Contents
- What is hyperplasia
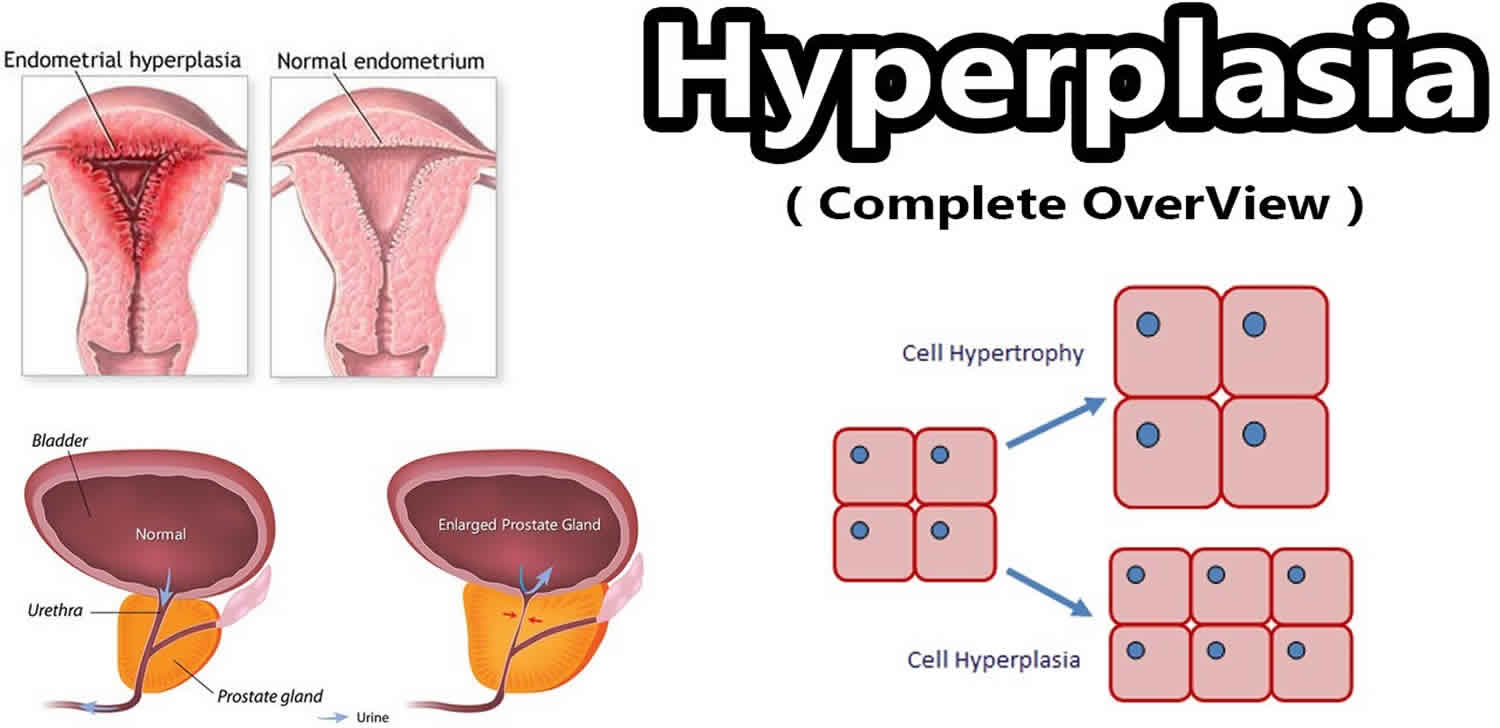
- Hypertrophy vs Hyperplasia
- Atypical hyperplasia of the breast
- Congenital adrenal hyperplasia
- Endometrial hyperplasia
- Prostatic hyperplasia
What is hyperplasia
Hyperplasia is an increase in the number of cells in an organ or tissue. These cells appear normal under a microscope. They are not cancer, but may become cancer. Normal cells may become cancer cells. Before cancer cells form in tissues of the body, the cells go through abnormal changes called hyperplasia and dysplasia. In hyperplasia, there is an increase in the number of cells in an organ or tissue that appear normal under a microscope. In dysplasia, the cells look abnormal under a microscope but are not cancer. Hyperplasia and dysplasia may or may not become cancer.
Hypertrophy vs Hyperplasia
Hypertrophy is an increase in the number or size of the cells of which a tissue is composed as the result of increase in the function of that tissue.
Atypical hyperplasia of the breast
Atypical hyperplasia is a precancerous condition that affects cells in the breast. Atypical hyperplasia describes an accumulation of abnormal cells in the breast.
Atypical hyperplasia isn’t cancer, but it can be a forerunner to the development of breast cancer. Over the course of your lifetime, if the atypical hyperplasia cells keep dividing and become more abnormal, this can transition into noninvasive breast cancer (carcinoma in situ) or invasive breast cancer.
If you’ve been diagnosed with atypical hyperplasia, you have an increased risk of developing breast cancer in the future. For this reason, doctors often recommend intensive breast cancer screening and medications to reduce breast cancer risk.
Make an appointment with your doctor if you have any signs or symptoms that worry you.
Atypical hyperplasia typically doesn’t cause symptoms, but it may cause changes to appear on a mammogram. Atypical hyperplasia is usually discovered during a breast biopsy to investigate an abnormality found on a mammogram. Sometimes atypical hyperplasia is discovered on a biopsy done for a different condition.
Atypical hyperplasia of the breast causes
It’s not clear what causes atypical hyperplasia.
Atypical hyperplasia forms when breast cells become abnormal in number, size, shape, growth pattern and appearance. The appearance of the abnormal cells determines the type of atypical hyperplasia:
- Atypical ductal hyperplasia causes abnormal cells that appear similar to the cells of the breast ducts.
- Atypical lobular hyperplasia causes abnormal cells that appear similar to the cells of the breast lobules.
Atypical hyperplasia is thought to be part of the complex transition of cells that may evolve into breast cancer. The progression to breast cancer typically involves:
- Hyperplasia. The process begins when normal cell development and growth become disrupted, causing an overproduction of normal-looking cells (hyperplasia).
- Atypical hyperplasia. The excess cells stack upon one another and begin to take on an abnormal appearance. At this point, the cells have some, but not all, of the changes needed to become cancer.
- Noninvasive (in situ) cancer. The abnormal cells continue to progress in appearance and multiply, evolving into in situ cancer, in which cancer cells remain confined to the area where they start growing.
- Invasive cancer. Left untreated, the cancer cells may eventually become invasive cancer, invading surrounding tissue, blood vessels or lymph channels.
Atypical hyperplasia of the breast symptoms
Atypical hyperplasia usually doesn’t cause any specific symptoms.
Atypical hyperplasia of the breast complications
Increased risk of breast cancer
If you’ve been diagnosed with atypical hyperplasia, you have an increased risk of developing breast cancer in the future.
Women with atypical hyperplasia have a lifetime risk of breast cancer that is about four times higher than that of women who don’t have atypical hyperplasia. The risk of breast cancer is the same for women with atypical ductal hyperplasia and women with atypical lobular hyperplasia.
Recent research has revealed that the risk of breast cancer increases in the years after an atypical hyperplasia diagnosis:
- At 5 years after diagnosis, about 7 percent of women with atypical hyperplasia may develop breast cancer. Put another way, for every 100 women diagnosed with atypical hyperplasia, 7 can be expected to develop breast cancer five years after diagnosis. And 93 will not be diagnosed with breast cancer.
- At 10 years after diagnosis, about 13 percent of women with atypical hyperplasia may develop breast cancer. That means for every 100 women diagnosed with atypical hyperplasia, 13 can be expetected to develop breast cancer 10 years after diagnosis. And 87 will not develop breast cancer.
- At 25 years after diagnosis, about 30 percent of women with atypical hyperplasia may develop breast cancer. Put another way, for every 100 women diagnosed with atypical hyperplasia, 30 can be expected to develop breast cancer 25 years after diagnosis. And 70 will not develop breast cancer.
Being diagnosed with atypical hyperplasia at a younger age may increase the risk of breast cancer even more. For example, women diagnosed with atypical hyperplasia before age 45 seem to have a greater risk of developing breast cancer during their lifetimes.
Discuss your risk of breast cancer with your doctor. Understanding your risk can help you make decisions about breast cancer screening and risk-reducing medications.
Atypical hyperplasia of the breast diagnosis
Atypical hyperplasia is usually discovered after a biopsy to evaluate a suspicious area found on a mammogram or during a clinical breast exam. During the biopsy, tissue samples are removed and sent for analysis by a specially trained doctor (pathologist). The tissue samples are examined under a microscope, and the pathologist identifies atypical hyperplasia, if it’s present.
To further evaluate atypical hyperplasia, your doctor may recommend surgery to remove a larger sample of tissue to look for breast cancer. A diagnosis of atypical hyperplasia may lead to a surgical biopsy (wide local excision or lumpectomy) to remove all of the affected tissue. The pathologist looks at the larger specimen for evidence of in situ or invasive cancer.
Atypical hyperplasia of the breast treatment
Atypical hyperplasia is generally treated with surgery to remove the abnormal cells and to make sure no in situ or invasive cancer also is present in the area. Doctors often recommend more intensive screening for breast cancer and medications to reduce your breast cancer risk.
Follow-up tests to monitor for breast cancer
Your doctor may recommend you undergo tests to screen for breast cancer. This may increase the chance that breast cancer is detected early, when a cure is more likely. Talk about your breast cancer screening options with your doctor. Your options may include:
- Self-exams for breast awareness in order to develop breast familiarity and to detect any unusual breast changes
- Clinical breast exams by your health care provider annually
- Screening mammograms annually
- Screening breast MRI, depending on other risk factors, such as dense breasts, a strong family history or a genetic predisposition to breast cancer
Ways to reduce your risk of breast cancer
To reduce your risk of developing breast cancer, your doctor may recommend that you:
- Take preventive medications. Treatment with a selective estrogen receptor modulator, such as tamoxifen or raloxifene (Evista), for five years may reduce the risk of breast cancer. These drugs work by blocking estrogen from binding to estrogen receptors in breast tissue. Estrogen is thought to fuel the growth of some breast cancers. Tamoxifen is the only drug approved for use in premenopausal women. Another option for postmenopausal women may be aromatase inhibitors, such as exemestane (Aromasin) and anastrozole (Arimidex), which decrease production of estrogen in the body.
- Avoid menopausal hormone therapy. Researchers have concluded that combination hormone therapy to treat symptoms of menopause — estrogen plus progestin — increases breast cancer risk in postmenopausal women. Many breast cancers depend on hormones for growth.
Participate in a clinical trial. Clinical trials test new treatments not yet available to the public at large that may prove helpful in reducing breast cancer risk associated with atypical hyperplasia. Ask your doctor if you’re a candidate for any clinical trials.
- Consider risk-reducing (prophylactic) mastectomy. For women at very high risk of breast cancer, risk-reducing mastectomy — surgery to remove one or both breasts — reduces the risk of developing breast cancer in the future. You might be considered at very high risk of breast cancer if you have a genetic mutation in one of the breast cancer genes or you have a very strong family history of breast cancer that suggests a likelihood of having such a genetic mutation. But this surgery isn’t right for everyone. Discuss with your doctor the risks, benefits and limitations of this risk-reducing surgery in light of your personal circumstances. If you have a strong family history of breast cancer, you might benefit from meeting with a genetic counselor to evaluate your risk of carrying a genetic mutation and the role of genetic testing in your situation.
Coping and support
An atypical hyperplasia diagnosis can be stressful, since it increases your risk of breast cancer. Not knowing what the future holds may make you fearful for your health.
With time, every woman develops her own way of coping with atypical hyperplasia and her increased risk of breast cancer. Until you find your way of coping, consider trying to:
- Understand your individual risk of breast cancer. Breast cancer risk statistics can be overwhelming and frightening. Breast cancer risk statistics are developed by following many women with atypical hyperplasia and monitoring them for breast cancer. While these statistics can give you an idea of your prognosis, they can’t tell you about your own risk of breast cancer. Ask your doctor to explain your individual risk of breast cancer. Once you understand your personal risk of breast cancer, you can feel more comfortable making decisions about your treatment.
- Go to all of your follow-up appointments. If you’ve been diagnosed with atypical hyperplasia, your doctor may recommend more-frequent breast cancer screening exams and tests. You may find yourself distracted with worry before each exam because you’re afraid that your doctor will find breast cancer. Don’t let your fear stop you from going to your appointments. Instead, accept that fear is normal and find ways to cope. Relax, write your feelings in a journal or spend time with a close friend who can lift your spirits.
- Maintain your health. Make healthy lifestyle choices to keep yourself healthy. For instance, maintain a healthy weight, eat a healthy diet full of fruits and vegetables, get enough sleep so that you wake feeling rested, and limit the amount of alcohol you drink, if you choose to drink alcohol. You can’t control whether or not you get breast cancer, but you can keep healthy so that you’re well enough for breast cancer treatment, should you need it.
- Talk with other women in your situation. Talk to other women who have been diagnosed with atypical hyperplasia. Ask your doctor about support groups in your community. Another option is online message boards. Breast cancer organizations, such as BreastCancer.org, offer message boards for women with a high risk of breast cancer to connect with each other.
Congenital adrenal hyperplasia
Congenital adrenal hyperplasia (CAH) is a group of inherited genetic disorders that affect the adrenal glands, a pair of walnut-sized organs above your kidneys. A person with congenital adrenal hyperplasia lacks one of the enzymes the adrenal glands use to produce hormones that help regulate metabolism, the immune system, blood pressure and other essential functions.
Congenital adrenal hyperplasia affects the production of one or more of three steroid hormones: cortisol, which regulates your body’s response to illness or stress; mineralocorticoids, such as aldosterone, which regulate sodium and potassium levels; or androgens, such as testosterone, which are sex hormones. In many cases, congenital adrenal hyperplasia results in lack of cortisol and overproduction of androgen.
The milder and more common form of congenital adrenal hyperplasia is called nonclassic. The classic form, which is more severe, can be detected in newborn screening programs. Some forms of congenital adrenal hyperplasia can cause problems with normal growth and development in children and even be life-threatening.
Although there is no cure, with proper treatment, most people with congenital adrenal hyperplasia can lead normal lives.
Congenital adrenal hyperplasia causes
In 95 percent of cases, the enzyme lacking in congenital adrenal hyperplasia is 21-hydroxylase. Congenital adrenal hyperplasia may sometimes be called 21-hydroxylase deficiency. There are other much rarer enzyme deficiencies that also cause congenital adrenal hyperplasia.
Congenital adrenal hyperplasia is passed along in an inheritance pattern called autosomal recessive. Children who have the condition have two parents who either have congenital adrenal hyperplasia themselves or who are both carriers of the genetic mutation that causes the condition.
Risk factors for congenital adrenal hyperplasia
Factors that increase the risk of having congenital adrenal hyperplasia include:
- Parents who both have congenital adrenal hyperplasia or are both carriers of the genetic defect for the disorder
- People in certain ethnic groups, particularly Ashkenazi Jews, but also Hispanics, Italians, Yugoslavians and Yupik Inuits
Congenital adrenal hyperplasia prevention
There is no known way to prevent congenital adrenal hyperplasia. Your doctors may recommend genetic counseling if you’re thinking of starting a family and you’re at risk of having a child with congenital adrenal hyperplasia.
Congenital adrenal hyperplasia symptoms
Signs and symptoms of congenital adrenal hyperplasia vary, depending on which gene is defective and the level of enzyme deficiency.
There are two major types of congenital adrenal hyperplasia:
- Classic congenital adrenal hyperplasia. This more-severe form of the disease is usually detected in infancy.
- Nonclassic congenital adrenal hyperplasia. This milder and more common form may not become evident until childhood or early adulthood.
Classic congenital adrenal hyperplasia
Approximately two-thirds of people with classic congenital adrenal hyperplasia are classified as having the salt-losing form, while one-third have the simple-virilizing form. In both forms, affected females have genital ambiguity.
A child with classic congenital adrenal hyperplasia may experience:
- A lack in the production of cortisol in both the salt-losing and simple-virilizing forms. Most of the problems caused by classic Congenital adrenal hyperplasia are related to a lack of cortisol, which plays an important role in regulating your blood pressure, maintaining blood sugar and energy levels, and protecting your body against stress.
- A lack in the production of aldosterone in the salt-losing form. This can lead to low blood pressure, a lower sodium level and a higher potassium level. Sodium and potassium normally work together to help maintain the right balance of fluids in your body.
- Excess production of the male sex hormones (androgens such as testosterone). This can result in short height, early puberty and in females, abnormal genital development while in the womb.
Signs and symptoms of classic congenital adrenal hyperplasia in infants include:
- In females, enlarged clitoris or genitals that look more male than female (ambiguous genitalia) at birth, but males have normal appearing genitals
- Significant illness related to a lack of cortisol, aldosterone or both (adrenal crisis), which can be life-threatening
Signs and symptoms of classic congenital adrenal hyperplasia in children and adults include:
- Very early appearance of pubic hair
- Rapid growth during childhood, but shorter than average final height
Nonclassic congenital adrenal hyperplasia
This form of congenital adrenal hyperplasia is milder than classic congenital adrenal hyperplasia. Often there are no symptoms at birth. The condition is not identified on routine infant blood screening and often only becomes evident in late childhood or early adulthood. Hormone deficiency may only involve cortisol levels.
Although teenage and adult females may have normal appearing genitals at birth, later signs and symptoms often include:
- Irregular or absent menstrual periods
- Masculine characteristics such as facial hair, excessive body hair and a deepening voice
- Severe acne
In both females and males, signs and symptoms of nonclassic congenital adrenal hyperplasia also may include:
- Early appearance of pubic hair
- Rapid growth during childhood, but shorter than average final height
Classic congenital adrenal hyperplasia is usually detected at birth through required newborn screening or when female babies show ambiguous genitalia. Congenital adrenal hyperplasia may also be identified when male or female babies show signs of severe illness due to low levels of cortisol, aldosterone or both.
In nonclassic congenital adrenal hyperplasia, you may notice signs and symptoms of early puberty in your toddler or child. In this case, or if you have concerns about your child’s growth or development, make an appointment with your child’s pediatrician.
If you’re pregnant and may be at risk of congenital adrenal hyperplasia because of your own medical history or your ethnicity, ask your doctor about genetic counseling.
Congenital adrenal hyperplasia complications
Complications depend on the type of congenital adrenal hyperplasia and its severity.
People with classic congenital adrenal hyperplasia are at risk of experiencing adrenal crisis. This is caused by severely low levels of cortisol in the blood, resulting in diarrhea, vomiting, dehydration, low blood sugar levels and shock. It’s a life-threatening medical emergency that requires immediate treatment. Impaired production of aldosterone may occur as well, leading to dehydration with low sodium and high potassium levels. Adrenal crisis does not occur in the nonclassic form of congenital adrenal hyperplasia.
In classic and nonclassic congenital adrenal hyperplasia, males and females may eventually experience fertility problems.
Congenital adrenal hyperplasia diagnosis
Diagnosis of congenital adrenal hyperplasia may include the following tests.
Prenatal testing
Tests to diagnose congenital adrenal hyperplasia in fetuses can be done when siblings have the disease or family members are known to carry the gene defect. One of these tests may be done:
- Amniocentesis. This procedure involves using a needle to withdraw a sample of amniotic fluid from the womb, and then examining the cells.
- Chorionic villus sampling. This test involves withdrawing cells from the placenta for examination.
Newborns, infants and children
All newborns in the United States are screened for classic congenital adrenal hyperplasia caused by genetic 21-hydroxylase deficiency during the first few days of life. This test does not identify nonclassic congenital adrenal hyperplasia.
Diagnosis of congenital adrenal hyperplasia includes:
- Physical exam. The doctor examines your child and evaluates symptoms. If, based on these findings, the doctor suspects congenital adrenal hyperplasia, the next step is to confirm the diagnosis with blood and urine tests.
- Blood and urine tests. Tests used to diagnose congenital adrenal hyperplasia measure levels of hormones produced by the adrenal glands. A diagnosis can be made when there are abnormal levels of these hormones.
- Gene testing. In older children and young adults, genetic testing may be needed to diagnose congenital adrenal hyperplasia.
- Testing to determine a child’s sex. In female infants who have severe ambiguous genitalia, tests can be done to analyze chromosomes to identify genetic sex. Also, pelvic ultrasound can be used to identify the presence of female reproductive structures such as the uterus and ovaries.
Congenital adrenal hyperplasia treatment
Your doctor will likely refer your child to a specialist in childhood hormonal issues (pediatric endocrinologist) for treatment of congenital adrenal hyperplasia. The health care team may also include other specialists, such as urologists, psychologists and geneticists, as needed.
Treatment will depend on the type of congenital adrenal hyperplasia and the severity of symptoms and is aimed at reducing excess androgen production and replacing deficient hormones. People with nonclassical congenital adrenal hyperplasia may not require treatment or may need only small doses of corticosteroids.
Medications
Your child’s doctor may prescribe replacement hormone medication taken on a daily basis to restore normal levels of deficient hormones. Additional medications or higher doses may be needed during periods of illness or significant stress such as surgery.
Medications may include:
- Corticosteroids to replace cortisol ― this is the main treatment
- Mineralocorticoids to replace aldosterone to help retain salt and get rid of excess potassium
- Salt supplements to help retain salt
Monitoring the effectiveness of medication includes regularly scheduled:
- Physical exams. The doctor can check your child’s growth and development, including monitoring changes in height, weight, blood pressure and bone growth.
- Monitoring for side effects. The doctor can also monitor your child for side effects, such as the loss of bone mass and impaired growth, particularly if steroid-type replacement medication doses are high and used long term.
- Blood tests to check hormone levels. It’s critical to have regular blood tests that indicate whether medications need adjusting. Adequate cortisone replacement is needed to suppress androgens, allowing for normal height in growing children and minimizing masculine characteristics in females. However, too much cortisone may cause Cushing’s syndrome.
As adults, some men and women with nonclassic congenital adrenal hyperplasia are able to stop taking their replacement hormone medications. But others, particularly people with symptoms or with the classic form of congenital adrenal hyperplasia, may need to take replacement hormone medications indefinitely.
Possible reconstructive surgery for females
In some female infants with severe ambiguous genitalia as a result of classic congenital adrenal hyperplasia, reconstructive surgery to normalize the appearance and function of the genitals may be recommended.
This procedure may involve reducing the size of the clitoris and reconstructing the vaginal opening. The surgery is typically performed between 2 and 6 months of age. Females who have corrective genital surgery may need more cosmetic surgery later in life.
Some parents choose to wait for surgery until their child is old enough to understand the risks and choose his or her own gender assignment. However, performing corrective genital surgery when females are very young is technically easier than it is in later years.
Before making decisions about the best treatment approach for your child, talk with your doctor about these issues. Working together, you and your doctor can make informed choices that will help your child thrive.
Psychological support can be important to the emotional health and social adjustment of females with genital abnormalities.
Prenatal management
When identified before birth, treatment for congenital adrenal hyperplasia can begin while the fetus is still in the womb. A synthetic corticosteroid that crosses the placenta to the infant can be taken by the mother during pregnancy. This may reduce the secretion of male hormones (androgens), allowing female genitals to develop normally.
This treatment is still considered experimental. There’s no clear evidence yet about the long-term safety of this drug. Because of the side effects and how the treatment might affect brain development, this remains a controversial treatment.
Congenital adrenal hyperplasia prognosis
Many children with Congenital adrenal hyperplasia can successfully manage the condition by staying on their replacement hormone medications. They grow up to lead healthy lives with a normal life expectancy.
Coping and support
Early and steady support from family and health care professionals can help your child grow up to have normal self-esteem and a satisfying social life. These approaches may help:
- Include psychological counseling in your child’s treatment plan as needed
- Seek help from a mental health professional if you’re having trouble coping and to help you develop healthy parenting strategies
Endometrial hyperplasia
Endometrial hyperplasia occurs when the endometrium, the lining of the uterus, becomes too thick. Endometrial hyperplasia is not cancer, but in some cases, it can lead to cancer of the uterus.
Endometrial hyperplasia usually occurs after menopause, when ovulation stops and progesterone is no longer made. It also can occur during perimenopause, when ovulation may not occur regularly. Listed as follows are other situations in which women may have high levels of estrogen and not enough progesterone:
- Use of medications that act like estrogen
- Long-term use of high doses of estrogen after menopause (in women who have not had a hysterectomy)
- Irregular menstrual periods, especially associated with polycystic ovary syndrome or infertility
- Obesity
The endometrium changes throughout the menstrual cycle in response to hormones. During the first part of the cycle, the hormone estrogen is made by the ovaries. Estrogen causes the lining to grow and thicken to prepare the uterus for pregnancy. In the middle of the cycle, an egg is released from one of the ovaries (ovulation). Following ovulation, levels of another hormone called progesterone begin to increase. Progesterone prepares the endometrium to receive and nourish a fertilized egg. If pregnancy does not occur, estrogen and progesterone levels decrease. The decrease in progesterone triggers menstruation, or shedding of the lining. Once the lining is completely shed, a new menstrual cycle begins.
Types of endometrial hyperplasia
Endometrial hyperplasia is classified as simple or complex. Endometrial hyperplasia also is classified by whether certain cell changes are present or absent. If abnormal changes are present, it is called atypical. The terms are combined to describe the exact kind of hyperplasia:
- Simple endometrial hyperplasia
- Complex endometrial hyperplasia
- Simple atypical endometrial hyperplasia
- Complex atypical endometrial hyperplasia
Endometrial hyperplasia causes
Endometrial hyperplasia most often is caused by excess estrogen without progesterone. If ovulation does not occur, progesterone is not made, and the lining is not shed. The endometrium may continue to grow in response to estrogen. The cells that make up the lining may crowd together and may become abnormal. This condition, called hyperplasia, may lead to cancer in some women.
Risk factors are associated with endometrial hyperplasia
Endometrial hyperplasia is more likely to occur in women with the following risk factors:
- Age older than 35 years
- White race
- Never having been pregnant
- Older age at menopause
- Early age when menstruation started
- Personal history of certain conditions, such as diabetes mellitus, polycystic ovary syndrome (PCOS), gallbladder disease, or thyroid disease
- Obesity
- Cigarette smoking
- Family history of ovarian, colon, or uterine cancer
Endometrial hyperplasia prevention
You can take the following steps to reduce the risk of endometrial hyperplasia:
- If you take estrogen after menopause, you also need to take progestin or progesterone.
- If your menstrual periods are irregular, birth control pills (oral contraceptives) may be recommended. They contain estrogen along with progestin. Other forms of progestin also may be taken.
- If you are overweight, losing weight may help. The risk of endometrial cancer increases with the degree of obesity.
Endometrial hyperplasia symptoms
The most common sign of hyperplasia is abnormal uterine bleeding. If you have any of the following, you should see your health care provider:
- Bleeding during the menstrual period that is heavier or lasts longer than usual
- Menstrual cycles that are shorter than 21 days (counting from the first day of the menstrual period to the first day of the next menstrual period)
- Any bleeding after menopause
Endometrial hyperplasia diagnosis
There are many causes of abnormal uterine bleeding. If you have abnormal bleeding and you are 35 years or older, or if you are younger than 35 years and your abnormal bleeding has not been helped by medication, your health care provider may perform diagnostic tests for endometrial hyperplasia and cancer.
Transvaginal ultrasound may be done to measure the thickness of the endometrium. For this test, a small device is placed in your vagina. Sound waves from the device are converted into images of the pelvic organs. If the endometrium is thick, it may mean that endometrial hyperplasia is present.
The only way to tell for certain that cancer is present is to take a small sample of tissue from the endometrium and study it under a microscope. This can be done with an endometrial biopsy, dilation and curettage, or hysteroscopy.
Endometrial hyperplasia treatment
In many cases, endometrial hyperplasia can be treated with progestin. Progestin is given orally, in a shot, in an intrauterine device, or as a vaginal cream. How much and how long you take it depends on your age and the type of hyperplasia. Treatment with progestin may cause vaginal bleeding like a menstrual period.
If you have atypical hyperplasia, especially complex atypical hyperplasia, the risk of cancer is increased. Hysterectomy usually is the best treatment option if you do not want to have any more children.
Prostatic hyperplasia
Benign prostatic hyperplasia (BPH) — also called prostate gland enlargement — is a common condition as men get older. An enlarged prostate gland can cause uncomfortable urinary symptoms, such as blocking the flow of urine out of the bladder. It can also cause bladder, urinary tract or kidney problems.
There are several effective treatments for prostate gland enlargement, including medications, minimally invasive therapies and surgery. To choose the best option, you and your doctor will consider your symptoms, the size of your prostate, other health conditions you might have and your preferences.
If you’re having urinary problems, discuss them with your doctor. Even if you don’t find urinary symptoms bothersome, it’s important to identify or rule out any underlying causes. Untreated, urinary problems might lead to obstruction of the urinary tract.
If you’re unable to pass any urine, seek immediate medical attention.
Prostatic hyperplasia causes
The prostate gland is located beneath your bladder. The tube that transports urine from the bladder out of your penis (urethra) passes through the center of the prostate. When the prostate enlarges, it begins to block urine flow.
Most men have continued prostate growth throughout life. In many men, this continued growth enlarges the prostate enough to cause urinary symptoms or to significantly block urine flow.
It isn’t entirely clear what causes the prostate to enlarge. However, it might be due to changes in the balance of sex hormones as men grow older.
Risk factors for prostatic hyperplasia
Risk factors for prostate gland enlargement include:
- Aging. Prostate gland enlargement rarely causes signs and symptoms in men younger than age 40. About one-third of men experience moderate to severe symptoms by age 60, and about half do so by age 80.
- Family history. Having a blood relative, such as a father or a brother, with prostate problems means you’re more likely to have problems.
- Diabetes and heart disease. Studies show that diabetes, as well as heart disease and use of beta blockers, might increase the risk of benign prostatic hyperplasia.
- Lifestyle. Obesity increases the risk of benign prostatic hyperplasia, while exercise can lower your risk.
Prostatic hyperplasia symptoms
The severity of symptoms in people who have prostate gland enlargement varies, but symptoms tend to gradually worsen over time. Common signs and symptoms of benign prostate hyperplasia include:
- Frequent or urgent need to urinate
- Increased frequency of urination at night (nocturia)
- Difficulty starting urination
- Weak urine stream or a stream that stops and starts
- Dribbling at the end of urination
- Inability to completely empty the bladder
Less common signs and symptoms include:
- Urinary tract infection (UTI)
- Inability to urinate
- Blood in the urine
The size of your prostate doesn’t necessarily determine the severity of your symptoms. Some men with only slightly enlarged prostates can have significant symptoms, while other men with very enlarged prostates can have only minor urinary symptoms.
In some men, symptoms eventually stabilize and might even improve over time.
Other possible causes of urinary symptoms
Conditions that can lead to symptoms similar to those caused by enlarged prostate include:
- Urinary tract infection (UTI)
- Inflammation of the prostate (prostatitis)
- Narrowing of the urethra (urethral stricture)
- Scarring in the bladder neck as a result of previous surgery
- Bladder or kidney stones
- Problems with nerves that control the bladder
- Cancer of the prostate or bladder
Prostatic hyperplasia complications
Complications of an enlarged prostate can include:
- Sudden inability to urinate (urinary retention). You might need to have a tube (catheter) inserted into your bladder to drain the urine. Some men with an enlarged prostate need surgery to relieve urinary retention.
- Urinary tract infections (UTIs). Inability to fully empty the bladder can increase the risk of infection in your urinary tract. If UTIs occur frequently, you might need surgery to remove part of the prostate.
- Bladder stones. These are generally caused by an inability to completely empty the bladder. Bladder stones can cause infection, bladder irritation, blood in the urine and obstruction of urine flow.
- Bladder damage. A bladder that hasn’t emptied completely can stretch and weaken over time. As a result, the muscular wall of the bladder no longer contracts properly, making it harder to fully empty your bladder.
- Kidney damage. Pressure in the bladder from urinary retention can directly damage the kidneys or allow bladder infections to reach the kidneys.
Most men with an enlarged prostate don’t develop these complications. However, acute urinary retention and kidney damage can be serious health threats.
Having an enlarged prostate is not believed to increase your risk of developing prostate cancer.
Prostatic hyperplasia diagnosis
Your doctor will start by asking detailed questions about your symptoms and doing a physical exam. This initial exam is likely to include:
- Digital rectal exam. The doctor inserts a finger into the rectum to check your prostate for enlargement.
- Urine test. Analyzing a sample of your urine can help rule out an infection or other conditions that can cause similar symptoms.
- Blood test. The results can indicate kidney problems.
- Prostate-specific antigen (PSA) blood test. PSA is a substance produced in your prostate. PSA levels increase when you have an enlarged prostate. However, elevated PSA levels can also be due to recent procedures, infection, surgery or prostate cancer.
After that, your doctor might recommend additional tests to help confirm an enlarged prostate and to rule out other conditions. These tests include:
- Urinary flow test. You urinate into a receptacle attached to a machine that measures the strength and amount of your urine flow. Test results help determine over time if your condition is getting better or worse.
- Postvoid residual volume test. This test measures whether you can empty your bladder completely. The test can be done using ultrasound or by inserting a catheter into your bladder after you urinate to measure how much urine is left in your bladder.
- 24-hour voiding diary. Recording the frequency and amount of urine might be especially helpful if more than one-third of your daily urinary output occurs at night.
If your condition is more complex, your doctor may recommend:
- Transrectal ultrasound. An ultrasound probe is inserted into your rectum to measure and evaluate your prostate.
- Prostate biopsy. Transrectal ultrasound guides needles used to take tissue samples (biopsies) of the prostate. Examining the tissue can help your doctor diagnose or rule out prostate cancer.
- Urodynamic and pressure flow studies. A catheter is threaded through your urethra into your bladder. Water — or, less commonly, air — is slowly injected into your bladder. Your doctor can then measure bladder pressure and determine how well your bladder muscles are working. These studies are usually used only in men with suspected neurological problems and in men who have had a previous prostate procedure and still have symptoms.
- Cystoscopy. A lighted, flexible instrument (cystoscope) is inserted into your urethra, allowing your doctor to see inside your urethra and bladder. You will be given a local anesthetic before this test.
Prostatic hyperplasia treatment
A wide variety of treatments are available for enlarged prostate, including medication, minimally invasive therapies and surgery. The best treatment choice for you depends on several factors, including:
- The size of your prostate
- Your age
- Your overall health
- The amount of discomfort or bother you are experiencing
If your symptoms are tolerable, you might decide to postpone treatment and simply monitor your symptoms. For some men, symptoms can ease without treatment.
Medication
Medication is the most common treatment for mild to moderate symptoms of prostate enlargement. The options include:
- Alpha blockers. These medications relax bladder neck muscles and muscle fibers in the prostate, making urination easier. Alpha blockers — which include alfuzosin (Uroxatral), doxazosin (Cardura), tamsulosin (Flomax) and silodosin (Rapaflo) — usually work quickly in men with relatively small prostates. Side effects might include dizziness and a harmless condition in which semen goes back into the bladder instead of out the tip of the penis (retrograde ejaculation).
- 5-alpha reductase inhibitors. These medications shrink your prostate by preventing hormonal changes that cause prostate growth. These medications — which include finasteride (Proscar) and dutasteride (Avodart) — might take up to six months to be effective. Side effects include retrograde ejaculation.
- Combination drug therapy. Your doctor might recommend taking an alpha blocker and a 5-alpha reductase inhibitor at the same time if either medication alone isn’t effective.
- Tadalafil (Cialis). Studies suggest this medication, which is often used to treat erectile dysfunction, can also treat prostate enlargement.
Minimally invasive or surgical therapy
Minimally invasive or surgical therapy might be recommended if:
- Your symptoms are moderate to severe
- Medication hasn’t relieved your symptoms
- You have a urinary tract obstruction, bladder stones, blood in your urine or kidney problems
- You prefer definitive treatment
Minimally invasive or surgical therapy might NOT be an option if you have:
- An untreated urinary tract infection
- Urethral stricture disease
- A history of prostate radiation therapy or urinary tract surgery
- A neurological disorder, such as Parkinson’s disease or multiple sclerosis
Any type of prostate procedure can cause side effects. Depending on the procedure you choose, complications might include:
- Semen flowing backward into the bladder instead of out through the penis during ejaculation (retrograde ejaculation)
- Temporary difficulty with urination
- Urinary tract infection
- Bleeding
- Erectile dysfunction
- Very rarely, loss of bladder control (incontinence)
There are several types of minimally invasive or surgical therapies.
Transurethral resection of the prostate (TURP)
- A lighted scope is inserted into your urethra, and the surgeon removes all but the outer part of the prostate. TURP generally relieves symptoms quickly, and most men have a stronger urine flow soon after the procedure. After TURP you might temporarily need a catheter to drain your bladder.
Transurethral incision of the prostate (TUIP)
- A lighted scope is inserted into your urethra, and the surgeon makes one or two small cuts in the prostate gland — making it easier for urine to pass through the urethra. This surgery might be an option if you have a small or moderately enlarged prostate gland, especially if you have health problems that make other surgeries too risky.
Transurethral microwave thermotherapy (TUMT)
- Your doctor inserts a special electrode through your urethra into your prostate area. Microwave energy from the electrode destroys the inner portion of the enlarged prostate gland, shrinking it and easing urine flow. TUMT might only partially relieve your symptoms, and it might take some time before you notice results. This surgery is generally used only on small prostates in special circumstances because re-treatment might be necessary.
Transurethral needle ablation (TUNA)
- In this outpatient procedure, a scope is passed into your urethra, allowing your doctor to place needles into your prostate gland. Radio waves pass through the needles, heating and destroying excess prostate tissue that’s blocking urine flow.
- This procedure might be a good choice if you bleed easily or have certain other health problems. However, like TUMT, TUNA might only provide partial relief and results might take some time.
Laser therapy
A high-energy laser destroys or removes overgrown prostate tissue. Laser therapy generally relieves symptoms right away and has a lower risk of side effects than does nonlaser surgery. Laser therapy might be used in men who shouldn’t have other prostate procedures because they take blood-thinning medications.
The options for laser therapy include:
- Ablative procedures. These procedures vaporize obstructive prostate tissue to increase urine flow. Examples include photoselective vaporization of the prostate (PVP) and holmium laser ablation of the prostate (HoLAP). Ablative procedures can cause irritating urinary symptoms after surgery, so in rare situations another resection procedure might be needed at some point.
- Enucleative procedures. Enucleative procedures, such as holmium laser enucleation of the prostate (HoLEP), generally remove all the prostate tissue blocking urine flow and prevent regrowth of tissue. The removed tissue can be examined for prostate cancer and other conditions. These procedures are similar to open prostatectomy.
Prostatic urethral lift (PUL)
- In this relatively new transurethral procedure, special tags are used to compress the sides of the prostate to increase the flow of urine. The procedure might be recommended if you have lower urinary tract symptoms. However, PUL might not be as effective at reducing long-term urinary symptoms as TURP. More research is needed. PUL also might be offered to some men concerned about treatment impact on erectile dysfunction and ejaculatory problems, since the effect on ejaculation and sexual function is much lower with PUL than it is with TURP.
Embolization
- In this experimental procedure, the blood supply to or from the prostate is selectively blocked, causing the prostate to decrease in size. Long-term data on the effectiveness of this procedure aren’t available.
Open or robot-assisted prostatectomy
- The surgeon makes an incision in your lower abdomen to reach the prostate and remove tissue. Open prostatectomy is generally done if you have a very large prostate, bladder damage or other complicating factors. The surgery usually requires a short hospital stay and is associated with a higher risk of needing a blood transfusion.
Prostatic hyperplasia follow-up care
Your follow-up care will depend on the specific technique used to treat your enlarged prostate.
Your doctor might recommend limiting heavy lifting and excessive exercise for seven days if you have laser ablation, transurethral needle ablation or transurethral microwave therapy. If you have open or robot-assisted prostatectomy, you might need to restrict activity for six weeks.
Prostatic hyperplasia home remedies
To help control the symptoms of an enlarged prostate, try to:
- Limit beverages in the evening. Don’t drink anything for an hour or two before bedtime to avoid middle-of-the-night trips to the toilet.
- Limit caffeine and alcohol. They can increase urine production, irritate the bladder and worsen symptoms.
- Limit decongestants or antihistamines. These drugs tighten the band of muscles around the urethra that control urine flow, making it harder to urinate.
- Go when you first feel the urge. Waiting too long might overstretch the bladder muscle and cause damage.
- Schedule bathroom visits. Try to urinate at regular times — such as every four to six hours during the day — to “retrain” the bladder. This can be especially useful if you have severe frequency and urgency.
- Follow a healthy diet. Obesity is associated with enlarged prostate.
- Stay active. Inactivity contributes to urine retention. Even a small amount of exercise can help reduce urinary problems caused by an enlarged prostate.
- Urinate — and then urinate again a few moments later. This practice is known as double voiding.
- Keep warm. Colder temperatures can cause urine retention and increase the urgency to urinate.
Alternative medicine
The Food and Drug Administration hasn’t approved any herbal medications for treatment of an enlarged prostate.
Studies on herbal therapies as a treatment for enlarged prostate have had mixed results. One study found that saw palmetto extract was as effective as finasteride in relieving symptoms of benign prostatic hyperplasia, although prostate volumes weren’t reduced. But a subsequent placebo-controlled trial found no evidence that saw palmetto is better than a placebo.
Other herbal treatments — including beta-sitosterol extracts, pygeum and rye grass — have been suggested as helpful for reducing enlarged prostate symptoms. But the safety and long-term efficacy of these treatments hasn’t been proved.
If you take any herbal remedies, tell your doctor. Certain herbal products might increase the risk of bleeding or interfere with other medications you’re taking.





{kind=link}