
Contents
What is Erb’s palsy
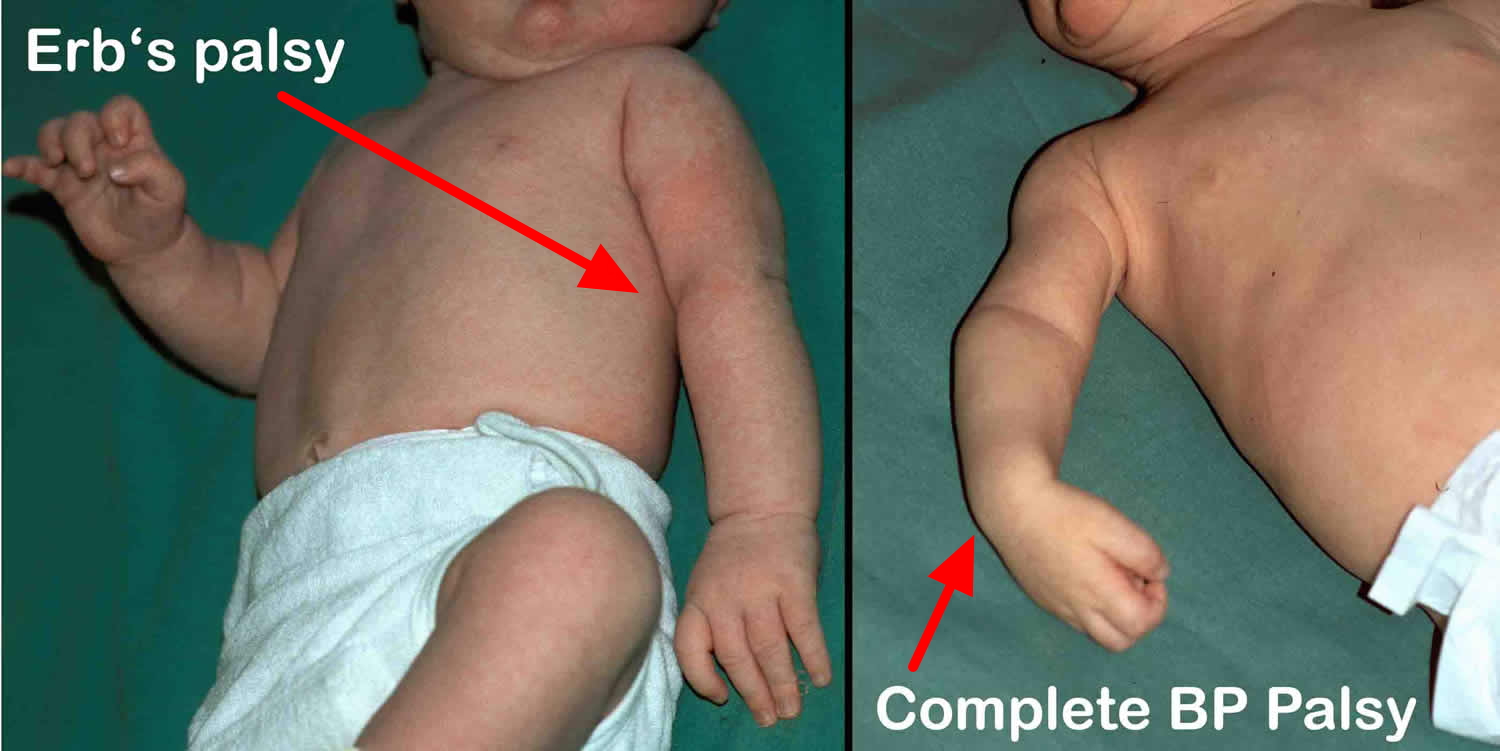
Erb’s palsy is also called Erb-Duchenne palsy refers to paralysis of the upper brachial plexus caused by injury to the superior roots of the brachial plexus (C5–C6). The position of the limb, under such conditions, is characteristic: the arm hangs by the side and is rotated medially; the forearm is extended and pronated (see Figure 4). The arm cannot be raised from the side; all power of flexion of the elbow is lost, as is also supination of the forearm — “waiter’s tip hand position” (hand turning backwards). Moro reflex is absent. Meanwhile, the grasp reflex is present which differentiates it from another brachial nerve palsy, Klumpke palsy (C7, C8, and T1). The newborn baby may have impaired sensation on the outer side of the arm and/or phrenic nerve palsy (C3, C4, and C5a).
Erb’s palsy relates to an injury to the superior roots of the brachial plexus of C5 and C6. Traction of the shoulder can injure the brachial plexus (particularly C5 and C6) during delivery. Erb’s palsy usually occurs in macrosomia (large baby) and shoulder dystocia infants who needed to be pulled from the birth canal 1. This maneuver causes stretching of the brachial plexus which may injure it. Other causes that lead to forced pulling of the shoulder include breech delivery, multipara mother, maternal obesity, maternal diabetes, or vacuum and forceps delivery 2. Erb’s palsy also may occur in cesarean section 2.
Erb’s palsy is a common birth injury with estimated prevalence ranges of 0.2 to 2.0 of every 1000 births 2. Erb’s palsy causes significant arm weakness that affects 0.4 to 5 in 10,000 births.
The resulting traction injury may vary from neurapraxia (a temporary loss of motor and sensory function due to blockage of nerve conduction) or axonotmesis (a more severe injury where the nerve axons and their myelin sheath are damaged but the endoneurium, perineurium and epineurium remain intact) to neurotmesis (the most serious nerve injury both the nerve and the nerve sheath are disrupted. While partial recovery may occur, complete recovery is impossible) and avulsion of rootlets (most severe form of brachial plexus injury where the nerve roots are torn off the spinal cord) from the spinal cord. Most individuals with neuropraxia injuries recover spontaneously with a 90-100% return of function. Axonometric lesions involve disruption of axon and myelin sheath. Recovery of axonometric lesions depend on the level of lesion, and it may take months to heal with proper treatment including physiotherapy. Neurotmesis is the worst prognosis, as the lesion causes irreversible damage affecting the axon, myelin sheath as well as the supporting structures through the nerve. The proximal end of nerve tries to regenerate by forming a neuroma in which the nerve has torn and healed but scar tissue puts pressure on the injured nerve and prevents it from conducting signals to the muscles. A nerve that is completely pulled apart cannot repair itself, so the muscles it controls are paralyzed. Sometimes it is possible to have an operation to mend the nerve and restore some function to the muscle, if this is necessary, the child is likely to be left with some residual weakness in the arm. In rare cases the nerve may be torn away from the spinal column itself – this is called an AVULSION in these cases it is imperative to consult a specialist in Brachial Plexus Injuries as soon as possible to discuss a treatment plan.
Possible complications include:
- Abnormal muscle contractions (contractures) or tightening of the muscles. These may be permanent.
- Permanent, partial, or total loss of function of the affected nerves, causing paralysis of the arm or arm weakness
The treatment of Erb’s palsy depends on the nature of damage, which is either nerve bruise (neuropraxia) or nerve tear. Nerve bruise (neuropraxia) usually resolve on its own over a period of months. However, in the latter case i.e. nerve tear, the following multiple approaches are advised, physiotherapy for regaining muscle usage 3, surgical interference 4 of nerve transplants (usually from the opposite leg), subscapularis releases, latissimus dorsi tendon transfers and rehabilitation therapy.
Fortunately, nearly all affected infants with Erb’s recover in the first few months 1. Erb’s palsy resolves completely in the first year of life in 80% to 96% of patients and in nearly 100% if recovery begins within four weeks of birth 5. Rarely is a child left with a significant disability. Hydrotherapy is a form of physical therapy used because of the anti-gravity environment. It minimized the stress on the musculoskeletal frame, allowing the neonate to move with less pain and at the same time strengthening muscles and reducing spasms. Paralyzed muscles relax in the opposite position of the waiter’s tip posture by abduction at the shoulder, external rotation of the arm, and supination of the forearm. Physiotherapy begins after two weeks. Surgical intervention, nerve graft, or nerve decompression is the next step if there is no response after 3 to 6 months 2.
Denervated muscle changes begin at the moment of injury, and without reinnervation, becomes irreversible at 18 to 24 months. These time-sensitive, irreversible changes are the scientific basis for early management recommendations. Neglected cases may lead to 20% to 30% permanent deficit of the nerve function 2.
Figure 1. Brachial plexus
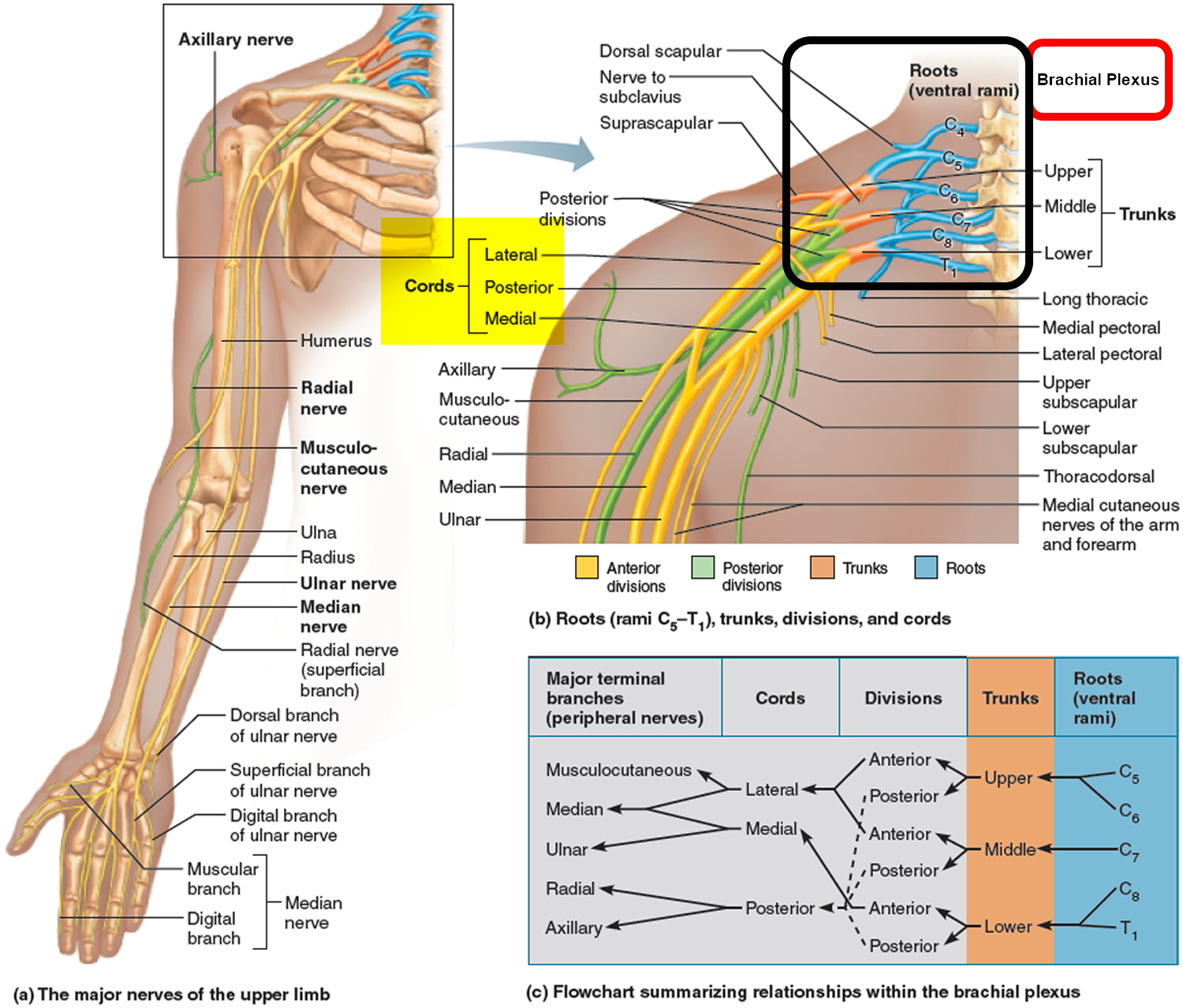
Figure 2. Brachial plexus origin and nerve branches
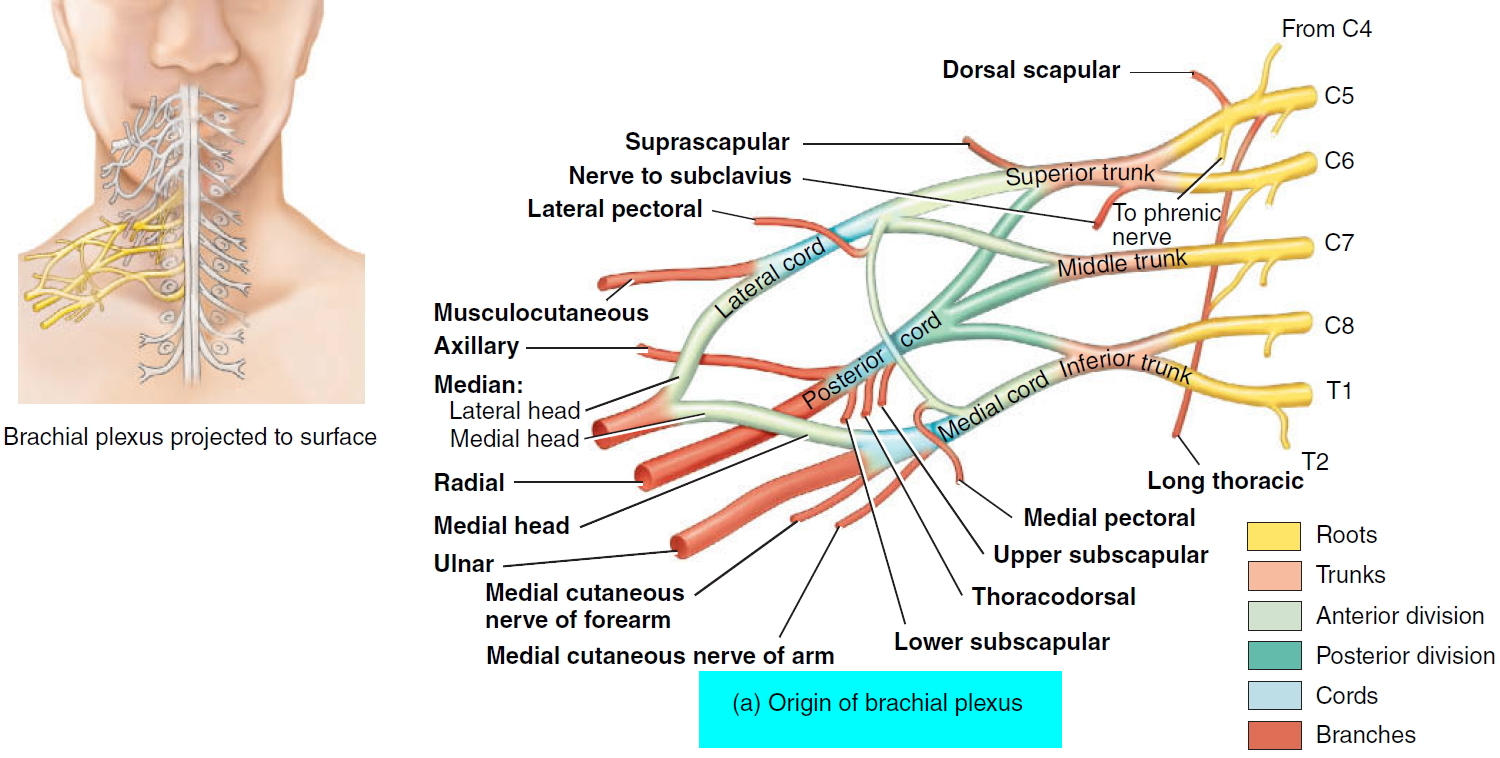 Figure 3. Brachial plexus motor and sensory innervation of the upper limb
Figure 3. Brachial plexus motor and sensory innervation of the upper limb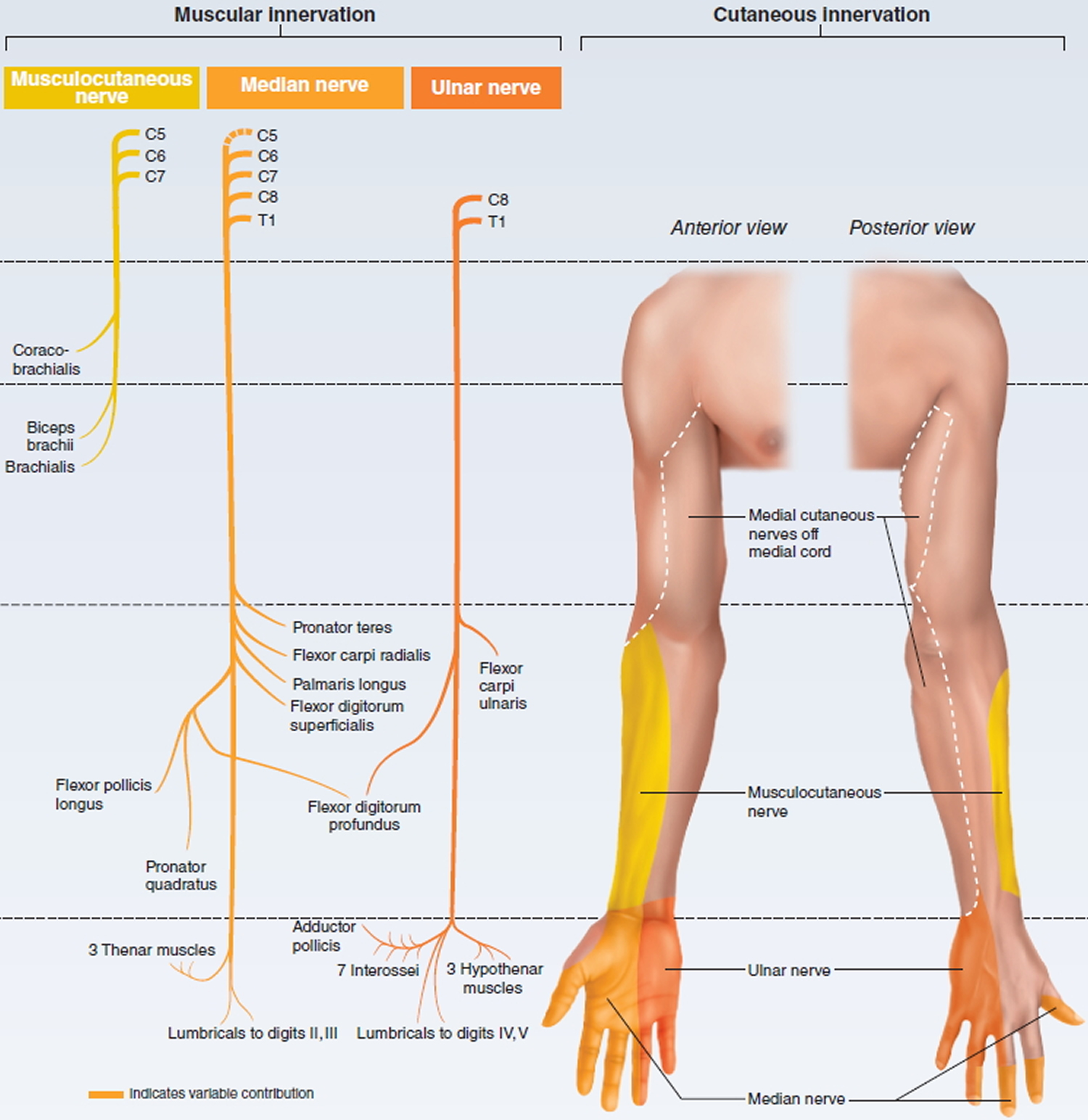
Figure 4. Erb’s palsy (C5-C6 nerve damage) waiter’s tip position
Erb’s palsy causes
Erb’s palsy results from a lesion at Erb’s point where C5 and C6 unite to form the upper trunk of the brachial plexus.
Damage to the upper nerves that make up the brachial plexus tends to occur when your shoulder is forced down while your neck stretches up and away from the injured shoulder. The lower nerves are more likely to be injured when your arm is forced above your head. These injuries can occur in several ways, including:
- Contact sports. Many football players experience burners or stingers, which can occur when the nerves in the brachial plexus get stretched beyond their limit during collisions with other players.
- Difficult births. Newborns can sustain brachial plexus injuries when there are problems during birth, such as a breech presentation or prolonged labor. If an infant’s shoulders get wedged within the birth canal, there is an increased risk of a brachial plexus palsy. Most often, the upper nerves are injured, a condition called Erb’s palsy. Total brachial plexus birth palsy occurs when both the upper and lower nerves are damaged.
- Trauma. Several types of trauma — including motor vehicle accidents, motorcycle accidents, falls or bullet wounds — can result in brachial plexus injuries.
- Inflammation. Inflammation may cause damage to the brachial plexus. A rare condition known as Parsonage-Turner syndrome (brachial plexitis) causes brachial plexus inflammation with no trauma and results in paralysis of some muscles of the arm.
- Tumors. Noncancerous (benign) or cancerous tumors can grow in the brachial plexus or put pressure on the brachial plexus or spread to the nerves, causing damage to the brachial plexus.
- Radiation treatment. Radiation treatment may cause damage to the brachial plexus.
Risk factors for brachial plexus injury
Participating in contact sports, particularly football and wrestling, or being involved in high-speed accidents increases your risk of brachial plexus injury.
Brachial plexus injury prevention
Although damage to your brachial plexus often can’t be prevented, you can take steps to reduce the risk of complications once an injury has occurred:
- For yourself. If you temporarily lose the use of your hand or arm, daily range-of-motion exercises and physical therapy can help prevent joint stiffness. Avoid burns or cuts, as you may not feel it if you’re experiencing numbness. If you’re an athlete who has experienced several injuries to the brachial plexus area, your doctor may suggest you wear specific padding to protect the area during sports.
- For your child. If you’re the parent of a child with a brachial plexus palsy, it’s important that you exercise your child’s joints and functioning muscles every day, beginning when your baby is about 3 weeks old. This helps prevent the joints from becoming permanently stiff and keeps your child’s working muscles strong and healthy.
Erb’s palsy symptoms
Erb’s palsy results from injury to nerve roots C5 and C6, with C7 also affected in 50% of instances 1. Muscles involved are listed in Table 1. The classical sign of Erb’s palsy is the ‘waiter’s tip hand’ (hand turning backwards). The arm hangs limply from the shoulder with internal rotation of the forearm plus wrist and finger flexion. Sometimes there are sensory deficits over the lateral proximal upper extremity 5. C3 and C4 are injured in about 5% of patients leading to phrenic nerve dysfunction and paralysis of the hemidiaphragm 6. Horner’s syndrome occurs rarely when the stellate ganglion is disrupted 5. Horner’s syndrome is when the eyelid droops and the pupil in the eye may be smaller. The baby may also have an associated Torticollis. Torticollis is where the baby faces away from their affected arm and is unable to face forward for any length of time. Your baby may also suffer from sensory loss in the arm and hand.
Table 1. Deficits as a result of brachial plexus injury
| eak movement | Cord segment | Muscle | Resulting position |
|---|---|---|---|
| Shoulder abduction | C5 | Deltoid | Adducted |
| Shoulder external rotation | C5 | Supra- and infraspinatus | Internally rotated |
| Elbow flexion | C5, C6 | Biceps, brachioradialis | Extended |
| Supination | C5, C6 | Supinators | Pronated |
| Wrist extension | C6, C7 | Extensors of wrist | Flexed |
| Finger extension | C6, C7 | Extensors of fingers | Flexed |
| Diaphragmatic descent | C4, C5 | Elevated |
Erb’s palsy diagnosis
Erb’s palsy is a disorder of clinical diagnosis, but some interventions can confirm it. An X-ray of the baby’s shoulder can exclude any fractured bone or problems with the shoulder or elbow joints. Electromyography (EMG) results can estimate and record the electrical activity of the muscle. Nerve conduction studies can measure the time required for the electrical stimulus to move through a particular nerve. An MRI can exclude any cancer or tumor that may affect the brachial plexus. CT myelography works by injecting the contrast material to give detail of neonate spinal cord and nerve root.
Erb’s palsy treatment
Initial treatment consists of coming to a proper diagnosis, which includes a careful history taking, detailed clinical examination, including a check for associated injuries like fractures of the clavicle and humerus. Electrophysiology is recommended at 4 weeks initially to confirm the diagnosis and get a baseline reading of the involvement of various nerves and muscles as well as sensory parameters. Counseling of parents is critical and clear open communication is strongly recommended. Gentle mobilisation of all joints of the affected limb is suggested to avoid stiffness. Splints may prevent flexion contractures of the wrist and fingers 7. “Gift wrapping” the baby in the typical traditional Indian style after morning bath is discouraged as it deprives the child of a chance to use that limb spontaneously. Repeat examinations are carried out every 4–6 weeks until 3 months. At this time, a decision is made about the need for surgery, which in turn depends on clinical and electrophysiological findings. MRI is considered very useful, at least in the adult palsy. However, clinical exam and electrophysiology can give adequate evidence of the status of the plexus and the indication for surgery.
If an MRI does not show root avulsion and there is no bicep function by five months of age, then exploratory surgery may be considered. A flail arm or Horner’s syndrome at three months may justify earlier surgery 8. Overall, based on retrospective case studies, approximately two-thirds of patients undergoing surgical exploration show improvement 9.
Brachial plexus injury exercises
Gentle massage of the arm and range-of-motion exercises are recommended for mild cases. The infant may need to be seen by specialists if the damage is severe or the condition does not improve in the first few weeks.
Surgery may be considered if some strength has not returned to the affected muscles by the time the baby is 3 to 9 months old.
Indications for Surgery
In case of global involvement, involvement of the hand or a flail upper limb, there is no real dispute about indication or timing of surgery. The dispute arises in the upper plexus lesions of Narakas Type I and II (see Table 2 below). The author follows Prof. Gilbert’s criteria of using the biceps brachii as an indicator of recovery in upper plexus lesions. Following the landmark theses by Tassin 10 it was generally agreed that a lack of antigravity biceps function at 3 months is an indication for surgery in C5-C6+/–C7 lesions. The logic behind this caveat is that the biceps is the only C5–C6 innervated muscle whose function cannot be duplicated by other muscles, and therefore is a good uncluttered indicator of C5-C6 recovery. The shoulder, for example, is moved by multiple muscles, which have various innervations and represent many neurotomes, and is therefore considered unsuitable for making this judgement call. Biceps recovery indicates the good health of C5–C6 and the upper trunk all the way to the upper arm. Clarke and his group 11 developed an alternative Active Movement Scale (AMS) in Toronto (see Table 3). They use this scoring and are prepared to wait for a much longer observation period to come to a decision. They also use the “Cookie” test around 8–9 months in children who are on the borderline of surgery and conservative treatment to make a final call regarding the indication of surgery. While there is merit in this system, the resource requirement in terms of physical and occupational therapists dedicated to this clinic, etc. exceeds that which is typically available. In addition, the system is cumbersome to administer at this point in time and may not offer a great advantage over Gilbert’s rather simpler indication.
Table 2. Narakas classification
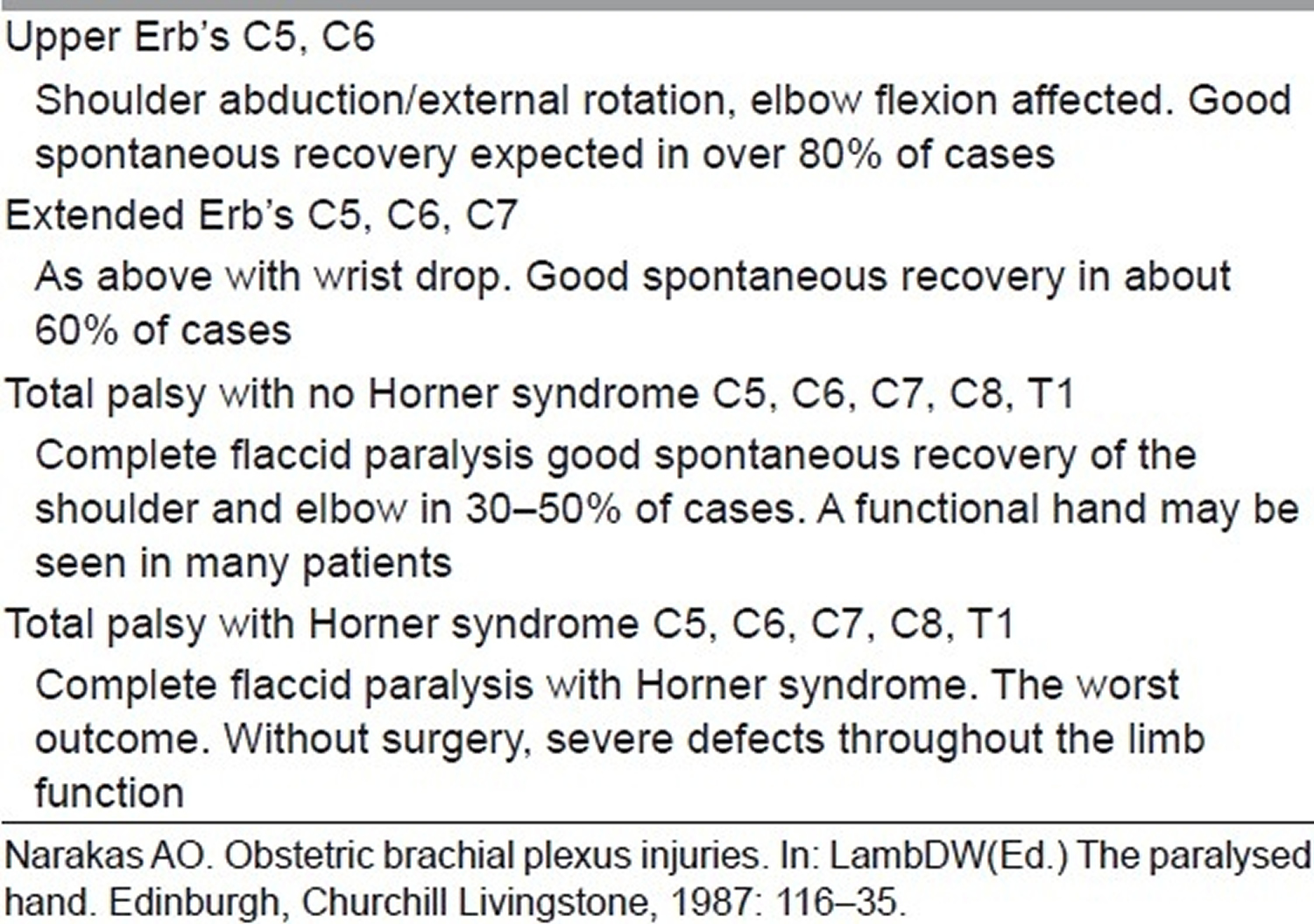
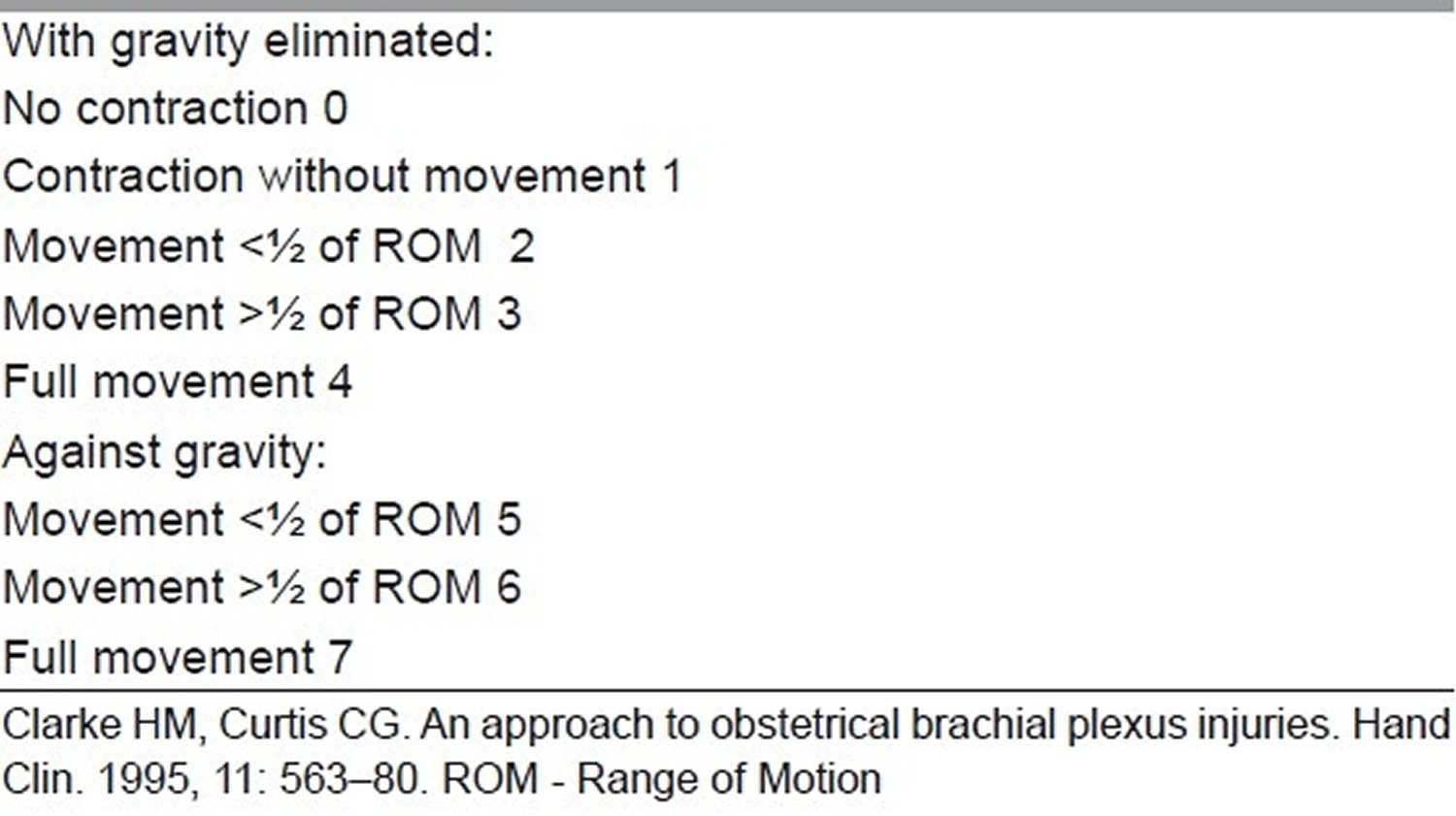
Table 3. Toronto active movement scale of Clarke and Curtis
Waters, in a review 12, has summarized the issue with the following observation: “Infants who recover partial antigravity upper trunk muscle strength in the first 2 months of life should have a full and complete recovery over the first 1–2 years of life. Infants who do not recover antigravity biceps strength by 5–6 months of life should have microsurgical reconstruction of the brachial plexus, as successful surgery will result in a better outcome than natural history alone. Infants with partial recovery of C5–C6–C7 antigravity strength during months 3 through 6 of life will have permanent, progressive limitations of motion and strength; they also are at risk for the development of joint contractures in the affected limb.”
Thatte 13 uses Gilbert’s criteria for the decision, i.e. if a child with upper plexus lesion does not have a biceps function exceeding MRC grade 3 (antigravity movement) at 3 months of age, then surgery is recommended for nerve repair. In cases where there is visible biceps contraction but triceps co-contraction preventing elbow flexion, or biceps being 2+ but not really 3, etc., the surgeon can wait and watch with/without botox to triceps up to 6 months by which time the picture is clear. If the bicpes continues to be under MRC grade 3, then surgery is better than conservative treatment 13.
Erb’s palsy surgery
Surgery consists of a complete exploration of the supra and infraclavicular plexus and nerve repair using microsurgical techniques based on merits, i.e. after assessing the injury and its pathophysiology, the surgeon can decide on the strategy to be used. Thatte et al. 13 have recently published a detailed paper describing the technique for exposure of the brachial plexus, which can be used for further reading. Typically, the preference in a total palsy is to hand function, while in an upper plexus it is of course to reconstruct the nerves for elbow and shoulder function. The suprascapular nerve supplying the supra and infraspinatus is a crucial nerve for shoulder abduction and external rotation and needs to be targeted with priority, either from one of the roots or separately with the spinal accessory nerve as the donor. The lower trunk/medial cord for hand and musculocutaneous nerve for biceps are the other priorities.
Intraplexus neurotisation thus uses existing healthy root stumps, which are ruptured for reconstruction by joining them with the distal target trunks, cords or nerves using nerve grafts. The source of nerve grafts is both sural nerves and the ipsilateral medial cutaneous nerve of forearm (MCNF) and superficial radial nerve (SRN), especially in global severe palsies if grafts are falling short. Not all cases may be of rupture; there can be avulsions as well, and therefore no roots may be available. Depending on the number of roots available, a policy is evolved for neurotisation.
Global palsy strategy
- Four or five roots available: Very rare; just direct them to respective trunks/cords.
- Three roots available: One each to medial, lateral and posterior cords. Spinal accessory to suprascapular nerve depending on the pathoanatomy of the upper trunk lesion.
- Two roots available: Root 1 to lower trunk/medial cord, Root 2 to lateral cord (or shared between lateral and posterior cords) and spinal accessory to suprascapular nerve. Some authorities would prefer Root 2 to posterior division of upper trunk/posterior cord and 2 or 3 intercostal nerves to biceps. Their point is getting a strong triceps and a stable shoulder with deltoid and triceps as well as the rotator cuff is important to balance a well-recovered biceps. This is logical; however, the addition of intercostal nerves adds to surgical time, blood loss and increases surgical risks and morbidity and needs to considered carefully before attempting. In well-equipped centres with blood bank support, ICU for children and experienced anaesthesiologists, it can be done if the child is fit.
- One root available: Root to lower trunk/medial cord + spinal accessory to suprascapular nerve, 2 or 3 intercostal nerves to biceps. Shoulder will need secondary transfers if possible.
- Zero roots – rare total avulsion: Opp. C7 root (posterior division) to lower trunk/medial cord and spinal accessory to musculocutaneous nerve or spinal accessory to suprascapular nerve and intercostal nerves to musculocutaneous nerve plus one intercostal nerve to long head of triceps. If the child is healthy and fit for prolonged anaesthesia-or stagger in a second session in a couple of months if there is any concern on this count.
- Upper plexus: C5–C6
- Both roots available: Typically C5 to anterior division of upper trunk and C6 to posterior division of upper trunk.
- One root available: Root to anterior division of upper trunk (or both divisions if they are of really good quality with plenty of healthy axons) and XI nerve to suprascapular nerve. Intercostal nerves can be used for additional neurotisation depending on situation and fitness.
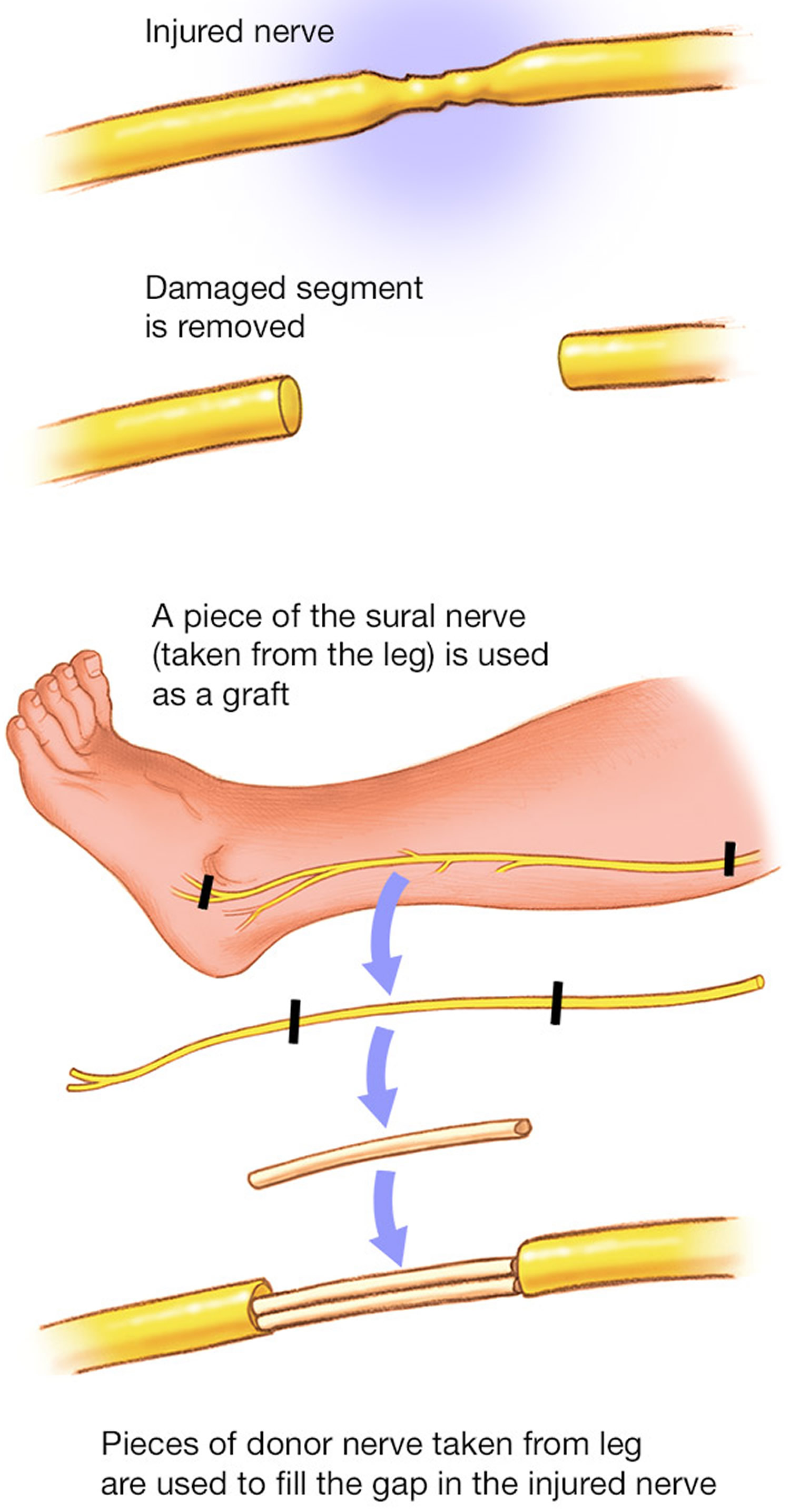
Figure 5. Nerve graft – Nerve tissue can be removed from other parts of your body to replace the damaged portions of your brachial plexus nerves.
Distal nerve transfers
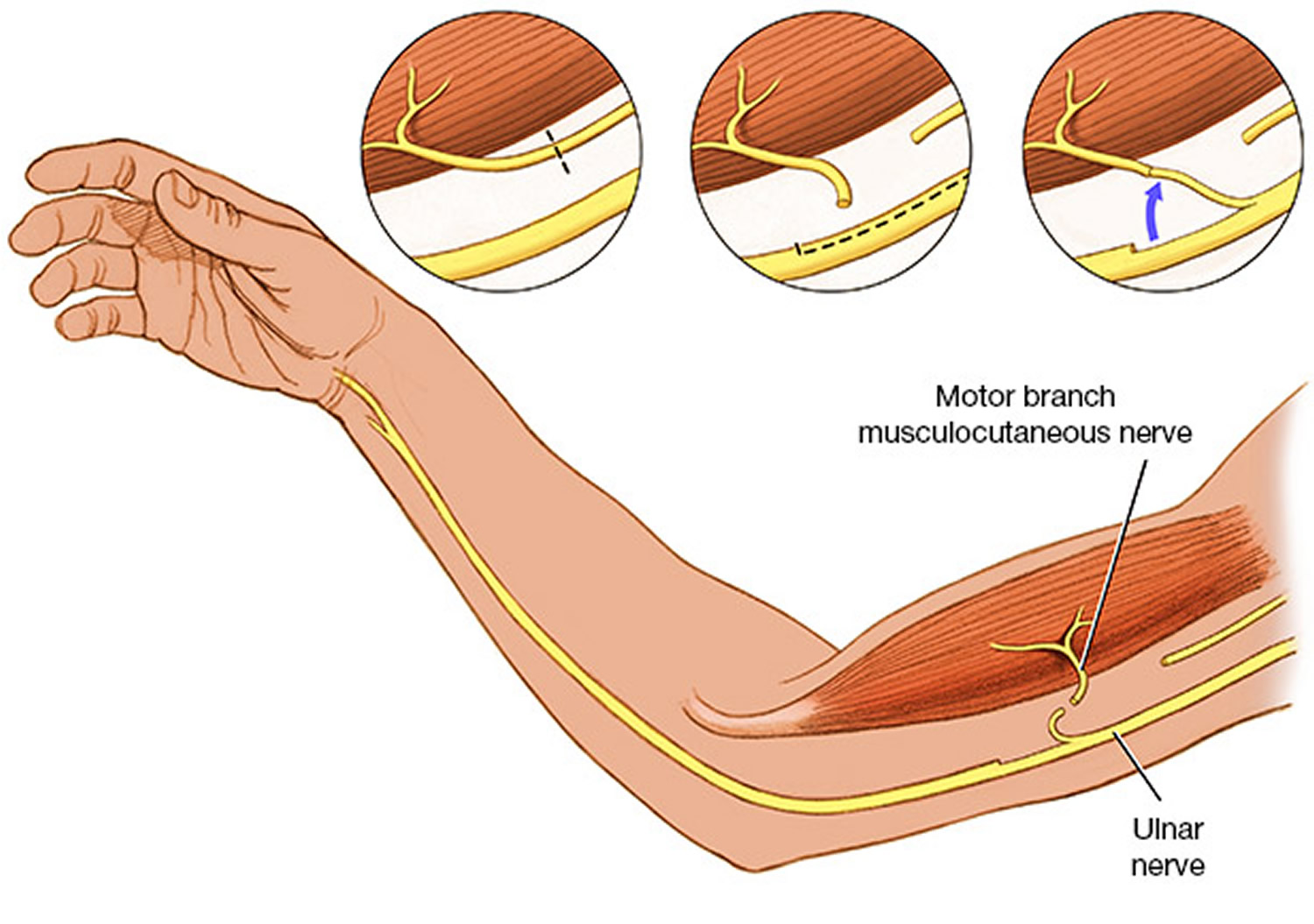
The entire protocol given above is without considering the additional use of distal nerve transfers in upper plexus lesion. Following the description by Oberlin 14 and Somsak 15 of nerve transfers for elbow flexion and deltoid reinnervation, the whole landscape in adult plexus injury changed dramatically. This philosophy is now coming in play in the birth brachial plexus injury reconstruction as well in selected cases. Oberlin 14 described the use of motor fascicles of the ulnar nerve for reinnervation of the biceps via the musculocutaneous nerve.
Subsequently, this has been modified to ulnar to biceps and median to brachialis. Somsak 15 described the use of the branch to long head of triceps for the anterior division of the axillary nerve to reinnervate the deltoid. The interesting point about distal transfers is the speed of neurotisation, since the nerve is coapted very close to the hilum of the muscle and the growing axons reach the end plates much faster.
In upper plexus lesions (C5, C6), these transfers allow for leaving the neuroma undisturbed and doing a triple transfer consisting of spinal accessory to suprascapular nerve, Oberlin and Somsak transfers to reconstruct shoulder abduction and external rotation, as well as elbow flexion. If the C7 is involved, then the triceps is often not functioning and the Somsak transfer is not possible; it also often means wrist extension is affected. In such cases, intercostal nerves can be used for the deltoid as described by Somsak 16 and intraplexal neurotisation can be used for the C7 posterior division to help reinnervate both triceps and wrist extension.
There is considerable disagreement about this. The two European doyens, Gilbert and Raimondi 17, argue that if roots are available, it is preferable to do a classical reinnervation and reserve distal transfers for later use. This allows reinnervation of all muscles supplied by those trunks/cords in a proper manner and yet leaves the distal transfers in reserve in case of unfavourable outcome. As mentioned earlier, distal transfers can be done at a late stage as they reach the muscle very rapidly. There is also no conclusive evidence in the form of a properly conducted prospective study to show that distal transfers give better results compared to classical neurotisation in the long run.
In the Indian scenario, distal transfers have a great benefit of targeting select muscles with no visible function without cutting the neuroma. Thus, for late referrals where some movements are seen, these are not lost even temporarily due to resection of the neuroma. This has social implications in this country because many parents and grandparents are not willing to risk losing existing movements (however inadequate they may be) to gain an eventual better result. Gilbert has reported similar social taboos in the Middle East.
Figure 6. Nerve transfer – Nerve transfers are particularly helpful in the most serious types of brachial plexus injuries, called avulsions, when the nerve root has been torn out of the spinal cord. They may also be used when surgeons are trying to speed up muscle recovery.
Secondary surgery
Secondary surgery is performed to treat either untreated older children or as a follow-up to primary nerve reconstruction. Secondary surgery involves surgery on shoulder, elbow as well as the hand.
Shoulder
Typically, shoulder surgery is performed to treat an internal rotation contracture combined with poor abduction. This is typically caused by co-contraction of abductors with adductors and internal with external rotators. The deltoid and supraspinatus along with the trapezius and serratus anterior are involved in various stages of shoulder abduction. The infraspinatus and teres minor are external rotators, while four big muscles, viz. pectoralis major, teres major, latissimus dorsi and subscapularis, are involved in adduction and internal rotation. In the recovering plexus (both natural and in those with nerve reconstruction), there is a tendency of mix-up of the growing axons to target muscles. This results in co-contraction of these groups. In such a battle, the four big muscles mentioned above are the invariable winners leading to an internal rotation contracture and an inability to abduct fully. If the anterior and posterior axillary folds of these children are felt during an attempted abduction, this co-contraction of one or both folds (containing the pectoralis major, teres major and latissimus dorsi, respectively) can be easily felt and helps determine the choice of muscle to release and transfer. Internal rotation contracture, if allowed to persist, leads to glenoid deformation and posterior subluxation of the humeral head. It is advisable to prevent this by early surgery in these instances to restore function and avoid deformity. Mallet’s score 18 is often used to assess the shoulder function before and after surgery (Table 3). Gilbert 19 also used a scoring system for shoulder (Table 5).
Table 4. The Mallet score
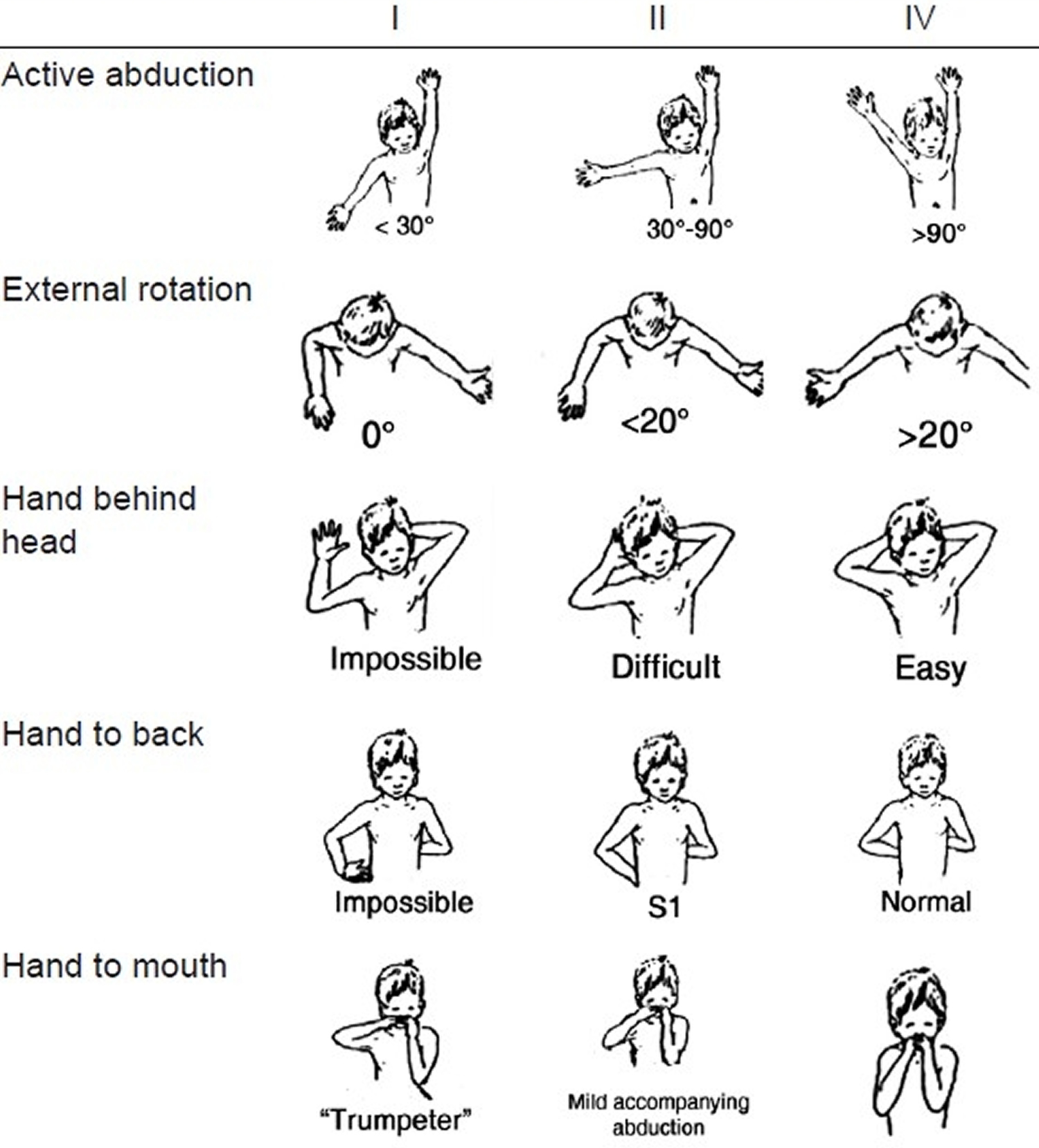
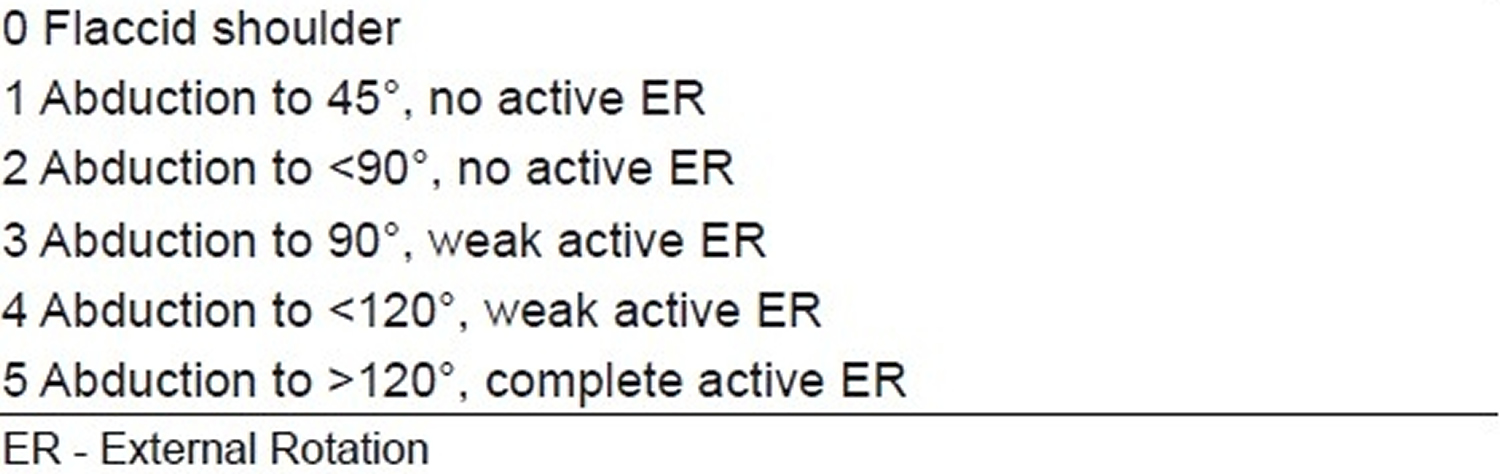
Table 5. Gilbert score for shoulder results
Elbow
Surgery is directed towards restoration of either flexion or extension. For elbow flexion, typical transfers are triceps to biceps and Steindler’s flexoroplasty. Rarely, an latissimus dorsi transfer can be theoretically used, but the author has no experience of it in birth brachial plexus injury. For extension, the transfer of choice is deltoid to triceps. The posterior half of the deltoid is detached and extended with fascia lata to attach it to the triceps insertion.
Hand
Raimondi 20 (Table 6) describes an excellent system of assessing the hand. A plethora of tendon transfers can be used to improve hand function. They are based on standard tendon transfers done for peripheral nerve lesions and very valuable insights gained through the voluminous Indian work on leprosy tendon transfers. But there are a few caveats for transfers in the hand following birth brachial plexus injury, given as follows:
- Birth brachial plexus injury cases have relatively weaker donors to achieve the desired function as the donor muscle too is often reinnervated. Full function, therefore, may not be achieved.
- Children keep recovering hand function for 3–4 years both naturally as well as after nerve surgery (unless of course you know that a particular nerve is not targeted at all).
- It is better to splint with appropriate splints in the interim.
- Start transfers only after about 3.5–4 years to get optimum results.
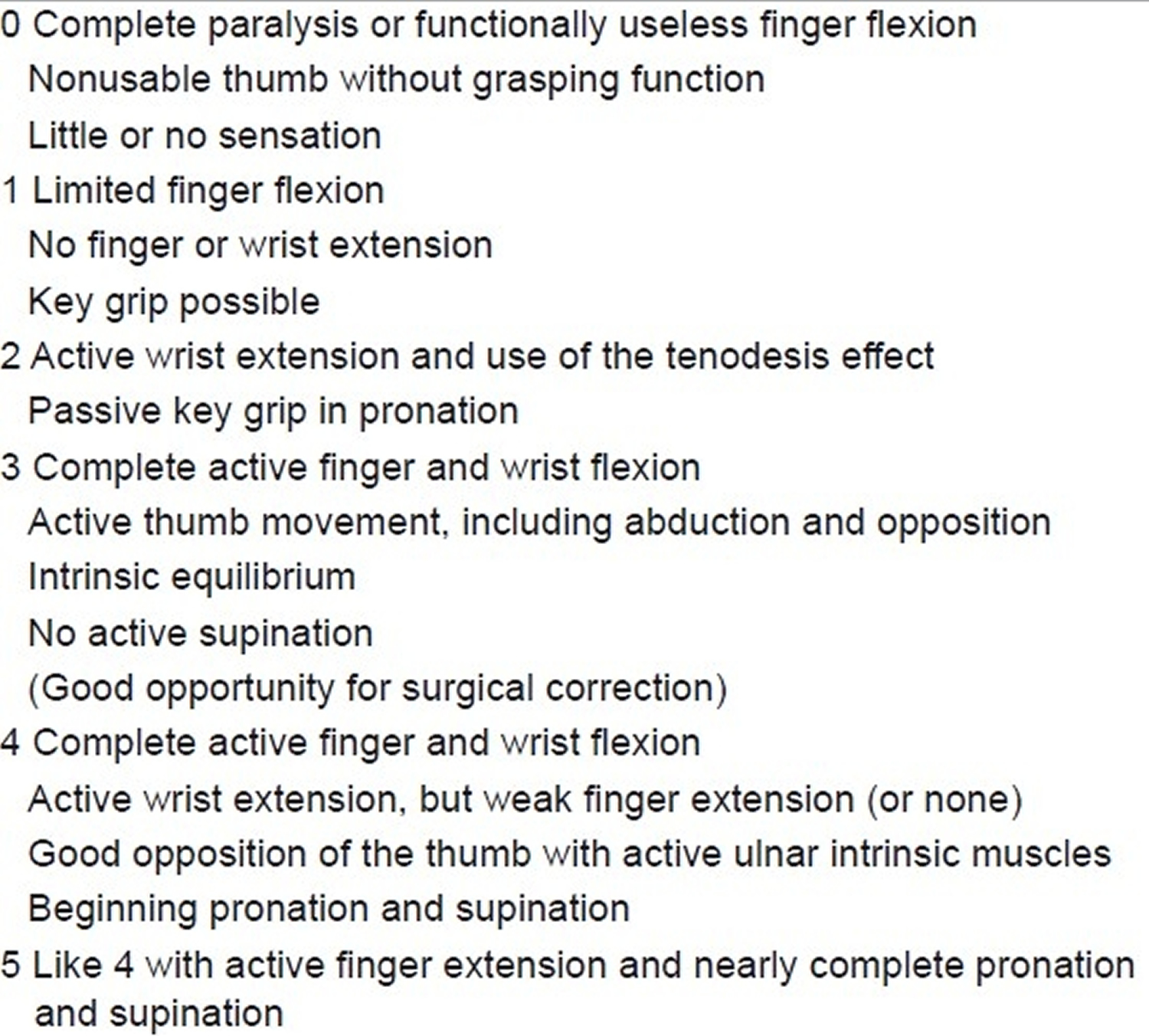
Table 6. Raimondi score for hand function
- Chater M, Camfield P, Camfield C. Erb’s palsy – Who is to blame and what will happen?. Paediatr Child Health. 2004;9(8):556-560. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724163/[↩][↩][↩][↩]
- Ali CDM, Madhani NB. Erb Palsy. [Updated 2018 May 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513260[↩][↩][↩][↩][↩]
- Low J, Reed A. Electrotherapy Explained Principles and Practice. 2nd ed. Linacre House, Jordan Hill, Oxford: Butterworth-Heinemann Ltd; 1994. Electrical stimulation of nerve and muscle; pp. 41–111. pp 393. OX2 8DP.[↩]
- Functional outcome of nerve transfer for restoration of shoulder and elbow function in upper brachial plexus injury. Venkatramani H, Bhardwaj P, Faruquee SR, Sabapathy SR. J Brachial Plex Peripher Nerve Inj. 2008 May 27; 3:15.[↩]
- Volpe JJ. Neurology of the newborn. 3rd Edn. Philadelphia, Pennsylvania: WB Saunders; 1995. pp. 781–4.[↩][↩][↩]
- Shenaq SM, Berzin E, Lee R, Laurent JP, Nath R, Nelson MR. Brachial plexus birth injuries and current management. Clin Plast Surg. 1998;25:527–36.[↩]
- Rehabilitation program for children with brachial plexus and peripheral nerve injury. Ramos LE, Zell JP. Semin Pediatr Neurol. 2000 Mar; 7(1):52-7.[↩]
- Rehabilitation pr ogram for children with brachial plexus and peripheral nerve injury. Ramos LE, Zell JP. Semin Pediatr Neurol. 2000 Mar; 7(1):52-7.[↩]
- A systematic review of brachial plexus surgery for birth-related brachial plexus injury. McNeely PD, Drake JM. Pediatr Neurosurg. 2003 Feb; 38(2):57-62.[↩]
- Tassin JL. Thesis. Paris: Universite Paris VII; 1983. Paralysies obstetricales du plexus brachial: Evolution spontanee, resultats des interventions reparatrices precoces.[↩]
- Clarke HM, Curtis CG. An approach to obstetrical brachial plexus injuries. Hand Clin. 1995;11:563–81. https://www.ncbi.nlm.nih.gov/pubmed/8567739[↩]
- Waters PM. Update on management of pediatric brachial plexus palsy. J Pediatr Orthop. 2005;25:116–26. https://www.ncbi.nlm.nih.gov/pubmed/15614072[↩]
- Thatte MR, Mehta R. Obstetric brachial plexus injury. Indian Journal of Plastic Surgery : Official Publication of the Association of Plastic Surgeons of India. 2011;44(3):380-389. doi:10.4103/0970-0358.90805. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3263264/[↩][↩][↩]
- Oberlin C, Beal D, Leechavengvongs S, Salon A, Dauge MC, Sarcy JJ. Nerve transfer to biceps muscle using a part of ulnar nerve for C5/C6 avulsion of the brachial plexus. Anatomical study and report of 4 cases. J Hand Surg. 1994;19:232–7. https://www.ncbi.nlm.nih.gov/pubmed/8201186[↩][↩]
- Leechavengvongs S, Witoonchart K, Uerpairojkit C, Thuvasethakul P. Nerve transfer to deltoid muscle using the nerve to the long head of the triceps, part II: A report of 7 cases. J Hand Surg Am. 2003;28:633–8. https://www.ncbi.nlm.nih.gov/pubmed/12877852[↩][↩]
- Malungpaishrope K, Leechavengvongs S, Uerpairojkit C, Witoonchart K, Jitprapaikulsarn S, Chongthammakun S. Nerve transfer to deltoid muscle using the intercostal nerves through the posterior approach: An anatomic study and two case reports. J Hand Surg Am. 2007;32:218–24. https://www.ncbi.nlm.nih.gov/pubmed/17275597[↩]
- Gilbert A, Raimondi P. Presentations in Club Narakas meeting Lisbon Mallet, J. Paralysie obstandricale. Revue de Chimrgie Orthopedique et Reparatrice de L’Appareil Moteur. 2011;58(Suppl):116.[↩]
- Pagnotta A, Haerle M, Gilbert A. Long-term results on abduction and external rotation of the shoulder after latissimus dorsi transferfor sequelae of obstetric palsy. Clin Orthop Relat R. 2004;426:199–205. https://www.ncbi.nlm.nih.gov/pubmed/15346074[↩]
- Thatte MR, Agashe MV, Rao A, Rathod CM, Mehta R. Clinical outcome of shoulder muscle transfer for shoulder deformities in obstetric brachial plexus palsy: A study of 150 cases. Indian J Plast Surg. 2011;44:21–8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3111117/[↩]
- Raimondi P. Presented at the International Meeting on Obstetric Brachial Plexus Palsy. The Netherlands: Heerlen; 1993. Evaluation of results in obstetric brachial plexus palsy: The hand.[↩]





{kind=link}