Contents
HDL cholesterol
HDL stands for high density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke 1, 2, 3. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL 4, 5. However, several recent investigations, including many clinical trials focusing on increasing HDL cholesterol levels with drug therapies did not show any beneficial effect on cardiovascular disease 6, 7, starting a lively debate about the appropriateness of HDL as a therapeutic target. A recent meta-analysis reported that the total number of HDL particles, as well as numbers of small and medium, but less so large HDL particles, are associated with incident of atherosclerotic cardiovascular diseases 8, 9. A recent Mendelian randomization study found genetically causal associations of coronary artery disease or heart attack (myocardial infarction) with the concentrations of medium and small HDL particles, but not with large HDL particles 10, 11. This heterogeneity is potentially important since lipid-modifying drugs cause diverse changes in HDL particle size, number, and composition. Treatment with nicotinic acid and CETP inhibitors increases HDL cholesterol levels more profoundly than HDL particles, while treatment with fibrates increases HDL particles more strongly than HDL cholesterol 12. Recent large epidemiological studies showed extremely high levels of HDL cholesterol had an adverse effect on death from atherosclerotic cardiovascular disease 13, 14, 15, 16, 17. In addition, HDL is a rather complex family of different particles, being composed of sub-species differing in size, density, shape, charge, and composition, undergoing continuous remodelling processes in your blood 18. This remarkable heterogeneity of the HDL particle family may explain why HDL cannot always be considered ‘anti-atherogenic’, but can sometimes become dysfunctional or even ‘pro-atherogenic’ 19. This new insight into the complex functions of HDL has reinforced the idea that HDL is not merely a cholesterol transporter, but, rather possesses several additional functional properties including cholesterol efflux capacity, anti-oxidant, anti-inflammatory, and immune-regulating activities 18. This led to the suggestion that the functionality of HDL, that is determined by its composition and post-translational modifications are more important determinants for protection against cardiovascular disease than the HDL cholesterol levels of 20, 21.
Cholesterol travels through your blood on proteins called lipoproteins (see Figure 2). High density lipoprotein (HDL) is the smallest circulating lipoprotein and is found near all cells. HDLs are predominantly spherical particles of varying size, surface charge and lipid and apolipoprotein composition 22. All HDLs have the same overall structure: a water insoluble, neutral lipid core mainly cholesteryl esters and some triglycerides surrounded by a surface monolayer mainly phospholipids and some unesterified cholesterol in which apolipoproteins are embedded (see Figure 1) 19. Particles with a hydrophobic neutral lipid core form spherical-like structures approximately 8–11 nm in diameter (referred to as α-migrating HDL, based on their migration on agarose gel), whereas particles depleted of neutral lipids form disc-like structures 22. Detailed analysis of HDL particle revealed the existence of two major HDL apolipoproteins, apolipoprotein A-I (apoA-1 or APOA1) and apolipoprotein A-2 (apoA-II) that account for ~70% and ~20% of HDL protein mass, with small amounts of other apoproteins such as apoA-IV, apoA-V, apoC and apoE 23, 24, 25, 26, 27. Additionally, HDL has been shown to contain a lot more proteins (>80) like the lipocalins apoD and apoM 28. Due to differences in apolipoproteins (Apo), phospholipids, cholesterol and cholesteryl esters, high density lipoproteins have differences in surface charge and density and can thereby be classified into Gamma (γ-), Alpha (α-) or preBeta (preβ-) migrating particles or into larger-sized, lower-density (HDL2a and HDL2b) and smaller-sized, higher-density (HDL3a, HDL3b, and HDL3c) sub-classes 29, 30, 31.
Historically, HDL was first sub-fractionated based on the density of lighter and larger HDL2 (HDL2a and HDL2b) and heavier and smaller HDL3 (HDL3a, HDL3b, and HDL3c) sub-fractions 32. Another early classification of HDL sub-fractions was based on the presence or absence of apoA-II, the second most abundant protein in HDL. These types of classifications had, however, limited impact on routine diagnostic testing, because of lacking evidence for superiority 19. Separation of HDL into discrete HDL size fractions can now be readily done by nuclear magnetic resonance (NMR) spectroscopy in clinical laboratories, providing the ratio of large-to-small HDL, which may be useful for assessing not only cardiovascular risk but also insulin resistance and other conditions 32. Recent advances in mass spectrometry allow the comprehensive quantification of the proteome in total HDL as well as distinct sub-classes 33, 34, 35, 36. At this time, there is only limited commercial availability of these advanced HDL sub-fractionation tests and hence they are not widely used but they are being actively investigated for their clinical utility 19.
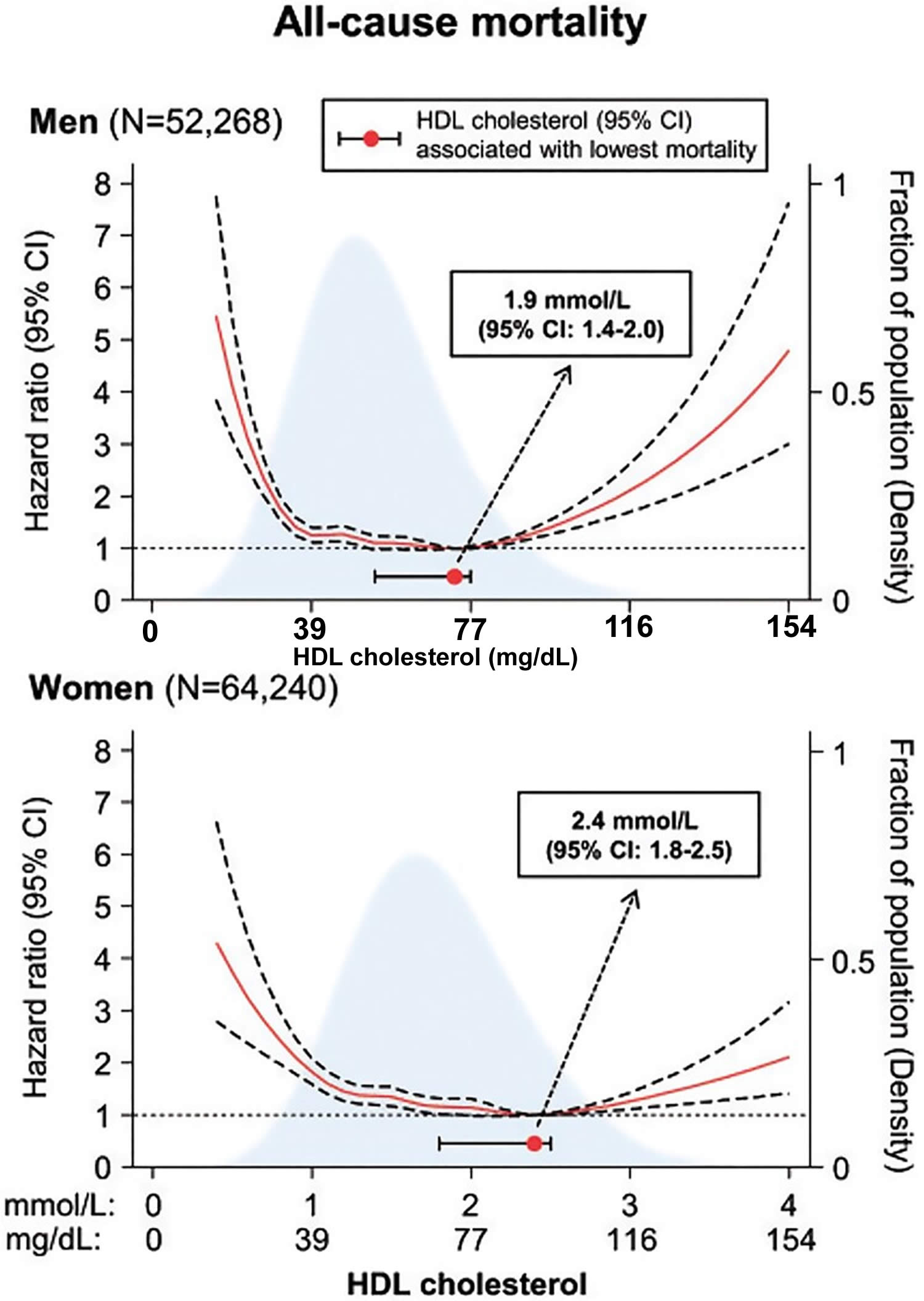
From a functional point of view, HDL cholesterol is not a causal marker because the many functions of HDL are exerted either by entire HDL particles or specific components other than cholesterol 19. Furthermore, low HDL cholesterol is strongly associated with increased levels of triglyceride-rich lipoproteins. Low HDL levels are nowadays widely considered as an indirect and non-causal biomarker of elevated atherosclerotic cardiovascular disease risk reflecting the atherogenicity of elevated plasma levels of triglyceride-rich lipoprotein and their remnants 37. Both low and extremely high HDL levels are associated with an increased risk of all-cause mortality 14.
Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
Experts believe HDL cholesterol may act in a variety of helpful ways that tend to reduce the risk for heart disease 38:
- HDL cholesterol scavenges and removes LDL or “bad” cholesterol.
- HDL reduces, reuses, and recycles LDL cholesterol by transporting it to the liver where it can be reprocessed.
- HDL cholesterol acts as a maintenance crew for the inner walls (endothelium) of blood vessels. Damage to the inner walls is the first step in the process of atherosclerosis, which causes heart attacks and strokes. HDL scrubs the wall clean and keeps it healthy.
- HDL cholesterol below 40mg/dL are strongly associated with increased risk of coronary artery disease and peripheral arterial disease and are characterized by an atherogenic dyslipidemia consisting of high levels of LDL particles, elevated triglycerides and increased insulin resistance.
- Low HDL cholesterol levels are associated with an increased risk of autoimmune disease 39 and cancer 40, 41, 42, 43; for cancer, the risk increase was more pronounced for low apoA-I than for low HDL leve 41, suggesting that HDL particles rather than their cholesterol content drive this association.
- High HDL cholesterol 60 mg/dL or higher is Protective against heart disease.
- Several recent investigations, including many clinical trials focusing on increasing HDL cholesterol levels with drug therapies did not show any beneficial effect on cardiovascular disease 6, 7. A recent meta-analysis reported that the total number of HDL particles, as well as numbers of small and medium, but less so large HDL particles, are causal associations of coronary artery disease or atherosclerotic cardiovascular disease 8, 10, 9. A recent Mendelian randomization study found genetically causal associations of coronary artery disease or heart attack (myocardial infarction) with the concentrations of medium and small HDL particles, but not with large HDL particles 10, 11.
- Recent large epidemiological studies showed extremely high levels of HDL cholesterol had an adverse effect on death from atherosclerotic cardiovascular disease 13, 14, 15, 16, 17. In addition, HDL is a rather complex family of different particles, being composed of sub-species differing in size, density, shape, charge, and composition, undergoing continuous remodelling processes in your blood 18. This remarkable heterogeneity of the HDL particle family may explain why HDL cannot always be considered ‘anti-atherogenic’, but can sometimes become dysfunctional or even ‘pro-atherogenic’ 19. This new insight into the complex functions of HDL has reinforced the idea that HDL is not merely a cholesterol transporter, but, rather possesses several additional functional properties including cholesterol efflux capacity, anti-oxidant, anti-inflammatory, and immune-regulating activities 18. This led to the suggestion that the functionality of HDL, that is determined by its composition and post-translational modifications are more important determinants for protection against cardiovascular disease than the HDL cholesterol levels of 20, 21.
- Despite the clinical utility of low HDL cholesterol, the associations between HDL cholesterol and atherosclerotic cardiovascular disease are not linear and vary according to race or ethnicity. There is a U-shaped association between HDL cholesterol and atherosclerotic cardiovascular disease mortality, with a linear inverse association preserved below 40mg/dL HDL in men and below 50-58 mg/dL HDL in women, no association across the normal range (40-96 mg/dL in men and 50-134 mg/dL in women), and a modest but increased atherosclerotic cardiovascular disease risk at HDL cholesterol levels above 90 mg/dL in Asians, above 97 mg/dL in White male and above 135 mg/dL in White female populations 40, 17. Moreover, the links between HDL cholesterol and atherosclerotic cardiovascular disease among Blacks may be attenuated or even trend in the opposite direction compared to Whites 9.
People with high blood triglycerides usually also have lower HDL cholesterol. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do.
A healthy HDL cholesterol level may protect against heart attack and stroke. Studies show low levels of HDL cholesterol increase the risk of heart disease. HDL cholesterol does not completely eliminate LDL cholesterol. Only one-fourth to one-third of blood cholesterol is carried by HDL.
HDL levels should be around 50 mg/dL. Some people can raise HDL by::
- Exercising for at least 30 minutes 5 times a week
- Quitting smoking
- Avoiding saturated fats
- Losing weight
Others may need medicine to get HDL to a beneficial level, and should work with your doctor on a treatment plan.
Figure 1. HDL cholesterol structure
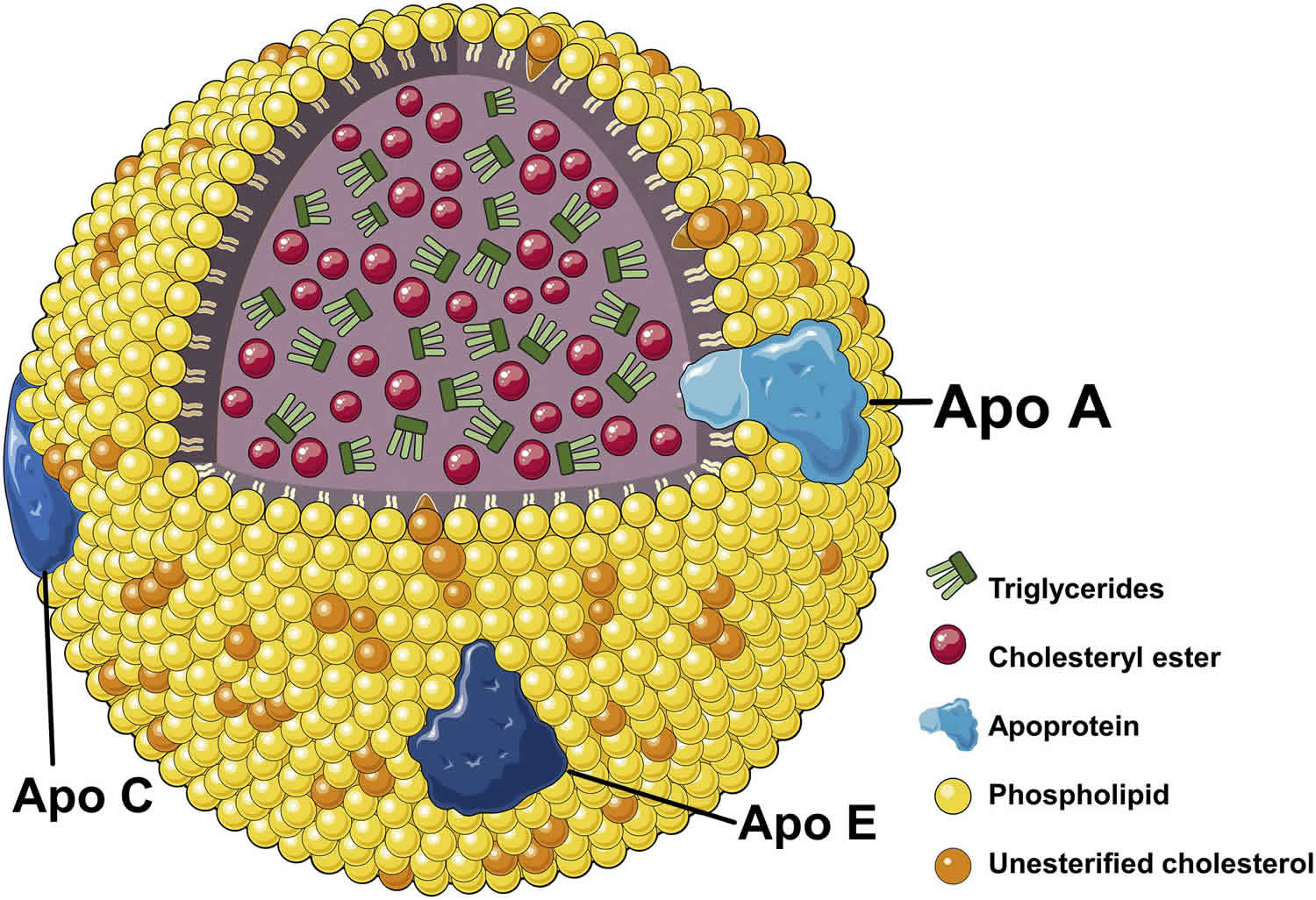
Footnotes: Generalized structure of high-density lipoprotein (HDL) cholesterol. High-density lipoprotein (HDL) particles carry a large number of proteins and lipids, which contribute to their compositional and functional complexity. High-density-lipoproteins (HDL) particles consist of a core of triglycerides and cholesteryl esters. This core is surrounded by a phospholipid monolayer containing unesterified cholesterol and several apoproteins (mostly apoA-1). In their mature form, HDL contains a nonpolar lipid core mainly consisting of cholesteryl esters and triglycerides surrounded by a single surface monolayer of phospholipids (mainly phosphatidylcholine), unesterified cholesterol and amphipathic apolipoproteins. Based the presence of absence of cholesteryl esters, HDL has either a discoidal or a spherical shape. HDL can be further subdivided into larger-sized, lower-density (HDL2a and HDL2b) and smaller-sized, higher-density (HDL3a, HDL3b, and HDL3c) sub-classes 29. Apolipoproteins associated with HDL can undergo post-translational modifications. The major apolipoprotein constituents of HDL are apoA-I (70%) and apoA-II (20%), with small amounts of other apoproteins such as apoA-IV, apoA-V, apoC and apoE 27. Additionally, HDL has been shown to contain a lot more proteins (>80) like the lipocalins apoD and apoM 28.
[Source 44 ]Figure 2. Lipoprotein
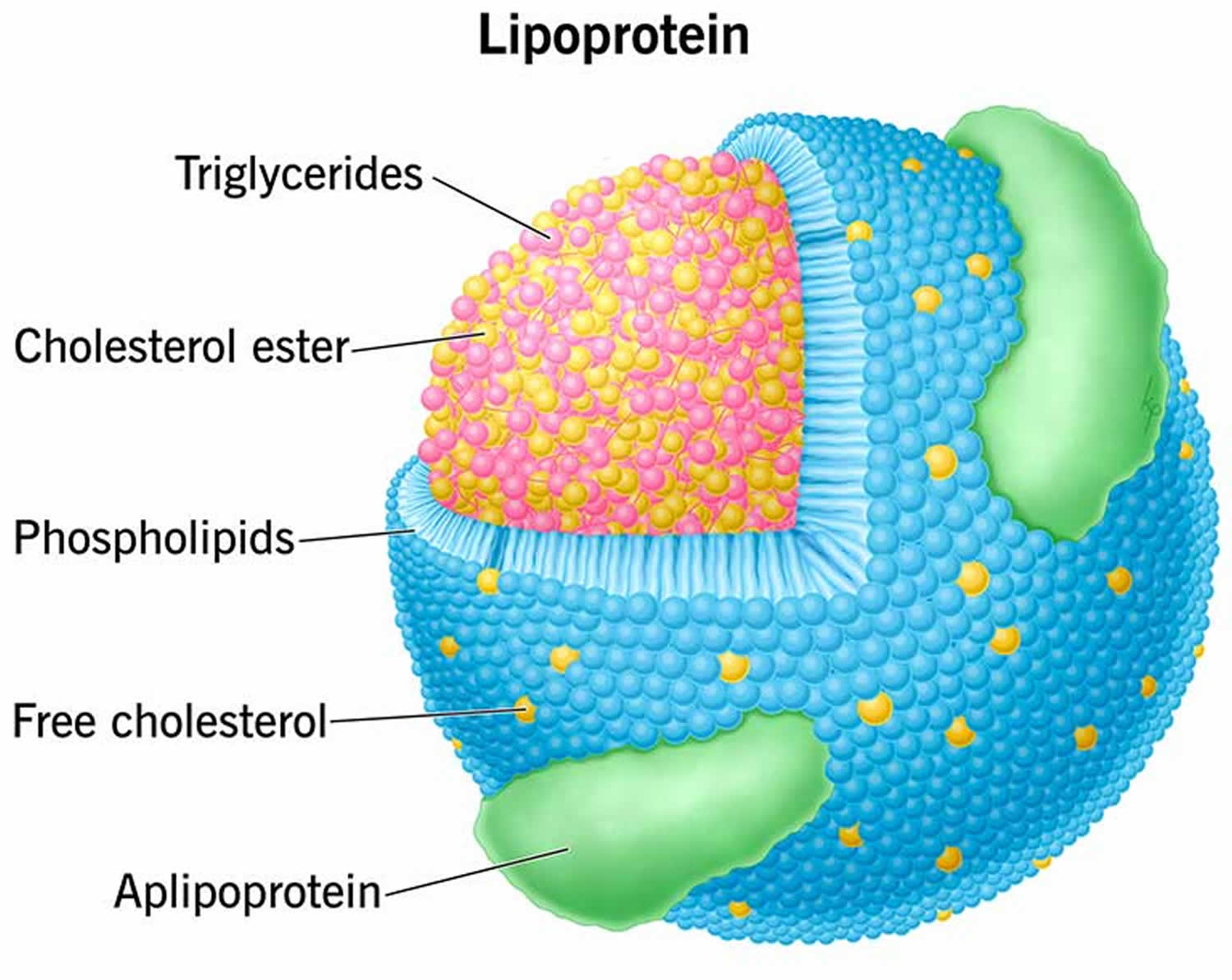 Footnote: Lipoprotein contains both proteins and lipids.
Footnote: Lipoprotein contains both proteins and lipids.Figure 3. General overview of HDL metabolism
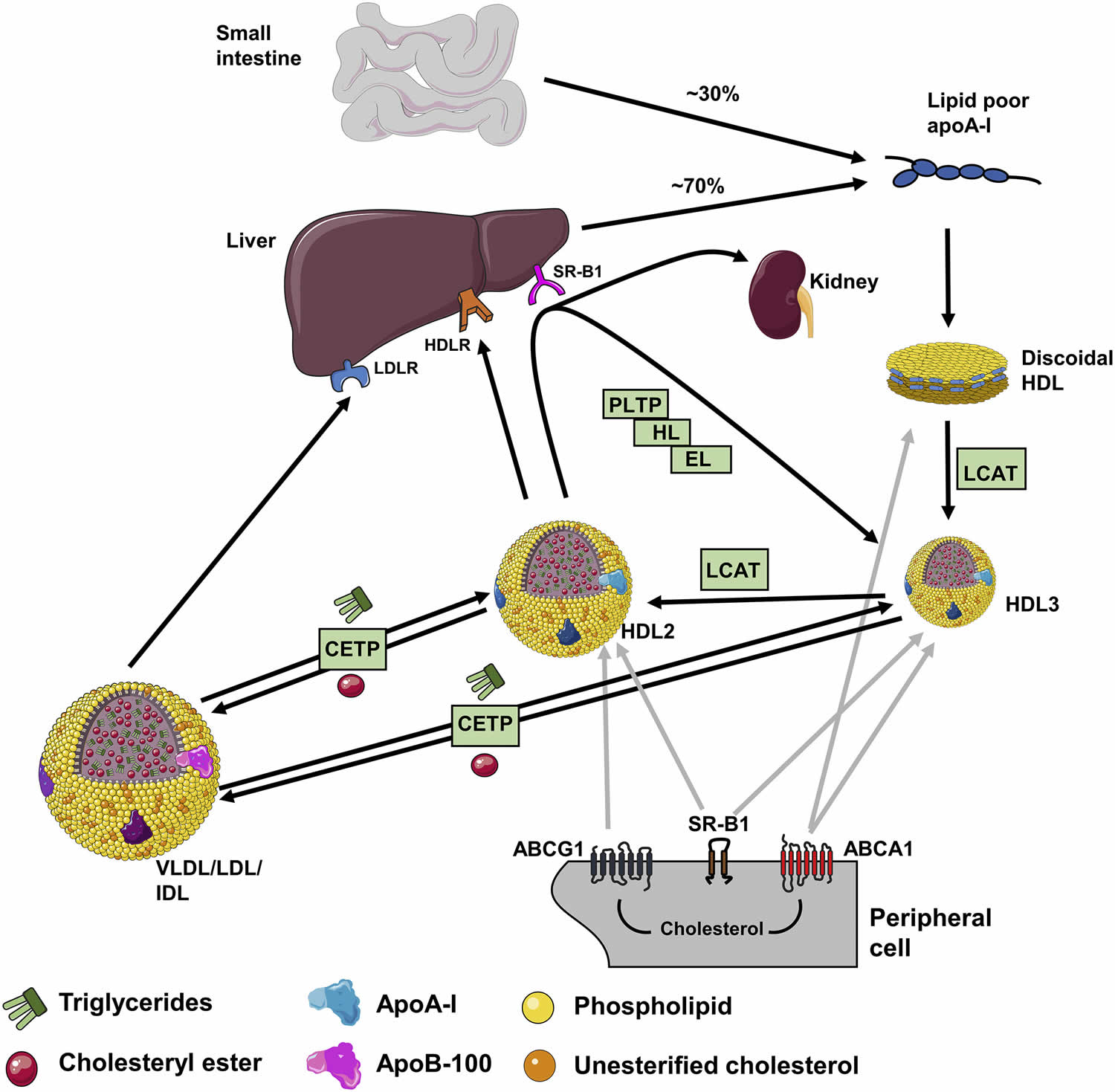
Footnotes: General overview of HDL metabolism. Apolipoprotein A-I (ApoA-I) is produced in the liver and intestines and subsequently forms discoidal HDL after interacting with the ATP-binding cassette transporter A1 (ABCA1). Continued cholesterol export via ABCG1 and via scavenger receptor class B member 1 (SR-B1) in macrophages and enzymatic reactions mediated by lecithin-cholesterol acyltransferase (LCAT) result in the conversion into spherical HDL3 and HDL2 particles. Cholesterol and cholesteryl esters can be transferred to the liver by two main pathways, directly through binding to scavenger receptor class B member 1 (SR-B1) in the liver and subsequent excretion via the kidneys, or indirectly by being transferred to very-low-density lipoproteins (VLDL), intermediate-density-lipoproteins (IDL) and low-density lipoproteins (LDL) by cholesteryl ester transfer protein (CETP), followed by uptake of these lipoproteins via the LDL receptor (LDLR) in liver cells (hepatocytes). Additionally, HDL can be catabolized in the liver via its uptake as holoparticles through a yet to be identified HDL receptor (HDLR). HDL2 can be remodeled by processes that are catalyzed by hepatic lipase (HL), endothelial lipase (EL) and plasma phospholipid transfer protein (PLTP), resulting in the formation of lipid-poor HDL particles which again interact with ATP-binding cassette transporter A1 (ABCA1) for a next lipidation cycle.
[Source 44 ]Figure 4. Cholesterol transfers between high-density lipoprotein, very-low-density lipoprotein, low-density lipoprotein, and cells.
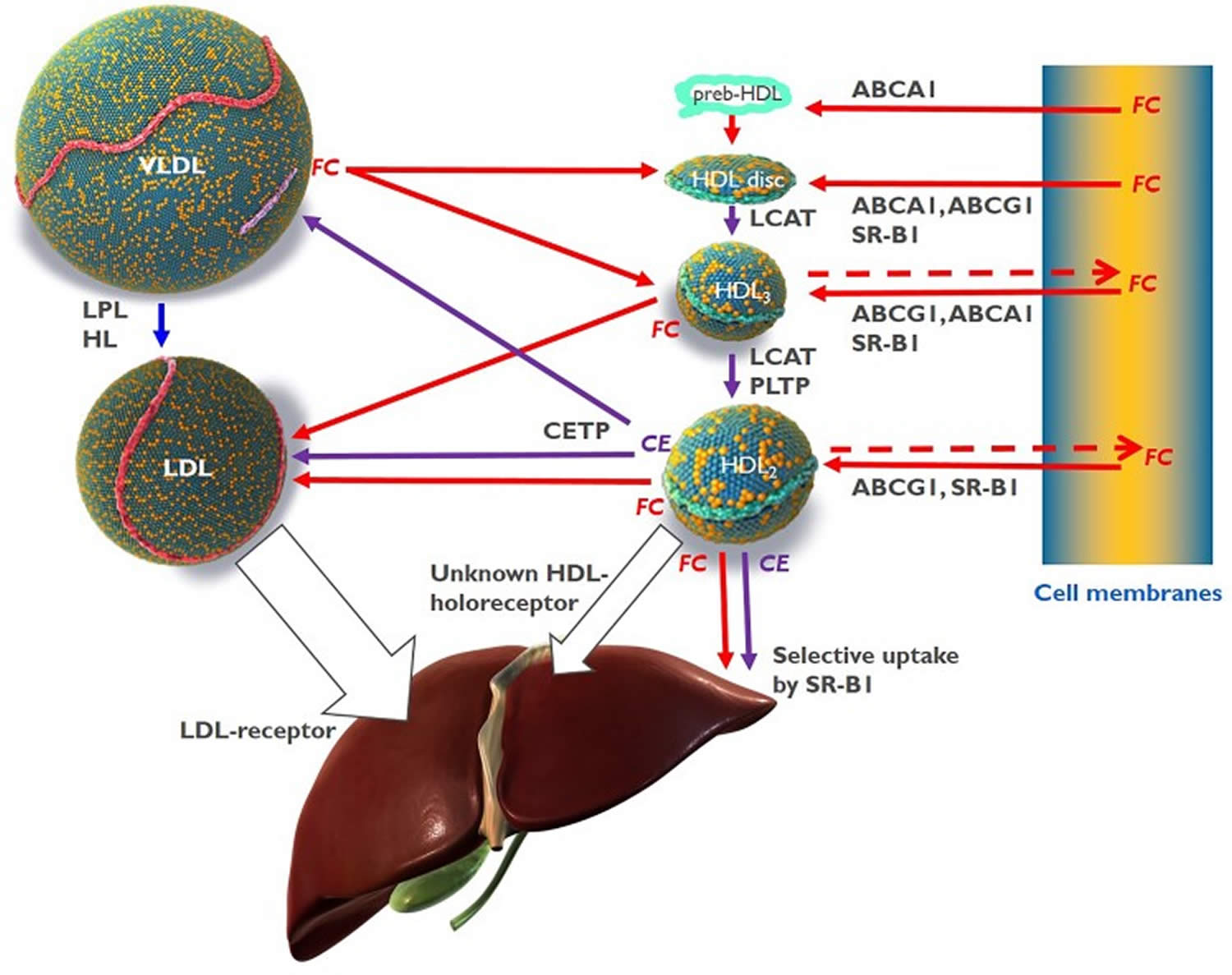
Abbreviations: ABCA1 = ATP-binding cassette transporter A1; ABCG1 = ATP-binding cassette transporter G1; CE = cholesteryl ester; CETP = cholesteryl ester transfer protein; FC = free cholesterol, unesterified cholesterol; HDL = high-density lipoprotein; HL = hepatic lipase; LCAT = lecithin:cholesterol acyltransferase; LDL = low-density lipoprotein; LPL = lipoprotein lipase; PLTP = phospholipid transfer protein; SR-B1 = scavenger receptor B1.
[Source 19 ]Figure 5. High-density lipoprotein levels and risk of all-cause mortality in men and women
What is cholesterol?
Cholesterol is a waxy, fat-like substance that’s found in all the cells in your body. Cholesterol is produced by your liver, adrenal glands, intestines, and in gonads and 20 to 25% of cholesterol comes from your diet (foods you eat) 45. Cholesterol is an essential component of all cell membranes – it helps to maintain structural integrity and fluidity of cell membranes, allowing your cells to change shapes easily without cell walls 46. More than 90% of cellular cholesterol is located at the plasma membrane 47. Your body needs some cholesterol to make hormones such as testosterone and estrogen, vitamin D and the biosynthesis of bile acids in your liver that help you digest foods 48, 49, 50.
Cholesterol travels through your blood on proteins called lipoproteins. One type, LDL (low-density lipoprotein), is sometimes called the “bad” cholesterol. A high LDL level leads to a buildup of cholesterol in your arteries. Another type, HDL (high-density lipoprotein), is sometimes called the “good” cholesterol. HDL carries cholesterol from other parts of your body back to your liver. Then your liver removes the cholesterol from your body.
Types of cholesterol:
- HDL stands for high-density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL. Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, Type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
- LDL stands for low-density lipoprotein or LDL-C (low-density lipoprotein cholesterol). LDL is sometimes called “bad cholesterol” because a high LDL level leads to the buildup of plaque in your arteries. LDL is the most important lipid for predicting your heart disease risk. Low-density lipoprotein (LDL or ‘bad’) cholesterol can join with fats and other substances to build up (also known as plaque) in the inner walls of your arteries, which starts a disease process called atherosclerosis. The arteries can become clogged and narrow, and blood flow is reduced. When plaque builds up in your coronary arteries that supply blood to your heart, you are at greater risk of having a heart attack. Since LDL is the bad kind of cholesterol, a low LDL level is considered good for your heart health. A diet high in saturated and trans fat is unhealthy because it tends to raise LDL cholesterol levels. Your LDL levels may be high if you eat a diet with a lot of saturated fat, cholesterol, or both. Sometimes, an under-active thyroid called hypothyroidism may also increase LDL levels.
- VLDL stands for very low-density lipoprotein or VLDL-C (very low-density lipoprotein cholesterol). Some people also call VLDL a “bad cholesterol” because it too contributes to the buildup of plaque in your arteries. But VLDL and LDL are different; VLDL mainly carries triglycerides and LDL mainly carries cholesterol. VLDL particles are released into the blood by the liver and circulate in the bloodstream, ultimately being converted into LDL as they lose triglyceride, having carried it to other parts of the body. According to the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Guidelines ATP III, there is growing evidence that VLDL plays an important role in atherogenesis, in which plaques form on the interior walls of arteries, narrowing these passageways and restricting blood flow, which can lead to heart disease and increase the risk of stroke. Currently, direct measurement of VLDL cholesterol requires specialized testing. However, since VLDL-C contains most of the circulating triglyceride (if a person is fasting) and since the composition of the different particles is relatively constant, it is possible to estimate the amount of VLDL-C based on the triglyceride value. To estimate VLDL-C, divide the triglyceride value by 5 if the value is in mg/dL or divide by 2.2 if the value is in mmol/L. In most cases, this formula provides a good estimate of VLDL-C. However, this formula becomes less accurate with increased triglyceride levels when, for example, a person has not fasted before having blood drawn. The calculation is not valid when the triglyceride level is greater than 400 mg/dl (4.5 mmol/L) because other lipoproteins are usually present. In this situation, VLDL-C may be measured directly using specialized testing.
- Triglycerides. Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. Triglycerides are fats that provide energy for your muscles. If you eat foods with a lot of saturated fat or carbohydrates, you will raise your triglyceride levels. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels. Elevated triglycerides levels are thought to lead to a greater risk of heart disease, but scientists do not agree that high triglycerides alone are a risk factor for heart disease. Normal triglyceride levels vary by age and sex. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with metabolic syndrome or diabetes also have high triglyceride levels. Extremely high triglyceride levels (more than 1000 mg/dL) can lead to abdominal pain and a life-threatening disorder of the pancreas called pancreatitis. Factors that can contribute to elevated triglyceride levels:
- Overweight or obesity
- Insulin resistance or metabolic syndrome
- Diabetes mellitus, especially with poor glucose control
- Alcohol consumption, especially in excess
- Excess sugar intake, especially from processed foods
- High saturated fat intake
- Hypothyroidism
- Chronic kidney disease
- Physical inactivity
- Pregnancy (especially in the third trimester)
- Inflammatory diseases (such as rheumatoid arthritis, systemic lupus erythematosus
- Some medications may also increase triglycerides.
Your body naturally produces all the LDL (bad) cholesterol it needs. However, the genes you inherit and your lifestyle habits play a major role in your cholesterol levels. The most common cause of high cholesterol is an unhealthy lifestyle. An unhealthy lifestyle makes your body produce more LDL cholesterol than it needs. This can include:
- Unhealthy eating habits or unhealthy diet, such as eating lots of bad fats. One type, saturated fat, is found in some meats, dairy products, chocolate, baked goods, and deep-fried and processed foods. Eating a lot of foods high in saturated fats raises “bad” LDL cholesterol levels. Another type, trans fat, is in some fried and processed foods. Eating these fats can raise your LDL (bad) cholesterol. No more than 10% of your daily calories should come from saturated fats.
- Lack of physical activity, with lots of sitting and little exercise. This lowers your HDL (good) cholesterol.
- Smoking or exposure to tobacco smoke, which lowers HDL cholesterol, especially in women. It also raises your LDL cholesterol.
- Being overweight or obese.
- Stress may raise levels of certain hormones, such as corticosteroids. These can cause your body to make more cholesterol.
- Drinking too much alcohol (more than two drinks a day for men or one drink a day for women) can raise your total cholesterol level.
- Getting little or low-quality sleep has been linked to lower cardiovascular health.
Genetics may also cause people to have high cholesterol. For example, some people inherit genes from their mother, father or even grandparents that cause them to have too much cholesterol. This is called familial hypercholesterolemia (FH). The severity of familial hypercholesterolemia is related to the duration and degree of LDL cholesterol in the blood. Familial hypercholesterolemia is dangerous because it can cause premature atherosclerotic heart disease. If you have a family history of familial hypercholesterolemia or problems related to high cholesterol, get your cholesterol levels checked.
High cholesterol usually causes no signs or symptoms. Cholesterol travels through your blood silently. And it turns into atherosclerotic plaque (hardened deposits) silently. Plaque buildup is like someone tip-toeing on carpet. You might not see or notice its presence for a long time. You may have no symptoms until you have a heart attack or stroke. At that point, the plaque is like high heels on a hardwood floor. And it’s already caused serious damage to your body.
You can live for many years with high cholesterol and not even know it. That’s why it’s essential to get your cholesterol levels checked on a regular basis. If your cholesterol levels are too high (hyperlipidemia), that’s a red flag for you and your doctor. High cholesterol is a major risk factor for heart disease. But catching it early gives you a chance to make changes and get your cholesterol to a healthy level.
You can find out your cholesterol level with a cholesterol or lipid profile blood test. If you are concerned about your cholesterol level, talk to your doctor. You will need to stop eating for 10 to 12 hours before a cholesterol or lipid profile blood test, and the only liquid you may drink is water.
Lifestyle changes such as regular physical activity, losing excess weight, quitting if you smoke and healthy eating are the first line of defense against high cholesterol. Eating lots of fruit and vegetables, whole grains (especially oats), and beans and lentils can help lower your cholesterol. You can also help by losing weight, avoiding foods that are high in saturated fat, quitting smoking and being active. But, if you’ve made these important lifestyle changes and your cholesterol levels remain high, your doctor might recommend medication.
To reduce your risk with high cholesterol, it’s important to:
- Quit cigarette smoking.
- Do regular aerobic exercise.
- Identify and treat high blood pressure.
- Maintain a healthy weight.
- Diagnose and treat diabetes.
- Have a healthy diet.
High cholesterol is one of the major controllable risk factors for coronary heart disease, heart attack and stroke. If you have other risk factors such as smoking, high blood pressure or diabetes, your risk increases even more. The more risk factors you have and the more severe they are, the higher your overall risk.
Remember, making even modest changes now can help to prevent significant medical issues later. Do all you can to reduce your risk for the serious effects of heart attack and stroke.
Figure 6. Cholesterol molecular structure
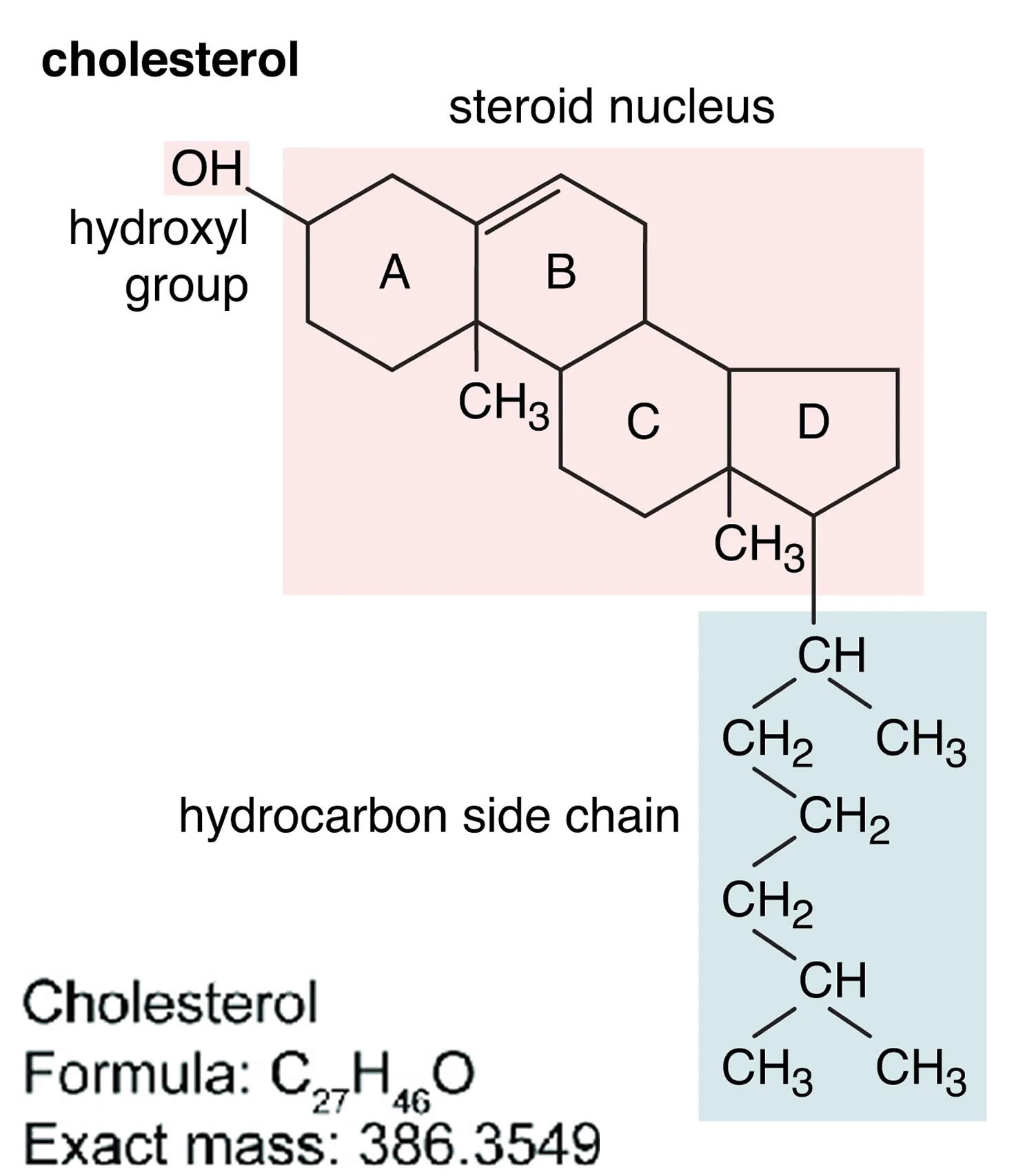
Footnotes: A cholesterol molecule contains three major parts: 1) tetracyclic carbon ring (A, B, C and D) as the core of steroids, 2) polar hydroxyl (OH) group attached to ring A, and 3) short non-polar carbon chain attached to ring D 51, 52. All four rings (A, B, C and D) of the sterol group are in a trans conformation, making cholesterol a planner molecule. The double bond between C5 and C6 helps to keep the rigidity of cholesterol.
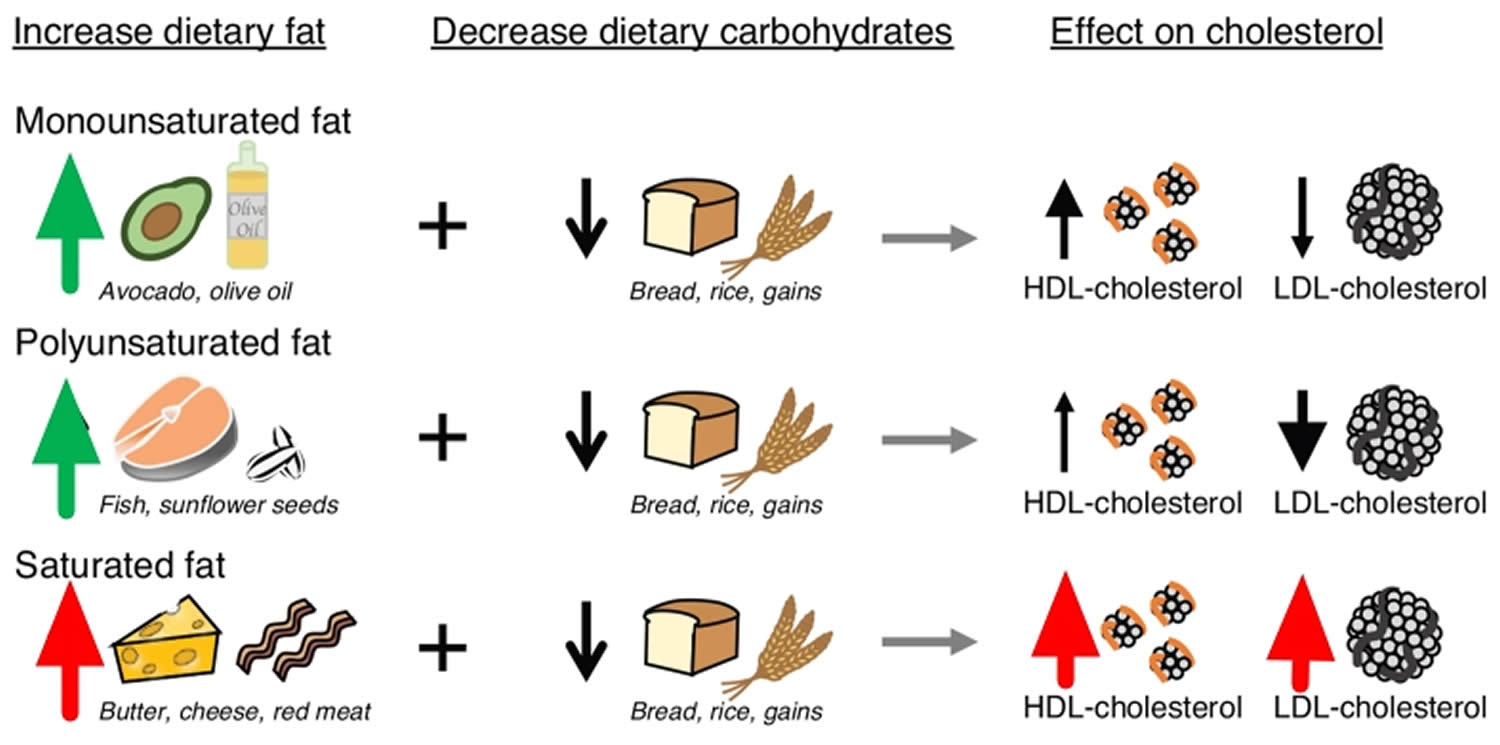
[Source 53 ]Figure 7. Effects of dietary fat and carbohydrate on plasma cholesterol levels
HDL cholesterol function
HDL transports harmful cholesterol from other parts of your body including your arteries back to your liver and HDL also serves many other functions including communication with cells and the inactivation of biohazards like bacterial lipopolysaccharides 19. These functions are exerted by entire HDL particles or distinct proteins or lipids carried by HDL rather than by its cholesterol cargo measured as HDL cholesterol 55, 56. As discussed earlier, high-density lipoproteins contain several other apolipoproteins in addition to apoA-I. The second most abundant HDL apolipoprotein is apoA-II, followed by apoA-IV, the C apolipoproteins, apoE and apoM. These apolipoproteins all contribute to HDL structural stability and, in some cases, HDL function. HDLs also transport a cargo of other proteins that potentially further impact on HDL function.
In addition to the aforementioned proteins that are predominantly associated with lipid metabolism, HDLs contain proteins that promote proteolysis (e.g. alpha-1-antitrypsin), preventing and stopping bleeding a process called hemostasis (alpha-2-HS-glycoprotein), immunity (e.g. the acute phase reactant SAA4), complement activation (e.g. complement C3), and inflammation (e.g. haptoglobin-related protein) 22. As the concentration of most HDL-associated proteins is lower than the plasma concentration of HDL particles, each protein can associate only with specific HDL particle subsets 55. One notable example is the complex consisting of apoA-I, haptoglobin-related protein, and apoL1 by which haptoglobin-related protein provides the binding to Trypanosoma and the internalized apoL1 elicits the lysosomal swelling, ultimately killing Trypanosoma 57. By contrast, the lipid composition of HDL particles is highly dynamic. ABCA1 fluxes glycerophospholipids and cholesterol from cell membranes, especially to lipid-free apoA-I as well as to small, lipid-poor HDL. Lecithin cholesterol acyl transferase (LCAT) generates cholesteryl esters and lysophosphatidylcholines by the transfer of sn-2 fatty acids from phosphatidylcholines to the 3-OH group of cholesterol. Endothelial lipase and hepatic lipase hydrolyse phosphatidylcholines and triglycerides of HDL, respectively, generating free fatty acids, lysophosphatidylcholines, and diacylglycerols, which also are bioactive molecules. Cholesteryl ester transfer protein (CETP) exchanges cholesteryl esters of HDL for triglycerides from apoB-containing lipoproteins and phospholipid transfer protein (PLTP) transfers phospholipids from apoB-containing lipoproteins to HDL as well as between different HDLs 58. In addition, lipids are fluxed between HDL and cells and between HDL and other lipoproteins following concentration gradients or affinity. For example, unesterified cholesterol is readily accepted by HDL from both lipolysed triglyceride-rich lipoproteins (TGRLs) or cell membranes but also transferred from HDL to LDL or cells 59, 60.
In summary, HDLs exert multiple functions that protect the organism from chemical or biological harm or help to repair the tissue damage caused by noxious agents. HDLs do so by three principal mechanisms.
Figure 8. High density lipoprotein cholesterol functions and diseases
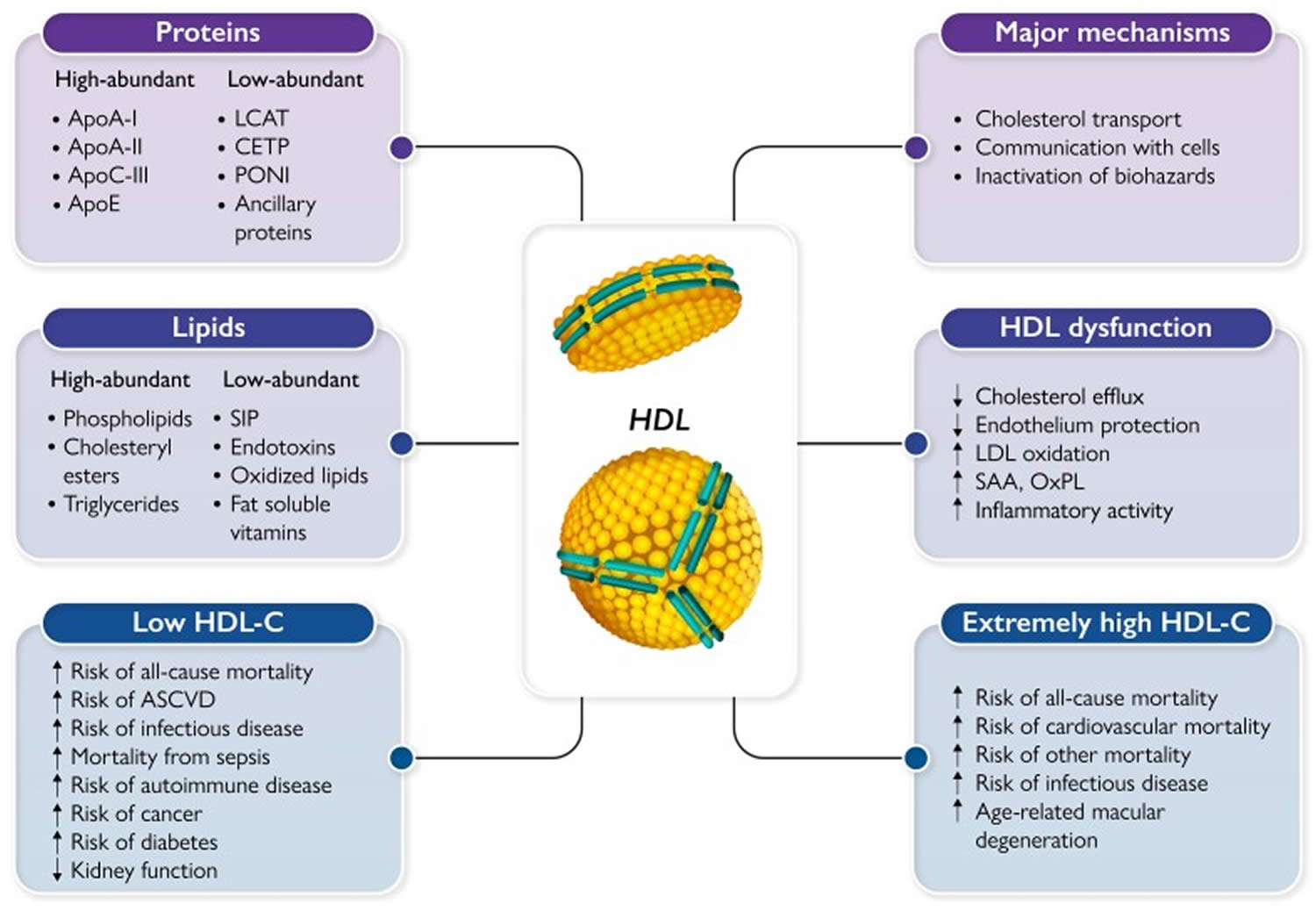
Footnotes: High density lipoproteins (HDL) exert multiple protective activities, essentially by three major mechanisms. HDLs, however, can lose their protective functions and even gain adverse functions in chronic diseases or during infections. U-shaped relationships between HDL-cholesterol (HDL-C) levels and several conditions have been reported, being both low HDL cholesterol and extremely high HDL cholesterol levels associated with an increased risk of several diseases and mortality.
Abbreviations: LCAT = lecithin:cholesterol acyltransferase; CETP = cholesteryl ester transfer protein; PONI = paraoxonase 1; S1P = sphingosine-1-phosphate; ASCVD = atherosclerotic cardiovascular disease; LDL = low-density lipoprotein; SAA = serum amyloid A; OxPL = oxidized phospholipids
[Source 19 ]Cholesterol transport
The most intensively investigated function of HDL is reverse cholesterol transport by carrying harmful cholesterol from other parts of your body including your arteries back to your liver. HDL formation is initiated by the secretion of lipid free apoA-I by the liver comprising about 70% of total apoA-I production 61 and the intestine comprising about 30% of total apoA-I production 62. This lipid free apoA-I interacts with the ATP-binding cassette transporter A1 (ABCA1) on peripheral cells, leading to the transfer of cholesterol and cellular phospholipids from the cell membrane to apoA-I (Figure 3). Through a series of intermediate steps, the lipidated apoA-I is progressively converted into discoidal pre-β-migrating HDL particles that consist of a phospholipid bilayer surrounded by two apoA-I molecules/particle 63. Subsequently, the enzyme lecithin cholesterol acyltransferase (LCAT) mediates the esterification of cholesterol, converting discoidal pre-β-migrating HDL particles into α-migrating, spherical HDL particles with a central core of cholesteryl esters 64 and two molecules of apoA-I. Small spherical HDL subsequently acquire additional free cholesterol that effluxes from peripheral cells via ABCA1 and ABCG1. Esterification of this newly acquired cholesterol by LCAT generates large HDL particles with three or more apoA-I molecules/particle. Furthermore, phospholipid transfer protein (PLTP) plays a vital role in the remodelling of HDL, by transferring phospholipids from chylomicrons and VLDL to HDL 65. This transfer of phospholipids can destabilize HDL, leading to fusion and the formation of larger α-migrating HDL particles 66. Spherical HDL particles can also undergo modification through bi-directional exchange of cholesteryl esters and triglycerides with apoB containing lipoproteins (VLDL and LDL) mediated by cholesteryl ester transfer protein (CETP). As CETP predominately supports the transfer of cholesteryl esters from HDL towards apoB containing lipoproteins in exchange for triglycerides, this process will result in triglyceride–rich HDL 67, 68. The exact mechanism of the HDL-CETP interactions remains part of active research, as some studies suggest that CETP bind to HDL by hydrophobic interaction whereas others suggest it is rather a protein-protein interactions 69. The formation of a hydrophobic channel by SR-B1, allowing cholesterol diffusion from HDL into the plasma membrane, can further remodel HDL 70. Additionally, hepatic lipase can hydrolyse HDL phospholipids and triglycerides, driving the transition of HDL2 into HDL3 particles 71. This remodelling is accompanied by the dissociation of lipid-free or lipid-poor apoA-I, while endothelial lipase remodels HDL without such dissociation 72. In the kidney, this lipid-free apoA-I undergoes glomerular filtration and can subsequently either be degraded, excreted through the urine or partially reabsorbed, thereby regulating the plasma levels of apoA-I and HDL 73, 74.
HDL Antioxidant properties
HDLs reduce oxidative stress in low density lipoproteins (LDLs) and other atherogenic lipoproteins by accepting lipid hydroperoxides and detoxifying them into lipid hydroxides that are cleared from the circulation by the liver 22. Small HDLs inhibit oxidation more effectively than large HDLs 75. This can potentially negate, the reduced cardioprotection that is associated with low plasma HDL levels 22. It also raises the possibility that treatment with drugs that increase the level of large HDLs may not improve the antioxidant properties of HDLs 22.
Paraoxonase1 (PON1) and platelet-activating factor acetyl hydrolase (PAF-AH) contribute to the antioxidant properties of HDLs independent of reducing lipid hydroperoxides to hydroxides 22. Although paraoxonase1 (PON1) knockout mice are atherosclerosis-prone, and overexpression of human PON1 reduces atherosclerosis in mice 76, 77, the mechanism by which PON1 inhibits oxidation, and its impact on atherosclerotic lesion development, is not well understood. The mechanism of the antioxidant properties of platelet-activating factor acetyl hydrolase (PAF-AH) have been elucidated, and include the hydrolysis of oxidised fatty acid constituents in phospholipids. However, the precise contribution of platelet-activating factor acetyl hydrolase (PAF-AH) to the antioxidant properties of HDLs requires further clarification. Interventions that exploit these cardioprotective functions of HDLs have yet to be developed.
HDL Anti-diabetic properties
HDLs and HDL apolipoproteins improve glycemic control in animal models of diabetes by enhancing pancreatic Beta-cell function and survival and improving insulin sensitivity 78. HDLs also inhibit Beta-cell apoptosis and protect Beta-cells from oxidation by low-density lipoproteins (LDLs) 79, 80.
Evidence that the anti-diabetic functions of HDLs are clinically relevant has emerged from a meta-analysis of all cholesteryl transfer protein (CETP) inhibitor trials showing a 12% reduction in incident diabetes 81. A more detailed in analysis of dalcetrapib revealed that the reduced incidence in diabetes may be a consequence of the treatment-related increase in HDL cholesterol but not change in body mass index (BMI) and regression from diabetes to no diabetes 82. These studies provided the first direct evidence that increasing HDL levels may reduce cardiometabolic risk. Identification of specific HDL subpopulations that mediate these effects would enable this approach to be further developed treatments to increasing a specific HDL particle.
HDL Anti-inflammatory properties
Inflammation is a key driver of chronic diseases such as atherosclerotic cardiovascular disease and diabetes as well as infections and malignancies. HDLs directly affect the inflammatory process and HDLs reduce inflammation in multiple cell types, including endothelial cells and macrophages 83, 84, 85. In endothelial cells HDLs inhibit inflammation by reducing activation of nuclear factor-κB (NF-κB) and 3β-hydroxysteroid-Δ24 reductase, by activating the cytoprotective enzyme, heme oxygenase-1 and by inhibiting inflammasome activation 86, 83. HDLs exert these effects by several mechanisms including the interaction of HDL-associated apoM/sphingosine-1-phosphate (S1P) with S1P receptors 87. They also reduce inflammation in monocytes and attenuate the binding of monocytes to adhesion molecules on the surface of activated endothelial cells 87, 88.
Approximately ~90-95% of the apoA-I in plasma is bound to HDL particles, but pro-inflammatory states can cause it to dissociate into the circulation in a lipid-free or lipid-poor form 89. The role of HDLs and apoA-I in macrophage inflammation, a key driver of atherosclerotic lesion progression, has been investigated extensively.8, 10, 19–25, 27 While early studies focused on the anti-inflammatory effects of HDLs 83, 88, 84, 90, 91, 85, 92, more recent studies showing that HDLs and apoA-I can also be pro-inflammatory 90, 93, 94 may be one explanation for the limited success of HDL-raising drugs in reducing atherosclerotic cardiovascular disease. However, the pro-inflammatory effects of HDLs could be beneficial in other diseases, such as sepsis, where enhanced inflammation may promote efficient clearance of bacteria 94. Understanding the mechanistic links between HDLs and their role in inflammation is vital for understanding the prognostic and therapeutic potential of high-density lipoprotein class.
Whether HDLs and apoA-I are pro- or anti-inflammatory depends on several structural or functional features, including HDL composition, macrophage cholesterol content and signalling pathways 84, 90, 93. Macrophages produce pro- and anti-inflammatory cytokines. Production of pro-inflammatory cytokines occurs downstream of Toll-like receptors (TLRs) that are activated by components of viruses or bacteria. The best known examples of this is are lipopolysaccharide (LPS) that activates TLR4, and lipoteichoic acid (LTA) that activates Toll-like receptor 2 (TLR2) 95. While HDLs and apoA-I suppress inflammation by binding directly to and neutralising lipopolysaccharide (LPS) or lipoteichoic acid (LTA), they also affect Toll-like receptor (TLR) activation and downstream signalling pathways directly 95.
Communication with cells
HDLs regulate the differentiation, proliferation, migration, survival, and function of many cell types. HDLs modulate the inflammatory action of innate and adaptive immune cells 96, support the integrity and functionality of endothelial barriers, stimulate angiogenesis 97 and secure energy homeostasis by stimulating insulin synthesis and secretion by pancreatic beta cells as well as glucose uptake by adipocytes and myocytes 78. Principally, these cellular responses result from either altered cholesterol homeostasis due to fluxes of cholesterol between cells and HDL, specific molecular interactions between HDL and cells, or combinations thereof.
First, cholesterol efflux alters the cholesterol content of specific plasma membrane domains, so-called rafts, that are enriched with signalling molecules, resulting in different effects depending on the cell type. Examples are the activation of endothelial nitric oxide synthase (eNOS) by HDL/SR-BI interaction in caveolae of endothelial cells 98 as well as the dampening of toll-like receptor-4 response in monocytes 84 or T-cell receptor signalling in lymphocytes 99; cholesterol efflux also alters the transcription of sterol-regulated genes 100.
Second, the interactions of HDL with SR-BI or apoA-I with ABCA1 induce signal transduction via the recruitment of intracellular proteins, which in turn activate different cellular responses such as eNOS activation in endothelial cells or glucose uptake into myocytes 101, 102.
Third, HDLs transport agonists of specific signalling receptors; the interaction of S1P with S1P receptors activates diverse signalling cascades and results in many protective effects on endothelial functions, including the induction of nitric oxide (NO) production and the maintenance of the endothelial barrier integrity 97, 103. Furthermore, S1P facilitates the trans-endothelial transport of HDL and thereby entry into extravascular tissues and spaces, where HDL exerts its protective activities 104. S1P also modulates inflammatory effects on macrophages and lymphocytes and promotes the survival of hearts and kidneys exposed to hypoxia, ischemia-reperfusion injury, or toxic drugs 103.
Fourth, HDLs deliver cargo into cells either by selective uptake, i.e. independently of the entire particle, or via holoparticle uptake 105. SR-BI mediates the selective uptake not only of lipids but also microRNAs (miR) carried by HDL 106. HDL-holoparticle uptake in the liver plays an important role in the metabolism of HDL 107. In addition, monocyte-derived macrophages and enterocytes also internalize entire HDL particles, but the mechanism or the consequence of this is not understood 108, 109.
In summary, HDLs elicit a plethora of cellular responses by employing several modes of communication. Some mechanisms, for example, S1P receptor activation or cholesterol efflux, lead to many diverse responses in different cell types. Vice versa, identical responses can be evoked by several modes of action.
Inactivation of biohazards
By its amphiphilic structure and its cycling between extravascular and intravascular compartments, HDLs bind potentially toxic substances, such as bacterial lipopolysaccharides, oxidized lipids, as well as some lipophilic xenobiotics 110, 111. In plasma, potentially hazardous molecules are either eliminated by reverse transport to the liver or inactivated directly on the surface of HDLs. The best-investigated example for the latter situation is the hydrolysis of oxidized phospholipids by paraoxonase 1, lipoprotein-associated phospholipase A2, and LCAT 112, 113, 114. HDLs also exert direct antimicrobial effects on viruses and even protozoa 57, 111, 115. At least in vitro, HDL or apoA-I interfere with the entry or fusion of viruses with target cells (Pirillo A, Catapano AL, Norata GD. HDL in infectious diseases and sepsis. Handb Exp Pharmacol. 2015;224:483-508. doi: 10.1007/978-3-319-09665-0_15)). Of note, SR-BI is an entry route of several viruses into cells 116 and this process may be competed by HDLs 117.
Finally, HDLs is enriched with proteases and protease inhibitors which modulate platelet aggregation, coagulation, fibrinolysis, complement activation, and tissue degradation. They help to counteract downstream adverse effects of injuries, infections, and inflammation and support wound healing 118. Of note, functionally related proteins tend to cluster within distinct sub-populations of HDL 33, 34.
Effects of dietary fat on high density lipoprotein
Most studies of diet and HDL have focused on the effect of dietary macronutrients – carbohydrate, fat, and protein – on HDL-cholesterol levels. Dietary fat when it replaces carbohydrate increases HDL-cholesterol
Saturated, monounsaturated, and n−6 polyunsaturated fats have this effect (Fig. (Fig.1),1), saturated more so than monounsaturated or polyunsaturated fat [1,2]. Carbohydrate lowers HDL-cholesterol by about 5 mg/dL per 10 percentage points of total daily calories exchanged with fat [2]. The HDL-cholesterol lowering effect of carbohydrate occurs whether the carbohydrate is refined or whole grain, or low or high glycemic index [3]. Because fat and carbohydrate are macronutrients, supplying energy, another reference point is needed to determine direct effects of increasing dietary fat. Using protein as the reference, dietary fat replacing protein raises HDL-cholesterol even more than fat replacing carbohydrate [4]. Therefore, it is fair to conclude that dietary fat directly increases HDL-cholesterol regardless of whether it replaces carbohydrate or protein. However, the metabolic basis is not well established.
What can you do if your HDL cholesterol is Low?
If your HDL levels is low, you can take several steps to boost your HDL level and reduce your heart disease risk 119:
- Get physically active or exercise – Aerobic exercise for 30 to 60 minutes on most days of the week can help pump up your HDL levels. Some studies suggest that physical activity can raise HDL cholesterol. The American Heart Association recommends three to four 40-minute sessions of moderate- to vigorous-intensity aerobic activity per week for adults trying to lower their LDL cholesterol or blood pressure.
- Eat better fats. The monounsaturated and polyunsaturated fats described above can raise HDL cholesterol levels.
- Cut out trans fats. Not only do they increase LDL cholesterol, they decrease HDL cholesterol too.
- Quit smoking – Tobacco smoke lowers HDL, and quitting can increase HDL levels.
- Keep a healthy weight – Being overweight increases LDL cholesterol and reduces HDL cholesterol levels. Losing even a few pounds will increase your HDL-C and lower your LDL-C and blood pressure. Avoiding obesity besides improving HDL levels, reduces risk for heart disease and multiple other health conditions.
What is LDL cholesterol?
LDL (“bad”) cholesterol can contribute to the formation of plaque buildup in the arteries (atherosclerosis). This is linked to higher risk for heart attack and stroke.
You want your LDL below 70 milligrams per deciliter (mg/dl).
If you have high LDL or total cholesterol, you can lower your risk of heart disease by:
- Stop smoking if you smoke
- Maintaining a healthy weight
- Avoid foods high in saturated fat, dietary cholesterol, and extra calories
- Limiting your alcohol and salt intake
- Exercise for at least 30 minutes on most days
- Managing stress.
High low density lipoprotein (LDL) cholesterol
Anyone can develop high cholesterol. High cholesterol can be caused by many different things; some you can control, and others you can’t.
- Your lifestyle:
- Eating too much saturated fat – this reduces the liver’s ability to remove cholesterol, so it builds up in the blood
- Being physically inactive – being active raises the level of ‘good’ cholesterol and reduces the level of ‘bad’ cholesterol
- Smoking - this can lead to high cholesterol levels, reduce your HDL (good) cholesterol and it causes tar to build up in your arteries, making it easier for cholesterol to stick to your artery walls.
- Your age, biological sex and ethnic background:
- getting older – having higher cholesterol is more likely as we age
- male – males are more likely to have high cholesterol
- ethnic background – if you are from a south Asian background, you are more likely to have high cholesterol.
- Your genes. Genes carry the information that determine your features or characteristics that are passed on to you — or inherited — from your parents.
- Familial hypercholesterolemia (FH), is an inherited condition, meaning you were born with it. It’s often passed down through families in faulty genes and can lead to very high levels of cholesterol, even if you do not have other risk factors.
- Familial combined hyperlipidemia
- Familial dysbetalipoproteinemia
- Familial hypertriglyceridemia
- Lipoprotein-A also called lipoprotein (a), or LP(a), is made in your liver and carries fats around the body. High Lipoprotein-A is a condition that can cause heart problems like heart attack and stroke. This is because Lipoprotein-A is ‘sticky’ and can build up in your arteries. It’s usually an inherited condition but there are other causes.
- Your general health:
- Kidney disease – when your kidneys aren’t working well, it also changes the way your body handles cholesterol, which can lead to high cholesterol
- Liver disease – an important job of the liver is to both produce cholesterol and clear it from the body, but if the liver isn’t working well it struggles to do this, increasing your risk of high cholesterol
- Being overweight, especially with excess fat around your middle
- Type 2 diabetes put you at greater risk of having high cholesterol
- Polycystic ovary syndrome (PCOS)
- Pregnancy and other conditions that increase levels of female hormones
- Sleep apnea
- Having an underactive thyroid (hypothyroidism – when your body doesn’t make enough thyroid hormone)
- Growth hormone deficiency (when not enough of the growth hormone is made).
For people with conditions such as lupus and HIV, the condition itself and the medicine used to treat it may lead to unhealthy cholesterol levels.
Medicines such as certain birth control pills, diuretics (water pills), beta-blockers, and some medicines used to treat depression may also raise cholesterol levels.
Some medicines that you take for other health problems can raise your level of “bad” LDL cholesterol or lower your level of “good” HDL cholesterol, including:
- Arrhythmia medicines, such as amiodarone
- Beta-blockers for relieving angina chest pain or treating high blood pressure
- Chemotherapy medicines used to treat cancer
- Diuretics, such as thiazide, to treat high blood pressure
- Immunosuppressive medicines, such as cyclosporine, to treat inflammatory diseases or to prevent rejection after organ transplant
- Retinoids to treat acne
- Steroids, such as prednisone, to treat inflammatory diseases such as lupus, rheumatoid arthritis, and psoriasis
Risk factors for developing high cholesterol
Factors that can increase your risk of bad cholesterol include:
- Poor diet. Eating saturated fat, found in animal products, and trans fats, found in some commercially baked cookies and crackers and microwave popcorn, can raise your cholesterol level. Foods that are high in cholesterol, such as red meat and full-fat dairy products, will also increase your cholesterol.
- Age. Your cholesterol levels tend to rise as you get older. For instance, as you age, your liver becomes less able to remove LDL cholesterol. Even though it is less common, younger people, including children and teens, can also have high cholesterol.
- Sex. Between ages 20 and 39, men have a greater risk for high total cholesterol than women. A woman’s risk goes up after menopause. Menopause lowers levels of female hormones that may protect against high blood cholesterol. After menopause, women’s levels of total and “bad” LDL cholesterol usually go up, while their levels of “good” HDL cholesterol go down.
- Heredity. High blood cholesterol can run in families.
- Weight. Being overweight or having obesity raises your cholesterol level. Having a body mass index (BMI) of 30 or greater puts you at risk of high cholesterol.
- Race. Certain races may have an increased risk of high cholesterol.
- Overall, non-Hispanic White people are more likely than other groups to have high levels of total cholesterol.
- Asian Americans, including those of Indian, Filipino, Japanese, and Vietnamese descent, are more likely to have high levels of “bad” LDL cholesterol than other groups.
- Hispanic Americans are more likely to have lower levels of “good” HDL cholesterol than other groups.
- African Americans are more likely than other groups to have high levels of “good” HDL cholesterol.
- Lack of exercise. Being physically inactive contributes to overweight and can raise LDL and lower HDL. Exercise helps boost your body’s HDL, or “good,” cholesterol while increasing the size of the particles that make up your LDL, or “bad,” cholesterol, which makes it less harmful.
- Smoking. Cigarette smoking damages the walls of your blood vessels, making them more prone to accumulate fatty deposits. Smoking might also lower your level of HDL, or “good,” cholesterol.
- Diabetes. High blood sugar contributes to higher levels of a dangerous cholesterol called very-low-density lipoprotein (VLDL) and lower HDL cholesterol. High blood sugar also damages the lining of your arteries.
How to lower LDL cholesterol
You can lower your LDL cholesterol level by adopting a heart-healthy lifestyle changes. They include eating a healthy diet, weight management, and regular physical activity.
- Choose heart-healthy foods. The DASH eating plans can help you lower your “bad” LDL cholesterol. These plans encourage:
- Limiting saturated fats found in fatty cuts of meats, dairy products, and desserts
- Eating whole grains, fruits, and vegetables rather than refined carbohydrates such as sweets and other high-sugar foods
- Eating a variety of nuts
- Preparing foods with little or no salt
- Get regular physical activity. Studies have shown that physical activity can lower LDL “bad” cholesterol and triglycerides and raise your “good” HDL cholesterol. For example, resistance training among postmenopausal women may decrease total cholesterol, LDL cholesterol, and triglycerides. Before starting any exercise program, ask your provider what level of physical activity is right for you.
- Aim for a healthy weight. Research has shown that adults with overweight and obesity can lower “bad” LDL cholesterol and raise “good” HDL cholesterol by losing only 3% to 5% of their weight.
- Manage stress. Research has shown that chronic stress can sometimes increase LDL cholesterol levels and decrease HDL cholesterol levels.
- Quit smoking. If you smoke, quit. Smoking can raise your risk of heart disease and heart attack and worsen other heart disease risk factors. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke.
- Get enough good quality sleep. Getting 7 to 9 hours of sleep a day lowers your risk for high “bad” cholesterol (LDL) and total cholesterol.
- Limit alcohol. Visit the National Institute on Alcohol Abuse and Alcoholism for resources on support and treatment to stop drinking.
If your healthy lifestyle changes alone do not lower your cholesterol enough, you may also need to take medicines. There are several types of cholesterol-lowering drugs available, including statins. If you take medicines to lower your cholesterol, you still should continue with the lifestyle changes.
Some people with familial hypercholesterolemia (FH) may receive a treatment called lipoprotein apheresis. This treatment uses a filtering machine to remove LDL cholesterol from the blood. Then the machine returns the rest of the blood back to the person.
Eating a heart-healthy diet
From a dietary standpoint, the best way to lower your cholesterol is reduce your intake of saturated fat, trans fat and cholesterol. The American Heart Association recommends limiting saturated fat to less than 6% of daily calories and minimizing the amount of trans fat you eat.
Reducing these fats means limiting your intake of red meat and dairy products made with whole milk. Choose skim milk, low-fat or fat-free dairy products instead. It also means limiting fried food and cooking with healthy oils, such as vegetable oil.
A heart-healthy diet emphasizes fruits, vegetables, whole grains, poultry, fish, nuts and nontropical vegetable oils, while limiting red and processed meats, sodium and sugar-sweetened foods and beverages.
Many diets fit this general description. For example, the DASH (Dietary Approaches to Stop Hypertension) eating plan promoted by the National Heart, Lung, and Blood Institute as well as diets suggested by the U.S. Department of Agriculture and the American Heart Association are heart-healthy approaches. Such diets can be adapted based on your cultural and food preferences.
Becoming more physically active
A sedentary lifestyle lowers HDL cholesterol. Less HDL means there’s less good cholesterol to remove bad cholesterol from your arteries.
Physical activity is important. At least 150 minutes of moderate-intensity aerobic exercise a week is enough to lower both cholesterol and high blood pressure. And you have lots of options: brisk walking, swimming, bicycling or even yard work can fit the bill.
Quitting smoking
Smoking and vaping lowers HDL cholesterol.
Worse still, when a person with unhealthy cholesterol levels also smokes, risk of coronary heart disease increases more than it otherwise would. Smoking also compounds the risk from other risk factors for heart disease, such as high blood pressure and diabetes.
By quitting, smokers can lower their LDL cholesterol and increase their HDL cholesterol levels. It can also help protect their arteries. Nonsmokers should avoid exposure to secondhand smoke.
Losing weight
Being overweight or obese tends to raise bad cholesterol and lower good cholesterol. But a weight loss of as little as 5% to 10% can help improve cholesterol numbers. Losing even 5 to 10 pounds can help lower cholesterol levels.
Manage stress
Research has shown that chronic stress can sometimes raise your LDL cholesterol and lower your HDL cholesterol. Try to reduce your stress. You can do that by deep breathing and relaxation techniques. Examples include meditation and gentle exercise (such as walking or yoga). Also talking with a friend, family member, or health care professional may be helpful.
Medications for high cholesterol
Your doctor might suggest medication to help keep your cholesterol in the healthy range. The choice of medication or combination of medications depends on various factors, including your personal risk factors, your age, your health and possible drug side effects. Common choices include:
- Statins. Statins block a substance your liver needs to make cholesterol. This causes your liver to remove cholesterol from your blood. Statins can also help your body reabsorb cholesterol from built-up deposits on your artery walls, potentially reversing coronary artery disease. Choices include atorvastatin (Lipitor), fluvastatin (Lescol XL), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor). The common side effects of statins are muscle pains and muscle damage, reversible memory loss and confusion, and elevated blood sugar.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Cholesterol absorption inhibitors. Your small intestine absorbs the cholesterol from your diet and releases it into your bloodstream. The drug ezetimibe (Zetia) helps reduce blood cholesterol by limiting the absorption of dietary cholesterol. Ezetimibe can be used with a statin drug.
- Bempedoic acid. This newer drug works in much the same way as statins but is less likely to cause muscle pain. Adding bempedoic acid (Nexletol) to a maximum statin dosage can help lower LDL significantly. A combination pill containing both bempedoic acid and ezetimibe (Nexlizet) also is available.
- Bile-acid-binding resins. Your liver uses cholesterol to make bile acids, a substance needed for digestion. The medications cholestyramine (Prevalite), colesevelam (Welchol) and colestipol (Colestid) lower cholesterol indirectly by binding to bile acids. This prompts your liver to use excess cholesterol to make more bile acids, which reduces the level of cholesterol in your blood.
- Injectable medications. A newer class of drugs, known as PCSK9 inhibitors, can help the liver absorb more LDL cholesterol — which lowers the amount of cholesterol circulating in your blood. Alirocumab (Praluent) and evolocumab (Repatha) might be used for people who have a genetic condition that causes very high levels of LDL or in people with a history of coronary disease who have intolerance to statins or other cholesterol medications. PCSK9 inhibitors are injected under the skin every few weeks and are expensive.
If you also have high triglycerides, your doctor might prescribe:
- Fibrates. Fibrates mostly lower triglycerides and, to a lesser degree, raise HDL levels. Fibrates are less effective in lowering LDL levels. The medications fenofibrate (Tricor, Fenoglide, others) and gemfibrozil (Lopid) reduce your liver’s production of very-low-density lipoprotein (VLDL) cholesterol and speed the removal of triglycerides from your blood. VLDL cholesterol contains mostly triglycerides. Using fibrates with a statin can increase the risk of statin side effects.
- Nicotinic acid also called niacin or vitamin B3. Niacin is the generic name for nicotinic acid (pyridine-3-carboxylic acid), nicotinamide (niacinamide or pyridine-3-carboxamide), and related derivatives, such as nicotinamide riboside 120. Niacin is a water-soluble B3 vitamin that should be taken only under physician supervision. Niacin limits your liver’s ability to produce LDL and VLDL cholesterol. It improves all lipoproteins—total cholesterol, LDL, triglycerides, and HDL—when taken in doses well abovethe vitamin requirement. But niacin doesn’t provide additional benefits over statins. Niacin has also been linked to liver damage and strokes, so most doctors now recommend it only for people who can’t take statins.
- Omega-3 fatty acid supplements. Omega-3 fatty acid supplements can help lower your triglycerides. They are available by prescription or over-the-counter. If you choose to take over-the-counter supplements, get your doctor’s OK. Omega-3 fatty acid supplements could affect other medications you’re taking.
If you are on such medication, you might need regular cholesterol tests to check that they are working well and that you are taking the right dose. If you decide to take cholesterol medication, your doctor might recommend liver function tests to monitor the medication’s effect on your liver.
Experts from the National Cholesterol Education Program (NCEP) say that more aggressive cholesterol treatment is needed for people at high risk of dying from a heart attack or cardiovascular disease. The basic message of the group’s recommendations is the lower the better when it comes to levels of low-density lipoprotein (LDL) or “bad cholesterol”. The updated recommendations say that almost all high-risk patients with LDL cholesterol levels of 100 mg/dL or higher should begin taking cholesterol-lowering medicine.
Lipoprotein apheresis
Some people with familial hypercholesterolemia may benefit from lipoprotein apheresis to lower their blood cholesterol levels. Lipoprotein apheresis uses a filtering machine to remove unwanted substances from the body. The machine removes “bad” LDL cholesterol from the blood, then returns the remainder of the blood to your body.
Alternative medicine
Few natural products have been proved to reduce cholesterol, but some might be helpful. With your doctor’s OK, consider these cholesterol-lowering supplements and products:
- Barley
- Plant sterols and stanols, found in oral supplements, some fortified orange juices and some margarines, such as Promise Activ
- Blond psyllium, found in seed husk and products such as Metamucil
- Oat bran, found in oatmeal and whole oats
Another popular cholesterol-lowering supplement is red yeast rice. There is evidence that red yeast rice can help lower your LDL cholesterol. Some red yeast rice products contain substances called monacolins, which are produced by the yeast. However, the U.S. Food and Drug Administration (FDA) has said that red yeast rice products that contain monacolin K, a naturally occurring form of the prescription cholesterol-lowering drug lovastatin and can cause the same types of side effects and drug interactions as lovastatin, cannot be sold legally as dietary supplements in the United States. Other red yeast rice products contain little or no monacolin K, and it is not known whether these products have any effect on cholesterol levels. Unfortunately, there is no way to know how much monacolin K is present in most red yeast rice products.
If you buy red yeast rice supplements in the United States, there’s no way to know whether you’re getting enough monacolin K to lower your LDL cholesterol. In other countries, lovastatin in red yeast rice products is potentially dangerous because there’s no way to know how much might be in a particular product or what the quality of the lovastatin is.
- Flaxseed. Studies of flaxseed preparations to lower cholesterol levels report mixed results. A 2009 review of the scientific research of flaxseed for lowering cholesterol found modest improvements in cholesterol, seen more often in postmenopausal women and in people with high initial cholesterol concentrations.
- Garlic. Some evidence indicates that taking garlic supplements can slightly lower blood cholesterol levels. A recent review of the research on garlic supplements concluded that they can lower cholesterol if taken for more than 2 months, but their effect is modest in comparison with the effects of cholesterol-lowering drugs. However, a National Center for Complementary and Integrative Health-funded study on the safety and effectiveness of three garlic preparations (fresh garlic, dried powdered garlic tablets, and aged garlic extract tablets) for lowering blood cholesterol levels found no effect. Although garlic supplements appear to be safe for most adults, they can thin the blood in a manner similar to aspirin, so use caution if you are planning to have surgery or dental work. Garlic supplements have also been found to interfere with the effectiveness of saquinavir, a drug used to treat HIV infection.
- Some soy products can have a small cholesterol-lowering effect. An analysis of data from 35 studies indicated that soy foods were more effective in lowering cholesterol than soy protein supplements and that isoflavones (substances in soy that have a weak estrogenic effect) did not lower cholesterol. The effect of soy is much smaller than that of cholesterol-lowering drugs.
- Limited evidence indicates that green tea may have a cholesterol-lowering effect. The evidence on black tea is less consistent.
- Chromium, vitamin C, artichoke extract, the herb Hibiscus sabdariffa, coenzyme Q10, and selenium have been studied for cholesterol but have not been found to be effective. Research findings don’t show clear evidence regarding the cholesterol-lowering effects of policosanol (derived from sugar cane) and guggulipid (from the mukul mirth tree in western India).
Even if you take cholesterol-lowering supplements, remember the importance of a healthy lifestyle, and take medication to reduce your cholesterol as directed. Tell your doctor which supplements you take.
High cholesterol
High cholesterol also called hypercholesterolemia, hyperlipidemia or lipid disorder (dyslipidemia) is when you have too much “bad cholesterol” [too much non-HDL cholesterol and LDL (bad) cholesterol] in your blood, which can increase your risk of having a heart attack, stroke and other atherosclerotic cardiovascular disease 121. A stroke occurs when a blood clot blocks blood flow to part of your brain. If you have too much cholesterol in your blood, it can combine with other substances in the blood to form plaque. Plaque sticks to the walls of your arteries. This buildup of plaque is known as atherosclerosis. It can lead to coronary artery disease, where your coronary arteries become narrow or even completely blocked, which can cause a heart attack (myocardial infarction). A heart attack occurs when your heart muscle tissue does not receive vital oxygen and nutrients. Atherosclerosis (buildup of plaque in arteries) is the process that causes the artery wall to get thick and stiff. The disease process begins when LDL (“bad” cholesterol) deposits cholesterol in the artery wall. Your body has an immune response to protect itself and sends white blood cells called macrophages to engulf the invading cholesterol in the artery wall. When the macrophages are full of cholesterol, they are called foam cells because of their appearance. As more foam cells collect in the artery wall, a fatty streak develops between the intima and the media. If the process is not stopped, the fatty streak becomes a plaque, which pushes the intima into the lumen, narrowing the blood flow. The plaque develops a fibrous coating on its outer edges. But if cholesterol continues to collect in foam cells inside the plaque, the fibrous outer coating can weaken and eventually rupture. Smaller arteries downstream from the rupture can quickly become blocked. Over time, a clot may develop at the rupture site and completely block the artery.
Evidence shows that the atherosclerotic process begins in childhood and progresses slowly into adulthood. Later in life, this often leads to coronary heart disease, the leading cause of death in the United States.
Cholesterol comes from two sources. Your liver makes all of the cholesterol your body needs to form cell membranes and to make certain hormones. Cholesterol is also found in foods from animal sources, such as egg yolks, meat, and cheese, which is called dietary cholesterol. Although we often blame the cholesterol found in foods that we eat for raising blood cholesterol, the main culprit is actually saturated fat. Foods rich in saturated fat include butter fat in milk products, fat from red meat, and tropical oils such as coconut oil.
There are usually no symptoms of high cholesterol. But if left untreated, it can lead to heart attack and stroke.
High cholesterol is often a hidden risk factor which means it can happen without us knowing until it’s too late. Undiagnosed or untreated high blood cholesterol can lead to serious problems, such as heart attack and stroke. That is why it’s so important to get your cholesterol level checked. Talk to your doctor about your risk and steps you can take to keep your cholesterol levels in a healthy range.
Cholesterol can enter your artery wall, damage its integrity and lead to the formation of atherosclerotic plaque (hardened deposits). This process of plaque buildup is called atherosclerosis. It can lead to serious problems like:
- Coronary artery disease: Blocked blood flow to your heart.
- Peripheral artery disease: Blocked blood flow to your legs and arms.
- Carotid artery disease: Blocked blood flow to your brain.
Cholesterol levels
Your cholesterol levels show how much cholesterol is circulating in your blood. Your blood cholesterol levels tell you how much lipid or fat is in your blood and your cholesterol levels are expressed in milligrams per deciliter (mg/dL).
Total blood or serum cholesterol is a composite of different measurements. Your “total blood cholesterol” is calculated by adding your HDL (“good” cholesterol) and LDL (“bad” cholesterol) cholesterol levels, plus 20% of your triglyceride level.
The formula for calculating your “total blood cholesterol”: Total cholesterol = HDL + LDL + 20% triglycerides.
- “Total cholesterol” is the total amount of cholesterol that’s circulating in your blood. Your “Total cholesterol” should be below 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L.
- Your HDL “good” cholesterol is the one number you want to be high, ideally above 60 mg/dL (1.55 mmol/L) or higher.
- Your LDL “bad” cholesterol should be below 100 mg/dL (less than 2.59 mmol/L).
- Your triglycerides should be below 150 mg/dL (less than 1.70 mmol/L). Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels.
- Talk with your doctor about what your results mean for you and how to manage your cholesterol.
“Normal cholesterol levels” are less important than your overall cardiovascular risk. Like HDL and LDL cholesterol levels, your total blood cholesterol level should be considered in context with your other known risk factors. To determine your cardiovascular risk, your doctor will consider your cholesterol test results in context with your age, sex and family history. Other risk factors, such as smoking, diabetes and high blood pressure, will be considered as well. If your risk remains uncertain, and treatment options are unclear, your doctor may consider other factors and/or request a coronary artery calcium measurement to provide greater insight into your risk and help in decision-making.
In general, you want to have a total cholesterol level below 200 mg/dL or 5.18 mmol/L. Between 200 mg/dL and 239 mg/dL, your cholesterol level is elevated or borderline-high and should be lowered if you can. With a total cholesterol level of 240 mg/dL or above, your cholesterol level is high, and there is a need for action. For example, changing your diet, beginning an exercise program, and taking statins or other cholesterol-lowering medicines are all ways to lower your cholesterol level.
A decision about needing medication for high cholesterol is based on all your risk factors, not just the cholesterol. A cardiovascular risk assessment predicts your risk of heart attack or stroke in the next 10 years. A free online computer programme that predicts it is called QRISK, so you may hear your doctor talk about a ‘QRISK score’. If it suggests a 10 per cent risk or higher, you may be offered dietary advice and drug treatment (usually a statin) to help lower your cholesterol. The treatment is usually long-term. Increasingly, we are looking at an individual’s lifetime risk, rather than just a 10-year risk, and basing the advice on that figure.
Other free online cardiovascular risk assessment tools:
If you already know your cholesterol levels, that will make the free online cardiovascular risk assessment tools more accurate. If you have already developed heart disease, then taking statins has been proven to reduce your risk of a heart event, even if your cholesterol levels aren’t high.
Figure 9. Cholesterol levels
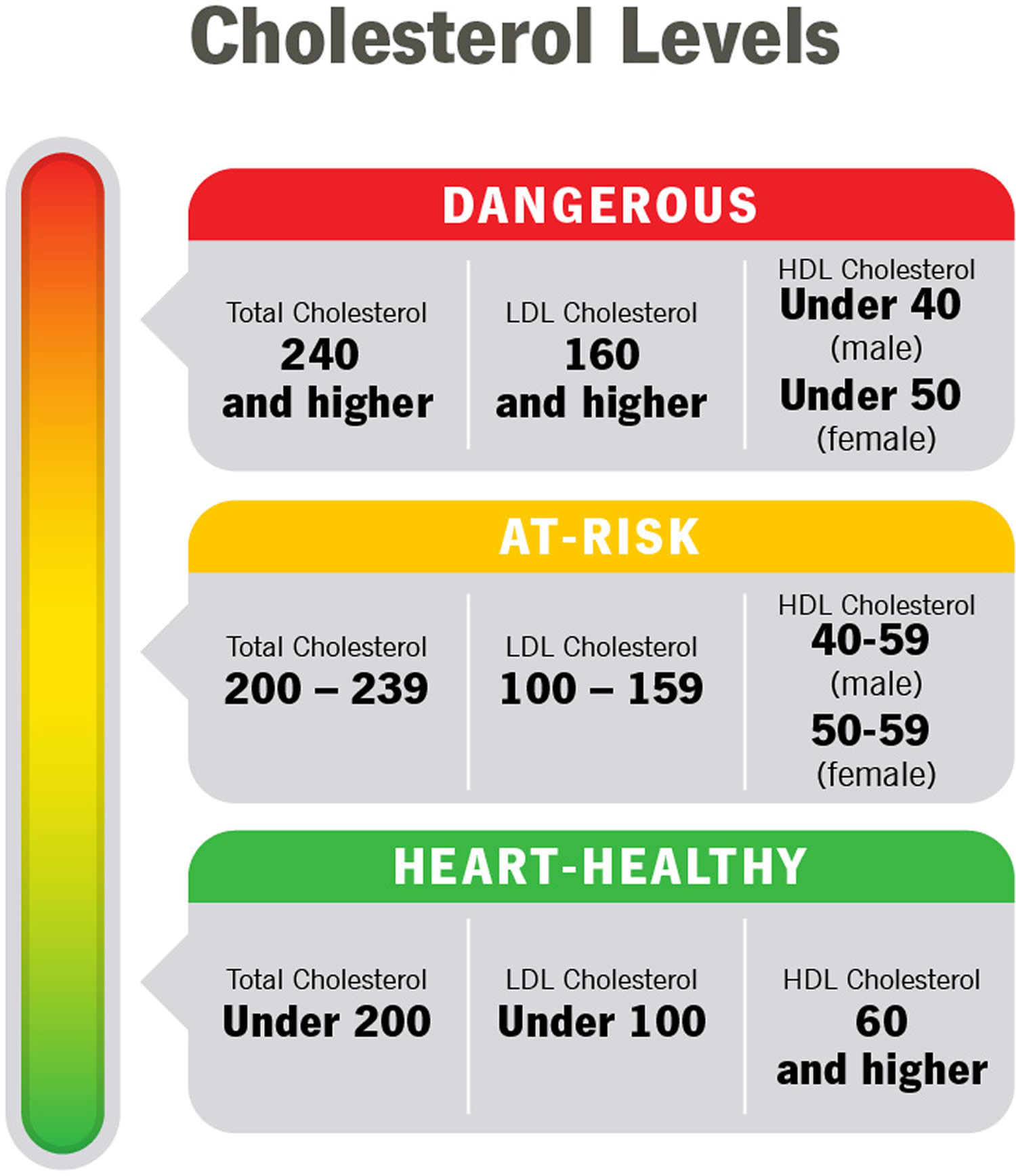
Table 1. Normal Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) | HDL (“good” cholesterol) |
|---|---|---|---|---|
| 19 and younger | Below 170 milligrams per deciliter of blood (mg/dL) | Below 120 mg/dL | Below 110 mg/dL | Above 45 mg/dL |
| 20 and older Male | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 40 mg/dL or higher |
| 20 and older Female | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 50 mg/dL or higher |
Footnotes: As you review your results, remember that you want your LDL to be low and your HDL to be high. Ideally, your HDL should be above 60 mg/dL (1.55 mmol/L). It’s the helpful cholesterol. An HDL above 60 mg/dL (greater than 1.55 mmol/L) offers you protection against heart disease.
Table 2. High Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) |
|---|---|---|---|
| 19 and younger | Borderline high: 170-199 mg/dL High: 200 mg/dL or higher | Borderline high: 120-144 mg/dL High: 145 mg/dL or higher | Borderline high: 110-129 mg/dL High: 130 mg/dL or higher |
| 20 and older | Borderline high: 200-239 mg/dL High: 240 mg/dL or higher | High: 130 mg/dL or higher | Near-optimal: 100-129 mg/dL Borderline high: 130-159 mg/dL High: 160-189 mg/dL Very high: 190 mg/dL or higher |
Footnotes: High cholesterol generally means your total cholesterol is 200 mg/dL (greater than 5.18 mmol/L) or higher. But doctors use additional categories like “borderline high” and “near optimal” to break down your results. If your numbers are close to normal levels, they may be easier to manage through lifestyle and dietary changes.
Table 3. Desirable Cholesterol Levels
| Desirable Cholesterol Levels | |
|---|---|
| Total cholesterol | Less than 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L |
| LDL (“bad” cholesterol) | Less than 100 mg/dL (2.59 mmol/L) |
| HDL (“good” cholesterol) | 60 mg/dL (1.55 mmol/L) or higher |
| Triglycerides | Less than 150 mg/dL (1.70 mmol/L) |
I have high cholesterol when should I be worried?
There’s no level of cholesterol at which you will or won’t have a heart attack. Most doctors don’t base their advice or treatment on cholesterol results alone unless you have familial hypercholesterolemia. That’s why the numbers above only refer to those at high risk. If you’re not at high risk, your doctor looks at your cholesterol level alongside other risk factors such as blood pressure and body mass index (your weight/height ratio), and lifestyle factors such as smoking, diet and physical activity.
What cholesterol level means I need medication?
A decision about needing medication for high cholesterol is based on all your risk factors, not just the cholesterol. A cardiovascular risk assessment predicts your risk of heart attack or stroke in the next 10 years. A free online computer programme that predicts it is called QRISK, so you may hear your doctor talk about a ‘QRISK score’. If it suggests a 10 per cent risk or higher, you may be offered dietary advice and drug treatment (usually a statin) to help lower your cholesterol. The treatment is usually long-term. Increasingly, we are looking at an individual’s lifetime risk, rather than just a 10-year risk, and basing the advice on that figure.
Other free online cardiovascular risk assessment tools:
If you already know your cholesterol levels, that will make the free online cardiovascular risk assessment tools more accurate. If you have already developed heart disease, then taking statins has been proven to reduce your risk of a heart event, even if your cholesterol levels aren’t high.
- Gofman JW, Glazier F, Tamplin A, Strisower B, De Lalla O. Lipoproteins, coronary heart disease, and atherosclerosis. Physiol Rev 1954;34:589–607. doi: 10.1152/physrev.1954.34.3.589[↩]
- Conroy RM, Pyörälä K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetière P, Jousilahti P, Keil U, et al.; SCORE Project Group Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 200324987–1003doi: 10.1016/s0195-668x(03)00114-3[↩]
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 201974e177–e232doi: 10.1016/j.jacc.2019.03.010[↩]
- Gordon DJ, Probstfield JL, Garrison RJ, Neaton JD, Castelli WP, Knoke JD, Jacobs DR Jr, Bangdiwala S, Tyroler HA. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 1989 Jan;79(1):8-15. doi: 10.1161/01.cir.79.1.8[↩]
- Castelli WP, Garrison RJ, Wilson PWF, Abbott RD, Kalousdian S, Kannel WB. Incidence of Coronary Heart Disease and Lipoprotein Cholesterol Levels: The Framingham Study. JAMA. 1986;256(20):2835–2838. doi:10.1001/jama.1986.03380200073024[↩]
- Armitage J, Holmes MV, Preiss D. Cholesteryl Ester Transfer Protein Inhibition for Preventing Cardiovascular Events: JACC Review Topic of the Week. J Am Coll Cardiol. 2019 Feb 5;73(4):477-487. doi: 10.1016/j.jacc.2018.10.072[↩][↩]
- Keene D, Price C, Shun-Shin MJ, Francis DP. Effect on cardiovascular risk of high density lipoprotein targeted drug treatments niacin, fibrates, and CETP inhibitors: meta-analysis of randomised controlled trials including 117,411 patients. BMJ. 2014 Jul 18;349:g4379. doi: 10.1136/bmj.g4379[↩][↩]
- Wu Y, Fan Z, Tian Y, Liu S, Liu S. Relation between high density lipoprotein particles concentration and cardiovascular events: a meta-analysis. Lipids Health Dis. 2018 Jun 19;17(1):142. doi: 10.1186/s12944-018-0732-6[↩][↩]
- Singh K, Chandra A, Sperry T, Joshi PH, Khera A, Virani SS, Ballantyne CM, Otvos JD, Dullaart RPF, Gruppen EG, Connelly MA, Ayers CR, Rohatgi A. Associations Between High-Density Lipoprotein Particles and Ischemic Events by Vascular Domain, Sex, and Ethnicity: A Pooled Cohort Analysis. Circulation. 2020 Aug 18;142(7):657-669. doi: 10.1161/CIRCULATIONAHA.120.045713[↩][↩][↩]
- Zhao Q, Wang J, Miao Z, Zhang NR, Hennessy S, Small DS, Rader DJ. A Mendelian randomization study of the role of lipoprotein subfractions in coronary artery disease. Elife. 2021 Apr 26;10:e58361. doi: 10.7554/eLife.58361[↩][↩][↩]
- Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet. 2012 Aug 11;380(9841):572-80. doi: 10.1016/S0140-6736(12)60312-2. Epub 2012 May 17. Erratum in: Lancet. 2012 Aug 11;380(9841):564.[↩][↩]
- Masana L, Cabré A, Heras M, Amigó N, Correig X, Martínez-Hervás S, Real JT, Ascaso JF, Quesada H, Julve J, Palomer X, Vázquez-Carrera M, Girona J, Plana N, Blanco-Vaca F. Remarkable quantitative and qualitative differences in HDL after niacin or fenofibrate therapy in type 2 diabetic patients. Atherosclerosis. 2015 Feb;238(2):213-9. doi: 10.1016/j.atherosclerosis.2014.12.006[↩]
- Zhong S, Sharp DS, Grove JS, Bruce C, Yano K, Curb JD, Tall AR. Increased coronary heart disease in Japanese-American men with mutation in the cholesteryl ester transfer protein gene despite increased HDL levels. J Clin Invest. 1996 Jun 15;97(12):2917-23. doi: 10.1172/JCI118751[↩][↩]
- Madsen CM, Varbo A, Nordestgaard BG. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: two prospective cohort studies. Eur Heart J. 2017 Aug 21;38(32):2478-2486. doi: 10.1093/eurheartj/ehx163[↩][↩][↩][↩]
- Ko DT, Alter DA, Guo H, Koh M, Lau G, Austin PC, Booth GL, Hogg W, Jackevicius CA, Lee DS, Wijeysundera HC, Wilkins JT, Tu JV. High-Density Lipoprotein Cholesterol and Cause-Specific Mortality in Individuals Without Previous Cardiovascular Conditions: The CANHEART Study. J Am Coll Cardiol. 2016 Nov 8;68(19):2073-2083. doi: 10.1016/j.jacc.2016.08.038[↩][↩]
- Liu C, Zhang Y, Ding D, Li X, Yang Y, Li Q, Zheng Y, Wang D, Ling W. Cholesterol efflux capacity is an independent predictor of all-cause and cardiovascular mortality in patients with coronary artery disease: A prospective cohort study. Atherosclerosis. 2016 Jun;249:116-24. doi: 10.1016/j.atherosclerosis.2015.10.111[↩][↩]
- Hirata A, Sugiyama D, Watanabe M, Tamakoshi A, Iso H, Kotani K, Kiyama M, Yamada M, Ishikawa S, Murakami Y, Miura K, Ueshima H, Okamura T; Evidence for Cardiovascular Prevention from Observational Cohorts in Japan (EPOCH–JAPAN) Research Group. Association of extremely high levels of high-density lipoprotein cholesterol with cardiovascular mortality in a pooled analysis of 9 cohort studies including 43,407 individuals: The EPOCH-JAPAN study. J Clin Lipidol. 2018 May-Jun;12(3):674-684.e5. doi: 10.1016/j.jacl.2018.01.014[↩][↩][↩]
- Pirillo A, Catapano AL, Norata GD. Biological Consequences of Dysfunctional HDL. Curr Med Chem. 2019;26(9):1644-1664. doi: 10.2174/0929867325666180530110543[↩][↩][↩][↩]
- von Eckardstein A, Nordestgaard BG, Remaley AT, Catapano AL. High-density lipoprotein revisited: biological functions and clinical relevance. Eur Heart J. 2023 Apr 21;44(16):1394-1407. doi: 10.1093/eurheartj/ehac605[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Constantinou C, Karavia EA, Xepapadaki E, Petropoulou PI, Papakosta E, Karavyraki M, Zvintzou E, Theodoropoulos V, Filou S, Hatziri A, Kalogeropoulou C, Panayiotakopoulos G, Kypreos KE. Advances in high-density lipoprotein physiology: surprises, overturns, and promises. Am J Physiol Endocrinol Metab. 2016 Jan 1;310(1):E1-E14. doi: 10.1152/ajpendo.00429.2015[↩][↩]
- Karavia EA, Zvintzou E, Petropoulou PI, Xepapadaki E, Constantinou C, Kypreos KE. HDL quality and functionality: what can proteins and genes predict? Expert Rev Cardiovasc Ther. 2014 Apr;12(4):521-32. doi: 10.1586/14779072.2014.896741[↩][↩]
- Rohatgi A, Westerterp M, von Eckardstein A, Remaley A, Rye KA. HDL in the 21st Century: A Multifunctional Roadmap for Future HDL Research. Circulation. 2021 Jun 8;143(23):2293-2309. doi: 10.1161/CIRCULATIONAHA.120.044221[↩][↩][↩][↩][↩][↩][↩]
- Baker HN, Jackson RL, Gotto AM Jr. Isolation and characterization of the cyanogen bromide fragments from the high-density apolipoprotein glutamine I. Biochemistry. 1973 Sep 25;12(20):3866-71. doi: 10.1021/bi00744a011[↩]
- Lux SE, John KM, Brewer HB Jr. Isolation and characterization of apoLp-Gln-II (apoA-II), a plasma high density apolipoprotein containing two identical polypeptide chains. J Biol Chem. 1972 Dec 10;247(23):7510-8[↩]
- Rader DJ. Molecular regulation of HDL metabolism and function: implications for novel therapies. J Clin Invest. 2006 Dec;116(12):3090-100. doi: 10.1172/JCI30163[↩]
- Weng W, Breslow JL. Dramatically decreased high density lipoprotein cholesterol, increased remnant clearance, and insulin hypersensitivity in apolipoprotein A-II knockout mice suggest a complex role for apolipoprotein A-II in atherosclerosis susceptibility. Proc Natl Acad Sci U S A. 1996 Dec 10;93(25):14788-94. doi: 10.1073/pnas.93.25.14788[↩]
- D.J. Rader, H.H. Hobbs. Disorders of Lipoprotein Metabolism (2015).MC GRAW-HILL[↩][↩]
- Shao B, Heinecke JW. Quantifying HDL proteins by mass spectrometry: how many proteins are there and what are their functions? Expert Rev Proteomics. 2018 Jan;15(1):31-40. doi: 10.1080/14789450.2018.1402680[↩][↩]
- Kontush A, Lindahl M, Lhomme M, Calabresi L, Chapman MJ, Davidson WS. Structure of HDL: particle subclasses and molecular components. Handb Exp Pharmacol. 2015;224:3-51. doi: 10.1007/978-3-319-09665-0_1[↩][↩]
- Blanche PJ, Gong EL, Forte TM, Nichols AV. Characterization of human high-density lipoproteins by gradient gel electrophoresis. Biochim Biophys Acta. 1981 Sep 24;665(3):408-19. doi: 10.1016/0005-2760(81)90253-8[↩]
- Kunitake ST, La Sala KJ, Kane JP. Apolipoprotein A-I-containing lipoproteins with pre-beta electrophoretic mobility. J Lipid Res. 1985 May;26(5):549-55.[↩]
- Rosenson RS, Brewer HB Jr, Chapman MJ, Fazio S, Hussain MM, Kontush A, Krauss RM, Otvos JD, Remaley AT, Schaefer EJ. HDL measures, particle heterogeneity, proposed nomenclature, and relation to atherosclerotic cardiovascular events. Clin Chem. 2011 Mar;57(3):392-410. doi: 10.1373/clinchem.2010.155333[↩][↩]
- Davidson WS, Shah AS, Sexmith H, Gordon SM. The HDL Proteome Watch: Compilation of studies leads to new insights on HDL function. Biochim Biophys Acta Mol Cell Biol Lipids. 2022 Feb;1867(2):159072. doi: 10.1016/j.bbalip.2021.159072[↩][↩]
- Goetze S, Frey K, Rohrer L, Radosavljevic S, Krützfeldt J, Landmesser U, Bueter M, Pedrioli PGA, von Eckardstein A, Wollscheid B. Reproducible Determination of High-Density Lipoprotein Proteotypes. J Proteome Res. 2021 Nov 5;20(11):4974-4984. doi: 10.1021/acs.jproteome.1c00429[↩][↩]
- Sacks FM, Liang L, Furtado JD, Cai T, Davidson WS, He Z, McClelland RL, Rimm EB, Jensen MK. Protein-Defined Subspecies of HDLs (High-Density Lipoproteins) and Differential Risk of Coronary Heart Disease in 4 Prospective Studies. Arterioscler Thromb Vasc Biol. 2020 Nov;40(11):2714-2727. doi: 10.1161/ATVBAHA.120.314609[↩]
- Karathanasis SK, Freeman LA, Gordon SM, Remaley AT. The Changing Face of HDL and the Best Way to Measure It. Clin Chem. 2017 Jan;63(1):196-210. doi: 10.1373/clinchem.2016.257725[↩]
- Langsted A, Jensen AMR, Varbo A, Nordestgaard BG. Low High-Density Lipoprotein Cholesterol to Monitor Long-Term Average Increased Triglycerides. J Clin Endocrinol Metab. 2020 Apr 1;105(4):dgz265. doi: 10.1210/clinem/dgz265[↩]
- Centers for Heart Disease and Stroke Prevention. State Heart Disease and Stroke Prevention Programs Address High Blood Cholesterol. https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_state_cholesterol.htm[↩]
- Madsen CM, Varbo A, Nordestgaard BG. Low HDL Cholesterol and High Risk of Autoimmune Disease: Two Population-Based Cohort Studies Including 117341 Individuals. Clin Chem. 2019 May;65(5):644-652. doi: 10.1373/clinchem.2018.299636[↩]
- Madsen CM, Varbo A, Nordestgaard BG. Novel Insights From Human Studies on the Role of High-Density Lipoprotein in Mortality and Noncardiovascular Disease. Arterioscler Thromb Vasc Biol. 2021 Jan;41(1):128-140. doi: 10.1161/ATVBAHA.120.314050[↩][↩]
- Pedersen KM, Çolak Y, Bojesen SE, Nordestgaard BG. Low high-density lipoprotein and increased risk of several cancers: 2 population-based cohort studies including 116,728 individuals. J Hematol Oncol. 2020 Sep 30;13(1):129. doi: 10.1186/s13045-020-00963-6[↩][↩]
- Pirro M, Ricciuti B, Rader DJ, Catapano AL, Sahebkar A, Banach M. High density lipoprotein cholesterol and cancer: Marker or causative? Prog Lipid Res. 2018 Jul;71:54-69. doi: 10.1016/j.plipres.2018.06.001[↩]
- Chandler PD, Song Y, Lin J, Zhang S, Sesso HD, Mora S, Giovannucci EL, Rexrode KE, Moorthy MV, Li C, Ridker PM, Lee IM, Manson JE, Buring JE, Wang L. Lipid biomarkers and long-term risk of cancer in the Women’s Health Study. Am J Clin Nutr. 2016 Jun;103(6):1397-407. doi: 10.3945/ajcn.115.124321[↩]
- Nazir S, Jankowski V, Bender G, Zewinger S, Rye KA, van der Vorst EPC. Interaction between high-density lipoproteins and inflammation: Function matters more than concentration! Adv Drug Deliv Rev. 2020;159:94-119. doi: 10.1016/j.addr.2020.10.006[↩][↩]
- Norum KR, Berg T, Helgerud P, Drevon CA. Transport of cholesterol. Physiol Rev. 1983 Oct;63(4):1343-419. https://doi.org/10.1152/physrev.1983.63.4.1343[↩]
- Maekawa M, Fairn GD. Complementary probes reveal that phosphatidylserine is required for the proper transbilayer distribution of cholesterol. J Cell Sci. 2015;128:1422–33. doi: 10.1242/jcs.164715[↩]
- Goluszko P, Nowicki B. Membrane cholesterol: a crucial molecule affecting interactions of microbial pathogens with mammalian cells. Infect Immun. 2005;73:7791–6. doi: 10.1128/IAI.73.12.7791-7796.2005[↩]
- Mauvais-Jarvis F, editor. Sex and gender factors affecting metabolic homeostasis, diabetes and obesity. Vol. 1043. Cham: Springer International Publishing; 2017.[↩]
- Faridi KF, Lupton JR, Martin SS, Banach M, Quispe R, Kulkarni K, et al. Vitamin D deficiency and non-lipid biomarkers of cardiovascular risk. Arch Med Sci. 2017;13:732–7. doi: 10.5114/aoms.2017.68237[↩]
- Boyer JL. Bile formation and secretion. Compr Physiol. 2013 Jul;3(3):1035-78. doi: 10.1002/cphy.c120027[↩]
- Zhou Y, Briand V, Sharma N, Ahn S, Kasi R. Polymers comprising cholesterol: synthesis, self-assembly, and applications. Materials (Basel) 2009;2:636–60. doi: 10.3390/ma2020636[↩]
- Song Y, Kenworthy AK, Sanders CR. Cholesterol as a co-solvent and a ligand for membrane proteins. Protein Sci. 2014;23:1–22. doi: 10.1002/pro.2385[↩]
- Li LH, Dutkiewicz EP, Huang YC, Zhou HB, Hsu CC. Analytical methods for cholesterol quantification. J Food Drug Anal. 2019 Apr;27(2):375-386. doi: 10.1016/j.jfda.2018.09.001[↩]
- Sacks FM, Andraski AB. Dietary fat and carbohydrate affect the metabolism of protein-based high-density lipoprotein subspecies. Curr Opin Lipidol. 2022 Feb 1;33(1):1-15. doi: 10.1097/MOL.0000000000000809[↩]
- Furtado JD, Yamamoto R, Melchior JT, Andraski AB, Gamez-Guerrero M, Mulcahy P, He Z, Cai T, Davidson WS, Sacks FM. Distinct Proteomic Signatures in 16 HDL (High-Density Lipoprotein) Subspecies. Arterioscler Thromb Vasc Biol. 2018 Dec;38(12):2827-2842. doi: 10.1161/ATVBAHA.118.311607[↩][↩]
- Mendivil CO, Furtado J, Morton AM, Wang L, Sacks FM. Novel Pathways of Apolipoprotein A-I Metabolism in High-Density Lipoprotein of Different Sizes in Humans. Arterioscler Thromb Vasc Biol. 2016 Jan;36(1):156-65. doi: 10.1161/ATVBAHA.115.306138[↩]
- Wheeler RJ. The trypanolytic factor-mechanism, impacts and applications. Trends Parasitol. 2010 Sep;26(9):457-64. doi: 10.1016/j.pt.2010.05.005[↩][↩]
- Zannis VI, Fotakis P, Koukos G, Kardassis D, Ehnholm C, Jauhiainen M, Chroni A. HDL biogenesis, remodeling, and catabolism. Handb Exp Pharmacol. 2015;224:53-111. doi: 10.1007/978-3-319-09665-0_2[↩]
- Cedó L, Metso J, Santos D, García-León A, Plana N, Sabate-Soler S, Rotllan N, Rivas-Urbina A, Méndez-Lara KA, Tondo M, Girona J, Julve J, Pallarès V, Benitez-Amaro A, Llorente-Cortes V, Pérez A, Gómez-Coronado D, Ruotsalainen AK, Levonen AL, Sanchez-Quesada JL, Masana L, Kovanen PT, Jauhiainen M, Lee-Rueckert M, Blanco-Vaca F, Escolà-Gil JC. LDL Receptor Regulates the Reverse Transport of Macrophage-Derived Unesterified Cholesterol via Concerted Action of the HDL-LDL Axis: Insight From Mouse Models. Circ Res. 2020 Aug 28;127(6):778-792. doi: 10.1161/CIRCRESAHA.119.316424[↩]
- Pownall HJ, Rosales C, Gillard BK, Gotto AM Jr. High-density lipoproteins, reverse cholesterol transport and atherogenesis. Nat Rev Cardiol. 2021 Oct;18(10):712-723. doi: 10.1038/s41569-021-00538-z[↩]
- Timmins JM, Lee JY, Boudyguina E, Kluckman KD, Brunham LR, Mulya A, Gebre AK, Coutinho JM, Colvin PL, Smith TL, Hayden MR, Maeda N, Parks JS. Targeted inactivation of hepatic Abca1 causes profound hypoalphalipoproteinemia and kidney hypercatabolism of apoA-I. J Clin Invest. 2005 May;115(5):1333-42. doi: 10.1172/JCI23915[↩]
- Brunham LR, Kruit JK, Iqbal J, Fievet C, Timmins JM, Pape TD, Coburn BA, Bissada N, Staels B, Groen AK, Hussain MM, Parks JS, Kuipers F, Hayden MR. Intestinal ABCA1 directly contributes to HDL biogenesis in vivo. J Clin Invest. 2006 Apr;116(4):1052-62. doi: 10.1172/JCI27352[↩]
- Favari E, Chroni A, Tietge UJ, Zanotti I, Escolà-Gil JC, Bernini F. Cholesterol efflux and reverse cholesterol transport. Handb Exp Pharmacol. 2015;224:181-206. doi: 10.1007/978-3-319-09665-0_4[↩]
- Zannis VI, Chroni A, Krieger M. Role of apoA-I, ABCA1, LCAT, and SR-BI in the biogenesis of HDL. J Mol Med (Berl). 2006 Apr;84(4):276-94. doi: 10.1007/s00109-005-0030-4[↩]
- Masson D, Jiang XC, Lagrost L, Tall AR. The role of plasma lipid transfer proteins in lipoprotein metabolism and atherogenesis. J Lipid Res. 2009 Apr;50 Suppl(Suppl):S201-6. doi: 10.1194/jlr.R800061-JLR200[↩]
- Settasatian N, Duong M, Curtiss LK, Ehnholm C, Jauhiainen M, Huuskonen J, Rye KA. The mechanism of the remodeling of high density lipoproteins by phospholipid transfer protein. J Biol Chem. 2001 Jul 20;276(29):26898-905. doi: 10.1074/jbc.M010708200[↩]
- Camont L, Chapman MJ, Kontush A. Biological activities of HDL subpopulations and their relevance to cardiovascular disease. Trends Mol Med. 2011 Oct;17(10):594-603. doi: 10.1016/j.molmed.2011.05.013[↩]
- Pirillo A, Norata GD, Catapano AL. High-density lipoprotein subfractions–what the clinicians need to know. Cardiology. 2013;124(2):116-25. doi: 10.1159/000346463[↩]
- Zhang M, Charles R, Tong H, Zhang L, Patel M, Wang F, Rames MJ, Ren A, Rye KA, Qiu X, Johns DG, Charles MA, Ren G. HDL surface lipids mediate CETP binding as revealed by electron microscopy and molecular dynamics simulation. Sci Rep. 2015 Mar 4;5:8741. doi: 10.1038/srep08741[↩]
- Rodrigueza WV, Thuahnai ST, Temel RE, Lund-Katz S, Phillips MC, Williams DL. Mechanism of scavenger receptor class B type I-mediated selective uptake of cholesteryl esters from high density lipoprotein to adrenal cells. J Biol Chem. 1999 Jul 16;274(29):20344-50. doi: 10.1074/jbc.274.29.20344[↩]
- von Eckardstein A, Nofer JR, Assmann G. High density lipoproteins and arteriosclerosis. Role of cholesterol efflux and reverse cholesterol transport. Arterioscler Thromb Vasc Biol. 2001 Jan;21(1):13-27. doi: 10.1161/01.atv.21.1.13[↩]
- Jahangiri A, Rader DJ, Marchadier D, Curtiss LK, Bonnet DJ, Rye KA. Evidence that endothelial lipase remodels high density lipoproteins without mediating the dissociation of apolipoprotein A-I. J Lipid Res. 2005 May;46(5):896-903. doi: 10.1194/jlr.M400212-JLR200[↩]
- Hammad SM, Stefansson S, Twal WO, Drake CJ, Fleming P, Remaley A, Brewer HB Jr, Argraves WS. Cubilin, the endocytic receptor for intrinsic factor-vitamin B(12) complex, mediates high-density lipoprotein holoparticle endocytosis. Proc Natl Acad Sci U S A. 1999 Aug 31;96(18):10158-63. doi: 10.1073/pnas.96.18.10158[↩]
- Yang H, Fogo AB, Kon V. Kidneys: key modulators of high-density lipoprotein levels and function. Curr Opin Nephrol Hypertens. 2016 May;25(3):174-9. doi: 10.1097/MNH.0000000000000217[↩]
- Kontush A, Chantepie S, Chapman MJ. Small, dense HDL particles exert potent protection of atherogenic LDL against oxidative stress. Arterioscler Thromb Vasc Biol. 2003 Oct 1;23(10):1881-8. doi: 10.1161/01.ATV.0000091338.93223.E8[↩]
- Shih DM, Gu L, Xia YR, Navab M, Li WF, Hama S, Castellani LW, Furlong CE, Costa LG, Fogelman AM, Lusis AJ. Mice lacking serum paraoxonase are susceptible to organophosphate toxicity and atherosclerosis. Nature. 1998 Jul 16;394(6690):284-7. doi: 10.1038/28406[↩]
- Tward A, Xia YR, Wang XP, Shi YS, Park C, Castellani LW, Lusis AJ, Shih DM. Decreased atherosclerotic lesion formation in human serum paraoxonase transgenic mice. Circulation. 2002 Jul 23;106(4):484-90. doi: 10.1161/01.cir.0000023623.87083.4f[↩]
- Manandhar B, Cochran BJ, Rye KA. Role of High-Density Lipoproteins in Cholesterol Homeostasis and Glycemic Control. J Am Heart Assoc. 2020 Jan 7;9(1):e013531. doi: 10.1161/JAHA.119.013531[↩][↩]
- Yalcinkaya M, Kerksiek A, Gebert K, Annema W, Sibler R, Radosavljevic S, Lütjohann D, Rohrer L, von Eckardstein A. HDL inhibits endoplasmic reticulum stress-induced apoptosis of pancreatic β-cells in vitro by activation of Smoothened. J Lipid Res. 2020 Apr;61(4):492-504. doi: 10.1194/jlr.RA119000509[↩]
- Abderrahmani A, Niederhauser G, Favre D, Abdelli S, Ferdaoussi M, Yang JY, Regazzi R, Widmann C, Waeber G. Human high-density lipoprotein particles prevent activation of the JNK pathway induced by human oxidised low-density lipoprotein particles in pancreatic beta cells. Diabetologia. 2007 Jun;50(6):1304-14. doi: 10.1007/s00125-007-0642-z[↩]
- Masson W, Lobo M, Siniawski D, Huerín M, Molinero G, Valéro R, Nogueira JP. Therapy with cholesteryl ester transfer protein (CETP) inhibitors and diabetes risk. Diabetes Metab. 2018 Dec;44(6):508-513. doi: 10.1016/j.diabet.2018.02.005[↩]
- Schwartz GG, Leiter LA, Ballantyne CM, Barter PJ, Black DM, Kallend D, Laghrissi-Thode F, Leitersdorf E, McMurray JJV, Nicholls SJ, Olsson AG, Preiss D, Shah PK, Tardif JC, Kittelson J. Dalcetrapib Reduces Risk of New-Onset Diabetes in Patients With Coronary Heart Disease. Diabetes Care. 2020 May;43(5):1077-1084. doi: 10.2337/dc19-2204[↩]
- Thacker SG, Zarzour A, Chen Y, Alcicek MS, Freeman LA, Sviridov DO, Demosky SJ Jr, Remaley AT. High-density lipoprotein reduces inflammation from cholesterol crystals by inhibiting inflammasome activation. Immunology. 2016 Nov;149(3):306-319. doi: 10.1111/imm.12638[↩][↩][↩]
- De Nardo D, Labzin LI, Kono H, Seki R, Schmidt SV, Beyer M, Xu D, Zimmer S, Lahrmann C, Schildberg FA, Vogelhuber J, Kraut M, Ulas T, Kerksiek A, Krebs W, Bode N, Grebe A, Fitzgerald ML, Hernandez NJ, Williams BR, Knolle P, Kneilling M, Röcken M, Lütjohann D, Wright SD, Schultze JL, Latz E. High-density lipoprotein mediates anti-inflammatory reprogramming of macrophages via the transcriptional regulator ATF3. Nat Immunol. 2014 Feb;15(2):152-60. doi: 10.1038/ni.2784[↩][↩][↩][↩]
- Suzuki M, Pritchard DK, Becker L, Hoofnagle AN, Tanimura N, Bammler TK, Beyer RP, Bumgarner R, Vaisar T, de Beer MC, de Beer FC, Miyake K, Oram JF, Heinecke JW. High-density lipoprotein suppresses the type I interferon response, a family of potent antiviral immunoregulators, in macrophages challenged with lipopolysaccharide. Circulation. 2010 Nov 9;122(19):1919-27. doi: 10.1161/CIRCULATIONAHA.110.961193[↩][↩]
- Wu BJ, Chen K, Shrestha S, Ong KL, Barter PJ, Rye KA. High-density lipoproteins inhibit vascular endothelial inflammation by increasing 3β-hydroxysteroid-Δ24 reductase expression and inducing heme oxygenase-1. Circ Res. 2013 Jan 18;112(2):278-88. doi: 10.1161/CIRCRESAHA.111.300104[↩]
- Ruiz M, Frej C, Holmér A, Guo LJ, Tran S, Dahlbäck B. High-Density Lipoprotein-Associated Apolipoprotein M Limits Endothelial Inflammation by Delivering Sphingosine-1-Phosphate to the Sphingosine-1-Phosphate Receptor 1. Arterioscler Thromb Vasc Biol. 2017 Jan;37(1):118-129. doi: 10.1161/ATVBAHA.116.308435[↩][↩]
- Murphy AJ, Woollard KJ, Hoang A, Mukhamedova N, Stirzaker RA, McCormick SP, Remaley AT, Sviridov D, Chin-Dusting J. High-density lipoprotein reduces the human monocyte inflammatory response. Arterioscler Thromb Vasc Biol. 2008 Nov;28(11):2071-7. doi: 10.1161/ATVBAHA.108.168690[↩][↩]
- Jahangiri A, de Beer MC, Noffsinger V, Tannock LR, Ramaiah C, Webb NR, van der Westhuyzen DR, de Beer FC. HDL remodeling during the acute phase response. Arterioscler Thromb Vasc Biol. 2009 Feb;29(2):261-7. doi: 10.1161/ATVBAHA.108.178681[↩]
- Fotakis P, Kothari V, Thomas DG, Westerterp M, Molusky MM, Altin E, Abramowicz S, Wang N, He Y, Heinecke JW, Bornfeldt KE, Tall AR. Anti-Inflammatory Effects of HDL (High-Density Lipoprotein) in Macrophages Predominate Over Proinflammatory Effects in Atherosclerotic Plaques. Arterioscler Thromb Vasc Biol. 2019 Dec;39(12):e253-e272. doi: 10.1161/ATVBAHA.119.313253[↩][↩][↩]
- Yvan-Charvet L, Kling J, Pagler T, Li H, Hubbard B, Fisher T, Sparrow CP, Taggart AK, Tall AR. Cholesterol efflux potential and antiinflammatory properties of high-density lipoprotein after treatment with niacin or anacetrapib. Arterioscler Thromb Vasc Biol. 2010 Jul;30(7):1430-8. doi: 10.1161/ATVBAHA.110.207142[↩]
- Westerterp M, Fotakis P, Ouimet M, Bochem AE, Zhang H, Molusky MM, Wang W, Abramowicz S, la Bastide-van Gemert S, Wang N, Welch CL, Reilly MP, Stroes ES, Moore KJ, Tall AR. Cholesterol Efflux Pathways Suppress Inflammasome Activation, NETosis, and Atherogenesis. Circulation. 2018 Aug 28;138(9):898-912. doi: 10.1161/CIRCULATIONAHA.117.032636[↩]
- Smoak KA, Aloor JJ, Madenspacher J, Merrick BA, Collins JB, Zhu X, Cavigiolio G, Oda MN, Parks JS, Fessler MB. Myeloid differentiation primary response protein 88 couples reverse cholesterol transport to inflammation. Cell Metab. 2010 Jun 9;11(6):493-502. doi: 10.1016/j.cmet.2010.04.006[↩][↩]
- van der Vorst EPC, Theodorou K, Wu Y, Hoeksema MA, Goossens P, Bursill CA, Aliyev T, Huitema LFA, Tas SW, Wolfs IMJ, Kuijpers MJE, Gijbels MJ, Schalkwijk CG, Koonen DPY, Abdollahi-Roodsaz S, McDaniels K, Wang CC, Leitges M, Lawrence T, Plat J, Van Eck M, Rye KA, Touqui L, de Winther MPJ, Biessen EAL, Donners MMPC. High-Density Lipoproteins Exert Pro-inflammatory Effects on Macrophages via Passive Cholesterol Depletion and PKC-NF-κB/STAT1-IRF1 Signaling. Cell Metab. 2017 Jan 10;25(1):197-207. doi: 10.1016/j.cmet.2016.10.013[↩][↩]
- Morin EE, Guo L, Schwendeman A, Li XA. HDL in sepsis – risk factor and therapeutic approach. Front Pharmacol. 2015 Oct 23;6:244. doi: 10.3389/fphar.2015.00244[↩][↩]
- Bonacina F, Pirillo A, Catapano AL, Norata GD. HDL in Immune-Inflammatory Responses: Implications beyond Cardiovascular Diseases. Cells. 2021 Apr 29;10(5):1061. doi: 10.3390/cells10051061[↩]
- Robert J, Osto E, von Eckardstein A. The Endothelium Is Both a Target and a Barrier of HDL’s Protective Functions. Cells. 2021 Apr 28;10(5):1041. doi: 10.3390/cells10051041[↩][↩]
- Yuhanna IS, Zhu Y, Cox BE, Hahner LD, Osborne-Lawrence S, Lu P, Marcel YL, Anderson RG, Mendelsohn ME, Hobbs HH, Shaul PW. High-density lipoprotein binding to scavenger receptor-BI activates endothelial nitric oxide synthase. Nat Med. 2001 Jul;7(7):853-7. doi: 10.1038/89986[↩]
- Ito A, Hong C, Oka K, Salazar JV, Diehl C, Witztum JL, Diaz M, Castrillo A, Bensinger SJ, Chan L, Tontonoz P. Cholesterol Accumulation in CD11c+ Immune Cells Is a Causal and Targetable Factor in Autoimmune Disease. Immunity. 2016 Dec 20;45(6):1311-1326. doi: 10.1016/j.immuni.2016.11.008[↩]
- Price NL, Zhang X, Fernández-Tussy P, Singh AK, Burnap SA, Rotllan N, Goedeke L, Sun J, Canfrán-Duque A, Aryal B, Mayr M, Suárez Y, Fernández-Hernando C. Loss of hepatic miR-33 improves metabolic homeostasis and liver function without altering body weight or atherosclerosis. Proc Natl Acad Sci U S A. 2021 Feb 2;118(5):e2006478118. doi: 10.1073/pnas.2006478118[↩]
- Linton MF, Tao H, Linton EF, Yancey PG. SR-BI: A Multifunctional Receptor in Cholesterol Homeostasis and Atherosclerosis. Trends Endocrinol Metab. 2017 Jun;28(6):461-472. doi: 10.1016/j.tem.2017.02.001[↩]
- Tang S, Tabet F, Cochran BJ, Cuesta Torres LF, Wu BJ, Barter PJ, Rye KA. Apolipoprotein A-I enhances insulin-dependent and insulin-independent glucose uptake by skeletal muscle. Sci Rep. 2019 Feb 4;9(1):1350. doi: 10.1038/s41598-018-38014-3[↩]
- Cartier A, Hla T. Sphingosine 1-phosphate: Lipid signaling in pathology and therapy. Science. 2019 Oct 18;366(6463):eaar5551. doi: 10.1126/science.aar5551[↩][↩]
- Velagapudi S, Rohrer L, Poti F, Feuerborn R, Perisa D, Wang D, Panteloglou G, Potapenko A, Yalcinkaya M, Hülsmeier AJ, Hesse B, Lukasz A, Liu M, Parks JS, Christoffersen C, Stoffel M, Simoni M, Nofer JR, von Eckardstein A. Apolipoprotein M and Sphingosine-1-Phosphate Receptor 1 Promote the Transendothelial Transport of High-Density Lipoprotein. Arterioscler Thromb Vasc Biol. 2021 Oct;41(10):e468-e479. doi: 10.1161/ATVBAHA.121.316725[↩]
- Zanoni P, Velagapudi S, Yalcinkaya M, Rohrer L, von Eckardstein A. Endocytosis of lipoproteins. Atherosclerosis. 2018 Aug;275:273-295. doi: 10.1016/j.atherosclerosis.2018.06.881[↩]
- Cuesta Torres LF, Zhu W, Öhrling G, Larsson R, Patel M, Wiese CB, Rye KA, Vickers KC, Tabet F. High-density lipoproteins induce miR-223-3p biogenesis and export from myeloid cells: Role of scavenger receptor BI-mediated lipid transfer. Atherosclerosis. 2019 Jul;286:20-29. doi: 10.1016/j.atherosclerosis.2019.04.227[↩]
- Martinez LO, Najib S, Perret B, Cabou C, Lichtenstein L. Ecto-F1-ATPase/P2Y pathways in metabolic and vascular functions of high density lipoproteins. Atherosclerosis. 2015 Jan;238(1):89-100. doi: 10.1016/j.atherosclerosis.2014.11.017[↩]
- Gerster R, Eloranta JJ, Hausmann M, Ruiz PA, Cosin-Roger J, Terhalle A, Ziegler U, Kullak-Ublick GA, von Eckardstein A, Rogler G. Anti-inflammatory Function of High-Density Lipoproteins via Autophagy of IκB Kinase. Cell Mol Gastroenterol Hepatol. 2014 Dec 26;1(2):171-187.e1. doi: 10.1016/j.jcmgh.2014.12.006[↩]
- Lucero D, Islam P, Freeman LA, Jin X, Pryor M, Tang J, Kruth HS, Remaley AT. Interleukin 10 promotes macrophage uptake of HDL and LDL by stimulating fluid-phase endocytosis. Biochim Biophys Acta Mol Cell Biol Lipids. 2020 Feb;1865(2):158537. doi: 10.1016/j.bbalip.2019.158537[↩]
- Zheng A, Dubuis G, Georgieva M, Mendes Ferreira CS, Serulla M, Del Carmen Conde Rubio M, Trofimenko E, Mercier T, Decosterd L, Widmann C. HDLs extract lipophilic drugs from cells. J Cell Sci. 2022 Mar 1;135(5):jcs258644. doi: 10.1242/jcs.258644[↩]
- Meilhac O, Tanaka S, Couret D. High-Density Lipoproteins Are Bug Scavengers. Biomolecules. 2020 Apr 12;10(4):598. doi: 10.3390/biom10040598[↩][↩]
- Mackness M, Mackness B. Human paraoxonase-1 (PON1): Gene structure and expression, promiscuous activities and multiple physiological roles. Gene. 2015 Aug 1;567(1):12-21. doi: 10.1016/j.gene.2015.04.088[↩]
- Rallidis LS, Tellis CC, Lekakis J, Rizos I, Varounis C, Charalampopoulos A, Zolindaki M, Dagres N, Anastasiou-Nana M, Tselepis AD. Lipoprotein-associated phospholipase A(2) bound on high-density lipoprotein is associated with lower risk for cardiac death in stable coronary artery disease patients: a 3-year follow-up. J Am Coll Cardiol. 2012 Nov 13;60(20):2053-60. doi: 10.1016/j.jacc.2012.06.057[↩]
- Ossoli A, Simonelli S, Varrenti M, Morici N, Oliva F, Stucchi M, Gomaraschi M, Strazzella A, Arnaboldi L, Thomas MJ, Sorci-Thomas MG, Corsini A, Veglia F, Franceschini G, Karathanasis SK, Calabresi L. Recombinant LCAT (Lecithin:Cholesterol Acyltransferase) Rescues Defective HDL (High-Density Lipoprotein)-Mediated Endothelial Protection in Acute Coronary Syndrome. Arterioscler Thromb Vasc Biol. 2019 May;39(5):915-924. doi: 10.1161/ATVBAHA.118.311987[↩]
- Pirillo A, Catapano AL, Norata GD. HDL in infectious diseases and sepsis. Handb Exp Pharmacol. 2015;224:483-508. doi: 10.1007/978-3-319-09665-0_15[↩]
- Wei C, Wan L, Yan Q, Wang X, Zhang J, Yang X, Zhang Y, Fan C, Li D, Deng Y, Sun J, Gong J, Yang X, Wang Y, Wang X, Li J, Yang H, Li H, Zhang Z, Wang R, Du P, Zong Y, Yin F, Zhang W, Wang N, Peng Y, Lin H, Feng J, Qin C, Chen W, Gao Q, Zhang R, Cao Y, Zhong H. HDL-scavenger receptor B type 1 facilitates SARS-CoV-2 entry. Nat Metab. 2020 Dec;2(12):1391-1400. doi: 10.1038/s42255-020-00324-0[↩]
- Cho KH, Kim JR, Lee IC, Kwon HJ. Native High-Density Lipoproteins (HDL) with Higher Paraoxonase Exerts a Potent Antiviral Effect against SARS-CoV-2 (COVID-19), While Glycated HDL Lost the Antiviral Activity. Antioxidants (Basel). 2021 Feb 1;10(2):209. doi: 10.3390/antiox10020209[↩]
- Gordon SM, Remaley AT. High density lipoproteins are modulators of protease activity: Implications in inflammation, complement activation, and atherothrombosis. Atherosclerosis. 2017 Apr;259:104-113. doi: 10.1016/j.atherosclerosis.2016.11.015[↩]
- American Heart Association. Why Cholesterol Matters. http://heartinsight.heart.org/Summer-2017/Why-Cholesterol-Matters/[↩]
- Kirkland JB. Niacin. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease, 11th ed. Baltimore, MD: Williams & Wilkins; 2014:331-40.[↩]
- K. Suckling, Atherosclerosis, Reference Module in Biomedical Sciences, Elsevier, 2014. ISBN 9780128012383 https://doi.org/10.1016/B978-0-12-801238-3.00190-2[↩]
- National Cholesterol Education Program. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. https://www.nhlbi.nih.gov/files/docs/guidelines/atp3xsum.pdf[↩]





{kind=link}