
Contents
What is failure to thrive
Failure to thrive is defined as decelerated or arrested physical growth (height and weight measurements fall below the third or fifth percentile, or a downward change in growth across two major growth percentiles) and is associated with abnormal growth and development 1. Failure to thrive is defined as children or baby who don’t meet the expected standards of weight gain and have poor linear (height) growth within the first few years of life 2. Many things can cause failure to thrive, including illnesses and eating problems or inadequate nutrition. Once doctors find the cause of the problem, they can work with families to help get a child back into a healthy growth pattern.
Failure to thrive lacks a clear definition, in part because it’s not a disease or disorder itself. Previously, failure to thrive was categorized as either organic (underlying medical condition) or non-organic (no known medical condition). However, this categorization is considered outdated as the causes and effects of malnutrition are usually intertwined in most children. Rather, failure to thrive is a sign that a child is undernourished. In general, children who fail to thrive don’t receive or cannot take in, keep, or use the calories that would help them grow and gain enough weight.
Doctors usually diagnose failure to thrive in infants and toddlers — an important time of physical and mental development. After birth, a child’s brain grows as much in the first year as it will grow for the rest of a child’s life. Poor nutrition during this period may have lasting harmful effects on brain development.
Most babies double their birth weight by 4 months and triple it by age 1, but children who fail to thrive usually don’t meet those milestones. Sometimes, a child who starts out “plump” and seems to be growing well may gain less weight later. After a while, height growth may slow as well.
If failure to thrive continues, undernourished infants might:
- lose interest in their surroundings
- avoid eye contact
- become fussy
- not reach developmental milestones like sitting up, walking, and talking at the usual age
If you notice a drop in weight gain or your baby doesn’t seem to have a normal appetite, see your child’s doctor. Also call about any major change in eating patterns. Toddlers and older children may have days and sometimes weeks when they show little interest in eating, but that shouldn’t happen in infants.
If you have trouble feeding your baby, your doctor can help. When a child doesn’t readily eat, parents can become frustrated and feel they’re doing something wrong. That can make the problem worse, causing stress for you and your baby. Instead, get help for both of you by talking to your doctor.
Who is affected by failure to thrive?
Infants born into families with inadequate support or understanding of infant needs may not provide the right kinds or amounts of food. For example, too much fruit juice, problems breastfeeding, or failure to introduce solids at an appropriate age may lead to too little calories being consumed. Babies and children with developmental delay or problems swallowing may consume too few calories. Conditions such as cystic fibrosis, celiac disease, or severe allergy or intolerance may consume enough food but not be able to absorb it properly. A child with a chronic medical condition, such as congenital heart disease or a genetic syndrome, may need more calories than expected. In severe cases, neglect or abuse may be associated with failure to thrive if food is purposely withheld from a baby.
Does my child have failure to thrive?
If you’re worried that your child is failing to thrive, remember that many things can cause slower weight gain. For instance, breastfed babies and bottle-fed babies often gain weight at different rates in the early newborn period.
Genetics also play a big role in weight gain. So if a baby’s parents are slim, the baby may not put on pounds quickly. However, infants should still gain weight steadily. As a general guideline, babies usually eat often in a 24-hour period and should gain about 1 ounce a day in the first month of life. It can be hard to judge this from home (even if you have a scale), so it’s important to see your child’s doctor regularly. Doctors can check for problems at regular well-child checkups, so it’s important to keep these appointments.
Failure to thrive causes
Failure to thrive has many different causes, and sometimes more than one cause may contribute to the condition at the same time. If an infant is not offered enough food or is not willing to eat enough food, or vomits repeatedly (such as with severe gastroesophageal reflux), there will not be enough calories to support growth. A child who is unable to absorb enough calories (such as with severe allergies or a medical condition like cystic fibrosis) will also not grow as expected. Any condition that causes a child to need more calories than normally expected may also lead to failure to thrive.
A number of things can cause failure to thrive, including:
- Not enough food offered. In some cases, parents mistakenly cause the problem. Sometimes a parent measures formula incorrectly, causing an infant to get too few calories. Problems with breastfeeding or transitioning to solids also can cause failure to thrive. Parents who worry their child will get fat may restrict the amount of calories they give their infants. And sometimes parents don’t pay enough attention to their children’s hunger cues or can’t afford enough food for their children.
- The child eats too little. Some children have trouble eating enough food because of prematurity, developmental delays, or conditions like autism in which they do not like eating foods of certain textures or tastes.
- Health problems involving the digestive system. Several health conditions can prevent a child from gaining weight. These include gastroesophageal reflux (GER), chronic diarrhea, cystic fibrosis, chronic liver disease, and celiac disease. With reflux, the esophagus may become so irritated that a child refuses to eat because it hurts. Persistent diarrhea can make it hard for the body to hold on to the nutrients and calories from food. Cystic fibrosis, chronic liver disease, and celiac disease all cause problems with the body’s ability to absorb nutrients. The child may eat a lot, but the body doesn’t absorb and retain enough of that food. Kids with celiac disease are allergic to gluten, a protein found in wheat and other grains. The immune system’s abnormal response to this protein damages the lining of the intestine so it can’t absorb nutrients properly.
- Food intolerance. A food intolerance, which is different from a food allergy, means the body is sensitive to certain foods. For example, milk protein intolerance means the body can’t absorb foods that have milk proteins, such as yogurt and cheese, which could lead to failure to thrive.
- An ongoing illness or disorder. A child who has trouble eating — because of prematurity or a cleft lip or palate, for example — may not take in enough calories to support normal growth. Other conditions involving the heart, lungs, or endocrine system can increase the amount of calories a child needs and make it hard for the child to eat enough to keep up.
- Infections. Parasites, urinary tract infections (UTIs), tuberculosis, and other infections can force the body to use nutrients rapidly and decrease appetite. This can lead to short- or long-term failure to thrive.
- Metabolic disorders. Metabolic disorders are health conditions that make it hard for the body to break down, process, or take energy from food. They also can cause a child to eat poorly or vomit.
Factors in the child’s environment include:
- Loss of emotional bond between parent and child
- Poverty
- Problems with child-caregiver relationship
- Parents do not understand the appropriate diet needs for their child
- Exposure to infections, parasites, or toxins
- Poor eating habits, such as eating in front of the television and not having formal meal times
Sometimes a mix of medical problems and environmental factors leads to failure to thrive. For instance, if a baby has severe GER and is reluctant to eat, feeding times can be stressful. The baby may become upset and frustrated, and the caregiver might be unable to feed the child enough food.
Other times, doctors aren’t sure exactly what causes the problem.
Failure to thrive symptoms
Children who fail to thrive do not grow and develop normally as compared to children of the same age. They seem to be much smaller or shorter. Teenagers may not have the usual changes that occur at puberty.
The following are the most common symptoms of failure to thrive. However, each child may experience symptoms differently. Symptoms may include:
- Lack of appropriate weight gain
- Irritability
- Easily fatigued
- Excessive sleepiness
- Lack of age-appropriate social response (i.e., smile)
- Does not make vocal sounds
- Delayed motor development
- Learning and behavior difficulties later in childhood
Symptoms of failure to thrive include:
- Height, weight, and head circumference do not match standard growth charts
- Weight is lower than third percentile of standard growth charts or 20% below the ideal weight for their height
- Growth may have slowed or stopped
The following may be delayed or slow to develop in children who fail to thrive:
- Physical skills, such as rolling over, sitting, standing and walking
- Mental and social skills
- Secondary sexual characteristics (delayed in adolescents)
Babies who fail to gain weight or develop often lack interest in feeding or have a problem receiving the proper amount of nutrition. This is called poor feeding.
Other symptoms that may be seen in a child that fails to thrive include:
- Constipation
- Excessive crying
- Excessive sleepiness (lethargy)
- Irritability
The symptoms of failure to thrive may resemble other conditions or medical problems. Always consult your child’s physician for a diagnosis.
Failure to thrive possible complications
- Permanent mental, emotional, or physical delays can occur.
- When to Contact a Medical Professional
Failure to thrive diagnosis
Many babies go through brief periods when their weight gain levels out, or they even lose a little weight. This is not unusual. However, if a baby doesn’t gain weight for 3 months in a row during the first year of life, doctors usually become concerned.
Failure to thrive is usually discovered and diagnosed by the infant’s physician. Infants are always weighed and measured when seen by their physicians for well-baby check-ups. Doctors use standard growth charts to plot weight, length, and head circumference, which are measured at each well-child exam. Children may have failure to thrive if they fall below a certain weight range for their age or fail to gain weight at the expected rate.
Your child’s doctor will initiate a more complete evaluation when your infant’s growth, development, and functioning are found to be delayed. Doctors might order tests (such as a complete blood count or urine test) to check for underlying medical problems. If a particular disease or disorder is suspected, the doctor might order other tests to check for that condition.
A special test called the Denver Developmental Screening Test may be used to show any delays in development. A growth chart outlining all types of growth since birth is created.
The following tests may be done:
- Complete blood count (CBC)
- Electrolyte balance
- Hemoglobin electrophoresis to check for conditions such as sickle cell disease
- Hormone studies, including thyroid function tests
- X-rays to determine bone age
- Urinalysis
A few different growth chart patterns might signal a health problem, such as:
- When a child’s weight or height percentile changes from a certain pattern it’s been following. For example: If height and weight consistently are on the 60th percentile line until a child is 5 years old, then the height has dropped to the 30th percentile at age 6, that might indicate that there’s a growth problem because the child is not following his or her previous growth pattern. Many kids may show changes in growth percentiles at certain points in development, when it’s normal for growth rates to vary more from child to child. This is particularly common during infancy and puberty.
- When kids don’t get taller at the same rate at which they’re gaining weight. Let’s say a boy’s height is in the 40th percentile and his weight is in the 85th percentile. (So he’s taller than 40% of kids his age, but weighs more than 85% of kids his age.) That might be a problem. On the other hand, if he’s in the 85th percentile for height and weight and follows that pattern consistently over time, that usually means that he’s a normal child who’s just larger than average.
If you have any questions about your child’s growth — or growth charts — talk with your doctor.
To see if there’s a problem, doctors will ask for a child’s detailed health history, including a feeding history. This helps doctors see whether underfeeding, household stresses, or feeding problems might be to blame. A nutritionist or other health care professional also may track the calories in a child’s diet to make sure the child is getting enough.
Growth Charts
Growth charts are a standard part of any checkup, and they show health care providers how kids are growing compared with other kids of the same age and gender. They also allow doctors and nurses to see the pattern of kids’ height and weight gain over time, and whether they’re developing proportionately.
Let’s say a child was growing along the same pattern until he was 2 years old, then suddenly started growing at a much slower rate than other kids. That might indicate a health problem. Doctors could see that by looking at a growth chart.
Doctors interpret the growth charts in the context of the child’s overall well-being, environment, and genetic background. Is the child meeting other developmental milestones? Are there other signs that a child is not healthy? How tall or heavy are the child’s parents and siblings? Was the child born prematurely? Has the child started puberty earlier or later than average? These are all factors that the doctor will use to help understand the numbers on the growth chart.
Girls and boys are measured on different growth charts because they grow in different patterns and at different rates.
And one set of charts is used for babies, from birth to 24 months. Another set of charts is used for kids ages 2 to 20 years old.
Up until the time babies are 24 months old, doctors measure weight, length, and head circumference.
With older kids (2 to 20 years old), doctors measure weight, height, and body mass index (BMI). It’s important to look at and compare weight and height measurements to get a full picture of a child’s growth.
Commonly used standard growth charts include the following:
Figure 1. Boys Growth Charts from Birth to 24 Months (Head circumference-for-age and Weight-for-length percentiles)
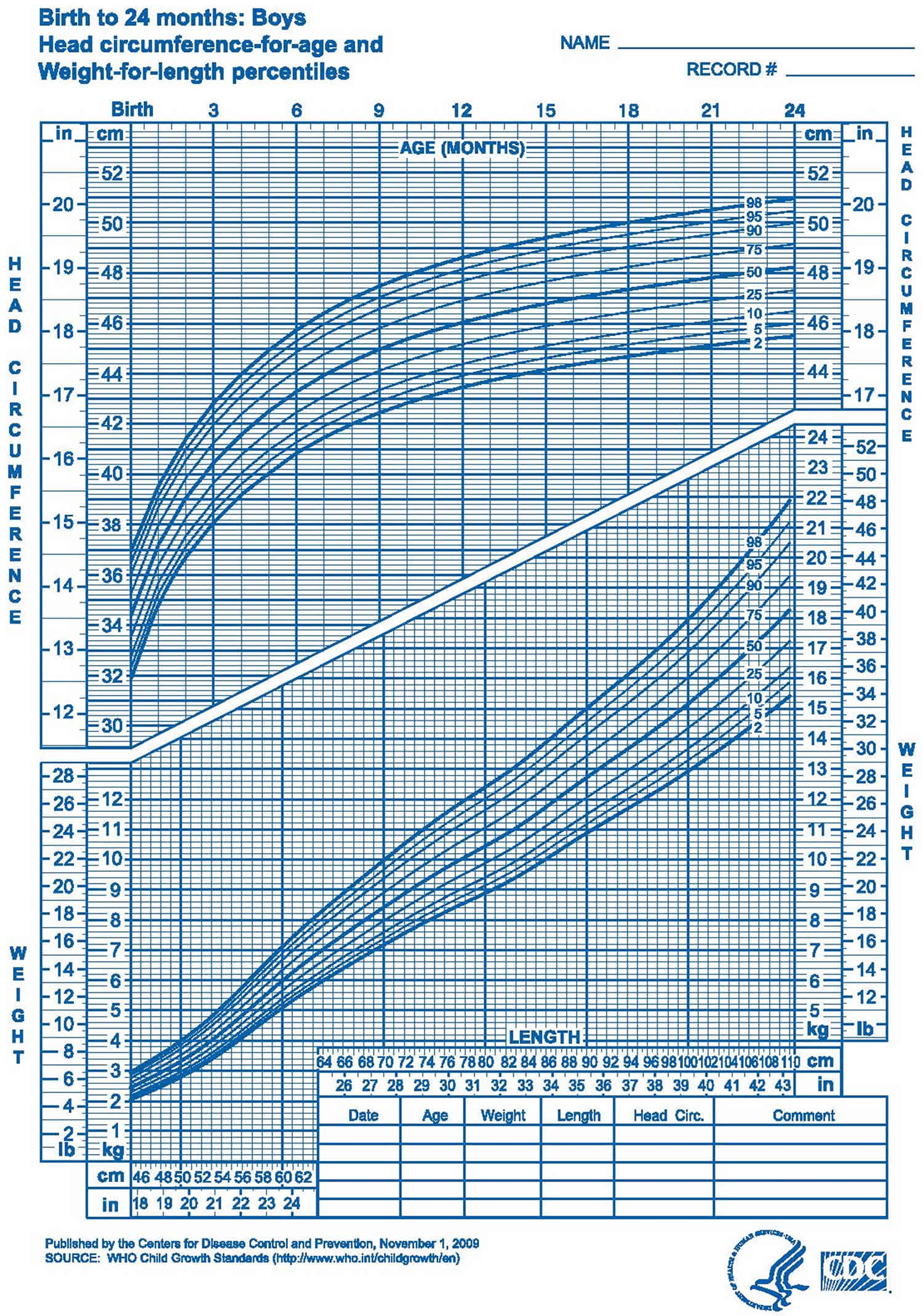
Figure 2. Boys Growth Charts from Birth to 24 Months (Length-for-age and Weight-for-age percentiles)
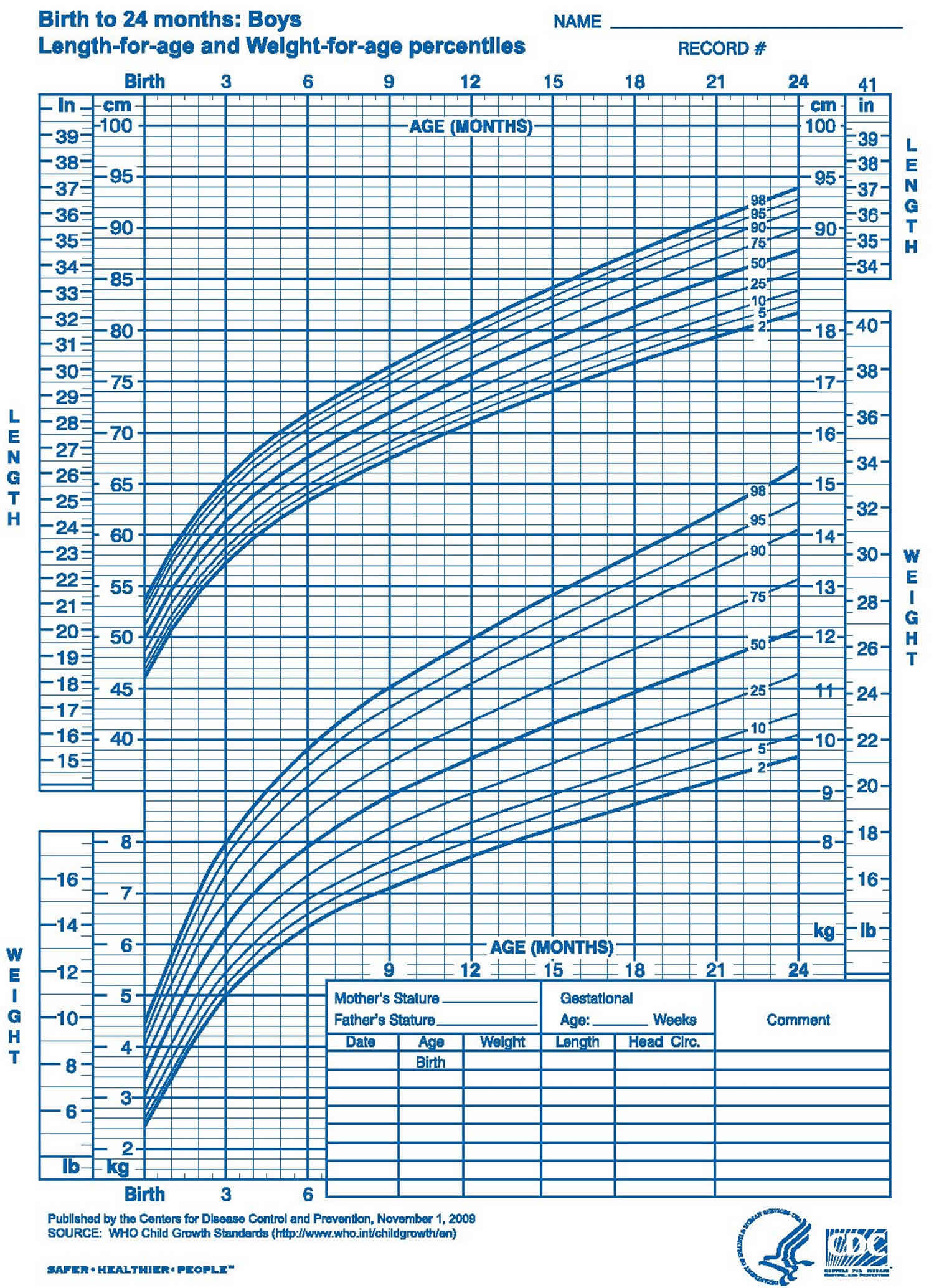 Figure 3. Boys Growth Charts from 2 to 20 Years (Stature-for-age and Weight-for-age percentiles)
Figure 3. Boys Growth Charts from 2 to 20 Years (Stature-for-age and Weight-for-age percentiles)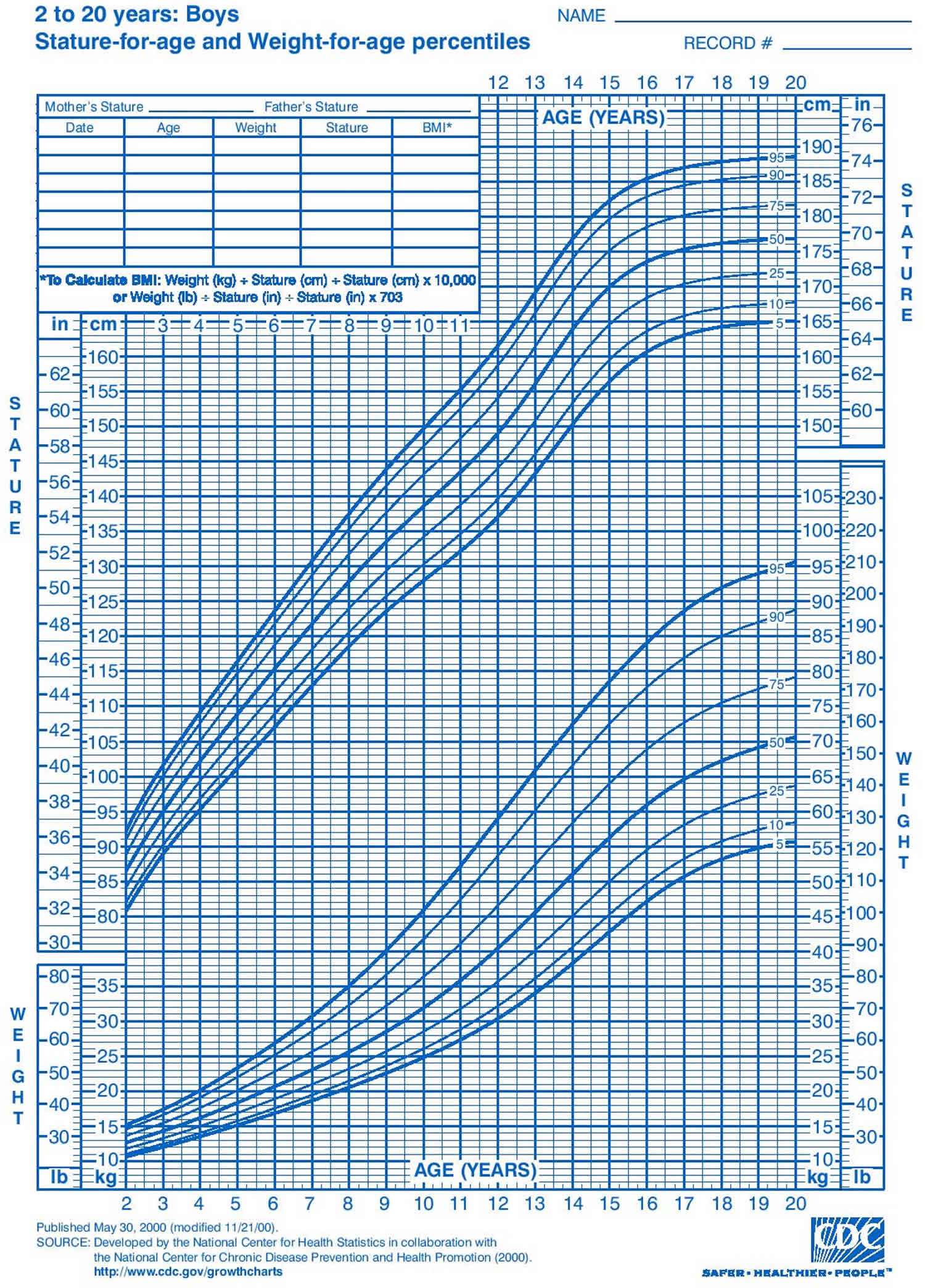
Figure 4. Boys Growth Charts from 2 to 20 Years (Body mass index-for-age percentiles)
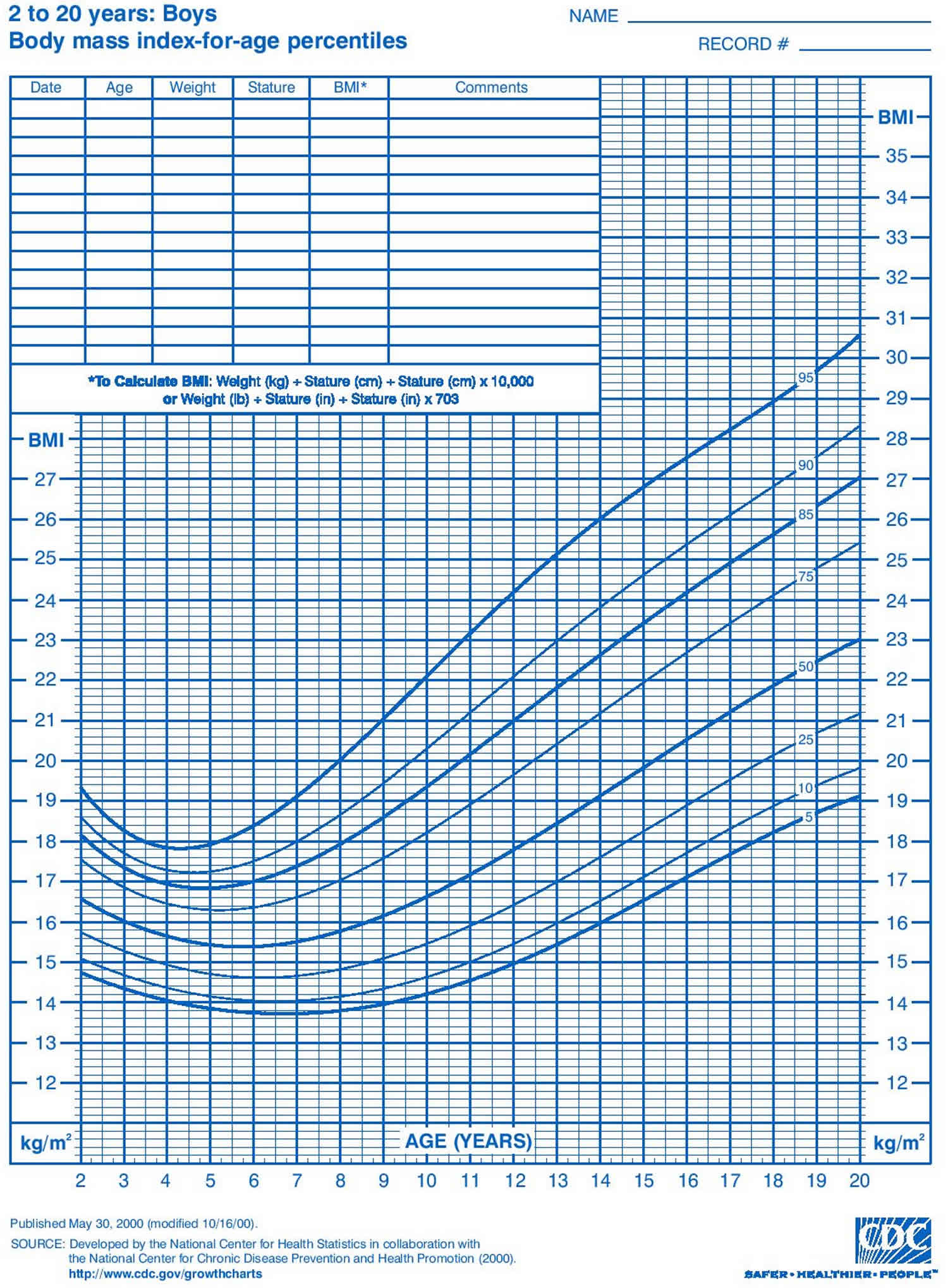
Figure 5. Girls Growth Charts from Birth to 24 Months (Head circumference-for-age and Weight-for-length percentiles)
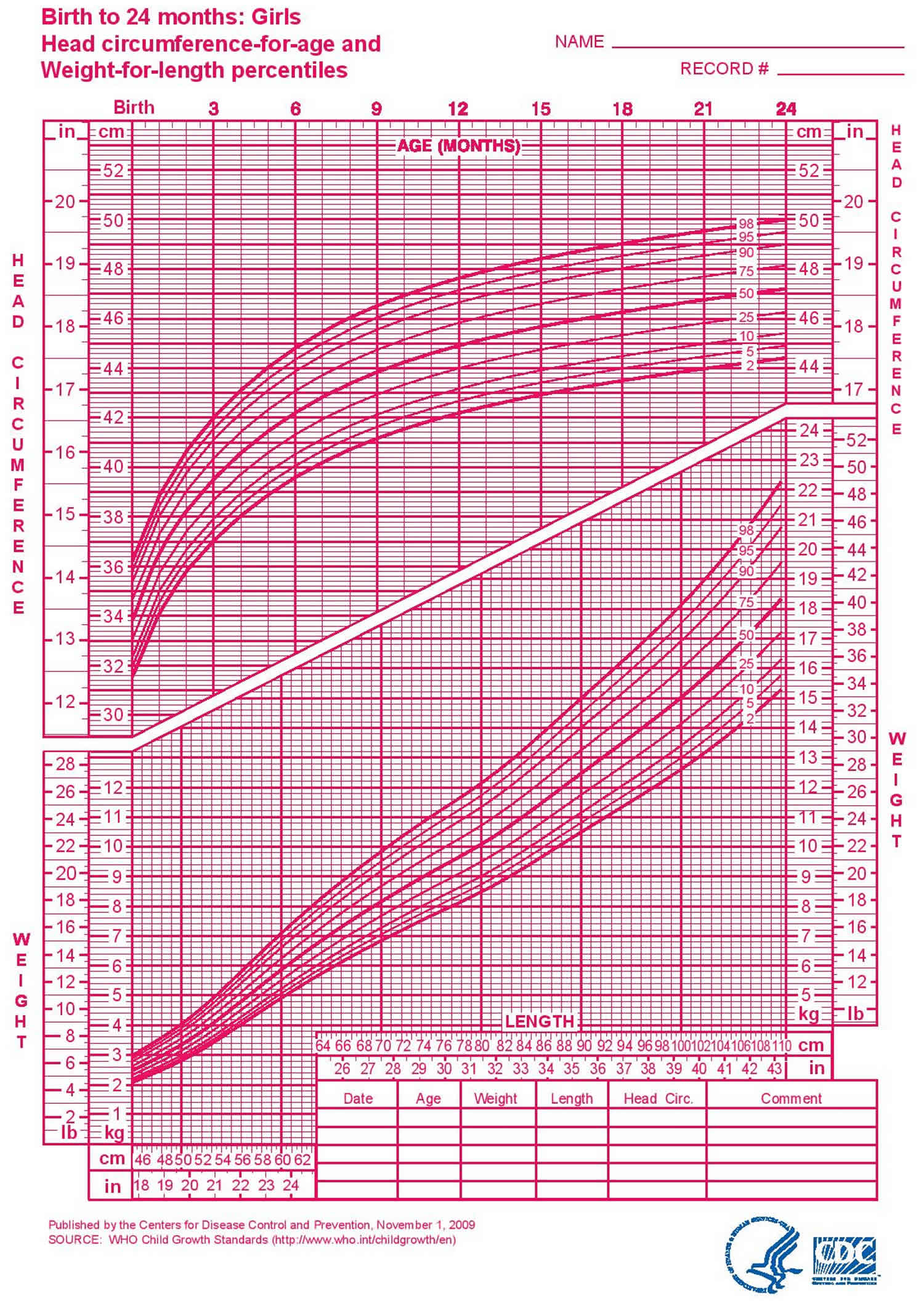
Figure 6. Girls Growth Charts from Birth to 24 Months (Length-for-age and Weight-for-age percentiles)
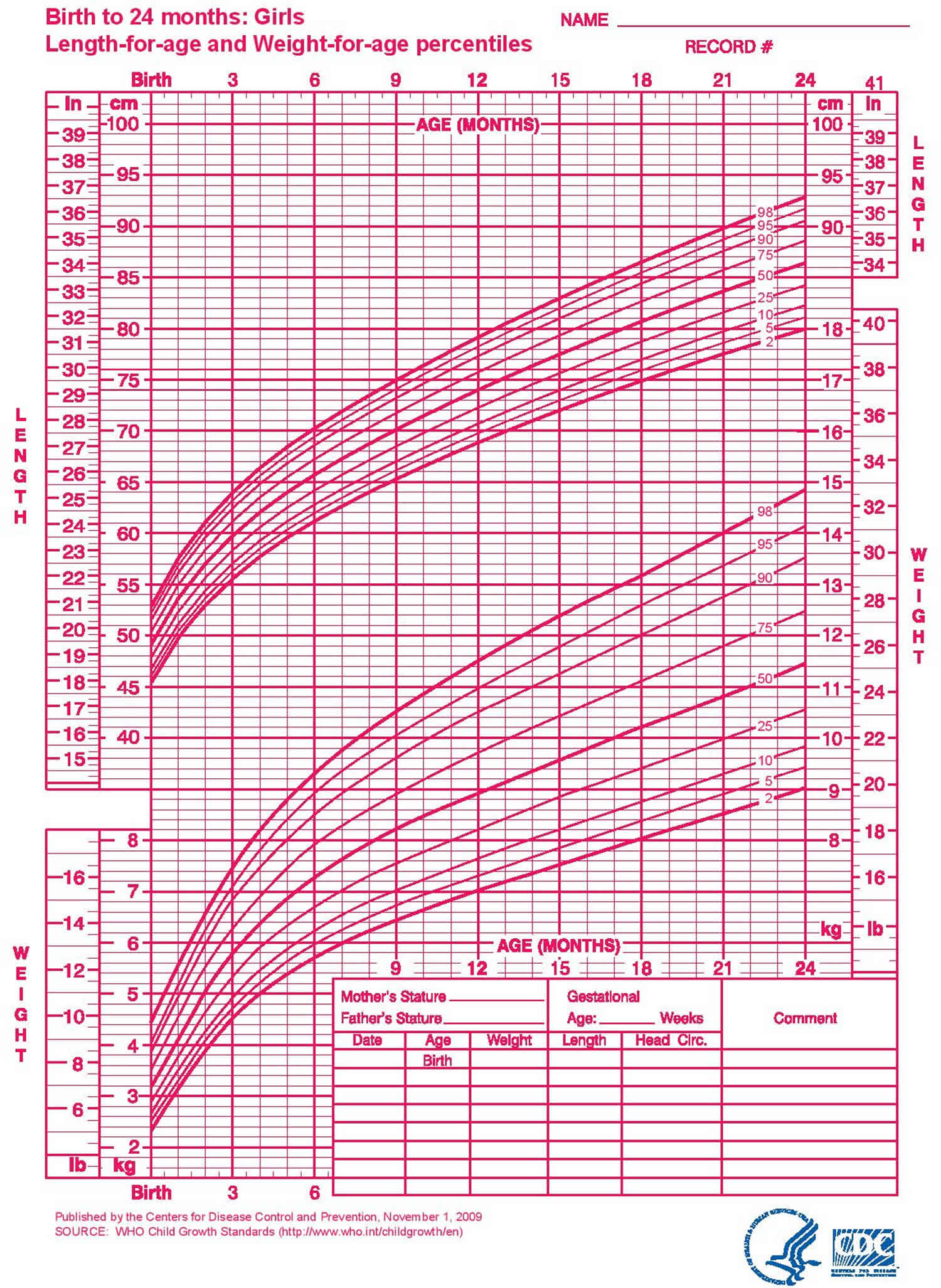 Figure 7. Girls Growth Charts from 2 to 20 Years (Stature-for-age and Weight-for-age percentiles)
Figure 7. Girls Growth Charts from 2 to 20 Years (Stature-for-age and Weight-for-age percentiles)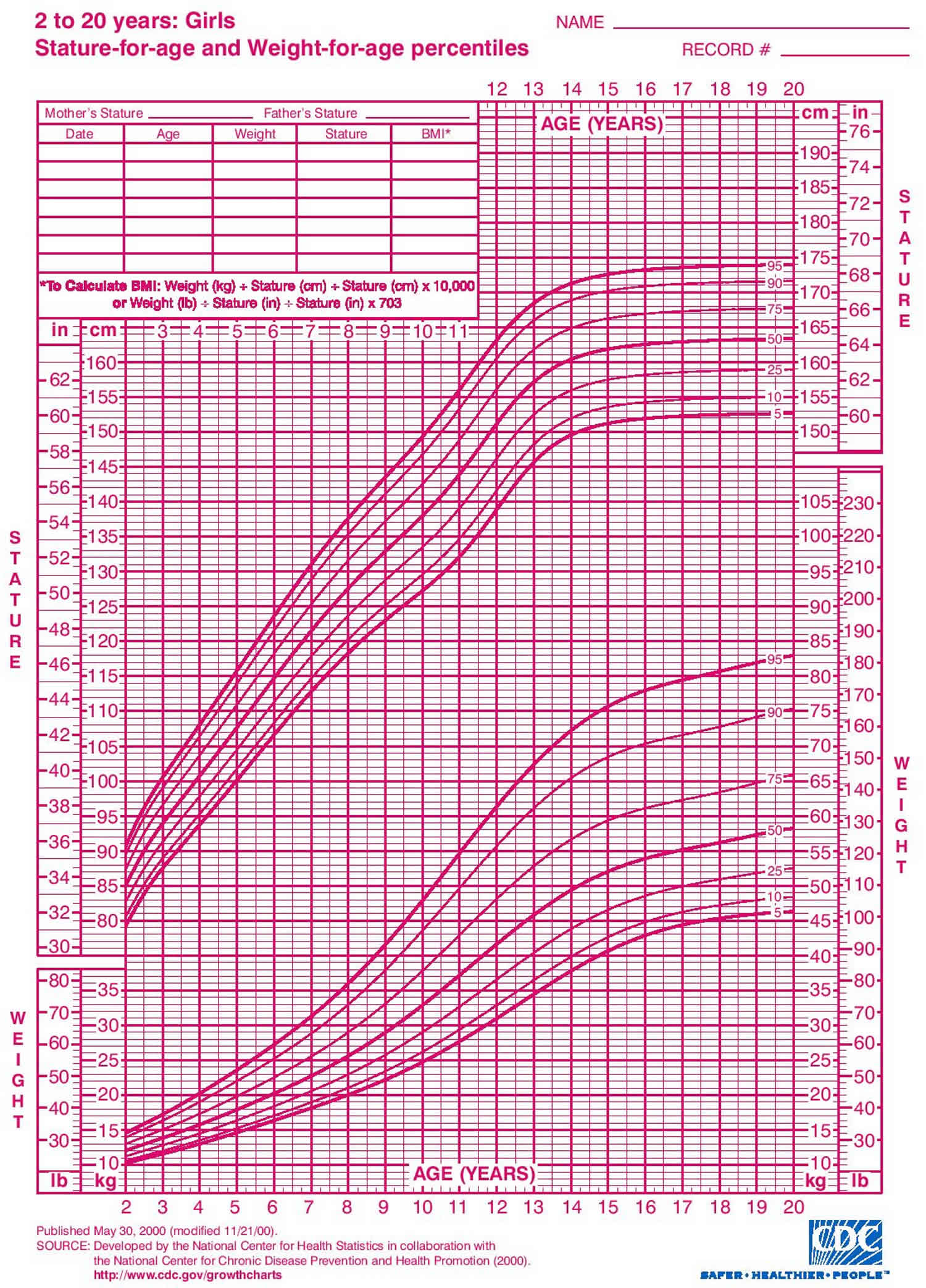
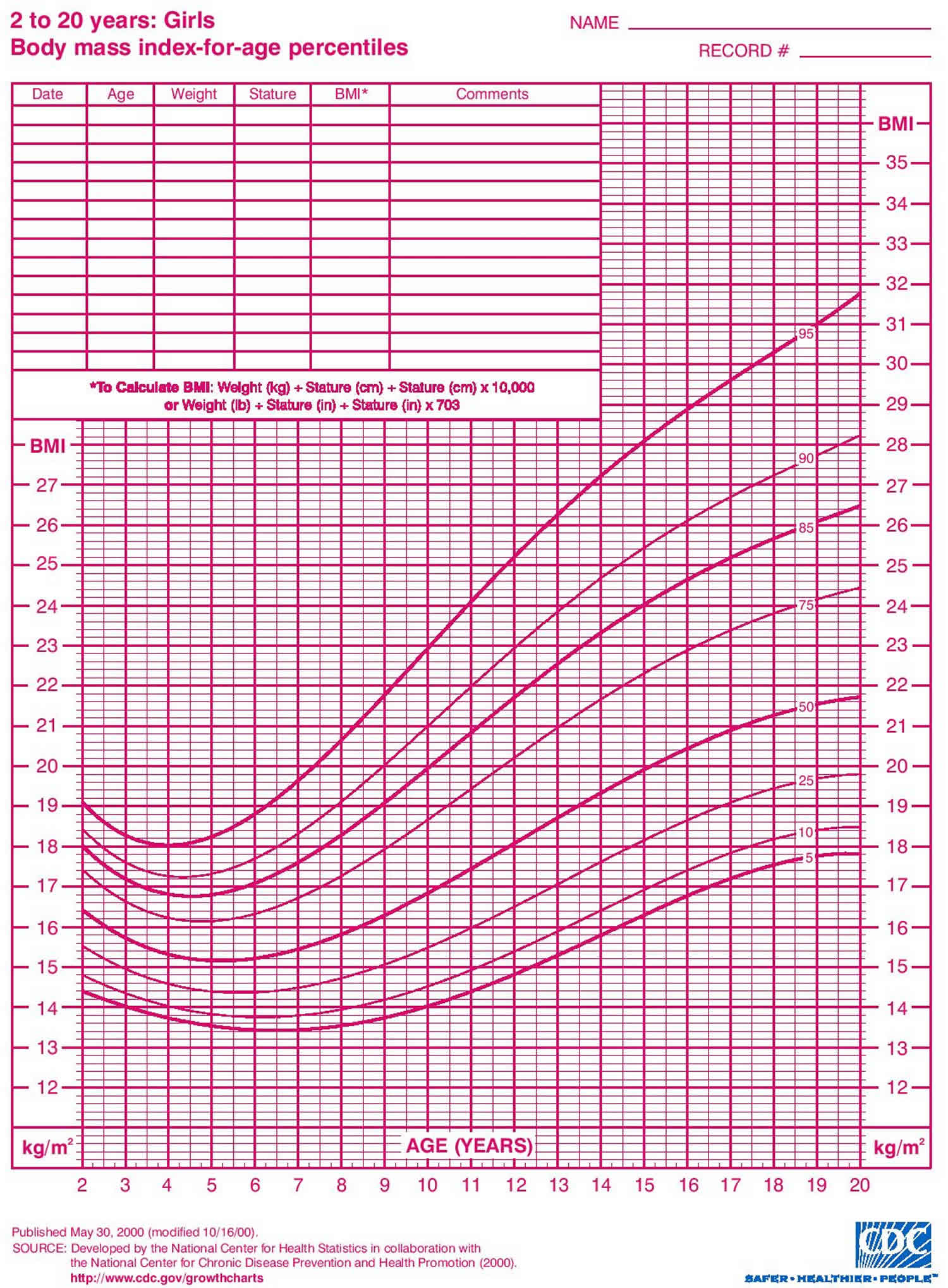
Figure 8. Girls Growth Charts from 2 to 20 Years (Body mass index-for-age percentiles)
Why is Head Circumference Measured?
In babies, head circumference (the distance around the largest part of the head) can provide clues about brain development. If a baby’s head is bigger or smaller than most other kids’ or the head circumference stops increasing or increases quickly, it may indicate a problem.
For example, an unusually large head may be a sign of hydrocephalus, a buildup of fluid inside the brain. A head that’s smaller than average may be a sign that the brain is not developing properly or has stopped growing.
What are Percentiles?
Percentiles are measurements that show where a child is compared with others. On the growth charts, the percentiles are shown as lines drawn in curved patterns.
When doctors plot a child’s weight and height on the chart, they see which percentile line those measurements land on. The higher the percentile number, the bigger a child is compared with other kids of the same age and gender, whether it’s for height or weight; the lower the percentile number, the smaller the child is. For example, if a 4-year-old boy’s weight is in the 10th percentile, that means that 10% of boys that age weigh less than he does and 90% of 4-year-old boys weigh more.
How are Percentiles Determined?
The Centers for Disease Control and Prevention (CDC) created the growth charts that are most commonly used in the United States. They were last updated in 2000. After collecting growth measurements from thousands of U.S. children over a period of time, the CDC was able to show the range of these measurements on one chart, using percentile curves.
Being in a high or a low percentile does not necessarily mean that a child is healthier or has a growth or weight problem. Let’s say that 4-year-old boy, who is in the 10th percentile for weight, is also in the 10th percentile for height. So 10% of kids are shorter and weigh less than he does, and most kids — 90% — are taller and weigh more. That just means that he’s smaller than average, which usually doesn’t mean there is a problem. If his parents and siblings are also smaller than average, and there are other signs that he’s healthy and developing well, doctors would likely conclude that there’s no cause for concern.
What’s the Ideal Percentile for my child?
There is no one ideal number. Healthy children come in all shapes and sizes, and a baby who is in the 5th percentile can be just as healthy as a baby who is in the 95th percentile.
Ideally, each child will follow along the same growth pattern over time, growing in height and gaining weight at the same rate, with the height and weight in proportion to one another. This means that usually a child stays on a certain percentile line on the growth curve. So if our 4-year-old boy on the 10th percentile line has always been on that line, he is continuing to grow along his pattern, which is a good sign.
Failure to thrive treatment
Treatment for children who fail to thrive involves making sure that the child gets the calories needed to grow and addressing any underlying feeding issues. This often requires the help of a care team that may include:
- the primary care doctor or pediatrician
- a registered dietitian to evaluate the child’s dietary needs
- occupational therapists to help caregivers and the child develop successful feeding behaviors
- speech therapists to address any sucking or swallowing problems
- a social worker if a family has trouble getting enough food for the child
- psychologists and other mental health professionals if there are any behavioral issues
- specialists (such as a cardiologist, neurologist, or gastroenterologist) to treat underlying health conditions
Specific treatment for failure to thrive will be determined by your child’s physician based on:
- Your child’s age, overall health, and medical history
- Extent of your child’s symptoms
- Cause of the condition
- Your child’s tolerance for specific medications, procedures, or therapies
- Expectations for the course of the condition
- Your opinion or preference
The individual issues involved in causing failure to thrive are almost always complex. Treatment depends on the cause of the condition and may involve a team of healthcare providers, including social workers, nutritionists, physical therapists, geneticists, and other specialists.
Treatment depends on the cause of the delayed growth and development. Delayed growth due to nutritional problems can be helped by showing the parents how to provide a well-balanced diet.
Do not give your child dietary supplements such as Boost or Ensure without talking to your provider first.
Other treatment depends on how severe the condition is. The following may be recommended:
- Increase the number of calories and amount of fluid the infant receives
- Correct any vitamin or mineral deficiencies
- Identify and treat any other medical conditions
Usually, children who have failure to thrive can be treated at home along with regular doctor visits. The doctor will recommend high-calorie foods and may place an infant on a high-calorie formula. Depending on the child’s feeding habits, doctors may recommend offering foods of certain textures, spacing out meals to make sure children are hungry, avoiding “empty” calories like juices and candies, and other strategies depending on the child’s condition and family situation.
In cases of severe failure to thrive, a child who is not growing with initial treatment may need tube feedings. In tube feedings, a tube is put in that runs from the nose into the stomach. Liquid nutrition is provided at a steady rate through the tube and is usually given at nighttime only. The child can continue with daily activities and eat freely during the day. Once he or she starts getting more calories, the child will feel better and will probably start to eat more on his or her own. At that point, the tube can be removed.
Children with extreme failure to thrive might need to be treated in a hospital. There, they will be fed and monitored around the clock for 10 to 14 days (or longer), until they gain some weight. After that, it still can take months until the symptoms of severe malnutrition are gone.
How long treatment lasts can vary. Weight gain takes time, so it might be several months before a child is back in the normal range. When the condition is due to a chronic illness or disorder, children may have to be monitored regularly at their doctor’s office. In those cases, treatment may take even longer, perhaps for a lifetime.
Failure to thrive prognosis
Normal growth and development may be affected if a child fails to thrive for a long time.
Normal growth and development may continue if the child has failed to thrive for a short time, and the cause is determined and treated.





{kind=link}