Contents
What is hemothorax
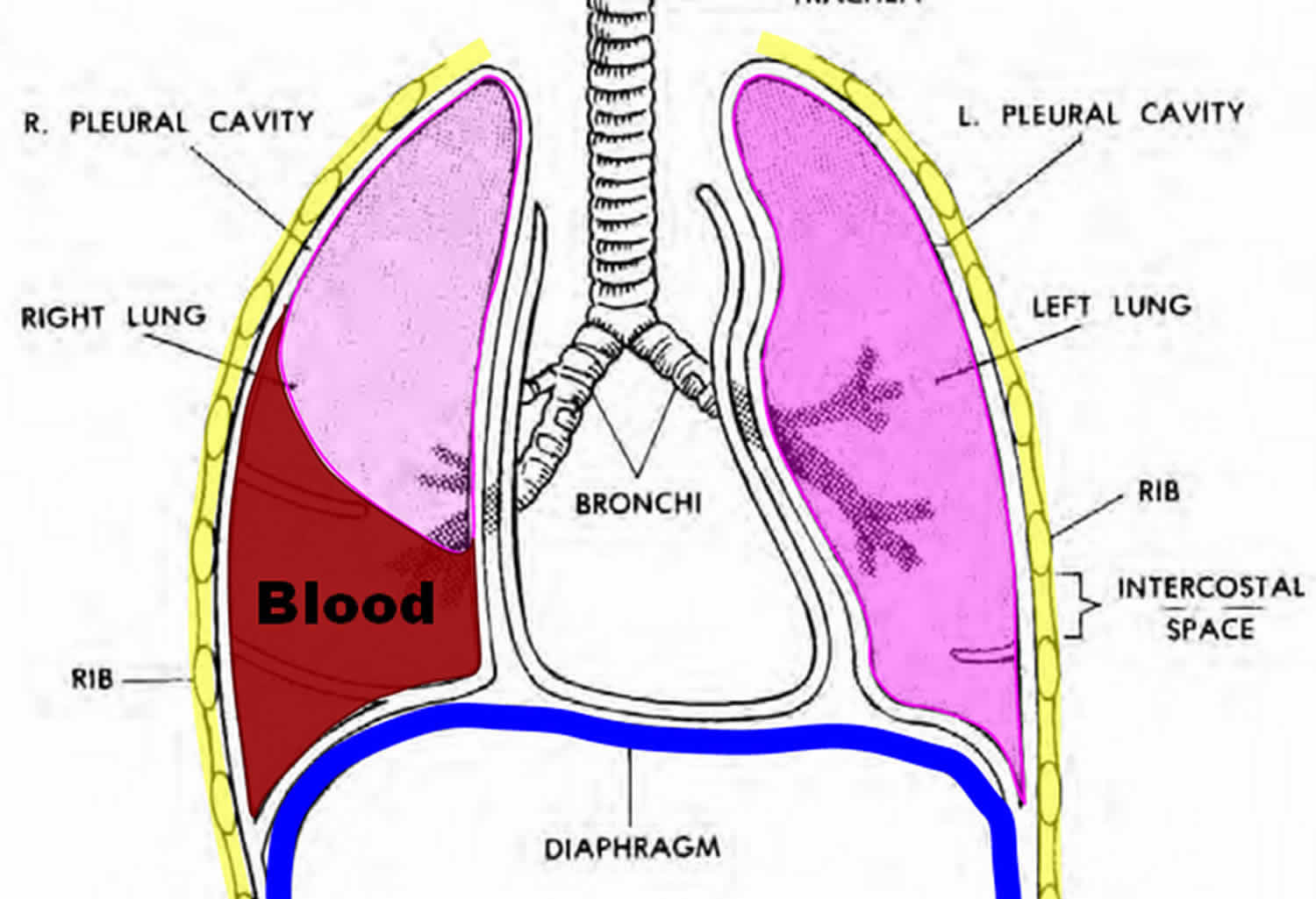
Hemothorax is a collection of blood in the space between the chest wall and the lung (the pleural cavity). A hemothorax is sometimes defined by pleural fluid with a hematocrit > 50% of the blood hematocrit. If a hemothorax occurs concurrently with a pneumothorax (collapsed lung) it is then termed a hemopneumothorax.
A tension hemothorax refers to hemothorax that results from massive intrathoracic bleeding, causing ipsilateral lung compression and mediastinal displacement 1.
Call your local emergency services number for an ambulance if you have:
- Any serious injury to the chest
- Chest pain or shortness of breath
Go to the emergency room or call your local emergency number if you have:
- Dizziness, lightheadedness, fever and cough, or a feeling of heaviness in your chest
- Severe chest, neck, jaw, shoulder or arm pain
- Severe difficulty breathing
Tension hemothorax
A tension hemothorax refers to hemothorax that exert considerable mass effect. It often results from massive intrathoracic hemorrhage and often causing ipsilateral lung compression and mediastinal displacement 2.
Figure 1. Hemothorax
Hemothorax vs Pneumothorax
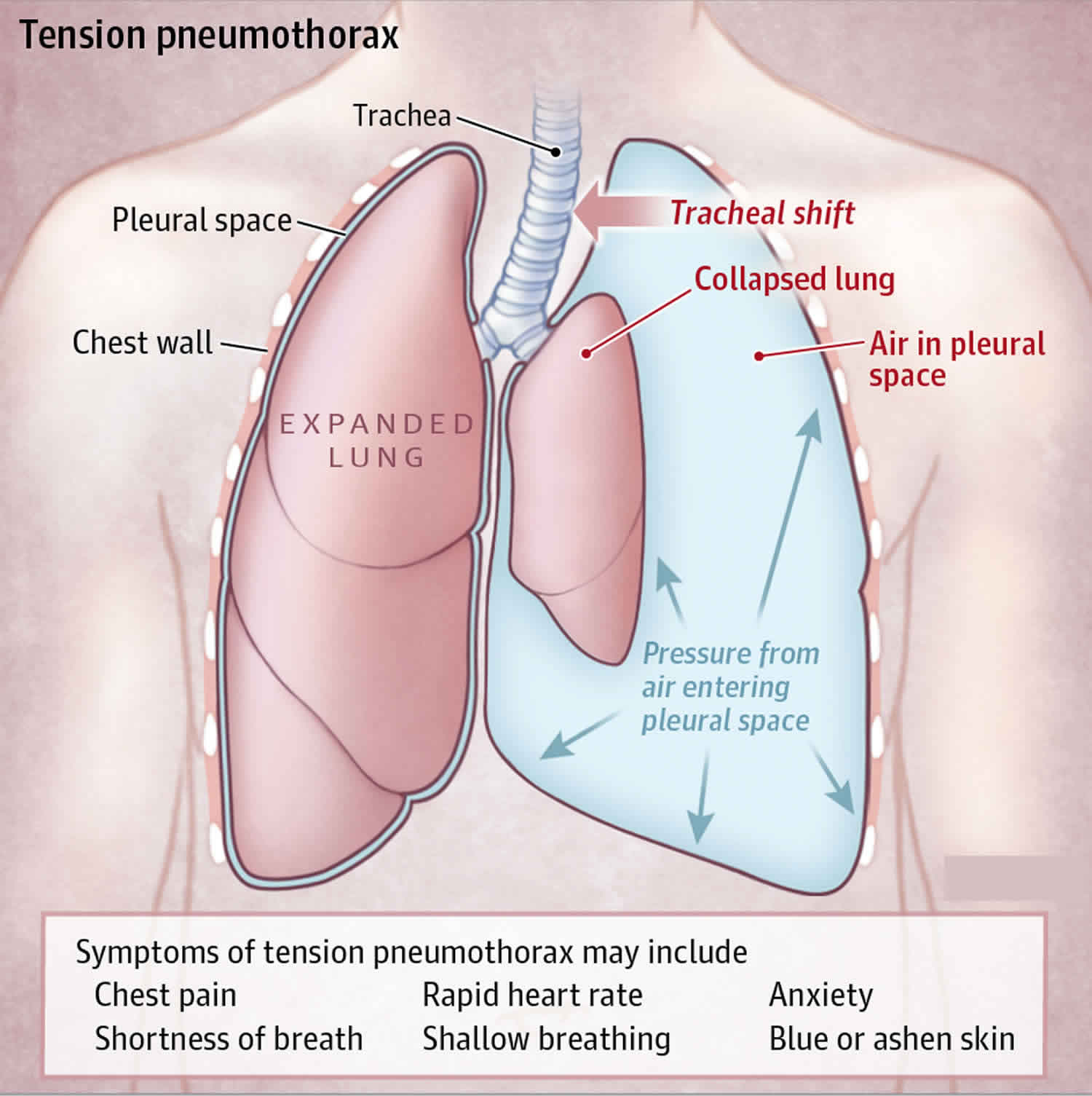
A pneumothorax is a collapsed lung. A pneumothorax occurs when air leaks into the space (pleural cavity) between your lung and chest wall. This air pushes on the outside of your lung and makes it collapse, so your lung cannot expand as much as it normally does when you take a breath. In most cases, only a portion of the lung collapses.
A pneumothorax can be caused by a blunt or penetrating chest injury (e.g., gunshot or knife wound to the chest, rib fracture), certain medical procedures, or damage from underlying lung disease. In some cases, a collapsed lung is caused by air blisters (blebs) that break open, sending air into the space around the lung. This can result from air pressure changes such as when scuba diving or traveling to a high altitude. Or pneumothorax may occur for no obvious reason.
Tall, thin people and smokers are more at risk for a pneumothorax.
Lung diseases can also increase the chance of getting a pneumothorax. These include:
- Asthma
- Chronic obstructive pulmonary disease (COPD)
- Cystic fibrosis
- Tuberculosis
- Whooping cough
Symptoms usually include sudden chest pain and shortness of breath. On some occasions, a collapsed lung can be a life-threatening event.
Treatment for a pneumothorax usually involves inserting a flexible tube or needle between the ribs to remove the excess air. However, a small pneumothorax may heal on its own.
Figure 2. Pneumothorax
Pneumothorax causes
A pneumothorax can be caused by:
- Chest injury. Any blunt or penetrating injury to your chest can cause lung collapse. Some injuries may happen during physical assaults or car crashes, while others may inadvertently occur during medical procedures that involve the insertion of a needle into the chest.
- Lung disease. Damaged lung tissue is more likely to collapse. Lung damage can be caused by many types of underlying diseases, including chronic obstructive pulmonary disease (COPD), cystic fibrosis and pneumonia.
- Ruptured air blisters. Small air blisters (blebs) can develop on the top of your lung. These blebs sometimes burst — allowing air to leak into the space that surrounds the lungs.
- Mechanical ventilation. A severe type of pneumothorax can occur in people who need mechanical assistance to breathe. The ventilator can create an imbalance of air pressure within the chest. The lung may collapse completely.
Risk factors for a pneumothorax
Risk factors for a pneumothorax include:
- Your sex. In general, men are far more likely to have a pneumothorax than are women.
- Smoking. The risk increases with the length of time and the number of cigarettes smoked, even without emphysema.
- Age. The type of pneumothorax caused by ruptured air blisters is most likely to occur in people between 20 and 40 years old, especially if the person is a very tall and underweight.
- Genetics. Certain types of pneumothorax appear to run in families.
- Lung disease. Having an underlying lung disease — especially chronic obstructive pulmonary disease (COPD) — makes a collapsed lung more likely.
- Mechanical ventilation. People who need mechanical ventilation to assist their breathing are at higher risk of pneumothorax.
- Previous pneumothorax. Anyone who has had one pneumothorax is at increased risk of another, usually within one to two years of the first.
Pneumothorax smptoms
The main symptoms of a pneumothorax are sudden chest pain and shortness of breath. But these symptoms can be caused by a variety of health problems, and some can be life-threatening. If your chest pain is severe or breathing becomes increasingly difficult, get immediate emergency care.
Common symptoms of a collapsed lung include:
- Sharp chest or shoulder pain, made worse by a deep breath or a cough
- Shortness of breath
- Nasal flaring (from shortness of breath)
A larger pneumothorax causes more severe symptoms, including:
- Bluish color of the skin due to lack of oxygen (cyanosis)
- Chest tightness
- Lightheadedness and near fainting
- Easy fatigue
- Rapid heart rate
- Shock and collapse
Pneumothorax complications
Many people who have had one pneumothorax can have another, usually within one to two years of the first. Air may sometimes continue to leak if the opening in the lung won’t close. Surgery may eventually be needed to close the air leak.
Shock, if there are serious injuries or infection, severe inflammation, or fluid in the lung develops.
Pneumothorax diagnosis
Your health care provider will listen to your breathing with a stethoscope. If you have a collapsed lung, there are decreased breath sounds or no breath sounds on the affected side. You may also have low blood pressure.
Tests that may be ordered include:
- Arterial blood gases and other blood tests
- Chest x-ray
- CT scan if other injuries or conditions are suspected
- Electrocardiogram
A pneumothorax is generally diagnosed using a chest X-ray. In some cases, a computerized tomography (CT) scan may be needed to provide more-detailed images. CT scanners combine X-ray images taken from many different directions to produce cross-sectional views of internal structures.
Pneumothorax treatment
The goal in treating a pneumothorax is to relieve the pressure on your lung, allowing it to re-expand. Depending on the cause of the pneumothorax, a second goal may be to prevent recurrences. The methods for achieving these goals depend on the severity of the lung collapse and sometimes on your overall health.
Observation
If only a small portion of your lung is collapsed, your doctor may simply monitor your condition with a series of chest X-rays until the excess air is completely absorbed and your lung has re-expanded. Normally this takes a week or two. Supplemental oxygen may speed the absorption process.
Needle or chest tube insertion
If a larger area of your lung has collapsed, it’s likely that a needle or chest tube will be used to remove the excess air.
The hollow needle or tube is inserted between the ribs into the air-filled space that is pressing on the collapsed lung. With the needle, a syringe is attached so that the doctor can pull out the excess air — just like a syringe is used to pull blood from a vein. A chest tube may be attached to a suction device that continuously removes air from the chest cavity.
Surgery
If a chest tube doesn’t solve your pneumothorax, surgery may be necessary to close the air leak. In most cases, the surgery can be performed through small incisions, using a tiny fiber-optic camera and narrow, long-handled surgical tools. The surgeon will look for the leaking bleb and close it off.
In some cases, a substance may be used to irritate the tissues around the lung so that they’ll stick together and seal any leaks. Rarely, the surgeon will have to make a larger incision between the ribs to get better access to multiple or larger air leaks.
Pneumothorax prognosis
If you have a collapsed lung, you are more likely to have another one in the future if you:
- Are tall and thin
- Continue to smoke
- Have had two collapsed lungs in the past
How well you do after having a collapsed lung depends on what caused it.
Hemothorax causes
The most common cause of hemothorax is penetrating or blunt trauma to the chest (traumatic hemothorax) 3.
A hemothorax can also result without any trauma and, in these situations, it is termed a spontaneous hemothorax. This can occur in the setting of 4:
- Lung or pleural cancer — primary or secondary (metastatic, or from another site)
- usually occurs with thoracic wall tumors
- thoracic wall schwanommas
- thoracic wall neurofibromas
- soft-tissue tumors
- sarcomas: thoracic angiosarcomas
- hepatocellular carcinomas: with thoracic invasion or thoracic metastases
- lung cancer is a distinctly uncommon cause of hemothorax even in the setting of pleural extension 4
- Spontaneous pneumothorax – spontaneous hemopneumothorax
- Anticoagulant medication
- Vascular rupture
- aortic dissection
- rupture of coronary arteries such as right coronary artery during an angioplasty
- thoracic arteriovenous malformations
- pulmonary arteriovenous malformation 5
- thoracic endometriosis
- death of lung tissue (pulmonary infarction)
- pleural adhesions with pneumothorax
- hematologic abnormalities: coagulopathy
- hemophilia or blood clotting defect
- connective tissue disease
- Ehlers-Danlos syndrome type 4: has been associated with hemothorax in the setting of internal mammary artery rupture
- Congenital bony exostoses
- Chest (thoracic) or heart surgery
- Tear in a blood vessel when placing a central venous catheter or when associated with severe high blood pressure
- Tuberculosis
Hemothorax prevention
Use safety measures (such as seat belts) to avoid injury. Depending on the cause, a hemothorax may not be preventable.
Hemothorax signs and symptoms
Hemothorax symptoms include:
- Anxiety
- Chest pain
- Low blood pressure (shock)
- Pale, cool and clammy skin
- Rapid heart rate
- Rapid, shallow breathing
- Restlessness
- Shortness of breath
Hemothorax possible complications
Hemothorax complications may include:
- Collapsed lung, or pneumothorax, leading to respiratory failure (inability to breathe properly, provide the body enough oxygen and remove carbon dioxide)
- Fibrosis or scarring of the pleural membranes and underlying lung tissue
- Infection of the pleural fluid (empyema)
- Pneumonia
- Shock and death in severe circumstances
Hemothorax diagnosis
Your health care provider will listen to your breathing with a stethoscope. If you have a hemothorax, there are decreased breath sounds or absent breath sounds on the affected side.
Signs or findings of hemothorax may be seen on the following tests:
- Chest x-ray
- CAT or CT scan
- Pleural fluid analysis (often very bloody or blood-tinged)
- Thoracentesis (drainage of pleural fluid through a needle or catheter)
Plain radiograph
Chest radiographic appearance of a large hemothorax may be similar to that of pleural effusion. It can be almost impossible to differentiate a hemothorax from other causes of pleural effusions.
Ultrasound
May have a very high sensitivity (92%), specificity (100%) positive predictive values (100%) and negative predictive values (98%) in detection of a hemothorax the context of preceding trauma 2.
CT scan
CT scan is useful in determining the nature of the pleural fluid in the setting of trauma by assessing the attenuation value. Blood in the pleural space typically has an attenuation of 35-70 HU 6. Pleural fluid attenuation measurement should be routine in the interpretation of chest trauma CT to distinguish simple fluid from acute blood.
In the setting of trauma, there may be other ancillary features such as pulmonary contusions and lacerations.
Hemothorax treatment
The exact management strategy will depend on underlying cause. In general hemothorax management options include:
- drainage for symptomatic therapy
For a clotted hemothorax options include:
- video-assisted thoracoscopic surgery (VATS)
- intrapleural fibrinolytic therapy
The goal of treatment is to get the person stable, stop the bleeding, and remove the blood and air in the pleural space.
- A chest tube is inserted through the chest wall between the ribs to drain the blood and air.
- It is left in place and attached to suction for several days to re-expand the lung.
If a chest tube alone does not control the bleeding, surgery (thoracotomy) may be needed to stop the bleeding.
The cause of the hemothorax will be also treated. The underlying lung may have collapsed. This can lead to breathing difficulty. In people who have had an injury, chest tube drainage may be all that is needed. Surgery may not be necessary.
What to expect at the emergency department
Your doctor will measure and monitor the person’s vital signs, including temperature, pulse, breathing rate, and blood pressure. Symptoms will be treated as needed. The person may receive:
- Breathing support — This may include oxygen, endotracheal intubation (tube through the nose or mouth into the trachea) and ventilator (breathing machine)
- Blood tests and possible blood transfusion
- Chest tube (tube through the skin and muscles between the ribs into the space around the lungs) if there is lung collapse
- CAT/CT scan
- Pleural fluid analysis (fluid is often very bloody or blood-tinged)
- EKG/ECG
- Fluids given through the vein (IV)
- Medicines to treat symptoms
- X-rays of chest and abdomen or other parts of the body if there are additional injuries
Hemothorax chest tube
A chest tube, also known as a thoracostomy tube, is a flexible tube that can be inserted through the chest wall between the ribs into the pleural space.
Doctors use a chest tube into create negative pressure in your chest cavity and allow re-expansion of your lung. A chest tube helps remove air (pneumothorax), blood (hemothorax), fluid (pleural effusion or hydrothorax), chyle (chylothorax), or purulence (empyema) from the intrathoracic space 7. There are other uses for a chest tube that are not as common and rarely indicated. Typically for a tension pneumothorax needle decompression occurs first and chest tube placement quickly follows after the patient stabilizes from decompression.
If the chest tube is placed for traumatic hemothorax, the indications for a thoracotomy include an initial sanguineous output of 1500 cc or an average of 200 cc/hr over 4 hours consecutive hours 7.
For post-traumatic retained hemothorax the literature is shifting toward early video-assisted thoracic surgery (VATS) if thoracostomy tube management fails 7. Some of the options on management included placement of a second chest tube versus tPA administration through the tube if you think the hemothorax has turned into a clot 7. Some trauma or CT surgeons are now taking patients straight to video-assisted thoracic surgery (VATS) if there is a retained hemothorax after the first thoracostomy tube 8.
Chest tubes are commonly made from PVC or silicone 7. They range in from 6 French to 40 French. The majority are fenestrated along the sides of the insertion end, and the tubes have a radiopaque stripe. After placement, the distal end of the tube is connected to a pleura-evac system. There are three chambers of a pleura-evac: suction chamber, water seal chamber, and the collection chamber. The water seal chamber acts as a one-way valve allowing air to escape from gravity, but not to re-enter the thoracic cavity 9.
Hemothorax prognosis
The outcome depends on the cause of the hemothorax, the amount of blood loss and how quickly treatment is given.
In the case of major trauma, the outcome will depend on the severity of the injury and the rate of bleeding.
- Ho ML, Gutierrez FR. Chest radiography in thoracic polytrauma. AJR Am J Roentgenol. 2009;192 (3): 599-612. https://www.ajronline.org/doi/full/10.2214/AJR.07.3324[↩]
- Fourdrain A, Lafitte S, Iquille J, De Dominicis F, Berna P. Delayed-onset tension hemothorax following blunt trauma and the rupture of a previously undiagnosed aberrant right subclavian artery. J Thorac Dis. 2017;9(3):E245-E248. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5394085/[↩]
- Sinha P, Sarkar P. Late clotted haemothorax after blunt chest trauma. J Accid Emerg Med. 1998;15(3):189-91. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1343064/pdf/jaccidem00024-0049.pdf[↩]
- Ali HA, Lippmann M, Mundathaje U et-al. Spontaneous hemothorax: a comprehensive review. Chest. 01;134 (5): 1056-65. https://journal.chestnet.org/article/S0012-3692(08)60370-0/fulltext[↩][↩]
- Berg AM, Amirbekian S, Mojibian H et-al. Hemothorax due to rupture of pulmonary arteriovenous malformation: an interventional emergency. Chest. 01;137 (3): 705-7. doi:10.1378/chest.09-0344[↩]
- Kaewlai R, Avery LL, Asrani AV et-al. Multidetector CT of blunt thoracic trauma. Radiographics. 2008;28 (6): 1555-70. https://pubs.rsna.org/doi/pdf/10.1148/rg.286085510[↩]
- Ravi C, McKnight CL. Chest Tube. [Updated 2018 Nov 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459199[↩][↩][↩][↩][↩]
- Lai Y, Wang X, Zhou H, Kunzhou PL, Che G. Is it safe and practical to use a Foley catheter as a chest tube for lung cancer patients after lobectomy? A prospective cohort study with 441 cases. Int J Surg. 2018 Aug;56:215-220.[↩]
- Goncalves Mendes Neto A, Jabuonski TA. Pigtail Catheter vs Chest Tube as the Initial Treatment for Pneumothorax. Chest. 2018 Sep;154(3):725.[↩]





{kind=link}