What is exostosis
Exostosis are benign bony protuberances with unknown etiology 1. Exostosis has accounted for 50 % of primary benign bone tumors and has been observed to occur at the metaphysis of long bones or originate from the surface of flat bones 2. Exostosis generally occurs at the proximal femoral or distal tibial metaphysis 3. Exostosis of the rib makes up a small proportion of the cases of exostosis 2. Solitary exostosis occurs in both infants and adults 2, and is generally asymptomatic. When an X-ray diagnosis of an asymptomatic case is not definitive, a CT or MRI scan is useful.
Primary exostosis occurs as solitary or multifocal lesions, and multiple exostosis is a hereditary disease that occurs in infants 4. Hereditary multiple exostoses also referred to as diaphyseal aclasis or familial osteochondromatosis. is a rare disorder that is characterized by benign cartilaginous tumors called exostoses that form next to growing skeletal elements 5. Hereditary multiple exostoses is a rare autosomal dominant skeletal disorder with almost complete penetrance (95%) due to loss of functional mutations in two genes: exostosin-1 (EXT-1) and exostosin-2 (EXT-2) genotypes 6. Hereditary multiple exostoses is manifested by skeletal deformities caused by abnormal bone growth 4.
Hereditary multiple exostoses has an estimated prevalence of 1 per 50,000 individuals in Caucasians who are the most common race affected 7. The incidence in the Western population is only 1.5%, with a male : female (M : F) ratio of 1.5 : 1 8. These genes are linked to heparan sulfate synthesis, but the specific molecular mechanisms leading to the disruption of the cartilage structure and the consequent formation of exostoses is not yet clearly understood 9. However, heparan sulfate is an essential component of the body and is present in the growth plates. Heparan sulfate has numerous functions including regulation of the distribution and availability of the growth and signal proteins and their respective interactions 10. Osteocartilaginous exostoses (Osteochrondromas) arise from the epiphyses of long bones as exophytic lesions. The exostoses are a result of dysplasia in the peripheral part of the growth plate. The bones that are most commonly affected are the lower femur, upper tibia (i.e., around the knee), and upper humerus but may also be found in other bones like the scapula and ilium where they can be missed clinically 11. Facial bones are not affected as they grow by intramembranous ossification. An osteochondroma is a benign cartilage-capped bony outgrowth which may present as sessile or pedunculated 12. It is made up of cortex and marrow cavity that are continuous with the host bone. The pedunculated osteochondromas are always directed away from the growth plate and the joint. The most common site for the osteochondromas is the lateral side of the most active growth plate of a long bone. Osteochondromas grow and increase in size in childhood until closure of the growth plate 13.
The osteochondromas tend to become symptomatic around 3 years of age. Most of the affected children will experience pain and restricted joint motion. Some exostoses can also interfere with normal growth plate development, giving rise to limb deformities and eventual limb shortening. Boys are most commonly affected and clinical attention is usually sought when the exostoses compress a nerve or blood vessel and in rare circumstances when there is malignant transformation. In the majority of cases, they complicate as chondrosarcomas. However, other tumor types (osteosarcoma, malignant fibrous histiocytomas, and fibrosarcomas) have also been seen. However these are rare 14. Malignant transformation has only been reported in the literature only about thirteen times, making it a very rare occurrence. A recent study has also shown that moderate defects or osteochondroma-like outgrowths are present in the cranial base of hereditary multiple exostoses patients 15.
The prognosis of patients with hereditary multiple exostoses that develop osteoblastic osteosarcoma is good when the disease is localized and is managed by a multidisciplinary team of orthopaedic surgeon, radiologist, pathologist, geneticist, and an oncologist. Bone conserving treatment when instituted spares the affected limb. Further management will include insertion of a bone prosthesis to ensure bone strengthening and stability at the tumor site after chemotherapy.
Exostosis ear
External auditory canal exostoses are the most common benign (harmless) tumors of the external auditory canal, and their pathology is attributed to bony outgrowths that arise from the tympanic portion of the temporal bone 16. These benign tumors are caused by prolonged and repeated exposure to cold water (particularly below 19ºC) 17. It is known as “surfer’s ears”, because 59.8%–73.5% of surfers have evidence of this condition 17. Professional surfers are more likely to have exostosis compared with amateur surfers. Although such exostoses are usually asymptomatic, they can cause recurrent otitis externa, ear fullness, hearing loss, ear pain, tinnitus, itching, and a sensation of blockage in affected ears on progression 18.
Surfer’s exostoses are more commonly seen in individuals who participate frequently in aquatic activities 19 and are thought to be caused by repeated exposure to cold water and wind 20. It has been suggested that repeated cold water exposure leads to a recurrent periostitis 20 and an increase in osteoblastic activity 21 resulting in hyperostosis 22 and formation of exostoses. It has been shown that those who participate in cold-water surfing are more likely to develop external auditory canal exostosis, and that with an increasing length of exposure to cold water (in years) there is an increase in the severity of lesions 23. As such, surfer’s exostoses are so named because of those individuals who develop these lesions, a significant proportion are cold-water surfers 23.
There is probably a geographical tendency to develop these lesions; if one lives in a coastal region, one may be more likely to surf or to be exposed to the conditions which encourage exostoses to develop. Indeed, this appears to be reflected in the populations examined in the literature 24. It is difficult to ascertain the true age and gender prevalence of external auditory canal exostoses given that anyone can participate in aquatic sports such as cold-water surfing. However, one study found that Australian male surfers were more likely to develop these lesions than females 25. However, while more men were included in the study (which may reflect actual participation in this sport), the likelihood and severity of developing these lesions depended on the number of years surfed, as discussed above 25.
The majority of patients are asymptomatic and aural care to microsuction impacted wax and debris is only required infrequently. Those with exostoses severely obstructing the external auditory canal are prone to recurrent episodes of otitis externa and related conductive hearing loss 26; surgical resection is considered when there is severe external auditory canal obstruction, along with severely symptomatic patients 27. When surfers are made aware of the risk of developing external auditory canal exostosis, the use of preventative measures (e.g. ear plugs) increases 28, advocating an increased awareness of this condition in this population and the healthcare professionals who treat them.
The main differential diagnosis for external auditory canal exostosis is an external auditory canal osteoma 29. These lesions are usually pedunculated, arise from bony cartilaginous junctions and given that they are slow growing, are usually asymptomatic and discovered incidentally (i.e. high-resolution computed tomography of the temporal bones performed for another indication) 30. Among cancers of the external auditory canal, squamous cell carcinoma is the most frequent. These cancers typically have symptoms such as ear discharge and ear pain. The tumor is unilateral, hemorrhagic, and progressive. Bilateral and multiple lesions are rare. Nevus cell nevus is a unilateral, sessile, single black torose. Bilateral or multiple lesions are rare. The average size is about 10 mm, but a giant tumor may protrude from the auricle. Although frequent symptoms are ear fullness or hearing loss, asymptomatic cases are also found. The pathology of ostosis is attributed to ossification of the connective tissue. However, the accurate pathology is unclear. The tumor is single, unilateral and pedunculated with a smooth surface; multiple and bilateral lesions are rare. Gradual progression of the disease is accompanied by symptoms of ear fullness and hearing loss.
Figure 1. Exostosis ear
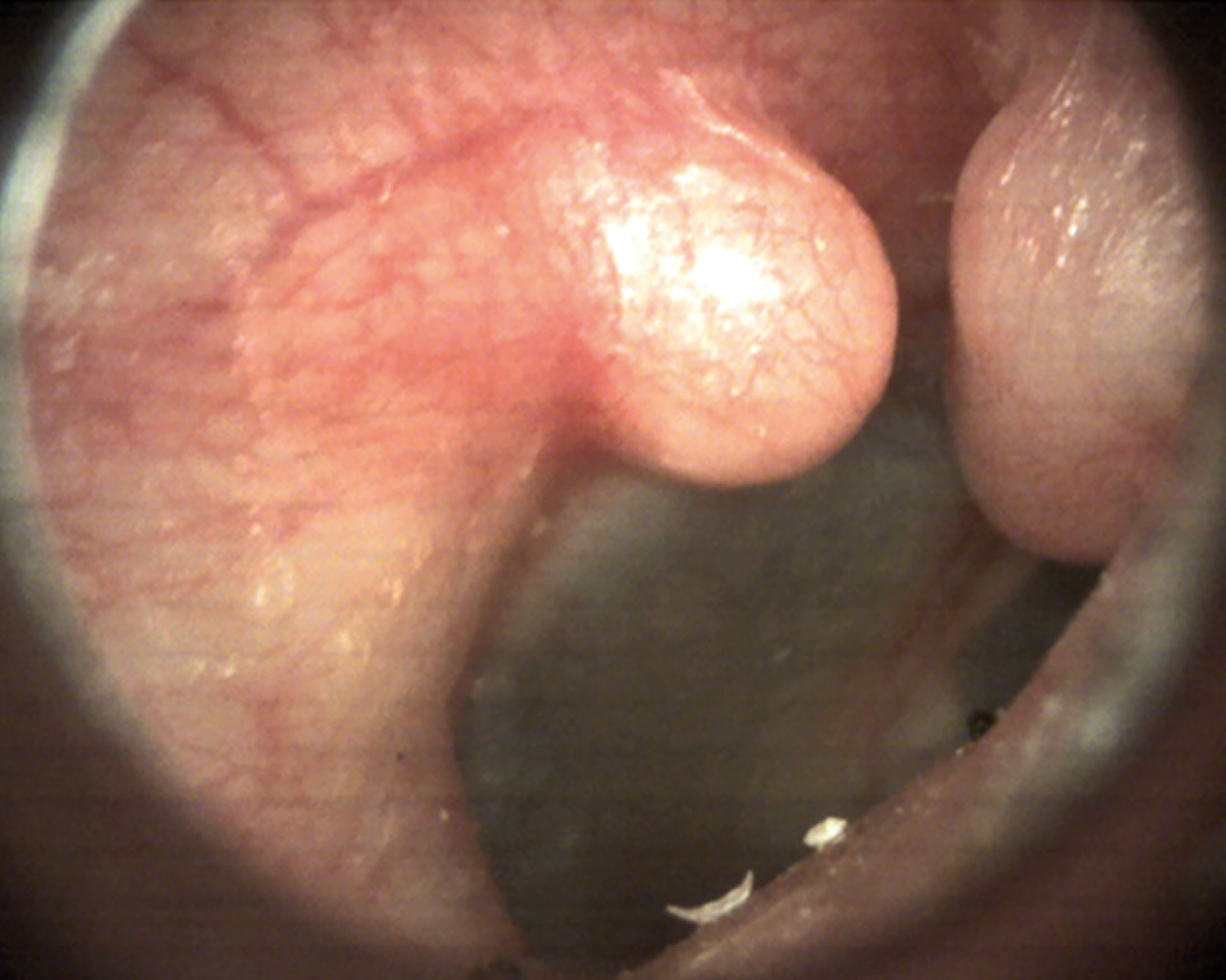
Foonote: Photograph of a right external auditory canal exostosis in a 48-year-old, healthy man, who had been a cold-water surfer for 20 years presented with a 5-year history of a sensation of blockage in his ears while swimming.
[Source 29]Subungual exostosis
A subungual exostosis is a rare and benign bony overgrowth that is permanently attached to the tip of the toe 31. It was first described by Dupuytren, who observed subungual exostosis on toes; Hutchinson later reported subungual exostosis on fingertips 32. The pathology of subungual exostosis differs from that of osteocartilaginous exostoses. Subungual exostosis usually involves the overgrowth of normal bone, which may occur beneath the toenail or on the side of the toe, and can obstruct nail growth 33. While chronic irritation is thought to be the cause of metaplasia in fibrocartilage, the pathogenesis remains unknown. According to the literature, trauma, chronic infection, tumor, hereditary anomalies and the activation of a cartilaginous cyst are all possible causes 34. Some studies have reported that trauma is the main contributing factor in the development of subungual exostosis, with subsequent acute and chronic inflammation causing cartilaginous metaplasia 35. An alternative view is that chronic infection is the result and not the cause of subungual exostosis 36.
Subungual exostosis is most commonly diagnosed in children and young adults; most of these lesions are located in the big toe, although they can occur (albeit infrequently) in other toes 33. Only a small percentage of these lesions occur in the fingers 34. Regarding its pathology, subungual exostosis commonly presents as swelling beneath the nail, causing separation between the nail and toe. It is frequently misdiagnosed and incorrectly treated.
Microscopic findings include trabecular bone formation at the basement layer and a proliferating fibrocartilaginous cap. Immature subungual exostosis usually involves a thick cartilaginous layer, while mature lesions have a thin cartilaginous layer. Mature lesions consist mainly of trabecular bone tissue. The cartilaginous cap includes mitotic hypercellularity and dense nuclei. Although these findings suggest malignancy, the lack of anaplasia indicates that the lesions are benign 37. The differential diagnosis includes a wide range of benign and malignant tumours, skin lesions, chronic infections, soft tissue and nail pathologies. Radiological findings generally provide sufficient information for diagnosis 33. Magnetic resonance imaging (MRI) is helpful in the diagnosis of subungual exostosis due to its ability to detect the different signal formations of tumors 38.
Figure 2. Subungual exostosis (located in the 3rd toe of the right foot)

Retrocalcaneal exostosis
Retrocalcaneal exostosis also known as Haglund’s deformity, was first described in 1928 by Patrick Haglund 39, is a chronic enlargement of the posterior-superior prominence of the calcaneum, where there is a bony enlargement at the attachment of the Achilles tendon 40. Retrocalcaneal exostosis is a normal anatomical variant often referred to as the Mulholland deformity or ‘pump bump’ as adjoining soft tissues can get irritated when this bony lump rubs against rigid shoes especially by footwear with rigid backs such as pumps leading to insertional Achilles tendinitis 41. Retrocalcaneal exostosis often leads to retrocalcaneal bursitis, calcaneal tendon bursitis, and thickening and inflammation of the calcaneal tendon. This combination of pathology is known as Haglund’s syndrome. Inflammation of the different parts of soft tissue in the area can lead to an isolated condition; however, the treatment options are different in these conditions, and so they should be differentiated.
Although a very common clinical condition, retrocalcaneal exostosis is still poorly understood 42. Retrocalcaneal exostosis has no definitive cause, but various probable causes like a tight Achilles tendon, a high arch of the foot, and heredity have been proposed. It usually affects middle-aged people, females more than males, and it is often bilateral. Retrocalcaneal exostosis is characterized by pain in the back of the heel, which is more after rest. Clinical evaluation and lateral radiographs of the ankle are mostly enough to make a diagnosis of Haglund’s syndrome. The pain could be due to associated Achilles tendonitis and retrocalcaneal bursitis 43. This condition can mimic other causes of hind foot pain like isolated retrocalcaneal bursitis, plantar fasciitis, and seronegative spondyloarthropathies 44.
Retrocalcaneal exostosis is often treated conservatively by reassessment of the shoe of the patient and heel pads or heel lifts in the cases of high arched feet 45 . Casting may be necessary for pain reduction and an ice bag may be necessary to deal with swelling. Anti-inflammatory drugs (oral or topical), stretching exercises, and physiotherapy may relieve tension from the calcaneal tendon. Local perilesional steroid injections are also used in refractory cases 46.
If conservative treatment is not effective then surgical excision of the bony exostoses of the calcaneum is only required in resistant cases. Surgical treatment options like retrocalcaneal decompression and calcaneal ostectomy or osteotomy are used 47. Inadequate bone resection can lead to the recurrence of symptoms 48.
Figure 3. Retrocalcaneal exostosis (Haglund’s deformity)
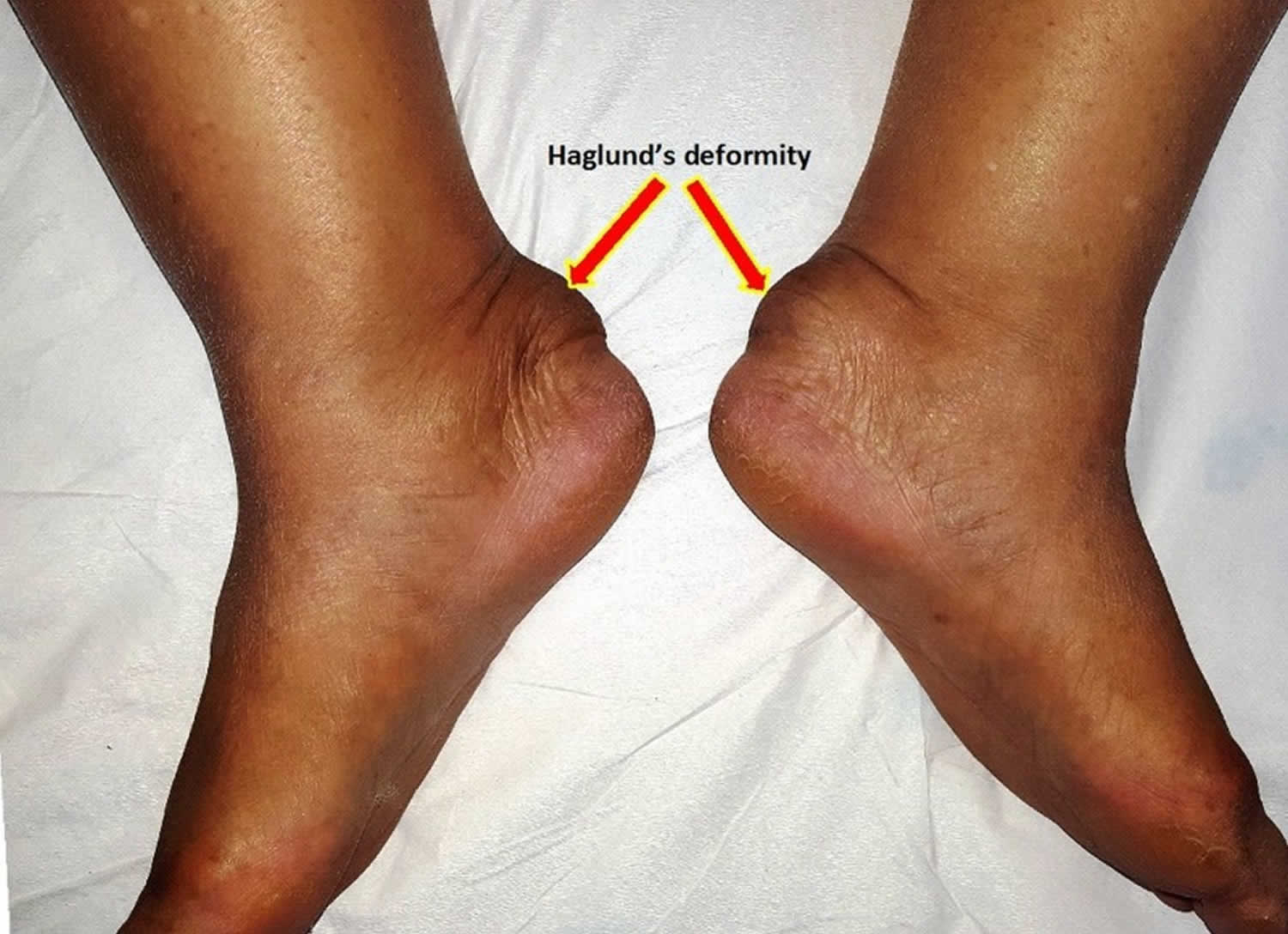
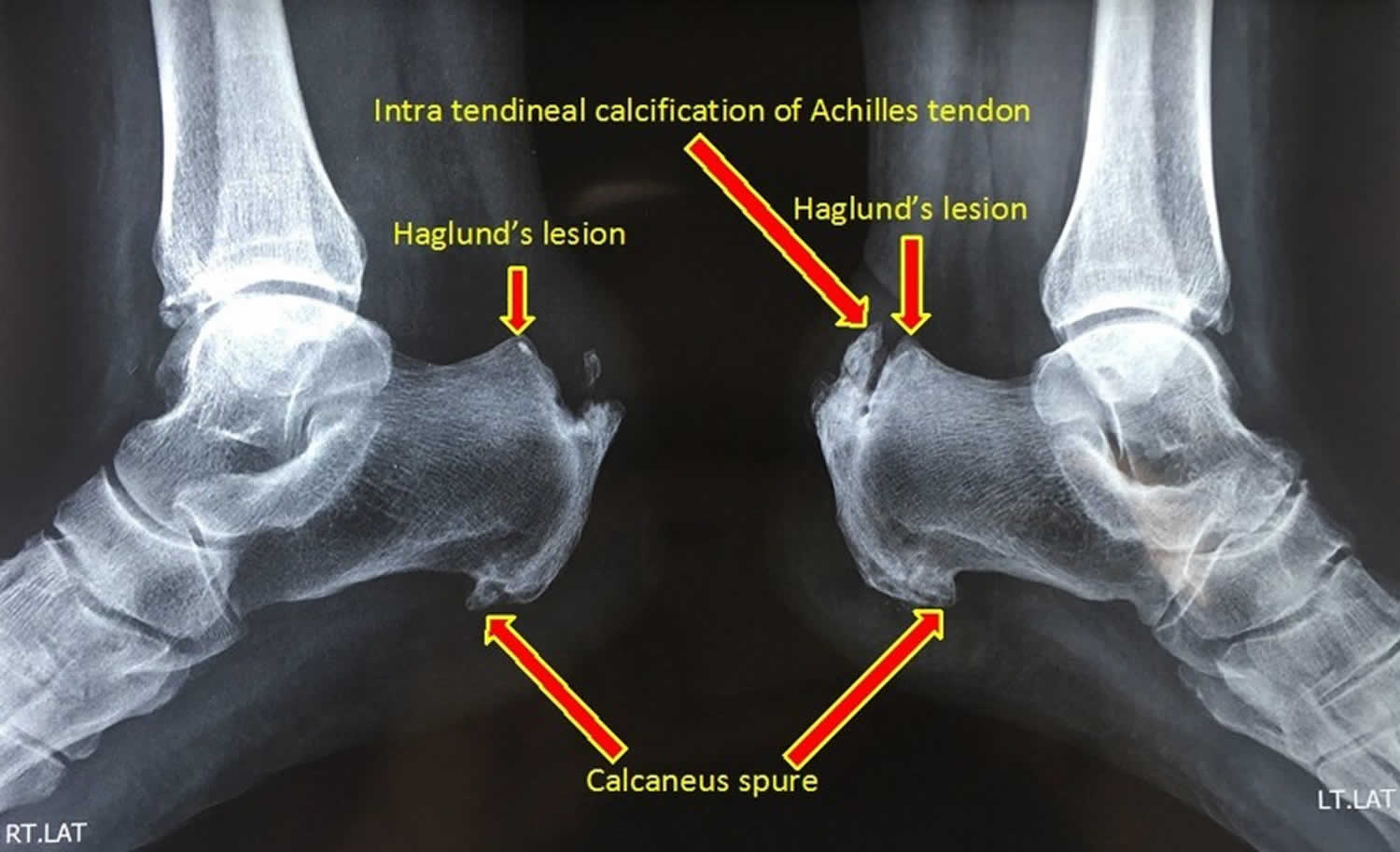
Footnote: Lateral radiograph of ankles showing bony enlargement at the posterosuperior aspect of both calcaneum
[Source 42]Buccal exostosis
Buccal exostoses are benign bilateral, smooth surface growth occurring on the outer or facial surface of the maxilla and less commonly, the mandible, found usually in the premolar and molar region 49. The cause is still not established, but it has been suggested that the bony overgrowth can be because of abnormally increased masticatory forces to the teeth or outcome of a mild, chronic periosteal inflammation 49. Buccal exostoses tend to appear in early adolescence and early adult years and may very slowly increase in size with time. Buccal exostoses are painless, self-limiting and may increase patient concern about poor esthetics, inability to perform oral hygiene procedures, and compromised periodontal health by causing food lodgment.
Buccal exostoses are normally self-limiting and painless. Their size may increase to several centimeters thus contributing to periodontal disease of adjoining teeth by retaining food during chewing instead of flushing away. Usually no treatment is required, but for those possibly affecting the periodontal condition, or when the protruberances cause pain or discomfort to the patient, or when these bony enlargements cause pseudo swelling over the lip, then conservative surgical excision can be performed.
The diagnosis of a buccal exostosis is based on clinical and radiographic findings. An additional biopsy for diagnostic support is usually not recommended 49. It remains important to distinguish exostoses from early osseosarcomas and chondrosarcomas. Furthermore, the patients with multiple bony growths, not in the classic buccal exostoses locations should be evaluated for Gardner’s syndrome. Intestinal polyposis and cutaneous cysts or fibromas are other common features of the autosomal dominant Gardner’s syndrome 50.
Neither the torus nor the bony exostosis require treatment unless it becomes large enough to interfere with function, denture placement, cause recurring traumatic surface ulceration (usually from sharp food such as potato chips or fish bones) or as used to get autograft as it is a potent donor site 51. When treatment is elected, the bony mass may be removed using bone cutting bur or chiseled off through the base of the lesion.
Figure 4. Buccal exostosis

Figure 5. Mouth exostosis
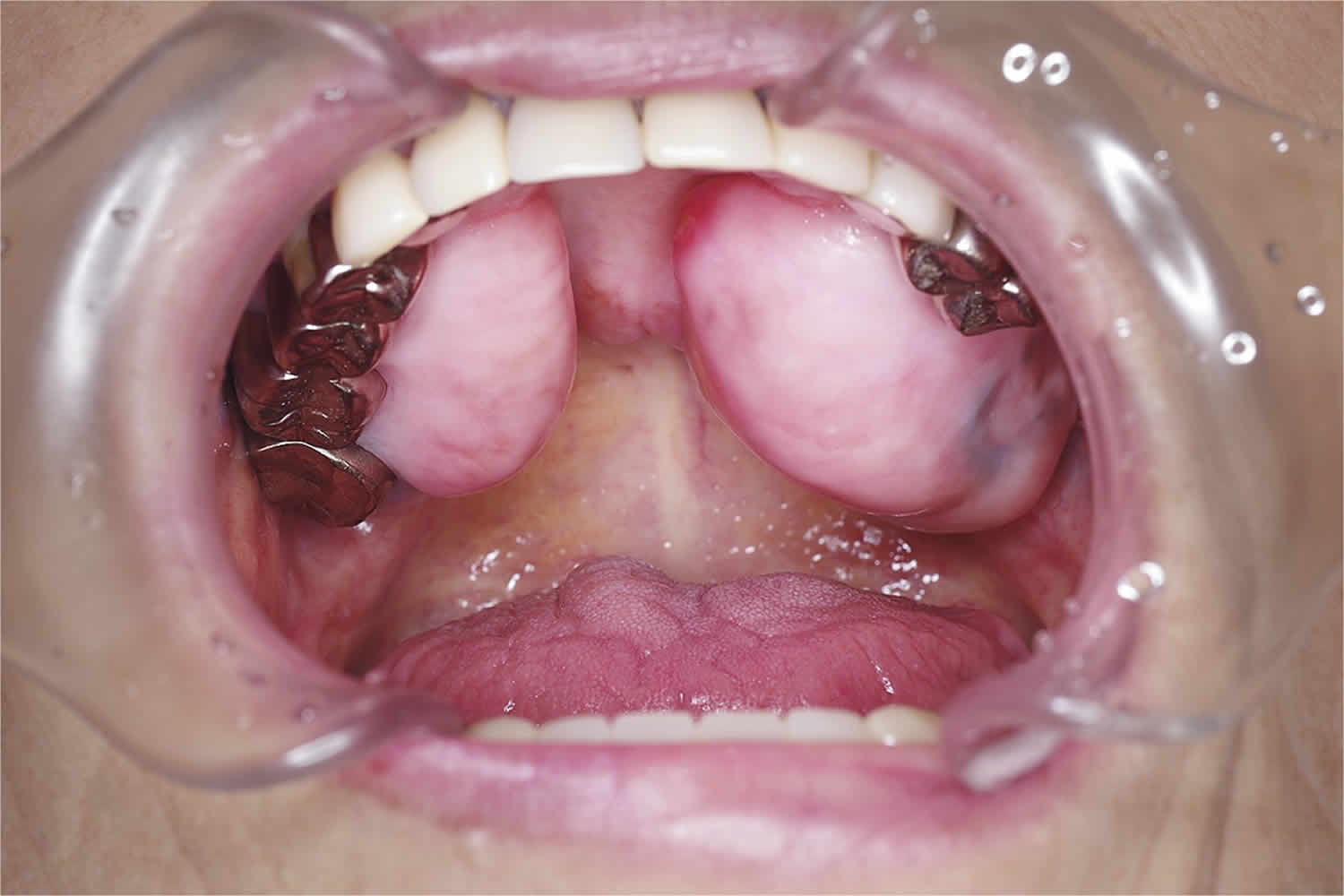
Footnote: In this 73-year-old woman, oral exostosis had been present since childhood without any disturbance in her daily life and was an incidental finding
[Source 52]- Kumar Singh A, Sulugodu Ramachandra S, Arora S, Dicksit DD, Kalyan CG, Singh P. Prevalence of oral tori and exostosis in Malaysian population – A cross-sectional study. Journal of Oral Biology and Craniofacial Research. 2017;7(3):158-160. doi:10.1016/j.jobcr.2017.08.008. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5670296/[↩]
- Khosla A, Parry RL. Costal osteochondroma causing pneumothorax in an adolescent: a case report and review of the literature. J Pediatr Surg. 2010;45:2250–3. doi: 10.1016/j.jpedsurg.2010.06.045.[↩][↩][↩]
- Reynolds JR, Morgan E. Haemothorax caused by a solitary costal exostosis. Thorax. 1990;45:68–9. doi: 10.1136/thx.45.1.68.[↩]
- Cowles RA, Rowe DH, Arkovitz MS. Hereditary multiple exostoses of the ribs: an unusual cause of hemothorax and pericardial effusion. J Pediatr Surg. 2005;40:1197–200. doi: 10.1016/j.jpedsurg.2005.03.064[↩][↩]
- Huegel J, Enomoto-Iwamoto M, Sgariglia F, Koyama E, Pacifici M. Heparanase Stimulates Chondrogenesis and Is Up-Regulated in Human Ectopic Cartilage: A Mechanism Possibly Involved in Hereditary Multiple Exostoses. The American Journal of Pathology. 2015;185(6):1676-1685. doi:10.1016/j.ajpath.2015.02.014. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450318/[↩]
- EXT-mutation analysis and loss of heterozygosity in sporadic and hereditary osteochondromas and secondary chondrosarcomas. Bovée JV, Cleton-Jansen AM, Wuyts W, Caethoven G, Taminiau AH, Bakker E, Van Hul W, Cornelisse CJ, Hogendoorn PC. Am J Hum Genet. 1999 Sep; 65(3):689-98.[↩]
- Bukara E, Buteera AM, Karakire R, et al. Osteoblastic Osteosarcoma Arising beneath an Osteochondroma in an 11-Year-Old Male with Multiple Hereditary Exostoses. Case Reports in Orthopedics. 2018;2018:8280415. doi:10.1155/2018/8280415. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6079448/[↩]
- Ryckx A., Somers J., Allaert L. Hereditary multiple exostosis. Acta Orthopaedica Belgica. 2013;79(6):597–607[↩]
- Lind T., Tufaro F., McCormick C., Lindahl U., Lidholt K. The putative tumor suppressors EXT1 and EXT2 are glycosyltransferases required for the biosynthesis of heparan sulfate. Journal of Biological Chemistry. 1998;273(41):26265–26268. doi: 10.1074/jbc.273.41.26265.[↩]
- Zak B. M., Schuksz M., Koyama E., et al. Compound heterozygous loss of Ext1 and Ext2 is sufficient for formation of multiple exostoses in mouse ribs and long bones. Bone. 2011;48(5):979–987. doi: 10.1016/j.bone.2011.02.001[↩]
- Bovée J. V. M. G. Multiple osteochondromas. Orphanet Journal of Rare Diseases. 2008;3(1):p. 3. doi: 10.1186/1750-1172-3-3[↩]
- Murphey M. D., Choi J. J., Kransdorf M. J., Flemming D. J., Gannon F. H. Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation. Radiographics. 2000;20(5):1407–1434. doi: 10.1148/radiographics.20.5.g00se171407[↩]
- Resnick D., Kyriakos M., Greenway G. D. Osteochondroma. In: Resnick D., editor. Diagnosis of Bone and Joint Disorders. 3rd. Philadelphia, PA, USA: Saunders; 1995. pp. 3725–3746.[↩]
- Lamovec J., Spiler M., Jevtic V. Osteosarcoma arising in a solitary osteochondroma of the fibula. Archives of Pathology & Laboratory Medicine. 1999;123(9):832–834 https://www.ncbi.nlm.nih.gov/pubmed/10458834[↩]
- Sinha S., Mundy C., Bechtold T., et al. Unsuspected osteochondroma-like outgrowths in the cranial base of hereditary multiple exostoses patients and modeling and treatment with a BMP antagonist in mice. PLoS Genetics. 2017;13(4, article e1006742) doi: 10.1371/journal.pgen.1006742[↩]
- Kutz JWJrFayad JN. Exostosis of the external auditory canal. Ear Nose Throat J 2006; 85:142.[↩]
- Alexander VLau ABeaumont EHope A. The effects of surfing behavior on the development of external auditory canal exostosis. Eur Arch Otorhinolaryngol 2015; 272:1643–9.[↩][↩]
- John WHEric PW. External auditory exostoses: Evaluation and treatment. Head and Neck Surgery 2008; 138:672–8.[↩]
- Wong B.J., Cervantes W., Doyle K.J., Karamzadeh A.M., Boys P., Brauel G. Prevalence of external auditory canal exostoses in surfers. Arch Otolaryngol Head Neck Surg. 1999;125(9):969–972.[↩]
- Barbon D.A., Hegde R., Li S., Abdelbaki A., Baja D. Bilateral external auditory exostoses causing conductive hearing loss: a case report and literature review of the surfer’s ear. Cureus. 2017;9(10):e1810.[↩][↩]
- Attlmayr B., Smith I.M. Prevalence of ‘surfer‘s ear’ in Cornish surfers. J Laryngol Otol. 2015;129(5):440–444.[↩]
- Kutz J.W., Jr, Fayad J.N. Exostosis of the external auditory canal. Ear Nose Throat J. 2006;85(3):142.[↩]
- Alexander V., Lau A., Beaumont E., Hope A. The effects of surfing behaviour on the development of external auditory canal exostosis. Eur Arch Otorhinolaryngol. 2015;272(7):1643–1649.[↩][↩]
- Paddock M, Lau K, Raghavan A, Dritsoula A. Surfer’s exostosis in a child who does not surf. Radiology Case Reports. 2018;13(3):531-533. doi:10.1016/j.radcr.2018.02.010. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5966629/[↩]
- Hurst W., Bailey M., Hurst B. Prevalence of external auditory canal exostoses in Australian surfboard riders. J Laryngol Otol. 2004;118(5):348–351.[↩][↩]
- Kroon D.F., Lawson M.L., Derkay C.S., Hoffmann K., McCook J. Surfer’s ear: external auditory exostoses are more prevalent in cold water surfers. Otolaryngol Head Neck Surg. 2002;126(5):499–504.[↩]
- Altuna Mariezkurrena X., Vea Orte J.C., Camacho Arrioaga J.J., Algaba Guimerá J. Surgical treatment of exostosis in the external auditory canal. Acta Otorrinolaringol Esp. 2006;57(6):257–261.[↩]
- Reddy V.M., Lau A.S., Abdelrahman T., Flanagan P.M. Surfers’ awareness of the preventability of ‘surfer‘s ear’ and use of water precautions. J Laryngol Otol. 2011;125(6):551–553.[↩]
- Y. Hirose, K. Shikino, M. Ikusaka; Surfer’s ear and external auditory canal exostoses, QJM: An International Journal of Medicine, Volume 109, Issue 11, 1 November 2016, Pages 759, https://doi.org/10.1093/qjmed/hcw148[↩][↩]
- Sente M. External auditory canal osteoma. Srp Arh Celok Lek. 2009;137(1–2):73–76.[↩]
- Malkoc M, Korkmaz O, Keskinbora M, et al. Surgical treatment of nail bed subungual exostosis. Singapore Medical Journal. 2016;57(11):630-633. doi:10.11622/smedj.2015180. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5331139/[↩][↩]
- Hutchinson J. Subungual exostosis of the great toe: excision with success. Lancet. 1857;2:246–7.[↩]
- Evison G, Price CH. Subungual exostosis. Br J Radiol. 1966;39:451–5.[↩][↩][↩]
- Carroll RE, Chance JT, Inan Y. Subungual exostosis in the hand. J Hand Surg Br. 1992;17:569–74.[↩][↩]
- Ilyas W, Geskin L, Joseph AK, Seraly MP. Subungual exostosis of the third toe. J Am Acad Dermatol. 2001;45(6 Suppl):S200–1.[↩]
- Landon GC, Johnson KA, Dahlin DC. Subungual exostoses. J Bone Joint Surg Am. 1979;61:256–9.[↩]
- Resnick D, Kyriakos M, Greenway GD. Tumors and tumor-like lesions of bone: imaging and pathology of specific lesions. In: Resnick D, editor. Diagnosis of Bone and Joint Disorders. Philadelphia: WB Saunders Company; 1995. pp. 3628–938.[↩]
- Teh J, Whiteley G. MRI of soft tissue masses of the hand and wrist. Br J Radiol. 2007;80:47–63.[↩]
- Haglund P. Beitrag zur Klinik der Achillesshne. Arch Orthop Chir 1928;2013:49[↩]
- Haglund’s syndrome. Sella EJ, Caminear DS, McLarney EA. J Foot Ankle Surg. 1998 Mar-Apr; 37(2):110-4; discussion 173. https://www.ncbi.nlm.nih.gov/pubmed/9571457/[↩]
- Gillott E, Ray P. Tuberculosis of the calcaneum masquerading as Haglund’s deformity: a rare case and brief literature review. BMJ Case Reports. 2013;2013:bcr2013009252. doi:10.1136/bcr-2013-009252. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3669966/[↩]
- Vaishya R, Agarwal AK, Azizi AT, Vijay V. Haglund’s Syndrome: A Commonly Seen Mysterious Condition. Muacevic A, Adler JR, eds. Cureus. 2016;8(10):e820. doi:10.7759/cureus.820. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5101401/[↩][↩]
- Haglund’s syndrome. Two case reports. [Article in English, Spanish] Jiménez Martín F, Alonso Valdazo MD, Díaz Peña G, Fernández Leroy J, Hernández Herrero D, Díaz García F. Rheumatol Clin. 2016:0–6.[↩]
- Haglund syndrome with pump bump. Kucuksen S, Karahan AY, Erol K. Med Arch. 2012; 66(6):425-7.[↩]
- Haglund’s deformity and retrocalcaneal bursitis. Stephens MM. Orthop Clin North Am. 1994 Jan; 25(1):41-6.[↩]
- Haglund’s syndrome. Sella EJ, Caminear DS, McLarney EA. J Foot Ankle Surg. 1998 Mar-Apr; 37(2):110-4; discussion 173.[↩]
- Comparison of results of retrocalcaneal decompression for retrocalcaneal bursitis and insertional achilles tendinosis with calcific spur. Watson AD, Anderson RB, Davis WH. Foot Ankle Int. 2000 Aug; 21(8):638-42.[↩]
- Understanding the pathologic Haglund’s deformity. Reinherz RP, Smith BA, Henning KE. J Foot Surg. 1990 Sep-Oct; 29(5):432-5.[↩]
- Medsinge SV, Kohad R, Budhiraja H, Singh A, Gurha S, Sharma A. Buccal Exostosis: A Rare Entity. Journal of International Oral Health : JIOH. 2015;7(5):62-64. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4441241/[↩][↩][↩][↩]
- Jainkittivong A, Langlais RP. Buccal and palatal exostoses: Prevalence and concurrence with tori. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(1):48–53.[↩]
- Puttaswamaiah RN, Galgali SR, Gowda VS. Exostosis: a donor site for autograft. Indian J Dent Res. 2011;22(6):860–2.[↩]
- Oral Maxillary Exostosis. N Engl J Med 2015; 373:1457 https://www.nejm.org/doi/full/10.1056/NEJMicm1414626[↩]





{kind=link}