Contents
- What is hemodialysis
- Hemodialysis vs dialysis
- How does hemodialysis work
- What happens to your blood while it’s in the filter
- Can hemodialysis do everything my kidneys once did?
- Can dialysis cure my kidney disease?
- How long will each hemodialysis treatment last?
- Will I be uncomfortable on hemodialysis?
- How will I pay for my dialysis?
- Can dialysis patients continue to work?
- Can dialysis patients travel?
- What happens if I have been on dialysis and I decide to stop?
- What happens to your blood while it’s in the filter
- Where can I have hemodialysis?
- Home hemodialysis
- Hemodialysis procedure
- Hemodialysis complications
- Peritoneal dialysis vs hemodialysis
- Types of peritoneal dialysis
- Where can I do peritoneal dialysis?
- How do I prepare for peritoneal dialysis?
- Peritoneal dialysis training
- How do you perform a peritoneal dialysis?
- What changes will I have to make when I start peritoneal dialysis?
- Peritoneal dialysis possible side effects and complications
- How will you know if your peritoneal dialysis is working?
- Hemodialysis diet
- Why is it important to keep track of how much liquid you eat and drink?
- Why you need to be on a special hemodialysis diet?
- What if I have high cholesterol?
- What if I have diabetes?
- What you need to know about potassium
- What you need to know about phosphorus
- What you need to know about protein
- What you need to know about sodium
- What you need to know about calories
- Should you take vitamin and mineral supplements?
- Meat and Protein
- Grains/Cereals/Bread
- Milk/Yogurt/Cheese
- Fruit/Juice
- Vegetables and Salads
- Dessert
- Sample Menu
- How will I know if I am eating right to keep me healthy?
What is hemodialysis
Hemodialysis is a type of dialysis which is a treatment to filter wastes and water from your blood, as your kidneys did when they were healthy. Hemodialysis is a way to artificially clean your blood if your kidneys are no longer able to cope. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood.
Hemodialysis can help you feel better and live longer, but it’s not a cure for kidney failure.
Table 1. Kidney Failure Treatment Options
| Treatment | Schedule | Location | Availability | Equipment and Supplies | Training Required | Diet | Level of Freedom | Level of Responsibility |
| In-Center Hemodialysis | Three treatments a week for about 4 hours. | Dialysis center. | Available in most communities; may require travel in some rural areas. | No equipment or supplies in the home. | Little training required; clinic staff perform most tasks. | Must limit fluids, sodium, potassium, and phosphorus. | Little freedom during treatments. Greater freedom on nontreatment days. | Some patients prefer to let clinic staff perform all tasks. |
| Home Hemodialysis | More flexibility in determining your schedule of treatments. | Home. | More widely used as smaller and simpler machines are developed. | Hemodialysis machine connected to plumbing, chair. | You and a partner must attend several training sessions. | Must limit fluids, sodium, potassium, and phosphorus. | More freedom to set your own schedule. You’re still linked to a machine for several hours a week. | You and your partner have to monitor vital signs and clean and set up equipment. Can be stressful on your partner. |
| Continuous Ambulatory Peritoneal dialysis (CAPD) | Four to six exchanges a day, every day. | Any clean environment that allows solution exchanges. | Widely available. | Bags of dialysis solution take up storage space. | You’ll need to attend several training sessions. You may need to bring a partner. | Must limit sodium and calories. | You can move around, exercise, work, drive, etc., with solution in your abdomen. | You must perform exchanges four to six times a day, every day. |
| Automated Peritoneal Dialysis | Three to five exchanges a night, every night, with an additional exchange begun first thing in the morning. | Any clean environment that allows solution exchanges. | Widely available. | Cycling machine, bags of dialysis solution. | You’ll need to attend several training sessions. You may need to bring a partner. | Must limit sodium and calories. | You’re linked to a machine during the night. You’re free from exchanges during the day. | You must set up your cycler every night. |
| Kidney Transplant (Deceased Donor) | You may wait several years before a suitable kidney is available. After surgery, you’ll have regular checkups with your doctor. | The transplant surgery takes place in a hospital. | Transplant centers are located throughout the country. However, the demand for kidneys is far greater than the supply. | No equipment or supplies needed. | You’ll need to learn about your medicines and when to take them. | Fewer dietary restrictions. | Offers the greatest amount of freedom. | You must take anti-rejection medicines every day. |
| Kidney Transplant (Living Donor) | If a friend or family member is donating, you can schedule the surgery when you’re both ready. After surgery, you’ll have regular checkups with your doctor. | The transplant surgery takes place in a hospital. | Transplant centers are located throughout the country. However, the demand for kidneys is far greater than the supply. | No equipment or supplies needed. | You’ll need to learn about your medicines and when to take them. | Fewer dietary restrictions. | Offers the greatest amount of freedom. | You must take anti-rejection medicines every day. |
Table 2. Dialysis center and home hemodialysis comparison
| Dialysis Center and Home Hemodialysis Comparison Chart | ||
| Dialysis center | Home | |
| Schedule | Three treatments a week for about 4 hours. Monday, Wednesday, Friday; or Tuesday, Thursday, Saturday. | Flexible. Three to seven short or long treatments per week at times that work best for you. |
| Availability | Available in most communities; may require travel in some rural areas. | Becoming more widely available as smaller equipment is developed. |
| Machine/supplies | The clinic has the machine and supplies. | The machine and 2- to 4-weeks’ worth of supplies are in the home. You may need minor changes in your home to connect the machine to electricity and water. |
| Training | The clinic teaches about treatments, diet, liquids, medicines, lab tests, etc. | You and a partner must attend 3 to 8 weeks of home hemodialysis training. |
| Diet and liquids | Strict limits on liquids, phosphorus, sodium, and potassium intake. | Fewer limits on liquids or diet, based on the amount of hemodialysis and lab tests. |
| Level of freedom | Less freedom on treatment days. May feel washed out and tired for hours after each treatment. | More freedom because you set the treatment schedule to meet the total amount prescribed. Work and travel are much easier. |
| Amount of work | Center staff members do hemodialysis tasks. They can teach you to do some tasks. | You and your partner must set up, run, and clean the machine; check vital signs; track the treatments and send in forms; and order supplies. |
| Payment | Medicare and most other health plans cover three hemodialysis treatments a week. | Medicare covers three hemodialysis treatments a week and may cover more for medical reasons; other health plans may cover all hemodialysis treatments. |
Hemodialysis vs dialysis
Dialysis is a way to artificially clean the blood if your kidneys are no longer able to cope.
There are two main types of dialysis:
- Hemodialysis, in which your blood is circulated through a dialysis machine for cleaning.
- Peritoneal dialysis, which uses the peritoneal membrane in your abdomen (tummy) to filter blood allowing cleaning to take place inside the body.
How does hemodialysis work
During hemodialysis, your blood goes through a filter, called a dialyzer, outside your body. A dialyzer is sometimes called an “artificial kidney.”
At the start of a hemodialysis treatment, a dialysis nurse or technician places two needles into your arm. You may prefer to put in your own needles after you’re trained by your health care team. A numbing cream or spray can be used if placing the needles bothers you. Each needle is attached to a soft tube connected to the dialysis machine.
The dialysis machine pumps blood through the filter and returns the blood to your body. During the process, the dialysis machine checks your blood pressure and controls how quickly
- blood flows through the filter
- fluid is removed from your body
Figure 1. How hemodialysis work
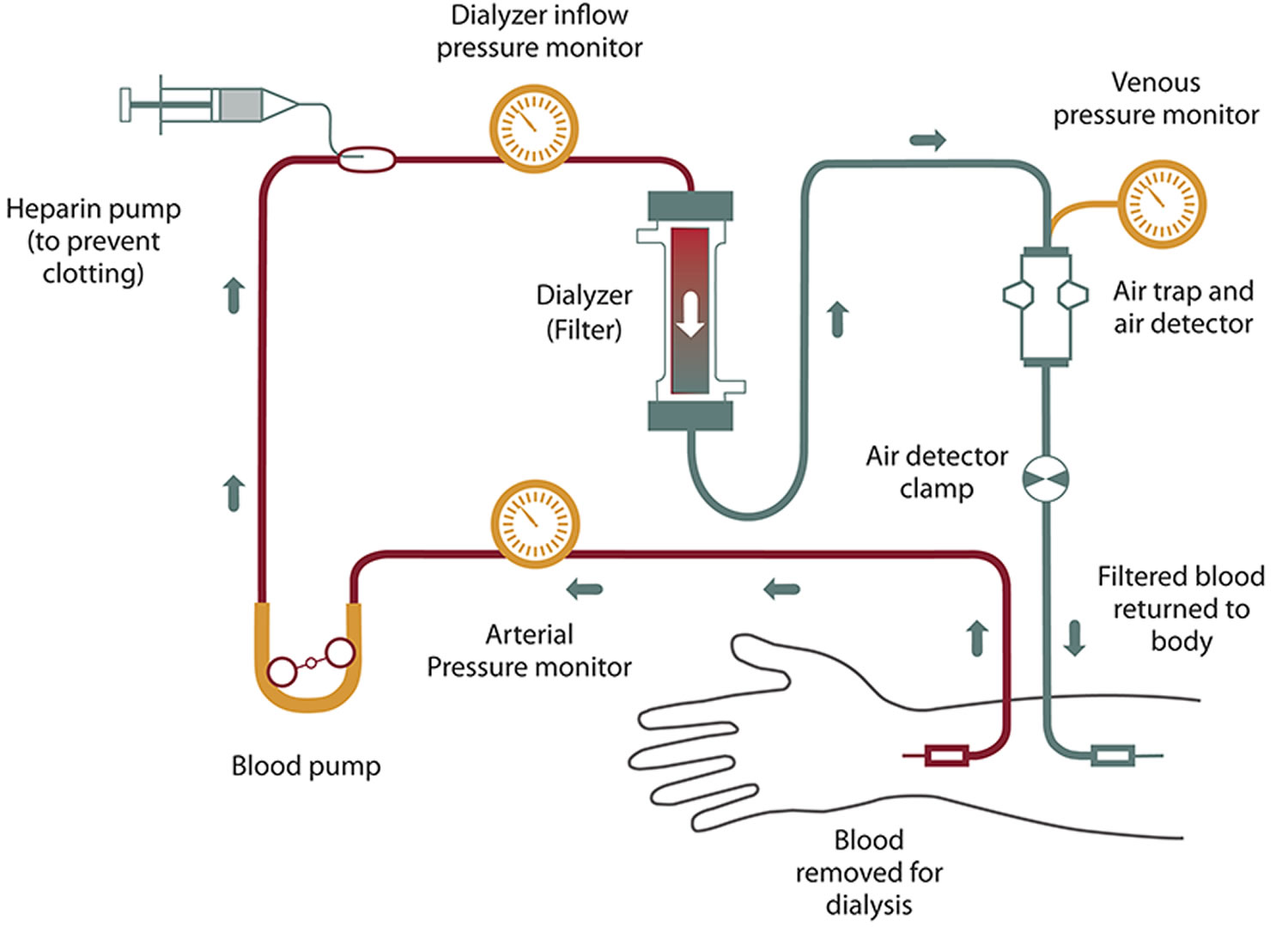 Figure 2. Hemodialysis – during hemodialysis, your blood is pumped through a filter, called a dialyzer.
Figure 2. Hemodialysis – during hemodialysis, your blood is pumped through a filter, called a dialyzer.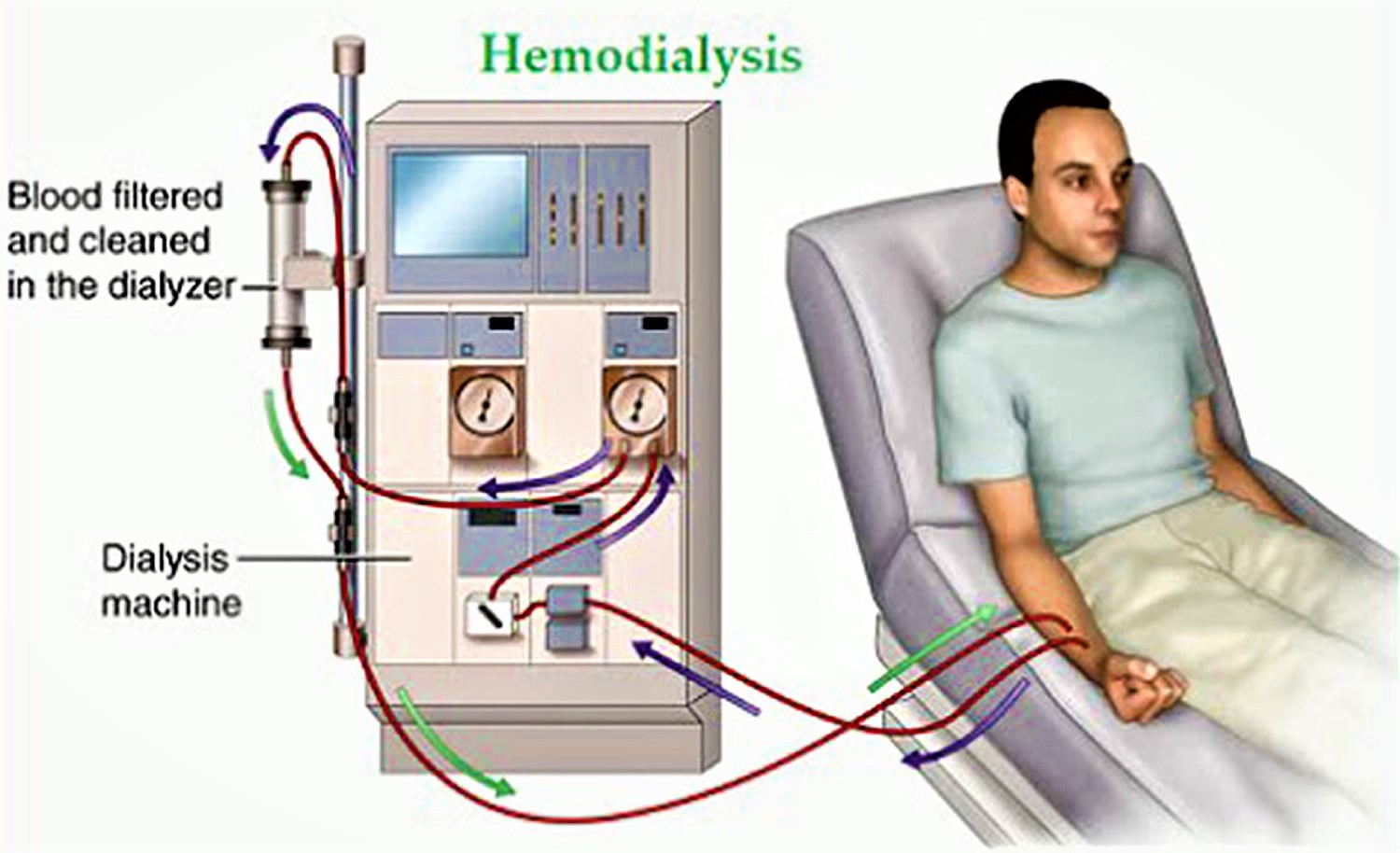
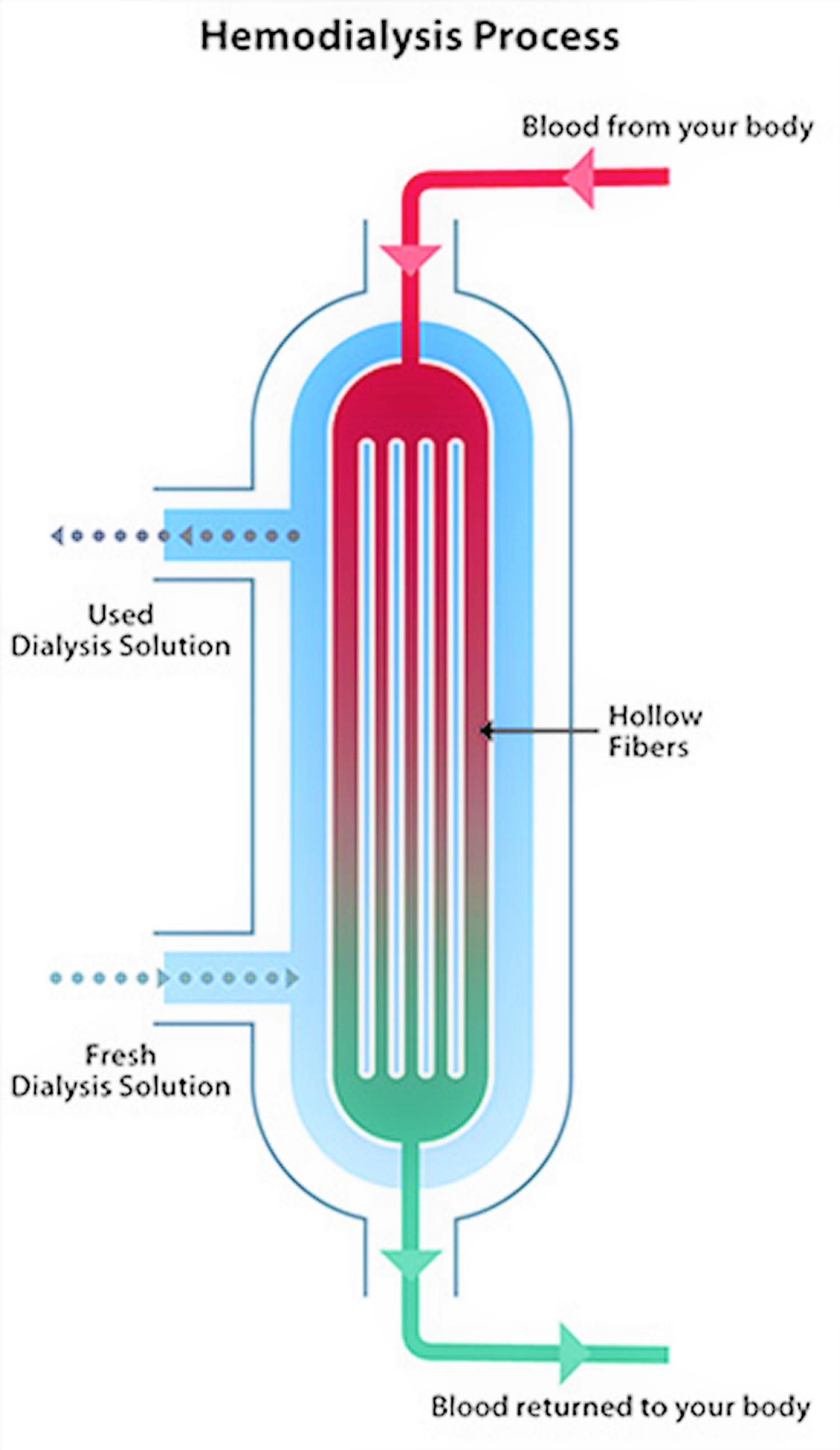
What happens to your blood while it’s in the filter
Blood enters at one end of the filter and is forced into many, very thin, hollow fibers. As your blood passes through the hollow fibers, dialysis solution passes in the opposite direction on the outside of the fibers. Waste products from your blood move into the dialysis solution. Filtered blood remains in the hollow fibers and returns to your body.
Your nephrologist—a doctor who specializes in kidney problems—will prescribe a dialysis solution to meet your needs. The dialysis solution contains water and chemicals that are added to safely remove wastes, extra salt, and fluid from your blood.
Your doctor can adjust the balance of chemicals in the solution if:
- your blood tests show your blood has too much or too little of certain minerals, such as potassium or calcium
- you have problems such as low blood pressure or muscle cramps during dialysis
Figure 3. Hemodialysis filter – dialyzer (in the hemodialysis filter, your blood flows inside hollow fibers that filter out wastes and extra salt and water.)
Can hemodialysis do everything my kidneys once did?
No. Hemodialysis can replace part, but not all, of your kidney function. Dialysis will help improve your energy level, and changes you make to your diet can help you feel better. Limiting how much water and other liquid you drink and take in through foods can help keep too much fluid from building up in your body between treatments. Medicines also help you maintain your health while on dialysis.
Can dialysis cure my kidney disease?
In some cases of sudden or acute kidney failure, dialysis may only be needed for a short time until the kidneys get better. However, when chronic kidney disease progresses to kidney failure over time, your kidneys do not get better and you will need dialysis for the rest of your life unless you are able to receive a kidney transplant.
How long will each hemodialysis treatment last?
In a dialysis center, hemodialysis is usually done 3 times per week for about 4 hours at a time. People who choose to do hemodialysis at home may do dialysis treatment more frequently, 4-7 times per week for shorter hours each time.
Your doctor will give you a prescription that tells you how much treatment you need. Studies have shown that getting the right amount of dialysis improves your overall health, keeps you out of the hospital and enables you to live longer. Your dialysis care team will monitor your treatment with monthly lab tests to ensure you are getting the right amount of dialysis. One of the measures your dialysis care team may use is called urea reduction ratio (URR). Another measure is called Kt/V (pronounced kay tee over vee). Ask your dialysis care team what measure they use and what your number is. To ensure that you are getting enough dialysis:
- your Kt/V should be at least 1.2 or
- your urea reduction ratio (URR) should be at least 65 percent.
Will I be uncomfortable on hemodialysis?
When you begin hemodialysis, the needles put in your fistula or graft may be uncomfortable. Most patients get used to this in time. Your dialysis care team will make sure you are as comfortable as possible during your treatment. Symptoms like cramps, headaches, nausea or dizziness are not common, but if you do have any of them, ask your dialysis care team if any of the following steps could help you:
- Slow down your fluid removal, which could increase your dialysis time.
- Increase the amount of sodium in your dialysate.
- Check your high blood pressure medications.
- Adjust your dry weight, or target weight.
- Cool the dialysate a little.
- Use a special medication to help prevent low blood pressure during dialysis.
You can help yourself by following your diet and fluid allowances. The need to remove too much fluid during dialysis is one of the things that may make you feel uncomfortable during your treatment.
How will I pay for my dialysis?
Dialysis is expensive. However, the federal government’s Medicare program pays 80 percent of all dialysis costs for most patients. Private health insurance or state medical aid may also help with the costs. For more information on insurance please go here (https://www.kidney.org/atoz/content/insurance).
Can dialysis patients continue to work?
Yes. Many dialysis patients continue to work or return to work after they have gotten used to dialysis. If your job has a lot of physical labor (heavy lifting, digging, etc.), you may need to change your duties.
Some people continue to work full time as they begin treatment. Others switch to a part-time or flexible schedule. Some people ask for jobs that are less physically demanding.
You may need to work different hours to go to hemodialysis. Or you may need a clean, private area where you can do peritoneal dialysis.
You should feel free to talk to your employer about job changes that might make it easier for you to work. Remember, your employer probably won’t know what changes you might need if you don’t ask for them.
Your employer may not know much about kidney disease or how it may affect your abilities. There might be concerns about how much work you can do and how much time off you will need. There could also be concerns about how much your health benefits will cost the company. You may want to ask your doctor or another member of your healthcare team to talk with your employer about these. A little information about your illness, abilities, and limitations can do a lot to ease an employer’s concerns. Here are a few of the topics you and your employer may want to discuss:
- Changing your work schedule to allow for dialysis and healthcare visits
- Making up time taken off for medical reasons
- Physical limitations, if any
- What to do in case of an emergency
Employers may not know about tax credits they can get for making changes to the workplace.
The Civil Rights Act, the Rehabilitation Act, and the Americans with Disabilities Act all protect you from job discrimination. Examples of discrimination include being fired or being turned down for a job or a promotion because of an illness or condition that does not affect your ability to do your job. The Department of Labor handles complaints filed under the Rehabilitation Act.
If you work for a company with 15 or more employees, the Americans with Disabilities Act (ADA) requires your employer to make any “reasonable accommodations” that you might need in order to work. Examples include:
- Making parking lots, bathrooms, and work areas handicapped accessible
- Having flexible work schedules
- Reassigning you to a less strenuous job if you request one and one is available
- Assigning any of your non-essential tasks to other employees, at your request
The Equal Employment Opportunity Commission handles complaints under the ADA.
If you work at least 20 weeks of the year for an employer with 50 or more employees, you may qualify for the Family and Medical Leave Act (FMLA). The FMLA allows for 12 weeks of unpaid, job-protected leave for medical reasons.
If you had group health insurance coverage before the leave, it will continue under the same terms or conditions. Your employer can ask for medical certification stating that you have a serious illness, but cannot punish you for taking leave to have surgery or begin treatment. Your spouse, children, or parents may also be eligible for FMLA leave if you need them to provide you with care or transportation. The Department of Labor handles complaints under the FMLA.
Can dialysis patients travel?
Yes. Dialysis centers are located in every part of the United States and in many foreign countries.
Before you travel, you must make an appointment for dialysis treatments at another center. The staff at your center may be able to help you arrange this appointment.
Many dialysis centers have a staff member who is experienced in arranging dialysis treatments away from home (transient dialysis). Some centers will assist patients in making their own arrangements. Ask your social worker or primary nurse if there is such a person at your center.
It is important to start planning at least six to eight weeks in advance. More time should be allowed for popular vacation spots or travel during holidays. Be flexible about the dates for your trip as space in dialysis units may be limited. If you would prefer to have your treatments on specific days and at specific times, let the center know in advance. The unit may not always be able to honor your request, however, because space is limited.
You or your patient travel coordinator may need to contact more than one center in order to find a center that can provide dialysis for you. Check with the center as soon as you arrive to confirm your appointment. You may also want to visit the center and meet the staff so you will feel more comfortable. Before doing this, however, make an appointment with the social worker or nurse manager of the dialysis center you plan to visit.
What happens if I have been on dialysis and I decide to stop?
If you’ve been on dialysis and wish to stop, you’ll still receive supportive care. The dialysis social worker may be able to help you develop an end-of-life care plan before you stop dialysis.
Where can I have hemodialysis?
You can receive treatment at a dialysis center or at home. Each location has its pros and cons.
Dialysis center
Most people go to a dialysis center for treatment. At the dialysis center, health care professionals set up and help you connect to the hemodialysis machine. A team of health care workers will be available to help you. You will continue to see your doctor. Other team members may include nurses, health care technicians, a dietitian, and a social worker.
Set schedule
You’ll have a fixed time slot for your treatments, usually three times per week: Monday, Wednesday, and Friday; or Tuesday, Thursday, and Saturday. Each hemodialysis session lasts about 4 hours. When choosing a hemodialysis schedule, think about your work and child care or other caregiving duties.
Nighttime option
Some hemodialysis centers offer nighttime treatments. These treatments occur at the dialysis center 3 nights a week while you sleep, which takes longer. Getting longer overnight hemodialysis treatments means:
- your days are free.
- you have fewer diet changes.
- your liquid allowance (how much liquid you can drink) is closer to normal.
- you may have a better quality of life than with a standard hemodialysis schedule. Longer treatment sessions may reduce your symptoms.
How do I find a dialysis center?
Your doctor, nurse, or social worker can help you find a dialysis center that’s convenient for you. Under Medicare rules, you have the right to choose the dialysis center where you’ll receive treatment. You may want to use Dialysis Facility Compare (https://www.medicare.gov/DialysisFacilityCompare/), which rates all dialysis centers according to quality. Your doctor will give your medical information to the dialysis center you choose.
Most large cities have more than one dialysis center to choose from. You can visit the centers to see which one best fits your needs. For example, you can ask about a center’s rules for laptop and cellphone use, as well as for having visitors. You may want the center to be close to your home to save travel time. If you live in a rural area, the closest dialysis center may be far from your home. If you’d have a hard time getting to the dialysis center, you may want to consider home dialysis treatments such as home hemodialysis or peritoneal dialysis.
Home hemodialysis
Home hemodialysis lets you have longer or more frequent dialysis, which comes closer to replacing the work healthy kidneys do—usually three to seven times per week, and with treatment sessions that last between 2 and 10 hours. Machines for home use are small enough to sit on an end table.
If you choose to have your treatments at home, you’ll still see your doctor once per month.
Flexible schedule
You can choose a schedule that fits the way you live. You can use:
- Standard home hemodialysis — three times a week or every other day for 3 to 5 hours
- Short daily hemodialysis — 5 to 7 days per week for 2 to 4 hours at a time
- Nightly home hemodialysis — three to six times per week while you sleep
Your doctor will decide how many treatments you need each week for daily or nightly home hemodialysis.
More dialysis filters your blood more thoroughly
Compared with a standard hemodialysis schedule, daily or nightly home hemodialysis will let you:
- eat and drink more normally
- take fewer blood pressure medicines
Healthy kidneys work 24 hours a day, 7 days a week. Getting more hemodialysis feels more like having healthy kidneys and lowers your chances for problems that are common with a standard hemodialysis schedule, such as:
- painful muscle cramps from removing too much fluid too quickly
- high blood pressure, which can cause a headache or, in rare cases, a stroke
- low blood pressure, which can make you faint, feel sick to your stomach, or be more likely to fall
- high phosphate levels, which can weaken bones and make your skin itch
Better quality of life
Standard hemodialysis can make you feel tired or washed out for several hours after each treatment. People who have switched from standard hemodialysis to longer or more frequent hemodialysis report they feel better, with more energy, less nausea, and better sleep. They also may report a better quality of life 2.
Training for home hemodialysis
Most dialysis centers require that you have a trained partner in your home during hemodialysis treatments, so you must ask a family member or friend to go through the training with you. The clinic’s home-training nurse will teach you important safety skills.
During training, you and your care partner will learn to:
- set up the machine
- take steps to prevent infection
- place needles into the vascular access
- respond to any alarms from the machine
- check your weight, temperature, blood pressure, and pulse
- record treatment details for the clinic
- clean the machine
- throw out used supplies safely
- track used supplies and order new ones
Training may take 4½ to 6 hours, 5 days a week, for 3 to 8 weeks. If you already know how to place the needles into your access, training may take less time.
The home-training nurse will make sure that you and your partner feel confident and may visit your home to help with your first at-home treatment. In addition to providing training and a hemodialysis machine that stays in your home, the dialysis center also provides 24-hour support if you have a question or problem. Some programs also monitor treatments over the internet.
Hemodialysis procedure
Dialysis is a complex treatment that takes time to understand.
Take care of the blood vessels in your arms
It’s important for you to protect the veins in your arm prior to starting dialysis. If you have kidney disease, remind health care providers to draw blood and insert IV lines only in veins below your wrist; for example, ask them to use a vein in the back of your hand. If an arm vein is damaged by an IV line or by repeated blood draws, that vein may not be able to be used for dialysis.
Vascular access surgery
One important step before starting hemodialysis treatment is having minor surgery to create a vascular access. Your vascular access will be your lifeline through which you’ll connect to the dialyzer. Dialysis moves blood through the filter at a high rate. Blood flow is very strong. The machine withdraws and returns almost a pint of blood to your body every minute. The access will be the place on your body where you insert needles to allow your blood to flow from and return to your body at a high rate during dialysis.
Three types of vascular access exist
- an arteriovenous (AV) fistula
- an arteriovenous (AV) graft
- a catheter
Work closely with your nephrologist and vascular surgeon—a surgeon who works with blood vessels—to make sure the access is in place in plenty of time. Healing may take several months. The goal is for your access to be ready for use when you are ready for dialysis.
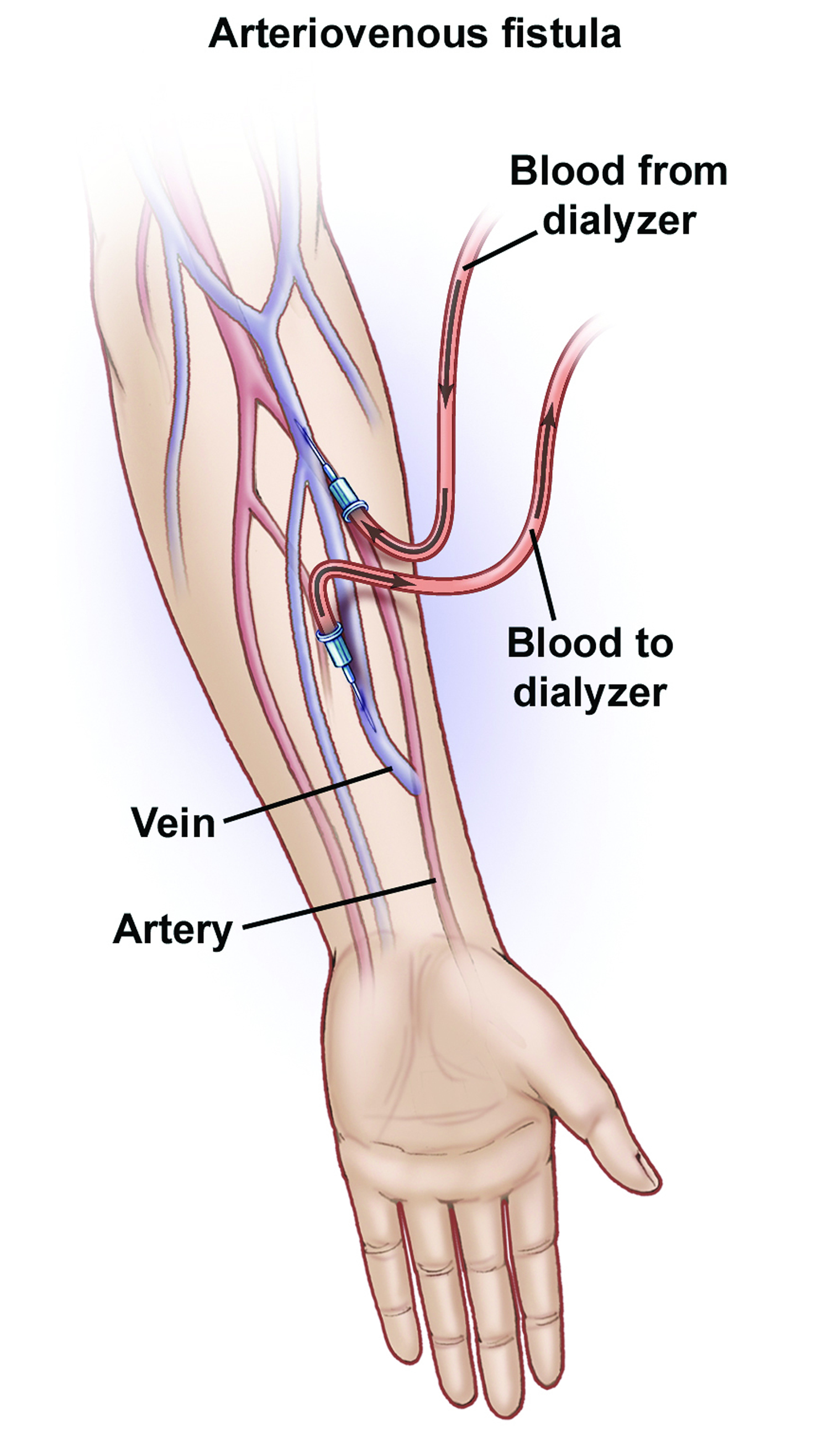
Arteriovenous fistula
The best type of long-term access is an arteriovenous fistula. A surgeon connects an artery to a vein, usually in your arm, to create an arteriovenous fistula. An artery is a blood vessel that carries blood away from your heart. A vein is a blood vessel that carries blood back toward your heart. When the surgeon connects an artery to a vein, the vein grows wider and thicker, making it easier to place the needles for dialysis. The arteriovenous fistula also has a large diameter that allows your blood to flow out and back into your body quickly. The goal is to allow high blood flow so that the largest amount of blood can pass through the dialyzer.
The arteriovenous fistula is considered the best option because it:
- provides highest blood flow for dialysis
- is less likely to become infected or clot
- lasts longer
Most people can go home after outpatient surgery. You will get local anesthesia to numb the area where the vascular surgeon creates the arteriovenous fistula. Depending on your situation, you may get general anesthesia and not be awake during the procedure.
The preferred location for placing an arteriovenous fistula for the first time is distally at the radius, thus making it possible to place a second fistula proximally if the first one failed to mature. The order of preference for creating an arteriovenous fistula 3:
- Distal Radio-Cephalic (Distal radial artery to cephalic vein)
- Proximal Radio-Cephalic (Proximal radial artery to cephalic vein)
- Brachio-Cephalic (Brachial artery to Cephalic vein)
- Brachio-Basilic (Brachial artery to Basilic vein)
Figure 4. Arteriovenous fistula for dialysis
Arteriovenous graft
If problems with your veins prevent you from having an arteriovenous fistula, you may need an arteriovenous graft instead. To create an arteriovenous graft, your surgeon uses a man-made tube to connect an artery to a vein. You can use an arteriovenous graft for dialysis soon after surgery. However, you’re more likely to have problems with infection and blood clots. Repeated blood clots can block the flow of blood through the graft and make it hard or impossible to have dialysis.
Catheter for temporary access
If your kidney disease has progressed quickly, or you have not had a vascular access placed before you need dialysis, you may need a venous catheter—a small, soft tube inserted into a vein in your neck, chest, or leg near the groin—as a temporary access. A nephrologist or an interventional radiologist—a doctor who uses medical imaging equipment to perform surgery—places the venous catheter while you’re in a hospital or at an outpatient clinic. You’ll receive local anesthesia and medicine to keep you calm and relaxed during the procedure.
What changes will I have to make when I start hemodialysis?
You have to adjust your life to build your hemodialysis treatment sessions into your routine. If you have in-center dialysis, you may need to rest after each treatment. Adjusting to the effects of kidney failure and the time you spend on hemodialysis can be hard. You may need to make changes in your work or home life, giving up some activities and responsibilities. Accepting these changes can be hard on you and your family. A mental health counselor or social worker can answer your questions and help you cope .
You will have to change what you eat and drink. Your health care team may adjust the medicines that you take.
Take care of your hemodialysis access
Your hemodialysis access is your lifeline. You will need to protect your access. Wash the area around your access with soap and warm water every day. Check the area for signs of infection, such as warmth or redness. When blood is flowing through your access and your access is working well, you can feel a vibration over the area. Let your dialysis center know if you can’t feel the vibration.
Sometimes, even when you are very careful, your access may clot or become infected.
Clots can form inside the opening of the catheter or form on the outside of the catheter and block the opening. This can cause blood to flow at a slower rate than the rate your doctor ordered. If the blood flow rate remains low for more than one dialysis treatment, the catheter should be checked and treated the same day. Early treatment may prevent the clot from totally blocking the catheter. It is important to restore the recommended blood flow rate and treat clots that are forming so that your catheter continues to work well and you get the amount of dialysis you need.
Infection can also occur even with a good blood flow rate. It is important to follow your catheter care instructions, exactly as you were taught, in order to avoid infection. You should know the following signs and symptoms of a catheter infection and report them to your doctor or dialysis team right away, so you can get the proper treatment as quickly as possible. The signs and symptoms of an infection include:
- Fever
- Chills
- Drainage from the catheter exit site
- Redness or tenderness around the catheter exit site
General feeling of weakness and illness
Treatment depends on the type of infection but may include:
- An ointment applied directly to the infected area if it is an exit site infection.
- Antibiotic medication if there is drainage from the exit site.
- An intravenous IV antibiotic (a solution containing an antibiotic that is administered directly into a vein) if the infection has spread to the blood.
Make changes to what you eat and drink
If you’re on hemodialysis, you may need to limit:
- sodium in foods and drinks.
- high-phosphorus foods.
- the amount of liquid you drink, including liquid found in foods. Fluid builds up in your body between hemodialysis treatments.
You may also need to:
- add protein to your diet because hemodialysis removes protein
- choose foods with the right amount of potassium
- take vitamins made for people with kidney failure
- find healthy ways to add calories to your diet because you may not have a good appetite
Eating the right foods can help you feel better when you’re on hemodialysis. Talk with your dialysis center’s dietitian to find a hemodialysis meal plan that works for you.
Points to remember
- Your choices about what to eat and drink while on hemodialysis can make a difference in how you feel and can make your treatments work better.
- Between dialysis treatment sessions, wastes can build up in your blood and make you sick. You can reduce waste buildup by controlling what you eat and drink.
- It helps to limit or avoid foods and beverages that have lots of:
- potassium
- phosphorus
- sodium—for example, vegetable juice and sports drinks
- You may feel better if you keep track of and limit how much liquid you eat and drink.
- Hemodialysis removes extra fluid from your body. However, hemodialysis can remove only so much fluid at a time safely. If you come to your hemodialysis with too much fluid in your body, your treatment may make you feel ill. You may get muscle cramps or have a sudden drop in blood pressure that causes you to feel dizzy or sick to your stomach.
- Potassium levels can rise between hemodialysis sessions and affect your heartbeat. Eating too much potassium can be dangerous to your heart and may even cause death.
- Too much phosphorus in your blood pulls calcium from your bones. Losing calcium may make your bones weak and likely to break.
- Renal dietitians encourage most people on hemodialysis to eat high-quality protein because it produces less waste for removal during dialysis. High-quality
- protein comes from meat, poultry, fish, and eggs.
- Sodium is a part of salt. Sodium is found in many canned, packaged, frozen, and fast foods. Sodium is also found in many condiments, seasonings, and meats. Too much sodium makes you thirsty, which makes you drink more liquid.
- Everyone’s calorie needs are different. You might need to cut down on calories if you are overweight, or you might need to find ways to add calories to your diet if you are losing weight without trying.
You may not get enough vitamins and minerals in your diet because you have to avoid so many foods. Your health care provider may prescribe a vitamin and mineral supplement designed specifically for people with kidney failure. For safety reasons, talk with your health care provider before using probiotics, dietary supplements, or any other medicine together with or in place of the treatment your health care provider prescribes.
How will I know if my hemodialysis is working?
You’ll know your hemodialysis treatments are working by how you feel. Your energy level may increase and you may have a better appetite. Hemodialysis reduces salt and fluid buildup, so you should have less shortness of breath and swelling as well.
To make the most of your hemodialysis treatment, keep to your ideal “dry weight.” Your ideal dry weight is your weight when you don’t have extra fluid in your body. If you’re careful about the sodium in your diet and the hemodialysis is working, you should be able to reach your ideal dry weight at the end of every hemodialysis treatment. When hemodialysis treatments are working and you keep to your ideal dry weight, your blood pressure should be well controlled.
In addition, blood tests can show how well your hemodialysis treatments are working. Once a month, whether you’re on home or dialysis center hemodialysis, your dialysis center will test your blood.
To see whether hemodialysis is removing enough urea, the dialysis clinic should periodically—normally once a month—test your blood to measure the hemodialysis adequacy. Blood is sampled at the start of hemodialysis and at the end. The levels of urea in the two blood samples are then compared. Two methods are generally used to assess dialysis adequacy, URR (urea reduction ratio) and Kt/V.
What is the urea reduction ratio (URR)?
URR stands for urea reduction ratio, meaning the reduction in urea as a result of dialysis. The urea reduction ratio is one measure of how effectively a dialysis treatment removed waste products from the body and is commonly expressed as a percentage.
Example: If the initial, or predialysis, urea level was 50 milligrams per deciliter (mg/dL) and the postdialysis urea level was 15 mg/dL, the amount of urea removed was 35 mg/dL.
- 50 mg/dL – 15 mg/dL = 35 mg/dL
The amount of urea removed (35 mg/dL) is expressed as a percentage of the predialysis urea level (50 mg/dL).
- 35/50 = 70/100 = 70%
Although no fixed percentage can be said to represent an adequate dialysis, patients generally live longer and have fewer hospitalizations if the urea reduction ratio is at least 60 percent. As a result, some experts recommend a minimum urea reduction ratio of 65 percent.
The urea reduction ratio is usually measured only once every 12 to 14 treatments, which is once a month. The urea reduction ratio may vary considerably from treatment to treatment. Therefore, a single value below 65 percent should not be of great concern, but a patient’s average urea reduction ratio should exceed 65 percent.
What is the Kt/V?
Kt/V is another way of measuring dialysis adequacy. In this measurement,
- K stands for the dialyzer clearance, the rate at which blood passes through the dialyzer, expressed in milliliters per minute (mL/min)
- t stands for time
- Kt, the top part of the fraction, is clearance multiplied by time, representing the volume of fluid completely cleared of urea during a single treatment
- V, the bottom part of the fraction, is the volume of water a patient’s body contains
Example: If the dialyzer’s clearance is 300 mL/min and a dialysis session lasts for 180 minutes (3 hours), Kt will be 300 mL/min multiplied by 180 minutes. The result comes to 54,000 mL, or 54 liters.
- Kt = 300 mL/min multiplied by 180 minutes
- Kt = 54,000 mL = 54 liters
The body is about 60 percent water by weight. If a patient weighs 70 kilograms (kg), or 154 pounds (lbs), V will be 42 liters.
- V = 70 kg multiplied by .60 = 42 liters
So the ratio—K multiplied by t to V, or Kt/V—compares the amount of fluid that passes through the dialyzer with the amount of fluid in the patient’s body. The Kt/V for this patient would be 1.3.
- Kt/V = 54/42 = 1.3
How Does the Kt/V Compare with the urea reduction ratio?
The Kt/V is mathematically related to the urea reduction ratio and is in fact derived from it, except that the Kt/V also takes into account two additional factors:
- urea generated by the body during dialysis
- extra urea removed during dialysis along with excess fluid
The Kt/V is more accurate than the urea reduction ratio in measuring how much urea is removed during dialysis, primarily because the Kt/V also considers the amount of urea removed with excess fluid. Consider two patients with the same urea reduction ratio and the same postdialysis weight, one with a weight loss of 1 kg—about 2.2 lbs—during the treatment and the other with a weight loss of 3 kg-about 6.6 lbs. The patient who loses 3 kg will have a higher Kt/V, even though both have the same urea reduction ratio.
The fact that a patient who loses more weight during dialysis will have a higher Kt/V does not mean it is better to gain more water weight between dialysis sessions so more fluid has to be removed, because the extra fluid puts a strain on the heart and circulation. However, patients who lose more weight during dialysis will have a higher Kt/V for the same level of urea reduction ratio.
On average, a Kt/V of 1.2 is roughly equivalent to a urea reduction ratio of about 63 percent. Thus, another standard of adequate dialysis is a minimum Kt/V of 1.2. The Kidney Disease Outcomes Quality Initiative group has adopted the Kt/V of 1.2 as the standard for dialysis adequacy 4. Like the urea reduction ratio, the Kt/V may vary considerably from treatment to treatment because of measurement error and other factors. So while a single low value is not always of concern, the average Kt/V should be at least 1.2. In some patients with large fluid losses during dialysis, the Kt/V can be greater than 1.2 with a urea reduction ratio slightly below 65 percent—in the range of 58 to 65 percent. In such cases, the Kidney Disease Outcomes Quality Initiative guidelines consider the Kt/V to be the primary measure of adequacy.
Is a urea reduction ratio of 65 percent or a Kt/V of 1.2 good enough?
These dialysis adequacy guidelines were determined on the basis of studies in large groups of patients. These studies generally showed that patients with lower Kt/V and urea reduction ratio numbers had more health problems and a greater risk of death. However, the HEMO study showed that a Kt/V greater than 1.2 did not result in improved outcomes.
If a patient’s Kt/V is always above 1.2 and the urea reduction ratio is close to 65 percent, then the patient’s treatment is meeting adequacy guidelines. The patient’s urea reduction ratio may be a few points below 65 if the person has large fluid losses during dialysis.
What can patients do to improve their Kt/V?
If a patient’s average Kt/V—usually the average of three measurements—is consistently below 1.2, the patient and the nephrologist need to discuss ways to improve it. Since the V value is fixed, Kt/V can be improved either by increasing K or t.
Increase Blood Flow through the Dialyzer
Increasing K depends primarily on the rate of blood flow through the dialyzer. No matter how good a dialyzer is, how well it works depends primarily on moving blood through it. In many patients, a good rate is difficult to achieve because of vascular access problems.
If a patient’s blood flow rate is good, further improvements in clearance can be obtained by using a big dialyzer or, in some cases, by increasing the flow rate for dialysis solution from the usual 500 mL/min to 600 or 800 mL/min. A good flow rate for adult patients is 350 mL/min and higher. A few centers are even using two dialyzers at the same time to increase K in larger than average patients.
However, the rate of blood flow through the dialyzer is key, and a good vascular access is crucial to make sure a patient is getting good clearance.
Increase Time on Dialysis
The other way to improve the Kt in Kt/V is to increase t by dialyzing for a longer period. For example, if the Kt/V is 0.9 and the goal is 1.2, then 1.2/0.9 = 1.33, so 1.33 times more Kt is needed. If K is not changed, this means the length of the session needs to increase by 33 percent. If the inadequate sessions lasted 3 hours, they should be increased to 4 hours.
Identify and Eliminate Circulation Problems
If during any given month a patient’s Kt/V is extremely low, the measurement should be repeated, unless a reason for the low Kt/V is obvious. Obvious reasons include treatment interruption, problems with blood or solution flow, and a problem in sampling either the pre- or postdialysis blood. If no reason for the sudden drop is apparent, then a problem with needle placement, like accidental needle reversal, or with the vascular access, such as recirculation, should be suspected.
Hemodialysis complications
You could have a problem with your vascular access, which is the most common reason someone on hemodialysis needs to go to the hospital. Any type of vascular access may:
- become infected
- have poor blood flow or blockage from a blood clot or scar
These problems can keep your treatments from working. You may need to have more procedures to replace or repair your access for it to work properly.
Sudden changes in your body’s water and chemical balance during treatment can cause additional problems, such as:
- muscle cramps.
- a sudden drop in blood pressure, called hypotension. Hypotension can make you feel weak, dizzy, or sick to your stomach.
Your doctor can change your dialysis solution to help avoid these problems. The longer and more frequent treatments of home hemodialysis are less likely to cause muscle cramps or rapid changes in blood pressure than standard in-center dialysis.
You can lose blood if a needle comes out of your access or a tube comes out of the dialyzer. To prevent blood loss, dialysis machines have a blood leak detector that sets off an alarm. If this problem occurs at the clinic, a nurse or technician will be on hand to act. If you’re using home dialysis, your training will prepare you and your partner to fix the problem.
You may need a few months to adjust to hemodialysis. Always report problems to your health care team, who often can treat side effects quickly and easily. You can avoid many side effects by following an eating plan you develop with your dietitian, limiting liquid intake, and taking your medicines as directed.
Peritoneal dialysis vs hemodialysis
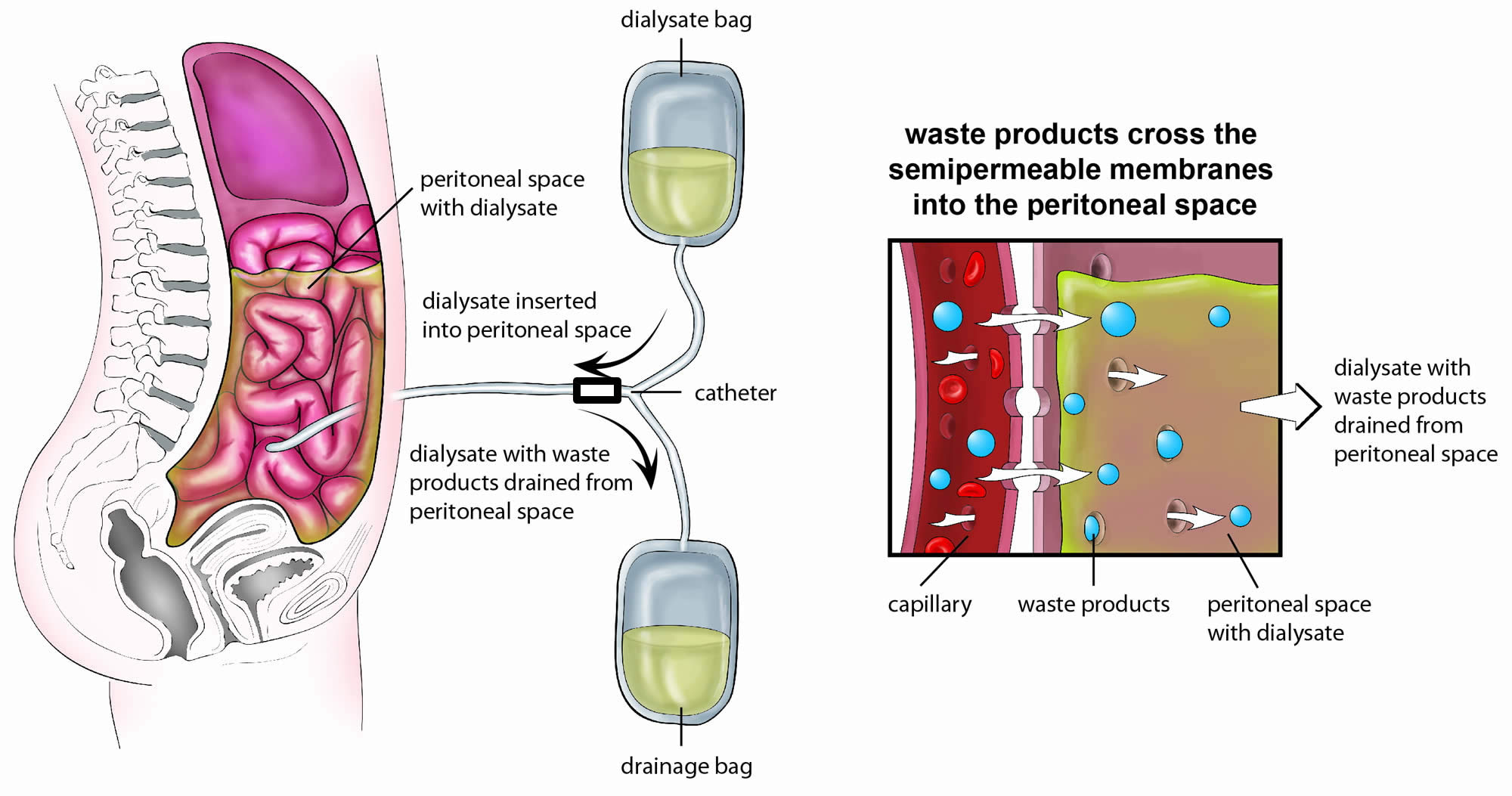
When kidneys fail, waste products such as urea and creatinine build up in the blood. One way to remove these wastes is a process called peritoneal dialysis. Peritoneal dialysis is a treatment for kidney failure that uses the lining of your abdomen, or belly, to filter your blood inside your body. The walls of the abdominal cavity are lined with a membrane called the peritoneum. During peritoneal dialysis, a mixture of dextrose (sugar), salt, and other minerals dissolved in water, called dialysis solution, is placed in a person’s abdominal cavity through a catheter. The body’s peritoneal membrane enclosing the digestive organs allows waste products and extra body fluid to pass from the blood into the dialysis solution. These wastes then leave the body when the used solution is drained from the abdomen. Each cycle of draining and refilling is called an exchange. The time the solution remains in the abdomen between exchanges is called the dwell time. During this dwell time, some of the dextrose in the solution crosses the membrane and is absorbed by the body.
A few weeks before you start peritoneal dialysis, a surgeon places a soft tube, called a catheter, in your belly.
When you start treatment, dialysis solution—water with salt and other additives—flows from a bag through the catheter into your belly. When the bag is empty, you disconnect it and place a cap on your catheter so you can move around and do your normal activities. While the dialysis solution is inside your belly, it absorbs wastes and extra fluid from your body.
After a few hours, the solution and the wastes are drained out of your belly into the empty bag. You can throw away the used solution in a toilet or tub. Then, you start over with a fresh bag of dialysis solution. When the solution is fresh, it absorbs wastes quickly. As time passes, filtering slows. For this reason, you need to repeat the process of emptying the used solution and refilling your belly with fresh solution four to six times every day. This process is called an exchange.
You can do your exchanges during the day, or at night using a machine that pumps the fluid in and out. For the best results, it is important that you perform all of your exchanges as prescribed. Dialysis can help you feel better and live longer, but it is not a cure for kidney failure.
Figure 5. Peritoneal dialysis
How will I feel when the dialysis solution is inside my belly?
You may feel the same as usual, or you may feel full or bloated. Your belly may enlarge a little. Some people need a larger size of clothing. You shouldn’t feel any pain. Most people look and feel normal despite a belly full of solution.
Types of peritoneal dialysis
You can choose the type of peritoneal dialysis that best fits your life:
- continuous ambulatory peritoneal dialysis (CAPD)
- automated peritoneal dialysis
The main differences between the two types of peritoneal dialysis are:
- the schedule of exchanges
- one uses a machine and the other is done by hand
If one type of peritoneal dialysis doesn’t suit you, talk with your doctor about trying the other type.
Continuous ambulatory peritoneal dialysis
Continuous ambulatory peritoneal dialysis (CAPD) doesn’t use a machine. You do the exchanges during the day by hand.
You can do exchanges by hand in any clean, well-lit place. Each exchange takes about 30 to 40 minutes. During an exchange, you can read, talk, watch television, or sleep. With continuous ambulatory peritoneal dialysis (CAPD), you keep the solution in your belly for 4 to 6 hours or more. The time that the dialysis solution is in your belly is called the dwell time. Usually, you change the solution at least four times a day and sleep with solution in your belly at night. You do not have to wake up at night to do an exchange.
Automated peritoneal dialysis
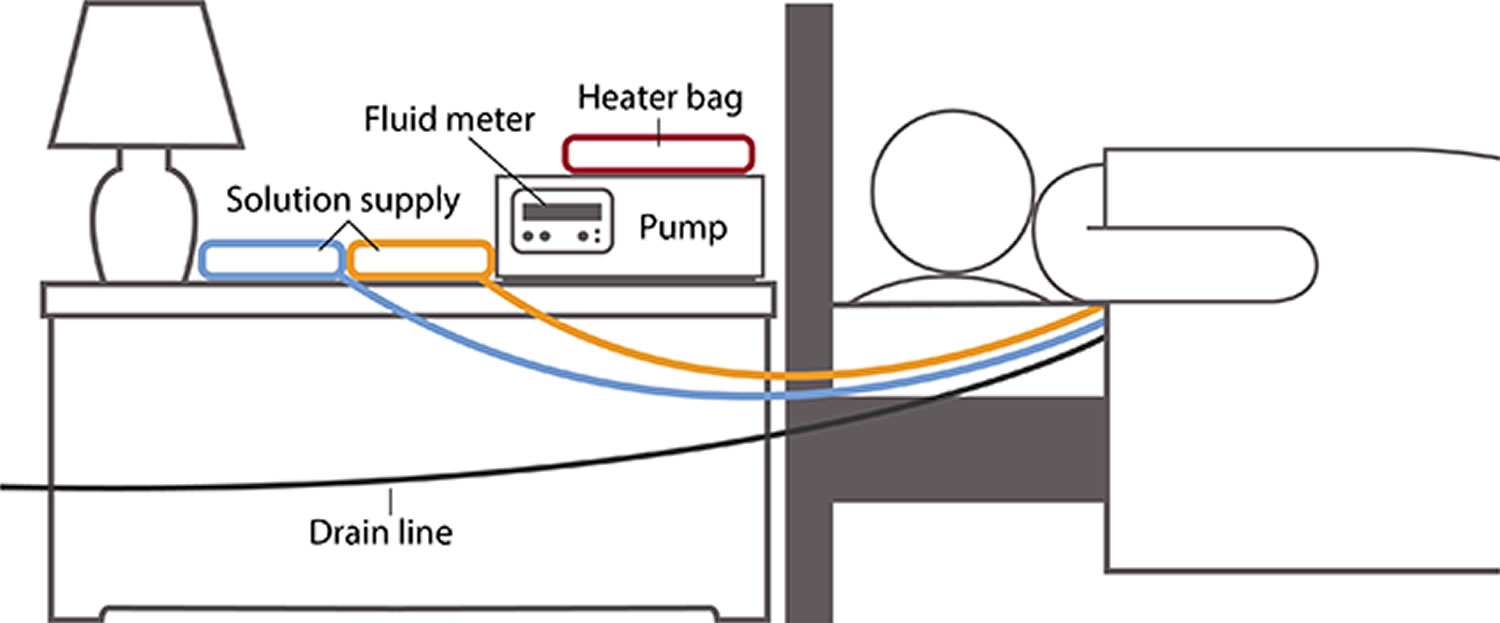
With automated peritoneal dialysis, a machine called a cycler fills and empties your belly three to five times during the night while you sleep. In the morning, you begin the day with fresh solution in your belly. You may leave this solution in your belly all day or do one exchange in the middle of the afternoon without the machine. People sometimes call this treatment continuous cycler-assisted peritoneal dialysis (CCPD).
Figure 6. Automated peritoneal dialysis
Where can I do peritoneal dialysis?
You can do both continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis in any clean, private place, including at home, at work, or when traveling.
Before you travel, you can have the manufacturer ship the supplies to where you’re going so they’ll be there when you get there. If you use automated peritoneal dialysis, you’ll have to carry your machine with you or plan to do exchanges by hand while you’re away from home.
How do I prepare for peritoneal dialysis?
Surgery to put in your catheter
Before your first treatment, you will have surgery to place a catheter into your belly. Planning your catheter placement at least 3 weeks before your first exchange can improve treatment success.
Although you can use the catheter for dialysis as soon as it’s in place, the catheter tends to work better when you have 10 to 20 days to heal before starting a full schedule of exchanges.
Your surgeon will make a small cut, often below and a little to the side of your belly button, and then guide the catheter through the slit into your peritoneal cavity. You’ll receive general or local anesthesia , and you may need to stay overnight in the hospital. However, most people can go home after the procedure.
You’ll learn to care for the skin around the catheter, called the exit site, as part of your dialysis training.
Peritoneal dialysis training
After training, most people can perform both types of peritoneal dialysis on their own. You’ll work with a dialysis nurse for 1 to 2 weeks to learn how to do exchanges and avoid infections. Most people bring a family member or friend to training. With a trained friend or family member, you’ll be prepared in case you have a sick day and need help with exchanges.
If you choose automated peritoneal dialysis, you’ll learn how to:
- prepare the cycler
- connect the bags of dialysis solution
- place the drain tube
If you choose automated peritoneal dialysis, you also need to learn how to do exchanges by hand in case of a power failure or if you need an exchange during the day in addition to nighttime automated peritoneal dialysis.
How do you perform a peritoneal dialysis?
You’ll need the following supplies:
- transfer set
- dialysis solution
- supplies to keep your exit site clean
If you choose automated peritoneal dialysis you’ll need a cycler.
Your health care team will provide everything you need to begin peritoneal dialysis and help you arrange to have supplies such as dialysis solution and surgical masks delivered to your home, usually once a month. Careful hand washing before and wearing a surgical mask over your nose and mouth while you connect your catheter to the transfer set can help prevent infection.
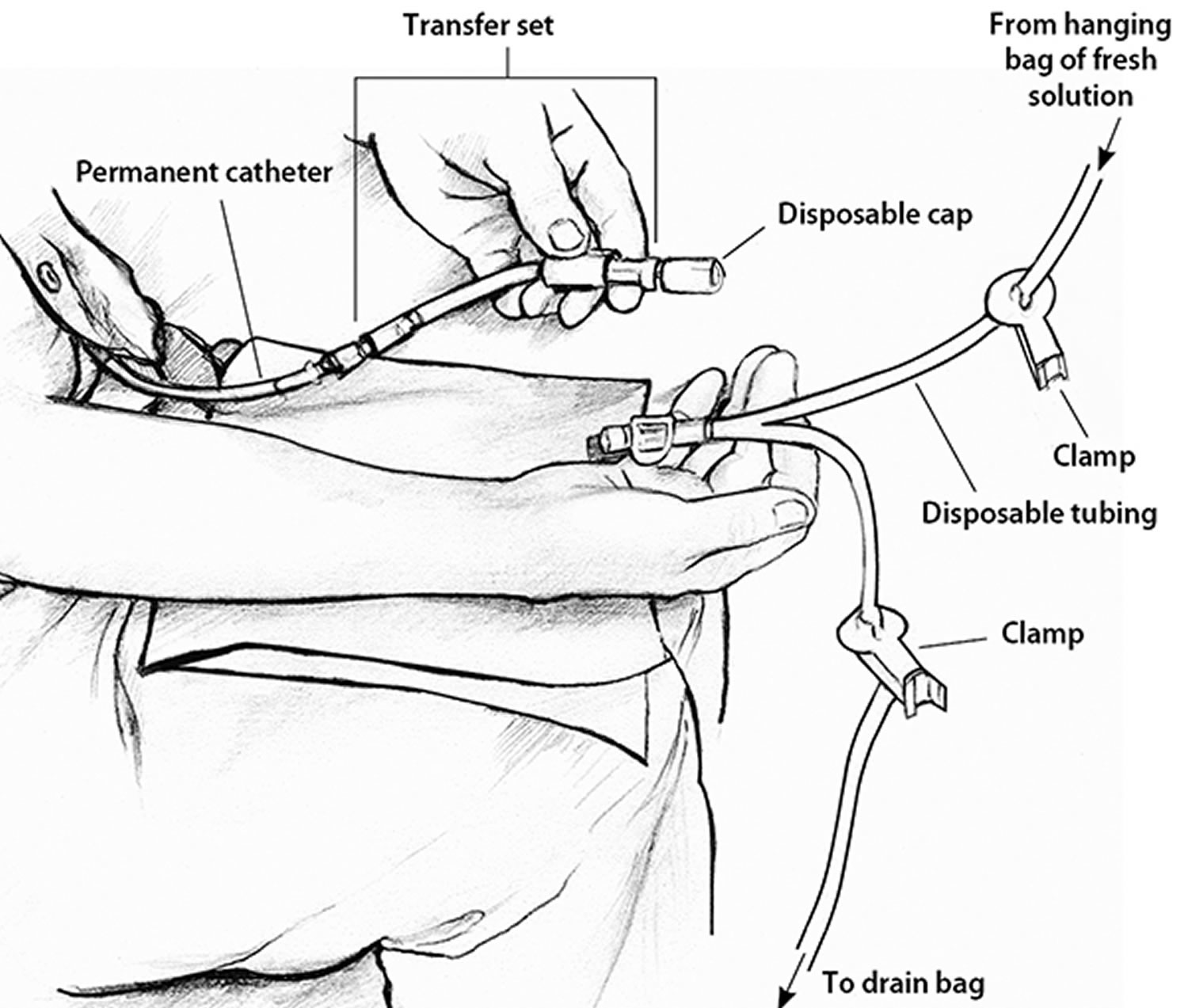
Use a transfer set to connect your catheter to the dialysis solution
A transfer set is tubing that you use to connect your catheter to the bag of dialysis solution. When you first get your catheter, the section of tube that sticks out from your skin will have a secure cap on the end to prevent infection. A connector under the cap will attach to any type of transfer set.
Between exchanges, you can keep your catheter and transfer set hidden inside your clothing. At the beginning of an exchange, you’ll remove the disposable cap from the transfer set and connect the set to a tube that branches like the letter Y. One branch of the Y-tube connects to the drain bag, while the other connects to the bag of fresh dialysis solution.
Figure 7. How to connect your catheter to the transfer set to do your peritoneal dialysis
Use dialysis solution as prescribed
Dialysis solution comes in 1.5-, 2-, 2.5-, or 3-liter bags. Solutions contain a sugar called dextrose or a compound called icodextrin and minerals to pull the wastes and extra fluid from your blood into your belly. Different solutions have different strengths of dextrose or icodextrin. Your doctor will prescribe a formula that fits your needs.
You’ll need a clean space to store your bags of solution and other supplies.
Doing a peritoneal dialysis by hand
- After you wash your hands and put on your surgical mask, drain the used dialysis solution from your belly into the drain bag. Near the end of the drain, you may feel a mild tugging sensation that tells you most of the fluid is gone. Close the transfer set.
- Warm each bag of solution to body temperature before use. You can use an electric blanket, or let the bag sit in a tub of warm water. Most solution bags come in a protective outer wrapper, and you can warm them in a microwave. Don’t microwave a bag of solution after you have removed it from its wrapper.
- Hang the new bag of solution on a pole and connect it to the tubing.
- Remove air from the tubes—allow a small amount of fresh, warm solution to flow directly from the new bag of solution into the drain bag.
- Clamp the tube that goes to the drain bag.
- Open or reconnect the transfer set, and refill your belly with fresh dialysis solution from the hanging bag.
Using a cycler for automated peritoneal dialysis exchanges
In automated peritoneal dialysis, you use a machine called a cycler to fill and drain your belly. You can program the cycler to give you different amounts of dialysis solution at different times.
Each evening, you set up the machine to do three to five exchanges for you. You connect three to five bags of dialysis solution to tubing that goes into the cycler—one bag of solution for each exchange. The machine may have a special tube to connect the bag for the last exchange of the night.
At the times you set, the cycler:
- releases a clamp and allows used solution to drain out of your belly into the drain line
- warms the fresh dialysis solution before it enters your body
- releases a clamp to allow body-temperature solution to flow into your belly
A fluid meter in the cycler measures and records how much solution the cycler removes. Some cyclers compare the amount that was put in with the amount that drains out. This feature lets you and your doctor know if the treatment is removing enough fluid from your body.
Some cyclers allow you to use a long drain line that drains directly into your toilet or bathtub. Others have a disposal container.
What changes will I have to make when I start peritoneal dialysis?
Daily routine
Your schedule will change as you work your dialysis exchanges into your routine. If you do continuous ambulatory peritoneal dialysis (CAPD) during the day, you have some control over when you do the exchanges. However, you’ll still need to stop your normal activities and take about 30 minutes to perform an exchange. If you do automated peritoneal dialysis, you’ll have to set up your cycler every night.
Physical activity
You may need to limit some physical activities when your belly is full of dialysis solution. You may still be active and play sports, but you should discuss your activities with your health care team.
Make changes to what you eat and drink
If you’re on peritoneal dialysis, you may need to limit:
- sodium
- phosphorus
- calories in your eating plan
You may also need to:
- watch how much liquid you drink and eat. Your dietitian will help you determine how much liquid you need to consume each day.
- add protein to your diet because peritoneal dialysis removes protein.
- choose foods with the right amount of potassium.
- take supplements made for people with kidney failure.
Eating the right foods can help you feel better while you’re on peritoneal dialysis. Talk with your dialysis center’s dietitian to find a meal plan that works for you.
Medicines
Your doctor may make changes to the medicines you take.
Coping
Adjusting to the effects of kidney failure and the time you spend on dialysis can be hard for both you and your family. You may:
- have less energy
- need to give up some activities and duties at work or at home
A counselor or social worker can answer your questions and help you cope .
Take care of your exit site, supplies, and catheter to prevent infections
Your health care team will show you how to keep your catheter clean to prevent infections. Here are some general rules:
- Store your supplies in a cool, clean, dry place.
- Inspect each bag of solution for signs of contamination, such as cloudiness, before you use it.
- Find a clean, dry, well-lit space to perform your exchanges.
- Wash your hands every time you need to handle your catheter.
- Clean your skin where your catheter enters your body every day, as instructed by your health care team.
- Wear a surgical mask when performing exchanges.
Peritoneal dialysis possible side effects and complications
Possible complications from peritoneal dialysis include infection, hernia, and weight gain.
Infection
One of the most serious problems related to peritoneal dialysis is infection. You can get an infection of the skin around your catheter exit site or you can develop peritonitis, an infection in the fluid in your belly. Bacteria can enter your body through your catheter as you connect or disconnect it from the bags.
- Seek immediate care if you have signs of infection
Signs of an exit site infection include redness, pus, swelling or bulging, and tenderness or pain at the exit site. Health care professionals treat infections at the exit site with antibiotics.
Peritonitis may cause:
- pain in the abdomen
- fever
- nausea or vomiting
- redness or pain around your catheter
- unusual color or cloudiness in used dialysis solution
- the catheter cuff to push out from your body—the cuff is the part of the catheter that holds it in place
Health care professionals treat peritonitis with antibiotics. Antibiotics are added to the dialysis solution that you can usually take at home. Quick treatment may prevent additional problems.
Hernia
A hernia is an area of weakness in your abdominal muscle.
Peritoneal dialysis increases your risk for a hernia for a couple of reasons. First, you have an opening in your muscle for your catheter. Second, the weight of the dialysis solution within your belly puts pressure on your muscle. Hernias can occur near your belly button, near the exit site, or in your groin. If you have a swelling or new lump in your groin or belly, talk with your health care professional.
Weight gain from fluid and dextrose (glucose)
The longer the dialysis solution remains in your belly, the more dextrose (glucose) your body will absorb from the dialysis solution. This can cause weight gain over time.
Limit weight gain
With continuous ambulatory peritoneal dialysis (CAPD), you might have a problem with the long overnight dwell time. If your body absorbs too much fluid and dextrose overnight, you may be able to use a cycler to exchange your solution once while you sleep. This extra exchange will shorten your dwell time, keep your body from absorbing too much fluid and dextrose, and filter more wastes and extra fluid from your body.
With automated peritoneal dialysis, you may absorb too much solution during the daytime exchange, which has a long dwell time. You may need an extra exchange in the midafternoon to keep your body from absorbing too much solution and to remove more wastes and extra fluid from your body.
Your dietitian can provide helpful guidance to reduce weight gain.
How will you know if your peritoneal dialysis is working?
To find out if your peritoneal dialysis exchanges are removing enough wastes from your body, you’ll have a blood test and collect used dialysis solution once a month. If you’re still urinating, you may need to collect urine.
These tests help your doctor prescribe a dialysis schedule and dose to meet your health needs. If your dialysis schedule isn’t removing enough wastes or your body is absorbing too much dextrose, your doctor will make adjustments.
Many factors affect how much waste and extra fluid are removed from the blood. Some factors—such as the patient’s size and the permeability, or speed of diffusion, of the peritoneum—cannot be controlled. Dialysis solution comes in 1.5-, 2-, 2.5-, or 3-liter bags for manual exchanges and 5- or 6-liter bags for automated exchanges. The dialysis dose can be increased by using a larger fill volume, but only within the limits of the person’s abdominal capacity. Everyone’s peritoneum filters wastes at a different rate. In some people, the peritoneum does not allow wastes to enter the dialysis solution efficiently enough to make peritoneal dialysis feasible.
Other factors that determine how efficiently a person’s blood is filtered can be controlled. Controllable factors include the number of daily exchanges and the dwell times. When fresh solution is first placed in the abdomen, it draws in wastes rapidly. As wastes fill the solution, it cleans the blood less efficiently. For example, a patient may perform one exchange with a 6-hour dwell time, during which the solution pulls in nearly as much urea as it can hold. But in the second half of that dwell time, urea is being removed from the blood very slowly. If the patient performed two exchanges with 3-hour dwell times instead, the amount of urea removed would be substantially greater than that removed in one 6-hour dwell time.
Another way to increase the amount of fluid and waste drawn into the peritoneal cavity is to use dialysis solution with a higher concentration of dextrose. Dialysis solution comes in 1.5 percent, 2.5 percent, and 4.25 percent dextrose (glucose) concentrations. A higher dextrose concentration moves fluid and more wastes into the abdominal cavity, increasing both early and long-dwell exchange efficiency. Eventually, however, the body absorbs dextrose from the solution. As the concentration of dextrose in the body comes closer to that in the solution, dialysis becomes less effective, and fluid is slowly absorbed from the abdominal cavity.
Testing for efficiency of peritoneal dialysis
The tests to see whether the exchanges are removing enough urea are especially important during the first weeks of dialysis, when the health care team needs to determine whether the patient is receiving an adequate amount, or dose, of dialysis.
The peritoneal equilibration test—often called the PET—measures how much dextrose has been absorbed from a bag of infused dialysis solution and how much urea and creatinine have entered into the solution during a 4-hour dwell. The peritoneal transport rate varies from person to person. People who have a high rate of transport absorb dextrose from the dialysis solution quickly, and they should be given a dialysis schedule that avoids exchanges with a long dwell time because they tend to absorb too much dextrose and dialysis solution from such exchanges.
In the clearance test, samples of used solution drained over a 24-hour period are collected, and a blood sample is obtained during the day when the solution is collected. The amount of urea in the solution is compared with the amount in the blood to see how effective the current peritoneal dialysis schedule is in clearing the blood of urea. If the patient has more than a few ounces of urine output per day, the urine should also be collected during this period to measure its urea concentration.
From the used solution, urine, and blood measurements, one can compute a urea clearance, called Kt/V, and a creatinine clearance rate—normalized to body surface area. The residual clearance of the kidneys is also considered. Based on these measurements, one can determine whether the peritoneal dialysis dose is adequate.
If the laboratory results show that the dialysis schedule is not removing enough urea and creatinine, the doctor may change the prescription by:
- increasing the number of exchanges per day for patients treated with continuous ambulatory peritoneal dialysis (CAPD) or per night for patients treated with continuous cycler-assisted peritoneal dialysis (CCPD)
- increasing the volume—amount of solution in the bag—of each exchange in continuous ambulatory peritoneal dialysis (CAPD)
- adding an extra, automated middle-of-the-night exchange to the continuous ambulatory peritoneal dialysis (CAPD) schedule
- adding an extra middle-of-the-day exchange to the continuous ambulatory peritoneal dialysis (CAPD) schedule
- using a dialysis solution with a higher dextrose concentration
Compliance
One of the big problems with peritoneal dialysis is that patients sometimes do not perform all of the exchanges recommended by their medical team. They either skip exchanges or sometimes skip entire treatment days when using continuous cycler-assisted peritoneal dialysis (CCPD). Skipping peritoneal dialysis treatments has been shown to increase the risk of hospitalization and death.
Residual Kidney Function
Normally the peritoneal dialysis prescription factors in the amount of residual kidney function. Residual function typically falls, although slowly, over the months or even years of treatment with peritoneal dialysis. This means that, more often than not, the number of peritoneal dialysis exchanges prescribed, or the volume of exchanges, needs to be increased as residual function falls.
Your doctor should determine your dose of peritoneal dialysis on the basis of practice guidelines published by the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative. Your health care provider should work closely with you to ensure that the proper peritoneal dialysis dose is administered. To maximize your health and prolong your life, you should follow instructions carefully to get the most out of your dialysis exchanges.
Hemodialysis diet
The renal dietitian at your dialysis center will help you plan a diet for your special needs.
Use this as a guide only until your dietitian prepares a personalized meal plan for you. You will need to:
- Eat more high protein foods.
- Eat less high salt, high potassium, and high phosphorus foods.
- Learn how much fluid you can safely drink (including coffee, tea, and water).
You will need to carefully plan your meals and keep track of the amount of liquids you eat and drink. It helps to limit or avoid foods and beverages that have lots of:
- potassium
- phosphorus
- sodium—for example, vegetable juice and sports drinks
Why is it important to keep track of how much liquid you eat and drink?
You may feel better if you keep track of and limit how much liquid you eat and drink. Excess fluid can build up in your body and may cause:
- swelling and weight gain between dialysis sessions
- changes in your blood pressure
- your heart to work harder, which can lead to serious heart trouble
- a buildup of fluid in your lungs, making it hard for you to breathe
Hemodialysis removes extra fluid from your body. However, hemodialysis can remove only so much fluid at a time safely. If you come to your hemodialysis with too much fluid in your body, your treatment may make you feel ill. You may get muscle cramps or have a sudden drop in blood pressure that causes you to feel dizzy or sick to your stomach.
Your health care provider can help you figure out how much liquid is right for you.
One way to limit how much liquid you have is to limit the salt in the foods you eat. Salt makes you thirsty, so you drink more. Avoid salty foods such as chips and pretzels.
Your renal dietitian will give you other tips to help you limit how much liquid you consume while making sure you don’t feel too thirsty.
What foods count as liquid and why?
Foods that are liquid at room temperature, such as soup, contain water. Gelatin, pudding, ice cream, and other foods that include a lot of liquid in the recipe also count. Most fruits and vegetables contain water, such as melons, grapes, apples, oranges, tomatoes, lettuce, and celery. When you count up how much liquid you have in a day, be sure to count these foods.
What is my dry weight?
Your dry weight is your weight after a hemodialysis session has removed all extra fluid from your body. Controlling your liquid intake helps you stay at your proper dry weight. If you let too much fluid build up between sessions, it is harder to achieve your dry weight. Your health care provider can help you figure out what dry weight is right for you.
My dry weight goal: _____________.
Why you need to be on a special hemodialysis diet?
Because your kidneys are not able to get rid of enough waste products and fluids from your blood and your body now has special needs, you will need to limit fluids and change your intake of certain foods in your diet. How well you feel will depend on:
- eating the right kind and amounts of food from your diet
- having the hemodialysis treatments your doctor orders for you
- taking the medications your doctor orders for you.
Your diet is very important to your care. It is important that you have the right amount of protein, calories, fluids, vitamins and minerals each day. Your dietitian will help you plan your meals to make sure you get the proper balance.
Is there anything else I should know?
The following important tips can be helpful with your diet:
- Fresh or plain frozen vegetables contain no added salt. Drain all the cooking fluid before serving.
- Canned fruits usually contain less potassium than fresh fruits. Drain all the fluid before serving.
- Non-dairy creamers are low in phosphorus and can be used in place of milk.
- Labels on food packages will give you information about some of the ingredients that may not be allowed in your diet. Learn to read these labels.
- To help you avoid salt, many herbs and spices can be used to make your diet more interesting. Check with your dietitian for a list of these.
What if I have high cholesterol?
Changing your diet may help lower the cholesterol level in your blood. Your dietitian will talk with you about the kinds of fat and animal foods you eat. Also, your doctor may decide you need a special medication to reduce the cholesterol in your blood.
What if I have diabetes?
In some cases, you may need to make only a few changes in your diet to fit your needs as a kidney patient. For example, some of the free foods you have been using may need to be limited on your kidney diet. Your dietitian will help develop a meal plan especially for you.
What you need to know about potassium
Healthy kidneys keep the right amount of potassium in your blood to keep your heart beating at a steady pace. Potassium levels can rise between hemodialysis sessions and affect your heartbeat. Eating too much potassium can be dangerous to your heart and may even cause death.
To control potassium levels, limit potassium-rich foods such as avocados, bananas, kiwis, and dried fruit. Choose fruits and vegetables that are lower in potassium. Have very small portions of foods that are higher in potassium, such as one or two cherry tomatoes on a salad or a few raisins in your oatmeal.
You can remove some of the potassium from potatoes by dicing or shredding them and then boiling them in a full pot of water.
Your renal dietitian will give you more specific information about the potassium content of foods.
What you need to know about phosphorus
Too much phosphorus in your blood pulls calcium from your bones. Losing calcium may make your bones weak and likely to break. Also, too much phosphorus may make your skin itch. Limiting phosphorus can be hard because foods that contain phosphorus, such as meat and milk, also contain the protein you need. You should be careful to eat enough protein; however, not so much that you get too much phosphorus. Processed and packaged foods contain especially high levels of phosphorus. You can also find phosphorus naturally in foods such as poultry, fish, nuts, peanut butter, beans, cola, tea, and dairy products. Usually, people on hemodialysis should only have a 1/2 cup of milk per day. Your renal dietitian will give you more specific information about phosphorus.
You may need to take a phosphate binder such as sevelamer (Renvela), calcium acetate (PhosLo), lanthanum carbonate (Fosrenol), or calcium carbonate to control the phosphorus in your blood between hemodialysis sessions. These medicines act like plastic bags with zip tops. The phosphorus binder “seals” the phosphorus from food and moves it out through stool so the phosphorous does not enter the bloodstream.
What you need to know about protein
Renal dietitians encourage most people on hemodialysis to eat high-quality protein because it produces less waste for removal during dialysis. High-quality protein comes from meat, poultry, fish, and eggs. Avoid processed meats such as hot dogs and canned chili, which have high amounts of sodium and phosphorus.
What you need to know about sodium
Sodium is a part of salt. Sodium is found in many canned, packaged, frozen, and fast foods. Sodium is also found in many condiments, seasonings, and meats. Too much sodium makes you thirsty, which makes you drink more liquid.
- Use less salt and eat fewer salty foods: this may help to control blood pressure and reduce weight gains between dialysis sessions.
- Use herbs, spices, and low-salt flavor enhancers in place of salt.
- Avoid salt substitutes made with potassium.
Try to eat fresh, naturally low-sodium foods. Look for products labeled “low sodium,” especially in canned and frozen foods.
Do not use salt substitutes because they contain potassium. Talk with your renal dietitian about spices you can use to flavor your food. Your renal dietitian can help you find spice blends without sodium or potassium.
What you need to know about calories
All foods contain calories, and you need calories for energy. Many people on hemodialysis do not have a good appetite and do not get enough calories. If you find you do not feel like eating, talk with your renal dietitian to find healthy ways to add calories to your diet. Vegetable oils—such as olive oil, canola oil, and safflower oil—are good sources of calories and are the healthiest way to add fat to your diet if you need to gain weight. Use them generously on breads, rice, and noodles only if your renal dietitian tells you to add calories to your diet.
Butter and margarines are rich in calories; however, they are mainly saturated fat. Saturated fats and trans fats can clog your arteries. Use them less often. Soft margarine that comes in a tub is better than stick margarine. Choose a soft margarine with less saturated and trans fats.
Talk with your renal dietitian about the types and amounts of fat you need in your diet. Everyone will have different needs that a renal dietitian can help address.
Hard candy, sugar, honey, jam, and jelly provide calories and energy without fat or adding other things that your body does not need. If you have diabetes, be careful about eating sweets and talk with your renal dietitian before adding sweets to your food plan.
Should you take vitamin and mineral supplements?
You may not get enough vitamins and minerals in your diet because you have to avoid so many foods. Hemodialysis also removes some vitamins from your body. Your health care provider may prescribe a vitamin and mineral supplement designed specifically for people with kidney failure.
Warning: Do not take nutritional supplements you can buy over the counter. These supplements may contain vitamins or minerals that are harmful to you. For safety reasons, talk with your health care provider before using probiotics, dietary supplements, or any other medicine together with or in place of the treatment your health care provider prescribes.
Meat and Protein
People on dialysis need to eat more protein. Protein can help maintain blood protein levels and improve health. Eat a high protein food (meat, fish, poultry, fresh pork, or eggs) at every meal, or about 8-10 ounces of high protein foods everyday.
3 ounce = the size of a deck of cards, a medium pork chop, a ¼ pound hamburger patty, ½ chicken breast, a medium fish fillet.
1 ounce = 1 egg or ¼-cup egg substitute, ¼-cup tuna, ¼-cup ricotta cheese, 1 slice of low sodium lunchmeat.
Note: Even though peanut butter, nuts, seeds, dried beans, peas, and lentils have protein, these foods are generally not recommended because they are high in both potassium and phosphorus.
Grains/Cereals/Bread
Unless you need to limit your calorie intake for weight loss and/or manage carbohydrate intake for blood sugar control, you may eat, as you desire from this food group. Grains, cereals, and breads are a good source of calories. Most people need 6 -11 servings from this group each day.
Avoid “whole grain” and “high fiber” foods (like whole wheat bread, bran cereal and brown rice) to help you limit your intake of phosphorus. By limiting dairy–based foods you protect your bones and blood vessels.
Amounts equal to one serving:
- 1 slice bread (white, rye, or sourdough)
- ½ English muffin
- ½ bagel
- ½ hamburger bun
- ½ hot dog bun
- 1 6-inch tortilla
- ½ cup cooked pasta
- ½ cup cooked white rice
- ½ cup cooked cereal (like cream of wheat)
- 1 cup cold cereal (like corn flakes or crispy rice)
- 4 unsalted crackers
- 1½ cups unsalted popcorn
- 10 vanilla wafers
Milk/Yogurt/Cheese
Limit your intake of milk, yogurt, and cheese to ½-cup milk or ½-cup yogurt or 1-ounce cheese per day. Most dairy foods are very high in phosphorus.
The phosphorus content is the same for all types of milk – skim, low fat, and whole! If you do eat any high-phosphorus foods, take a phosphate binder with that meal.
Dairy foods “low” in phosphorus (ask your dietitian about the serving size that is right for you):
- Butter and tub margarine
- Cream cheese
- Heavy cream
- Ricotta cheese
- Brie cheese
- Non-dairy whipped topping
- Sherbet
If you have or are at risk for heart disease, some of the high fat foods listed above may not be good choices for you.
Certain brands of non-dairy creams and “milk” (such as rice milk) are low in phosphorus and potassium. Ask your dietitian for details.
Fruit/Juice
All fruits have some potassium, but certain fruits have more than others and should be limited or totally avoided. Limiting potassium protects your heart.
Always AVOID star fruit (carambola).
- Eat 2-3 servings of low potassium fruits each day.
- One serving = ½-cup or 1 small fruit or 4 ounces of juice.
Limit or avoid:
- Oranges and orange juice
- Kiwis
- Nectarines
- Prunes and prune juice
- Raisins and dried fruit
- Bananas
- Melons (cantaloupe and honeydew)
Choose:
- Apple (1)
- Berries (½ cup)
- Cherries (10)
- Fruit cocktail, drained (½ cup)
- Grapes (15)
- Peach (1 small fresh or canned, drained)
- Pear, fresh or canned, drained (1 halve)
- Pineapple (½ cup canned, drained)
- Plums (1-2)
- Tangerine (1)
- Watermelon (1 small wedge)
Drinks:
- Apple cider
- Cranberry juice cocktail
- Grape juice
- Lemonade
Vegetables and Salads
All vegetables have some potassium, but certain vegetables have more than others and should be limited or totally avoided. Limiting potassium intake protects your heart.
Eat 2-3 servings of low-potassium vegetables each day. One serving = ½-cup.
Choose:
- Broccoli (raw or cooked from frozen)
- Cabbage
- Carrots
- Cauliflower
- Celery
- Cucumber
- Eggplant
- Garlic
- Green and Wax beans (“string beans”)
- Lettuce-all types (1 cup)
- Onion
- Peppers-all types and colors
- Radishes
- Watercress
- Zucchini and Yellow squash
Limit or avoid:
- Potatoes (including French Fries, potato chips and sweet potatoes)
- Tomatoes and tomato sauce
- Winter squash
- Pumpkin
- Asparagus (cooked)
- Avocado
- Beets
- Beet greens
- Cooked spinach
- Parsnips and rutabaga
Dessert
Depending on your calorie needs, your dietitian may recommend high-calorie deserts. Pies, cookies, sherbet, and cakes are good choices (but limit dairy-based desserts and those made with chocolate, nuts, and bananas). If you are a diabetic, discuss low carbohydrate dessert choices with your dietitian.
Sample Menu
This meal plan provides 2150 Calories, 91 grams protein, 2300 mg sodium, 1800 mg (46 mEq) potassium, 950 mg phosphorus. 38 ounces of oral fluid.
Breakfast
- Cranberry Juice, 4 ounces
- Eggs (2) or ½-cup egg substitute
- Toasted white bread, 2 slices, with Butter or tub margarine or fruit spread
- Coffee, 6 ounces
Lunch
- Tuna salad sandwich made with 3 ounces tuna on a hard roll with lettuce and mayonnaise.
- (Other good choices for sandwiches include egg and chicken salad, lean roast beef, low salt ham and turkey breast.)
- Coleslaw, ½-cup
- Pretzels (low salt)
- Canned and drained peaches, ½-cup
- Ginger Ale, 8 ounces
Cola drinks are high in phosphorus. Choose ginger ale or lemon-lime beverages instead.
Dinner
- Hamburger patty, 4 ounces on a bun with 1-2 teaspoons ketchup
- Salad (1 cup): lettuce, cucumber, radishes, peppers, with olive oil and vinegar dressing
- Lemonade, 8 ounces
Aim for at least 2-3 “fish” meals each week. Many fish are rich in heart-healthy “omega-3” fats. Tuna and salmon (rinsed or canned without salt) and shellfish are excellent heart healthy protein choices.
Snack/Dessert
- Milk, 4 ounces
- Slice of apple pie
How will I know if I am eating right to keep me healthy?
Because you are on dialysis, you have some very special needs. Eating well helps you stay healthy. Eating poorly can increase your risk of illness. Your dietitian will talk with you about how well you are eating.
Some questions you might be asked:
- Have you noticed a change in the kind or amount of food you eat each day?
- Have you had any problems eating your usual or recommended diet?
- Have you lost weight without trying?
- Have you noticed any changes in your strength or ability to take care of yourself?
Your dietitian or nurse might look at the fat and muscle stores in your face, hands, arms, shoulders, and legs. Your dialysis care team will look for changes in your blood level of proteins, and especially one called albumin. A change in this protein can mean that you are losing body protein.
Some special blood tests that are done each month are called Kt/V or urea reduction ratio. These tests help your doctor decide if you are getting enough dialysis. Getting the right amount of dialysis is important to help you feel your best.
A change in your fat and muscle stores or any of these blood tests could be a sign that you are not getting enough dialysis. Along with the Kt/V, these tests provide information about your intake of protein or your protein equivalent of nitrogen appearance. Using the protein equivalent of nitrogen appearance, your albumin and any changes in your appetite, your dietitian will determine if you are eating enough of the right foods. The right amount of dialysis is needed to make sure you are able to enjoy your food while keeping you healthy.
- Kidney Failure Treatment Options – Comparison Chart. https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/choosing-treatment/comparison-chart[↩][↩]
- Hall YN, Larive B, Painter P, et al. Effects of six versus three times per week hemodialysis on physical performance, health, and functioning: Frequent Hemodialysis Network (FHN) randomized trials. Clinical Journal of the American Society of Nephrology. 2012;7(5):782–794.[↩]
- McCann M, Einarsdottir H, Van Waeleghem JP, Murphy F, Sedgewick J. Vascular access management 1: an overview. J Ren Care. (2008);34: 77–84. doi: 10.1111/j.1755-6686.2008.00022.x https://www.ncbi.nlm.nih.gov/pubmed/18498572[↩]
- National Kidney Foundation: K/DOQI clinical practice guidelines for hemodialysis adequacy, 2000. American Journal of Kidney Disease. 2001;37(suppl 1):S7-S64.[↩]





{kind=link}