell tumors (GCTs) can start in the:
- testicles
- ovaries
- chest (mediastinal germ cell tumors)
- back of the tummy (retroperitoneal germ cell tumor)
- brain (pineal region tumor)
- lower spine (sacrococcygeal germ cell tumor)
Germ cell tumors that grow outside the ovary or testicle are called extragonadal germ cell tumors (EGGCTs) and they are very rare. “Extragonadal” means outside of the gonads (sex organs). Extragonadal germ cell tumors (EGGCTs) may begin to grow anywhere in your body but usually begin in organs such as the pineal gland in your brain, in the mediastinum (area between the lungs), or in the retroperitoneum (the back wall of the abdomen). Extragonadal germ cell tumors (EGGCTs) can be benign (noncancer) or malignant (cancer). Benign extragonadal germ cell tumors are called benign teratomas. These are more common than malignant extragonadal germ cell tumors and often are very large.
Malignant extragonadal germ cell tumors are divided into two types, nonseminoma and seminoma. Nonseminomas tend to grow and spread more quickly than seminomas. They usually are large and cause signs and symptoms. If untreated, malignant extragonadal germ cell tumors may spread to the lungs, lymph nodes, bones, liver, or other parts of the body.
The main treatments are surgery and chemotherapy. Your treatment depends on your type of germ cell tumor and whereabouts it is in your body.
Testis anatomy
The testes or testicles (a single testicle is called a testis), are paired oval glands in the scrotum measuring about 5 cm (2 inch) long and 2.5 cm (1 inch) in diameter. Testicles are part of the male reproductive system. Each testis (singular) has a mass of 10–15 grams. The 2 oval glands are each normally a little smaller than a golf ball in adult males. They’re held within a sac of skin called the scrotum. The scrotum hangs under the base of the penis.
Testicles have 2 main functions:
- They make male hormones (androgens) such as testosterone.
- They make sperm, the male cells needed to fertilize a female egg cell to start a pregnancy.
The testes develop near the kidneys, in the posterior portion of the abdomen and they usually begin their descent into the scrotum through the inguinal canals (passageways in the lower anterior abdominal wall) during the latter half of the seventh month of fetal development.
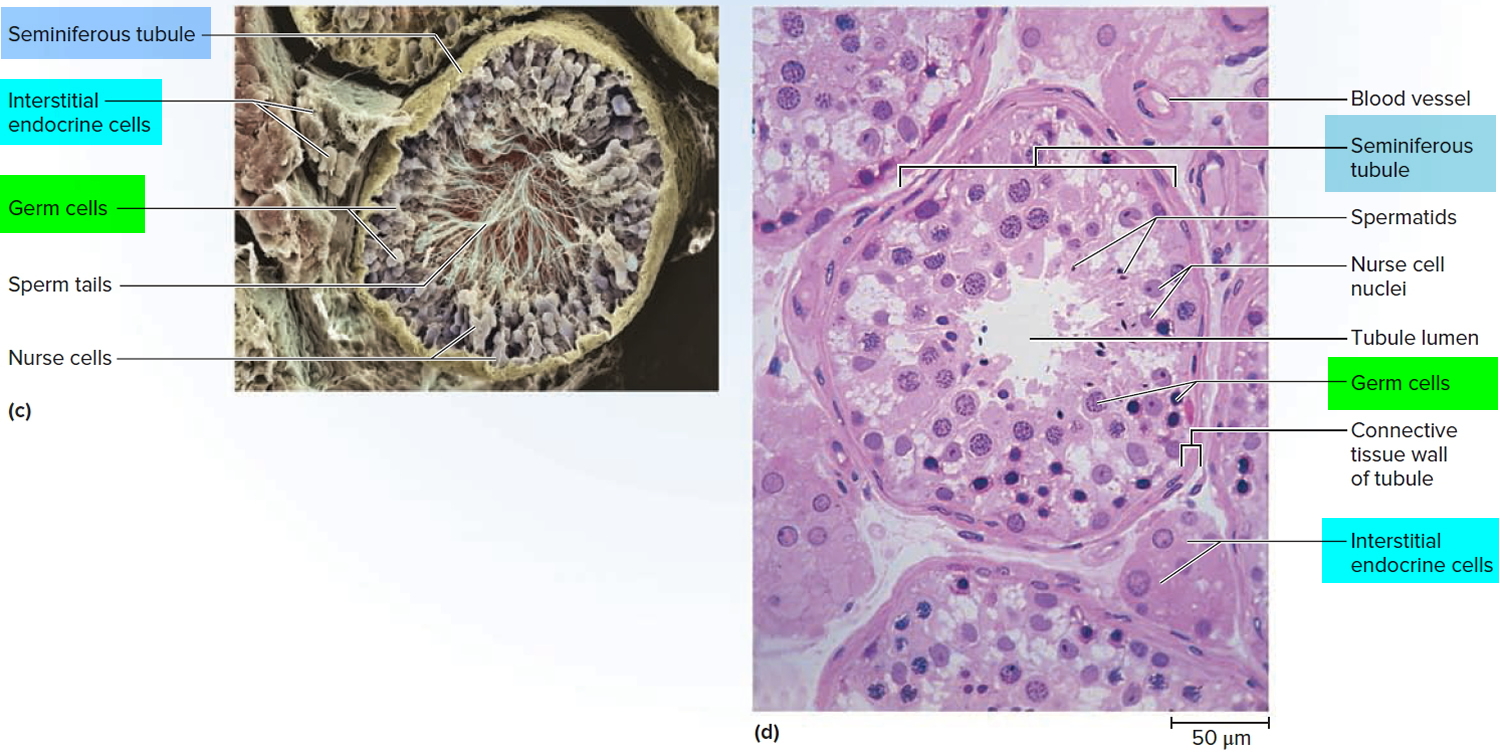
A serous membrane called the tunica vaginalis, which is derived from the peritoneum and forms during the descent of the testes, partially covers the testes. A collection of serous fluid in the tunica vaginalis is called a hydrocele. It may be caused by injury to the testes or inflammation of the epididymis. Usually, no treatment is required. Internal to the tunica vaginalis the testis is surrounded by a white fibrous capsule composed of dense irregular connective tissue, the tunica albuginea; it extends inward, forming septa that divide the testis into a series of internal compartments called lobules. Each of the 200–300 lobules contains one to three tightly coiled tubules, the seminiferous tubules, where sperm are produced. The process by which the seminiferous tubules of the testes produce sperm is called spermatogenesis.
The seminiferous tubules contain two types of cells: spermatogenic cells, the sperm-forming cells, and sustentacular cells or Sertoli cells, which have several functions in supporting spermatogenesis. Stem cells called spermatogonia develop from primordial germ cells that arise from the yolk sac and enter the testes during the fifth week of development. In the embryonic testes, the primordial germ cells differentiate into spermatogonia, which remain dormant during childhood and actively begin producing sperm at puberty. Toward the lumen of the seminiferous tubule are layers of progressively more mature cells. In order of advancing maturity, these are primary spermatocytes, secondary spermatocytes, spermatids, and sperm cells. After a sperm cell, or spermatozoon, has formed, it is released into the lumen of the seminiferous tubule. Sperm cells are then stored in a small coiled tube behind each testicle called the epididymis. This is where they mature.
During ejaculation, sperm cells are carried from the epididymis through the vas deferens to seminal vesicles, where they mix with fluids made by the vesicles, prostate gland, and other glands to form semen. This fluid then enters the urethra, the tube in the center of the penis through which both urine and semen leave the body.
Embedded among the spermatogenic cells in the seminiferous tubules are large sustentacular cells or Sertoli cells, which extend from the basement membrane to the lumen of the tubule. Internal to the basement membrane and spermatogonia, tight junctions join neighboring sustentacular cells to one another. These junctions form an obstruction known as the blood–testis barrier because substances must first pass through the sustentacular cells before they can reach the developing sperm. By isolating the developing gametes from the blood, the blood–testis barrier prevents an immune response against the spermatogenic cell’s surface antigens, which are recognized as “foreign” by the immune system. The blood–testis barrier does not include spermatogonia.
Sustentacular cells (Sertoli cells) support and protect developing spermatogenic cells in several ways. They nourish spermatocytes, spermatids, and sperm; phagocytize excess spermatid cytoplasm as development proceeds; and control movements of spermatogenic cells and the release of sperm into the lumen of the seminiferous tubule. They also produce fluid for sperm transport, secrete the hormone inhibin, and regulate the effects of testosterone and FSH (follicle-stimulating hormone).
In the spaces between adjacent seminiferous tubules are clusters of cells called interstitial cells or Leydig cells. These cells secrete testosterone, the most prevalent androgen. An androgen is a hormone that promotes the development of masculine characteristics. Testosterone also promotes a man’s libido (sexual drive).
The scrotum (bag), the supporting structure for the testes, consists of loose skin and underlying subcutaneous layer that hangs from the root (attached portion) of the penis. Externally, the scrotum looks like a single pouch of skin separated into lateral portions by a median ridge called the raphe. Internally, the scrotal septum divides the scrotum into two compartments, each containing a single testis. The location of the scrotum and the contraction of its muscle fibers regulate the temperature of the testes. Normal sperm production requires a temperature about 2–3°C below core body temperature. This lowered temperature is maintained within the scrotum because it is outside the pelvic cavity. In response to cold temperatures, the cremaster and dartos muscles contract. Contraction of the cremaster muscles moves the testes closer to the body, where they can absorb body heat. Contraction of the dartos muscle causes the scrotum to become tight (wrinkled in appearance), which reduces heat loss. Exposure to warmth reverses these actions.
Figure 1. Male reproductive system
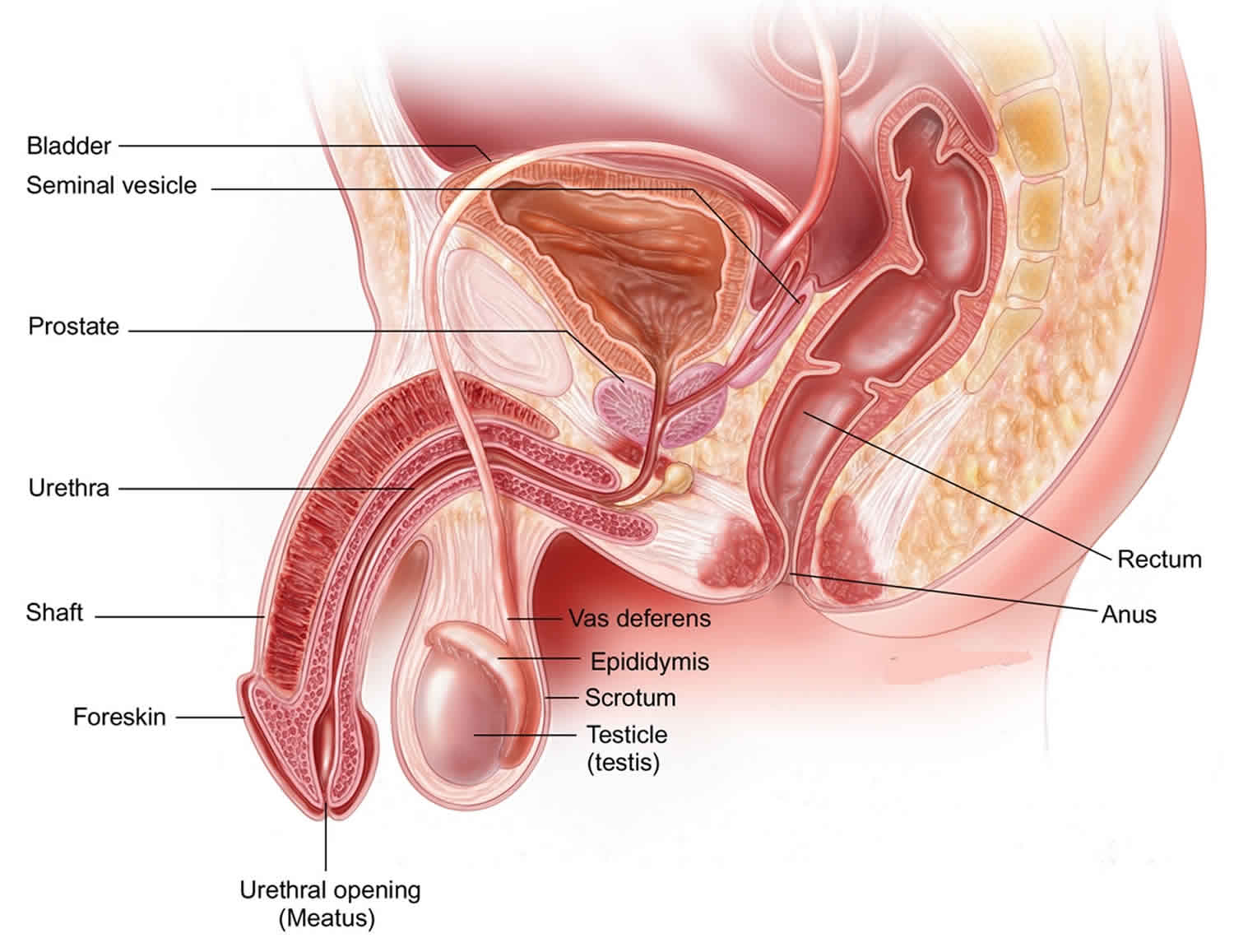
Figure 2. Testicle anatomy
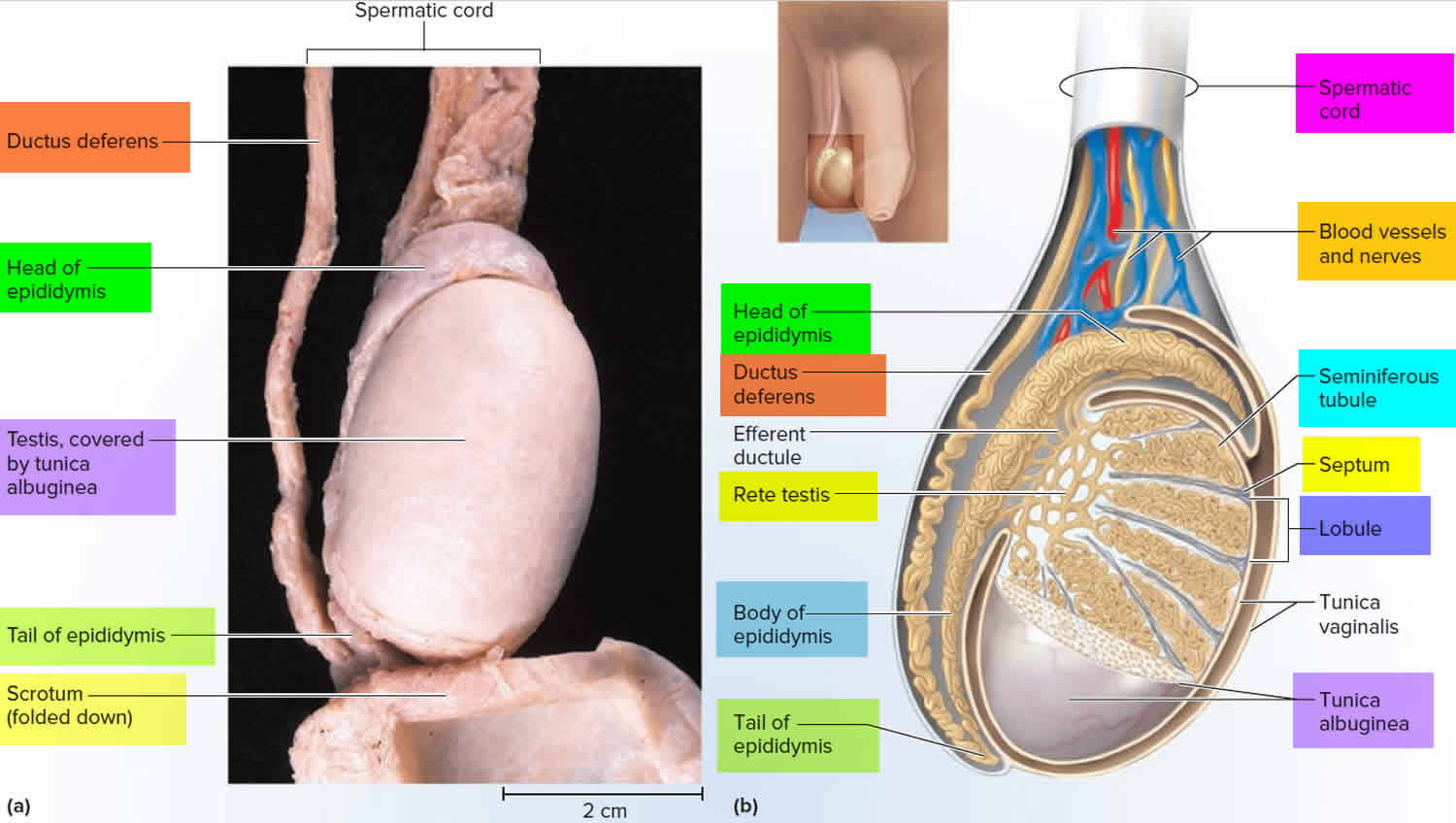
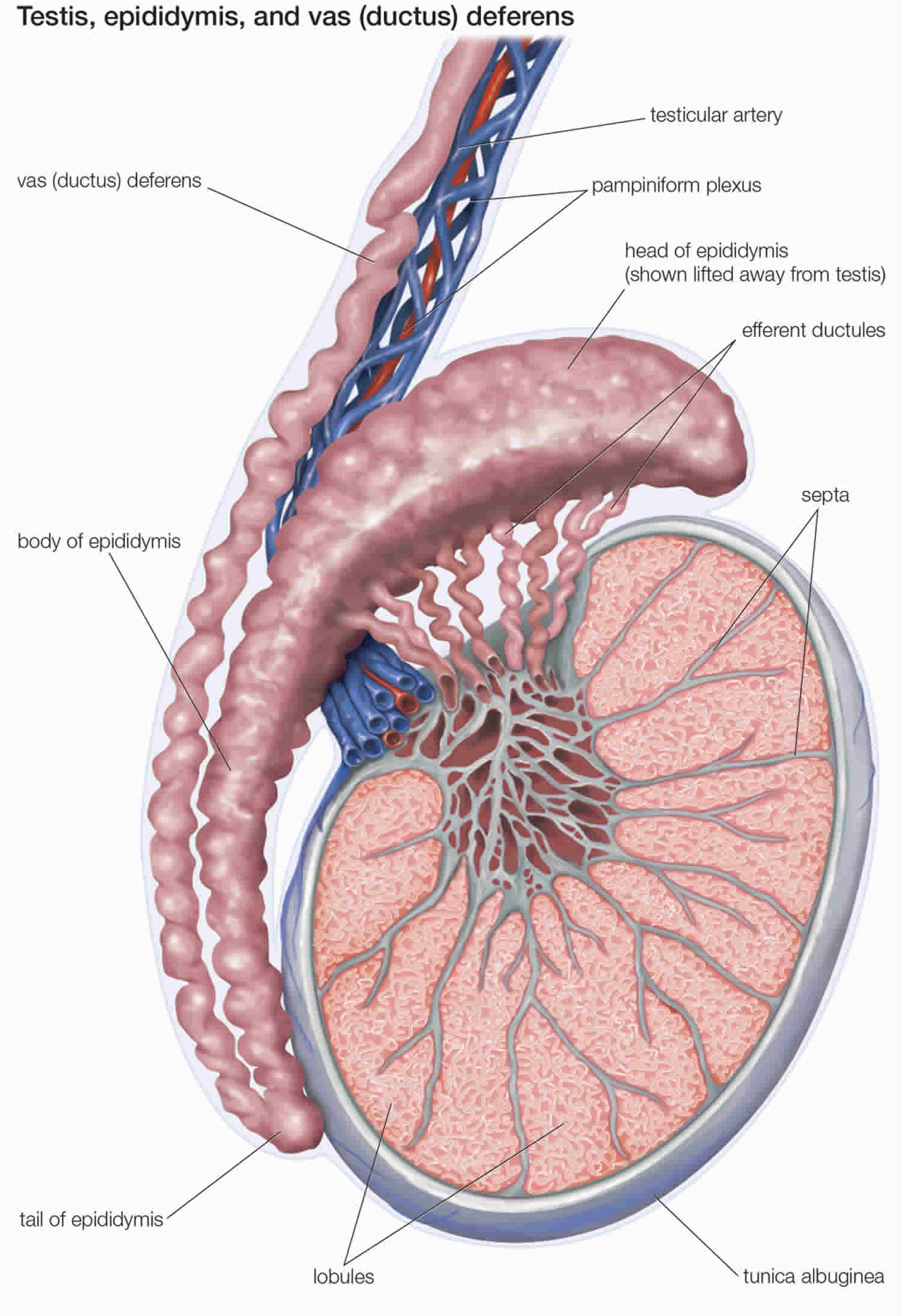
Figure 3. Scanning electron micrograph of the seminiferous tubules
Embryonal carcinoma causes
Scientists aren’t sure what causes embryonal carcinoma. Normal germ cells form in a developing human embryo. These cells eventually travel to the embryo’s ovaries or testicles, becoming egg cells or sperm cells. In contrast, germ cell tumors consist of cells that don’t develop into fully formed eggs or sperm. The germ cells divide abnormally and become a tumor in your ovaries or testicles instead. In the case of extragonadal tumors, the germ cells travel to odd places in your body — like your chest, brain, belly, low back and tailbone — to form tumors.
Factors that may increase a man’s risk of developing testicular cancer are:
- Abnormal testicle development
- History of an undescended testicle (one or both testicles fail to move into the scrotum before birth)
- Exposure to certain chemicals
- Family history of testicular cancer
- HIV infection
- History of testicular cancer
- Klinefelter syndrome
- Infertility
- Tobacco use
- Down syndrome
Testicular cancer is the most common cancer in young and middle-aged men. It can also occur in older men, and in rare cases, in younger boys.
White men are more likely than African American and Asian American men to develop this type of cancer.
There is no evidence linking testicular cancer to a vasectomy.
Risk factor for embryonal carcinoma
Anything that increases a person’s chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop embryonal carcinoma and it will develop in people who don’t have any known risk factors. Talk with your doctor if you think you may be at risk. Risk factors for embryonal carcinoma include 12, 9, 13:
- Age: Most men are diagnosed between the age 25 and 35.
- Race: Testicular germ cell tumors are more common among White, American Indian, and Alaska Native men are several times more likely to get testicular cancer than Black, Asian American, and Pacific Islander men. The reason for this is not known.
- Family history: Having a family history of testicular cancer (especially in a father or brother). Your risk may be greater if a close biological relative also has a germ cell tumor.
- Undescended testicle (cryptorchidism): Undescended testicle or cryptorchidism means that one or both testicles fail to move from the abdomen (belly) into the scrotum before birth. Males with cryptorchidism are many times more likely to get testicular cancer than those with normally descended testicles.
- Hereditary syndromes: Some conditions that run in families can raise the risk of embryonal tumor. Examples include Fanconi anemia, Li-Fraumeni syndrome, nevoid basal cell carcinoma syndrome, Rubinstein-Taybi syndrome and Turcot syndrome.
Embryonal carcinoma prevention
There’s no way to prevent testicular cancer. If you get testicular cancer, there’s nothing you could have done to prevent it.
Testicular cancer screening
Some doctors recommend regular testicle self-exams. During a testicular self-exam you feel your testicles for any lumps or other changes. If you notice any changes that last longer than two weeks, make an appointment with your doctor.
Not all doctors agree with this recommendation. There’s no research to show that self-exams can lower the risk of dying of testicular cancer. Even when it is found at a late stage, testicular cancer is likely to be cured.
Embryonal carcinoma symptoms
These and other signs and symptoms may be caused by testicular cancer or by other conditions. Check with your doctor if you have any of the following.
Symptoms of embryonal carcinoma include:
- A swollen testicle.
- A painful or painless mass or lump in your testicle.
- A change in how your testicle feels.
- Heaviness or discomfort in a testicle or in your scrotum.
- A dull ache in the lower abdomen or the groin.
- A sudden build-up of fluid in the scrotum.
Other symptoms may be signs that the testicular cancer has spread beyond your testicle. These include:
- Low back pain.
- Flank pain (pain in the side of your body between your upper belly and back).
- Shortness of breath (dyspnea).
- Cough or coughing up blood (hemoptysis).
Embryonal carcinoma diagnosis
You might find lumps, swelling or other symptoms of testicular cancer on your own. Your doctor will ask about your symptoms and medical history. Your doctor will perform a physical exam to check for lumps in your testicle and swelling in the lymph nodes in your abdomen. Swollen lymph nodes may be a sign of cancer spread.
Tests used to diagnose embryonal carcinoma include:
- Ultrasound: Usually, the first imaging test you’ll need is an ultrasound of both testicles. A testicular ultrasound test uses sound waves to make pictures. It can be used to make pictures of the scrotum and testicles. During an ultrasound you lie on your back with your legs spread. A health care provider puts a clear gel on the scrotum. A hand-held probe is moved over the scrotum to make the pictures. Ultrasound gives your doctor more clues about any lumps around your testicle. It can help your doctor see whether the lumps look like something that isn’t cancer or if they look like cancer. An ultrasound shows whether the lumps are inside or outside your testicle. Lumps inside the testicle are more likely to be testicular cancer. If an ultrasound reveals signs of a tumor, you may need additional imaging tests to check for cancer spread. Tests may include a CT scan (computed tomography scan), an X-ray or an MRI (magnetic resonance imaging).
- Serum tumor marker tests: Your doctor will check your blood for signs of certain tumor markers linked to testicular cancer. These include alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG) and lactate dehydrogenase (LDH). They’re sometimes present with embryonal carcinoma — but not always.
- Beta human chorionic gonadotropin (β-HCG) is produced by embryonal carcinoma and choriocarcinoma and is the most commonly elevated tumor marker in patients with nonseminomatous germ cell tumors. Beta-hCG is also elevated in 15% to 25% of patients with seminomas 14.
- Alpha fetoprotein (AFP) is absent in the serum of normal adults but is detectable in patients with nonseminomatous germ cell tumors and hepatocellular carcinoma. Alpha fetoprotein (AFP) is not elevated in patients with pure seminomas 14.
- Lactate dehydrogenase (LDH) is a less sensitive and less specific tumor marker than beta-hCG or AFP for men with nonseminomatous germ cell tumors (NSGCTs) but is elevated in 40% to 60% of men with testicular germ cell tumors 14.
- Inguinal orchiectomy (surgery to remove a testicle): If your doctor thinks a lump on your testicle may be cancerous, you might have surgery to remove your testicle. The testicle is sent to a lab for testing. The tests can show whether it’s cancerous. A doctor will need to examine the tumor cells beneath a microscope to confirm that it’s embryonal carcinoma. With testicular cancer, removing just a sample of tissue (as is usually the case in a biopsy) puts you at risk of the cancer cells spreading.
- The majority of germ cell tumors can be accurately diagnosed using light microscopy after a thorough evaluation of the morphological features that include cells with large, pleomorphic nuclei with one or more large nucleoli, dense cytoplasm that is amphophilic, poorly defined cytoplasmic membranes, numerous mitotic figures, and frequent apoptotic bodies 15. However, in some cases, additional immunohistochemical studies may be necessary, particularly if the tumor sample is poorly fixed. The most helpful markers for identifying EC are CD30 and OCT4, although OCT4 alone does not differentiate between embryonal carcinoma and seminoma, unlike CD30 16.
Determining the type of cancer
Tests on your cancer cells give your health care team information about the type of testicular cancer that you have. Your care team considers your cancer type when deciding on your treatment.
The most common types of testicular cancer include:
- Seminoma. Seminoma testicular cancers tend to happen at an older age. Seminomas often grow and spread more slowly than nonseminomas.
- Nonseminoma. Nonseminoma testicular cancers tend to happen earlier in life. They grow and spread quickly. Several types of nonseminomas exist. They include choriocarcinoma, embryonal carcinoma, teratoma and yolk sac tumor.
Other types of testicular cancer exist, but they are very rare.
Embryonal carcinoma pathology
Grossly, embryonal carcinoma is a tan to a yellow tumor that often exhibits large areas of hemorrhage and necrosis. Embryonal carcinoma is usually poorly circumscribed with a variegated, soft cut surface. Embryonal carcinoma consists of undifferentiated malignant cells resembling primitive epithelial cells from early-stage embryos with crowded pleomorphic nuclei 17.
The microscopic appearance of embryonal carcinomas varies considerably as they may grow in solid sheets or papillary, glandular-alveolar, or tubular patterns. Embryonal carcinoma commonly shows 3 growth patterns: solid, glandular, and tubulopapillary (Figure 4).
Figure 4. Embryonal carcinoma histologic features
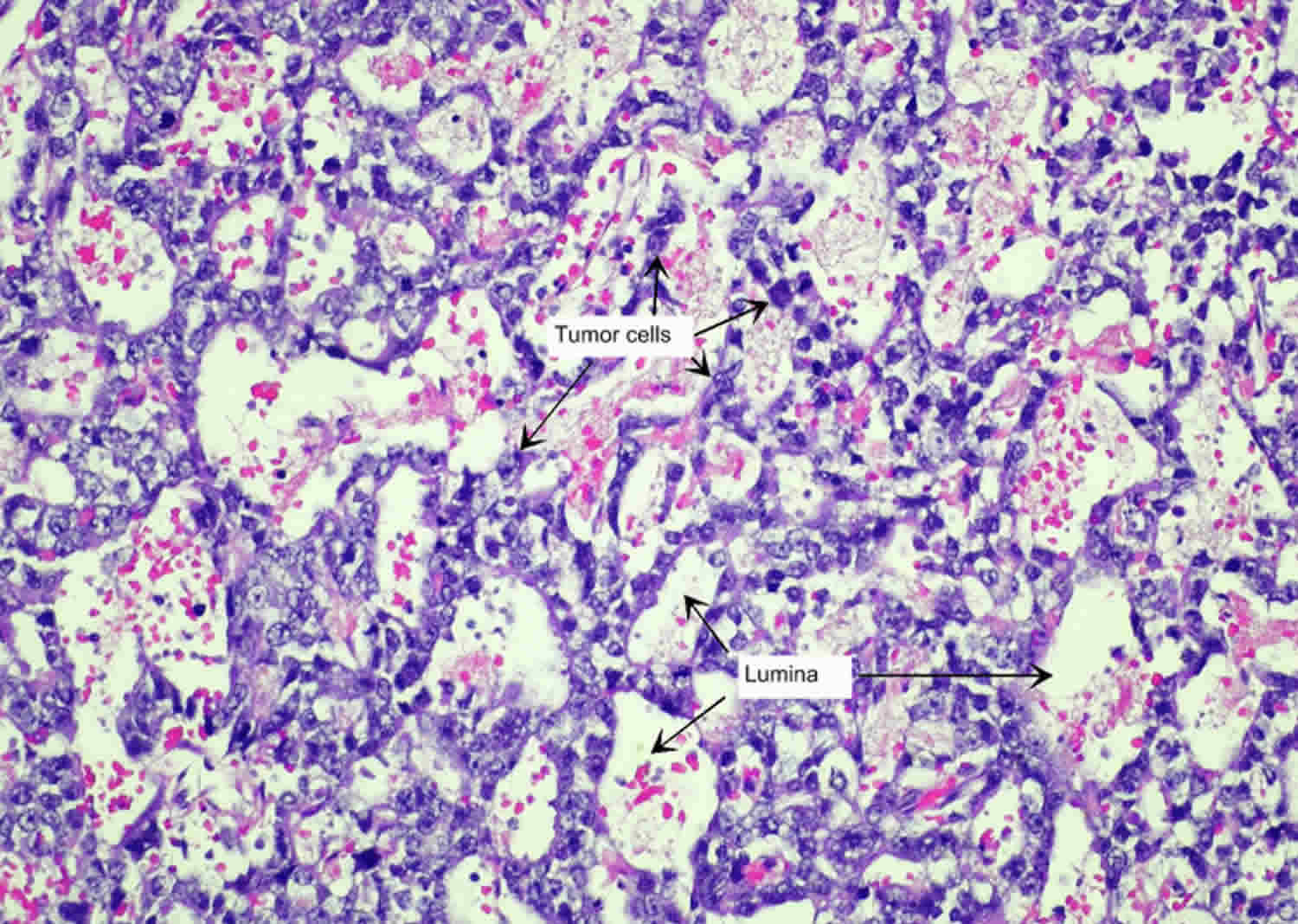
Footnotes: Histologic features of embryonal carcinoma. Embryonal carcinomas are composed of primitive, anaplastic cells. The image shows tubular/glandular pattern in which cuboidal to columnar cells form gland-like or tubule-like structures. The enclosed lumina are cleft-like or round (×400).
[Source 18 ]Staging embryonal carcinoma of testis
Once your doctor confirms your diagnosis, the next step is to see whether the cancer has spread beyond the testicle and if so, how far. This is called the cancer’s stage or staging. Cancer stage is the best predictor of your prognosis (outlook) how likely your cancer is to be cured. Doctors also use a cancer’s stage when talking about survival statistics. Early-stage embryonal carcinoma is often curable. But it spreads so fast that up to 40% of cancers have already metastasized (spread to distant parts of your body) by the time your doctor diagnose them.
Tests for staging testicular cancer include:
- Computerized tomography (CT) scan. CT scans take a series of X-ray pictures of your belly, chest and pelvis. A health care provider checks the pictures for signs that cancer has spread.
- Serum tumor marker tests. These include alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG) and lactate dehydrogenase (LDH). Tumor marker tests are often repeated after surgery to remove the testicle. The results help your doctor decide whether you might need additional treatments to kill the cancer cells. Tumor marker tests might be used during and after cancer treatment to monitor your condition.
The earliest stage of testicular cancer is stage 0 (zero) also called germ cell neoplasia in situ (GCNIS) 19. The other stage groupings range from 1 (I) through 3 (III). There is no stage 4 (IV) testicular cancer 19. Some stages are split further to cover more details, using capital letters (A, B, etc.) 19.
As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage 3 (III), means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
The staging system most often used for testicular cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 4 key pieces of information 19:
- The size and extent of the main tumor (T): How large is the tumor? Has it grown into nearby structures or organs?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes ? How many, and how big are they? The lymphatic invasion has been identified as a significant contributor to the spread of metastases in embryonal carcinomas, affecting mainly the retro-peritoneal para-aortic nodes and then moving on to mediastinal and supraclavicular nodes 10, 11.
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant parts of the body? Embryonal carcinoma usually spreads to the lungs, but it may also spread to your liver, brain, and bones 2.
- The serum (blood) levels of tumor markers (S): Are any tumor marker levels higher than normal? This includes alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG) and lactate dehydrogenase (LDH).
Numbers or letters after T, N, M, and S provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, M, and S categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The system described below is the most recent AJCC system, effective as of January 2018. It’s used for germ cell tumors (seminomas and non-seminomas) that occur after puberty, and for sex cord stromal tumors (Leydig cell tumors and Sertoli cell tumors) 19.
Testicular cancer might be given a clinical T category (written as cT) based on the results of a physical exam, biopsy, and imaging tests. Once surgery is done, the pathologic T category (written as pT) is determined by examining tissue removed during the operation.
Testicular cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Stages of testicular cancer
| American Joint Committee on Cancer (AJCC) Stage | Stage grouping | Stage description* |
|---|---|---|
| 0 | pTis N0 M0 S0 | The cancer is only in the seminiferous tubules (small tubes inside each testicle). It has not grown into other parts of the testicle (pTis). It hasn’t spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| 1 | pT1-pT4 N0 M0 SX | The tumor has grown beyond the seminiferous tubules, and might have grown outside the testicle and into nearby structures (pT1-pT4). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| 1A | pT1 N0 M0 S0 | The tumor has grown beyond the seminiferous tubules, but is still within the testicle, and it hasn’t grown into nearby blood vessels or lymph nodes (pT1). The cancer hasn’t spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| 1B | pT2-pT4 N0 M0 S0 | The tumor has grown outside of the testicle and into nearby structures (pT2-pT4). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). All tumor marker levels are within normal limits (S0). |
| 1S | Any pT (or TX) N0 M0 S1-S3 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). At least one tumor marker level is higher than normal (S1-S3). |
| 2 | Any pT (or TX) N1-N3 M0 SX | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to 1 or more nearby lymph nodes (N1-N3), but it hasn’t spread to distant parts of the body (M0). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| 2A | Any pT (or TX) N1 M0 S0 or S1 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least 1 nearby lymph node (but no more than 5, if checked by surgery), and none of the lymph nodes are larger than 2 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least 1 tumor marker level is slightly higher than normal (S1). |
| 2B | Any pT (or TX) N2 M0 S0 or S1 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least 1 nearby lymph node that’s larger than 2 cm but no larger than 5 cm across, OR it has grown outside of a lymph node, OR more than 5 nodes contain cancer (found during surgery) (N2). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least 1 tumor marker level is slightly higher than normal (S1). |
| 2C | Any pT (or TX) N3 M0 S0 or S1 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to at least 1 nearby lymph node that’s larger than 5 cm across (N3). The cancer has not spread to distant parts of the body (M0). All tumor marker levels are within normal limits (S0), or at least 1 tumor marker level is slightly higher than normal (S1). |
| 3 | Any pT (or TX) Any N M1 SX | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant parts of the body (M1). Tumor marker test results aren’t available, or the tests haven’t been done (SX). |
| 3A | Any pT (or TX) Any N M1a S0 or S1 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). All tumor marker levels are within normal limits (S0), or at least 1 tumor marker level is slightly higher than normal (S1). |
| 3B | Any pT (or TX) N1-N3 M0 S2 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to 1 or more nearby lymph nodes (N1-N3), but it hasn’t spread to distant parts of the body (M0). At least 1 tumor marker level is much higher than normal (S2). |
| OR | ||
| Any pT (or TX) Any N M1a S2 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). At least 1 tumor marker level is much higher than normal (S2). | |
| 3C | Any pT (or TX) N1-N3 M0 S3 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer has spread to 1 or more nearby lymph nodes (N1-N3), but it hasn’t spread to distant parts of the body (M0). At least 1 tumor marker level is very high (S3). |
| OR | ||
| Any pT (or TX) Any N M1a S3 | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes or to the lungs (M1a). At least 1 tumor marker level is very high (S3). | |
| OR | ||
| Any pT (or TX) Any N M1b Any S | The tumor might or might not have grown outside the testicle (any pT), or the extent of the tumor can’t be assessed for some reason (TX). The cancer might or might not have spread to nearby lymph nodes (any N). It has spread to distant parts of the body other than the lymph nodes or to the lungs (M1b). Tumor marker levels might or might not be higher than normal (any S). | |
Footnotes: * The following additional category is not listed on the table above; NX = Nearby lymph nodes cannot be assessed due to lack of information.
[Source 19 ]Embryonal carcinoma treatment
The most common treatments for embryonal carcinoma include surgery to remove the cancer and chemotherapy. Your treatment plan depends on lots of factors. These include your cancer stage, overall health and treatment preferences. Specific treatments include:
- Radical inguinal orchiectomy: Your doctor will remove the affected testicle. Your doctor will seal nearby blood vessels and lymph tissue to prevent the possibility of the cancer spreading.
- Retroperitoneal lymph node dissection (RPLND): Your doctor may remove the lymph nodes in the back of your abdomen (retroperitoneal lymph node) if embryonal carcinoma has spread there or if there’s a chance of spread.
- Chemotherapy: Embryonal carcinoma usually responds well to chemotherapy. Chemotherapy treatment uses drugs to kill cancer cells. You may need chemotherapy after surgery to kill any remaining cancer cells. Sometimes, with advanced-stage embryonal carcinoma, doctors prescribe chemo before surgery.
Radical inguinal orchiectomy
All testicular cancers are typically treated with this surgery, even those that have spread. Surgery to remove a testicle with cancer is called a radical inguinal orchiectomy. An incision (cut) is made just above the pubic area, and the testicle is gently removed from the scrotum through the opening. The surgeon then removes the entire tumor along with the testicle and spermatic cord. The spermatic cord contains part of the vas deferens, as well as blood and lymph vessels that could act as pathways for testicular cancer to spread to the rest of the body. To lessen the chance of this, these vessels are tied off early in the operation.
Effects of orchiectomy
Losing one testicle usually has no effect on a man’s ability to get an erection and have sex. But if both testicles are removed, sperm cannot be made and a man becomes infertile. Also, without testicles, a man cannot make enough testosterone, which can decrease sex drive and affect his ability to have erections. Other effects could include fatigue, hot flashes, and loss of muscle mass. These side effects can be avoided by taking testosterone supplements, either in a gel, a patch, or a shot. Pills are generally not reliable sources of testosterone.
Usually men with testicular cancer are young and may be concerned about changes in how they look. They may be dating and worry about a partner’s reaction, or they may be athletic and feel embarrassed by the missing testicle when in locker rooms.
To restore a more natural look, a man can have a testicular prosthesis surgically implanted in his scrotum. The prosthesis approved for use in the United States is filled with saline (salt water) and comes in different sizes to match the remaining testicle. When in place, it can look like a normal testicle. There can be a scar after the operation, but it’s often partly hidden by pubic hair. Some men might want a prosthesis, while others might not. You should discuss your wishes with your surgeon before surgery. It could also help to talk with someone who has a testicular prosthesis, to hear what it has been like for them.
Neo-adjuvant chemotherapy
Neoadjuvant chemotherapy involves administering chemotherapy before the primary cancer treatment, like surgery, with the goal of shrinking tumors and potentially making surgery more effective or less extensive. Non-seminomatous germ cell tumors are the most sensitive testicular cancers to cisplatin-based chemotherapy. Patients with elevated alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG) and and lactic dehydrogenase (LDH) tumor markers are typically given 3-4 cycles of bleomycin, etoposide, and cisplatin (BEP) chemotherapy 1. After completion of chemotherapy, tumor markers are repeated to see the decline in values, along with a contrast-enhanced CT scan to evaluate for any residual mass. If a mass is present with normal tumor markers, this is considered an indication for retroperitoneal lymph node dissection (RPLND). In patients who developed pulmonary fibrosis or with a history of significant pre-existing pulmonary disease, bleomycin would be contraindicated. If the patient still has elevated tumor markers, second-line chemotherapy, including vincristine, ifosfamide, and cisplatin (VIP), should be considered 1. Other second and third-line agents include gemcitabine, etoposide, paclitaxel, and oxaliplatin. Chemotherapy causes azoospermia (absence of sperm from the fluid ejaculated during orgasm) in most patients for at least 2 to 3 years after treatment. Cisplatin and similar alkylating agents are the most injurious to spermatogenesis, with Sertoli cells being relatively sensitive but Leydig cells being relatively resistant. Sertoli cells are also very radiosensitive. Overall, fertility is reduced by an average of 30% after chemotherapy treatment for non-seminomatous germ cell tumors 20, 21, 22.
Other potential side effects of chemotherapy include peripheral neuropathy, renal failure, myelosuppression, loss of hearing, increased cardiovascular disorders, and hypogonadism.
Retroperitoneal lymph node dissection (RPLND)
A nerve-sparing retroperitoneal lymph node dissection (RPLND) that preserves ejaculation in virtually every patient has been described in clinical stage 1 patients and appears to be as effective as the standard retroperitoneal lymph node dissection (RPLND) 23, 24, 25. Surgery should be followed by monthly determination of serum markers and chest x-rays for the first year and every-other-month determinations for the second year 26.
Men undergoing retroperitoneal lymph node dissection (RPLND), who are found to have pathological stage 1 disease, have a roughly 10% risk of relapsing subsequently, whereas men with pathological stage 2 disease (i.e., those who are found to have lymph node metastases at retroperitoneal lymph node dissection) have as much as a 50% risk of relapse without further treatment 27. Two cycles of post-retroperitoneal lymph node dissection chemotherapy using either bleomycin, etoposide, and cisplatin (BEP) or etoposide plus cisplatin (EP) lowers the risk of relapse in men with pathological stage 2 disease to about 1% 28, 29. Most patients in studies of retroperitoneal lymph node dissection underwent the operation at a center of excellence with a urological surgeon who had performed hundreds of such operations. The ability of less-experienced urologists to achieve similar results is unknown.
In patients with pathological stage 1 disease after retroperitoneal lymph node dissection (RPLND), the presence of lymphatic or venous invasion or a predominance of embryonal carcinoma in the primary tumor appears to predict for relapse 30, 31, 32. In a large, Testicular Cancer Intergroup Study, the relapse rate among men with pathological stage 1 disease was 19% in those with vascular invasion versus 6% in those without vascular invasion. One study reported that the relapse rate for men with pathological stage 1 disease was 21.2% (18 of 85 men relapsed), if their tumors were predominantly embryonal carcinoma and 29% if there was a predominance of embryonal carcinoma plus lymphovascular invasion versus 3% (5 of 141 men relapsed), if there was not a predominance of embryonal carcinoma 30, 31.
Among pathological stage 2 patients, the relapse rate was 32% among men with embryonal carcinoma-predominant tumors compared with 15.6% in the other stage 2 patients. The risk of metastatic disease (i.e., either pathological stage 2 disease or relapsed pathological stage 1 disease) in men with tumors showing a predominance of embryonal carcinoma plus lymphovascular invasion was 62% compared with 16% in men with neither risk factor.
These data have shown that high-risk patients undergoing retroperitoneal lymph node dissection (RPLND) have a substantial risk of subsequently receiving chemotherapy. Data from one institution have shown that about one-half of men with stage 1 pure embryonal carcinoma undergoing retroperitoneal lymph node dissection (RPLND) will subsequently receive cisplatin-based chemotherapy 33.
Retroperitoneal dissection of lymph nodes (RPLND) is not helpful in the management of children, and potential morbidity of the surgery is not justified by the information obtained 34. In men who have undergone retroperitoneal lymph node dissection (RPLND), chemotherapy is employed immediately on first evidence of recurrence.
Effects of lymph node dissection
Surgery to remove retroperitoneal lymph nodes is a major operation. Serious complications are not common, but they can happen. About 5% to 10% of patients have short-term problems after surgery, such as infection or bowel obstruction (blockage). The standard approach for an retroperitoneal lymph node dissection (RPLND) requires a large incision in the abdomen, which will leave a scar and can take some time to heal. Your ability to get up and around after the operation will be limited for some time. This is less likely to be an issue if you have laparoscopic surgery, which uses smaller incisions.
This type of surgery does not cause impotence – a man can still have erections and sex. But it might damage some of the nerves that control ejaculation. If these nerves are damaged, when a man ejaculates, the semen doesn’t come out through the urethra to exit the body but rather goes backwards into the bladder. This is called retrograde ejaculation, and it can make it hard to father children.
To save the normal ejaculation function, surgeons have developed a type of retroperitoneal lymph node surgery called nerve-sparing surgery that’s very successful when done by experienced doctors. Testicular cancer often affects men at an age when they might be trying to have children. These men may wish to discuss nerve-sparing surgery with their doctors, as well as sperm banking (freezing and storing sperm cells obtained before treatment). Men with testicular cancer often have lower than normal sperm counts, which can sometimes make it hard to collect a good sperm sample.
Treatment Options by Stage
Stage 1 non-seminoma germ cell tumors
Nearly all of these cancers can be cured, but the treatment is different from that of seminomas. As with seminomas, the initial treatment is surgery to remove the testicle and tumor (called radical inguinal orchiectomy). The other treatment choices will depend on the stage.
Choices for stage 1A (T1)
- Careful observation (surveillance): Surveillance is preferred by most experts, but it requires a lot of doctor visits and tests. A typical schedule might include visits every 2 months for the first year, with CT scans every 4 to 6 months; then every 3 months for the second year, with scans every 6 to 12 months. As time goes on and you have no problems, the time between visits and tests gets longer. If the cancer does come back (relapse), it’s usually within the first year or two. Relapses are generally treated with chemo. Even though more patients will have a relapse with surveillance than with lymph node dissection, the cure rates are much the same because the relapses are usually found early.
- Retroperitoneal lymph node dissection (RPLND): Having the lymph nodes at the back of the abdomen (belly) removed has the advantage of a high initial cure rate, but the disadvantages of major surgery with its possible complications, including losing the ability to ejaculate normally. After RPLND, if cancer is found in the nodes, chemo may be recommended.
- Chemotherapy: Instead of surgery, the doctor may suggest 1 cycle of the BEP regimen (bleomycin, etoposide, and cisplatin). This helps reduce the risk of relapse.
Choices for stage 1B (T2, T3, or T4)
- Retroperitoneal lymph node dissection (RPLND): This is surgery to remove the lymph nodes at the back of the abdomen (belly). If cancer is found in the lymph nodes, chemo is often recommended depending on the number of nodes with cancer in them. (See below.)
- Chemotherapy: Instead of surgery, the doctor may recommend 1 cycle of the BEP regimen (bleomycin, etoposide, and cisplatin). This can help reduce the risk that the cancer will come back. If cancer was found in the lymph nodes after surgery, 2 to 4 cycles of BEP or EP (etoposide and cisplatin) may be given, depending on how many nodes had cancer in them. This has a high cure rate, but it can have side effects (which are mostly short-term).
- Careful observation (surveillance): This requires frequent doctor visits and tests for several years. This may be an option for some T2 tumors that haven’t reached blood vessels.
Stage 1S non-seminoma germ cell tumors
If your tumor marker levels (like AFP or HCG) are still high even after the cancer has been removed, but the CT scan doesn’t show a tumor, chemo is typically recommended. This may be either 3 cycles of BEP (bleomycin, etoposide, and cisplatin) or 4 cycles of EP (etoposide and cisplatin).
Stage 2 non-seminoma germ cell tumors
Surgery is done first to remove the testicle and spermatic cord (called a radical inguinal orchiectomy). After surgery, treatment choices depend on the details of the cancer.
Stage 2A non-seminoma germ cell tumors
Treatment depends on tumor marker levels after surgery and the extent of spread to the retroperitoneal lymph nodes. These are the lymph nodes at the back of the abdomen (belly).
If tumor marker levels are normal, there are 2 main options:
- Retroperitoneal lymph node dissection (RPLND): This is surgery to remove the lymph nodes at the back of the abdomen. If the lymph nodes that were removed contain cancer, chemo (typically for 2 cycles) might be given. If there’s no cancer in the nodes, the doctor will watch closely for signs that the cancer has come back.
- Chemotherapy: This would include either 4 cycles of EP (etoposide and cisplatin) or 3 cycles of BEP (bleomycin, etoposide, and cisplatin). Surgery might be done after this if there are signs there might still be cancer present.
If tumor markers are still higher than normal after the initial surgery, treatment is typically with chemo as listed above (EP or BEP)..
Stage 2B non-seminoma germ cell tumors
Treatment depends on tumor marker levels after surgery and the extent of spread to the lymph nodes at the back of the abdomen (belly). These are called the retroperitoneal lymph nodes.
If tumor marker levels are normal, the options are:
- Chemotherapy: Either 4 cycles of EP (etoposide and cisplatin) or 3 cycles of BEP (bleomycin, etoposide, and cisplatin) may be used. Surgery may then be done to take out all enlarged nodes if the tumor marker return to normal.
- Retroperitoneal lymph node dissection (RPLND): In few select cases, where the cancer has spread only to these lymph nodes, surgery may be done to take them out. Chemo may then be given after surgery.
If tumor markers are still higher than normal after the initial surgery, treatment is typically with chemo as listed above (EP or BEP).
Stage 3 non-seminoma germ cell tumors
Even though stage 3 cancers have spread by the time they are found, most of them can still be cured.
Stage 3 non-seminomas are treated with radical inguinal orchiectomy, followed by chemotherapy. Depending on the risk group the cancer falls into, this might be with:
- EP (etoposide and cisplatin) for 4 cycles
- BEP (bleomycin, etoposide, and cisplatin) for 3 or 4 cycles
- VIP (etoposide, ifosfamide, and cisplatin) for 4 cycles
If there’s a high suspicion that the cancer might be a testicular choriocarcinoma, chemo may be started without a biopsy or surgery to remove the testicle.
If the cancer has spread to the brain, surgery (if there are only 1 or 2 tumors in the brain), radiation therapy aimed at the brain, or both may also be used. If the tumors in the brain are not bleeding or causing symptoms, some doctors may choose to start the chemo first.
Once chemo is complete, the doctor looks for any cancer that’s left. If scans and tumor marker levels are normal, no further treatment may be needed.
Sometimes a few tumors might be left after treatment. These are most often in the lung or in the retroperitoneal lymph nodes. Further treatment at this point depends on the type of cancer:
- A stage 3 non-seminoma tumor that remains after treatment is usually removed surgically, which may result in a cure. If cancer is found in the tumors removed, you might need more chemo, maybe with different drugs. After this, surgery might be done to take out any tumors that remain.
If the cancer is resistant to chemo or has spread to many organs, the usual doses of chemo may not always be enough. The doctor might recommend high-dose chemo followed by a stem cell transplant. Enrolling in a clinical trial of a newer chemo regimen might be another good option.
Recurrent testicular cancer
If the cancer goes away with treatment and then comes back, it’s said to have recurred or relapsed. If this happens, it’s usually within the first 2 years after treatment. In general, if the cancer recurs, it’s probably best to get a second opinion from a center with extensive experience in treating relapsed testicular cancer before starting treatment.
Treatment of recurrent germ cell tumors depends on the initial treatment and where the cancer recurs. Cancer that comes back in the retroperitoneal lymph nodes can be treated by surgery to remove the nodes (RPLND) if the recurrence is small and if the only surgical treatment given before was orchiectomy. Depending on the results of the surgery, chemo may be recommended as well.
- If it looks as if cancer has recurred in a lot of the retroperitoneal lymph nodes or if the cancer has returned elsewhere, chemo is usually recommended. This may be followed by surgery.
- If a man’s cancer recurs after chemo or if treatment is no longer working, he will be treated with different chemo, which typically includes ifosfamide, cisplatin, and either etoposide, paclitaxel, or vinblastine.
The treatment of testicular cancer that has come back after chemo is not always as effective as doctors would like, so some doctors may advise high-dose chemo followed by a stem cell transplant. This may be a better option for some men with recurrent disease, rather than standard chemo. Clinical trials of newer treatments may also be good options.
Embryonal carcinoma prognosis
An international germ cell tumor prognostic (IGCC) classification has been developed based on a retrospective analysis of 5,202 patients with metastatic nonseminomatous and 660 patients with metastatic seminomatous germ cell tumors 35. All patients received treatment with cisplatin- or carboplatin-containing therapy as their first chemotherapy course. The prognostic classification, shown below, was agreed on in 1997 by all major clinical trial groups worldwide 35. It is used for reporting clinical trial results of patients with germ cell tumors.
A meta-analysis of treatment outcomes for patients with advanced nonseminoma suggested that 5-year survival rates have improved for those patients with a poor prognosis during the period of 1989 to 2004 36. In addition to improved therapy, the improvement in survival rates could be the result of publication bias, changes in patient selection in reported clinical trials, or more sensitive staging methods that could migrate less-advanced stages to more-advanced stage categories (i.e., stage migration).
Good Prognosis
Nonseminoma
- Testis/retroperitoneal primary, and
- No nonpulmonary visceral metastases, and
- Good markers–all of:
- Alpha-fetoprotein (AFP) less than 1,000 ng/mL, and
- Beta-human chorionic gonadotropin (beta-hCG) less than 5,000 IU/mL (1,000 ng/mL), and
- Lactate dehydrogenase (LDH) less than 1.5 × the upper limit of normal
A total of 56% to 61% of nonseminomas are good prognosis. The 5-year progression-free survival rate is 89%; the 5-year survival rate is 92%–94%.
Intermediate Prognosis
Nonseminoma
- Testis/retroperitoneal primary, and
- No nonpulmonary visceral metastases, and
- Intermediate markers–any of:
- Alpha-fetoprotein (AFP) 1,000 ng/mL or more and 10,000 ng/mL or less, or
- Beta-human chorionic gonadotropin (beta-hCG) 5,000 IU/L or more and 50,000 IU/L or less, or
- Lactate dehydrogenase (LDH) 1.5 or more × N* and less than 10 × N*
- *[Note: N indicates the upper limit of normal for the LDH assay.]
A total of 13% to 28% of nonseminomas are intermediate prognosis. The 5-year progression-free survival rate is 75%; the 5-year survival rate is 80%–83%.
Poor Prognosis
Nonseminoma
- Mediastinal primary, or
- Nonpulmonary visceral metastases, or
- For markers–any of:
- Alpha-fetoprotein (AFP) more than 10,000 ng/mL, or
- Beta-human chorionic gonadotropin (beta-hCG) more than 50,000 IU/mL (10,000 ng/mL), or
- Lactate dehydrogenase (LDH) more than 10 × the upper limit of normal
A total of 16% to 26% of nonseminomas are poor prognosis. The 5-year progression-free survival rate is 41%; the 5-year survival rate is 71%.
- Nauman M, Leslie SW. Nonseminomatous Testicular Tumors. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK568754[↩][↩][↩]
- Testicular embryonal carcinoma metastatic to the labial mucosa of the upper lip. Poulopoulos A, Antoniades K, Kiziridou A, et al. Oral oncology. 2001;37:397–399. doi: 10.1016/s1368-8375(00)00104-4[↩][↩]
- Pure embryonal carcinoma of the testis in an adult male patient: case report. Kucuk S, Kucuk IG, Mizrak B, et al. Public health, economics and management in medicine. 2021;26:30.[↩][↩][↩]
- An overview of testicular germ cell tumors. Bahrami A, Ro JY, Ayala AG. Arch Pathol Lab Med. 2007;131:1267–1280. doi: 10.5858/2007-131-1267-AOOTGC[↩]
- Testicular embryonal carcinoma presenting as chest wall subcutaneous mass. Khan L, Verma S, Singh P, Agarwal A. J Cytol. 2009;26:39–40. doi: 10.4103/0970-9371.54868[↩][↩]
- Combined embryonal cell carcinoma and granulomatous orchitis of the testis. Martin A, Anderson S. J Diagn Med Sonogr. 2019;35:413–417.[↩]
- Pure embryonal carcinoma of testis presenting with extensive metastasis. Jagtap SV, Bisht TT, Jagtap SS, et al. Int J Med Sci Public Health. 2015;4:145–147.[↩][↩]
- What Is Testicular Cancer? https://www.cancer.org/cancer/types/testicular-cancer/about/what-is-testicular-cancer.html[↩]
- Testicular Cancer Treatment (PDQ®)–Health Professional Version. https://www.cancer.gov/types/testicular/hp/testicular-treatment-pdq[↩][↩]
- Ayala AG, Ro JY. Testicular tumors: clinically relevant histological findings. Semin Urol Oncol. 1998 May;16(2):72-81.[↩][↩]
- Dunphy CH, Ayala AG, Swanson DA, Ro JY, Logothetis C. Clinical stage I nonseminomatous and mixed germ cell tumors of the testis. A clinicopathologic study of 93 patients on a surveillance protocol after orchiectomy alone. Cancer. 1988 Sep 15;62(6):1202-6. doi: 10.1002/1097-0142(19880915)62:6<1202::aid-cncr2820620627>3.0.co;2-s[↩][↩]
- Risk Factors for Testicular Cancer. https://www.cancer.org/cancer/types/testicular-cancer/causes-risks-prevention/risk-factors.html[↩]
- Lutke Holzik MF, Rapley EA, Hoekstra HJ, Sleijfer DT, Nolte IM, Sijmons RH. Genetic predisposition to testicular germ-cell tumours. Lancet Oncol. 2004 Jun;5(6):363-71. doi: 10.1016/S1470-2045(04)01493-7[↩]
- Gilligan TD, Seidenfeld J, Basch EM, Einhorn LH, Fancher T, Smith DC, Stephenson AJ, Vaughn DJ, Cosby R, Hayes DF; American Society of Clinical Oncology. American Society of Clinical Oncology Clinical Practice Guideline on uses of serum tumor markers in adult males with germ cell tumors. J Clin Oncol. 2010 Jul 10;28(20):3388-404. doi: 10.1200/JCO.2009.26.4481[↩][↩][↩]
- Apoptosis in spermatocytic and usual seminomas: a light microscopic and immunohistochemical study. Bishop EF, Badve S, Morimiya A, Saxena R, Ulbright TM. Mod Pathol. 2007;20:1036–1044. doi: 10.1038/modpathol.3800933[↩]
- Testicular embryonal carcinoma: a morphologic study of 180 cases highlighting unusual and unemphasized aspects. Kao CS, Ulbright TM, Young RH, Idrees MT. Am J Surg Pathol. 2014;38:689–697. doi: 10.1097/PAS.0000000000000171[↩]
- Williamson SR, Delahunt B, Magi-Galluzzi C, Algaba F, Egevad L, Ulbright TM, Tickoo SK, Srigley JR, Epstein JI, Berney DM; Members of the ISUP Testicular Tumour Panel. The World Health Organization 2016 classification of testicular germ cell tumours: a review and update from the International Society of Urological Pathology Testis Consultation Panel. Histopathology. 2017 Feb;70(3):335-346. doi: 10.1111/his.13102[↩]
- Wang L, Matloob A, Asiry S, Khader SN. Educational Case: Testicular Germ Cell Tumor: Clinical Presentation, Pathogenesis, and Diagnostic and Therapeutic Modalities. Acad Pathol. 2020 Dec 11;7:2374289520975173. doi: 10.1177/2374289520975173[↩]
- Testicular Cancer Stages. https://www.cancer.org/cancer/types/testicular-cancer/detection-diagnosis-staging/staging.html[↩][↩][↩][↩][↩][↩]
- Spermon JR, Kiemeney LA, Meuleman EJ, Ramos L, Wetzels AM, Witjes JA. Fertility in men with testicular germ cell tumors. Fertil Steril. 2003 Jun;79 Suppl 3:1543-9. doi: 10.1016/s0015-0282(03)00335-2[↩]
- Gandini L, Sgrò P, Lombardo F, Paoli D, Culasso F, Toselli L, Tsamatropoulos P, Lenzi A. Effect of chemo- or radiotherapy on sperm parameters of testicular cancer patients. Hum Reprod. 2006 Nov;21(11):2882-9. doi: 10.1093/humrep/del167[↩]
- Huyghe E, Matsuda T, Daudin M, Chevreau C, Bachaud JM, Plante P, Bujan L, Thonneau P. Fertility after testicular cancer treatments: results of a large multicenter study. Cancer. 2004 Feb 15;100(4):732-7. doi: 10.1002/cncr.11950[↩]
- Foster RS, McNulty A, Rubin LR, Bennett R, Rowland RG, Sledge GW, Bihrle R, Donohue JP. The fertility of patients with clinical stage I testis cancer managed by nerve sparing retroperitoneal lymph node dissection. J Urol. 1994 Oct;152(4):1139-42; discussion 1142-3. doi: 10.1016/s0022-5347(17)32523-5[↩]
- Donohue JP. Evolution of retroperitoneal lymphadenectomy (RPLND) in the management of non-seminomatous testicular cancer (NSGCT). Urol Oncol. 2003 Mar-Apr;21(2):129-32. doi: 10.1016/s1078-1439(02)00212-0[↩]
- Heidenreich A, Albers P, Hartmann M, Kliesch S, Kohrmann KU, Krege S, Lossin P, Weissbach L; German Testicular Cancer Study Group. Complications of primary nerve sparing retroperitoneal lymph node dissection for clinical stage I nonseminomatous germ cell tumors of the testis: experience of the German Testicular Cancer Study Group. J Urol. 2003 May;169(5):1710-4. doi: 10.1097/01.ju.0000060960.18092.54[↩]
- van As NJ, Gilbert DC, Money-Kyrle J, Bloomfield D, Beesley S, Dearnaley DP, Horwich A, Huddart RA. Evidence-based pragmatic guidelines for the follow-up of testicular cancer: optimising the detection of relapse. Br J Cancer. 2008 Jun 17;98(12):1894-902. doi: 10.1038/sj.bjc.6604280[↩]
- Williams SD, Stablein DM, Einhorn LH, Muggia FM, Weiss RB, Donohue JP, Paulson DF, Brunner KW, Jacobs EM, Spaulding JT, et al. Immediate adjuvant chemotherapy versus observation with treatment at relapse in pathological stage II testicular cancer. N Engl J Med. 1987 Dec 3;317(23):1433-8. doi: 10.1056/NEJM198712033172303[↩]
- Behnia M, Foster R, Einhorn LH, Donohue J, Nichols CR. Adjuvant bleomycin, etoposide and cisplatin in pathological stage II non-seminomatous testicular cancer. the Indiana University experience. Eur J Cancer. 2000 Mar;36(4):472-5. doi: 10.1016/s0959-8049(99)00316-0[↩]
- Kondagunta GV, Sheinfeld J, Mazumdar M, Mariani TV, Bajorin D, Bacik J, Bosl GJ, Motzer RJ. Relapse-free and overall survival in patients with pathologic stage II nonseminomatous germ cell cancer treated with etoposide and cisplatin adjuvant chemotherapy. J Clin Oncol. 2004 Feb 1;22(3):464-7. doi: 10.1200/JCO.2004.07.178[↩]
- Hermans BP, Sweeney CJ, Foster RS, Einhorn LE, Donohue JP. Risk of systemic metastases in clinical stage I nonseminoma germ cell testis tumor managed by retroperitoneal lymph node dissection. J Urol. 2000 Jun;163(6):1721-4.[↩][↩]
- Sweeney CJ, Hermans BP, Heilman DK, Foster RS, Donohue JP, Einhorn LH. Results and outcome of retroperitoneal lymph node dissection for clinical stage I embryonal carcinoma–predominant testis cancer. J Clin Oncol. 2000 Jan;18(2):358-62. doi: 10.1200/JCO.2000.18.2.358[↩][↩]
- Sesterhenn IA, Weiss RB, Mostofi FK, Stablein DM, Rowland RG, Falkson G, Rivkind SE, Vogelzang NJ. Prognosis and other clinical correlates of pathologic review in stage I and II testicular carcinoma: a report from the Testicular Cancer Intergroup Study. J Clin Oncol. 1992 Jan;10(1):69-78. doi: 10.1200/JCO.1992.10.1.69[↩]
- Stephenson AJ, Bosl GJ, Bajorin DF, Stasi J, Motzer RJ, Sheinfeld J. Retroperitoneal lymph node dissection in patients with low stage testicular cancer with embryonal carcinoma predominance and/or lymphovascular invasion. J Urol. 2005 Aug;174(2):557-60; discussion 560. doi: 10.1097/01.ju.0000165163.03805.37[↩]
- Huddart SN, Mann JR, Gornall P, Pearson D, Barrett A, Raafat F, Barnes JM, Wallendsus KR. The UK Children’s Cancer Study Group: testicular malignant germ cell tumours 1979-1988. J Pediatr Surg. 1990 Apr;25(4):406-10. doi: 10.1016/0022-3468(90)90381-i[↩]
- International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J Clin Oncol. 1997 Feb;15(2):594-603. doi: 10.1200/JCO.1997.15.2.594[↩][↩]
- van Dijk MR, Steyerberg EW, Habbema JD. Survival of non-seminomatous germ cell cancer patients according to the IGCC classification: An update based on meta-analysis. Eur J Cancer. 2006 May;42(7):820-6. doi: 10.1016/j.ejca.2005.08.043[↩]





{kind=link}