
Contents
- What does high triglycerides mean
- Do high-carbohydrate diets increase triglycerides and risk for cardiovascular disease?
- Do sugars cause high triglycerides?
- How can individuals change the way they eat to improve their triglyceride levels?
- What foods and beverages are the main sources of added sugars in Americans’ diets?
- Why are sweetened beverages so important for high triglycerides?
- Are some sugars worse than others?
- What’s the difference between triglycerides and cholesterol?
- Normal and high triglyceride levels
- High triglycerides symptoms
- What causes high triglycerides
- How are high triglycerides found?
- High triglycerides treatment
What does high triglycerides mean
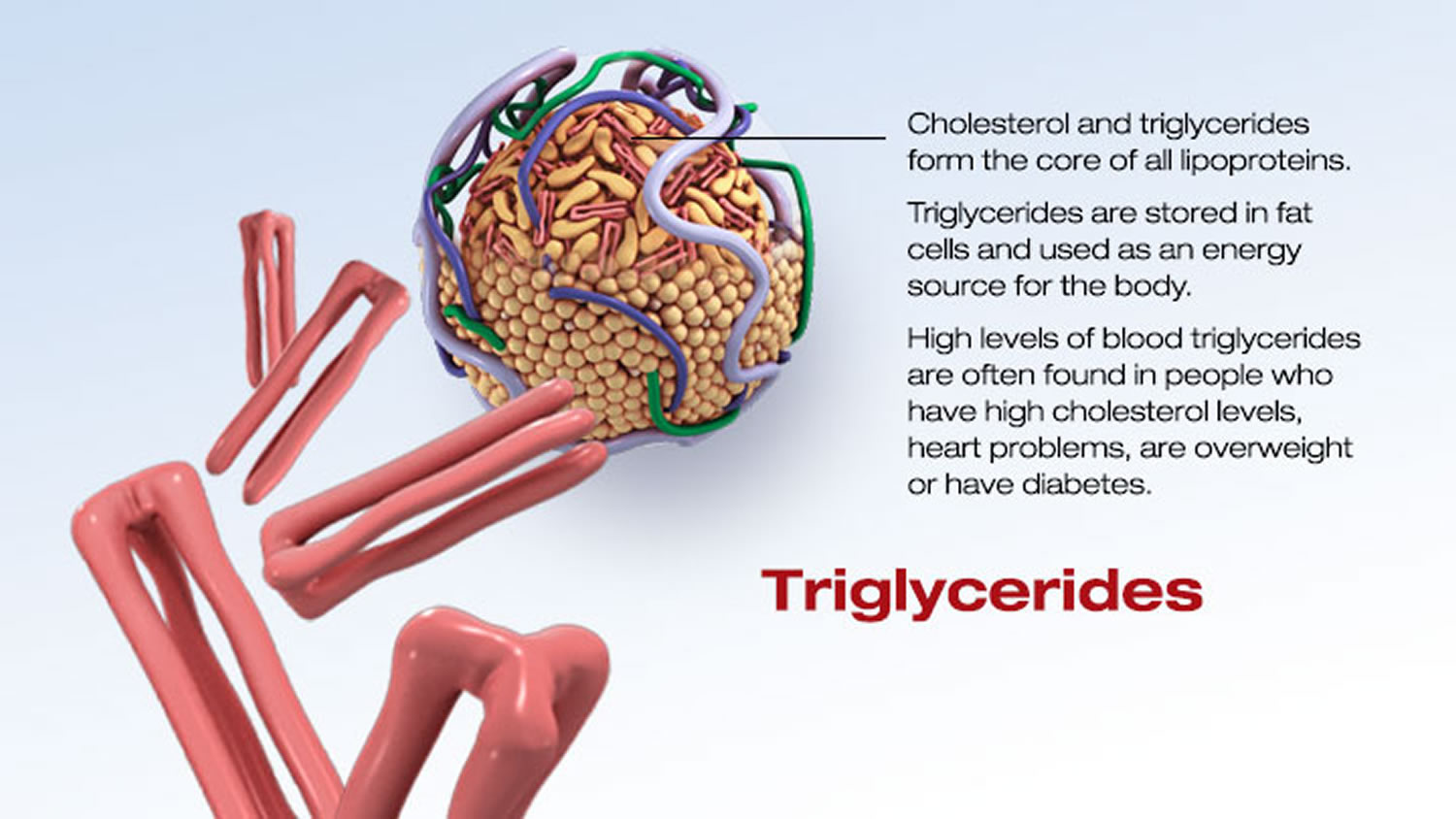
High triglycerides also called as hypertriglyceridemia, is when your fasting blood triglycerides is above 150 to 199 mg/dL (1.7-2.2 mmol/L) [in adults]. Most often, having high triglycerides has no warning signs or symptoms. Levels above 150mg/dl (1.7 mmol/L) may raise your risk for heart disease. A triglyceride level of 150 mg/dL (1.7 mmol/L) or higher is also a risk factor for metabolic syndrome. Above 2,000 mg/dL (22.58 mmol/L) poses a high risk for pancreatitis [inflammation of the pancreas]. Triglycerides are the most common type of fat in your body and triglycerides store excess energy (calories) from your diet, thus triglycerides is a major source of energy for your body. Triglycerides is stored in your body’s fat (adipose) cells and is also found in foods such as dairy products, meat and cooking oils. Some triglycerides circulate in your blood to provide fuel for muscles to work. After a person eats, an increased level of triglycerides is found in the blood as the body converts the excess calories (energy you don’t need right away) into fat. Triglycerides move via the blood from the gut to adipose (fat) tissue for storage. In between meals, triglycerides are released from fat tissue to be used as an energy source for your body. Most triglycerides are carried in the blood by lipoproteins called very low-density lipoproteins (VLDL).
If you are diabetic and your blood sugar (glucose) is out of control, your triglycerides may be very high.
Certain drugs such as corticosteroids, protease inhibitors for HIV, beta blockers, and estrogens can increase blood triglyceride levels.
Triglycerides change dramatically in response to meals, increasing as much as 5 to 10 times higher than fasting levels just a few hours after eating. Even fasting levels vary considerably day to day. Therefore, modest changes in fasting triglycerides measured on different days are not considered to be abnormal.
Normal triglyceride levels vary by age and sex. Triglycerides normally increase with age.
Also, many people with high triglycerides have other lipid problems or other risk factors for heart disease. A high triglyceride level is one part of the metabolic syndrome, a cluster of risk factors that increase the risk for heart disease and diabetes. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with heart disease or diabetes also have high triglyceride levels.
The most common reasons for high triglycerides include:
- Regularly eating more calories that you burn off, especially if you eat a lot of sugar,
- Being overweight or having obesity,
- Cigarette smoking,
- Excessive alcohol use,
- Lack of exercise,
- Metabolic syndrome,
- Type 2 diabetes, and
- Familial combined hyperlipidemia, a genetic disorder that runs in the family. It results in high triglycerides, high “bad” (low density lipoprotein, or LDL) cholesterol, and low “good” (high-density lipoprotein, or HDL) cholesterol.
Sometimes high triglycerides are a side effect of taking certain medications, such as:
- Diuretics
- Estrogen and progestin
- Retinoids
- Steroids
- Beta blockers
- Some immunosuppressants
- Some HIV medications
A high triglyceride level combined with high LDL “bad” cholesterol or low HDL “good” cholesterol is linked with fatty buildups within the artery walls, which increases your risk of heart attack and stroke.
Your body needs some cholesterol to work properly. But if you have too much of LDL “bad” cholesterol and triglycerides in your blood, it can combine with other substances in the blood and stick to the walls of your arteries. This is called plaque. Plaque can narrow your arteries or even block them.
The plaque buildup in arteries that LDL cholesterol and triglycerides contribute to is known as atherosclerosis (“hardening of the arteries”). When plaque builds up, it can partly or entirely block the blood flow of an artery in the heart, brain, pelvis, legs, arms or kidneys. This can lead to coronary heart disease, angina (chest pain), carotid artery disease, peripheral artery disease and chronic kidney disease.
However, it is unclear if high triglycerides alone are a risk factor for cardiovascular disease (heart disease and stroke). Triglycerides do not directly cause the plaque that can block your heart’s arteries (atherosclerosis) and lead to a heart attack. Yet, cholesterol in triglyceride-rich particles in the blood may add to plaque formation.
Atherosclerosis can also lead to a heart attack or stroke. That’s because a couple of things can happen where plaque occurs:
- A piece of plaque may break off.
- A blood clot (thrombus) may form on the uneven surface of plaque buildup.
If either of these travels through the body, ultimately lodging in an artery to the heart, it causes a heart attack. If lodged in an artery to, or in, the brain, a stroke results.
Studies have consistently linked high triglycerides levels with heart disease, heart attacks, and stroke, especially in people with low levels of “good” HDL cholesterol and in those with type 2 diabetes.
High triglycerides can affect more than your heart and blood vessels. Very high triglycerides raise the risk for pancreatitis, an inflammation of the pancreas. The
pancreas is large gland behind the stomach that makes key hormones like insulin. It helps your body maintain healthy blood glucose (sugar) levels. Pancreatitis can cause stomach pain and digestive problems. It can damage the pancreas and, over a long time, can lead to diabetes.
The good news is that there’s a lot you can do on your own to lower triglycerides and improve health.
- Get more physical activity. Exercise can have a big impact on triglyceride levels. Experts recommend that everybody get at least 30 minutes of exercise at least five times a week. If you’re out of shape, start slowly. Begin with a quick walk three times a week and then build up from there.
- Lose some weight. If you’re heavy, shed a few pounds and try to maintain an ideal body weight. Exercise will help, but you also need to focus on diet. The key is to eat fewer calories — whether they come from fats, carbs, or protein. Focus on a diet that’s high in fruits, vegetables, lean proteins, and low-fat dairy products. Cutting down on sugary foods — like sodas — could really help, too.
- Choose better fats. Pay more attention to the fats you eat. Eat fewer foods with unhealthy fats (found in meat, butter, and cheese) and trans fats (in processed foods and margarines), as well as cholesterol. Boost your intake of healthy monounsaturated and polyunsaturated fats, which are found in olive oil, nuts, and some fish. Studies have found that the omega-3s in fatty fish — like tuna, salmon, mackerel, and sardines — are particularly good at lowering triglyceride levels. Because even healthy fats are high in calories, you still need to eat these foods in moderation.
- Cut down on alcohol. Even small amounts of alcohol seem to cause big spikes in triglyceride levels. Limit alcohol intake to one drink a day.
- Fish oil with omega-3 fatty acids can help keep triglycerides under control.
- Niacin (nicotinic acid) can lower triglycerides by up to 50%. It’s available as a non-prescription supplement.
Do high-carbohydrate diets increase triglycerides and risk for cardiovascular disease?
Evidence from a statement released by the National Heart, Lung and Blood Institute, panel on Detection, Evaluation, and treatment of High Blood Cholesterol in Adults (ATP III), suggests that very high intakes of carbohydrates (greater than 60 percent of total calories) are accompanied by a rise in triglycerides.
The recommendation by the Heart, Lung and Blood Institute (ATP III) regarding dietary “Carbohydrate intakes should be limited to 60 percent of total calories. Lower intakes (e.g., 50 percent of calories) should be considered for persons with metabolic syndrome who have elevated triglycerides or low HDL cholesterol (the good cholesterol).
Do sugars cause high triglycerides?
Yes. Added sugars intake does appear to be connected with increased triglyceride levels, a known risk factor for developing heart disease.
Eating added sugars often means a person is consuming less fiber. This is important because increasing fiber in the diet is associated with decreasing energy intake (calories), which can result in weight loss. For those who are at a greater than ideal body weight, weight loss is an important therapy for lowering triglycerides.
Fructose is metabolized differently than other sugars such as glucose. Because it may raise triglycerides, its use should be limited if levels are outside the normal range.
How can individuals change the way they eat to improve their triglyceride levels?
All people, whether or not they have high triglycerides, should limit their intake of added sugars. If a person has triglycerides that are outside the normal range it is especially important to limit daily calories from added sugar to no more than 5 percent to 10 percent (no more than 100 calories for most women and no more than 150 calories per day for most men). Sugar has no nutritional value other than to provide calories. To ensure proper nutrient intake in the diet and limit excess calories, people should be sure foods high in added sugars are not taking the place of foods with essential nutrients or are increasing their total calorie intake.
Added sugars are sugars and syrups that are added to foods or beverages during processing or preparation. They do not include naturally occurring sugars such as those found in milk (lactose) and fruits (fructose). For those people above 150 mg/dL (1.7 mmol/L) triglycerides, limit fructose and work with your healthcare provider to monitor your fructose intake, and emphasize more vegetables and fruits that are lower in fructose.
What foods and beverages are the main sources of added sugars in Americans’ diets?
Regular soft drinks, fruit drinks (fruitades and fruit punch), desserts (cakes, cookies, pies), syrups and jellies, candy, ready to eat cereals, milk based products such as sweetened yogurts, sweet milk, and ice cream, and grain products like sweet rolls and cinnamon toast. High fructose corn-syrup is 55% fructose, and 45% glucose – not 100% fructose.
Why are sweetened beverages so important for high triglycerides?
People who consume large amounts of beverages with added sugars tend to consume more calories overall and tend to gain weight. A major contributor of added sugars to American diets is sugar sweetened beverages. Currently, it is estimated that soft drink consumption alone accounts for one third of added sugars intake in the U.S. diet.
Added sugars (or added sweeteners) include natural sugars (such as white sugar, brown sugar, honey, etc.) as well as other caloric sweeteners that are chemically manufactured (such as high fructose corn syrup, maltodextrin, etc).
Americans should limit their intake of sugary beverages. The American Heart Association recommends consuming no more than 5.1 ounces (145 grams) of sugar-sweetened beverages per day, based on a 2000 calorie per day diet.
Are some sugars worse than others?
In addition to limiting added sugars, those with triglycerides outside the normal range should limit fructose consumption to 50 to 100 grams per day, because fructose raises triglycerides. Fructose, or fruit sugar, is a simple monosaccharide (type of sugar) found in many foods and fruits. It is one of the three important dietary monosaccharides, along with glucose and galactose. It is part of the chemical structure of sucrose, or table sugar.
According to USDA data, a 12-ounce cola has 22g of fructose, 1.5 oz raisins have 13g of fructose, and an apple has 4-10g of fructose. Limiting fructose may be difficult because fructose is not listed on the nutrition facts panel.
Common sources of fructose:
- Cola or Lemon-Lime Soda (12 oz) = 22 g fructose
- Ginger Ale with HFCS (12 oz) = 17 g fructose
- Raisins (1.5 oz box) = 13 g fructose
- Agave Nectar (tablespoon) = 8.9 g fructose
- Honey (tablespoon) = 8.6 g fructose
- Applesauce (3.5 oz) = 8 g fructose
- Fruit (apple, pear) = 4–10 g fructose
- Molasses (tablespoon) = 2.6 g fructose
- Table sugar (teaspoon) = 2 g fructose
What’s the difference between triglycerides and cholesterol?
Triglycerides and cholesterol are different types of lipids that circulate in your blood:
- Triglycerides store unused calories and provide your body with energy.
- Cholesterol is used to build cells and certain hormones.
Normal and high triglyceride levels
Your doctor will usually check for high triglycerides as part of a cholesterol test, which is sometimes called a lipid panel or lipid profile. You’ll have to fast before blood can be drawn for an accurate triglyceride measurement.
For adults, triglyceride levels results are categorized as follows:
- Normal: Less than 150 mg/dL (1.7 mmol/L)
- Mild high: 150 to 199 mg/dL (1.7-2.2 mmol/L)
- Moderate high: 200 to 999 mg/dL (2.3-11.3 mmol/L)
- Severe high: 1,000 to 1,999 mg/dL (11.3-22.6 mmol/L)
- Very severe: Greater than 2,000 mg/dL (22.6 mmol/L)
Note: For improved metabolic health and protection to the heart and blood vessels, the American Heart Association now recommends an optimum fasting triglyceride level of 100 mg/dL (1.12 mmol/L). This puts an even stronger emphasis on lifestyle change which has been the recommended therapy for mildly elevated triglycerides. However, the American Heart Association does not recommend people use drug therapy to achieve this optimal level because there has not been adequate study to show that drug therapy to lower triglycerides to this level is helpful. Many people will be able to reduce their triglycerides as well as other metabolic risk factors such as elevated blood sugar and elevated blood pressure with diet, weight loss and increased physical activity.
For children, teens and young adults:
- From newborn to age 9
- Acceptable: Less than 75 mg/dL (0.85 mmol/L)
- Borderline high: 75-99 mg/dL (0.85-1.12 mmol/L)
- High: Greater than 100 mg/dL (1.13 mmol/L)
- For ages 10-19 years
- Acceptable: Less than 90 mg/dL (1.02 mmol/L)
- Borderline high: 90-129 mg/dL (1.02-1.46 mmol/L)
- High: Greater than 130 mg/dL (1.47 mmol/L)
- For young adults older than 19
- Acceptable: Less than 115 mg/dL (1.30 mmol/L)
- Borderline high: 115-149 mg/dL (1.30-1.68 mmol/L)
- High: Greater than 150 mg/dL (1.7 mmol/L)
When triglycerides are very high (greater than 1000 mg/dL (11.30 mmol/L)), there is a risk of developing pancreatitis in children and adults. Treatment to lower triglycerides should be started as soon as possible.
Note: These values are based on fasting triglyceride levels.
The plasma level of triglyceride is a well-established independent biomarker of cardiovascular disease risk 1 and triglyceride-rich lipoproteins have atherogenic properties. Triglyceride predicts cardiovascular disease in a wide range of circumstances. Its association with cardiovascular disease risk is partly attenuated by adjustment for HDL cholesterol, with which it is moderately correlated 2.
Genetic variation associated with lifelong low triglyceride levels is associated with a lower incidence of cardiovascular disease 3. Triglyceride is carried primarily within large lipoproteins, chylomicrons, and VLDL (very low density lipoprotein), which are also rich in cholesterol and like LDL can enter the arterial wall and stimulate atherosclerosis. These triglyceride-rich lipoproteins carry various atherogenic proteins such as apolipoprotein C-III, itself associated with atherosclerosis and cardiovascular disease 4.
Replacing 1% of daily energy intake from saturated fat with polyunsaturated or monounsaturated fat lowers triglyceride by 0.9 or 0.4 mg/dL 5 perhaps more in those with hypertriglyceridemia 6.
Replacing the 1% saturated fat with 1% carbohydrates raises serum triglycerides by ≈1 mg/dL. Dietary carbohydrates raise plasma triglyceride levels by increasing the production by the liver of triglycerides and subsequent incorporation into VLDL (very low density lipoprotein) 6. The magnitude that dietary carbohydrates increase plasma triglyceride is similar whether the carbohydrate has a high or low glycemic index 7.
High triglycerides symptoms
Usually, most people with high triglyceride levels have no symptoms and the only means of discovering a high level is with blood tests. However, in rare cases, a person may have an extremely high level of triglycerides (well above 1000 mg/dL) sustained over time and the individual may experience repeated bouts of acute pancreatitis. Some of the signs and symptoms include pain in the upper half of the stomach area that develops suddenly and then gradually gets worse, fever, nausea, vomiting, and sometimes jaundice. A person with severely high levels may also develop lesions on the skin called xanthomas. These typically appear as several small, round, solid, yellow bumps mostly on the back, chest, buttocks, shoulders and thighs.
What causes high triglycerides
Elevated triglycerides can be caused by several factors. They are overweight and obesity, physical inactivity, cigarette smoking, excess alcohol consumption and a diet very high in carbohydrates (more than 60 percent of total calories).
Table 1. Disorders mainly causing high triglycerides
| Primary disorders |
| Familial hypertriglyceridemia |
| Familial combined hyperlipidemia |
| Congenital deficiency of lipoprotein lipase |
| Deficiency of apoprotein CII |
| Familial dysbetalipoproteinemia |
| Secondary disorders |
| Uncontrolled diabetes mellitus |
| Nephrotic syndrome |
| Dysproteinemias |
| Oral contraceptives |
| Thiazide diuretics |
| Beta-adrenergic blocking agents |
| Alcohol |
The primary disorders predominantly causing high triglyceride are: (1) familial hypertriglyceridemia, (2) familial combined hyperlipidemia, (3) congenital deficiency of lipoprotein lipase, (4) deficiency of apoprotein CII and (5) familial dysbetalipoproteinemias 8.
Familial hypertriglyceridemia is a common autosomal dominant disorder characterized by increased plasma concentration of very-low-density lipoprotein (VLDL) (type 4 lipoprotein pattern) 8. Moderate elevations of triglycerides usually occur during early adulthood, and a triad of obesity, hyperglycemia, and hyperinsulinemia can be seen in affected individuals. In individuals with moderate elevation in plasma triglycerides associated with a normal cholesterol level, the possibility of familial hypertriglyceridemia should be suspected 8. Although patients with familial hypertriglyceridemia usually have moderate elevation of plasma triglycerides, whenever conditions known to elevate triglyceride, such as diabetes mellitus or alcohol or oral contraceptive consumption, concurrently occur, they may develop a profound hypertriglyceridemia and a mixed hyperlipidemia (type 5 lipoprotein pattern). An increased incidence of atherosclerosis has been reported. Hypertension and hyperuricemia have also been frequently observed.
Congenital lipoprotein lipase deficiency is a rare autosomal recessive disorder secondary to absence or severe diminution in the activity of lipoprotein lipase. Affected individuals are homozygous for a mutation that prevents normal expression of lipoprotein lipase activity. The parents, although clinically normal, are obligate heterozygotes. This enzymatic disorder is reflected in a massive accumulation of chylomicrons in the plasma without elevation of very-low-density lipoprotein (VLDL) (type 1 lipoprotein pattern). Triglycerides may reach levels of 2000 to 10,000 mg/dl. This disorder usually appears in childhood with recurrent bouts of abdominal pain secondary to pancreatitis. Another characteristic feature of the disorder is the occurrence of eruptive xanthomas, predominantly in the buttocks and other pressure-sensitive areas of the body, attributed to the deposition of chylomicron triglycerides in histiocytes. The elevation in chylomicrons may also cause a lipemic serum, a picture of lipemia retinalis, and hepatosplenomegaly. The diagnosis is suspected by the presence of a lipemic plasma in a young patient who has fasted for 12 hours. Overnight incubation of a test tube of such plasma in a refrigeration at 4°C demonstrates a visible white layer at the top of the tube. Failure of lipoprotein lipase levels to increase after an infusion of heparin confirms the diagnosis. The occurrence of accelerated atherosclerosis is not reported in this condition.
Apoprotein CII deficiency is a rare autosomal recessive disorder caused by absence of apoprotein CII, a required co-factor for the activity of lipoprotein lipase. The ensuing functional deficiency in this enzyme leads to a clinical picture similar to that described above for congenital lipoprotein lipase deficiency. However, in contrast to what occurs in the latter disorder, affected individuals are diagnosed at later age and rarely present eruptive xanthomas. The usual presentation is also with recurrent abdominal pains secondary to acute pancreatitis. At times the diagnosis is made by chance discovery of a milky serum.
Due to the inherent defect in this condition, in which lipoprotein lipase is not activated, both chylomicrons and very-low-density lipoprotein (VLDL) are elevated in the blood causing a type 1 or type 5 lipoprotein pattern.
Familial dysbetalipoproteinemia, also called familial type 3 hyperlipoproteinemia, is a condition inherited through a single gene mechanism whose clinical presentation requires the presence of other genetic or environmental factors. Elevation of both plasma cholesterol and triglycerides occurs because of accumulation of remnant very-low-density lipoprotein (VLDL) particles in the plasma. The metabolic defect in most patients occurs in apolipoprotein E. This has three common alleles, designated E2, E3, and E4. Patients with this disorder have only apolipoprotein E2 in very-low-density lipoprotein (VLDL), which is less effective in facilitating clearance of remnants than E3 or E4. The condition occurs only in individuals who are homozygous for E2, that is, those with an E2/E2 genotype. Clinical evidence of hyperlipoproteinemia usually appears after the second decade. The characteristic clinical findings are xanthoma striata palmaris and tuberous and tuberoeruptive xanthomas over the elbows and knees. The disorder is associated with severe atherosclerosis of the coronary arteries, abdominal aorta, and peripheral arteries.
The diagnosis is facilitated by encountering a broad beta band on lipoprotein electrophoresis. Confirmation can be obtained in specialized laboratories either by measuring the chemical composition of the VLDL fraction after ultracentrifugation of the plasma or by determining for the E2 allele after isoelectric focusing of remnant proteins.
Several factors can contribute to high triglyceride level, including:
- Being overweight, or obesity
- Physical inactivity
- Cigarette smoking
- Excess alcohol consumption
- A diet very high in carbohydrates (more than 60 percent of total calories)
- Sometimes underlying diseases or genetic disorders can also cause high triglyceride levels.
These factors can be addressed with lifestyle changes.
Risk factors for developing high triglycerides
Risk factors for high triglycerides include:
- Lifestyle factors
- Being overweight or obese
- Not getting enough exercise
- Drinking too much alcohol
- Familial (inherited) disorders
- Type 2 diabetes (poorly controlled) or the metabolic syndrome
- Thyroid diseases (hypothyroidism)
- Liver or kidney diseases
- Pregnancy
- Medications
- Some “water” pills (thiazide diuretics)
- Beta-blockers
- Estrogen (birth control pills, hormone therapy)
- Isotretinoin for acne
- Corticosteroids for conditions such as asthma and arthritis
- Certain cholesterol-lowering drugs
- Protease inhibitors for HIV
- Immune suppressants (such as sirolimus)
- Some antipsychotics (mental health medicines)
Foods to avoid with high triglycerides
Sugar and refined carbohydrates
Simple carbohydrates, such as sugar and foods made with white flour or fructose, can increase triglycerides.
Examples of refined carbs
Refined Breads
Many of the breads found on grocery store shelves are considered refined carbohydrates. These breads are often made from enriched and bleached flours, and these flours are typically listed as the first or second ingredient on the nutrition label. In addition, the list of ingredients will often include vitamins and minerals that are added during the post-refining, enrichment process. Sourdough, white and plain wheat bread are excellent examples of refined breads, whereas 100 percent whole-wheat or whole-grain breads are not refined.
Refined Rice
Like bread, some forms of rice are considered to be refined grains. White rice and most of the quick-cook rices are refined and, as a result, do not contain an intact grain. They may be enriched to enhance their nutritional profile, but they typically lack the fiber found in the non-refined brown rice. One cup of white rice counts as 2 ounces of refined grains.
Refined Cereals
Many of the sugary, cold cereals found in grocery stores are considered to be refined grains. They are typically made from enriched flour due to the refining of their original wheat, corn or oat grain. Refined cereals typically have 2 or fewer grams of fiber per serving, and one cup of a refined cereal, such as corn flakes, counts as 1 ounce of refined grains.
Refined Pasta
Unlike whole wheat or whole grain pasta, refined pasta lacks much of the fiber and the B-complex vitamins found in the unprocessed version. Like other processed starches, refined pasta may be enriched with nutrients such as folate, thiamin and riboflavin, and some versions of refined pasta may even have omega 3 fatty acids added during processing. Thus, if you prefer the less grainy taste of refined pasta, make sure that it has been fully enriched with the aforementioned nutrients.
Refined Snack Foods
Snack foods are typically made with refined carbs such as bleached flours and sugar in order to increase palatability. These snack foods have little nutritional value and, as a result, provide empty calories in the diet. Cakes, cookies, pie, candy and chips are all examples of refined snack foods, and according to the U.S. Department of Agriculture, these foods should not constitute more than 120 to 330 calories per day.
List of refined carbs
Any foods that have been processed for quick consumption.
- Foods made with refined or “white” flour also contain less fiber and protein than whole-grain products.
- Snacks, such as crisps, sausage rolls, pies and pasties
- Granola bars
- Ice cream
- Donuts
- Cakes
- Twinkies
- Pastries
- Canned fruits with added sugar or syrup
- Sweets
- Fruit drinks
- Colas and carbonated sweetened beverages
- Energy drinks
- Sports drink
- Jams
- Crackers
- Dressings
- Sauces
- Cookies
- Fruit chews
- Pizzas
- Apple pies
- Anything with added sugar.
Sugar by Any Other Name
You don’t always see the word “sugar” on a food label. It sometimes goes by another name, like these:
- White sugar
- Brown sugar
- Raw sugar
- Agave nectar
- Brown rice syrup
- Corn syrup
- Corn syrup solids
- Coconut sugar
- Coconut palm sugar
- High-fructose corn syrup
- Invert sugar
- Dextrose
- Anhydrous dextrose
- Crystal dextrose
- Dextrin
- Evaporated cane juice
- Fructose sweetener
- Liquid fructose
- Glucose
- Lactose
- Honey
- Malt syrup
- Maple syrup
- Molasses
- Pancake syrup
- Sucrose
- Trehalose
- Turbinado sugar
Saturated fat and trans fats
Saturated fat and trans fats can increase your total cholesterol level and your non-HDL cholesterol (bad) level which increases the risk of fatty deposits building up in your arteries.
Saturated fat is mainly found in:
- butter
- lard
- fatty meats
- cheese
- cakes
- biscuits
- palm and coconut oil.
Trans fats are usually found in processed foods like biscuits, cakes, fast food and some margarines and spreads.
How are high triglycerides found?
A blood test called a lipid panel measures triglycerides and cholesterol. You should have this test after fasting (not eating or drinking anything but water) for at least 12 hours.
Adults should get this screening test every five years or sooner. If you have diabetes, a family history of high triglycerides, or other risk factors, you may need screening more often, according to the National Cholesterol Education Program Guidelines 9.
High triglycerides treatment
The goal of treatment is to lower your triglycerides. Patients with very severe high triglycerides should try to lower their triglycerides below 1,000 mg/dL (11.3 mmol/L), to reduce their risk for pancreatitis.
For many people, high triglycerides are caused by another disorder, such as diabetes, obesity, renal failure, or alcoholism. With these conditions, the strategy is to treat the primary cause. When high triglycerides are not caused by another disorder, they are often seen together with high cholesterol and treatment is directed toward lowering both cholesterol and triglycerides. Lifestyle changes, such as a healthy diet and increased exercise, are usually the primary strategy for lowering levels. If these fail, lipid-lowering medications such as statins are generally recommended.
Lifestyle changes
If you have mild to moderate hypertriglyceridemia, focus on cutting calories. Extra calories are converted to triglycerides and stored as fat. Reducing your calories will reduce triglycerides.
Lose weight
The first step for lowering triglycerides is to lose weight if you are overweight, exercise often, and eat a healthy diet low in saturated (bad) fat and sugar. Also, limit the amount of refined, processed grains you eat, such as white bread, rice, and pasta. Follow your doctor’s advice about limiting intake of alcohol, which
raises triglycerides in some people.
Exercise
Be active for at least 30 minutes a day. A good starting goal is at least 150 minutes a week, but if you don’t want to sweat the numbers, just move more!
Regular physical activity strengthens your heart and reduces your ‘bad’ cholesterol. Being active helps increase your ‘good’ HDL cholesterol while helping your body move the ‘bad’ non-HDL cholesterol to your liver where it will be disposed of.
You don’t have to join a gym or take up a sport, just look for chances to move more every day. Staying active is great way to keep your heart healthy.
Stop smoking
Quitting smoking can help to lower your cholesterol and improve your heart health. Smoking stops ‘good’ cholesterol doing its job of getting rid of your ‘bad’ cholesterol. Speak to your doctor about how to stop smoking as soon as you can. Not smoking will really help you avoid heart disease.
Limit how much alcohol you drink
Alcohol is high in calories and sugar and has a particularly potent effect on triglycerides. If you have severe hypertriglyceridemia, avoid drinking any alcohol.
High triglycerides diet
Eat a healthy balanced diet
Eating more fruit, vegetables and wholegrain is better than eating foods high in saturated fat and sugar. Eating a healthy, balanced diet low in saturated fats can also reduce your level of LDL “bad” cholesterol.
Avoid sugar and refined carbohydrates
Simple carbohydrates, such as sugar and foods made with white flour or fructose, can increase triglycerides.
Avoid or cut down on the following foods, which are high in saturated fat:
- fatty cuts of meat and meat products, such as sausages and pies
- butter, ghee and lard
- cream, soured cream, crème fraîche and ice cream
- cheese, particularly hard cheese
- cakes and biscuits
- milk chocolate
- coconut oil, coconut cream and palm oil
Choose healthier healthy monounsaturated and polyunsaturated fats such as:
- olive, rapeseed or sunflower oils and spreads
- vegetable oil spreads
- nuts
- seeds
- oily fish.
Choose more wholegrains and foods that are high in soluble fiber as this can help lower cholesterol such as:
- oats
- beans
- pulses
- lentils
- nuts
- fruits and vegetables.
Omega-3 fatty acids
Omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) lower triglycerides. However, too much omega-3 fatty acids can contribute to obesity.
These polyunsaturated (good) fats are found in oily fish such as salmon, mackerel and tuna. Omega-3 fatty acids is also found in avocados. In high doses, omega-3 fatty acids (EPA and DHA) can treat high triglycerides. For people with a high triglyceride level, at least 2 portions of oily fish a week is thought to be beneficial.
You can get high doses of omega-3 fatty acids in a fish oil supplement or by prescription. However, there’s no evidence that taking omega-3 fatty acid supplements has the same benefit.
Triglycerides-lowering medication
Besides lifestyle changes, you may also need drug treatment. There are several different types of cholesterol-lowering medication that work in different ways. Your doctor can advise you about the most suitable type of treatment, and may also prescribe medication to lower high blood pressure (hypertension) if it affects you.
For mildly or moderately high triglycerides, your doctor may prescribe one of these types of drugs:
Note: It is unclear if fibrates and niacin prevent heart attacks and strokes.
If your triglycerides are above 1,000 mg/dL, though, the first choice of medicine is a fibrate. You may need a statin, too, but experts advise against treatment with statins alone if your high triglycerides are severe or very severe. Fibrates are better than statins at lowering triglycerides. However, people with liver disease or gallbladder disease should not take fibrates.
Talk to your doctor about the risks and benefits of all these drugs. Medications do not cure the problem of high triglycerides, so you will need to take them long term. However, weight loss and other lifestyle changes can lower high trigylcerides enough to eliminate the need for medication.
Fibrates
Fibrates, which greatly lower triglycerides and sometimes raise HDL (good) cholesterol. In the U.S., these prescription drugs include gemfibrozil and fenofibrate.
Fibrates help to slow or halt the build-up of cholesterol in the arteries to reduce the risk of heart problems. They are given to people who have high cholesterol levels because they have a raised level of triglycerides in their blood.
Niacin (vitamin B3)
Niacin (vitamin B3) at doses of 1,000 to 3,000 mg per day, lowers triglycerides and LDL cholesterol and raises HDL cholesterol. These doses apply to immediate-release (released into the body right away) niacin, available by prescription or as a supplement.
The dose of sustained-release (released into the body over time) niacin, which is only available as a supplement, shouldn’t exceed 2,000 mg per day because of the risk of liver damage.
Statins
Your doctor may add a statin to your other drug treatment. Though statins mainly lower LDL cholesterol, they also can decrease triglycerides. Some studies show that statins reduce the risk of heart attacks and strokes.
Statins block the enzyme (a type of chemical) in your liver that helps to make cholesterol. This leads to a reduction in your blood cholesterol level.
You’ll usually be started on a medication called atorvastatin. Other statins include simvastatin and rosuvastatin.
When someone has side effects from using a statin, it’s described as having an “intolerance” to it. Side effects of statins include headaches, muscle pain and stomach problems, such as indigestion, diarrhea or constipation.
Statins will only be prescribed to people who continue to be at high risk of heart disease, because they need to be taken for life. Cholesterol levels start to rise again once you stop taking them.
Aspirin
In some cases, a low daily dose of aspirin may be prescribed, depending on your age (usually over 40 years old) and other risk factors.
Low-dose aspirin can help to prevent blood clots forming, particularly for someone who’s had a heart attack, has established vascular disease, or a high risk of developing cardiovascular disease.
You may also be advised to have periodic blood tests to ensure your liver is functioning well.
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, et. al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292–2333. doi: 10.1161/CIR.0b013e3182160726.[↩]
- Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, Boekholdt SM, Khaw KT, Gudnason V. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation. 2007;115:450–458. doi: 10.1161/CIRCULATIONAHA.106.637793.[↩]
- TG and HDL Working Group of the Exome Sequencing Project, National Heart, Lung, and Blood Institute. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med.2014;371:22–31.[↩]
- Wyler von Ballmoos MC, Haring B, Sacks FM. The risk of cardiovascular events with increased apolipoprotein CIII: a systematic review and meta-analysis. J Clin Lipidol. 2015;9:498–510. doi: 10.1016/j.jacl.2015.05.002.[↩]
- Mensink RP. Effects of Saturated Fatty Acids on Serum Lipids and Lipoproteins: A Systematic Review and Regression Analysis. Geneva, Switzerland: World Health Organization; 2016.[↩]
- Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S; on behalf of the American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292–2333. doi: 10.1161/CIR.0b013e3182160726.[↩][↩]
- Sacks FM, Carey VJ, Anderson CA, Miller ER 3rd, Copeland T, Charleston J, Harshfield BJ, Laranjo N, McCarron P, Swain J, White K, Yee K, Appel LJ. Effects of high vs low glycemic index ofdietary carbohydrate on cardiovascular disease risk factors andinsulin sensitivity: the OmniCarb randomized clinical trial. JAMA.2014;312:2531–2541. doi: 10.1001/jama.2014.16658.[↩]
- Cox RA, García-Palmieri MR. Cholesterol, Triglycerides, and Associated Lipoproteins. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 31. Available from: https://www.ncbi.nlm.nih.gov/books/NBK351[↩][↩][↩][↩]
- https://www.lipid.org/practicetools/guidelines/national[↩]





{kind=link}