
Contents
- What is flu shot
- Groups Recommended for Flu Shot
- Flu Shot Guidance for Use in Specific Situations
- Volume per Dose for Children and Adults
- Number of Doses for Children Aged 6 Months through 8 Years
- Pregnant Women
- Adults Aged ≥65 years
- Immunocompromised Persons
- High-Risk Persons and their Caregivers and Contacts
- Persons with a History of Egg Allergy
- Vaccination Issues for Travelers
- Vaccination and Influenza Antiviral Medications
- Flu Vaccine and People with Egg Allergies
- What is considered an egg allergy?
- How common is egg allergy in children and adults?
- What vaccine should I get if I am egg allergic, but I can eat lightly cooked eggs?
- What flu vaccine should I get if I get hives after eating egg-containing foods?
- What kind of flu vaccine should I get if I have more serious reactions to eating eggs or egg-containing foods like cardiovascular changes or a reaction requiring epinephrine?
- Are there still people with egg allergies who should not get flu vaccine?
- Why do flu vaccines contain egg protein?
- How much egg protein is in flu vaccine?
- Can egg protein in flu vaccine cause allergic reactions in persons with a history of egg allergy?
- How long after flu vaccination does a reaction occur in persons with a history of egg allergy?
- What is the flu?
- How flu shot works
- Is it safe to get a flu shot during pregnancy?
- Should I get a flu shot?
- Is it safe to get a flu shot if I have heart disease?
- Can you get the flu from the flu shot?
- When should I get a flu shot?
- Where to get flu shot?
- How long does the flu shot last?
- Can I get seasonal flu even though I got a flu vaccine this year?
- Does flu vaccine work right away?
- Are there some people who should not receive a flu vaccine?
- What is in the flu shot
- Flu shot effectiveness
- Flu shot side effects
What is flu shot
A flu shot also called flu vaccine that is given with a needle, usually in the arm. The seasonal flu shot causes antibodies to develop in your body about two weeks after you get it. These antibodies provide protection against infection with the flu viruses that are in the flu shot. The seasonal flu shot protects against the three or four influenza viruses that research indicates will be most common during the season.
Types of flu virus
There are 3 types of flu viruses. They are:
- Type A flu virus – this is usually the more serious type. The virus is most likely to mutate into a new version that people are not resistant to. The H1N1 (swine flu) strain is a type A virus, and flu pandemics in the past were type A viruses.
- Type B flu virus – this generally causes a less severe illness and is responsible for smaller outbreaks. It mainly affects young children.
- Type C flu virus – this usually causes a mild illness similar to the common cold.
Most years, 1 or 2 strains of type A flu circulate as well as type B.
In February each year, the World Health Organization (WHO) assesses the strains of flu virus that are most likely to be circulating in the northern hemisphere over the following winter. Based on this assessment, WHO recommends which flu strains the vaccines should contain for the forthcoming winter. Vaccine manufacturers then produce flu vaccines based on WHO’s recommendations. These flu shots are used in all the countries in the northern hemisphere, not just the US. Production of the vaccine starts in March each year after WHO’s announcement.
There are different types of flu shots, including some especially for people 65 and older. Ask your health care provider which one is right for you.
The Centers for Disease Control and Prevention (CDC) recommends use of injectable influenza vaccines (including inactivated influenza vaccines and recombinant influenza vaccines) during 2017-2018. The nasal spray flu vaccine (live attenuated influenza vaccine or LAIV) should not be used during 2017-2018.
Flu vaccines can protect against 3 or 4 types of flu virus (usually 2 A types and 1 or 2 B types).
For most flu vaccines, the strains of the viruses are grown in hens’ eggs. The viruses are then killed (deactivated) and purified before being made into the vaccine.
Because the injected flu vaccine is a killed vaccine, it cannot cause flu.
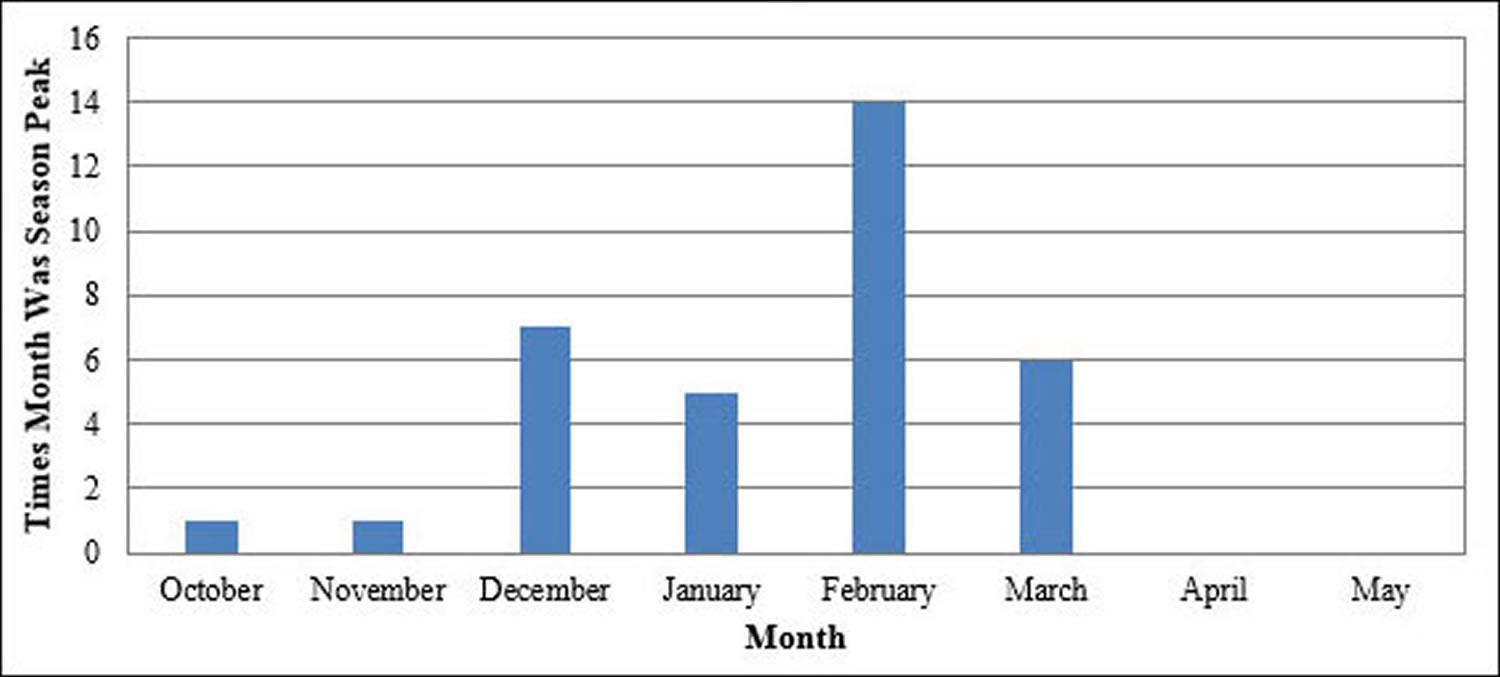
In the United States, flu season occurs in the autumn and winter. While influenza viruses circulate year-round, most of the time flu activity peaks between December and February, but activity can last as late as May.
Figure 1. Peak Month of Flu Activity 2015-2016
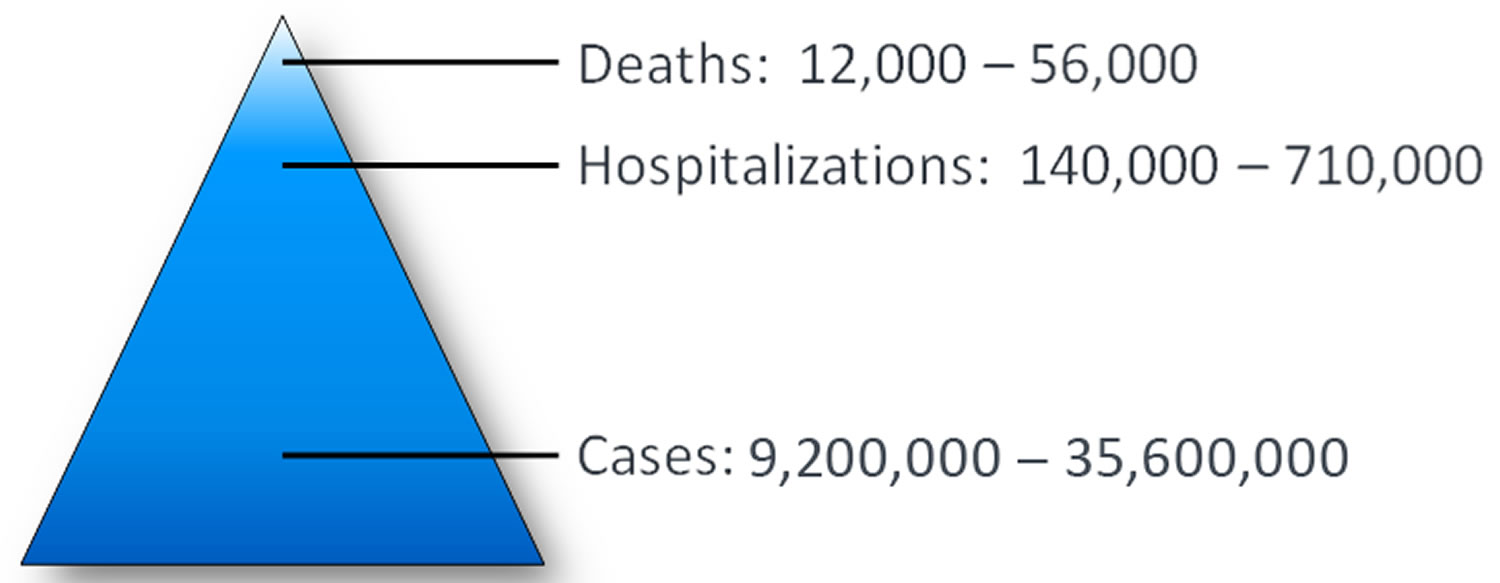
While the impact of influenza varies from season to season, it places a substantial burden on the health of people in the United States: millions of people become ill, hundreds of thousands are hospitalized and thousands or tens of thousands of people die from flu every year.
Figure 2. Health impacts and deaths from the flu
Influenza Vaccine Composition for 2017-2018
- All 2017-18 influenza vaccines licensed in the United States will contain hemagglutinin (HA) derived from influenza viruses antigenically similar to those recommended by FDA.
- 2017–18 trivalent vaccines:
- an A/Michigan/45/2015 (H1N1)pdm09–like virus;
- an A/Hong Kong/ 4801/2014 (H3N2)–like virus; and
- a B/Brisbane/60/2008–like virus (Victoria lineage).
- 2017–18 quadrivalent vaccines:
- the same three HA antigens as trivalent vaccines, plus
- a B/Phuket/3073/2013–like virus (Yamagata lineage).
For the 2017–18 season, quadrivalent and trivalent influenza vaccines will be available. Inactivated influenza vaccines (IIVs) will be available in trivalent (IIV3) and quadrivalent (IIV4) formulations. Recombinant influenza vaccine (RIV) will be available in trivalent (RIV3) and quadrivalent (RIV4) formulations. Live attenuated influenza vaccine (LAIV4) is not recommended for use during the 2017–18 season due to concerns about its effectiveness against (H1N1)pdm09 viruses during the 2013–14 and 2015–16 seasons. Recommendations for different vaccine types and specific populations are discussed. No preferential recommendation is made for one influenza vaccine product over another for persons for whom more than one licensed, recommended product is available.
The U.S. Food and Drug Administration (FDA) has licensed a new seasonal flu vaccine containing adjuvant for adults 65 years of age and older. An adjuvant is an ingredient added to a vaccine to create a stronger immune response to vaccination. The new flu vaccine, FLUAD™ was licensed in November 2015 and will be available during the 2017-2018 flu season. It contains MF59 adjuvant, an oil-in-water emulsion of squalene oil. FLUAD™ is the first adjuvanted seasonal flu vaccine marketed in the United States. MF59 is an oil-in-water emulsion of squalene oil. Squalene, a naturally occurring substance found in humans, animals and plants, is highly purified for the vaccine manufacturing process. FLUAD™ is approved for use among people 65 years and older, who often have a lower protective immune response after flu vaccination compared to younger, healthier people. Some adverse events (which are also reported after regular flu vaccines) were reported more frequently after vaccination with FLUAD™. The most common adverse events experienced during clinical studies were mild to moderate and were temporary, and included pain, redness at the injection site, headache, muscle aches, and malaise.
Table 1. U.S. Influenza Inactivated Influenza Vaccines (IIVs) Products for the 2017-18 Season
| TRADE NAME [MANUFACTURER] | PRESENTATION | AGE INDICATION | MERCURY, µG/0.5ML | LATEX | ROUTE |
|---|---|---|---|---|---|
| IIV QUADRIVALENT, STANDARD-DOSE (SD-IIV4) | |||||
| Afluria Quadrivalent [Seqirus] | 0.5 mL prefilled syringe | ≥5 yrs | NR | No | IM |
| 5.0 mL multi-dose vial | ≥5 yrs (needle/syringe)18 through 64 yrs (jet injector) | 24.5 | No | IM | |
| Fluarix Quadrivalent [GlaxoSmithKline] | 0.5 mL prefilled syringe | ≥6 months | NR | No | IM |
| FluLaval Quadrivalent [ID Biomedical Corp. of Quebec] | 0.5 mL prefilled syringe | ≥6 months | NR | No | IM |
| 5.0 mL multi-dose vial | ≥6 months | <25 | No | IM | |
| Fluzone Quadrivalent [Sanofi Pasteur] | 0.25 mL prefilled syringe | 6 through 35 months | NR | No | IM |
| 0.5 mL prefilled syringe | ≥3 yrs | NR | No | IM | |
| 0.5 mL single-dose vial | ≥3 yrs | NR | No | IM | |
| 5.0 mL multi-dose vial | ≥6 months | 25 | No | IM | |
| IIV QUADRIVALENT, STANDARD-DOSE, CELL CULTURE-BASED (ccIIV4) | |||||
| Flucelvax Quadrivalent [Seqirus] | 0.5 mL prefilled syringe | ≥4 yrs | NR | No | IM |
| 5.0 mL multi-dose vial | ≥4 yrs | 25 | No | IM | |
| IIV QUADRIVALENT, STANDARD-DOSE, INTRADERMAL (Intradermal IIV4) | |||||
| Fluzone Intradermal Quadrivalent [Sanofi Pasteur] | 0.1 mL single-dose prefilled micro-injection system | 18 through 64 yrs | NR | No | ID |
| IIV TRIVALENT, STANDARD-DOSE (SD-IIV3) | |||||
| Afluria [Seqirus] | 0.5 mL prefilled syringe | ≥5 yrs | NR | No | IM |
| 5.0 mL multi-dose vial | ≥5 yrs (needle/syringe) 18 through 64 yrs (jet injector) | 24.5 | No | IM | |
| Fluvirin [Seqirus] | 0.5 mL prefilled syringe | ≥4 yrs | ≤1 | Yes* | IM |
| 5.0 mL multi-dose vial | ≥4 yrs | 25 | No | IM | |
| ADJUVANTED IIV TRIVALENT, STANDARD-DOSE (aIIV3) | |||||
| Fluad [Seqirus] | 0.5 mL prefilled syringe | ≥65 yrs | NR | Yes* | IM |
| IIV TRIVALENT HIGH-DOSE (HD-IIV3) | |||||
| Fluzone High-Dose [Sanofi Pasteur] | 0.5 mL prefilled syringe | ≥65 yrs | NR | No | IM |
Abbreviations: IIV3 = Trivalent Inactivated Influenza Vaccine; IIV4 = Quadrivalent Inactivated Influenza Vaccine; ID = intradermal; IM = intramuscular; NR = not relevant (does not contain thimerosal); mos = months; yrs = years.
*Syringe tip cap may contain natural rubber latex
[Source 1]Inactivated influenza vaccine (IIV) Hemagglutinin Content
- Intramuscular SD-IIVs contain 15µg of HA per virus (45 µg total for SD-IIV3s and 60 µg total for SD-IIV4s) per 0.5 mL dose.
- Fluzone High-Dose (HD-IIV3) contains 60µg of HA per virus (180µg total) per 0.5 mL dose.
- Fluzone Intradermal Quadrivalent (intradermal IIV4) contains 9µg of each HA per virus (36µg total) per 0.1 mL dose.
Inactivated influenza vaccine (IIV) Administration
- IIVs are administered intramuscularly (IM), with the exception of Fluzone Intradermal Quadrivalent. For IM vaccines:
- Adults and older children: the deltoid is the preferred site;
- Infants and younger children: the anterolateral thigh is the preferred site.
- Detailed guidance for administration sites and needle length is available in Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP) at ACIP Vaccine Recommendations and Guidelines 2.
- Afluria and Afluria Quadrivalent are licensed for intramuscular administration via jet injector (the Pharmajet Stratis), for persons aged 18-64 years only.
- Fluzone Intradermal Quadrivalent is administered intradermally, preferably over the deltoid muscle, using the included delivery system.
Inactivated influenza vaccine (IIV) Contraindications and Precautions
Contraindications:
- History of severe allergic reaction to the vaccine or any of its components
- Advisory Committee on Immunization Practices (ACIP) recommends that persons with egg allergy of any severity receive influenza vaccine
- Information about vaccine components is located in package inserts from each manufacturer.
Precautions:
- Moderate to severe acute illness with or without fever.
- Guillain–Barré syndrome within 6 weeks following after a previous dose of influenza vaccine.
Table 2. U.S. Influenza Recombinant Influenza Vaccines (RIVs) Products for the 2017-18 Season
| TRADE NAME [MANUFACTURER] | PRESENTATION | AGE INDICATION | MERCURY, µG/0.5ML | LATEX | ROUTE |
|---|---|---|---|---|---|
| Flublok Quadrivalent (RIV4) [Protein Sciences] | 0.5 mL prefilled syringe | ≥18 yrs | NR | No | IM |
| Flublok (RIV3) [Protein Sciences] | 0.5 mL single-dose vial | ≥18 yrs | NR | No | IM |
Abbreviations: RIV3 = Trivalent Recombinant Influenza Vaccine; RIV4 = Quadrivalent Recombinant Influenza Vaccine; IM = intramuscular; NR = not relevant (does not contain thimerosal); yrs = years.
[Source 1]Recombinant Influenza Vaccine (RIV) Hemagglutinin Content
- Recombinant Influenza Vaccines (RIVs) contain 45µg of HA derived from each vaccine virus per 0.5mL dose (135µg total for RIV3 and 180 µg total for RIV4).
Recombinant Influenza Vaccine (RIV) Administration
- Recombinant Influenza Vaccine (RIV) is administered intramuscularly.
- Adults: deltoid is the preferred site.
- Detailed guidance for administration sites and needle length is available in Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP) at General Best Practice Guidelines for Immunization 2.
Recombinant Influenza Vaccine (RIV) Contraindications and Precautions
Contraindications:
- History of severe allergic reaction to any component of the vaccine.
- Information about vaccine components is located in package inserts from the manufacturer.
Precautions:
- Moderate to severe acute illness with or without fever.
- Guillain–Barré syndrome within 6 weeks following a previous dose of influenza
Table 3. U.S. Influenza Live Attenuated Influenza Vaccine (LAIV4) – NOTE: LAIV4 is NOT recommended for use in any population for 2017-18. Content provided for information only.
| TRADE NAME [MANUFACTURER] | PRESENTATION | AGEINDICATION | MERCURY, µG/0.5ML | LATEX | ROUTE |
|---|---|---|---|---|---|
| FluMist Quadrivalent (LAIV4) [MedImmune] | 0.2 mL single-dose prefilled intranasal sprayer | 2 through 49 yrs | NR | No | NAS |
Abbreviations: LAIV4 = Quadrivalent Live Attenuated Influenza Vaccine; NAS = intranasal; NR = not relevant (does not contain thimerosal); yrs = years.
[Source 1]Live Attenuated Influenza Vaccine (LAIV) Administration
Live Attenuated Influenza Vaccine (LAIV) is NOT recommended for use in any population for 2017-18. Providers who use it should note the following:
- Live Attenuated Influenza Vaccine (LAIV) is administered intranasally using the supplied prefilled, single-use sprayer containing 0.2 mL of vaccine.
- Half of the total sprayer contents is sprayed into the first nostril while the recipient is in the upright position.
- The attached divider clip is removed and the second half of the dose administered into the other nostril.
- If the vaccine recipient sneezes immediately after administration, the dose should not be repeated.
- If nasal congestion impedes delivery of the vaccine to the nasopharyngeal mucosa, deferral of administration should be considered, or another age-appropriate vaccine should be administered instead.
Live Attenuated Influenza Vaccine (LAIV) Contraindications and Precautions
Contraindications:
- History of severe allergic reaction to any vaccine component or after previous dose of any influenza vaccine;
- Information about vaccine components is located in package inserts from the manufacturer.
- Concomitant aspirin or salicylate-containing therapy in children and adolescents;
- Children aged 2 through 4 years who have received a diagnosis of asthma or whose parents or caregivers report that a health care provider has told them during the preceding 12 months that their child had wheezing or asthma or whose medical record indicates a wheezing episode has occurred during the preceding 12 months;
- Children and adults who are immunocompromised due to any cause (including immunosuppression caused by medications or by HIV infection);
- Close contacts and caregivers of severely immunosuppressed persons who require a protected environment;
- Pregnancy;
- Receipt of influenza antiviral medication within previous 48 hours.
Precautions:
- Moderate to severe acute illness with or without fever;
- History of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine;
- Asthma in persons aged ≥5 years;
- Other underlying medical conditions that might predispose to complications attributable to severe influenza (e.g., chronic pulmonary, cardiovascular [except isolated hypertension], renal, hepatic, neurologic, hematologic, or metabolic disorders (including diabetes mellitus).
Groups Recommended for Flu Shot
- Routine annual influenza vaccination is recommended for all persons aged ≥6 months who do not have contraindications.
- Emphasis should be placed on vaccination of high-risk groups and their contacts and caregivers (no hierarchy is implied by order of listing):
- Children aged 6-59 months;
- Adults aged ≥50 years;
- Persons with chronic pulmonary (including asthma), cardiovascular (except isolated hypertension), renal, hepatic, neurologic, hematologic, or metabolic disorders (including diabetes mellitus);
- Persons who are immunocompromised due to any cause, (including medications or HIV infection);
- Women who are or will be pregnant during the influenza season;
- Children and adolescents (aged 6 months through 18 years) receiving aspirin- or salicylate-containing medications and who might be at risk for Reye syndrome;
- Residents of nursing homes and other long-term care facilities;
- American Indians/Alaska Natives;
- Persons who are extremely obese (BMI ≥40); and
- Caregivers and contacts of those at risk:
- Health care personnel in inpatient and outpatient care settings, medical emergency-response workers, employees of nursing home and long-term care facilities who have contact with patients or residents, and students in these professions who will have contact with patients;
- Household contacts and caregivers of children aged ≤59 months (i.e., <5 years), particularly contacts of children aged <6 months, and adults aged ≥50 years; and
- Household contacts and caregivers of persons who are in one of the high-risk categories listed.
According to the Centers for Disease Control and Prevention (CDC) 3, everyone 6 months of age and older should get a flu shot every season. People with egg allergies should check with their doctors before getting a vaccine. Other exceptions are people who have:
- Had reactions to flu shots before
- Guillain-Barre Syndrome
- A fever
Table 4. Flu Shot – Who Should Not and Who Should Have It
| People who can get the flu shot: | People who can’t get the flu shot: | People who should talk to their doctor before getting the flu shot: |
|---|---|---|
|
|
|
| Note: There are certain flu shots that have different age indications. For example, people younger than 65 years of age should not get the high-dose flu shot or the flu shot with adjuvant, and people who are younger than 18 years old or older than 64 years old should not get the intradermal flu shot. | ||
Table 5. Contraindications and precautions to the use of influenza vaccines — United States, 2017–18 influenza season*
| Vaccine type | Contraindications | Precautions |
|---|---|---|
| IIV | History of severe allergic reaction to any component of the vaccine† or after previous dose of any influenza vaccine | Moderate-to-severe acute illness with or without fever History of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine |
| RIV | History of severe allergic reaction to any component of the vaccine | Moderate-to-severe acute illness with or without fever History of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine |
| LAIV For the 2017–18 season, ACIP recommends that LAIV not be used. Content is provided for information. | History of severe allergic reaction to any component of the vaccine† or after a previous dose of any influenza vaccine Concomitant aspirin or salicylate-containing therapy in children and adolescents Children aged 2 through 4 years who have received a diagnosis of asthma or whose parents or caregivers report that a health care provider has told them during the preceding 12 months that their child had wheezing or asthma or whose medical record indicates a wheezing episode has occurred during the preceding 12 months Children and adults who are immunocompromised due to any cause (including immunosuppression caused by medications or by HIV infection) Close contacts and caregivers of severely immunosuppressed persons who require a protected environment Pregnancy Receipt of influenza antiviral medication within the previous 48 hours | Moderate-to-severe acute illness with or without fever History of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine Asthma in persons aged ≥5 years Other underlying medical conditions that might predispose to complications after wild-type influenza infection (e.g., chronic pulmonary, cardiovascular [except isolated hypertension], renal, hepatic, neurologic, hematologic, or metabolic disorders [including diabetes mellitus]) |
Abbreviations: ACIP = Advisory Committee on Immunization Practices; IIV = Inactivated Influenza Vaccine; LAIV = Live-Attenuated Influenza Vaccine; RIV = Recombinant Influenza Vaccine.
* Immunization providers should check Food and Drug Administration–approved prescribing information for 2017–18 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, and precautions. Package inserts for US-licensed vaccines are available at https://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm093833.htm. † History of severe allergic reaction (e.g., anaphylaxis) to egg is a labeled contraindication to the use of IIV and LAIV. However, ACIP recommends that any licensed, recommended, and appropriate IIV or RIV may be administered to persons with egg allergy of any severity (see Persons with a History of Egg Allergy).
Flu Shot Guidance for Use in Specific Situations
Volume per Dose for Children and Adults
- Children aged 6 through 35 months may receive:
- 0.5mL Fluarix Quadrivalent (IIV4) intramuscularly, or
- 0.5mL FluLaval Quadrivalent (IIV4) intramuscularly, or
- 0.25mL Fluzone Quadrivalent (IIV4) intramuscularly.
- Note that dose volume differs for these three brands. Care should be taken to administer the correct dose.
- Children aged 3 through 17 years may receive 0.5mL intramuscularly of an age-appropriate IIV formulation.
- Adults aged 18 years and older may receive 0.5mL intramuscularly of an age-appropriate IIV or RIV.
Alternatively, adults aged 18 through 64 years may receive 0.1mL intradermally of Fluzone Intradermal Quadrivalent (administered using the included delivery device). - If a smaller intramuscular dose (e.g., 0.25mL) is administered to an adult, an additional dose should be administered to provide a full 0.5mL dose. If the error is discovered later (after the recipient has left the vaccination setting), a full 0.5mL dose should be administered as soon as the recipient can return.
Number of Doses for Children Aged 6 Months through 8 Years
- Determine the number of doses needed for this age group as follows:
- Has the child received ≥2 doses of trivalent or quadrivalent influenza vaccine before July 1, 2017? (*Note: Doses need not have been given during same or consecutive seasons)
- If Yes: 1 dose of 2017-18 influenza vaccine
- If No/Don’t Know: 2 doses of 2017-18 influenza vaccine (administered ≥4 weeks apart)
- Has the child received ≥2 doses of trivalent or quadrivalent influenza vaccine before July 1, 2017? (*Note: Doses need not have been given during same or consecutive seasons)
Pregnant Women
- All women who are pregnant or who might be pregnant during the influenza season should receive influenza vaccine.
- Any licensed, recommended, and age-appropriate, influenza vaccine may be used.
- LAIV is not recommended for use in any population for 2017-18. Providers who use it should note that LAIV should not be used during pregnancy.
- Influenza vaccine can be administered at any time during pregnancy, before and during the influenza season.
Adults Aged ≥65 years
- May receive any age-appropriate IIV (standard- or high-dose, trivalent or quadrivalent, adjuvanted or unadjuvanted) or RIV.
- High-dose IIV3 exhibited superior efficacy over comparator standard-dose IIV3 in a large randomized trial, and may provide better protection than standard dose IIV3 for this age group.
- However, vaccination should not be delayed to find a particular product if an appropriate one is available.
Immunocompromised Persons
- LAIV is not recommended for use in any population for 2017-18. Providers who use it should note that LAIV should not be used for immunocompromised persons.
- Immunocompromised persons should receive an age-appropriate IIV or RIV
- Immune response to vaccines might be blunted in immunocompromised persons.
- Timing of vaccination might be a consideration (e.g., in some period before or after an immunocompromising intervention).
- The Infectious Diseases Society of America (IDSA) has published detailed guidance for the selection and timing of vaccines for persons with specific immunocompromising conditions 6
High-Risk Persons and their Caregivers and Contacts
- High-risk persons and their caregivers and contacts (including those of immunosuppressed persons) may receive any age-appropriate IIV or RIV
- LAIV is not recommended for use in any population for 2017-18. Providers who use it should note that health care personnel or hospital visitors who receive LAIV should avoid providing care for severely immunosuppressed persons (those requiring a protected environment) for 7 days after vaccination.
Persons with a History of Egg Allergy
- Persons who are able to eat lightly cooked egg (e.g., scrambled egg) without reaction are unlikely to be egg-allergic.
- Persons who have experienced only hives after exposure to egg should receive any licensed, recommended, age-appropriate influenza vaccine (i.e., IIV or RIV).
- Persons reporting symptoms other than hives, such as angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, may also receive any licensed and recommended influenza vaccine that is otherwise appropriate.
- Additionally, for these persons, vaccine should be administered in an inpatient or outpatient medical setting and supervised by a health care provider who is able to recognize and manage severe allergic conditions.
- A previous severe allergic reaction to influenza vaccine, regardless of the component suspected of causing the reaction, is a contraindication to future receipt of the vaccine.
Vaccination Issues for Travelers
- Travelers who wish to reduce the risk for influenza infection should consider influenza vaccination, preferably ≥2 weeks before departure.
- Persons at high risk for complications of influenza who were not vaccinated during the preceding fall or winter should consider receiving influenza vaccine before departure, if they plan to travel to the tropics, with organized tourist groups or on cruise ships, or to the Southern Hemisphere during April–September.
- Influenza vaccine formulated for the Southern Hemisphere might differ in viral composition from Northern Hemisphere vaccine.
- Southern Hemisphere influenza vaccines are generally not available in the U.S.
- IIV and RIV may be administered to persons receiving influenza antiviral medications for treatment or chemoprophylaxis.
- LAIV is not recommended for use in any population for 2017-18. If used, note that influenza antivirals may reduce the effectiveness of LAIV, if administered within 48 hours before to 2 weeks after vaccination.
Flu Vaccine and People with Egg Allergies
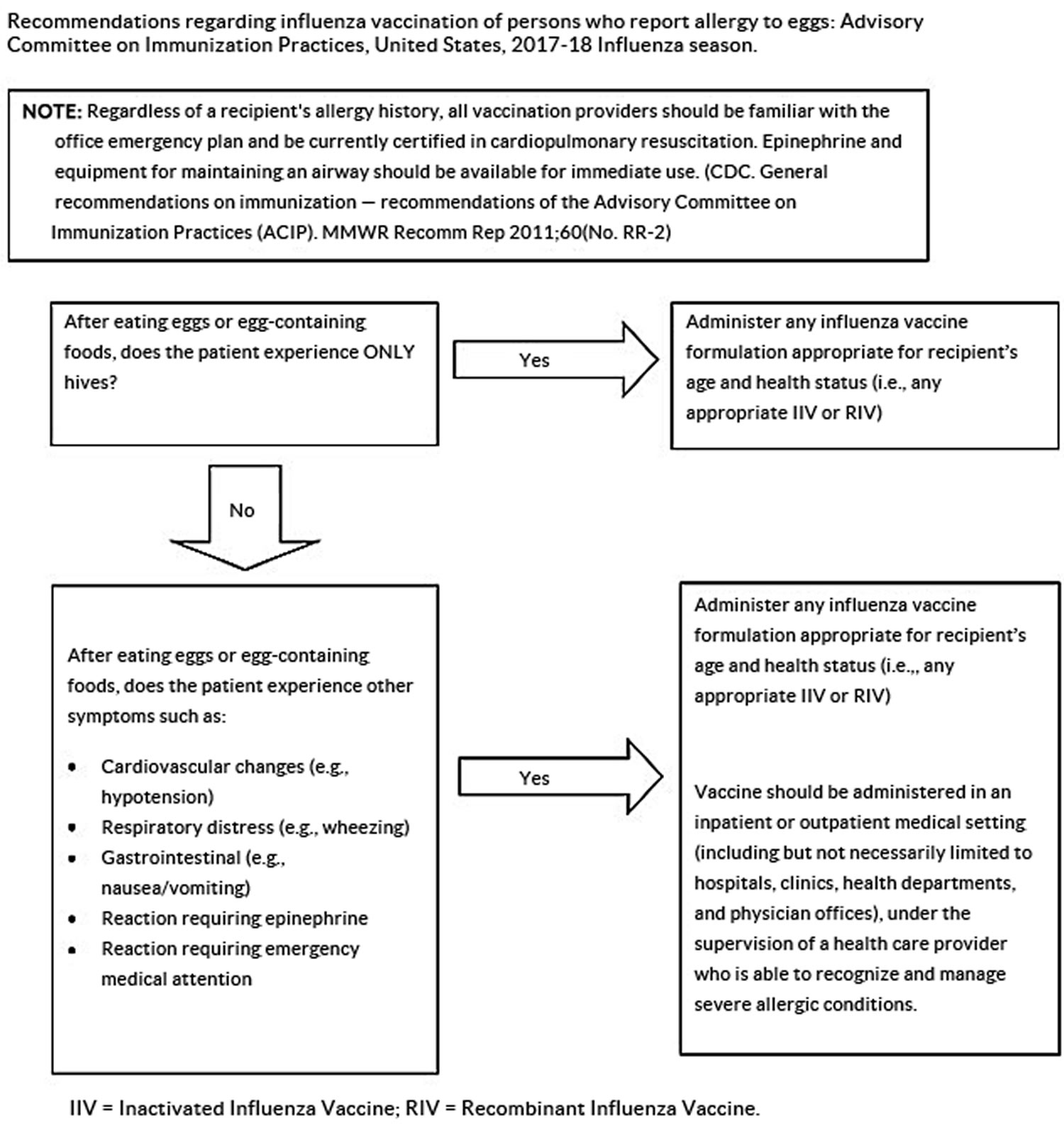
CDC and its Advisory Committee on Immunization Practices have not changed their recommendations regarding egg allergy and receipt of influenza (flu) vaccines 7. The recommendations remain the same as last season (2016-2017). Based on those recommendations, people with egg allergies no longer need to be observed for an allergic reaction for 30 minutes after receiving a flu vaccine. People with a history of egg allergy of any severity should receive any licensed, recommended, and age-appropriate influenza vaccine. Those who have a history of severe allergic reaction to egg (i.e., any symptom other than hives) should be vaccinated in an inpatient or outpatient medical setting (including but not necessarily limited to hospitals, clinics, health departments, and physician offices), under the supervision of a health care provider who is able to recognize and manage severe allergic conditions.
Most flu shots and the nasal spray flu vaccine are manufactured using egg-based technology. Because of this, they contain a small amount of egg proteins, such as ovalbumin. However, studies that have examined the use of both the nasal spray vaccine and flu shots in egg-allergic and non-egg-allergic patients indicate that severe allergic reactions in people with egg allergies are unlikely. A recent CDC study found the rate of anaphylaxis after all vaccines is 1.31 per one million vaccine doses given.
Figure 3. Flu Vaccine and People with Egg Allergies – CDC Recommendations
 [Source 7]
[Source 7]
Recommendations for flu vaccination of persons with egg allergy have not changed since the 2016-2017 flu season. CDC recommends:
- Persons with a history of egg allergy who have experienced only hives after exposure to egg should receive flu vaccine. Any licensed and recommended flu vaccine (i.e., any form of IIV or RIV) that is otherwise appropriate for the recipient’s age and health status may be used.
- Persons who report having had reactions to egg involving symptoms other than hives, such as angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, may similarly receive any licensed and recommended flu vaccine (i.e., any form of IIV or RIV) that is otherwise appropriate for the recipient’s age and health status. The selected vaccine should be administered in an inpatient or outpatient medical setting (including, but not necessarily limited to hospitals, clinics, health departments, and physician offices). Vaccine administration should be supervised by a health care provider who is able to recognize and manage severe allergic conditions.
- A previous severe allergic reaction to flu vaccine, regardless of the component suspected of being responsible for the reaction, is a contraindication to future receipt of the vaccine.
What is considered an egg allergy?
What are the signs and symptoms of an egg allergic reaction?
Egg allergy can be confirmed by a consistent medical history of adverse reactions to eggs and egg-containing foods, plus skin and/or blood testing for immunoglobulin E antibodies to egg proteins. Persons who are able to eat lightly cooked egg (e.g., scrambled egg) without reaction are unlikely to be allergic. Egg-allergic persons might tolerate egg in baked products (e.g., bread or cake). Therefore, tolerance to egg-containing foods does not exclude the possibility of egg allergy. Egg allergies can range in severity.
How common is egg allergy in children and adults?
Egg allergy affects about 1.3 % of all children and 0.2 % of all adults.
What vaccine should I get if I am egg allergic, but I can eat lightly cooked eggs?
If you are able to eat lightly cooked egg (e.g., scrambled egg) without reaction, you are unlikely to be allergic and can get any licensed flu vaccine (i.e., any form of inactivated influenza vaccine, live attenuated influenza vaccine, or recombinant influenza vaccine) that is otherwise appropriate for your age and health status.
What flu vaccine should I get if I get hives after eating egg-containing foods?
If you are someone with a history of egg allergy, who has experienced only hives after exposure to egg, you can get any licensed flu vaccine (i.e., any form of inactivated influenza vaccine, live attenuated influenza vaccine, or recombinant influenza vaccine) that is otherwise appropriate for your age and health.
What kind of flu vaccine should I get if I have more serious reactions to eating eggs or egg-containing foods like cardiovascular changes or a reaction requiring epinephrine?
If you are someone who has more serious reactions to eating eggs or egg-containing foods, like angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, you can get any licensed flu vaccine (i.e., any form of inactivated influenza vaccine, live attenuated influenza vaccine, or recombinant influenza vaccine) that is otherwise appropriate for your age and health status, but the vaccine should be given by a health care provider who can recognize and respond to a severe allergic response.
Are there still people with egg allergies who should not get flu vaccine?
People with egg allergy can receive flu vaccines according to the recommendations above. A person who has previously experienced a severe allergic reaction to flu vaccine, regardless of the component suspected of being responsible for the reaction should not get a flu vaccine again.
Why do flu vaccines contain egg protein?
Most flu vaccines today are produced using an egg-based manufacturing process and thus contain a small amount of egg protein called ovalbumin.
How much egg protein is in flu vaccine?
While not all manufacturers disclose the amount of ovalbumin in their vaccines, those that did from 2011–12 through 2014–15 reported maximum amounts of ≤1 µg/0.5 mL dose for flu shots and 0.24 µg/0.2 mL dose for the nasal spray vaccine. Cell-based flu vaccine (Flucelvax) likely has a much smaller amount of egg protein since the original vaccine virus is grown in eggs, but mass production of that vaccine does not occur in eggs. Recombinant vaccine (Flublok) is the only vaccine currently available that is completely egg free.
Can egg protein in flu vaccine cause allergic reactions in persons with a history of egg allergy?
Yes, allergic reactions can happen, but they occur very rarely with the flu vaccines available in the United States today. Occasional cases of anaphylaxis, a severe life-threatening reaction that involves multiple organ systems and can progress rapidly, in egg-allergic persons have been reported to the Vaccine Adverse Event Reporting System (VAERS) after administration of flu vaccine. Flu vaccines contain various components that may cause allergic reactions, including anaphylaxis. In a Vaccine Safety Datalink study, there were 10 cases of anaphylaxis after more than 7.4 million doses of inactivated flu vaccine, trivalent (IIV3) given without other vaccines, (rate of 1.35 per one million doses). Most of these cases of anaphylaxis were not related to the egg protein present in the vaccine. CDC and the Advisory Committee on Immunization Practices continue to review available data regarding anaphylaxis cases following flu vaccines.
How long after flu vaccination does a reaction occur in persons with a history of egg allergy?
Allergic reactions can begin very soon after vaccination. However, the onset of symptoms is sometimes delayed. In a Vaccine Safety Datalink study of more than 25.1 million doses of vaccines of various types given to children and adults over 3 years, only 33 people had anaphylaxis. Of patients with a documented time to onset of symptoms, eight cases had onset within 30 minutes of vaccination, while in another 21 cases, symptoms were delayed more than 30 minutes following vaccination, including one case with symptom onset on the following day.
What is the flu?
Flu is also known as influenza, is a contagious respiratory illness caused by flu viruses. It can cause mild to severe illness, and at times can lead to death. The flu is different from a cold. The flu usually comes on suddenly. The time from when a person is exposed to flu virus and infected to when symptoms begin is about 1 to 4 days, with an average of about 2 days.
People who have the flu often feel some or all of these symptoms:
- Fever or feeling feverish/chills (it’s important to note that not everyone with flu will have a fever)
- Cough
- Sore throat
- Runny or stuffy nose
- Muscle or body aches
- Headaches
- Fatigue (tiredness)
- Some people may have vomiting and diarrhea, though this is more common in children than adults.
Most people with the flu get better on their own. But it can be serious. It can cause complications and sometimes even death. Getting the flu vaccine every year is the best way to lower your chance of getting the flu and spreading it to others.
Table 6. Flu vs Cold
| Signs and Symptoms | Influenza | Cold |
|---|---|---|
| Symptom onset | Abrupt | Gradual |
| Fever | Usual; lasts 3-4 days | Rare |
| Aches | Usual; often severe | Slight |
| Chills | Fairly common | Uncommon |
| Fatigue, weakness | Usual | Sometimes |
| Sneezing | Sometimes | Common |
| Stuffy nose | Sometimes | Common |
| Sore throat | Sometimes | Common |
| Chest discomfort, cough | Common; can be severe | Mild to moderate; hacking cough |
| Headache | Common | Rare |
The emergency warning signs of flu sickness
Complications of flu can include bacterial pneumonia, ear infections, sinus infections, and worsening of chronic medical conditions, such as congestive heart failure, asthma, or diabetes.
In children
- Fast breathing or trouble breathing
- Bluish skin color
- Not drinking enough fluids
- Not waking up or not interacting
- Being so irritable that the child does not want to be held
- Flu-like symptoms improve but then return with fever and worse cough
- Fever with a rash
In adults
- Difficulty breathing or shortness of breath
- Pain or pressure in the chest or abdomen
- Sudden dizziness
- Confusion
- Severe or persistent vomiting
- Flu-like symptoms that improve but then return with fever and worse cough
In addition to the signs above, get medical help right away for any infant who has any of these signs:
- Being unable to eat
- Has trouble breathing
- Has no tears when crying
- Significantly fewer wet diapers than normal
How Flu Spreads
Most experts believe that flu viruses spread mainly by tiny droplets made when people with flu cough, sneeze or talk. These droplets can land in the mouths or noses of people who are nearby. Less often, a person might also get flu by touching a surface or object that has flu virus on it and then touching their own mouth, nose, or possibly their eyes.
Anyone can get the flu (even healthy people), and serious problems related to the flu can happen at any age, but some people are at high risk of developing serious flu-related complications if they get sick. This includes people 65 years and older, people of any age with certain chronic medical conditions (such as asthma, diabetes, or heart disease), pregnant women, and young children.
Period of Contagiousness
You may be able to pass on the flu to someone else before you know you are sick, as well as while you are sick. Although people with the flu are most contagious in the first 3-4 days after their illness begins, some otherwise healthy adults may be able to infect others beginning 1 day before symptoms develop and up to 5 to 7 days after becoming sick. Some people, especially young children and people with weakened immune systems, might be able to infect others with flu viruses for an even longer time.
Preventing Seasonal Flu
The first and most important step in preventing flu is to get a flu vaccination each year. CDC also recommends everyday preventive actions (like staying away from people who are sick, covering coughs and sneezes and frequent handwashing) to help slow the spread of germs that cause respiratory (nose, throat, and lungs) illnesses, like flu.
Diagnosing Flu
It is very difficult to distinguish the flu from other viral or bacterial causes of respiratory illnesses on the basis of symptoms alone. There are tests available to diagnose and detect influenza viruses in respiratory specimens. The most common are called “rapid influenza diagnostic tests (RIDTs).” RIDTs work by detecting the parts of the virus (antigens) that stimulate an immune response. These tests can provide results within approximately 10-15 minutes, but are not as accurate as other flu tests. Therefore, you could still have the flu, even though your rapid test result is negative. Other flu tests are called “rapid molecular assays” that detect genetic material of the virus. Rapid molecular assays produce results in 15-20 minutes and are more accurate than RIDTs. In addition, there are several more-accurate and sensitive flu tests available that must be performed in specialized laboratories, such as those found in hospitals or state public health laboratories. All of these tests require that a health care provider swipe the inside of your nose or the back of your throat with a swab and then send the swab for testing. Results may take one hour or several hours. However, rapid tests vary in their ability to detect flu viruses, depending on the type of rapid test used, and on the type of flu viruses circulating. Also, rapid tests appear to be better at detecting flu in children than adults. This variation in ability to detect viruses can result in some people who are infected with the flu having a negative rapid test result. (This situation is called a false negative test result.) Despite a negative rapid test result, your health care provider may diagnose you with flu based on your symptoms and their clinical judgment.
Will my health care provider test me for flu if I have flu-like symptoms?
Not necessarily. Most people with flu symptoms are not tested because the test results usually do not change how you are treated.
Your health care provider may diagnose you with flu based on your symptoms and their clinical judgment or they may choose to use an influenza diagnostic test. During an outbreak of respiratory illness, testing for flu can help determine if flu viruses are the cause of the outbreak. Flu testing can also be helpful for some people with suspected flu who are pregnant or have a weakened immune system, and for whom a diagnosis of flu can help their doctor make decisions about their care.
Treating Flu
There are influenza antiviral drugs that can be used to treat flu illness.
There are three FDA-approved antiviral drugs recommended by CDC to treat flu this season.
- oseltamivir (available as a generic version or under the trade name Tamiflu®),
- zanamivir (trade name Relenza®), and
- peramivir (trade name Rapivab®).
Generic oseltamivir and Tamiflu® are available as a pill or liquid suspension and are FDA approved for early treatment of flu in people 14 days old and older. Relenza® is a powder that is inhaled and approved for early treatment of flu in people 7 years of age and older. (Note: Relenza® is not recommended for people with breathing problems like asthma or COPD.) Rapivab® is given intravenously by a health care provider and is approved for early treatment of flu in people 2 years of age and older.
To treat the flu, oseltamivir and zanamivir are usually prescribed to be taken twice daily for 5 days, although people hospitalized with the flu may need antiviral treatment for longer than 5 days. Peramivir is given one time intravenously over a period of 15 to 30 minutes.
Can children take antiviral drugs?
Yes. Oseltamivir is recommended by the CDC and American Academy of Pediatrics (AAP) for early treatment of flu in people of any age, and for the prevention of flu (i.e., prophylaxis) in people 3 months of age and older. Zanamivir is recommended for early treatment of flu in people 7 years of age and older, and for the prevention of flu in people 5 years of age and older. Peramivir is recommended for early treatment in people 2 years of age and older.
Can pregnant women take antiviral drugs?
Yes. Oral oseltamivir is recommended for treatment of pregnant women with flu because compared to other recommended antiviral medications it has the most studies available to suggest that it is safe and beneficial during pregnancy.
How flu shot works
The injected flu vaccine stimulates your body’s immune system to make antibodies to attack the flu virus.
Antibodies are proteins that recognize and fight off germs, such as viruses, that have invaded your blood.
If you’re exposed to the flu virus after you’ve had the flu vaccine, your immune system will recognize the virus and immediately produce antibodies to fight it.
It may take 10 to 14 days for your immunity to build up fully after you have had the flu shot.
You need to have a flu shot every year, as the antibodies that protect you from flu decline over time, and flu strains can also change from year to year.
Flu vaccines cause antibodies to develop in the body about two weeks after vaccination. These antibodies provide protection against infection with the viruses that are in the vaccine.
The seasonal flu vaccine protects against the influenza viruses that research indicates will be most common during the upcoming season. Traditional flu vaccines (called “trivalent” vaccines) are made to protect against three flu viruses; an influenza A (H1N1) virus, an influenza A (H3N2) virus, and an influenza B virus. There are also flu vaccines made to protect against four flu viruses (called “quadrivalent” vaccines). These vaccines protect against the same viruses as the trivalent vaccine and an additional B virus.
Is it safe to get a flu shot during pregnancy?
Yes, it’s safe to get a flu shot during pregnancy. In fact, the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists recommend that all women who are pregnant during flu season get a flu shot, regardless of their trimester.
A flu shot during pregnancy can help:
- Prevent the flu and maternal complications. The flu is more likely to cause severe illness in pregnant women than in women who are not pregnant. Getting the flu during pregnancy increases your risk of becoming hospitalized. A flu shot will decrease your risk of getting the flu during your pregnancy.
- Prevent potential pregnancy problems due to the flu. Some research suggests that having the flu or a flu-like illness during the first trimester of pregnancy is linked with an increased risk of fetal birth defects. Flu during pregnancy is also linked with an increased risk of miscarriage, premature birth, low birth weight and fetal death.
- Protect your baby after birth. Infants are at increased risk of severe flu symptoms, but childhood flu vaccines can’t begin until a baby is 6 months old. If you have a flu shot during pregnancy, the antibodies you develop will pass through the placenta and breast milk, if you’re breast-feeding. These antibodies will help protect your baby from the flu after birth.
When you get vaccinated, request the flu shot — not the nasal spray vaccine. The flu shot is made from an inactivated virus, so it’s safe for both mother and baby during any stage of pregnancy. The nasal spray vaccine isn’t recommended for use in pregnant women.
While all vaccines carry some risk of adverse effects, such as an allergic reaction, no research has shown an increased risk of complications associated with the flu shot for pregnant women. Women can get the flu shot at any time during pregnancy. There also is no evidence that adverse effects occur in the children of women who receive vaccines with the mercury-based preservative thimerosal during pregnancy. In addition, single-dose flu shots don’t contain thimerosal. If you have concerns about the flu shot during pregnancy, talk to your doctor.
Should I get a flu shot?
It depends if you’re in the high-risk group of people who can develop severe flu complications when you have the flu.
Anyone can get the flu (even healthy people), and serious problems related to the flu can happen at any age, but some people are at high risk of developing serious flu-related complications if they get sick. This includes people 65 years and older, people of any age with certain chronic medical conditions (such as asthma, diabetes, or heart disease), pregnant women, and young children. If you have heart disease, flu shots can reduce your risk of flu-related complications. While doctors have long recommended that older adults and other high-risk groups get flu shots, they’re now emphasizing the importance of flu shots for those with heart disease too.
Most people who get the flu will have mild illness, will not need medical care or antiviral drugs, and will recover in less than two weeks. Some people, however, are more likely to get flu complications that can result in hospitalization and sometimes death. Pneumonia, bronchitis, sinus infections and ear infections are examples of flu-related complications. The flu also can make chronic health problems worse. For example, people with asthma may experience asthma attacks while they have the flu, and people with chronic congestive heart failure may experience a worsening of this condition triggered by flu. List below are the groups of people who are more likely to get serious flu-related complications if they get sick with influenza.
Why are flu shots important for those with heart disease?
If you have heart disease, you’re at increased risk of complications from the flu — including pneumonia, respiratory failure, heart attack and death. Having the flu can also worsen pre-existing conditions, such as heart failure, diabetes or asthma.
Even if you get the flu despite having a flu shot, you’ll probably have a less severe case of the flu. If you have heart disease, some research suggests that getting a flu shot might even lower your risk of a heart attack or other cardiovascular event, or death from a cardiovascular event. More research is needed to confirm this benefit, however.
It’s also a good idea to get a flu shot if you live with or care for someone who has heart disease. Lowering your risk of getting the flu will lower the risk of those around you.
Flu Complications
Most people who get influenza will recover in a few days to less than two weeks, but some people will develop complications (such as pneumonia) as a result of the flu, some of which can be life-threatening and result in death.
Sinus and ear infections are examples of moderate complications from flu, while pneumonia is a serious flu complication that can result from either influenza virus infection alone or from co-infection of flu virus and bacteria. Other possible serious complications triggered by flu can include inflammation of the heart (myocarditis), brain (encephalitis) or muscle (myositis, rhabdomyolysis) tissues, and multi-organ failure (for example, respiratory and kidney failure). Flu virus infection of the respiratory tract can trigger an extreme inflammatory response in the body and can lead to sepsis, the body’s life-threatening response to infection. Flu also can make chronic medical problems worse. For example, people with asthma may experience asthma attacks while they have the flu, and people with chronic heart disease may experience a worsening of this condition triggered by flu.
People at High Risk for Developing Flu-Related Complications
- Children younger than 5, but especially children younger than 2 years old
- Adults 65 years of age and older
- Pregnant women (and women up to two weeks postpartum)
- Residents of nursing homes and other long-term care facilities
- Also, American Indians and Alaska Natives
People who have medical conditions including:
- Asthma
- Neurological and neurodevelopmental conditions [including disorders of the brain, spinal cord, peripheral nerve, and muscle such as cerebral palsy, epilepsy (seizure disorders), stroke, intellectual disability, moderate to severe developmental delay, muscular dystrophy, or spinal cord injury].
- Chronic lung disease (such as chronic obstructive pulmonary disease [COPD] and cystic fibrosis)
- Heart disease (such as congenital heart disease, congestive heart failure and coronary artery disease)
- Blood disorders (such as sickle cell disease)
- Endocrine disorders (such as diabetes mellitus)
- Kidney disorders
- Liver disorders
- Metabolic disorders (such as inherited metabolic disorders and mitochondrial disorders)
- Weakened immune system due to disease or medication (such as people with HIV or AIDS, or cancer, or those on chronic steroids)
- People younger than 19 years of age who are receiving long-term aspirin therapy
- People with extreme obesity (body mass index [BMI] of 40 or more).
Note: There is no recommendation for pregnant women or people with pre-existing medical conditions to get special permission or written consent from their doctor or health care professional for influenza vaccination if they get vaccinated at a worksite clinic, pharmacy or other location outside of their physician’s office.
Is it safe to get a flu shot if I have heart disease?
Flu shots are safe for most people who have heart disease.
Flu vaccines are usually injected by needle into the upper extremity. Some people develop short-lived side effects, such as mild arm soreness at the injection site, a mild fever or muscle aches.
The flu vaccine that can be given as a nasal spray (FluMist) isn’t recommended for people with heart disease. This type of flu vaccine is made with live virus that can trigger flu symptoms in some people.
Talk to your doctor before getting a flu shot if:
- You’re allergic to eggs
- You’ve had a serious allergic reaction to the flu vaccine in the past
- You have a history of Guillain-Barre syndrome that developed after receiving a flu shot
- You’re sick with a fever at the time you plan to get a flu shot
Can you get the flu from the flu shot?
No, the flu shot cannot cause flu. The flu vaccines either contain inactivated virus, meaning the viruses are no longer infectious, or a particle designed to look like a flu virus to your immune system. While the nasal spray flu vaccine does contain a live virus, the viruses are changed so that they cannot give you the flu.
When should I get a flu shot?
You can get the flu shot each autumn when it becomes available, usually sometime in August through November.
- Optimally, vaccination should occur before onset of influenza activity in the community.
- Vaccination should be offered by end of October, if possible.
- Vaccination should be offered as long as influenza viruses are circulating and unexpired vaccine is available.
- Children aged 6 months through 8 years who require 2 doses should receive their first dose as soon as possible after vaccine becomes available, and the second dose ≥4 weeks later.
However, if flu shots are still available and you haven’t yet received a vaccination, you can still benefit from getting a flu shot in January or later. That’s because the flu season doesn’t usually peak until the winter.
Where to get flu shot?
Flu vaccines are offered in many locations, including doctor’s offices, clinics, health departments, pharmacies and college health centers, as well as by many employers, and even in some schools.
Even if you don’t have a regular doctor or nurse, you can get a flu vaccine somewhere else, like a health department, pharmacy, urgent care clinic, and often your school, college health center, or workplace.
The following Vaccine Locator (https://vaccinefinder.org/) is a useful tool for finding vaccine in your area.
How long does the flu shot last?
You need to have a flu shot every year, as the antibodies that protect you from flu decline over time, and flu strains can also change from year to year.
Why do I need a flu vaccine every year?
A flu vaccine is needed every season for two reasons. First, the body’s immune response from vaccination declines over time, so an annual vaccine is needed for optimal protection. Second, because flu viruses are constantly changing, the formulation of the flu vaccine is reviewed each year and sometimes updated to keep up with changing flu viruses. For the best protection, everyone 6 months and older should get vaccinated annually.
Can I get seasonal flu even though I got a flu vaccine this year?
Yes. There is still a possibility you could get the flu even if you got vaccinated. The ability of flu vaccine to protect a person depends on various factors, including the age and health status of the person being vaccinated, and also the similarity or “match” between the viruses used to make the vaccine and those circulating in the community. If the viruses in the vaccine and the influenza viruses circulating in the community are closely matched, vaccine effectiveness is higher. If they are not closely matched, vaccine effectiveness can be reduced. However, it’s important to remember that even when the viruses are not closely matched, the vaccine can still protect many people and prevent flu-related complications. Such protection is possible because antibodies made in response to the vaccine can provide some protection (called cross-protection) against different but related influenza viruses.
Does flu vaccine work right away?
No. It takes about two weeks after vaccination for antibodies to develop in the body and provide protection against influenza virus infection. That’s why it’s better to get vaccinated early in the fall, before the flu season really gets under way.
Are there some people who should not receive a flu vaccine?
The Centers for Disease Control and Prevention (CDC) 9 recommends everyone 6 months of age and older should receive an annual flu vaccination with rare exceptions.
Individuals who can’t get the flu shot include:
- Children younger than 6 months, since they are too young to get a flu shot.
- Individuals with severe, life-threatening allergies to flu vaccine or any ingredient(s) in the vaccine.
Individuals should talk with their doctor before getting the flu shot if they:
- Have had a severe allergy to eggs or any of the ingredients in the vaccine.
- See Special Considerations Regarding Egg Allergy for more information about egg allergies and flu vaccine.
- Have had Guillain-Barré syndrome (GBS).
- Are not feeling well.
There are multiple flu vaccines available, and not all flu vaccines can be given to people of all ages. Talk to your doctor if you have any questions regarding which flu vaccine options are best for you and your family.
What is in the flu shot
As there are lots of different flu vaccines produced each year, for more detailed information on ingredients ask your doctor or nurse for the patient information leaflet for the specific vaccine being offered.
Flu shot ingredients: for US-licensed flu vaccines are available at the U.S. Food and Drug Administration https://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm093833.htm
Flu shot effectiveness
The CDC conducts studies each year to determine how well the influenza (flu) vaccine protects against flu illness. While vaccine effectiveness can vary, recent studies show that flu vaccination reduces the risk of flu illness by between 40% and 60% among the overall population during seasons when most circulating flu viruses are well-matched to the flu vaccine. In general, current flu vaccines tend to work better against influenza B and influenza A(H1N1) viruses and offer lower protection against influenza A(H3N2) viruses.
Two general types of studies are used to determine how well flu vaccines work: randomized controlled trials and observational studies. Vaccine effectiveness refers to vaccine protection measured in observational studies that include people with underlying medical conditions who have been administered vaccines by different health care providers under real-world conditions.
The measurement of influenza vaccine efficacy and effectiveness can be affected by virus and host factors as well as the study methodology used. Therefore, vaccine efficacy/effectiveness point estimates have varied among published studies.
Virus factors
The protective benefits of influenza vaccination are generally lower during flu seasons where the majority of circulating influenza viruses differ from the influenza viruses used to make the vaccines. Influenza viruses are continuously changing through a natural process known as antigenic drift. However, the degree of antigenic drift and the frequency of drifted viruses in circulation can vary for each of the three or four viruses included in the seasonal flu vaccine. So even when circulating influenza viruses are mildly or moderately drifted in comparison to the vaccine, it is possible that people may still receive some protective benefit from vaccination; and if other circulating influenza viruses are well matched, the vaccine could still provide protective benefits overall. It is not possible to predict how well the vaccine and circulating strains will be matched in advance of the influenza season, nor is it possible to predict how this match may affect vaccine effectiveness.
Host factors
In addition to virus factors, host factors such as age, underlying medical conditions, history of prior infections and prior vaccinations can affect the benefits received from vaccination.
Flu vaccine effectiveness
Adults 65 years or older
Among older adults, annual influenza vaccination was recommended based on the high burden of influenza-related disease and demonstrated vaccine efficacy among younger adults. One randomized controlled trial of adults aged 60 years and older relied on serology for confirmation of influenza and reported a vaccine efficacy of 58% 10. However, it is unknown if infections were missed by serology among the study participants that were vaccinated and if the vaccine efficacy estimate is biased upwards. A meta-analysis of observational studies that used the test-negative design provided vaccine effectiveness estimates for adults aged >60 years against RT-PCR confirmed influenza infection. This meta-analysis reported significant vaccine effectiveness of 52% 11 during seasons when the vaccine and circulating viruses were well-matched. During seasons when the circulating viruses were antigenically drifted (not well matched), reported vaccine effectiveness was 36% 11.
An randomized controlled trial that compared a high-dose, inactivated influenza vaccine (containing four times the standard amount of influenza antigen) to standard dose vaccine in persons aged 65 years or older during the 2011-12 and 2012-13 influenza seasons found that rates of laboratory-confirmed influenza were 24% lower 12 among persons who received high-dose vaccine compared to standard dose influenza vaccine, indicating that high-dose vaccine provided 24% better protection against influenza than standard dose vaccine in this trial.
Several observational studies have reported significant vaccine effectiveness against RT-PCR confirmed influenza-related hospitalization among older adults. A three-year study (2006-07 through 2008-09) in Tennessee that used a test-negative design reported vaccine effectiveness of 61% 13 among hospitalized adults >50 years of age. In an analysis of two additional seasons, including 2010-11 and 2011-2012 (excluding 2009-10), vaccine effectiveness was 58% 14 against RT-PCR confirmed influenza associated hospitalizations for persons >50 years of age for the five seasons combined.
Adults
Several randomized controlled trials have been done in healthy adults aged <65 years 15, 16, 17. These studies have reported vaccine efficacy estimates ranging from 16%-75%; vaccine effectiveness of 16% was reported during a season with few influenza infections. An randomized controlled trial in South Africa among HIV infected adults reported vaccine efficacy of 76% 18. A meta-analysis that included data from randomized controlled trials of licensed inactivated influenza vaccines reported a pooled vaccine effectiveness of 59% 19 against influenza confirmed by RT-PCR or viral culture. In addition, randomized controlled trials of cell-based inactivated influenza vaccines (IIVs) and recombinant trivalent HA protein vaccines have been performed among healthy adults. In general, efficacy estimates for these types of vaccines are similar to other inactivated influenza vaccines that are egg-based 20.
Children
In a four-year randomized controlled trial of inactivated vaccines among children aged 1–15 years, vaccine efficacy was estimated at 77% against influenza A (H3N2) and 91% against influenza A (H1N1) virus infection 21. An randomized controlled trial of children aged 6–24 months reported vaccine efficacy of 66% against laboratory-confirmed influenza in 1999-2000 but no vaccine efficacy during the second year when there was little influenza activity 22. During 2010-11, the vaccine efficacy of a quadrivalent inactivated vaccine among children aged 3-8 years was 59% 23. In addition, a cluster-randomized trial conducted in Hutterite communities in Canada found that vaccinating children aged 3 to 15 years with trivalent inactivated influenza vaccine before the 2008-09 season reduced RT-PCR confirmed influenza in the entire community by 61%, including a 59% reduction in confirmed influenza among non-vaccinated community members, evidence of the “indirect” effect of influenza vaccination on prevention on disease transmission 24.
Several randomized controlled trials of live attenuated influenza vaccines among young children have demonstrated vaccine efficacy against laboratory confirmed influenza with estimates ranging from 74%-94% 25, 26. A study conducted among children aged 12 through 36 months living in Asia during consecutive influenza seasons reported efficacy for live attenuated influenza vaccine of 64%–70% 27.
In 2017, a study in the journal Pediatrics 28 was the first of its kind to show that flu vaccination also significantly reduced a child’s risk of dying from the flu. The study, which looked at data from four flu seasons between 2010 and 2014, found that flu vaccination reduced the risk of flu-associated death by half (51 percent) among children with underlying high-risk medical conditions and by nearly two-thirds (65 percent) among healthy children.
Pregnant women
An randomized controlled trial conducted among pregnant women in South Africa during 2011 and 2012 reported vaccine efficacy against RT-PCR confirmed influenza of 50% among HIV-negative women and 58% among HIV-positive women vaccinated during the third trimester 29. In addition, the trial showed that vaccination reduced the incidence of laboratory-confirmed influenza among infants born to HIV-negative women by 49%; the study was unable to assess vaccine efficacy among infants of HIV infected women. An observational study in the United States during 2010-11 and 2011-12 using a test-negative design reported vaccine effectiveness of 44% against influenza among pregnant woman 30.
A randomized trial in Bangladesh found that babies born to mothers vaccinated during pregnancy with trivalent inactivated influenza vaccines were significantly less likely to be born small for gestational age and weighed an average of 200g more than babies born to unvaccinated mothers 31. No effect of maternal immunization on infant birth weight was reported in the South African trial described above. Some observational studies in developed and developing countries have found lower risk of prematurity or low birth weight in babies born to vaccinated mothers, but the effect has not been consistently demonstrated 32.
How well does the live attenuated influenza vaccine (LAIV) work compared to inactivated influenza vaccine (IIV)?
Children
Three randomized clinical trials comparing live attenuated influenza vaccine to trivalent inactivated influenza vaccine in young children, 2-8 years of age, suggested that live attenuated influenza vaccine had superior efficacy compared to inactivated influenza vaccine 33. Recently, several observational studies suggest that LAIV did not consistently provide better protection against influenza than inactivated vaccine, especially against influenza caused by the 2009 H1N1 pandemic virus 34). However, a randomized, school-based study in Canada reported lower rates of confirmed influenza among students vaccinated with live-attenuated vaccine compared to students vaccinated with inactivated influenza vaccine, as well as decreased influenza transmission among family members of students vaccinated with live-attenuated influenza vaccines 35.
Adults
Clinical trials during 2004-05, 2005-06, and 2007-08 that compared inactivated influenza vaccines and live attenuated influenza vaccines to no vaccine among adults suggested that inactivated influenza vaccines provided better protection against influenza than live attenuated influenza vaccines in adults 36.
Flu shot side effects
Like any medical product, vaccines can cause side effects. Side effects of the flu vaccine are generally mild and go away on their own within a few days.
Most people who get a flu shot do not have any problems with the flu shots.
Common side effects from the flu shot include:
- Soreness, redness, and/or swelling from where the flu shot was given
- Headache
- Fever
- Nausea
- Muscle aches
- Hoarseness
- Sore, red or itchy eyes
- Cough
- Itching
- Fatigue
If these problems occur, they usually begin soon after the shot and last 1 or 2 days.
The flu shot, like other injections, can occasionally cause fainting.
More serious problems following a flu shot can include the following:
- Young children who get the flu shot along with pneumococcal vaccine (PCV13) and/or DTaP vaccine at the same time might be slightly more likely to have a seizure caused by fever. Ask your doctor for more information. Tell your doctor if a child who is getting flu vaccine has ever had a seizure.
- Some studies have found a possible small association of injectable flu vaccine with Guillain-Barré syndrome. Overall, these studies estimated the risk for Guillain-Barré syndrome after vaccination as fewer than 1 or 2 cases of Guillain-Barré syndrome per one million people vaccinated. Other studies have not found any association. Guillain-Barré syndrome also, rarely, occurs after flu illness. Even though Guillain-Barré syndrome following flu illness is rare, Guillain-Barré syndrome is more common following flu illness than following flu vaccination. Guillain-Barré syndrome has not been associated with the nasal spray flu vaccine.
Flu shot allergic reaction
With any vaccine, look for any unusual conditions, such as a high fever, behavior changes, or signs of a severe allergic reaction after vaccination.
Signs of a severe allergic reaction can include:
- Difficulty breathing
- Hoarseness or wheezing
- Swelling around the eyes or lips
- Hives
- Paleness
- Weakness
- A fast heart beat or dizziness
Life threatening allergic reactions to the flu shot are rare. These signs would most likely happen within a few minutes to a few hours after the vaccine is given.
If you think it is a severe allergic reaction or other emergency that can’t wait, call your local emergency services number and get to the nearest hospital. Otherwise, call your doctor.
Afterward, the reaction should be reported to the Vaccine Adverse Event Reporting System. Your doctor might file this report, or you can do it yourself through the Vaccine Adverse Event Reporting System website (https://vaers.hhs.gov/) or by calling 1-800-822-7967.
- 2017-18 Summary of Recommendations. https://www.cdc.gov/flu/professionals/acip/2017-18summary.htm[↩][↩][↩]
- ACIP Vaccine Recommendations and Guidelines. https://www.cdc.gov/vaccines/hcp/acip-recs/index.html[↩][↩]
- Influenza Vaccination Coverage. https://www.cdc.gov/flu/index.htm[↩]
- Vaccination: Who Should Do It, Who Should Not and Who Should Take Precaution. https://www.cdc.gov/flu/protect/whoshouldvax.htm[↩]
- Influenza vaccines — United States, 2017–18 influenza season* https://www.cdc.gov/flu/protect/vaccine/vaccines.htm[↩]
- 2013 IDSA Clinical Practice Guideline for Vaccination of the Immunocompromised Host. https://academic.oup.com/cid/article/58/3/e44/336537[↩]
- Flu Vaccine and People with Egg Allergies. https://www.cdc.gov/flu/protect/vaccine/egg-allergies.htm[↩][↩]
- Flu Symptoms & Complications. https://www.cdc.gov/flu/consumer/symptoms.htm[↩]
- Influenza Vaccination Coverage. https://www.cdc.gov/flu/fluvaxview/index.htm[↩]
- Govaert TM, Thijs CT, Masurel N, Sprenger MJ, Dinant GJ, Knottnerus JA. The efficacy of influenza vaccination in elderly individuals. A randomized double-blind placebo-controlled trial. JAMA. 1994;272(21):1661-5. https://jamanetwork.com/journals/jama/article-abstract/383571[↩]
- Darvishian M, Bijlsma MJ, Hak E, van den Heuvel ER. Effectiveness of seasonal influenza vaccine in community-dwelling elderly people: a meta-analysis of test-negative design case-control studies. Lancet Infect Dis 2014; 14(12): 1228-39.[↩][↩]
- DiazGranados CA, Dunning AJ, Kimmel M, Kirby D, Treanor J, Collins A, Pollak R, Christoff J, Earl J, Landolfi V, Martin E, Gurunathan S, Nathan R, Greenberg DP, Tornieporth NG, Decker MD, Talbot HK. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N Engl J Med. 2014;371:635-45.[↩]
- Talbot HK, Griffin MR, Chen Q, Zhu Y, Williams JV, Edwards, KM. Effectiveness of seasonal vaccine in preventing confirmed influenza-associated hospitalization in community dwelling older adults. J Infect Dis 2011; 203: 500–8.[↩]
- Chen Q, Griffin MR, Nian H, Zhu Y, Williams JV, Edwards, KM, Talbot HK. Influenza vaccine prevents medically attended influenza-associated acute respiratory illness in adults aged ≥50 years. J Infect Dis 2015; 211: 1045–50.[↩]
- Jackson LA, Gaglani MJ, Keyserling HL, et al. Safety, efficacy, and immunogenicity of an inactivated influenza vaccine in healthy adults: a randomized, placebo-controlled trial over two influenza seasons. BMC Infect Dis 2010; 10: 71.[↩]
- Monto AS, Ohmit SE, Petrie JG, et al. Comparative efficacy of inactivated and live attenuated influenza vaccines. N Engl J Med 2009; 361(13): 1260-7.[↩]
- eran J, Vesikari T, Wertzova V, et al. Efficacy of inactivated split-virus influenza vaccine against culture-confirmed influenza in healthy adults: a prospective, randomized, placebo-controlled trial. J Infect Dis 2009; 200(12): 1861-9.[↩]
- Madhi SA, Maskew M, Koen A, Kuwanda L, Besselaar TG, Naidoo D, Cohen C, Valette M, Cutland CL, Sanne I. Trivalent inactivated influenza vaccine in African adults infected with human immunodeficient virus: double blind, randomized clinical trial of efficacy, immunogenicity, and safety. Clin Infect Dis 2011; 52(1): 128-37.[↩]
- Osterholm MT, Kelley NS, Sommer A, et al. Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet ID 2011(12): 36-44. https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(11)70295-X/fulltext[↩]
- Barrett PN, Berezuk G, Fritsch S, et al. Efficacy, safety, and immunogenicity of a Vero-cell-culture-derived trivalent influenza vaccine: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2011; 377(9767): 751-9.[↩]
- Neuzil KM, Dupont WD, Wright PF, Edwards KM. Efficacy of inactivated and cold-adapted vaccines against influenza A infection, 1985 to 1990: the pediatric experience. Pediatr Infect Dis J. 2001;20(8):733-40 https://journals.lww.com/pidj/Abstract/2001/08000/Efficacy_of_inactivated_and_cold_adapted_vaccines.4.aspx[↩]
- Hoberman A, Greenberg DP, Paradise JL, Rockette HE, Lave JR, Kearney DH, Colborn DK, Kurs-Lasky M, Haralam MA, Byers CJ, Zoffel LM, Fabian IA, Bernard BS, Kerr JD. Effectiveness of inactivated influenza vaccine in preventing acute otitis media in young children: a randomized controlled trial. JAMA. 2003;290(12):1608-16. https://jamanetwork.com/journals/jama/fullarticle/197348[↩]
- Jain VK, Rivera L, Zaman K, et al. Vaccine for prevention of mild and moderate-to-severe influenza in children. N Engl J Med 2013; 369(26): 2481-91.[↩]
- Loeb M, Russell ML, Moss L, et al. Effect of influenza vaccination of children on infection rates in Hutterite communities: a randomized trial. JAMA 2010; 303(10): 943-50.[↩]
- Bracco Neto H, Farhat CK, Tregnaghi MW, et al. Efficacy and safety of 1 and 2 doses of live attenuated influenza vaccine in vaccine-naive children. Pediatr Infect Dis J 2009;28:365–71.[↩]
- Vesikari T, Fleming DM, Aristegui JF, et al. Safety, efficacy, and effectiveness of cold-adapted influenza vaccine-trivalent against community-acquired, culture-confirmed influenza in young children attending day care. Pediatrics 2006;118:2298–312.[↩]
- Tam JS, Capeding MR, Lum LC, et al. Efficacy and safety of a live attenuated, cold-adapted influenza vaccine, trivalent against culture-confirmed influenza in young children in Asia. Pediatr Infect Dis J 2007;26:619–28.[↩]
- Influenza Vaccine Effectiveness Against Pediatric Deaths: 2010–2014. Pediatrics Apr 2017, e20164244; DOI: 10.1542/peds.2016-4244 http://pediatrics.aappublications.org/content/early/2017/03/30/peds.2016-4244[↩]
- Madhi SA, Cutland CL, Kuwanda L, et al. Influenza vaccination of pregnant women and protection of their infants. N Engl J Med 2014; 371(10): 918-31.[↩]
- Thompson MG, Li DK, Shifflett P, et al. Effectiveness of seasonal trivalent influenza vaccine for preventing influenza virus illness among pregnant women: a population-based case-control study during the 2010-2011 and 2011-2012 influenza seasons. Clin Infect Dis 2014; 58(4): 449-57.[↩]
- Steinhoff MC, Omer SB, Roy E, et al. Neonatal outcomes after influenza immunization during pregnancy: a randomized controlled trial. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne 2012.[↩]
- Richards JL, Hansen C, Bredfeldt C, et al. Neonatal outcomes after antenatal influenza immunization during the 2009 H1N1 influenza pandemic: impact on preterm birth, birth weight, and small for gestational age birth. Clin Infect Dis 2013;56:1216-22.[↩]
- Belshe RB, Edwards KM, Vesikari T, Black SV, Walker RE, Hultquist M, Kemble G, Connor EM; CAIV-T Comparative Efficacy Study Group. Live attenuated versus inactivated influenza vaccine in infants and young children. N Engl J Med. 2007;356(7):685-96 http://www.columbia.edu/itc/hs/medical/pathophys/immunology/2008/teamA_fluvaccine.pdf[↩]
- Gaglani M , Pruszynski J, Murthy K, Clipper L, Robertson A, Reis M, Chung JR, Piedra PA, Avadhanula V, Nowalk MP Zimmerman RK, Jackson ML, Jackson LA, Petrie JG, Ohmit SE, Monto AS, McLean HQ, Belongia EA, Fry AM, Flannery B. Influenza Vaccine Effectiveness against the 2009 Pandemic A (H1N1) Virus Differed by Vaccine-type During 2013-14 in the United States. J Inf Dis (in press[↩]
- Kwong J, Pereira J, Quach S, Pellizzari R, Dusome E, Russell M, et al. Randomized evalution of live attenuated vs. trivalent inactivated influenza vaccines in schools (RELATIVES) pilot study: preliminary results from the household surveillance sub-study.[↩]
- Ohmit SE, Victor JC, Teich ER, et al. Prevention of symptomatic seasonal influenza in 2005-2006 by inactivated and live attenuated vaccines. J Infect Dis 2008; 198(3): 312-7.[↩]





{kind=link}