Contents
What is fragile X syndrome
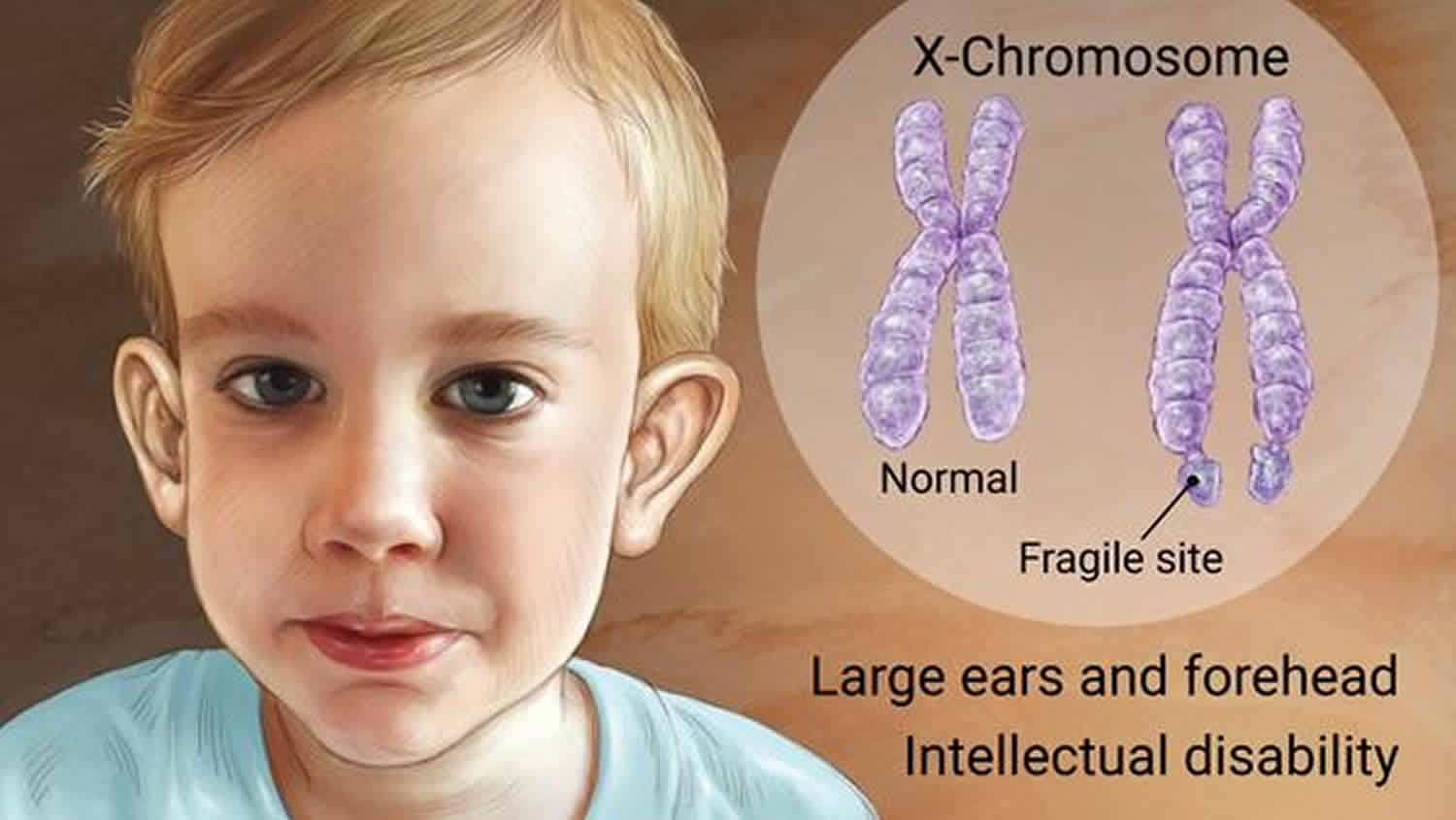
Fragile X syndrome is the most common form of inherited intellectual disability (learning disabilities and cognitive impairment) 1. Usually, males are more severely affected by this disorder than females. Affected individuals usually have delayed development of speech and language by age 2 2. Most males with fragile X syndrome have mild to moderate intellectual disability, while about one-third of affected females are intellectually disabled. Children with fragile X syndrome may also have anxiety and hyperactive behavior such as fidgeting or impulsive actions. They may have attention deficit disorder (ADD), which includes an impaired ability to maintain attention and difficulty focusing on specific tasks. About one-third of individuals with fragile X syndrome have features of autism spectrum disorders that affect communication and social interaction. Seizures occur in about 15 percent of males and about 5 percent of females with fragile X syndrome 2.
Fragile X syndrome affects both males and females. However, females often have milder symptoms than males. The exact number of people who have fragile X syndrome is unknown, but it has been estimated that about 1.4 per 10,000 males and 0.9 per 10,000 females have fragile X syndrome 3.
Most males and about half of females with fragile X syndrome have characteristic physical features that become more apparent with age. These features include a long and narrow face, large ears, a prominent jaw and forehead, unusually flexible fingers, flat feet, and in males, enlarged testicles (macroorchidism) after puberty.
Mutations in the fragile X mental retardation 1 (FMR1) gene cause fragile X syndrome. Normally, the gene makes a protein called fragile X mental retardation protein (FMRP) that you need for brain development. But the FMR1 gene mutation causes a person to make little or none of the protein. This causes the symptoms of Fragile X. People with only a small change in the gene might not show any signs of Fragile X. People with bigger changes can have severe symptoms.
Fragile X syndrome is inherited, which means it is passed down from parents to children. Anyone with the FMR1 gene mutation can pass it to their children. However, a person who inherits the gene mutation may not develop Fragile X syndrome. Males will pass it down to all of their daughters and not their sons. Females have a 50/50 chance to pass it along to both their sons and daughters. In some cases, an FMR1 premutation can change to a full mutation when it is passed from parent to child.
Fragile X syndrome symptoms might include:
- Intelligence problems, ranging from learning disabilities to severe intellectual disabilities
- Social and emotional problems, such as aggression in boys or shyness in girls
- Speech and language problems, especially in boys
- Sensitivity to noise, light, or other sensory information
People with Fragile X syndrome may not have noticeable symptoms, or they can have more serious symptoms that range from learning disabilities to cognitive and behavior problems.
Fragile X-associated disorders include:
- Fragile X syndrome
- Fragile X-associated primary ovarian insufficiency
- Fragile X-associated tremor/ataxia syndrome
A genetic blood test can diagnose Fragile X.
There is no cure for fragile X syndrome. You can treat some symptoms with educational, behavioral, or physical therapy, and with medicines. However, getting treatment early can help. Treatment services can help people learn important skills. Services can include therapy to learn to talk, walk, and interact with others. In addition, medicine can be used to help control some issues, such as behavior problems. To develop the best treatment plan, people with fragile X syndrome, parents, and health care providers should work closely with one another, and with everyone involved in treatment and support—which may include teachers, childcare providers, coaches, therapists, and other family members. Taking advantage of all the resources available will help guide success.
Early intervention services help children from birth to 3 years old (36 months) learn important skills. These services may improve a child’s development. Even if the child has not been diagnosed with fragile X syndrome, he or she may be eligible for services. These services are provided through an early intervention system in each state. Through this system, you can ask for an evaluation. In addition, treatment for particular symptoms, such as speech therapy for language delays, often does not need to wait for a formal diagnosis. While early intervention is extremely important, treatment services at any age can be helpful.
- Learn more about Early intervention here: https://www.parentcenterhub.org/ei-overview/
- You may also want to contact the National Fragile X Foundation: https://fragilex.org/
Are there specific disorders or conditions associated with Fragile X syndrome?
Fragile X Syndrome (fragile X syndrome) often occurs with other conditions. Some of these conditions include anxiety, attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorders, depression, difficult peer relationships, intellectual disabilities, and learning disabilities.
Among the other conditions associated with Fragile X syndrome are the following:
- Autism spectrum disorder. Up to one-half of people with Fragile X also meet the criteria for autism spectrum disorder 4.
- Mitral valve prolapse. In mitral valve prolapse, a heart condition, the valve that separates the upper and lower left chambers of the heart does not work properly. This condition is usually not life-threatening, but in severe cases, surgery might be required to correct the problem.
- Seizures. Up to one-fifth of children with Fragile X syndrome also have seizures. Seizures associated with the syndrome are more common in boys than in girls 5.
- Anxiety. There are many different types of anxiety disorders with many different causes and symptoms. These include generalized anxiety disorder, obsessive-compulsive disorder (OCD), panic disorder, post-traumatic stress disorder, separation anxiety, and different types of phobias. Separation anxiety is most common among young children. These children feel very worried when they are apart from their parents.
- Attention-Deficit/Hyperactivity Disorder (ADHD). Children with attention-deficit/hyperactivity disorder (ADHD) have trouble paying attention and controlling impulsive behaviors. They might act without thinking about what the result will be and, in some cases, they are also overly active. It is normal for children to have trouble focusing and behaving at one time or another. However, these behaviors continue beyond early childhood (0-5 years of age) among children with ADHD. Symptoms of ADHD can continue and can cause difficulty at school, at home, or with friends.
- Depression. Everyone feels worried, anxious, sad, or stressed from time to time. However, if these feelings do not go away and they interfere with daily life (for example, keeping a child home from school or other activities, or keeping an adult from working or attending social activities), a person might have depression. Having either a depressed mood or a loss of interest or pleasure for at least two weeks might mean that someone has depression. Children and teens with depression might be irritable instead of sad. Depression can be treated with counseling and medication.
- Difficult Peer Relationships. Fragile X syndrome can have many effects on a child’s development. It can make childhood friendships, or peer relationships, very difficult. These relationships contribute to children’s immediate happiness and may be very important to their long-term development. Children with fragile X syndrome might have difficulty in their peer relationships, for example, being rejected by peers or not having close friends. In some cases, children with peer problems may also be at higher risk for anxiety, behavioral and mood disorders, substance abuse and delinquency as teenagers.
- Intellectual Disability. People with intellectual disability have a significantly below-average score on a test of mental ability or intelligence and limitations in the ability to function in areas of daily life, such as communication, self-care, and getting along in social situations and school activities. Children with intellectual disability can and do learn new skills, but they develop more slowly than children with average intelligence and adaptive skills. There are different degrees of intellectual disability, ranging from mild to severe. A person’s level of intellectual disability can be defined by their intelligence quotient (IQ), or by the types and amount of support they need.
- Learning Disabilities. There are many kinds of learning disabilities (also called learning disorders). They can range from mild to severe and affect each person in different ways. Learning disabilities may affect a person’s ability to read, write, listen, talk, reason, do math, and pay attention.
What causes fragile X syndrome
Mutations in the fragile X mental retardation 1 (FMR1) gene cause fragile X syndrome. The FMR1 gene provides instructions for making a protein called fragile X mental retardation protein (FMRP). FMRP protein helps regulate the production of other proteins and plays a role in the development of synapses, which are specialized connections between nerve cells. Synapses are critical for relaying nerve impulses.
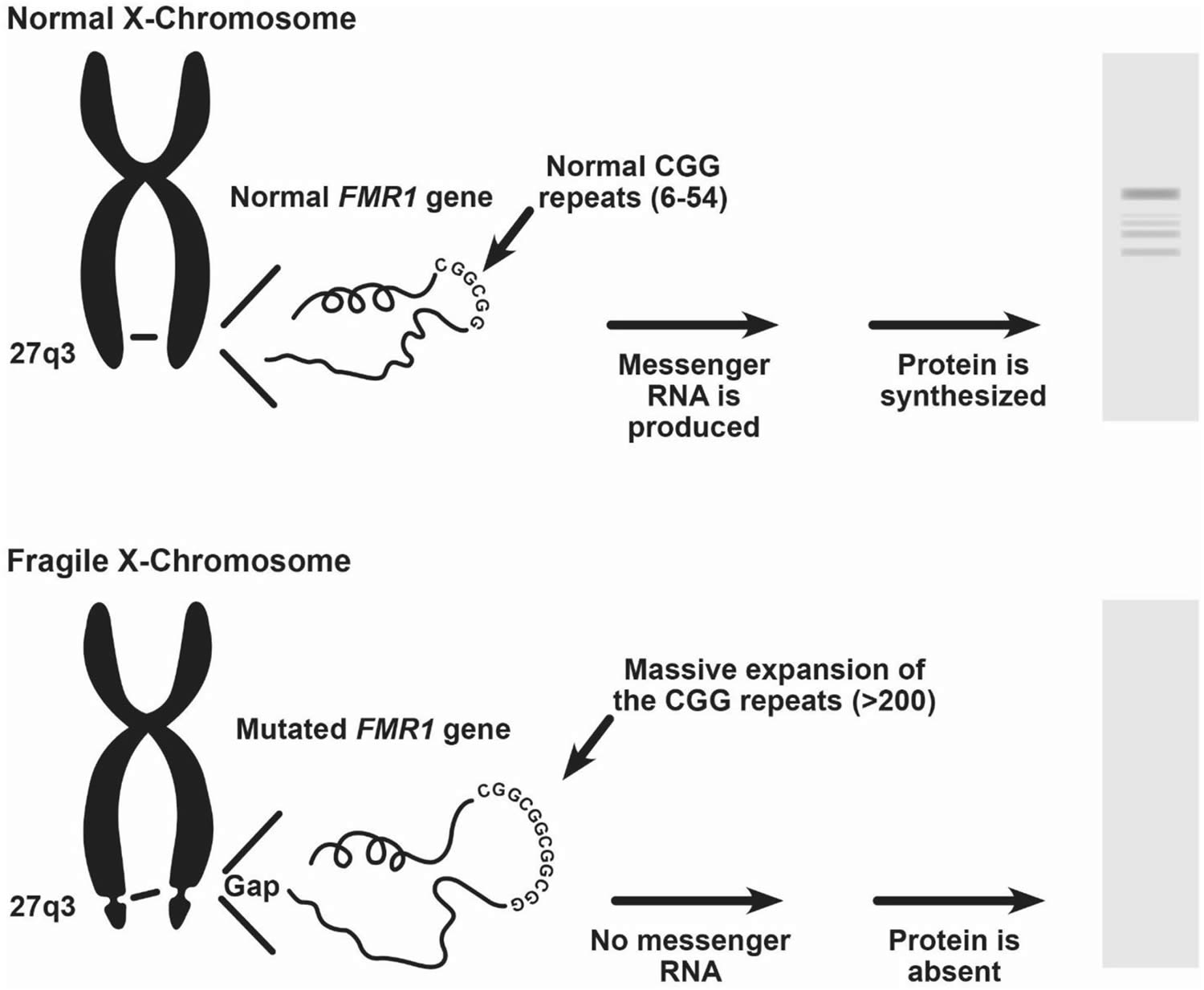
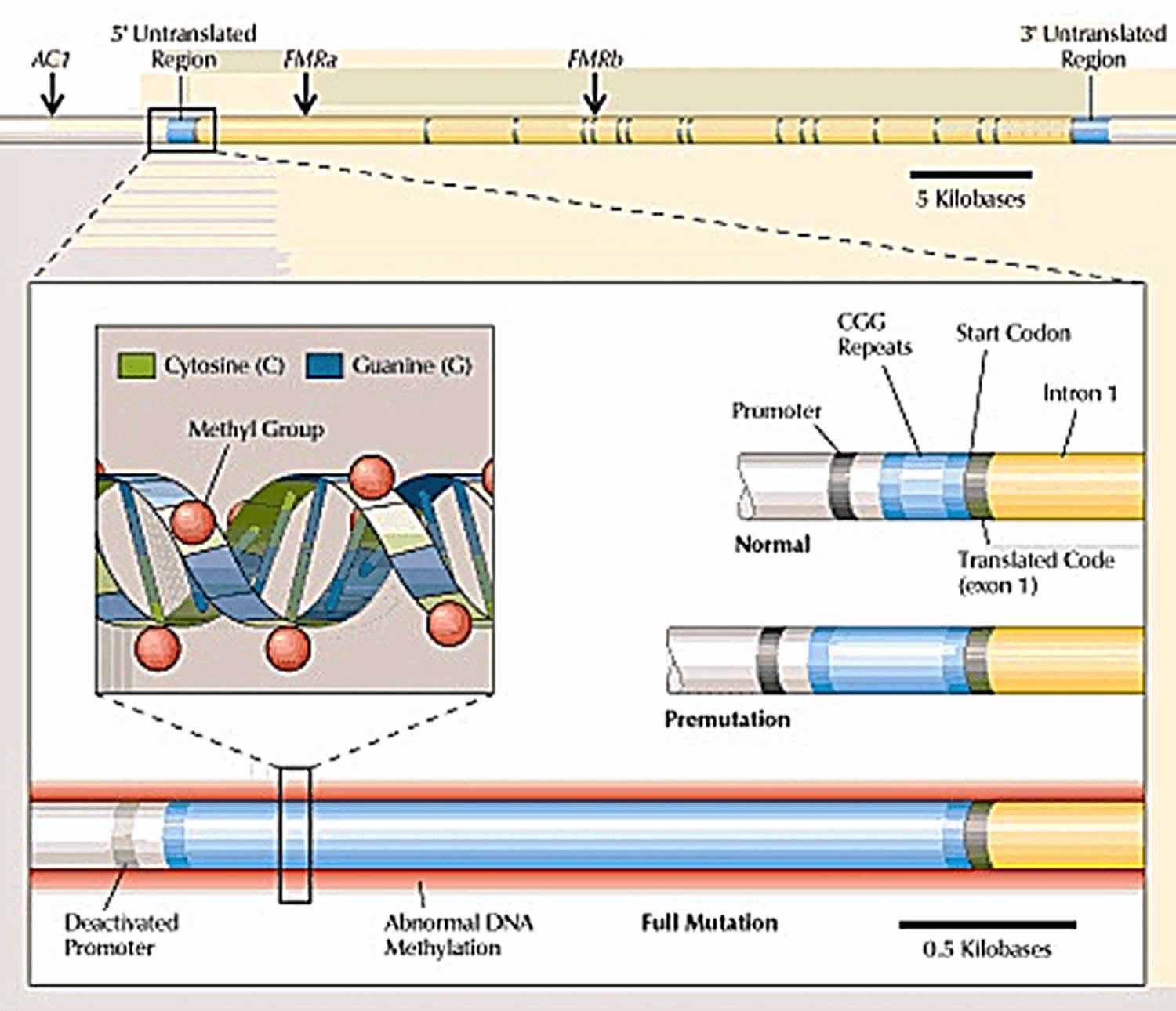
Nearly all cases of fragile X syndrome are caused by a mutation in which a DNA segment, known as the CGG triplet repeat, is expanded within the FMR1 gene. Normally, this DNA segment is repeated from 5 to about 40 times. The number of CGG triplet repeats, also called the “size of the mutation,” affects the type of symptoms and how serious the symptoms of Fragile X syndrome will be. In people with fragile X syndrome, the CGG segment is repeated more than 200 times. The abnormally expanded CGG segment turns off (silences) the FMR1 gene, which prevents the gene from producing FMRP. Loss or a shortage (deficiency) of this protein disrupts nervous system functions and leads to the signs and symptoms of fragile X syndrome.
Males and females with 55 to 200 repeats of the CGG segment are said to have an FMR1 gene premutation. Most people with a premutation are intellectually normal. In some cases, however, individuals with a premutation have lower than normal amounts of FMRP. As a result, they may have mild versions of the physical features seen in fragile X syndrome (such as prominent ears) and may experience emotional problems such as anxiety or depression. Some children with a premutation may have learning disabilities or autistic-like behavior. The premutation is also associated with an increased risk of disorders called fragile X-associated primary ovarian insufficiency (FXPOI) and fragile X-associated tremor/ataxia syndrome (FXTAS).
People with 200 or more repeats in the promoter part of the gene have a full mutation, meaning the gene might not work at all. People with a full mutation often have Fragile X syndrome.
Figure 1. Fragile X syndrome FMR1 gene mutation
Fragile X syndrome inheritance
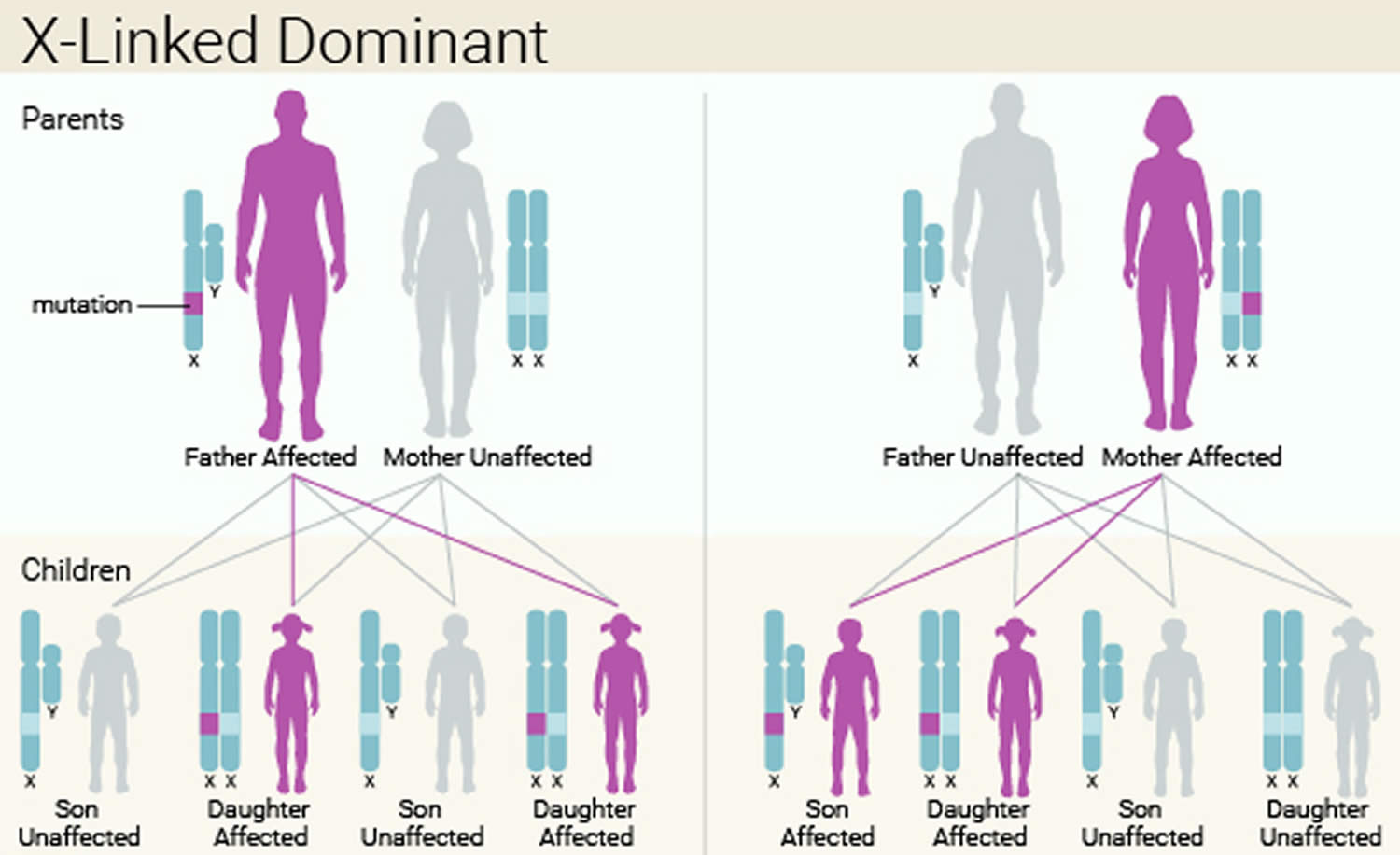
Fragile X syndrome is inherited in an X-linked dominant pattern. A condition is considered X-linked if the mutated gene that causes the disorder is located on the X chromosome, one of the two sex chromosomes. (The Y chromosome is the other sex chromosome in male.) Because both males (XY) and females (XX) have at least one X chromosome, both can pass on the mutated gene to their children. The inheritance is dominant if one copy of the altered gene in each cell is sufficient to cause the condition. X-linked dominant means that in females (who have two X chromosomes), a mutation in one of the two copies of a gene in each cell is sufficient to cause the disorder. In males (who have only one X chromosome), a mutation in the only copy of a gene in each cell causes the disorder. In most cases, males experience more severe symptoms of the disorder than females.
A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons (no male-to-male transmission).
In women, the FMR1 gene premutation on the X chromosome can expand to more than 200 CGG repeats in cells that develop into eggs. This means that women with the premutation have an increased risk of having a child with fragile X syndrome. By contrast, the premutation in men does not expand to more than 200 repeats as it is passed to the next generation. Men pass the premutation only to their daughters. Their sons receive a Y chromosome, which does not include the FMR1 gene.
- A father with the altered gene for Fragile X on his X chromosome will pass that gene on only to his daughters. To his sons he will pass on a Y chromosome, which doesn’t transmit Fragile X syndrome. Therefore, a father with the altered gene on his X chromosome and a mother with normal X chromosomes would have daughters with the altered gene for Fragile X, while none of their sons would have the mutated gene.
- A father can pass on the premutation form of the FMR1 gene to his daughters but not the full mutation. Even if the father himself has a full mutation of this gene, it appears that sperm can carry only the premutation. Scientists don’t understand how or why fathers can pass on only the milder form of Fragile X to their daughters. This remains an area of focused research.
- Mothers pass on only X chromosomes to their children, so if a mother has the altered gene for Fragile X, she can pass that gene to either her sons or her daughters. If a mother has the mutated gene on one X chromosome and has one normal X chromosome, and the father has no mutations, all the children have a 50-50 chance of inheriting the mutated gene.
- These 50-50 odds apply for each child the parents have. Having one child with the FMR1 mutation does not increase or decrease the chances of having another child with the mutated FMR1 gene. This is also true for the severity of the symptoms. Having one child with mild symptoms does not mean that the other children will have severe symptoms, and having a child with severe symptoms does not mean that the other children will have mild symptoms.
The frequency of Fragile X premutation is as follows:
1 in 151 females, or about 1 million women in the United States.
1 in 468 males, or about 320,000 men in the United States.
These statistics are important because both men and women are at risk for having symptoms linked to Fragile X-associated Disorders.
Women with a premutation reported their last menstrual cycle at an earlier age than women without a premutation (48 vs. 51 years).
Men and women with a premutation were more than four times as likely to report dizziness or fainting as people without a premutation (18% vs. 4%). Men and women with a premutation were more than twice as likely to report numbness as people without a premutation (29% vs. 13%).
This study of 6,747 older adults in Wisconsin found 30 people with a change in the FMR1 gene. Based on this relatively small number of people, the results should be interpreted with caution. These findings may not reflect all people in the United States with an FMR1 premutation For example a large Israeli study found approximately 1/130 women were FMR1 carriers.
Figure 2. Fragile X syndrome X-linked Dominant inheritance pattern
How does the FMR1 gene change as it is passed from parent to child?
The repeats in the promoter part of the FMR1 gene are unstable, and sometimes the number of repeats increases from one generation to the next.
A premutation gene is less stable than a full mutation gene. So as it passes from parent to child, a premutation gene might expand to become a full mutation gene. The chances of expansion depend on the number of repeats in the promoter of the premutation gene:
Normal
FMR1 genes that have 5 to 44 CGG repeats in the promoter are considered normal. When these genes are passed from parent to child, the number of repeats does not increase or decrease 6.
Intermediate
FMR1 genes with 45 to 54 CGG repeats in the promoter are considered intermediate, or borderline. An intermediate gene may expand from one generation to the next, depending on which parent has the gene.
- Mother to Child: Sometimes when a mother passes an intermediate gene to her child, the CGG repeats increase to a number seen with premutations. Research shows that an intermediate gene will not become a full mutation gene in one generation, and so a mother with an intermediate gene will not have a child with a full mutation.
- Father to Child: When intermediate genes are transmitted from father to child, they are generally stable and do not increase to premutations 7.
Premutations
Premutation (55 to 199 CGG repeats) FMR1 genes can expand to a full mutation from one generation to the next. The risk of expansion depends on which parent has the gene and the number of repeats in that gene.
- Mother to Child: An FMR1 gene from the mother with 100 CGG repeats is very likely to expand to a full mutation when passed to the child. About one-third of the time, an FMR1 gene from the mother with 70 to 79 CGG repeats expands to a full mutation in one generation 8.
- Father to Child: Premutations passed from father to child have almost no chance of expanding to full mutations 8
Fragile X syndrome symptoms
People with Fragile X do not all have the same signs and symptoms, but they do have some things in common. Symptoms are often milder in females than in males. Both men and women may have problems with tremors and poor coordination.
- Intelligence and learning. Many people with Fragile X have problems with intellectual functioning.
- These problems can range from the mild, such as learning disorders or problems with mathematics, to the severe, such as an intellectual or developmental disability.
- Fragile X syndrome may affect the ability to think, reason, and learn.
- Because many people with Fragile X also have attention disorders, hyperactivity, anxiety, and language-processing problems, a person with Fragile X may have more capabilities than his or her IQ (intelligence quotient) score suggests.
- Physical. Most infants and younger children with Fragile X don’t have any specific physical features of this syndrome. When these children start to go through puberty, however, many will begin to develop certain features that are typical of those with Fragile X.
- These features include a narrow face, large head, large ears, flexible joints, flat feet, and a prominent forehead.
- These physical signs become more obvious with age.
- Behavioral, social, and emotional. Most children with Fragile X have some behavioral challenges.
- They may be afraid or anxious in new situations.
- They may have trouble making eye contact with other people.
- Boys, especially, may have trouble paying attention or be aggressive.
- Girls may be shy around new people. They may also have attention disorders and problems with hyperactivity.
- Speech and language. Most boys with Fragile X have some problems with speech and language.
- They may have trouble speaking clearly, may stutter, or may leave out parts of words. They may also have problems understanding other people’s social cues, such as tone of voice or specific types of body language.
- Girls usually do not have severe problems with speech or language.
- Some children with Fragile X begin talking later than typically developing children. Most will talk eventually, but a few might stay nonverbal throughout their lives.
- Sensory. Many children with Fragile X are bothered by certain sensations, such as bright light, loud noises, or the way certain clothing feels on their bodies.
- These sensory issues might cause them to act out or display behavior problems.
Fragile X-Associated Tremor and Ataxia Syndrome
Fragile X-associated tremor and ataxia syndrome (FXTAS) is a late-onset condition (occurs in people older than age 50) that develops in some men and women with an altered form of the fragile X gene. Those with fragile X-associated tremor and ataxia syndrome (FXTAS) do not have the intellectual or developmental disabilities common in fragile X syndrome.
Current estimates suggest that about 30-40% of male FMR1 premutation carriers over 50 years of age, within families already known to have someone with Fragile X, will ultimately exhibit some features of fragile X-associated tremor and ataxia syndrome (FXTAS).
This figure may be as low as 10-20% in the general population, since the majority of carriers have a premutation in the lower range of CGG repeats, where the occurrence of fragile X-associated tremor and ataxia syndrome (FXTAS) appears to be reduced.
Though there are specific diagnostic criteria for fragile X-associated tremor and ataxia syndrome (FXTAS), some men may only exhibit some of the symptoms, and may not develop all of the cardinal features of the condition.
For men who are premutation carriers, the chance of developing core symptoms of FXTAS (tremor, problems with walking/balance) increases with age.
- From age 50-59 the chance is about 17%.
- From age 60-69 about 38%.
- From age 70-79 about 47%.
- Over 80 years old, about 75% will develop symptoms of FXTAS.
Studies of females have found that about 8-16% of premutation carriers, within families already known to have someone with a Fragile X condition, develop some FXTAS symptoms. The symptoms in females tend to be milder.
FXTAS may be one of the most common adult onset, single-gene neurological diseases; similar in prevalence to other neurodegenerative diseases such as ALS (Lou Gehrig’s disease); however more studies within the general population will be necessary before the true incidence is known.
Symptoms of fragile X-associated tremor and ataxia syndrome (FXTAS) vary among individuals. Typically, they include progressive signs of tremor, cerebellar ataxia, parkinsonism, and cognitive decline, with specific impairments in executive functioning. Additionally, psychiatric disturbances, autonomic dysfunction, and peripheral neuropathies may be present 9.
The first neurological sign at onset is variable. Tremor appears to be the sign most likely to trigger evaluation from a health provider. Action tremor is most common, although many affected individuals may not be aware of its impact on their daily living activities. Mild, intermittent tremor may be present for years before the diagnosis. Rest tremor is less common, but can also be present, especially in patients who have more of a parkinsonism presentation. Almost all affected persons develop cerebellar gait ataxia as the disease progresses. Tandem gait is abnormal and unexplained falls occur in ~35-50% of premutation carrier men who are older than 50 years of age 10. Other impairments, including parkinsonism, sensory neuropathy, and weakness, contribute to the poor balance observed in fragile X-associated tremor and ataxia syndrome (FXTAS). However, cerebellar dysarthric “scanning” speech, oculomotor findings and appendicular ataxia are all less common in fragile X-associated tremor and ataxia syndrome (FXTAS) than in other inherited cerebellar disorders. Although many affected patients have features of “classic” fragile X-associated tremor and ataxia syndrome (FXTAS), other neurological presentations, such as atypical parkinsonism, primary dementia, or neuromuscular abnormalities, can also occur as primary disease manifestations.
As the condition progresses, cognitive dysfunction such as executive impairment, memory deficits and eventually dementia may occur. These symptoms may influence intelligence, working memory, remote recall, information-processing speed, and temporal sequencing. Impaired executive function may lead to psychiatric and behavioral disorders as noted by increased anxiety, irritability, agitation, hostility, obsessive-compulsiveness, apathy, and depression.
Individuals with fragile X-associated tremor and ataxia syndrome (FXTAS) usually have abnormal MRI findings, such as white matter lesions, generalized brain atrophy, and/or increased T2 signal in the middle cerebellar peduncles (MCP sign), pons, periventricular region and/ or the splenium of the corpus callosum (CCS sign).
Currently, intervention is limited to symptomatic therapy as there have been no effective medications based on controlled clinical trials. Treatment recommendations are based on anecdotal reports and knowledge of other disorders that are similar to fragile X-associated tremor and ataxia syndrome (FXTAS) 9. For example, action tremor and parkinsonism in fragile X-associated tremor and ataxia syndrome (FXTAS) may respond to medications used for essential tremor and Parkinson disease, respectively. Action tremor may respond to B-blockers, primidone and topiramate. Deep brain stimulator surgery can be considered for tremor. Unilateral surgery with non-traditional targets may be less likely to worsen ataxia or cognition after surgery. Medications for cerebellar dysfunction can be considered, such as amantadine, buspirone, varenicline, riluzole, or ampyra, although none have proven efficacy in fragile X-associated tremor and ataxia syndrome (FXTAS) or other inherited ataxias. Treatment of psychiatric symptoms with selective serotonin inhibitors may be effective, although patients need to be monitored for worsening of balance.
It is important to note that treatments for fragile X-associated tremor and ataxia syndrome (FXTAS) should be individualized as symptoms vary in every individual. Treatments should also be approached globally utilizing medications, psychological counseling, rehabilitative interventions such as speech, occupational and physical therapy and gait training. Consideration should also be given to supportive services and counseling for the family. Specialty fields helpful in the care of individuals with fragile X-associated tremor and ataxia syndrome (FXTAS) include neurology, psychiatry, psychology, rehabilitation, urology, cardiology and movement disorders neurology.
Genetic counseling for individuals with fragile X-associated tremor and ataxia syndrome (FXTAS) and their family members is recommended, due to the inheritance of the X-linked FMR1 expansion mutation. All daughters of men diagnosed with fragile X-associated tremor and ataxia syndrome (FXTAS) (i.e., confirmed to have a premutation sized CGG repeat) are obligate FMR1 premutation carriers. For women with fragile X-associated tremor and ataxia syndrome (FXTAS) (again, with confirmed premutation sized CGG repeat expansions), each child will have a 50% chance of receiving the FMR1 mutation, with the potential of their premutation expanding to a full mutation (<200 repeats). The full mutation leads to fragile X syndrome, the most common inherited form of intellectual and developmental disabilities and the most common known single gene cause of Autism Spectrum Disorder (ASD). The expansion to the full mutation depends on the size and number of AGG interruptions in the premutation allele carried by the mother 11.
Features of Fragile X Syndrome in Males
A boy who has the full FMR1 mutation has fragile X syndrome and will have moderate intellectual disability. They have a particular facial appearance, characterized by a large head size, a long face, prominent forehead and chin and protruding ears. In addition males who have fragile X syndrome have loose joints (joint laxity), and large testes (after puberty).
Affected boys may have behavioral problems such as hyperactivity, hand flapping, hand biting, temper tantrums and autism. Other behaviors in boys after they have reached puberty include poor eye contact, perseverative speech, problems in impulse control and distractibility. Physical problems that have been seen include eye, orthopedic, heart and skin problems.
- Behavioral characteristics can include ADD, ADHD, autism and autistic behaviors, social anxiety, hand-biting and/or flapping, poor eye contact, sensory disorders and increased risk for aggression.
- The majority of males with fragile X syndrome demonstrate significant intellectual disability. Disabilities in fragile X syndrome include a range from moderate learning disabilities to more severe intellectual disabilities.
- Physical features may include large ears, long face, soft skin and large testicles (called “macroorchidism”) in post-pubertal males. Connective tissue problems may include ear infections, flat feet, high arched palate, double-jointed fingers and hyper-flexible joints.
- No one individual will have all the features of fragile X syndrome, and some features, such as a long face and macroorchidism, are more common after puberty.
- They are also very social and friendly, have excellent imitation skills, have a strong visual memory/long term memory, like to help others, are nice, thoughtful people and have a wonderful sense of humor.
Features of Fragile X Syndrome in Females
Girls who have the full FMR1 mutation have mild intellectual disability.
Family members who have fewer repeats in the FMR1 gene may not have intellectual disability, but may have other problems. Women with less severe changes may have premature menopause or difficulty becoming pregnant.
- The characteristics seen in males can also be seen in females, though females often have milder intellectual disability and a milder presentation of the syndrome’s behavioral and physical features.
- About one-third of females with fragile X syndrome have a significant intellectual disability.
- Others may have moderate or mild learning disabilities, emotional/mental health issues, general anxiety and/or social anxiety.
- A small percentage of females who have the full mutation of the FMR1 Gene that causes fragile X syndrome will have no apparent signs of the condition—intellectual, behavioral or physical. These females are often identified only after another family member has been diagnosed.
Fragile X-Associated Primary Ovarian Insufficiency
About 20% of women with the FMR1 premutation develop fragile X-associated primary ovarian insufficiency (FXPOI). Women with fragile X-associated primary ovarian insufficiency (FXPOI) is characterized by decreased ovarian function, which can lead to irregular menstrual periods, early infertility, and premature menopause in some female “carriers” of the FMR1 gene. Women with fragile X-associated primary ovarian insufficiency (FXPOI) are also at increased risk for heart disease and osteoporosis (thinning and weakening of the bones).
Women with fragile X-associated primary ovarian insufficiency (FXPOI) do not have an increased risk of fragile X-associated tremor and ataxia syndrome (FXTAS) compared with women who carry premutations and have normal ovarian function.
Fragile X syndrome and Autism
Fragile X syndrome is the most common known single gene cause of Autism spectrum disorder (ASD). Whereas autism spectrum disorder is a behavioral diagnosis, fragile X syndrome is a medical, or more accurately, a genetic diagnosis. When associated with fragile X syndrome, autism spectrum disorder is caused by the genetic change or mutation in the Fragile X gene. If a child is diagnosed with autism spectrum disorder and then diagnosed with fragile X syndrome, he or she still has autism spectrum disorder, it is just that the cause of their autism spectrum disorder is known. It is no different than someone with fragile X syndrome also having ADHD or any other behavioral symptom of fragile X syndrome.
Autism spectrum disorder is a complex complex neurological and developmental disorder that affects how a person behaves, interacts with others, communicates, and learns.
Autism spectrum disorder affects the structure and function of the brain and nervous system. Because it affects development, autism spectrum disorder is called a developmental disorder. Autism spectrum disorder can last throughout a person’s life.
People with this autism spectrum disorder have problems with 12:
- Communication and interaction with other people
- Restricted interests and repetitive behaviors
Different people with autism can have different symptoms. For this reason, autism is known as a spectrum disorder—which means that there is a range of similar features in different people with the disorder 12.
In giving a diagnosis of autism spectrum disorder, a health care provider will also specify whether the person also has:
- Intellectual problems, including problems with reasoning or memory
- Language problems, such as problems with speech
- Another medical or genetic condition that is related to or contributes to autism, such as seizures or Fragile X syndrome
Scientists don’t know exactly what causes autism spectrum disorder.
Autism was first described in the 1940s, but very little was known about it until the last few decades. Even today, there is a great deal that scientists don’t know about autism.
Because the disorder is so complex and no two people with autism are exactly alike, there are probably many causes for autism. It is also likely that there is not a single cause for autism, but rather that it results from a combination of causes.
About 10 percent of children with autism spectrum disorder are identified as having another genetic and chromosomal disorder, such as fragile X syndrome. Given the possibility of a link, it is recommended that all children with autism spectrum disorder, both male and female, be referred for genetic evaluation and testing for fragile X syndrome and any other genetic cause of autism spectrum disorder.
What are the symptoms of autism?
The symptoms of one person with autism can be very different from the symptoms of another person with autism. Health care providers think of autism as a spectrum disorder—which means that there is a range of similar features in different people with the disorder 12.
One person with autism may have mild symptoms, while another may have more serious symptoms, but they both have autism spectrum disorder.
Despite the range of possible symptoms, there are certain actions and behaviors that are common in autism spectrum disorder and could signal that a child is on the autism spectrum. Parents and caregivers who notice these “red flags” should speak to their child’s health care provider about autism and screening the child for autism spectrum disorder.
In general, the main signs and symptoms of autism spectrum disorder relate to:
- Communication and interactions with other people
- Routines or repetitive behaviors, sometimes called stereotyped behaviors
Health care providers organize some noticeable symptoms of autism into “red flags” to help parents and caregivers know what to look for as children grow and develop. These red flags are listed below.
Note about the red flags:
- Some of these red flags apply only at certain ages, so consider what is typical for other children your child’s age.
- Some red flags are more strongly associated with autism than others.
- If your child shows any red flags for autism, talk to his or her health care provider.
Communication
- Does not respond to his/her name by 12 months of age
- Cannot explain what he/she wants
- Doesn’t follow directions
- Seems to hear sometimes, but not other times
- Doesn’t point or wave “bye-bye”
- Used to say a few words or babble, but now does not
Social Behavior
- Doesn’t smile when smiled at
- Has poor eye contact
- Seems to prefer to play alone
- Gets things for him/herself only
- Is very independent for his/her age
- Seems to be in his/her “own world”
- Seems to tune people out
- Is not interested in other children
- Doesn’t point out interesting objects by 14 months of age
- Doesn’t like to play “peek-a-boo”
- Doesn’t try to attract his/her parent’s attention
Stereotyped Behavior
- Gets “stuck” doing the same things over and over and can’t move on to other things
- Shows unusual attachments to toys, objects, or routines (for example, always holding a string or having to put on socks before pants)
- Spends a lot of time lining things up or putting things in a certain order
- Repeats words or phrases (sometimes called echolalia)
How many children with fragile X syndrome have autism spectrum disorder?
Studies show that individuals with fragile X syndrome who have autism can have a more significant intellectual disability (lower IQ) than those with fragile X syndrome who do not have autism.
Many studies have evaluated the fragile X syndrome-autism spectrum disorder link over the past decade. Since many children with fragile X syndrome are interested in social interactions, they may not meet the diagnostic criteria for autism spectrum disorder, even though they exhibit some features of autism spectrum disorder such as poor eye contact, shyness, social anxiety, hand-flapping and sensory issues. Autism is much more common in boys with fragile X syndrome than in girls with fragile X syndrome. According to the Centers for Disease Control and Prevention (CDC), a national parent survey found that 46 percent of males and 16 percent of females with fragile X syndrome have been diagnosed or treated for autism spectrum disorder. The FORWARD Registry and Database tells us that 40 percent of individuals with fragile X syndrome are diagnosed with autism spectrum disorder by their doctor in the clinics of the Fragile X Clinical and Research Consortium.
What are the treatments for autism?
There is currently no one standard treatment for autism spectrum disorder.
But there are many ways to help minimize the symptoms and maximize abilities. People who have autism spectrum disorder have the best chance of using all of their abilities and skills if they receive appropriate therapies and interventions.
The most effective therapies and interventions are often different for each person. However, most people with autism spectrum disorder respond best to highly structured and specialized programs 13. In some cases, treatment can help people with autism to function at near-normal levels.
Research shows that early diagnosis and interventions, such as during preschool or before, are more likely to have major positive effects on symptoms and later skills.
Because there can be overlap in symptoms between autism spectrum disorder and other disorders, such as attention deficit hyperactivity disorder (ADHD), it’s important that treatment focus on a person’s specific needs, rather than the diagnostic label 14.
Treatments available for autism spectrum disorder include:
- Behavioral management therapy
- Cognitive behavior therapy
- Early intervention
- Educational and school-based therapies
- Joint attention therapy
- Medication treatment
- Nutritional therapy
- Occupational therapy
- Parent-mediated therapy
- Physical therapy
- Social skills training
- Speech-language therapy
If you have a question about treatment, talk to a health care provider who specializes in caring for people with autism spectrum disorder. These resources have more information about treatments for autism:
- The Centers for Disease Control and Prevention describes some treatment options (https://www.cdc.gov/ncbddd/autism/treatment.html)
- The Autism Speaks organization offers a Family Services Resources guide. You can search the guide to find autism-related care and services in your area (https://www.autismspeaks.org/)
Fragile X syndrome diagnosis
Health care providers often use a blood sample to diagnose Fragile X. The health care provider will take a sample of blood and will send it to a laboratory, which will determine what form of the FMR1 gene is present 15.
Fragile X DNA Test (FMR1 DNA Test)
Fragile X DNA testing detects more than 99 percent of individuals (both males and females) with fragile X syndrome, as well as Fragile X carriers.
Who should have Fragile X testing?
There are three general circumstances in which Fragile X testing should be considered:
- Clinical symptoms that suggest Fragile X Syndrome, Fragile X-Associated Tremor and Ataxia Syndrome (FXTAS) or infertility/Fragile X-Associated Primary Ovarian Insufficiency (FXPOI).
- A family history of Fragile X syndrome, Fragile X-Associated Tremor and Ataxia Syndrome (FXTAS), intellectual or learning disabilities or autism of unknown cause, or infertility.
- Family or personal history of a Fragile X Genetics and Inheritance (carrier).
Specific indications for testing include:
- Any male or female with intellectual disabilities, developmental delay, speech and language delay, autism or learning disabilities of unknown cause.
- Any female with infertility, elevated follicle-stimulating hormone (FSH) levels, premature ovarian failure, primary ovarian insufficiency or irregular menses.
- Any adult over 50 with features of Fragile X-Associated Tremor and Ataxia Syndrome (FXTAS), including intention tremors, ataxia, memory loss, cognitive decline, personality change, especially in combination with a positive family history of Fragile X.
- Any preconception or pregnant woman who expresses interest in or requests Fragile X carrier testing.
Lab Tests for Fragile X
The FMR1 DNA Test can be administered with two different lab procedures.
- The Southern blot analysis test determines if the gene has a full mutation, its approximate size, whether the gene has been “methylated” and if there is mosaicism of the gene (a mixture of different cell types).
- The polymerase chain reaction (PCR) analysis can determine the actual number of “CGG repeats” (a pattern of DNA) that are present in the Fragile X gene. For various technical reasons, PCR has been not the test of choice to diagnose a full mutation, but is quite accurate in determining premutation and normal gene repeat numbers. However, PCR is less expensive and quicker than Southern blot, and recent advances in technology have increased its ability to identify Fragile X full mutations. PCR may thus be the only test used in the near future.
Testing cost and reporting time
The blood test usually ranges from $300-$600, and results are usually available in 2-4 weeks.
How are testing arrangements made?
The test must be ordered by a genetic counselor or physician. A genetic counselor often will facilitate the testing, and make certain that the correct drawing, shipping and processing of the sample occurs. The genetic counselor is trained and experienced in the interpretation and explaining of the test results. She/he can coordinate any follow-up appointments and work with your physician to make referrals to resources in your area. You can locate a genetic counselor in your area by logging on to the “Find a counselor” feature on the National Society of Genetic Counselors website (https://www.nsgc.org/).
In most cases you will be directed to go to a blood drawing station for a blood drawing procedure. Although this facility is often referred to as a “lab,” it is not the actual lab doing the DNA test. After the blood is drawn it is sent to a specific genetics or “reference” lab for the genetic test.
If your insurance company (or state/public insurance such as Medicaid) is paying for the testing, it is likely that the sample will go to the laboratory with which they are contracted. If you are paying for the test yourself, your physician or genetic counselor can locate a genetics lab in your area or one with which they have a relationship.
Prenatal Testing (During Pregnancy)
Pregnant women who have an FMR1 premutation or full mutation may pass that mutated gene on to their children. A prenatal test allows health care providers to detect the mutated gene in the developing fetus. This important information helps families and providers to prepare for Fragile X syndrome and to intervene as early as possible.
Possible types of prenatal tests include:
- Amniocentesis. A health care provider takes a sample of amniotic fluid, which is then tested for the FMR1 mutation.
- Chorionic villus sampling (CVS). A health care provider takes a sample of cells from the placenta, which is then tested for the FMR1 mutation.
Because prenatal testing involves some risk to the mother and fetus, if you or a family member is considering prenatal testing for Fragile X, discuss all the risks and benefits with your health care provider.
Prenatal testing is not very common, and many parents do not know they carry the mutation. Therefore, parents usually start to notice symptoms in their children when they are infants or toddlers. The average age at diagnosis is 36 months for boys and 42 months for girls 16.
Diagnosis of Children
Many parents first notice symptoms of delayed development in their infants or toddlers. These symptoms may include delays in speech and language skills, social and emotional difficulties, and being sensitive to certain sensations. Children may also be delayed in or have problems with motor skills such as learning to walk.
A health care provider can perform developmental screening to determine the nature of delays in a child. If a health care provider suspects the child has Fragile X syndrome, he/she can refer parents to a clinical geneticist, who can perform a genetic test for Fragile X syndrome 16.
Other tests for children with developmental delay
Physicians and other providers ordering Fragile X testing often arrange for other genetic testing to provide more information on a child’s condition. Depending on the child’s presenting features or symptoms, this might include chromosome analysis, chromosome microarray (CGH), FISH testing (for other single gene conditions such as Velo-cardio-facial syndrome) and metabolic/ biochemical tests. Other types of medical evaluations might be recommended as well, including magnetic resonance imaging (MRI), electroencephalography (EEG), computer tomography (CT scan) or X-rays.
Chromosomal Microarray Analysis and the DNA Test for Fragile X
Chromosomal microarray analysis is a powerful test for detecting certain genetic causes of developmental disabilities; however, it is not able to detect Fragile X mutations of any kind.
For this reason, the diagnostic work-up of children with autism, global developmental delay, or intellectual disabilities should include both a microarray analysis and a separate Fragile X DNA analysis. If your child just had the microarray analysis but not the specific DNA test for Fragile X, then he has not been checked for Fragile X.
Fragile X syndrome treatment
There is no single treatment for Fragile X syndrome, but there are treatments that help minimize the symptoms of the condition. Individuals with Fragile X who receive appropriate education, therapy services, and medications have the best chance of using all of their individual capabilities and skills. Even those with an intellectual or developmental disability can learn to master many self-help skills.
Early intervention is important. Because a young child’s brain is still forming, early intervention gives children the best start possible and the greatest chance of developing a full range of skills. The sooner a child with Fragile X syndrome gets treatment, the more opportunity there is for learning.
Educational Treatments
Most children with Fragile X can benefit from special education services that are tailored to their particular strengths and weaknesses. Educational treatments should take the child’s specific symptoms of Fragile X into account to promote the best learning environment.
Teachers can use the National Fragile X Foundation’s Lesson Planning Guide for Fragile X to learn more about the best strategies for teaching children with Fragile X here: https://fragilex.org/learn/treatment-and-intervention/
Eligibility for Special Education
Most children with Fragile X are eligible for free, appropriate public education under federal law. Although a medical diagnosis does not guarantee access to special education services, most children with Fragile X will have certain cognitive or learning deficits that makes them eligible for services. Parents can contact a local school principal or special education coordinator to learn how to have a child examined to see if he or she qualifies for services under the Individuals with Disabilities Education Act.
Suggestions for Working with Individuals with Fragile X
Everyone with Fragile X is unique. However, those with this disorder often share some particular behaviors and intellectual characteristics. For example, children with Fragile X can easily become overwhelmed by crowds, noise, and touch. Other common characteristics include weak abstract thinking skills and poor quantitative (measuring and counting) skills. However, these children often have unique strengths as well, including visual memory. By taking these unique strengths and weaknesses into account, teachers can promote the best learning for these children.
Suggestions 17:
- Know the learning style of the individual.
- Develop a consistent daily schedule or routine.
- Use visual signs (pictures, sign language, logos, words) and concrete examples or materials to present ideas, concepts, steps, etc.
- Prepare the individual for any changes in routine by explaining these changes ahead of time, possibly by using visual signs.
- Include functional goals with academic goals; for instance, teach the individual the names of different pieces of clothing as well as how to dress himself/herself.
- Provide opportunities for the child to be active and move around.
- Use computers and interactive educational software.
- Provide a quiet place where the child can first retreat and then regroup.
What Type of Classroom
In general, there are three options for the classroom placement of a child with Fragile X, based on that child’s specific abilities and needs:
- Full inclusion in a regular classroom
- Inclusion with “pull-out” services
- Full-time special education classroom
Placement decisions should be based on each child’s needs and abilities.
The Individualized Educational Plan (IEP)
If a child with Fragile X syndrome qualifies for special services, a team of people will work together to design an IEP for the child. The team may include parents or caregivers, teachers, a school psychologist, and other specialists in child development or education. The IEP includes specific learning goals for that child, based on his or her needs and capabilities. The team also decides how best to carry out the IEP. It reaches a consensus on classroom placement for the child, determines any devices or special assistance the child needs, and identifies the specialists who will work with the child.
The special services team should evaluate the child on a regular basis. The team can chart progress and decide whether changes in treatment are needed (for instance, changes to the IEP, in classroom placement, or in the services provided).
Therapy Treatments
A variety of professionals can help individuals with Fragile X syndrome and their families manage the symptoms of the disorder. Those with Fragile X might benefit from services provided by several different specialists:
- Speech-language therapists can help people with Fragile X syndrome improve their pronunciation of words and sentences, slow down their speech, and use language more effectively.
- Occupational therapists help find ways to adjust tasks and conditions to match a person’s needs and abilities.
- Physical therapists design activities and exercises that help build motor control and improve posture and balance.
- Behavioral therapists try to understand why someone with Fragile X acts out, and they create ways and strategies for avoiding or preventing these situations from occurring while also teaching better or more positive ways to respond to situations.
Medication Treatments
To this point, the Food and Drug Administration (FDA) has not approved any drugs specifically for the treatment of Fragile X or its symptoms. But in many cases, medications are used to treat certain symptoms of Fragile X syndrome, as shown in the chart below. The NICHD does not endorse or support the use of any of these medications in treating the symptoms of Fragile X syndrome, or for other conditions for which the medications are not FDA approved.
Medication is most effective when paired with therapy designed to teach new coping or behavioral skills. Not every medication helps every child.
Please note that some of these medications carry serious risks. Others may make symptoms worse at first, or they may take several weeks to become effective. Doctors may have to try different dosages or combinations of medications to find the most effective plan. Families, caregivers, and doctors need to work together to ensure that a medication is working and that the medication plan is safe.
This chart is meant for reference ONLY and should not take the place of a health care provider’s advice. Discuss any questions about medication with a health care provider.
| Symptom | Generic Medication (Brand Name in Parentheses) |
|---|---|
| Seizures Mood instability |
|
| Attention deficit (with or without hyperactivity) |
|
| Hyperarousal Sensory overstimulation (often occurs with ADD/ADHD) |
|
| Aggression Intermittent explosive disorder Obsessive-compulsive disorder (often occurs with anxiety and/or depression) |
|
| Sleep disturbances |
|
Abbreviations: ADD = attention deficit disorder; ADHD = attention deficit hyperactivity disorder; TTS = transdermal therapeutic system.
- Fragile X Syndrome. https://medlineplus.gov/fragilexsyndrome.html[↩]
- Fragile X syndrome. https://ghr.nlm.nih.gov/condition/fragile-x-syndrome[↩][↩]
- Hunter J, Rivero-Arias O, Angelov A, Kim E, Fotheringham I, Leal J. Epidemiology of fragile X syndrome: a systematic review and meta-analysis. Am J Med Genet A. 2014 Jul 164A(7): 1648-58.[↩]
- Eunice Kennedy Shriver National Institute of Child Health and Human Development. (2009). NIH Research Plan on Fragile X Syndrome and Associated Disorders (NA). https://www.nichd.nih.gov/sites/default/files/publications/pubs/Documents/nih_fragilex_research_plan_2009.pdf[↩]
- Berry-Kravis, E., Raspa, M., Loggin-Hester, L., Bishop, E., Holiday, D., & Bailey, D. B. (2010). Seizures in fragile X syndrome: Characteristics and comorbid diagnoses. American Journal of Intellectual and Developmental Disabilities, 115, 461-472.[↩]
- Schultz-Pedersen, S., Hasle, H., Olsen, J. H., & Friedrich, U. (2001). Evidence of decreased risk of cancer in individuals with fragile X. American Journal of Medical Genetics, 103, 226-230.[↩]
- Sherman, S., Pletcher, B. A., & Driscoll, D. A. (2005). Fragile X syndrome: Diagnostic and carrier testing. Genetics in Medicine, 7, 584–587.[↩]
- Nolin, S. L., Brown, W. T., Glicksman, A., Houck, G. E., Jr., Gargano, A. D., Sullivan, A., et al. (2003). Expansion of the Fragile X CGG repeat in females with premutation or intermediate alleles. American Journal of Human Genetics, 72, 454-464.[↩][↩]
- Hagerman, R. J. & Hagerman, P. Fragile X-associated tremor/ataxia syndrome – features, mechanisms and management. Nature reviews. Neurology 12, 403-412, doi:10.1038/nrneurol.2016.82 (2016).[↩][↩]
- Leehey, M. A. Fragile X-associated tremor/ataxia syndrome: clinical phenotype, diagnosis, and treatment. Journal of investigative medicine : the official publication of the American Federation for Clinical Research 57, 830-836, doi:10.2310/JIM.0b013e3181af59c4 (2009).[↩]
- Nolin, S. L. et al. Fragile X full mutation expansions are inhibited by one or more AGG interruptions in premutation carriers. Genetics in medicine : official journal of the American College of Medical Genetics 17, 358-364, doi:10.1038/gim.2014.106 (2015).[↩]
- Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. (2013). American Psychiatric Association: Washington, DC.[↩][↩][↩]
- National Institute of Mental Health. (2011). A parent’s guide to autism spectrum disorder. https://www.nimh.nih.gov/health/publications/autism-spectrum-disorder/index.shtml[↩]
- Kotte, A., Joshi, G., Fried, R., Uchida, M., Spencer, A., Woodworth, K. Y., et al. (2013). Autistic traits in children with and without ADHD. Pediatrics, 132(3), e612–e622.[↩]
- Testing for Fragile X. https://fragilex.org/learn/testing/[↩]
- Bailey, D. B., Raspa, M., Bishop, E., & Holiday, D. (2009). No change in the age of diagnosis for fragile x syndrome: findings from a national parent survey. Pediatrics, 124, 527–533.[↩][↩]
- Treatment and Intervention. https://fragilex.org/learn/treatment-and-intervention/[↩]





{kind=link}