Contents
- What are ketones
- What is Ketosis ?
- Is ketosis the same as ketoacidosis?
- Ketones in urine
- Ketones in blood
What are ketones
Ketones or ketone bodies are intermediate products of fat metabolism. Ketones are produced when glucose is not available to the body’s cells as an energy source and/or when the body cannot use glucose as a fuel source because there is no insulin or not enough insulin. Ketones can form when a person does not eat enough carbohydrates (for example, in cases of fasting, starvation, high-protein diets, high-fat and low carb diet [e.g., ketogenic diet, Atkin’s diet]) or when a person’s body cannot use carbohydrates properly (e.g., type 1 diabetes, some type 2 diabetes). When carbohydrates are not available, the body metabolizes fat instead to get the energy it needs to keep functioning. When fat is metabolized, byproducts called ketone bodies build up in the blood, causing first ketosis and then progressing to ketoacidosis, a form of metabolic acidosis. This condition is most frequently seen with uncontrolled type 1 diabetes and can be a medical emergency. Moreover, in non-diabetics, strenuous exercise, exposure to cold, frequent, prolonged vomiting, and several digestive system diseases can also increase fat metabolism, resulting in ketosis and ketones in urine (ketonuria).
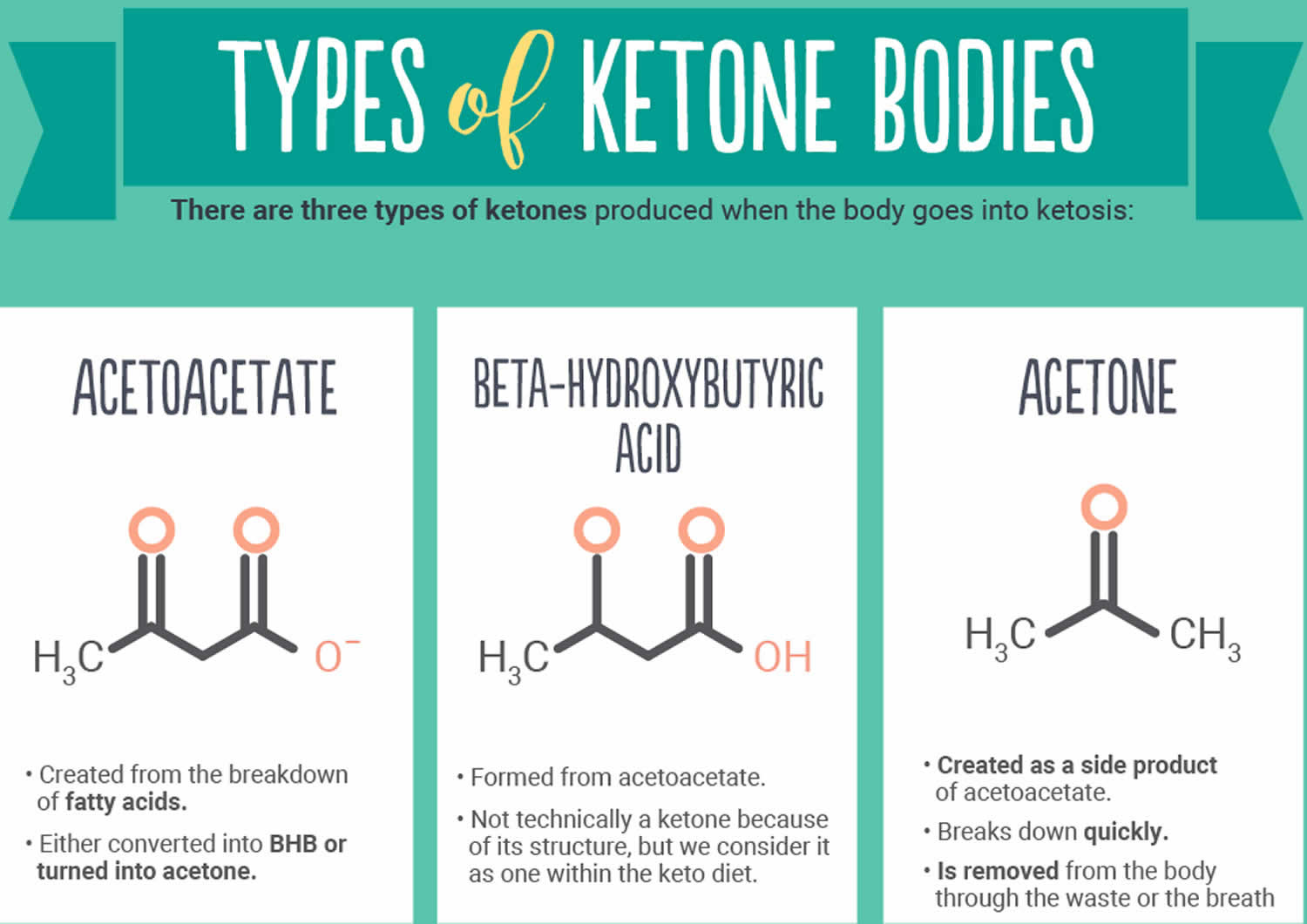
There are three ketone bodies:
- Acetoacetate,
- Beta-hydroxybutyrate, and
- Acetone.
Acetoacetate is created first. Beta-hydroxybutyrate is created from acetoacetate. Acetone is a spontaneously created side product of acetoacetate. Under normal conditions of adequate dietary carbohydrate, the production of free acetoacetic acid is negligible (<0.3 mmol/l) and this compound, transported via the blood stream, is rapidly metabolized by various tissues, especially the skeletal and heart muscles. In conditions of overproduction of acetoacetic acid, it accumulates above normal levels and part of it is converted to the other two ketone bodies leading to ketonemia and ketonuria (presence of ketone bodies in the blood and urine). Beta-hydroxybutyrate is the predominant ketone body present in severe diabetic ketoacidosis (DKA). Different ketone tests measure one or more ketone bodies, and their results are not interchangeable.
Acetone (produced by spontaneous decarboxylation of acetoacetate), being a very volatile compound, is eliminated mainly via respiration in the lungs, hence the characteristic sweet “fruity breath” breath odour of ketosis is caused by acetone, which, being a very volatile compound, is eliminated mainly via respiration in the lungs. Acetone even though it does not have metabolic functions, its presence can be useful from a clinical diagnostic point of view. Thus it is to be considered that a “fruity breath” indicates a condition of ketosis that could be physiological (fasting, low carbohydrate diet, post exercise) 1.
For the reasons described below, ketone levels are affected by several factors, such as energy balance, diet composition, diabetes (type 1 and 2) and physical activities, all of which underscore the importance of determining the accuracy of ketone levels, blood glucose and pH levels.
Ketone testing can be carried out at home. The most accurate way of testing for ketones is to use a blood glucose meter which can test for ketones as well as blood glucose levels. You can also test urine for ketone levels, however, the testing of urine means that the level you get is representative of your ketone levels up to a few hours ago.
- Blood ketone testing gives a snapshot of the status of ketone accumulation at the time that the sample was collected. Blood ketones may be measured in a laboratory or with a handheld monitor.
- The laboratory test uses serum, the liquid portion of the blood, and typically measures acetoacetate. Beta-hydroxybutyrate can be ordered as a separate blood test.
- When whole blood from a fingerstick is tested for ketones using a handheld monitor, the monitor measures beta-hydroxybutyrate. This test may be performed at a person’s bedside in a hospital or emergency room, in a doctor’s office, or performed by a person at home.
- Urine ketone testing reflects recent rather than current blood ketones. Urine testing is much more common than blood ketones testing. It may be performed by itself, with a urine glucose test, or as part of a urinalysis. The urine methods measure either acetoacetate or acetoacetate and acetone but do not usually detect beta-hydroxybutyrate.
Ketones and weight loss
As noted above, ketones are produced when the body burns fat. Therefore people that are losing a significant amount of weight may experience higher than normal ketone levels.
Ketone testing has also become used by people with type 2 diabetes on ketogenic diets to assess whether they are burning fat effectively.
Ketogenic diets are not usually recommended for people with insulin dependent diabetes as aiming for higher ketone levels could present a higher risk of ketoacidosis occurring.
Who needs to be aware of ketones?
The following people with diabetes should be aware of ketones and the symptoms of ketoacidosis:
- Anyone dependent on insulin – such as all people with type 1 diabetes
- People with type 2 diabetes that are taking SGLT2 inhibitors (such as Forxiga, Invokana and Jardiance)
It is essential to know what the symptoms are, and when you should test for ketones. Finding high levels of ketones present in your urine is a sign that the management of your diabetes needs adjusting.
Ketone testing will be important within pregnancy for anyone with diabetes on insulin. Pregnant women with type 2 diabetes or gestational diabetes that is not treated with insulin should contact their health team if experiencing the symptoms of ketoacidosis.
Ketone testing
Ketone testing is a key part of type 1 diabetes management as it helps to prevent a dangerous short term complication, ketoacidosis, from occurring.
If you have type 1 diabetes, it is recommended that you have ketone testing supplies on your prescription.
Ketone testing may also be useful in people with other types of diabetes that are dependent upon insulin.
Why diabetics need to test for ketones?
Ketones are produced by the body as an alternative source of energy to sugar. The body produces ketones by breaking down fats, this process is known as ketosis.
Ketones may be produced as part of weight loss, however, it’s important for people with diabetes on insulin to note that ketones can be produced when the body has insufficient insulin.
When the body has too little insulin, it means that cells of the body cannot take in enough sugar from the blood. To compensate for this, the body will start to break down fat to provide ketones.
However, if a high level of ketones is produced, this can cause the blood to become acidic which can lead to illness and even potential danger to organs if not treated in time.
What is Ketosis ?
Ketosis is a natural state the body finds itself in when it is using fat as its main fuel. This occurs when following a very low carb, ketogenic diet, and often during intermittent fasting too. Ketosis can be beneficial for a number of people but there are certain groups, such as people with type 1 diabetes, that need to be more careful. In these groups, very high ketone levels would lead to diabetic ketoacidosis, a dangerous situation caused by a lack of sufficient insulin.
What is nutritional ketosis?
Ketosis is a state the body goes into if it needs to break down body fat for energy. The state is marked by raised levels of ketones in the blood which can be used by the body as fuel. Ketones which are not used for fuel are excreted out of the body via the kidneys and the urine.
Under normal diet with average amount of carbohydrates and fat, insulin activates key enzymes in the glucose metabolic pathways, which store energy derived from carbohydrates, and when there is an absence or scarcity of dietary carbohydrates the resulting reduced insulin level leads to a reduction in fat formation (lipogenesis) and fat accumulation. After a few days of fasting, or of drastically reduced carbohydrate consumption (below 20 g/day), glucose reserves become insufficient both for normal fat oxidation via the supply of oxaloacetate in the Krebs cycle (which gave origin to the phrase ‘fat burns in the flame of carbohydrate’) and for the supply of glucose to the central nervous system 2, 3, 4, 5.
It should be stressed that, as shown in Table 1 (below), blood glucose level, even though reduced, remains within physiological levels 6. In fact glucose is formed from two sources: glucogenic amino acids and from glycerol liberated via lysis from triglycerides 7, 8. The importance of the second source increases progressively during the ketosis condition. In the first days of a ketogenic diet the main source of glucose is via neoglucogenesis from amino acids, as the days goes by, the contribution of amino acids decreases whilst the amount of glucose derived from glycerol increases. As a matter of fact glycerol (released from triglyceride hydrolysis) can produce more than 16% of glucose in the liver during a ketogenic diet and about 60% after a few days of complete fasting 7. According to Bortz (1972) of the new glucose formed from protein and glycerol 38% is derived from glycerol in the lean and 79% in the obese 9.
Figure 1. Metabolic pathway of ketosis and tissues ketolysis.
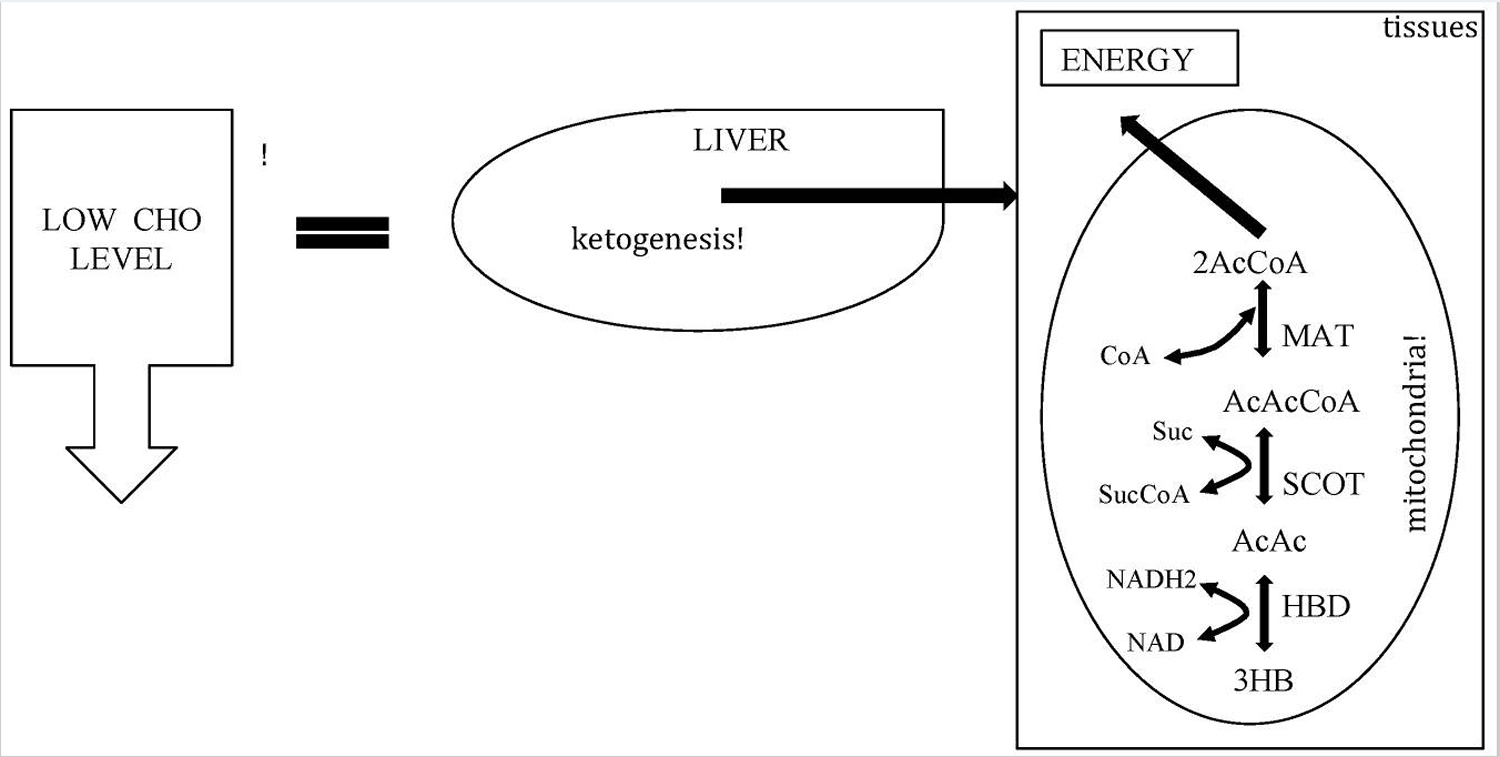
Footnote: CHO = carbohydrate.
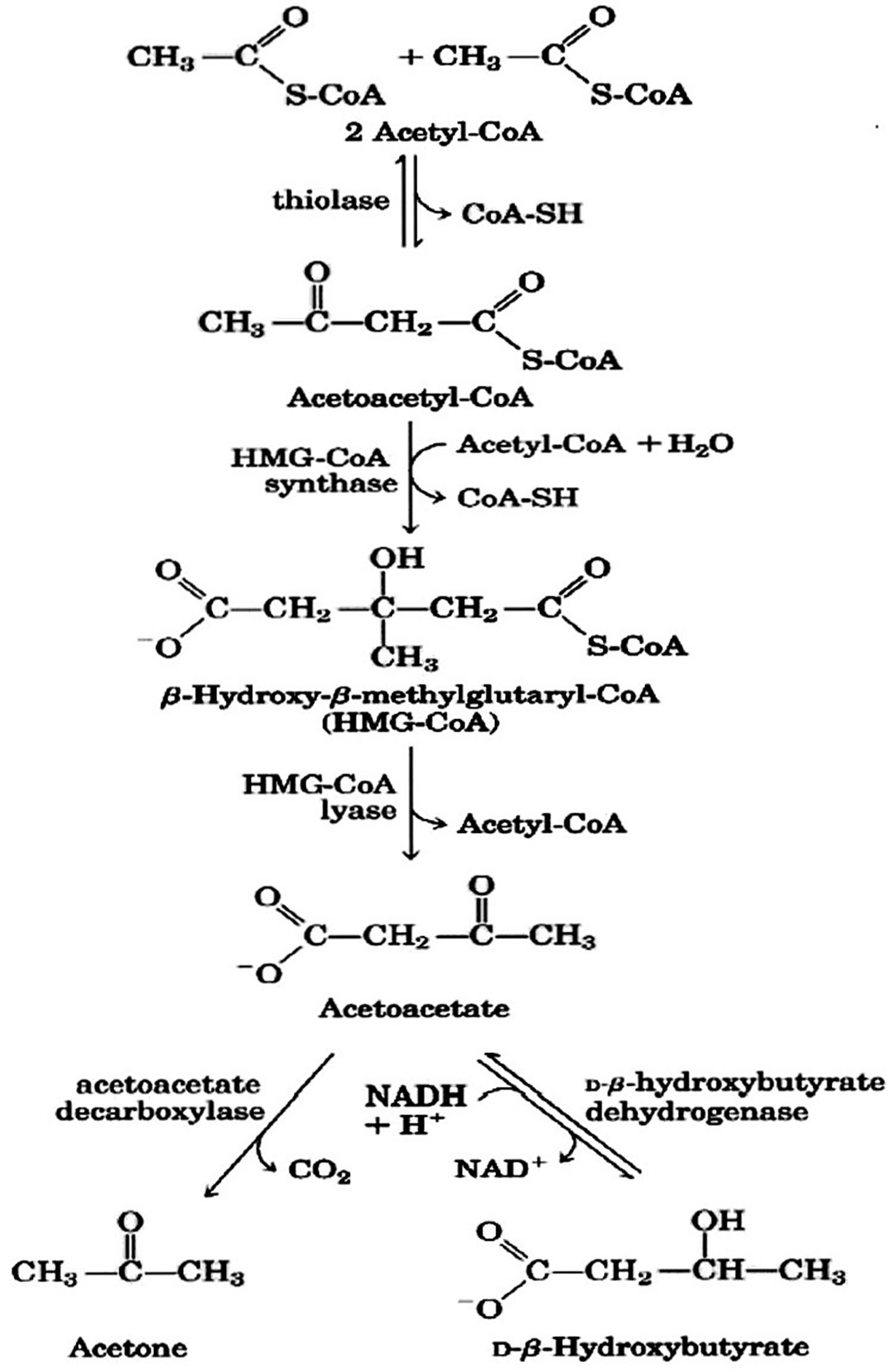
[Source 10 ]Figure 2. Ketone bodies formation from acetyl-CoA (acetyl coenzyme A).
 Footnote: Ketone bodies are used by tissues as a source of energy through a pathway that involves firstly that β-hydroxybutyric acid is converted back to acetoacetate (AcAc) this is then transformed into acetoacetyl-CoA and, finally, two molecules of acetyl-CoA are formed from acetoacetyl-CoA which are used in the Krebs cycle. [Source 10 ]
Footnote: Ketone bodies are used by tissues as a source of energy through a pathway that involves firstly that β-hydroxybutyric acid is converted back to acetoacetate (AcAc) this is then transformed into acetoacetyl-CoA and, finally, two molecules of acetyl-CoA are formed from acetoacetyl-CoA which are used in the Krebs cycle. [Source 10 ]The central nervous system (brain and spinal cord) cannot use fat as an energy source; hence, it normally utilizes glucose. After 3–4 days without carbohydrate consumption the central nervous system is ‘forced’ to find alternative energy sources, and as demonstrated by the classic experiments of Cahill and colleagues 2 this alternative energy source is derived from the overproduction of acetyl coenzyme A (acetyl CoA). This condition seen in prolonged fasting, type 1 diabetes and high-fat/low-carbohydrate diets (aka ketogenic diets) leads to the production of higher-than-normal levels of so-called ketone bodies, that is, acetoacetate, β-hydroxybutyric acid and acetone—a process called ketogenesis and which occurs principally in the mitochondrial matrix in the liver (see Figures 1 and 2) 11. It is important to underline that the liver produces ketone bodies, but is unable to utilize them because the absence of the enzyme 3-ketoacyl CoA transferase required to convert acetoacetate into acetoacetyl-CoA 12. Even though the main ketone body produced in the liver is acetoacetate, the primary circulating ketone is β-hydroxybutyrate 1. Under normal conditions of adequate dietary carbohydrate, the production of free acetoacetic acid is negligible (<0.3 mmol/l) and this compound, transported via the blood stream, is rapidly metabolized by various tissues, especially the skeletal and heart muscles. In conditions of overproduction of acetoacetic acid, it accumulates above normal levels and part of it is converted to the other two ketone bodies leading to ketonemia and ketonuria (presence of ketone bodies in the blood and urine).
Acetone (produced by spontaneous decarboxylation of acetoacetate), being a very volatile compound, is eliminated mainly via respiration in the lungs, hence the characteristic sweet “fruity breath” breath odour of ketosis is caused by acetone, which, being a very volatile compound, is eliminated mainly via respiration in the lungs. Acetone even though it does not have metabolic functions, its presence can be useful from a clinical diagnostic point of view. Thus it is to be considered that a “fruity breath” indicates a condition of ketosis that could be physiological (fasting, low carbohydrate diet, post exercise) 1.
Is ketosis the same as ketoacidosis?
Nutritional ketosis occurs when there is not enough carbohydrate in the diet to meet the body’s energy requirements. In this situation, the body switches over from burning sugar to burning fat as its main fuel. Fat, whether from the diet or the body’s stores, is broken down into ketones in the liver. These ketones are an efficient energy source for many organs, particularly the brain. Everyone has ketones in their blood at very low levels, under normal conditions. When the body enters ketosis, and so switches to burning mostly fat, levels of ketones in the blood increase.
Whereas physiological ketosis (nutritional and functional ketosis) is an important natural state allowing the body to run on fat for energy, diabetic ketoacidosis (DKA) is a dangerous and potentially fatal condition. Diabetic ketoacidosis occurs during situations of ‘internal starvation’ mainly in people with type 1 diabetes, when not enough insulin has been administered. In diabetic ketoacidosis, the body does not have enough insulin to allow blood glucose into cells. The body believes it is starving and so breaks down fat and protein into ketones at an alarming rate, far above what is seen in nutritional ketosis.
In most cases, ketoacidosis develops when there are both high ketone levels and high blood glucose.
It is of interest to underline that physiological ketosis (nutritional and functional ketosis) is a metabolic state characteristic of humans. Humans are more susceptible to ketosis-induced fasting due to the greater brain/body mass (this can explain why newborns are more susceptible to ketosis) 13. Under normal conditions the concentration of ketone bodies is very low (<0.3 mmol/L) compared to glucose (approx. 4 mmol) and since glucose and ketone bodies have a similar Km (or Michaelis-Menten constant) for glucose transport to the brain, the ketone bodies begin to be utilised as an energy source by the brain when they reach a concentration of about 4 mmol/L 14 which is close to the Km for the monocarboxylate transporter 15.
The ketone bodies begin to be utilized as an energy source by the central nervous system when they reach a concentration of about 4 mmol/l (normal level is <0.3 mmol/l), which is close to the Km for the monocarboxylate transporter 14, 11. The brain will use ketone bodies whenever provided with them (i.e., whenever blood ketone body levels rise). However, continued use of some glucose appears obligatory 16 and is supplied by way of hepatic gluconeogenesis 17.
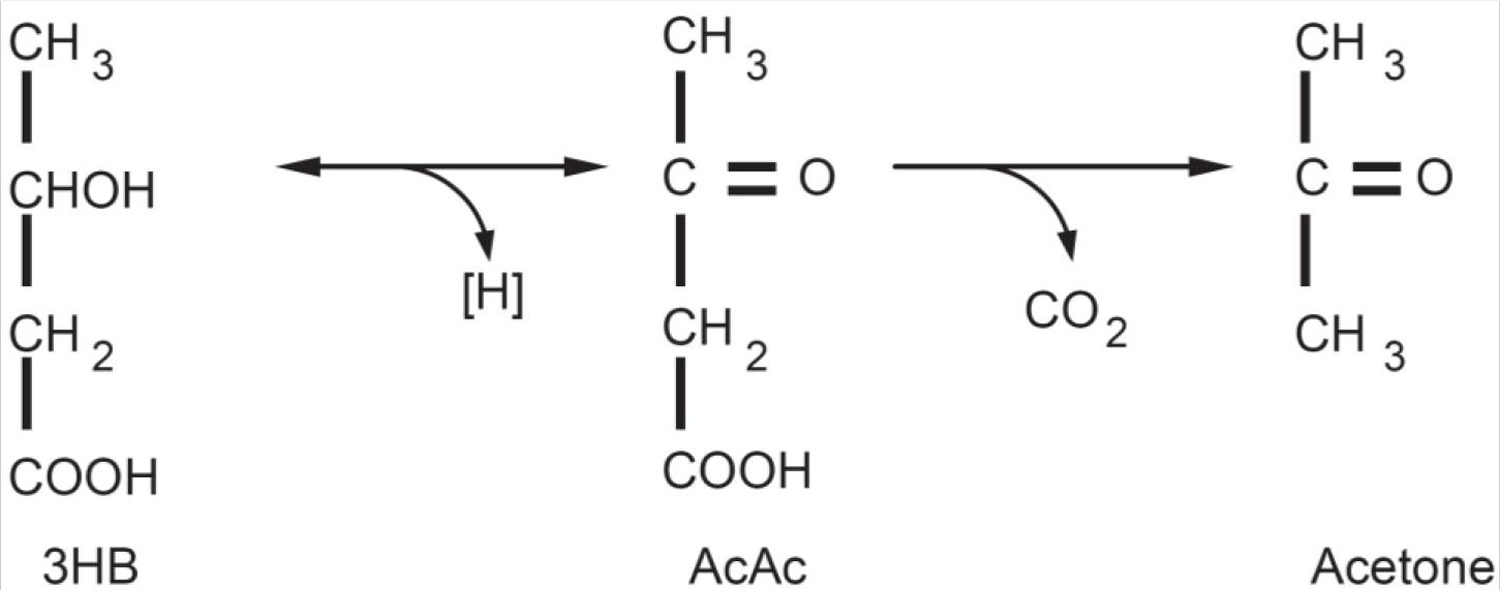
Figure 3. Ketone bodies: Acetoacetate (AcAc) is the principal ketone body. It is produced and utilized during intermediary metabolism and other ketone bodies are derived from it. Acetone is produced by the spontaneous decarboxylation of acetoacetate and is important from the clinical point of view because it is responsible for the fruity sweet odour of infant ketoacidosis. β-Hydroxybutyric acid (3HB) is produced via the reduction of acetoacetate. From a strictly biochemical point of view it is not actually a ketone body since the ketonic moiety is reduced to a hydroxyl group; it is though grouped among the ketone bodies. 3HB is relatively stable biochemically and is transported to the tissues where it is reconverted to AcAc.
| Blood levels | Normal diet | Ketogenic diet | Diabetic ketoacidosis |
|---|---|---|---|
| Glucose (mg/dl) | 80–120 | 65–80 | >300 |
| Insulin (μU/l) | 6–23 | 6.6–9.4 | ≅ 0 |
| Ketone bodies concentration (mℳ/l) | 0.1 | 7/8 | >25 |
| pH | 7.4 | 7.4 | <7.3 |
Footnote: Nutritional and Functional Ketosis are completely physiological mechanism and it was the biochemist Hans Krebs who first referred to physiological ketosis to differentiate it from the pathological ketoacidosis seen in type 1 diabetes 18. In physiological ketosis (which occurs during very-low-calorie ketogenic diets and in fasting), ketonemia reaches maximum levels of 7/8 mmol/l (it does not go higher precisely because the central nervous system efficiently uses these molecules for energy in place of glucose) and with no change in pH, whereas in uncontrolled diabetic ketoacidosis it can exceed 20 mmol/l with a concomitant lowering of blood pH 19, 20. Diabetic patients know that the detection in their urine of the ketone bodies is a danger signal that their diabetes is poorly controlled. Indeed, in severely uncontrolled diabetes, if the ketone bodies are produced in massive supranormal quantities, they are associated with ketoacidosis. In this life-threatening complication of diabetes mellitus, the acids 3-hydroxybutyric acid and acetoacetic acid are produced rapidly, causing high concentrations of protons, which overwhelm the body’s acid-base buffering system 17.
[Source 21 ]It is very important to note the difference between physiological ketosis (nutritional and functional ketosis) and pathological ketoacidosis (diabetic ketoacidosis).
- During Physiological ketosis, ketonemia (blood ketone bodies) reaches maximum levels of 7/8 mmol/L with no change in pH while in uncontrolled diabetic ketoacidosis it can exceed 20 mmol/L with a concomitant lowering of blood pH 22 (see Table 1). Blood levels of ketone bodies in healthy people do not exceed 8 mmol/L precisely because the central nervous system (brain) efficiently uses these molecules for energy in place of glucose.
- Diabetic Ketoacidosis is a dangerous complication faced by people with diabetes which happens when the body starts running out of insulin. Diabetic ketoacidosis is most commonly associated with type 1 diabetes, however, people with type 2 diabetes that produce very little of their own insulin may also be affected, but it may occur in situations of unusual physiologic stress. It is characterized by hyperglycemia (high blood glucose), hyperketonemia (very high blood ketone bodies), and metabolic acidosis (low blood pH). Hyperglycemia causes an osmotic diuresis with significant fluid and electrolyte loss. It causes nausea, vomiting, and abdominal pain and can progress to cerebral edema, coma, and death. Diabetic ketoacidosis is diagnosed by detection of hyperketonemia (very high blood ketone bodies) and anion gap metabolic acidosis in the presence of hyperglycemia 23. Ketoacidosis is a serious short term complication which can result in coma or even death if it is not treated quickly.
Under physiological ketosis or ketoacidosis, the liver metabolizes fatty acids to produce two water-soluble types of ketones: acetoacetic acid and beta-hydroxybutyric acid. A third type of ketone, i.e., acetone, is also produced by the enzymatic decarboxylation of acetoacetic acid. Due to its high vapor pressure, acetone crosses the membrane barrier into the alveoli of the lung and the airway. As a result, acetone is normally present in breath. Since, the ketone level in breath is reflective of ketone level in blood, breath acetone has been considered a reliable indicator of ketosis in adults consuming ketogenic meals 24 and can be used to predict plasma ketone bodies in children with epilepsy who are on a ketogenic diet 25. Most recently, breath acetone has been used as a new ketone biomarker because it is non-invasive, convenient, and an accurate reflection of the body’s ketone level 26. Breath testing for ketones has a high sensitivity and specificity and appears to be a noninvasive, convenient, and repeatable method for the diagnosis and therapeutic monitoring of ketosis 27.
Furthermore, there are other conditions, such as exercise that can actually decrease ketone levels in the blood by using ketone as an energy source in the muscles 28, 29. For the reasons described above, ketone levels are affected by several factors, such as energy balance, diet composition, diabetes (type 1 and 2) and physical activities, all of which underscore the importance of determining the accuracy of ketone levels, blood glucose and pH levels.
Who’s at greater risk of ketoacidosis?
Ketoacidosis is most common in children with type 1 diabetes. Diabetes association notes that in 2009-2010, 9% of children experienced at least one episode of diabetic ketoacidosis.
Groups at risk of ketoacidosis include, but is not limited to, people with:
- Type 1 diabetes
- Cystic fibrosis-related diabetes
- Pancreatectomy
- Type 2 diabetes with very little pancreatic function
It is possible, and can be beneficial, for people in these groups to follow a ketogenic lifestyle. However, it is important that your doctor is aware of your intention before you start. Your health team can help you with regard to how best to monitor for ketones and prevent ketoacidosis occurring.
Diabetic ketoacidosis symptoms
Diabetic ketoacidosis may itself be the symptom of undiagnosed type 1 diabetes.
Typical symptoms of diabetic ketoacidosis include:
- Vomiting
- Dehydration
- An unusual smell on the breath –sometimes compared to the smell of pear drops
- Deep laboured breathing (called kussmaul breathing) or hyperventilation
- Rapid heartbeat
- Confusion and disorientation
- Coma
Symptoms of diabetic ketoacidosis usually evolve over a 24 hour period if blood glucose levels become and remain too high (hyperglycemia).
How serious is diabetic ketoacidosis?
Diabetic ketoacidosis is a serious medical emergency. Without urgent treatment, this diabetes complication can lead to death. With adequate and rapid intervention and treatment, mortality rates are lowered to around 5%.
If someone with diabetes displays the signs of ketoacidosis, the situation should be treated as an emergency.
Causes and risk factors for diabetic ketoacidosis
As noted above, diabetic ketoacidosis is caused by the body having too little insulin to allow cells to take in glucose for energy.
This may happen for a number of reasons including:
- Having blood glucose levels consistently over 15 mmol/l
- Missing insulin injections
- If a fault has developed in your insulin pen or insulin pump
- As a result of illness or infections
- High or prolonged levels of stress
- Excessive alcohol consumption
- Illegal drug use
Diabetic ketoacidosis may also occur prior to a diagnosis of type 1 diabetes.
Ketoacidosis can occasionally occur in pregnancy and this can be very dangerous for both the mother to be and the child.
What is euglycemic diabetic ketoacidosis?
In most cases, ketoacidosis in people with diabetes will be accompanied by high sugar levels. However, ketoacidosis can also occur at low or normal blood glucose levels. This is referred to as euglycemic diabetic ketoacidosis and may occur if someone who is insulin dependent neither eats nor takes sufficient insulin for a prolonged period of time.
People on insulin pumps should be aware that euglycemic diabetic ketoacidosis could occur during or following exercise if insulin delivery is suspended for too long. Healthcare professionals recommend that insulin delivery is not suspended for more than 1 hour.
Can I get diabetic ketoacidosis if I have type 2 diabetes?
Yes, although it is not as common as in type 1 diabetes. It may occur in type 2 diabetes, especially when you have a severe infection or illness. Ketosis and ketoacidosis may also be seen in non-diabetics, people with starvation, alcoholism, and with high-fat, low-carbohydrate diets. It may be induced on purpose in some children with epilepsy who have frequent seizures and do not respond to available medications or other treatments.
How do I avoid diabetic ketoacidosis?
The best way to prevent diabetic ketoacidosis is to keep good blood glucose control at all times. Regularly testing your blood sugar levels at home will help you to manage your glucose levels.
If you experience difficulty in controlling your diabetes, speak to your doctor or diabetic consultant who can advise you or may refer you to go on a structured diabetes education course.
If you ever feel unwell or abnormal, you should test your blood sugar levels at once.
How is diabetic ketoacidosis diagnosed?
Diabetic ketoacidosis is usually diagnosed using blood and urine tests which measure the concentration of ketones in the blood or urine.
In addition to testing ketone levels, levels of potassium may also be measured as part of the treatment to check for signs of hypokalemia (low potassium levels). Potassium may be depleted as a result of excessive urination.
How is diabetic ketoacidosis treated?
Treatment of diabetic ketoacidosis involves administering intravenous fluids to correct dehydration and to replace any salts that may be lost from the body during ketoacidosis through passing excessive quantities of urine.
Insulin is also required to instantly suppress the ketone bodies that the body manufactures.
If an infection has been the underlying causes of diabetic ketoacidosis, you will be given a sick day plan to help you take the right amount of insulin. Close observation of the patient to quickly identify and prevent complications is essential and therefore you will usually be treated in hospital until your ketone levels have stabilised and you have returned to eating normally.
Can I test for ketones in my urine instead of my blood?
In many cases, yes, urine is tested much more frequently than blood. However, since it will not detect beta-hydroxybutyrate, the main ketone body with diabetic ketoacidosis (DKA), your healthcare provider may prefer that you monitor your blood.
Can I have ketosis or ketoacidosis and not know it?
You could have some degree of ketosis with few symptoms, but the accumulation of ketones triggers the symptoms, so they would emerge as concentrations increase.
Ketones in urine
The ketones in urine test is often used to help monitor people at a higher risk of developing ketones. These include people with type 1 or type 2 diabetes. If you have diabetes, ketones in urine can mean that you are not getting enough insulin. If you don’t have diabetes, you may still be at risk for developing ketones if you:
- Experience chronic vomiting and/or diarrhea
- Have a digestive disorder
- Participate in strenuous exercise
- Are on a very low-carbohydrate diet
- Have an eating disorder
- Are pregnant
Normal ketones urine test results
- A negative test result is normal.
- Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your provider about the meaning of your specific test results.
Normal results can vary, depending on your on your diet, activity level, and other factors. Because high ketone levels can be dangerous, be sure to talk to your health care provider about what is normal for you and what your results mean.
What are abnormal ketones in urine test results mean?
An abnormal ketones in urine test result means you have ketones in your urine. The results are usually listed as small, moderate, or large as follows:
- Small: <20 mg/dL
- Moderate: 30 to 40 mg/dL
- Large: >80 mg/dL
Ketones in urine causes
Ketones are not normally found in the urine. Ketones build up when the body needs to break down fats and fatty acids to use as fuel. This is most likely to occur when the body does not get enough sugar or carbohydrates.
Physiological ketosis (nutritional and functional ketosis) is a natural state the body finds itself in when it is using fat as its main fuel. This occurs when following a very low carb, ketogenic diet, and often during intermittent fasting too. Nutritional ketosis occurs when there is not enough carbohydrate in the diet to meet the body’s energy requirements. In this situation, the body switches over from burning sugar to burning fat as its main fuel. Fat, whether from the diet or the body’s stores, is broken down into ketones in the liver. These ketones are an efficient energy source for many organs, particularly the brain.
An abnormal ketones in urine test result may be due to:
- Fasting or starvation: such as with anorexia (an eating disorder)
- High protein or low carbohydrate diet
- Vomiting over a long period (such as during early pregnancy)
- Acute or severe illnesses, such as sepsis or burns
- High fevers
- The thyroid gland making too much thyroid hormone (hyperthyroidism)
- Nursing a baby, if the mother does not eat and drink enough
Everyone has ketones in their blood at very low levels, under normal conditions. When the body enters ketosis, and so switches to burning mostly fat, levels of ketones in the blood increase.
However, ketones in the urine is more common in type 1 diabetes. If you are suffering from high levels of ketones and contact your doctor or diabetes healthcare team as soon as possible.
This may be due to diabetic ketoacidosis (DKA). Diabetic ketoacidosis is a life-threatening problem that affects people with diabetes. It occurs when the body cannot use sugar (glucose) as a fuel source because there is no insulin or not enough insulin. Fat is used for fuel instead.
In a person who has diabetes, ketones in urine may be an early indication of insufficient insulin. With insufficient insulin, a diabetic cannot process glucose and instead metabolizes fat. This can cause ketones to build up in the blood, resulting first in ketosis and then progressing to ketoacidosis, a form of metabolic acidosis. Excess ketones and glucose are dumped into the urine by the kidneys in an effort to flush them from the body. This condition, called diabetic ketoacidosis (DKA), is most frequently seen with uncontrolled type 1 diabetes and can be a medical emergency.
Small or trace amounts of urine ketones may mean that ketone buildup is starting. You should test again in a few hours. Moderate or large amounts of urine ketones are a danger sign. They upset the chemical balance of your blood and can poison the body. Never exercise when your urine checks show moderate or large amounts of ketones and your blood glucose is high. These are signs that your diabetes is out of control. Talk to your doctor at once if your urine results show moderate or large amounts of ketones.
Why do I need a ketones in urine test?
Your health care provider may order a ketones in urine test if you have diabetes or other risk factors for developing ketones. You may also need this test if you have symptoms of ketoacidosis. These include:
- Nausea or vomiting
- Abdominal pain
- Confusion
- Trouble breathing
- Feeling extremely sleepy
People with type 1 diabetes are at a higher risk for ketoacidosis.
Ketones in urine symptoms
Ketone is a chemical produced when there is a shortage of carbohudrate in the blood and the body breaks down body fat for energy.
In healthy non-diabetic person, ketones in urine produce no symptoms except for the sweet “fruity breath” breath odour of ketosis is caused by acetone, which, being a very volatile compound, is eliminated mainly via respiration in the lungs.
In a diabetic, presence of high levels of ketones in the urine and bloodstream is a common complication of diabetes, which if left untreated can lead to ketoacidosis.
Typical symptoms of diabetic ketoacidosis include:
- Vomiting
- Dehydration
- An unusual smell on the breath –sometimes compared to the smell of pear drops
- Deep laboured breathing (called kussmaul breathing) or hyperventilation
- Rapid heartbeat
- Confusion and disorientation
- Coma
Symptoms of diabetic ketoacidosis usually evolve over a 24 hour period if blood glucose levels become and remain too high (hyperglycemia).
Protein and ketones in urine
The protein test pad provides a rough estimate of the amount of albumin in the urine. Albumin makes up about 60% of the total protein in the blood. Normally, there will be no protein or a small amount of protein in the urine. When urine protein is elevated, a person has a condition called proteinuria.
Proteinuria may occasionally be seen in healthy individuals. Healthy people can have temporary or persistent proteinuria due to stress, exercise, fever, aspirin therapy, or exposure to cold, for example. Repeat testing may be done once these conditions have resolved to determine whether the proteinuria is persistent.
If trace amounts of protein are detected, and depending on the person’s signs, symptoms and medical history, a repeat urinalysis and dipstick protein may be performed at a later time to see if there is still protein in the urine or if it has dropped back to undetectable levels.
If a large amount of protein is detected on a urinalysis and/or if the protein persists in repeated tests, a 24-hour urine protein test may be used as a follow-up test. Since the dipstick primarily measures albumin, the 24-hour urine protein test also may be ordered if a healthcare practitioner suspects that proteins other than albumin are being released into the urine.
Protein in the urine may be a sign of kidney disease. Small amounts of albumin may be found in the urine when kidney dysfunction begins to develop. A different test called a urine albumin test detects and measures small amounts of albumin in the urine. The urine albumin test is more sensitive than a dipstick urinalysis and is routinely used to screen people with chronic conditions that put them at risk for kidney disease, such as diabetes and high blood pressure.
Ketones in blood
Ketones blood test measures the amount of ketones in the blood. Blood ketones are primarily used to screen for, detect, and monitor a serious, sometimes life-threatening condition called diabetic ketoacidosis (DKA) in people with type 1 and sometimes type 2 diabetes. Diabetic ketoacidosis can occur when a diabetic’s blood glucose is significantly increased, with illness, severe infection, pregnancy, and a variety of other conditions.
Diabetic ketoacidosis is associated with sudden and severe high blood glucose (acute hyperglycemia), a severe insulin deficiency, and a disruption of the body’s acid-base balance. Excess ketones and glucose are dumped into the urine by the kidneys in an effort to flush them from the body. This causes increased urination, thirst, dehydration, and a loss of electrolytes. The affected person may also experience symptoms such as rapid breathing, shortness of breath, a fruity scent to the breath, nausea, vomiting, fatigue, confusion, and eventually coma.
Ketosis and ketoacidosis may also be seen with starvation, alcoholism, and with high-fat, low-carbohydrate diets (e.g., ketogenic diet, Atkin’s diet). It may be induced on purpose in some children with epilepsy who have frequent seizures and do not respond to available medications or other treatments.
There are three ketone bodies: acetoacetate, beta-hydroxybutyrate, and acetone. Beta-hydroxybutyrate is the predominant ketone body present in severe diabetic ketoacidosis. Different ketone tests measure one or more ketone bodies, and their results are not interchangeable.
Blood ketones are sometimes ordered, along with other tests such as blood gases, glucose, and electrolytes, to detect ketoacidosis in non-diabetics if they have signs and symptoms of diabetic ketoacidosis due to, for example, ingestion of excessive amounts of alcohol.
- If blood ketone levels are increased, then the person has some degree of ketosis or ketoacidosis.
- If levels are low or normal, then the person either does not have excess ketone production or the ketone body that is elevated is not being detected by the test method used.
When is blood ketones test ordered?
Blood ketone tests may be ordered when someone with diabetes has symptoms associated with diabetic ketoacidosis (DKA) and may also be performed whenever there is the potential for diabetic ketoacidosis (DKA) to develop, such as when a diabetic is sick or pregnant. With the availability of home monitoring, blood ketones can be ordered as frequently as the person’s healthcare provider recommends. Some signs and symptoms of ketoacidosis include:
- Increased urination, excessive thirst
- Dehydration, loss of electrolytes
- Rapid breathing, shortness of breath
- Fruity scent to the breath
- Nausea, vomiting
- Fatigue
- Confusion
- Coma (sometimes)
In non-diabetics, blood ketones are usually ordered when a person has symptoms associated with ketosis or ketoacidosis.
Recent studies have shown that serum ketones and beta-hydroxybutyrate testing are both effective in diagnosing diabetic ketoacidosis (DKA). Some healthcare practitioners prefer beta-hydroxybutyrate. In acute diabetic ketoacidosis (DKA), the ketone body ratio (beta-hydroxybutyrate:acetoacetate) rises from normal (1:1) to as high as 10:1. In response to insulin therapy, beta-hydroxybutyrate levels commonly decrease long before acetoacetate levels. However, beta-hydroxybutyrate is not available in all laboratories.
- Paoli A, Rubini A, Volek JS, Grimaldi KA. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. European Journal of Clinical Nutrition. 2013;67(8):789-796. doi:10.1038/ejcn.2013.116. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3826507/[↩][↩][↩]
- Brain metabolism during fasting. Owen OE, Morgan AP, Kemp HG, Sullivan JM, Herrera MG, Cahill GF Jr. J Clin Invest. 1967 Oct; 46(10):1589-95. https://www.ncbi.nlm.nih.gov/pubmed/6061736/[↩][↩]
- Amino acid metabolism during prolonged starvation. Felig P, Owen OE, Wahren J, Cahill GF Jr. J Clin Invest. 1969 Mar; 48(3):584-94. https://www.ncbi.nlm.nih.gov/pubmed/5773094/[↩]
- Owen O.E. Ketone bodies as a fuel for the brain during starvation. Biochem. Mol. Biol. Educ. 2005;33:246–251. doi: 10.1002/bmb.2005.49403304246.[↩]
- Liver and kidney metabolism during prolonged starvation. Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF Jr. J Clin Invest. 1969 Mar; 48(3):574-83. https://www.ncbi.nlm.nih.gov/pubmed/5773093/[↩]
- Targeting energy metabolism in brain cancer: review and hypothesis. Seyfried TN, Mukherjee P. Nutr Metab (Lond). 2005 Oct 21; 2:30. https://www.ncbi.nlm.nih.gov/pubmed/16242042/[↩]
- Lipolysis and gluconeogenesis from glycerol during weight reduction with very-low-calorie diets. Vazquez JA, Kazi U. Metabolism. 1994 Oct; 43(10):1293-9. https://www.ncbi.nlm.nih.gov/pubmed/7934983/[↩][↩]
- Gluconeogenesis and energy expenditure after a high-protein, carbohydrate-free diet. Veldhorst MA, Westerterp-Plantenga MS, Westerterp KR. Am J Clin Nutr. 2009 Sep; 90(3):519-26. https://www.ncbi.nlm.nih.gov/pubmed/19640952/[↩]
- Glycerol turnover and oxidation in man. Bortz WM, Paul P, Haff AC, Holmes WL. J Clin Invest. 1972 Jun; 51(6):1537-46. https://www.ncbi.nlm.nih.gov/pubmed/5024045/[↩]
- Paoli A. Ketogenic Diet for Obesity: Friend or Foe? International Journal of Environmental Research and Public Health. 2014;11(2):2092-2107. doi:10.3390/ijerph110202092. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945587/[↩][↩][↩]
- Pathways and control of ketone body metabolism: on the fringe of lipid biochemistry. Fukao T, Lopaschuk GD, Mitchell GA. Prostaglandins Leukot Essent Fatty Acids. 2004 Mar; 70(3):243-51. https://www.ncbi.nlm.nih.gov/pubmed/14769483/[↩][↩]
- Paoli A. Ketogenic Diet for Obesity: Friend or Foe? International Journal of Environmental Research and Public Health. 2014;11(2):2092-2107. doi:10.3390/ijerph110202092. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945587/ [↩]
- Role of beta-hydroxybutyric acid in the central regulation of energy balance. Laeger T, Metges CC, Kuhla B. Appetite. 2010 Jun; 54(3):450-5. https://www.ncbi.nlm.nih.gov/pubmed/20416348/[↩]
- The therapeutic implications of ketone bodies: the effects of ketone bodies in pathological conditions: ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. Veech RL. Prostaglandins Leukot Essent Fatty Acids. 2004 Mar; 70(3):309-19. https://www.ncbi.nlm.nih.gov/pubmed/14769489/[↩][↩]
- Diet-induced ketosis increases monocarboxylate transporter (MCT1) levels in rat brain. Leino RL, Gerhart DZ, Duelli R, Enerson BE, Drewes LR. Neurochem Int. 2001 May; 38(6):519-27. https://www.ncbi.nlm.nih.gov/pubmed/11248400/[↩]
- Fernstrom JD, Fernstrom MH. Nutrition and the brain. In: Gibney MJ, Macdonald IA, Roche HM, editor. Nutrition & Metabolism. Oxford, UK: Blackwell Science; 2003. pp. 145–167.[↩]
- Manninen AH. Metabolic Effects of the Very-Low-Carbohydrate Diets: Misunderstood “Villains” of Human Metabolism. Journal of the International Society of Sports Nutrition. 2004;1(2):7-11. doi:10.1186/1550-2783-1-2-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2129159/[↩][↩]
- Krebs HA. The regulation of the release of ketone bodies by the liver. Adv Enzyme Regul. 1966;4:339–354. https://www.ncbi.nlm.nih.gov/pubmed/4865971[↩]
- Paoli A, Canato M, Toniolo L, Bargossi AM, Neri M, Mediati M, et al. The ketogenic diet: an underappreciated therapeutic option. Clin Ter. 2011;162:e145–e153. https://www.ncbi.nlm.nih.gov/pubmed/22041813[↩]
- Cahill GF., Jr Fuel metabolism in starvation. Annu Rev Nutr. 2006;26:1–22. https://www.ncbi.nlm.nih.gov/pubmed/16848698[↩]
- Paoli A, Grimaldi K, Toniolo L, Canato M, Bianco A, Fratter A. Nutrition and acne: therapeutic potential of ketogenic diets. Skin Pharmacol Physiol. 2012;25:111–117. https://www.ncbi.nlm.nih.gov/pubmed/22327146[↩]
- Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Paoli A, Rubini A, Volek JS, Grimaldi KA. Eur J Clin Nutr. 2013 Aug; 67(8):789-96. https://www.ncbi.nlm.nih.gov/pubmed/23801097/[↩]
- Merck Sharp & Dohme Corp., Merck Manual. Diabetic Ketoacidosis (DKA). https://www.merckmanuals.com/professional/endocrine-and-metabolic-disorders/diabetes-mellitus-and-disorders-of-carbohydrate-metabolism/diabetic-ketoacidosis-dka[↩]
- Breath acetone is a reliable indicator of ketosis in adults consuming ketogenic meals. Musa-Veloso K, Likhodii SS, Cunnane SC. Am J Clin Nutr. 2002 Jul; 76(1):65-70. https://www.ncbi.nlm.nih.gov/pubmed/12081817/[↩]
- Breath acetone predicts plasma ketone bodies in children with epilepsy on a ketogenic diet. Musa-Veloso K, Likhodii SS, Rarama E, Benoit S, Liu YM, Chartrand D, Curtis R, Carmant L, Lortie A, Comeau FJ, Cunnane SC. Nutrition. 2006 Jan; 22(1):1-8. https://www.ncbi.nlm.nih.gov/pubmed/16183255/[↩]
- Breath ketone testing: a new biomarker for diagnosis and therapeutic monitoring of diabetic ketosis. Qiao Y, Gao Z, Liu Y, Cheng Y, Yu M, Zhao L, Duan Y, Liu Y. Biomed Res Int. 2014;2014:869186. https://www.ncbi.nlm.nih.gov/pubmed/24900994/[↩]
- Biomed Res Int. 2014;2014:869186. doi: 10.1155/2014/869186. Epub 2014 May 11. Breath ketone testing: a new biomarker for diagnosis and therapeutic monitoring of diabetic ketosis. https://www.ncbi.nlm.nih.gov/pubmed/24900994/[↩]
- Post-exercise ketosis and the hormone response to exercise: a review. Koeslag JH. Med Sci Sports Exerc. 1982; 14(5):327-34. https://www.ncbi.nlm.nih.gov/pubmed/6759842/[↩]
- Sasaki H, Ishikawa S, Ueda H, KIMURA Y. Response of acetone in expired Air during graded and prolonged exercise. Adv Exerc Sports Physiol. 2011;16:97–100.[↩]





{kind=link}