Contents
What is endophthalmitis
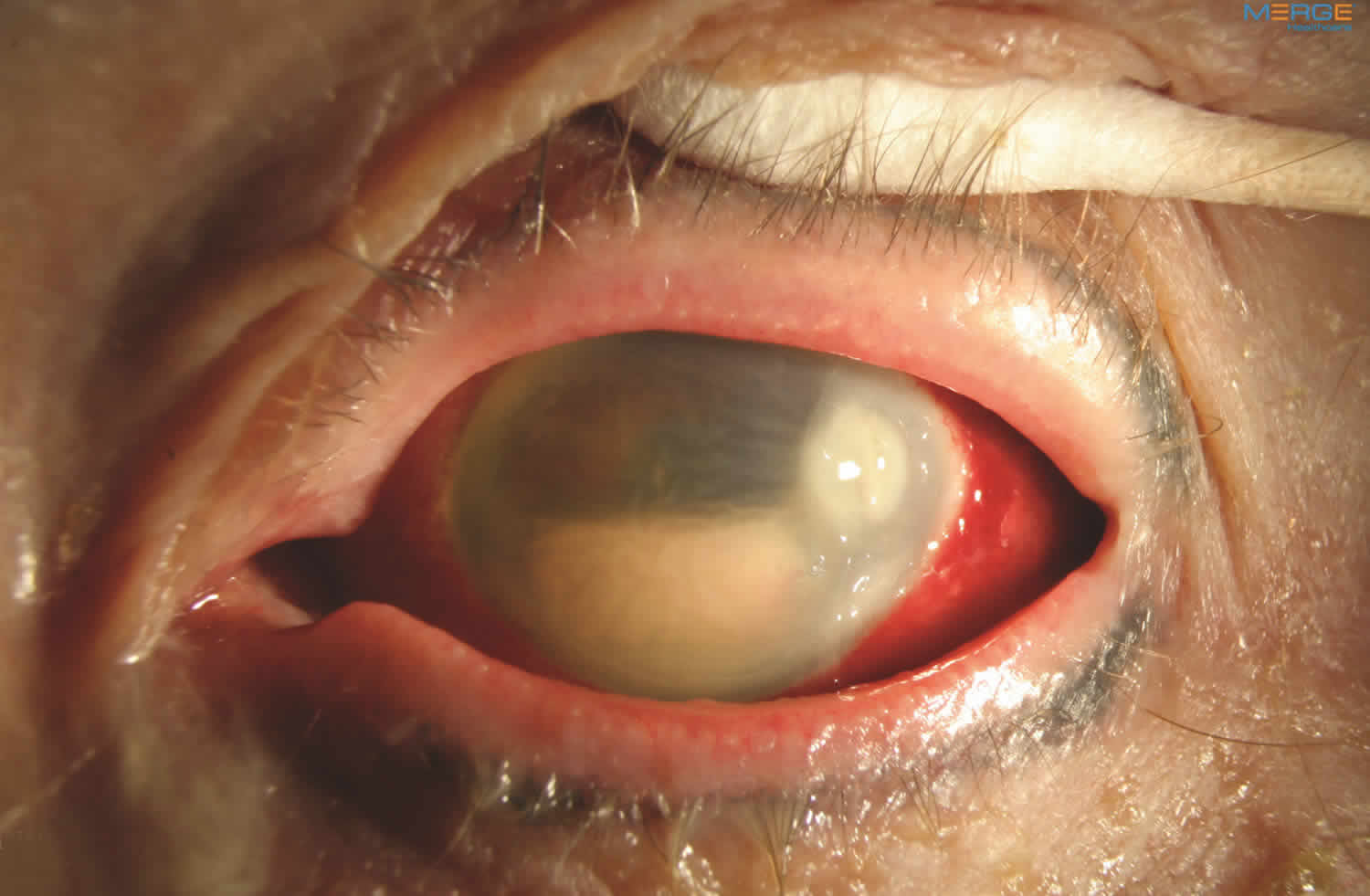
Endophthalmitis is serious infection inside the eye and endophthalmitis is a medical emergency. Endophthalmitis is a purulent inflammation of the intraocular fluids (vitreous and aqueous) usually due to infection. Endophthalmitis causes the white of the eye to be inflamed. There may be a white or yellow discharge on or inside the eyelid, and the cornea may show a white cloudiness. Progressive vitritis is the hallmark of any form of endophthalmitis 1. Histologically, massive infiltration of the vitreous cavity with inflammatory cells. There may also be a layer of white cells (hypopyon) present within the anterior chamber of the eye between the iris and the cornea (Figure 1).
Other symptoms of endophthalmitis include:
- Eye pain and redness
- Swelling of the eyelids
- Decreased vision
- Trouble looking at bright lights (photophobia), usually sudden onset
Endophthalmitis causes:
Endophthalmitis is caused by infection with bacteria or a fungus (candida endophthalmitis). Endophthalmitis very often occurs as a rare complication of cataract or other eye surgery.
- Acute postoperative endophthalmitis is the most common form of endophthalmitis
- Following cataract surgery 0.08% – 0.68%
- Rates increasing since clear corneal incisions
- Highest risk after secondary intraocular lense (0.2-0.367%), and lowest after pars plana vitrectomy (0.03-0.046%). Vitreous acts as a culture medium for micro-organisms, and hence after pars plana vitrectomy, the rates of endophthalmitis is least.
Endophthalmitis is usually a very serious problem and prompt examination by an ophthalmologist is essential to make an appropriate diagnosis and initiate treatment.
Immediate treatment with antibiotics is usually needed to preserve vision and to protect the health of the eye. A delay of even a few hours can result in irreversible vision loss in extreme cases. The choice of antibiotic may be adjusted depending on which organism is found to be causing the endophthalmitis. Antibiotics may be injected into the eye, given by vein (intravenously), or both.
People who have very poor vision when they are seen by a doctor may be given corticosteroids or have surgery. Corticosteroids can be given by mouth for a few days after the antibiotic injection, or, less commonly, they can be injected into the eye. Surgery may be needed to remove infected tissue from inside the eye, which may improve the chances of stopping the infection.
Endophthalmitis key facts
- Endophthalmitis is a medical emergency.
- Early diagnosis and treatment with antimicrobial therapy are critical
- Usually diagnosis must be made on clinical grounds
- Treat with empirical therapy, usually Vancomycin + Ceftazidime if bacterial
- Endophthalmitis Vitrectomy Study 2 showed that Pars Plana Vitrectomy was of benefit in patients with endophthalmitis following cataract extraction/intraocular lense or secondary intraocular lense placement who presented with light perception only visual acuity
- Although the role of vitrectomy in other forms of endophthalmitis is less clear, it remains an accepted adjunct to intravitreal antibiotics for treatment of moderate to severe cases
- Even with early and appropriate treatment, the prognosis for vision is often poor.
Figure 1. Endophthalmitis
Types of endophthalmitis
Endogenous endophthalmitis
Endogenous endophthalmitis originates from sources within the body. Endogenous endophthalmitis represents 2-8% of endophthalmitis cases. Patints usually have underlying disease. History of recent intravenous infusion, diabetes, HIV, IV drug abuse, renal failure on dialysis, cardiac disease, malignancy, immunosuppressive therapy, or indwelling catheters.
Liver abscess is the most common extraocular foci of infection, followed by pneumonia, endocarditis, soft tissue infection
Endogenous endophthalmitis treatment
- Cultures are essential and may be lifesaving
- Vitreous sample should be obtained in all cases
- Identification of organism is made by systemic culture of blood, urine or CSF in 75-80% of cases
- In contrast to postoperative endophthalmitis, systemic antibiotics are central to the treatment of endogenous endophthalmitis
- Focal chorioretinitis and associated mild vitritis can respond to systemic therapy alone
Exogenous endophthalmitis
- Acute Postoperative
- Chronic Postoperative
- Traumatic
- Filtering Bleb-Associated
- After Intravitreal Injections
Acute Postoperative Endophthalmitis
- Refers to infectious endophthalmitis shortly after ocular surgery
- Most present within 1-2 weeks, usually 3-5 days after the surgery.
- Initial symptoms: rapidly progressive, including pain, red eye, ocular discharge, and blurring
- Common signs: decreased visual acuity, lid swelling, conjunctival and corneal edema, anterior chamber cells + fibrin, hypopyon, vitreous inflammation, retinitis, and blunting of red reflex
- Retinal Periphlebitis – earliest sign
Traumatic endophthalmitis
Traumatic endophthalmitis causes
- Approximately 25% of endophthalmitis cases
- After open globe injury, chance of developing endophthalmitis is approx 7%
- Injuries including intraocular foreign body have higher rates
Risk factors
- Other risk factors: dirty wound, lens capsule rupture, age > 50, delayed presentation of more than 24 hours after injury
- Bacillus and Staphylococcus are common in penetrating trauma with intraocular foreign body
Diagnosis
- Primary repair and removal of intraocular foreign body as soon as possible
- Exclude the possibility of occult, retained intraocular foreign body
- CT scan with thin 1mm cuts
- Obtain cultures
- Intravitreal Vancomycin and Ceftazidime
- Some advocate Gentamicin + Clindamycin for synergistic effect against Bacillus and Staphylococcus
Treatment considerations
- Application of Endophthalmitis Vitrectomy Study 2 may not be appropriate, due to different organisms. In severe cases, vitrectomy should be strongly considered
- Some authors advocate therapeutic vitrectomy in all cases of traumatic endophthalmitis
- Others suggest performing vitrectomy only if patients do not respond after 48 hours or rapidly deteriorate in the first 24 hours following intravitreal antibiotics
- Post-traumatic endophthalmitis has worst visual prognosis than other categories
Prophylaxis after Penetrating Trauma
- Clinical evidence not established
- Some authors advocate intravitreal antibiotic administration in all cases of penetrating trauma
- Others recommend administration in the presence of risk factors (2 of 3: dirty wound, lens breach, or delay in closure over 24 hours)
- Systemic antibiotics: Intravenous cefazolin (1g every 6 hours for 48-72 hours) followed by an oral agent such as gatifloxacin or moxifloxacin for 7 days
Filtering Bleb-Associated Endophthalmitis
- Occurs as a result of pathogenic organisms gaining entry to intraocular tissue through the conjunctival filtering bleb
- Mean time b/w surgery and endophthalmitis is 19.1 months (range 3-9 years)
- 0.2 – 9.6% of glaucoma filtering procedures
- Increased incidence with use of antifibrotic agents
- Thin, cystic, avascular conjunctiva
- Blebitis – if no uveitis or vitritis
Endophthalmitis after Intravitreal Injection
- Increasing use of these agents, therefore concern for risk of endophthalmitis
- Like acute postoperative endophthalmitis, coagulase-negative staphylococci is the most common cause
- No infectious agent is identified in many cases
- Triamcinolone acetonide crystals can migrate into anterior chamber and mimic hypopyon
- 1.4% injection for Intravitreal Triamcinolone – intravitreal triamcinolone may play a role in endophthalmitis potentiation
- 0.2% injection for ranibizumab
Non-infectious Endophthalmitis after Triamcinolone Injection or intravitreal anti-VEGF (aflibercept) 3
- Crystals in anterior chamber or vitreous cavity can be difficult to distinguish from inflammatory reaction
- Use gravity-induced shifting of layered material and absence of anterior chamber flare or fibrin as a sign of a non-inflammatory cause
- Triamcinolone crystals may shift from the inferior anterior chamber angle when the pt is placed on his or her side, a phenomenon that does not occur with sticky, fibrin-laden material in a true inflammatory hypopyon
Management options
Close observation, topical steroids alone, oral levofloxacin alone.
Endophthalmitis causes
Acute cases of endophthalmitis are caused by gram-positive (or less frequently gram-negative) bacteria and are most often seen within 6 weeks after surgery or trauma to the eye.
Chronic cases that occur outside of the 6-week window are often related to a previous surgery and are commonly caused by slowly progressive infections such as Propionibacterium acnes or fungus.
Finally, systemic infections can spread to the eye causing endogenous endophthalmitis. This is often associated with systemic fungal or gram-negative bacterial infections. Patients who are debilitated, septicemic (bacteria in the bloodstream), and who have weakened immune systems are particularly susceptible, especially after surgical procedures.
Risk factors for endophthalmitis
Loss of vitreous gel (also referred to as vitreous humor), disrupted posterior capsule, poor wound closure, and prolonged surgery are risk factors for developing endophthalmitis. The incidence following penetrating trauma is 4–13% and may be as high as 30% after injuries in rural settings.
Risk factors for endophthalmitis after trauma include:
- Retained intraocular foreign body (having foreign material remain in your eye following an injury)
- Delayed surgery (longer than 24 hours) to repair a full-thickness laceration
- Rural setting (soil contamination)
- Damage to the lens during trauma
Endophthalmitis signs and symptoms
Endophthalmitis symptoms may be severe and include severe eye pain, redness in the white of the eye, extreme sensitivity to bright light, decreased vision, and occasionally swelling of the eyelid.
Endophthalmitis symptoms
- 94.3% reported blurred vision
- 82.1% red eye
- 74% pain- It is important that almost 25% patients did not have pain.
- 34.5% swollen lid
Endophthalmitis signs
- 85% hypopyon- Fifteen percent patients may not have a hypopyon.
- 79% hazy media
- 26% light perception vision only
When there is a doubt between post-operative inflammation and endophthalmitis with severe haze in the ocular media, or vitreous opacities clinically the possibility of an infection should be given priority.
Endophthalmitis diagnostic testing
To determine what organism has caused the infection, a biopsy of the fluid within your eye needs to be obtained. This fluid is then sent to the laboratory for a determination and to decide on the best treatment.
Presenting Visual Acuity
- Hand motion vs. light perception – when measuring visual acuity, the technique of differentiating light perception vs. hand motion vision is most important
- Pars plana vitrectomy recommended in patients with visual acuity of light perception.
- Hand motion or better, tap and inject intravitreal antibiotics.
- Endophthalmitis Vitrectomy Study 2 gave the standard criteria to evaluate visual acuity in endophthalmitis : ‘If no letters could be read on the (ETDRS) chart at 4 m, then at 1 m, vision was tested for the ability to count fingers. If the patient was unable to count fingers, vision was tested for the ability to recognize hand motions. For this, the patient’s opposite eye was occluded, and a light source, such as a lamp used for near vision, was directed from behind the patient to the examiner’s hand that either was stationary or was moved at one motion per second in a horizontal or vertical direction at a distance of 60 cm from the eye. The patient was asked to identify whether the examiner’s hand was still, moving sideways, or moving up and down. The presentation was repeated five times, and hand-motion visual acuity was considered present if the patient was able to identify the examiner’s action on at least four of the presentations. If the examiner was not convinced that hand motions could be detected, light perception was tested at 0.9 m with an indirect ophthalmoscope set at maximum intensity.
Ultrasound Evaluation
- Should be performed if significant media opacification prevents adequate view of the fundus
- Findings with endophthalmitis:
- Dispersed vitreous opacities with vitritis
- Chorioretinal thickening
- Rule out: retinal detachment or choroidals, dislocated lens material, retained foreign bodies
- Retinal or choroidal detachment are poor prognostic factors.
Microbiological Characteristics
- Bacteria are the most common infecting agents
- Causative organisms represent bacteria from patient’s own periocular flora, introduced during surgery. In cases of intravitreal medication associated endophthalmitis, causes include oral flora (treating physician or patient) or drug contamination. It is important therefore for these injections to not speak or to cover the treating physician with a mask and to ask the patient not to speak or use a drape.
- In the Endophthalmitis Vitrectomy Study 2, 94.2% of culture-confirmed cases involved Gram positive bacteria
- 70% were Gram positive, coagulase-negative Staphylococcus epidermidis
Obtaining Specimens for Microbiologic Studies
- In the Endophthalmitis Vitrectomy Study 2, vitreous samples yielded positive cultures more often than aqueous samples
- Aqueous samples were the only source of positive culture in 4.2% of eyes
- Can obtain at the time of pars plana vitrectomy, if indicated
Method of Obtaining Samples
- Eye surgically prepped with povidone-iodine 5% solution
- Surgical drape, lid speculum
- 30g needle attached to tuberculin syringe via limbus for anterior chamber tap, without collapsing anterior chamber
- Obtain 0.1 ml
- Vitreous specimen, obtain by either vitreous needle tap or by vitreous biopsy with a cutting/aspirating probe
Vitreous Specimen
- After conjunctival incision (if 20g), a vitrectomy probe attached to a tuberculin syringe is inserted into the vitreous cavity through a sclerotomy placed 3-4mm posterior to limbus
- Approx 0.1-0.3mL of vitreous is removed from the anterior vitreous cavity by using the automated cutting mechanism of the probe and slow, manual aspiration.
- Alternate method: vitreous needle tap – is performed by inserting 27 to 22g needle attached to a tuberculin syringe into the vitreous cavity through the pars plana (pull plunger back first to break the vacuum before inserting into the eye). Slowly aspirate. If no fluid vitreous can be obtained with a needle tap, a vitreous biopsy must be performed instead to avoid aspirating formed vitreous
Specimen
- Culture inoculation by the surgeon within minutes of obtaining specimens is ideal to maximize recovery of the organisms
- A spinal needle should be used to inject the specimen deeply into liquid media
- Gram stain, culture (aerobic, anaerobic, and fungal)
- Antibiotic sensitivities (although in the Endophthalmitis Vitrectomy Study, Vancomycin and amikacin empiric treatment covered 99.4% of all infecting organisms)
More recently, polymerase chain reaction (PCR) testing is being used more frequently to identify suspected pathogens in the sample. PCr testing requires the physician to specify the suspected organisms when requesting the test.
Endophthalmitis treatment
In acute cases, treating endophthalmitis is an emergency and needs to be performed as soon as possible. The procedure performed will depend on your vision. If your vision is very poor, you will need to undergo an emergency surgery called a vitrectomy to remove the infectious debris from your eye and to inject antibiotics or antifungal agents directly inside your eye. Cases with better vision may only require an injection of antibiotics or antifungal agents in the office. In rare cases, only antibiotic eye drops are required.
Pars Plana Vitrectomy
- Advantages: reduction of infecting organisms, toxins, inflammatory materials, and opacities. Allows collection of samples
- Disadvantages: Need for sophisticated equipment and the need for an operating theater.
- Vitrectomized eyes have more rapid clearance of intravitreal antibiotics
- In inflamed, aphakic, vitrectomized rabits, intravitreal vancomycin and ceftazidime half-lives are 7.5 and 5.1 hours, respectively, compared to 31.4 and 10.1 hours, respectively, in inflamed, phakic nonvitrectomized rabbits
Pars Plana Vitrectomy – obtaining sample
- Standard 3 port setup
- A vitreous sample of 0.2-0.5mL is first obtained without infusion using gentle manual aspiration into a syringe with a high cutting rate
- Infusion is then initiated and core vitrectomy performed
- The A/C is cleared for visualization as necessary
- In most cases, IOL need not be removed
- In the Endophthalmitis Vitrectomy Study, attempts were made to clear 50% or more of the vitreous
- Also in the Endophthalmitis Vitrectomy Study, no attempt to induce a posterior vitreous detachment if none was previously present
Immediate Pars Plana Vitrectomy vs. Tap & Inject
- In the Endophthalmitis Vitrectomy Study 2, patients who presented with light perception only visual acuity had a significant, threefold improved chance of obtaining 20/40 vision after immediate vitrectomy 4 compared to tap and inject (11%)
- 56% of obtaining 20/100 or better after immediate Pars Plana Vitrectomy compared to 30% after tap
- Hand motion or better vision no significant difference between the treatment groups in final visual acuity(consider earlier Pars Plana Vitrectomy for diabetics)
Intravitreal antibiotics
Current recommendations for empirical therapy (bacterial)
- Vancomycin 1.0 mg/0.1 mL
- Ceftazidime 2.25 mg/0.1 mL
- Amikacin 400 ug/0.1 mL for penicillin allergic pts (although usually can still inject Ceftazidime since there is low cross-reactivity between cephalosporins and penicillin; keep in mind that most penicillin “allergies” may not really be an allergic reaction; also low systemic absorption from ocular injection)
- 4th generation fluoroquinolones – unclear400 ug/0.1 mL of gatifloxacin or moxifloxacin
- Fungal: Amphotericin B 5-10 ug/0.1 mL
Complications of Intravitreal Antibiotics
- Corneal opacification and retinal toxicity
- Retinal toxicity with aminoglycosides, most notably gentamicin (even as low as 0.1mg)- macular infarct
- Less common with amikacin and tobramycin
- Amphotericin B – can also cause retinal toxicity
- Hemorrhagic occlusive retinal vasculitis (HORV) (rare) 2
Systemic Antibiotics
- Usually too slow to enter the eye in adequate concentrations
- In the Endophthalmitis Vitrectomy Study 2, there was no difference in visual acuity or media clarity with or without intravenous antibiotics (amikacin plus ceftazidime or amikacin plus ciprofloxacin) when given in addition to intravitreal antibiotics
- However, did not have available newer 4th generation fluoroquinolones with better ocular penetration. Systemic ceftazidime, cefazoline, ciprofloxacin, gatifloxacin3 and moxifloxacin has been shown to penetrate the blood ocular barrier efficiently.
Corticosteroids
- Goal is to modulate the host inflammatory response to the infection and minimize ocular damage from this response. Avoid when fungal infection is suspected.
- Intravitreal corticosteroids (dexamethasone) is controversial
- 2 retrospective nonrandomized studies showed 20/400 or better vision was obtained more in pts who received 400 ug adjuvant intravitreal dexamethasone
- Randomized, prospective trial of 63 pts showed in no difference in visual acuity at 12 weeks
- Another retrospective, nonrandomized trial of 57 patients showed worse visual acuity
Reinjection
A minority of patients will require further treatment, mainly for worsening ocular infectionIt typically requires more than 24 hours to observe an improvement in the clinical appearance after initial treatment. In many cases, the treated eyes look somewhat worse 1 day after treatment before improving subsequently
Considerations of reinjection
- Should be considered if the infection fails to stabilize or improve more than 48 hours after the first injection
- Based on consensus view, the Endophthalmitis Vitrectomy Study 2 protocol recommended reinjection if the infection was worsening at 36-60 hours after initial injection
- Often, 36 hours after treatment, culture results are available
- Decision to reinject antibiotics should not be taken lightly, since repeat injection may increase risk of retinal toxicity
- 100% retinal toxicity rates with 3 intravitreal doses of 1mg vanco combined with 400ug amikacin or 200 ug gent in rabbit eyes
- Patients with no culture growth, equivocal growth, or coagulase-negative staph had a 5% rate of additional procedures, compared to 30% in patients with cultures that grew Gram negative or other Gram positive organisms
Post-Trabeculectomy Endophthalmitis Treatment
- If only blebitis, conservative treatment with systemic and topical fortified antibiotic therapy
- If the vitreous is clear, examine thse pts frequently, treating for endophthalmitis if vitritis or acute hypopyon develops
- Needle aspiration of the bleb is not advised
- Studies suggest possible benefit from Pars Plana Vitrectomy
Endophthalmitis prognosis
The prognosis depends on the cause, duration, and type of organism that caused the infection. Outcomes are often less favorable for traumatic cases involving gram negative organisms. Some cases involving gram positive bacterial infections after cataract surgery fare better. Eyes with endophthalmitis often require frequent examinations to obtain the best outcomes.
The most common cause of visual loss in the Endophthalmitis Vitrectomy Study 2 was attributed to macular abnormalities, such as epiretinal membrane, macular edema, pigmentary degeneration, and ischemia.
Strongest predictor of poor visual outcome was light perception only vision
Other risk factors: older age, diabetes, corneal infiltrate or ring ulcer, compromised posterior chamber, low or high intraocular pressure, afferent pupillary defect, rubeosis, and absent red reflex
Coagulase-negative Staphylococcus epidermidis were most likely to obtain 20/100 final visual acuity or better (84%). Higher virulent organisms, such as Staphylococcus aureus, streptococcal species, and Gram negative (Pseudomonus) organisms were associated with worse visual outcomes.
- Endophthalmitis. https://eyewiki.org/Endophthalmitis[↩]
- Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol 1995;113:1479–1496.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Endophthalmitis, a review of current evaluation and management. Lemley et al. Retina 27:662-680, 2007[↩]
- Das T, Sharma S; Hyderabad Endophthalmitis Research Group.Current management strategies of acute post-operative endophthalmitis.Semin Ophthalmol. 2003;18(3):109-115[↩]





{kind=link}