
Contents
What is gluteus maximus
Gluteus maximus is the largest of the three gluteal muscles and most superficial of gluteal muscles 1. Gluteus maximus makes up most of the shape and form of your buttock and hip area. The gluteus maximus is a thick fleshy muscle with a quadrangular shape. Gluteus maximus is a large muscle and plays a prominent role in the maintenance of keeping the upper body erect. Gluteus maximus is also a site of intramuscular injection. Gluteus maximus overlies large sciatic nerve; covers ischial tuberosity only when standing; when sitting, moves superiorly, leaving ischial tuberosity exposed in the subcutaneous position.
Gluteus maximus principal function is the major extensor of the hip and it also externally rotates and abducts your thigh. Hip extension is an important action in daily activities (standing, stepping and walking) and sporting actions (running, sprint-running and jumping).
Gluteus maximus is innervated by the inferior gluteal nerve (L5–S2). Gluteus maximus dysfunction is most likely due to inferior gluteal nerve dysfunction; this would cause difficulty in rising from a seated position, climbing up stairs and loss of hip extension. The most common cause of inferior gluteal nerve dysfunction is a posterior hip dislocation. Another etiology is incorrect intramuscular (IM) injection placement. Intramuscular (IM) injection placement should be in the upper outer quadrant of the buttock. Otherwise, both the inferior and superior gluteal nerves are at risk of injury 2. Paralysis of the gluteus maximus does not affect walking on a plane surface 1. The gluteus maximus only contracts during a part of the stance phase. This phase occurs when the heal strikes the ground to when the foot is flat. The gluteus maximus works by resisting further flexion of the hip and initiate extension. The gluteus maximus actively functions when climbing upstairs or lifting from a seated position 3.
The gluteal muscles are a grouping of muscles that make up the buttock area. These muscles include:
- Gluteus maximus
- Gluteus medius
- Gluteus minimus
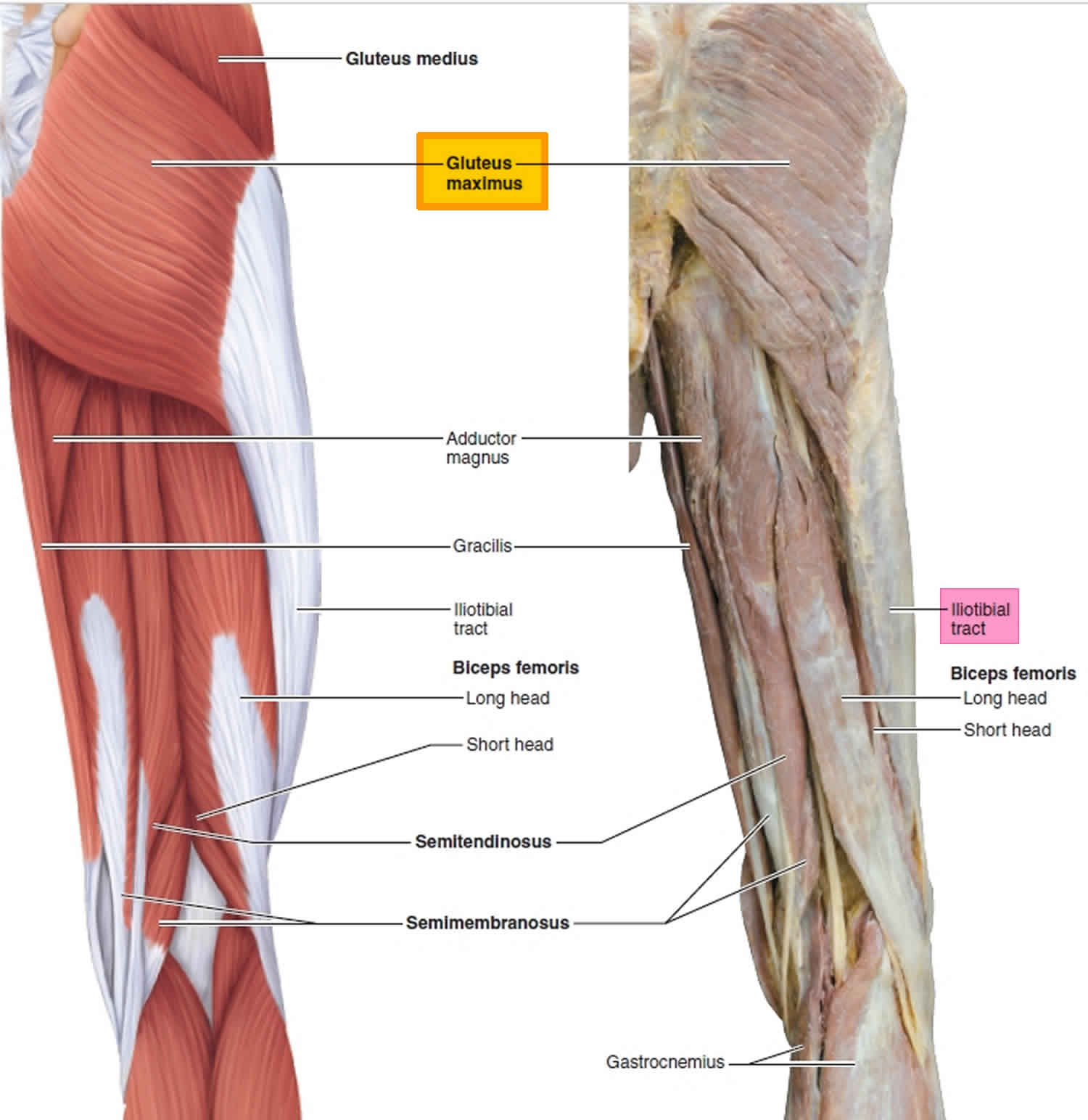
Figure 1. Gluteus maximus anatomy
Gluteus maximus origin and insertion
Gluteus maximus originates from the dorsal ilium, sacrum, and coccyx.
The gluteus maximus has two insertion points: superficial fibers to the greater trochanter and a band of the fascia lata (iliotibial tract) and the deep fibers that insert into the gluteal tuberosity of femur between the adductor magus and vastus lateralis. It originates in the gluteal surface of the ilium 4.
The gluteus maximus also has associations with three bursae 5. These include:
- The trochanteric bursa – separates the gluteus maximus from the greater trochanter
- Ischial bursa – separates the gluteus maximus from the ischial tuberosity
- The gluteofemoral bursa – separates the iliotibial tract from the vastus lateralis
Gluteus maximus blood supply and lymphatics
The gluteus maximus receives vascular supply by both the inferior and superior gluteal artery. These vessels enter the gluteus maximus at the center of the muscle. The inferior gluteal artery proceeds to descend along the greater trochanter of the femur. It accompanies the descent of the sciatic nerve, which proves to be critical as rupture of the inferior gluteal artery can cause gluteal compartment syndrome and sciatic nerve palsy 6. The artery supplies the superficial skin and anastomoses with the perforating arteries of the lower limb. The inferior gluteal artery is also susceptible to pseudoaneurysm formation following intramuscular injection 7.
Gluteus maximus innervation
The innervation of the gluteus maximus muscle is from the inferior gluteal nerve. The inferior gluteal nerve originates from the ventral rami of L5, S1, and S2. Classically, the inferior gluteal nerve was thought not to provide cutaneous innervation. However, the recent literature describes findings of cutaneous branches of the nerve which might contribute toward gluteal pain during lumbar disk herniation. Surgeons must also be aware of this nerve as injury might result in compression ulcers and various pain syndromes 8.
Gluteus maximus function
Gluteus maximus principal function is the major extensor of the thigh and it also externally rotates and abducts your thigh. Although a powerful extensor, gluteus maximus only acts when force is necessary. Gluteus maximus is most effective when thigh is flexed and force is necessary, as in rising from sitting, climbing stairs, straightening from a bending position, walking up stairs or on a hill and running. Gluteus maximus also acts on the pelvis, supports it and the trunk which is vital when a person is standing on one leg. By attaching to the tensor fascia lata, the gluteus maximus also steadies the femur 9. Gluteus maximus is generally inactive during standing and walking.
The gluteus maximus works with the semitendinosus and semimembranosus muscles to extend the hip. The muscle also works in conjunction with the iliopsoas, piriformis, and the obturator muscles to externally rotate the hip.
Gluteus maximus action
In athletes, the gluteus maximus muscle is among the most important to train due to its action of extension of the hip joint which translates to explosive movements 1. A 2018 study looked at the correlation between gluteus maximus muscle to quadriceps femoris ratio in faster athletes compared to slower athletes. Results yielded that the larger the ratio, the faster the athlete 10.
Another 2018 study suggests that associated hip muscles may become more atrophied after hip arthroplasty, but larger cohorts would be needed to clarify the results 11. Variability in the neuromuscular activity of the gluteus maximus in patellofemoral pain syndrome compared to healthy individuals was also documented 12.
Gluteus maximus exercises
Though several different gluteus maximus exercises exist, a comprehensive understanding of which exercises best target the gluteus maximus and the magnitude of muscular excitation associated with each exercise is yet to be established 13. The findings from this review 13 provide an indication of gluteus maximus excitation generated by a variety of hip extension body weight exercises, which may assist practitioners in making exercise selection decisions for programming.
Figure 2. Gluteus maximus workout
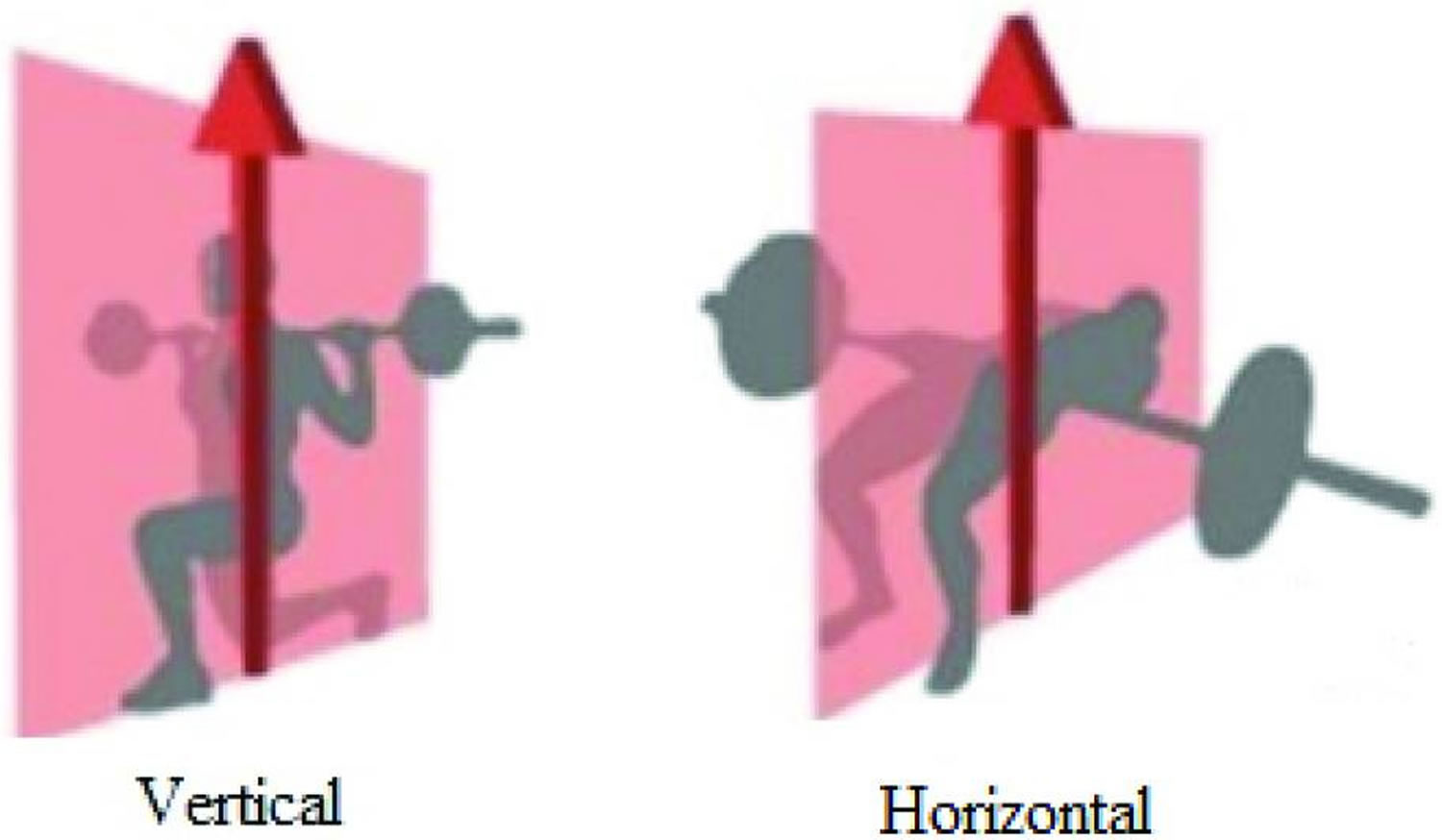
Table 1. Summary of all different gluteus maximus exercise studies reviewed
| Author and date | Subjects (Sex, age, height, mass) | Methodology (MVIC position and electrode site placement) | Hip extension exercises | Mean ± SD EMG excitation (%MVIC) |
| Worrell, Crisp, LaRosa 14 | Group 1: 6 males, 7 females (22 ± 8.6 years; 171 ± 15 cm; 69.1 ± 14.1 kg) Group 2: 13 males, 6 females (27.5 ± 5 years; 175 ± 9 cm; 73.3 ± 15.3 kg) | Prone hip extension against manual resistance at 0 ° of hip flexion. Placement half-way between the second sacral prominence and the greater trochanter of the femur. | Lateral step up (20 cm height) | 20 ± 11 group 1 16 ± 7 group 2 |
| Zeller, et al. 15 | 9 males (20.3 ± 1 years; 182 ± 5 cm; 78.8 ± 4.0 kg) 9 females (22 ± 8.6 years; 170 ± 6 cm; 64.3 ± 5.5 kg) | Prone hip extension against manual resistance with knee flexed at 90 ° Placement not specified. | Single leg squat | 62.7 ± 43 male 81.2 ± 28 female |
| Ayotte, et al. 16 | 16 males, 7 females (31.2 ± 5.8 years; 173.1 ± 10.1 cm; 77.0 ± 13.9 kg) | Supine hip extension against fixed resistance pad placed proximal to the popliteal fossa from 30 ° hip flexion. Placement 1/3rd of the distance from the second sacral vertebra to the greater trochanter. | Forward step up (15.2 cm height) Lateral step up (15.2 cm height) Retro step up (15.2 cm height) Single leg mini squat (15.2 cm depth) Single leg wall squat, other leg knee extended | 74 ± 43 56 ± 29 59 ± 35 57 ± 43 86 ± 43 |
| Ekstrom, Donatelli, Carp 17 | 19 males, 11 females (27 ± 8 years; 176 ± 8 cm; 74 ± 11 kg) | Prone hip extension against manual resistance applied above the knee with knee flexed to 90 ° Placement between the lateral edge of the sacrum and the posterosuperior edge of the greater trochanter. | Bridge Lateral step up (20.3 cm height) Lunge Quadruped hip extension with arm raise Single leg bridge | 25 ± 14 29 ± 13 36 ± 17 56.2 ± 22 40 ± 20 |
| Ekstrom, Osborn, Hauer 18 | 27 males, 32 females (age range 21-35 years) | Prone hip extension against manual resistance applied just above the knee with knee flexed at 90 ° Placement between the lateral edge of the sacrum and the posterosuperior edge of the greater trochanter. | Bridge Bridge with knees extended and feet on a swiss ball | 27 ± 13 20 ± 14 |
| Farrokhi, Pollard, Souza, et al. 19 | 5 males, 5 females (26.7 ± 3.2 years) | Prone hip extension against strap resistance positioned superior to the knee joint with the knee flexed to 90 ° Placement midway between the second sacral vertebra and the greater trochanter. | Lunge Lunge with trunk extension Lunge with trunk flexion | 18.5 ± 11.0 19.3 ± 11.8 22.3 ± 12.0 |
| Boudreau, Dwyer, Mattacola, et al. 20 | 22 males, 22 females (23.3 ± 5.1 years; 174.5 ± 9.1 cm; 74.6 ± 16.5 kg) | Standing hip extension against strap resistance placed around the distal third of the thigh with knee flexed to 90 ° Placement half the distance between the greater trochanter of the femur and the spinous process of the second sacral vertebra along an oblique angle at the level of the greater trochanter. | Forward step-up and over (20.3 cm height) Lunge Single leg squat | 16.5 ± 11.7 21.7 ± 14.7 35.2 ± 24.0 |
| Distefano, Blackburn, Marshall, et al. 21 | 9 males, 12 females (22 ± 3 years; 171 ± 11 cm; 70.4 ± 15.3 kg) | Prone hip extension against manual resistance with knee flexed at 90 ° Placement 1/3rd of the distance between the second sacral vertebra and the greater trochanter. | Lunge Lateral lunge Transverse lunge Single leg deadlift Single leg squat | 44 ± 23 41 ± 20 49 ± 20 59 ± 28 59 ± 27 |
| Lewis, Sahrmann 22 | 11 females (27.7 ± 6.2 years; 165.2 ± 3.6 cm; 62.3 ± 6.9 kg) | Prone hip extension against manual resistance with knee flexed at 90 ° Placement on the muscle belly. | Prone hip extension from hip flexion of 30 ° Prone hip extension from hip flexion of 30 ° with verbal cues to activate the glutes Prone hip extension from hip flexion of 30 ° with verbal cues to activate the hamstrings | 9.7 ± 2.9 21.6 ± 9.8 11.2 ± 5.2 |
| Sakamoto, et al. 23 | 16 males, 15 females (24.5 3.5 years; 170.0 ± 9.0 cm; 66.9 ± 11.9 kg | Prone hip extension against manual resistance with knee extension Placement 1/3rd of the distance between the second sacral vertebra and the greater trochanter. | Prone hip extension with knee extension Prone hip extension with 90 ° knee flexion Prone hip extension with lateral hip rotation and knee extension Prone hip extension with lateral hip rotation and knee flexion | 12.7 ± 8.6 23.1 ± 21.2 22.5 ± 10.4 21.2 ± 12.0 |
| Lubahn, Kernozek, Tyson, et al. 24 | 18 females (22.3 ± 2.3 years; 166.82 ± 9.2 cm; 61.1 ± 7.1 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement on the muscle belly. | Forward step up (Height unknown) Single leg squat Squat | 36.4 ± 18.6 47.4 ± 21.2 21.7 ± 15.8 |
| Boren, et al. 25 | 24 (Anthropometrical details not provided) | Prone hip extension against a strap with the knee flexed at 90 ° Placement not specified. | Forward step up (20 cm height) Lateral step up (15 cm height) Plank with bent leg hip extension Skater squat Single leg bridge Single leg deadlift Single leg squat Quadruped bent leg hip extension DOM Quadruped bent leg hip extension non-DOM | 54.7 63.8 106.2 66.2 54.2 58.8 70.7 59.7 21.0 |
| Bouillon, Wilhelm, Eisel, et al. 26 | 20 males, 20 females (22 ± 1 years; 170 ± 10 cm; 65 ± 13 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement inferior and medial to a line drawn between the PSIS and the posterior greater trochanter. | Lateral lunge Lunge | 12 ± 3 11 ± 2.5 |
| Nakagawa, et al. 27 | 20 males (23.5 ± 3.8 years; 176 ± 6.1 cm; 74.6 ± 9.1 kg) 20 females (21.8 ± 2.6 years; 163 ± 7.3 cm; 59.4 ± 7.3 kg) | Prone hip extension against strap with the knee flexed at 90 ° Placement parallel to the mid–muscle belly. | Single leg squat | 24.6 ± 2.7 females 18.9 ± 8.9 males |
| Tateuchi, Taniguchi, Mori, et al. 28 | 10 males, 6 females (24.3 ± 5.2 years; 165.7 ± 7.9 cm; 59.0 ± 8.0 kg) | Prone hip extension against manual resistance. Placement halfway on the line extending between the sacrum and greater trochanter. | Prone hip extension from 30 ° hip flexion to 10 ° hip extension | 10.9 ± 3.3 |
| De Ridder et al. 29 | 8 males, 6 females (24.7 ± 3.2 years; 172.9 ± 6.4 cm; 64.5 ± 12.5 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement midway between the posterosuperior iliac spine and the ischial tuberosity. | Prone back/torso extension Reverse hyperextension | 44.9 concentric 33.1 eccentric 30.3 concentric 20.3 eccentric |
| Kang, et al. 30 | 18 males, 12 females (22.8 ± 2.9 years; 170.3 ± 4.1 cm; 66.9 ± 10.8 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement halfway between the greater trochanter and second sacral vertebra in the middle of the muscle and at an oblique angle. | Prone hip extension with knee flexion with hip abducted 0 ° Prone hip extension with knee flexion with hip abducted 15 ° Prone hip extension with knee flexion with hip abducted 30 ° | 20.2 ± 8.6 23.4 ± 9.9 29.6 ± 11.5 |
| Lee, Ko, Lim 31 | 20 males (22.9 ± 2.1 years; 174.4 ± 3.9 cm; 70.0 ± 6.2 kg) | Side-lying hip abduction against strap resistance with the hip in 90 ° abduction. Placement 1/3rd of the distance between the second sacral vertebra and the greater trochanter. | Lunge Lunge with compression pelvic belt Single leg deadlift Single leg deadlift with compression pelvic belt Single leg squat Single leg squat with compression pelvic belt | 11.5 ± 6.9 13.9 ± 7.7 27.9 ± 18.4 36.3 ± 21.9 30.5 ± 19.4 35.5 ± 21.7 |
| Webster, Gribble 32 | 1 male, 8 females (22.9 ± 4.5 years; 164 ± 6.5 cm; 65.4 ± 10 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement half-way between the second sacral prominence and the greater trochanter of the femur. | Single leg squat with rotation Transverse lunge | 78 ± 45 58 ± 3 |
| Bolgla, et al. 33 | 18 males (24.3 ± 3.4 years; 180 ± 10 cm; 81.2 ± 9.7 kg) 16 females (24.0 ± 1.5 years; 165 ± 10 cm; 59.9 ± 8.8 kg) | Prone hip extension against strap with the knee flexed at 90 ° Placement parallel alignment over the belly. | Single leg wall slide, other leg knee flexed Single leg mini-squat Lateral step down (20 cm height) Forward step down (20 cm height) | 21.6 male 32.0 female 20.3 male 26.6 female 8.4 male 24.6 female 19.0 male 27.2 female |
| Hollman, Galardi, Lin, et al. 34 | 41 females (18-36 years) | Prone hip extension against strap with the knee flexed at 90 ° Placement at one-half the distance between the sacrum and greater trochanter. | Single leg squat | 20.9-23.8 |
| Emami, Arab, Ghamkhar 35 | 10 males (22.5 ± 3.8 years; 177 ± 7 cm; 74.1 ± 8.0 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement at the midpoint of a line running from S2 to the greater trochanter. | Prone hip extension with knee extension | 18.3 ± 12.1 |
| MacAskill, Durant, Wallace 36 | 14 males, 20 females (21.5 ± 1.7 years; 170.5 ± 11 cm; 67.6 ± 7.5 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement 1/3rd of the distance between the second sacral vertebra and the greater trochanter. | Forward step up (15 cm height) Lateral step up (15 cm height) | 28.7 ± 18.7 31 ± 19.9 |
| Park, Yoo 37 | 18 males (21.9 ± 2.2 years; 175.1 ± 5.3 cm; 66.6 ± 8.4 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement at half the distance between the trochanter and the sacral vertebrae in the middle of the muscle on an oblique angle. | Back/torso extension with extended knees and hands across chest Back/torso extension with extended knees and hands behind head Back/torso extension with flexed knees 90 ° and hands across chest Back/torso extension with flexed knees 90 ° and hands behind head | 28.3 ± 14.5 26.5 ± 13.6 34.8 ± 20.6 36.6 ± 22.6 |
| Suehiro, et al. 38 | 21 males (20.2 ± 0.4 years; 171.1 ± 5.0 cm; 64.3 ± 10.5 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement halfway between the greater trochanter and the second sacral vertebra. | Prone hip extension with 90 ° knee flexion and neutral hip position Prone hip extension with 90 ° knee flexion and 15 ° hip abduction Prone hip extension with 90 ° knee flexion and 15 ° hip abduction and 20 ° hip external rotation | 14.1 ± 9.4 22.5 ± 13.6 41.0 ± 23.6 |
| Kim, Kim 39 | 14 males, 16 females (24.7 ± 3.2 years; 167.5 ± 8.2 cm; 61.5 ± 6.9 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement 1/3rd the distance between the second sacral vertebrae and the greater trochanter. | Prone hip extension to 10 ° Prone hip extension to 10 ° with abdominal drawing-in Prone hip extension to 10 ° with pelvic tilt > 15 ° Prone hip extension to 10 ° with abdominal drawing-in with pelvic tilt > 15 ° | 23.9 ± 18.5 24.4 ± 14.3 32.5 ± 21.3 45.9 ± 33.7 |
| Kim, Yoo 40 | 18 males (23.3 ± 1.8 years; 177.4 ± 5.3 cm; 74.2 ± 7.2 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement not specified. | Prone hip extension with upper body on table Prone hip extension with body on floor | 62.3 ± 27.1 56.5 ± 20.2 |
| Mills, Frank, Goto, et al. 41 | 20 females (Anthropometrical details not provided) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement 1/3rd the distance between the second sacral vertebrae and the greater trochanter | Squat | 12.4 ± 6.3 |
| Yoon, Lee, An 42 | 15 subjects (26.7 ± 3.7 years; 167.1 ± 9.2 cm; 58.1 ± 11.7 kg) | MVIC position not specified Placement not specified | Prone hip extension from 0 ° hip flexion Prone hip extension from 15 ° hip flexion Prone hip extension from 30 ° hip flexion | 19.7 ± 7.9 22.5 ± 9.4 18.9 ± 7.8 |
| Youdas, Hartman, Murphy, et al. 43 | 13 males (23.4 ± 1.3 years; 180 ± 10 cm; 79.7 ± 10.6 kg) 13 females (23.5 ± 1.2 years; 170 ± 10 cm; 63.7 ± 7.4 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement on the muscle belly, parallel to the line of action. | Bridge Bridge with feet on swiss ball Single leg bridge Single leg bridge with foot on bosu Bridge with hamstring curl Bridge with feet on swiss ball and hamstring curl | 16.4 13.0 32.6 28.4 18.5 10.9 |
| Choi, Bak, Cho, et al. 44 | 14 males, 13 females (27.8 ± 5.8 years; 166.4 ± 10.1 cm; 66.2 ± 13.4 kg) | MVIC position not specified Placement between the sacrum and greater trochanter | Bridge Single leg bridge Single leg bridge (raised leg abducted to 30 °) | 41.5 ± 16.4 47.3 ± 16.0 46.7 ± 12.0 |
| Jeon, et al. 45 | 16 males (25.4 ± 4.2 years; 174.7 ± 2.8 cm; 73.1 ± 2.1 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement at the midpoint of the line extending between the greater trochanter and sacrum | Prone hip extension with upper body on table Prone hip extension with upper body on table and abdominals drawing-in Prone hip extension with upper body on table and flexed contralateral knee joint on a chair | 43.9 ± 16.1 47.5 ± 19.8 66.4 ± 25.8 |
| Lee, Song, Kwon 46 | 10 males, 10 females (21.1 ± 1.8 years; 168.7 ± 8.3 cm; 66.1 ± 12.3 kg) | MVIC method not specified. Placement at 50% on the line between the sacral vertebrae and the greater trochanter | Squat with 0 ° trunk flexion Squat with 15 ° trunk flexion Squat with 30 ° trunk flexion | 6.1 ± 4.0 6.3 ± 4.0 8.0 ± 4.9 |
| Selkowitz, Beneck, Powers 47 | 10 males, 10 females (27.9 ± 6.2 years; 170.5 ± 11.1 cm; 67.7 ± 14.1 kg) | Four conditions normalised to whichever contraction elicited greater EMG excitation: 1) Prone hip extension of 45 ° with the knee flexed at 90 ° against strap resistance. 2) Prone hip extension of 0 ° with the knee flexed at 90 ° against strap resistance. 3) Sidelying position with hip in 30 ° abduction and knee extended against strap. 4) As position 3 with hip in 45 ° flexion. Placement Gmax (S) inserted superior and lateral to the midpoint of a line drawn between the posterior superior iliac spine and the posterior greater trochanter, Gmax (I) inserted inferior and medial to the midpoint of the same line, such that it was 2.5 to 5.0 cm above the gluteal fold. | Bridge Forward step up Lunge Single leg bridge Squat Quadruped hip extension with knee extended Quadruped hip extension with knee flexed | 17.4 ± 12.0 (S) 22.3 ± 10.1 (I) 22.8 ± 15.6 (S) 15.7 ± 6.0 (I) 20.1 ± 11.1 (S) 18.5 ± 6.2 (I) 34.6 ± 16.8 (S) 36.7 ± 10.0 (I) 12.9 ± 7.9 (S) 10.5 ± 7.1 (I) 28.5 ± 16.6 (S) 31.2 ± 16.5(I) 30.1 ± 12.5 (S) 34.3 ± 16.3 (I) |
| Chan, et al. 48 | 10 males, 10 females (21.1 ± 1.7 years; 166.8 ± 7.9 cm; 58.1 ± 9.2 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement 1/3rd of the distance from iliac crest to greater trochanter, starting from greater trochanter. | Prone hip extension up to 20 ° with 90 ° knee flexion Prone hip extension up to 20 ° with 90 ° knee flexion with abdominal bracing | 14.8 concentric (S) 12.3 eccentric (S) 20.1 concentric (I) 11.7 eccentric (I) 19.7 concentric (S) 16.6 eccentric (S) 25.6 concentric (I) 36.0 eccentric (I) |
| Hollman, et al. 49 | 15 females (23.3 ± 1.7 years; 169.4 ± 8.3 cm; 62.6 ± 6.7 kg) | Prone hip extension against strap resistance with the knee flexed at 90 ° Placement halfway between the sacral vertebrae and the greater trochanter | Bridge Bridge with verbal and tactile cueing | 16.8 33.0 |
| Lehecka, et al. 50 | 12 males, 16 females (23.4 ± 2.3 years; 173 ± 11 cm; 72.6 ± 13.9 kg) | Prone hip extension against strap resistance with the knee flexed at 90 ° Placement anterosuperior to Gmax, inferior to the lateral aspect of the iliac crest on a line towards the greater trochanter on the muscle belly. | Single leg bridge. DOM leg 90 ° knee flexion with foot flat. Non-DOM leg knee extended Single leg bridge. DOM leg 135 ° knee flexion with foot flat. Non-DOM leg knee extended Single leg bridge. DOM leg 90 ° knee flexion with foot flat. Non-DOM leg knee relaxed in flexion and femur vertical Single leg bridge. DOM leg 90 ° knee flexion with dorsiflexed ankle. Non-DOM leg knee relaxed in flexion and femur vertical Single leg bridge. DOM leg 135 ° knee flexion with dorsiflexed ankle. Non-DOM leg knee relaxed in flexion and femur vertical | 51.0 ± 28.1 47.4 ± 24.8 47.2 ± 28.1 49.1 ± 26.4 40.4 ± 24.6 |
| Van Oosterwijck, et al. 51 | 4 males, 9 females (22.6 ± 2.1 years; 172 ± 7.3 cm; 61.3 ± 9.5 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement midway between the posterosuperior iliac spine and the ischial tuberosity). | Prone back/torso extension without lumbopelvic control strategy Prone back/torso extension with lumbopelvic control strategy Reverse hyperextension without lumbopelvic control strategy Reverse hyperextension with lumbopelvic control strategy | 23.8 ± 10.1 32.4 ± 21.6 22.0 ± 7.7 38.8 ± 24.1 |
| Youdas, et al. 52 | 13 males, 13 females (23.5 ± 1.2 years; 175.0 ± 10.0 cm; 71.7 ± 9.0 kg) | Prone hip extension against manual resistance with the knee flexed at 90 ° Placement parallel to the muscle’s line of action. | Single leg bridge Supine manual resisted hip extension | 33.8 34.7 |
Though several limitations exist within this review, some general observations can be made as follows:
- Body weight hip extension exercises provided a wide range of gluteus maximus electromyography excitation ranging from 6.1% to 106.2% maximum voluntary isometric contraction (MVIC);
- When pooled as an average, similar levels of excitation were found between force vectors though the range of excitation levels differed between vectors;
- Unilateral exercises produced higher electromyography values compared to the bilateral version of the same exercise;
- Females exhibited greater electromyography excitation than males in all hip extension exercises,
- Verbal and tactile cues increase gluteus maximus electromyography excitation, while bracing and drawing-in the abdominals also increase excitation levels; and,
- Hip extension exercises performed in greater degrees/angles of hip flexion, hip abduction or hip external rotation result in higher measured electromyography excitation levels.
The pooled averaged values for the same exercises should be interpreted as a guideline and caution should be used for interpreting their findings with further research into each exercise with the same methodology required to verify these results. Moreover, this review focused on body weight exercises, therefore, whether the loaded version of the same exercises in this review results in similar findings requires investigation. When strengthening a weaker muscle or muscle group, practitioners may wish to prescribe a gradual and progressive exercise program to ensure the targeted area is developed. Practitioners should initially consider exercises performed in the horizontal vector as they provide a large base of support and are less challenging compared to vertical vector exercises. Moreover, bi-lateral exercises should be mastered before prescribing unilateral versions. This may be of importance if individuals seek and implement a compensatory movement pattern when faced with weakness or dysfunction. Individuals may benefit from being prescribed exercises that they can perform with good technique without substitution. Subsequently, once this can be achieved, exercise difficulty can be progressed with more demanding exercises.
- Elzanie A, Borger J. Anatomy, Bony Pelvis and Lower Limb, Gluteus Maximus Muscle. [Updated 2019 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538193[↩][↩][↩]
- Apaydin N, Bozkurt M, Loukas M, Tubbs RS, Esmer AF. The course of the inferior gluteal nerve and surgical landmarks for its localization during posterior approaches to hip. Surg Radiol Anat. 2009 Jul;31(6):415-8[↩]
- DeJong AF, Mangum LC, Resch JE, Saliba SA. Detection of Gluteal Changes Using Ultrasound Imaging During Phases of Gait in Individuals With Medial Knee Displacement. J Sport Rehabil. 2018 Dec 17;:1-11.[↩]
- Barker PJ, Hapuarachchi KS, Ross JA, Sambaiew E, Ranger TA, Briggs CA. Anatomy and biomechanics of gluteus maximus and the thoracolumbar fascia at the sacroiliac joint. Clin Anat. 2014 Mar;27(2):234-40.[↩]
- Mu A, Peng P, Agur A. Landmark-Guided and Ultrasound-Guided Approaches for Trochanteric Bursa Injection: A Cadaveric Study. Anesth. Analg. 2017 Mar;124(3):966-971.[↩]
- Rocos B, Ward A. Gluteal compartment syndrome with sciatic nerve palsy caused by traumatic rupture of the inferior gluteal artery: a successful surgical treatment. BMJ Case Rep. 2017 Jan 25;2017[↩]
- Saad PF, Saad KR, Armstrong DM, Soares BL, de Almeida PH, Razuk Filho Á. Inferior gluteal artery pseudoaneurysm related to intramuscular injection. Int J Surg Case Rep. 2015;6C:29-32.[↩]
- Iwanaga J, Simonds E, Vetter M, Patel M, Oskouian RJ, Tubbs RS. The inferior gluteal nerve often has a cutaneous branch: A discovery with application to hip surgery and targeting gluteal pain syndromes. Clin Anat. 2018 Sep;31(6):937-941[↩]
- Kim SM, Yoo WG. Comparison of trunk and hip muscle activity during different degrees of lumbar and hip extension. J Phys Ther Sci. 2015 Sep;27(9):2717-8[↩]
- Sugisaki N, Kobayashi K, Tsuchie H, Kanehisa H. Associations Between Individual Lower-Limb Muscle Volumes and 100-m Sprint Time in Male Sprinters. Int J Sports Physiol Perform. 2018 Feb 01;13(2):214-219.[↩]
- Navandar A, Veiga S, Torres G, Chorro D, Navarro E. A previous hamstring injury affects kicking mechanics in soccer players. J Sports Med Phys Fitness. 2018 Dec;58(12):1815-1822[↩]
- Orozco-Chavez I, Mendez-Rebolledo G. Effect of squatting velocity on hip muscle latency in women with patellofemoral pain syndrome. J Phys Ther Sci. 2018 Mar;30(3):381-386[↩]
- Macadam P, Feser EH. EXAMINATION OF GLUTEUS MAXIMUS ELECTROMYOGRAPHIC EXCITATION ASSOCIATED WITH DYNAMIC HIP EXTENSION DURING BODY WEIGHT EXERCISE: A SYSTEMATIC REVIEW. Int J Sports Phys Ther. 2019;14(1):14-31. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6350668/[↩][↩]
- Worrell TW Crisp E LaRosa C. Electromyographic reliability and analysis of selected lower extremity muscles during lateral step-up conditions. J Athl Train. 1998;33(2):156.[↩]
- Zeller BL McCrory JL Ben Kibler W, et al. Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Amer J Sports Med. 2003;31(3):449-456.[↩]
- Ayotte NW Stetts DM Keenan G, et al. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight-bearing exercises. J Orthop Sports Phy Ther. 2007;37(2):48-55.[↩]
- Ekstrom RA Donatelli RA Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37(12):754-762[↩]
- Ekstrom RA Osborn RW Hauer PL. Surface electromyographic analysis of the low back muscles during rehabilitation exercises. J Orthop Sports Phys Ther. 2008;38(12):736-745.[↩]
- Farrokhi S Pollard CD Souza RB, et al. Trunk position influences the kinematics, kinetics, and muscle activity of the lead lower extremity during the forward lunge exercise. J J Orthop Sports Phys Ther. 2008;38(7):403-409[↩]
- Boudreau SN Dwyer MK Mattacola CG, et al. Hip-muscle activation during the lunge, single-leg squat, and step-up-and-over exercises. J Sport Rehab. 2009;18(1):91-103[↩]
- Distefano LJ Blackburn JT Marshall SW, et al. Gluteal muscle activation during common therapeutic exercises. J Orthop Sports Phys Ther. 2009;39(7):532-540[↩]
- Lewis CL Sahrmann SA. Muscle activation and movement patterns during prone hip extension exercise in women. J Athle Train. 2009;44(3):238-248[↩]
- Sakamoto A Teixeira-Salmela L Rodrigues dPF, et al. Gluteus maximus and semitendinosus activation during active prone hip extension exercises. Brazilian J Phys Ther. 2009;13(4):335-342[↩]
- Lubahn AJ Kernozek TW Tyson TL, et al. Hip muscle activation and knee frontal plane motion during weight bearing therapeutic exercises. Int J Sports Phys Ther. 2011;6(2):92.[↩]
- Boren K Conrey C Le Coguic J, et al. Electromyographic analysis of gluteus medius and gluteus maximus during rehabilitation exercises. Int J Sports Phys Ther. 2011;6(3):206[↩]
- Bouillon LE Wilhelm J Eisel P, et al. Electromyographic assessment of muscle activity between genders during unilateral weight-bearing tasks using adjusted distances. Int J Sports Phys Ther. 2012;7(6):595.[↩]
- Nakagawa TH Moriya ET Maciel CD, et al. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J Orthop Sports Phy Ther. 2012;42(6):491-501[↩]
- Tateuchi H Taniguchi M Mori N, et al. Balance of hip and trunk muscle activity is associated with increased anterior pelvic tilt during prone hip extension. J Electrom Kin. 2012;22(3):391-397[↩]
- De Ridder EM Van Oosterwijck JO Vleeming A, et al. Posterior muscle chain activity during various extension exercises: an observational study. BMC Muscul Dis. 2013;14(1):204[↩]
- Kang S-Y Jeon H-S Kwon O, et al. Activation of the gluteus maximus and hamstring muscles during prone hip extension with knee flexion in three hip abduction positions. Man Ther. 2013;18(4):303-307.[↩]
- Lee KS Ko E Lim CG. Effect of pelvic belt on gluteal muscles activity during therapeutic exercise. J Physl Ther Sci. 2013;25(3):337-340.[↩]
- Webster K Gribble P. A comparison of electromyography of gluteus medius and maximus in subjects with and without chronic ankle instability during two functional exercises. Phys Ther in Sport. 2013;14(1):17-22[↩]
- Bolgla L Cook N Hogarth K, et al. Trunk and hip electromyographic activity during single leg squat exercises do sex differences exist? Int J Sports Phys Ther. 2014;9(6):756.[↩]
- Hollman JH Galardi CM Lin I-H, et al. Frontal and transverse plane hip kinematics and gluteus maximus recruitment correlate with frontal plane knee kinematics during single-leg squat tests in women. Clin Biomech. 2014;29(4):468-474[↩]
- Emami M Arab AM Ghamkhar L. The activity pattern of the lumbo-pelvic muscles during prone hip extension in athltes with and without hamstring strain injuy. Int J Sports Phys Ther. 2014;9(3):312.[↩]
- MacAskill MJ Durant TJ Wallace DA. Gluteal muscle actvity during weightbearing and non-weightbearing exercise. Int J Sports Phys Ther. 2014;9(7):907[↩]
- Park S-y Yoo W-g. Effects of hand and knee positions on muscular activity during trunk extension exercise with the Roman chair. J Electrom Kin. 2014;24(6):972-976[↩]
- Suehiro T Mizutani M Okamoto M, et al. Influence of hip joint position on muscle activity during prone hip extension with knee flexion. J Phys Ther Sci. 2014;26(12):1895-1898[↩]
- Kim TW Kim YW. Effects of abdominal drawing-in during prone hip extension on the muscle activities of the hamstring, gluteus maximus, and lumbar erector spinae in subjects with lumbar hyperlordosis. J Phys Ther Scie. 2015;27(2):383-386[↩]
- Kim S-m Yoo W-g. Comparison of trunk and hip muscle activity during different degrees of lumbar and hip extension. J Phys Ther Sci. 2015;27(9):2717-2718[↩]
- Mills M Frank B Goto S, et al. Effect of restricted hip flexor muscle length on hip extensor muscle activity and lower extremity biomechanics in college-aged female soccer players. Int J Sports Phys Ther. 2015;10(7):946[↩]
- Yoon J-Y Lee M-R An D-H. Effect of initial position on the muscle activity of the hip extensors and amount of pelvic tilt during prone hip extension. J Phys Ther Sci.. 2015;27(4):1195-1197[↩]
- Youdas JW Hartman JP Murphy BA, et al. Magnitudes of muscle activation of spine stabilizers, gluteals, and hamstrings during supine bridge to neutral position. Physio Theory Pract. 2015;31(6):418-427[↩]
- Choi K Bak J Cho M, et al. The effects of performing a one-legged bridge with hip abduction and use of a sling on trunk and lower extremity muscle activation in healthy adults. J Phys The Sci. 2016;28(9):2625-2628[↩]
- Jeon I-c Kwon O-y Weon J-h, et al. Comparison of Hip and Back Muscle Activity and Pelvic Compensation in Healthy Subjects During Three Different Prone Table Hip Extension Exercises. J Sport Rehab. 2016:1-19[↩]
- Lee T-S Song M-Y Kwon Y-J. Activation of back and lower limb muscles during squat exercises with different trunk flexion. J Phys The Sci. 2016;28(12):3407-3410[↩]
- Selkowitz DM Beneck GJ Powers CM. Comparison of Electromyographic Activity of the Superior and Inferior Portions of the Gluteus Maximus Muscle During Common Therapeutic Exercises. J Orthop Sports Phys Ther. 2016;46(9):794-799[↩]
- Chan MK Chow KW Lai AY, et al. The effects of therapeutic hip exercise with abdominal core activation on recruitment of the hip muscles. BMC Muscul Dis. 2017;18(1):313[↩]
- Hollman JH Berling TA Crum EO, et al. Do Verbal and Tactile Cueing Selectively Alter Gluteus Maximus and Hamstring Recruitment During a Supine Bridging Exercise in Active Females? A Randomized Controlled Trial. J Sport Rehab. 2017:1-22.[↩]
- Lehecka B Edwards M Haverkamp R, et al. Building a better gluteal bridge: Electromyographic analysis of hip muscle activity during modified single-leg bridges. Int J Sports Phys Ther. 2017;12(4):543.[↩]
- Van Oosterwijck J De Ridder E Vleeming A, et al. Applying an active lumbopelvic control strategy during lumbar extension exercises: Effect on muscle recruitment patterns of the lumbopelvic region. Human Move Sci. 2017;54:24-33[↩]
- Youdas JW Hartman JP Murphy BA, et al. Electromyographic analysis of gluteus maximus and hamstring activity during the supine resisted hip extension exercise versus supine unilateral bridge to neutral. Physio Theory Pract. 2017;33(2):124-130.[↩]





{kind=link}