Contents
- What is a kidney function test
- Kidney function tests
- What happens if you have kidney disease
- Kidney
- How to test kidney function
- Urine Albumin and Albumin/Creatinine Ratio
- How is urine albumin/creatinine ratio test used?
- When is urine albumin/creatinine ratio ordered?
- What does abnormal urine albumin/creatinine ratio test result mean?
- What is the difference between serum/plasma albumin, prealbumin, and urine albumin tests?
- Is there anything I can do to prevent microalbuminuria?
- Are there other reasons for having increased urine albumin levels?
- Urine Albumin and Albumin/Creatinine Ratio
- What blood test for kidney function
- Blood Creatinine
- When is creatinine blood test ordered?
- What does a high creatinine blood test mean?
- What does a low creatinine blood test mean?
- What can I do to make my creatinine level normal?
- How does diet affect creatinine levels?
- What is creatine? If I take creatine, will my creatinine levels go up?
- Will exercise affect my creatinine levels?
- Do creatinine levels change with age?
- What is a BUN/Creatinine ratio?
- Besides measuring blood creatinine, are there other ways of estimating GFR?
- Urine creatinine test
- Creatinine clearance test
- Glomerular filtration rate
- How is estimated glomerular filtration rate used?
- When is estimated glomerular filtration rate ordered?
- How can actual glomerular filtration rate be determined?
- Could I calculate my own eGFR?
- What does abnormal glomerular filtration rate test result mean?
- Why might my healthcare provider repeat my eGFR test?
- What other findings might suggest kidney dysfunction?
- Why are factors such as age, sex, and race used in eGFR calculations?
- Blood Urea Nitrogen (BUN)
- When is blood urea nitrogen (BUN) ordered?
- What happens during a blood urea nitrogen (BUN) test?
- Will I need to do anything to prepare for the blood urea nitrogen (BUN) test?
- What do the blood urea nitrogen (BUN) results mean?
- What is a BUN/Creatinine ratio?
- What other tests are used with the blood urea nitrogen test to check how my kidneys are functioning?
- Cystatin C
- Blood Creatinine
- Kidney function test results
- What causes kidney failure
What is a kidney function test
You need to have kidney function test to check for your kidney’s health because you can’t feel kidney disease. Kidney tests are very important for people who have diabetes, high blood pressure, or heart disease. These conditions can hurt your kidneys. The routine blood and urine tests listed below may provide the first indication of a kidney problem or may be ordered if chronic kidney disease (CKD) is suspected due to a person’s signs and symptoms. These tests reflect how well the kidneys are removing excess fluids and wastes and some are included in the basic and comprehensive metabolic panels.
A blood pressure measurement is also important since high blood pressure (hypertension) can lead to chronic kidney disease (CKD). When a structural problem is suspected, a variety of imaging tests can be used to evaluate your kidneys. A sample of kidney tissue, a biopsy, is sometimes helpful in diagnosing the specific cause of a problem.
The National Kidney Foundation (https://www.kidney.org) and the National Kidney Disease Education Program (https://www.niddk.nih.gov/health-information/communication-programs/nkdep) recommend that people who are at high risk be screened for kidney disease to detect it in its earliest stages. Risk factors include diabetes, high blood pressure, heart disease, or a family history of these or kidney disease. The National Kidney Foundation (https://www.kidney.org) recommends that everyone with diabetes between the ages of 12 and 70 be screened for kidney disease at least once a year. At this time, there is no consensus on screening people who have no risk factors or symptoms. The National Kidney Foundation and National Kidney Disease Education Program recommend two tests, in addition to blood pressure measurement, to screen for kidney disease:
Two tests are used routinely to check for kidney disease:
- A blood test checks your GFR (glomerular filtration rate), which tells how well your kidneys are filtering.
- A urine test checks for albumin in your urine, a sign of kidney damage.
GFR (glomerular filtration rate) is the best test to measure your level of kidney function and determine your stage of kidney disease. Your doctor can calculate it from the results of your blood creatinine test, your age, body size and gender. Your GFR tells your doctor your stage of kidney disease and helps the doctor plan your treatment. If your GFR number is low, your kidneys are not working as well as they should. The earlier kidney disease is detected, the better the chance of slowing or stopping its progression. The normal level of glomerular filtration rate (GFR) varies according to age, sex, and body size. Normal glomerular filtration rate (GFR) in young adults is approximately 120 to 130 mL/min per 1.73 m² and declines with age 1.
Blood tests for kidney disease
The best measure of kidney function is the glomerular filtration rate (GFR), which can be estimated from a blood test that checks the blood for creatinine (a waste product made by muscle tissue). A normal result is higher than 90 mL/min/1.73 m². If the result is persistently less than 60 mL/min/1.73 m² for at least three months, this confirms that the person has chronic kidney disease.
Blood tests can reveal other abnormalities of kidney function, such as:
- high levels of acids (acidosis)
- anemia (insufficient red blood cells or hemoglobin, the protein in red blood cells that transports oxygen)
- high levels of potassium (hyperkalemia)
- low levels of salt (hyponatremia)
- changes to the levels of calcium and phosphate.
Urine tests for kidney disease
Albumin is a major protein normally present in your blood. A healthy kidney does not let albumin pass into the urine. A damaged kidney lets some albumin pass into the urine. The less albumin in your urine, the better. Normal urine protein elimination is less than 150 mg/day and less than 30 mg of albumin/day. A small amount of albumin in the urine is sometimes referred to as urine microalbumin or microalbuminuria. “Microalbuminuria” is slowly being replaced with the term “albuminuria,” which refers to any elevation of albumin in the urine. Elevated urine microalbumin levels may be seen temporarily with conditions such as infections, stress, pregnancy, diet, cold exposure, or heavy exercise. Persistent protein in the urine (microalbuminuria) suggests possible kidney damage or some other condition that requires additional testing to determine the cause.
Damaged or inflamed kidneys ‘leak’ substances such as blood or protein into the urine. The preferred test for detecting protein in the urine is a urine albumin-to-creatinine ratio (urine ACR) test, which shows the amount of albumin (a type of protein) in the urine.
A urine albumin-to-creatinine ratio (urine ACR) test should be done at least once a year if the person has diabetes or high blood pressure, and every two years if the person has any of the other identified risk factors for developing chronic kidney disease.
A urine albumin-to-creatinine ratio (urine ACR) test is performed by sending a sample of your urine to a laboratory for analysis.
Studies have shown that elevated levels of urinary albumin in people with diabetes or hypertension are associated with increased risk of developing cardiovascular disease. More recently, research has been focused on trying to determine if increased levels of albumin in the urine are also indicative of cardiovascular disease risk in those who do not have diabetes or high blood pressure.
How is the urine sample collected for testing?
A random sample of urine, a timed urine sample (such as 4 hours or overnight), or a complete 24-hour urine sample is collected in a clean container. The health practitioner or laboratory will provide a container and instructions for properly collecting the sample that is needed.
Kidney function tests
- Urine protein—a few different tests may be used to screen for protein in the urine:
- Urine total protein or urine protein to creatinine ratio (UP/CR)—detects not just albumin, but all types of proteins that may be present in the urine.
- Urinalysis—this is a routine test that can detect protein in the urine as well as red blood cells and white blood cells. These are not normally found in the urine and, if present, may indicate kidney disease.
- Urine albumin—this test may be done on a 24-hour urine sample, or both urine albumin and creatinine can be measured in a random urine sample and the albumin/creatinine ratio (ACR) can be calculated. The American Diabetes Association recommends albumin/creatinine ratio (ACR) as the preferred test for screening for albumin in the urine (microalbuminuria).
While urinalysis and urine total protein are not as sensitive as urine albumin for detecting kidney damage, these tests give fewer false signals of kidney damage.
- Estimated glomerular filtration rate (eGFR)—a blood creatinine test or possibly a cystatin C test is performed in order to calculate the eGFR. The glomerular filtration rate refers to the amount of blood that is filtered by the glomeruli per minute. As a person’s kidney function declines due to damage or disease, the filtration rate decreases and waste products begin to accumulate in the blood.
Some additional tests that may be ordered to evaluate for kidney disease include:
- Urea (urea nitrogen or BUN)—the level of this waste product in the blood increases as kidney filtration declines. Increased BUN levels suggest impaired kidney function, although they can also be elevated due to a condition that results in decreased blood flow to the kidneys, such as congestive hear failure, heart attack, or shock.
- Creatinine clearance—this test measures creatinine levels in both a sample of blood and a sample of urine from a 24-hour urine collection. The results are used to calculate the amount of creatinine that has been cleared from the blood and passed into the urine. This calculation allows for a general evaluation of the amount of blood that is being filtered by the kidneys in a 24-hour time period.
Tests to monitor kidney function
If a person has been diagnosed with a kidney disease, several laboratory tests may be ordered to help monitor kidney function. Some of these include:
- Blood levels of urea nitrogen (BUN) and creatinine are measured from time to time to see if the kidney disease is getting worse.
- The amount of calcium and phosphorus in the blood, blood gases (ABGs), and the balance of serum and urine electrolytes can also be measured as these are often affected by kidney disease.
- Hemoglobin in the blood, measured as part of a complete blood count (CBC), may also be evaluated as the kidneys make a hormone, erythropoietin, that controls red blood cell production and this may be affected by kidney damage.
- Erythropoietin may be measured directly, although this is not a routine test.
- Parathyroid hormone (PTH), which controls calcium levels, is often increased in kidney disease and may be checked to help determine if enough calcium and vitamin D are being taken to prevent bone damage.
- Cystatin C is another test that may sometimes be used as an alternative to creatinine to screen for and monitor kidney dysfunction in those with known or suspected kidney diseases.
- Both blood and urine beta 2 microglobulin (B2M) tests may be ordered along with other kidney function tests to evaluate kidney damage and disease and to distinguish between disorders that affect the glomeruli and the renal tubules. Normally, only small amounts of B2M are present in the urine, but when the renal tubules become damaged or diseased, B2M concentrations increase due to the decreased ability to reabsorb this protein. When the glomeruli in the kidneys are damaged, they are unable to filter out B2M, so the level in the blood rises. B2M tests may sometimes be ordered to monitor people who have had a kidney transplant, to detect early signs of rejection, and ordered to monitor people who are exposed to high levels of cadmium and mercury, such as with occupational exposure.
Tests to help determine the cause and/or guide treatment
Other tests may be ordered to help determine the cause and/or guide treatment, depending on several factors including a person’s signs and symptoms, physical examination, and medical history. Some examples of these tests include:
- Urinalysis with a urine culture may be done when someone has symptoms suggesting infection to confirm the presence of a bacterial infection.
- Hepatitis B or C testing—to detect a hepatitis viral infection associated with some types of kidney disease
- Antinuclear antibody (ANA)—to help identify an autoimmune condition such as lupus that may be affecting the kidneys.
- Kidney stone risk panel—this test evaluates a person’s risk of developing a kidney stone, to help guide and monitor treatment and prevention
- Kidney stone analysis—this test determines the composition of a kidney stone passed or removed from the urinary tract and may be done to help determine the cause of its formation, to guide treatment, and prevent recurrence
- Complement tests, most commonly C3 and C4—may be tested and monitored with glomerulonephritis
- Urine protein electrophoresis—may be done to determine the source of a high level of protein in the urine
- Myoglobin—in people who have had extensive damage to their skeletal muscles (rhabdomyolysis), a urine myoglobin test may be ordered to determine the risk of kidney damage. With severe muscle injury, blood and urine levels of myoglobin can rise very quickly.
Imaging techniques
If a structural problem or blockage is suspected, imaging of the kidneys can be helpful. Imaging techniques such as an ultrasound, CT scan (computed tomography), isotope scan, or intravenous pyelogram (IVP) may be used.
Kidney biopsy
A biopsy is sometimes used to help determine the nature and extent of structural damage to a kidney. Analyzing a small piece of kidney tissue, obtained using a biopsy needle and diagnostic imaging equipment, can sometimes be useful when disease of the glomeruli (or sometimes the tubules) is suspected.
Tests for biomarkers of acute kidney injury
Several biomarkers are gaining attention as early indicators of acute kidney injury (AKI). Studies suggest that blood or urine tests for these biomarkers can detect acute kidney damage earlier than currently used kidney function tests, such as serum creatinine. Early detection of acute kidney injury is critical because injury occurs rapidly over a period of hours to days. Acute kidney injury (AKI) biomarkers are still being studied and may become more widely available in the future.
Although acute kidney injury is a serious condition and costs the U.S. healthcare system millions of dollars each year, the measurement of acute kidney injury biomarkers does not directly help in treating people with acute kidney injury because there are no FDA-approved therapies currently available. When acute kidney injury is diagnosed, imaging scans of the kidneys are frequently performed to rule out the presence of an obstruction in the urinary tract. General supportive treatment may be given, such as IV fluids or transfusion of blood components. Drugs used to improve blood pressure and heart function may be used if a person is in shock. If a person does not recover from acute kidney injury spontaneously, some type of dialysis is required.
Examples of promising acute kidney injury biomarkers include:
- Urinary insulin-like growth factor-binding protein 7 (IGFBP7) and urinary tissue inhibitor of metalloproteinases-2 (TIMP-2)—these two markers have been combined into a point-of-care test. It is the first test approved by the U.S. Food and Drug Administration to help assess critically ill patients for risk of developing acute kidney injury within the next 12 hours.
- Neutrophil gelatinase-associated lipocalin (NGAL)—this is a protein that is found in many tissues in the body, including kidney cells. Part of the reason NGAL is a good indicator of acute kidney injury is that its level rises rapidly in response to kidney injury, typically within 2-4 hours.
What happens if you have kidney disease
Kidney disease can be treated. The sooner you know you have kidney disease, the sooner you can get treatment to help delay or prevent kidney failure. Treating kidney disease may also help prevent heart disease.
Treatment goals are to:
- Keep your GFR from going down
- Lower your urine albumin
No matter what your results are:
- Keep your blood pressure, blood glucose and blood cholesterol in your target range.
- Choose foods that are healthy for your heart and cut back on salt.
- Be more physically active.
- If you smoke, take steps to quit.
- Take medicines the way your provider tells you to.
Kidney
The paired kidneys are reddish, kidney bean–shaped organs located just above the waist between the peritoneum and the posterior wall of the abdomen. Because their position is posterior to the peritoneum of the abdominal cavity, the organs are said to be retroperitoneal (Figure 1). The kidneys are located between the levels of the last thoracic vertebrae T12 and third lumbar (L3) vertebrae, a position where they are partially protected by ribs 11 and 12. If these lower ribs are fractured, they can puncture the kidneys and cause significant, even life-threatening damage. The right kidney is slightly lower than the left (see Figure 1) because the liver occupies considerable space on the right side superior to the kidney.
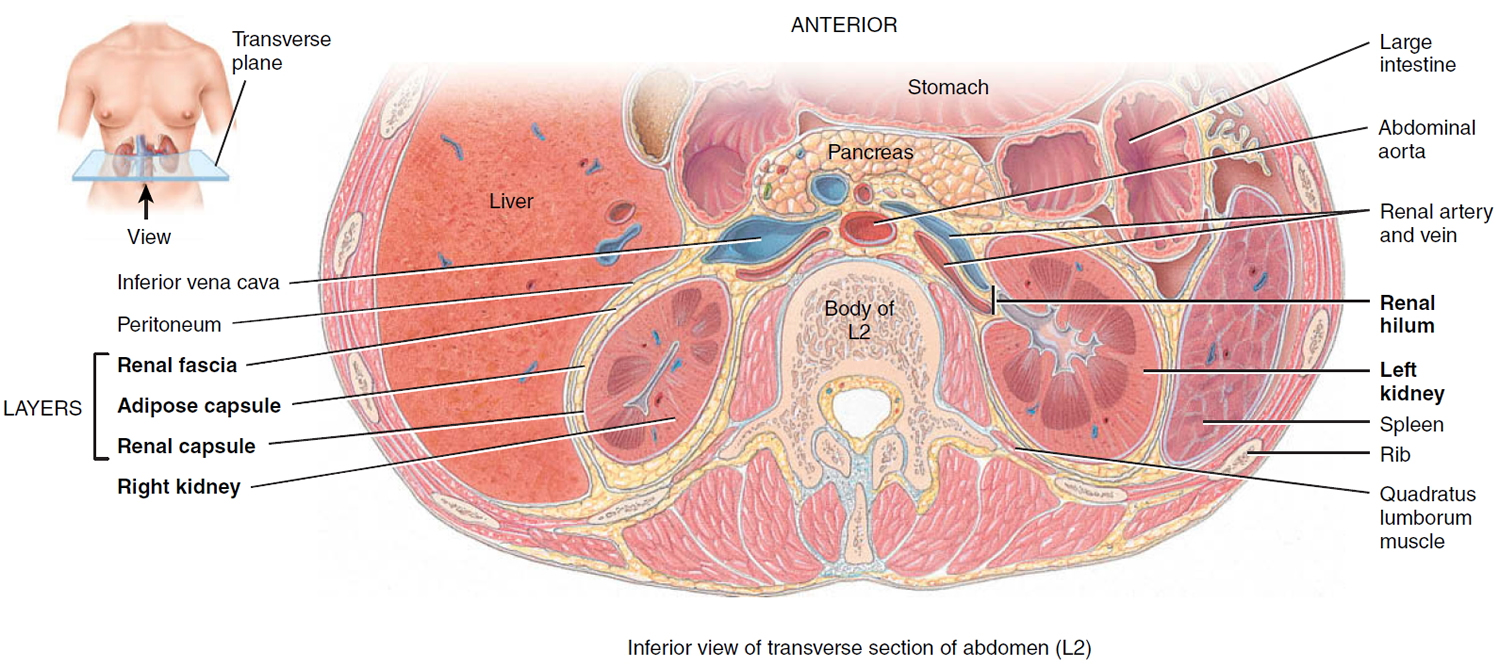
A typical adult kidney is 10–12 cm (4–5 in.) long, 5–7 cm (2–3 in.) wide, and 3 cm (1 in.) thick—about the size of a bar of bath soap—and weighs about 135–150 g (4.5–5 oz). The concave medial border of each kidney faces the vertebral column (see Figure 2). Near the center of the concave border is an indentation called the renal hilum, through which the ureter emerges from the kidney along with blood vessels, lymphatic vessels, and nerves.
Three layers of tissue surround each kidney. The deep layer, the renal capsule, is a smooth, transparent sheet of dense irregular connective tissue that is continuous with the outer coat of the ureter. It serves as a barrier against trauma and helps maintain the shape of the kidney. The middle layer, the adipose capsule, is a mass of fatty tissue surrounding the renal capsule. It also protects the kidney from trauma and holds it firmly in place within the abdominal cavity. The superficial layer, the renal fascia, is another thin layer of dense irregular connective tissue that anchors the kidney to the surrounding structures and to the abdominal wall. On the anterior surface of the kidneys, the renal fascia is deep to the peritoneum.
Figure 1. Kidney location
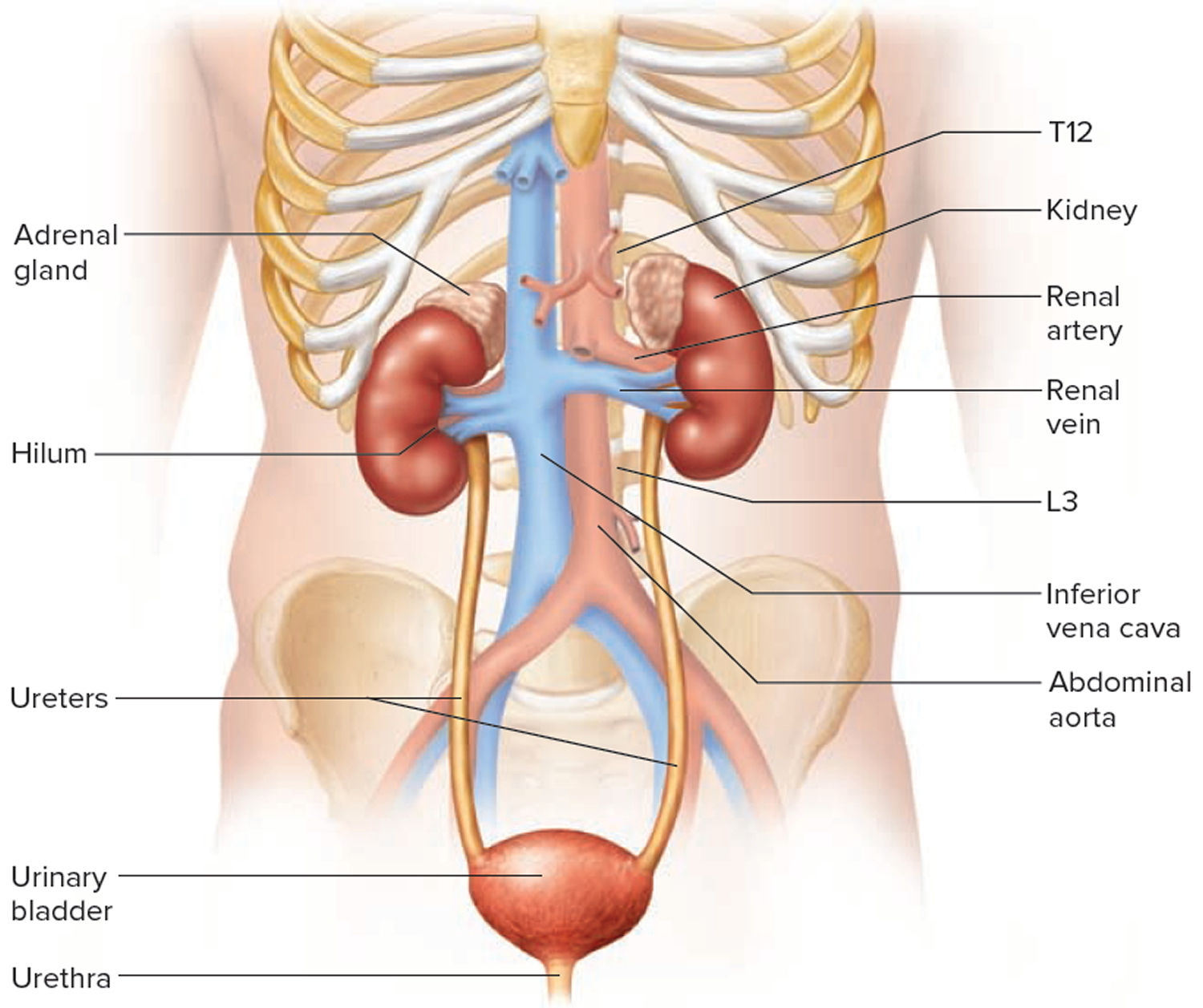
Figure 2. Kidney location (transverse section)
Kidney Anatomy
A frontal section through the kidney reveals two distinct regions: a superficial, light red region called the renal cortex and a deep, darker reddish-brown inner region called the renal medulla (medulla = inner portion) (Figure 3). The renal medulla consists of several cone-shaped renal pyramids. The base (wider end) of each pyramid faces the renal cortex, and its apex (narrower end), called a renal papilla, points toward the renal hilum. The renal cortex is the smooth-textured area extending from the renal capsule to the bases of the renal pyramids and into the spaces between them. It is divided into an outer cortical zone and an inner juxtamedullary zone. Those portions of the renal cortex that extend between renal pyramids are called renal columns.
Together, the renal cortex and renal pyramids of the renal medulla constitute the parenchyma or functional portion of the kidney. Within the parenchyma are the functional units of the kidney—about 1 million microscopic structures called nephrons. Filtrate (filtered fluid) formed by the nephrons drains into large papillary ducts, which extend through the renal papillae of the pyramids. The papillary ducts drain into cuplike structures called minor and major calyces. Each kidney has 8 to 18 minor calyces and 2 or 3 major calyces. A minor calyx receives filtrate from the papillary ducts of one renal papilla and delivers it to a major calyx. Once the filtrate enters the calyces it becomes urine because no further reabsorption can occur. The reason for this is that the simple epithelium of the nephron and ducts becomes transitional epithelium in the calyces. From the major calyces, urine drains into a single large cavity called the renal pelvis and then out through the ureter to the urinary bladder.
The hilum expands into a cavity within the kidney called the renal sinus, which contains part of the renal pelvis, the calyces, and branches of the renal blood vessels and nerves. Adipose tissue helps stabilize the position of these structures in the renal sinus.
Figure 3. Kidney anatomy
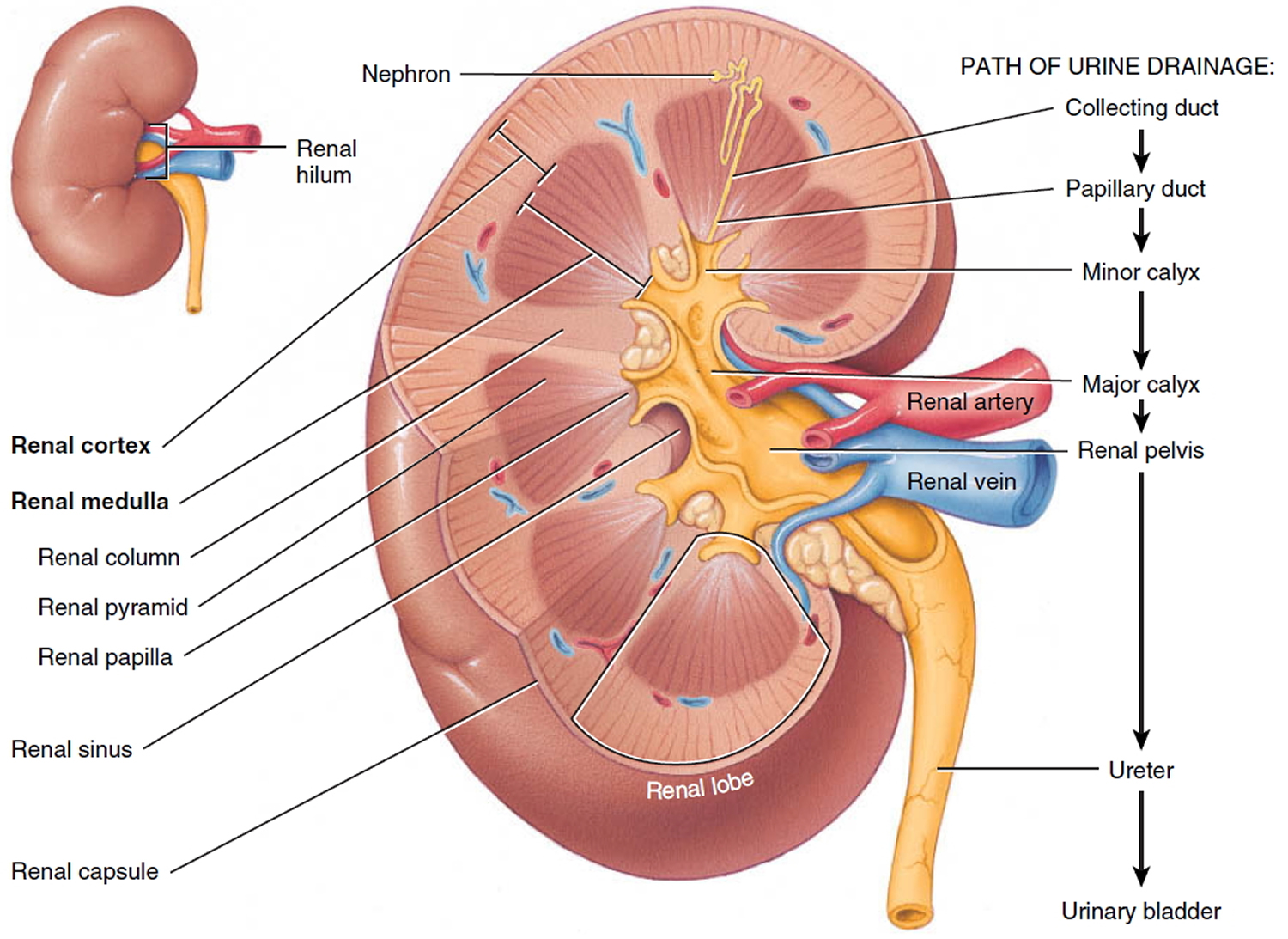
Figure 4. Kidney structure
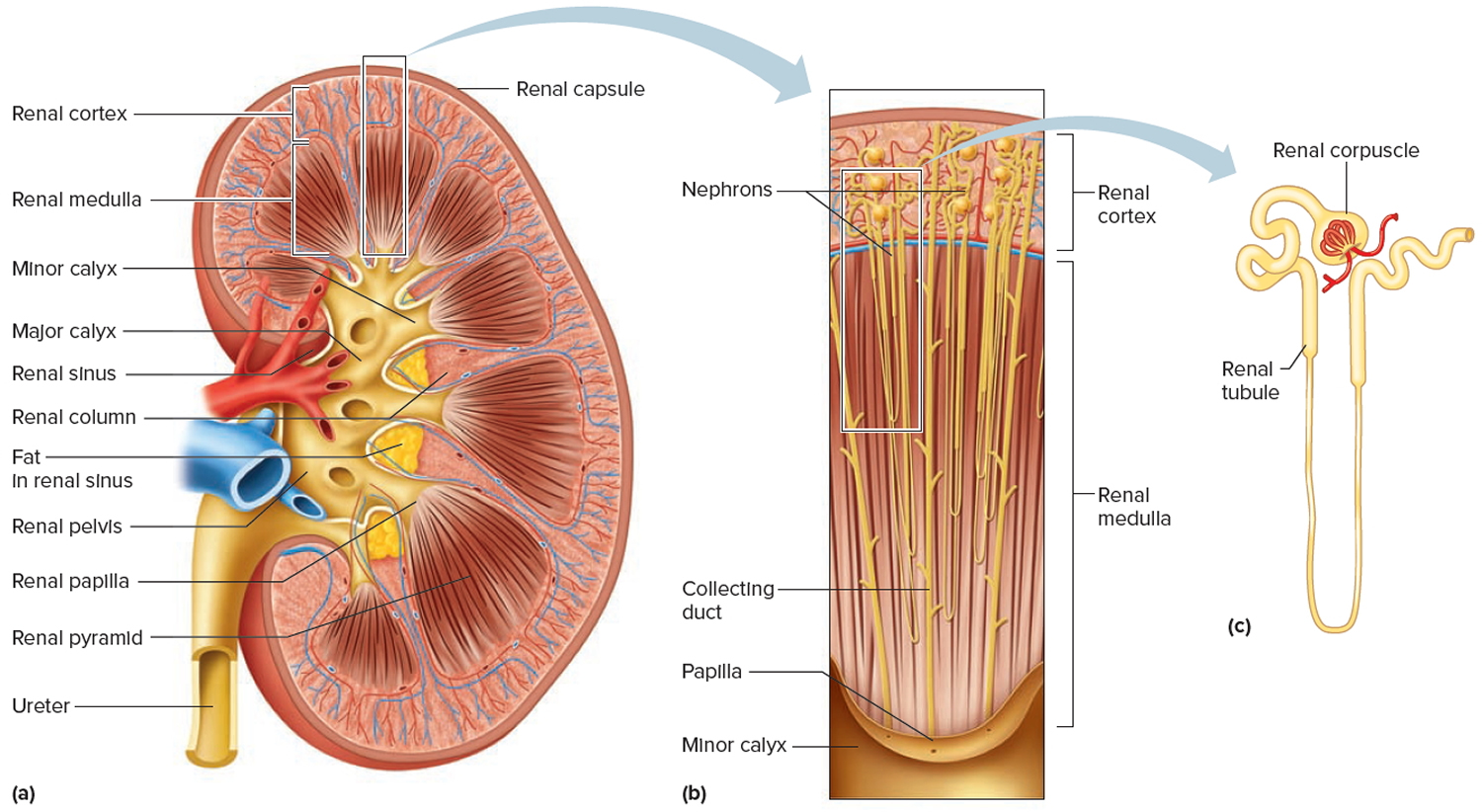
Figure 5. Microcirculation of the kidney
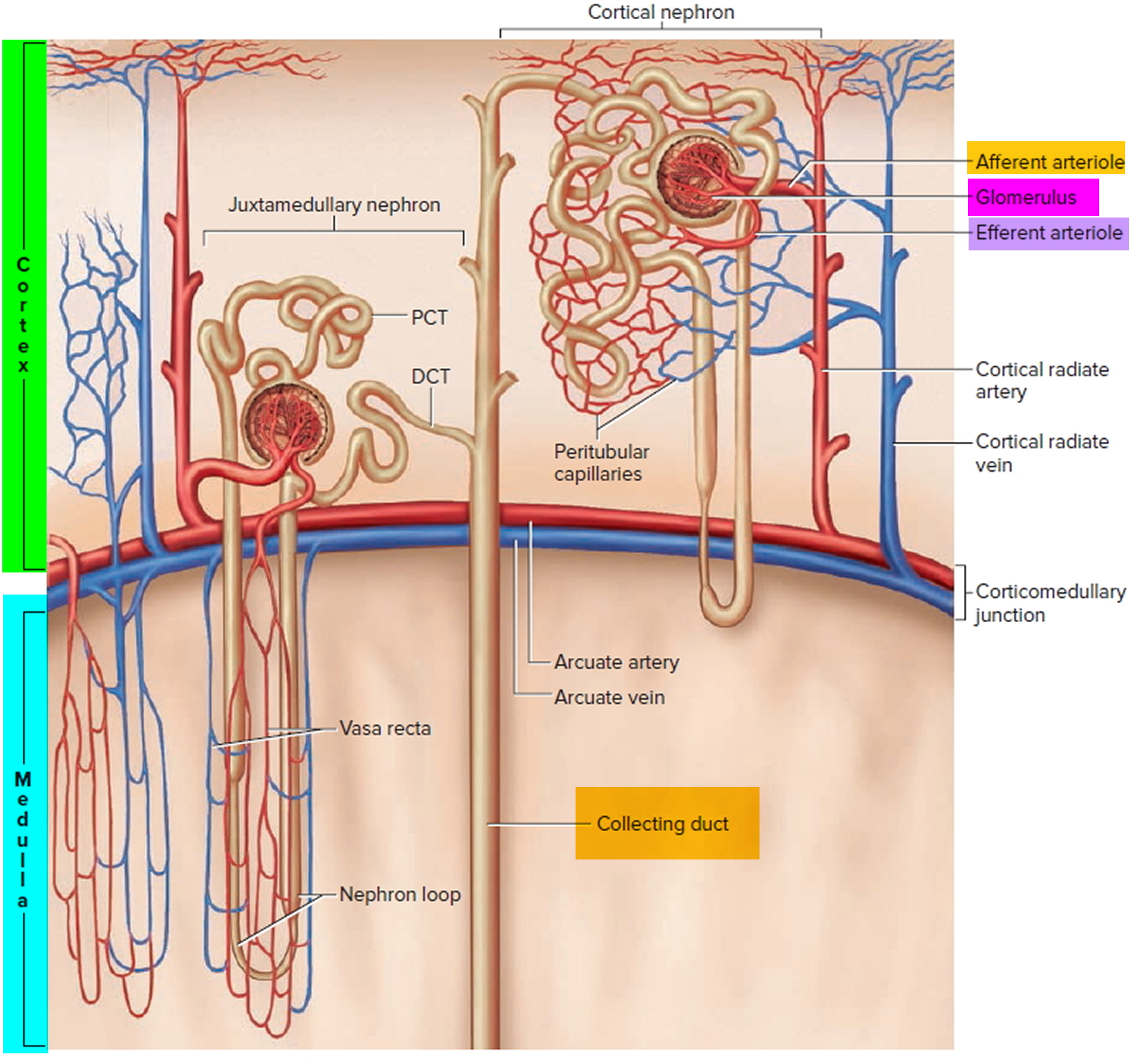
Note: DCT = distal convoluted tubule; PCT = proximal convoluted tubule
Kidney Function
The primary function of the kidneys is to help maintain homeostasis by regulating the composition (including pH) and the volume of the extracellular fluid. The kidneys accomplish this by removing metabolic wastes from the blood and combining the wastes with excess water and electrolytes to form urine, which they then excrete.
Kidneys maintain homeostasis
- Regulatory function
+ Control composition and volume of blood
+ Maintain stable concentrations of inorganic anions such as sodium (Na), potassium (K), and calcium (Ca)
+ Maintain acid-base balance - Excretory function
+ Produce urine
+ Remove metabolic wastes
+ Including nitrogenous waste
Kidneys blood filtration and urine production
- Filtration: Glomeruli generate ultrafiltrate of the plasma.
- Reabsorption: Tubules selectively reabsorb substances from the ultrafiltrate.
- Secretion: Tubules secrete substances into the urine.
Examples:
- Potassium is reabsorbed from and secreted into the urine by the tubules.
- Sodium is generally reabsorbed by the tubules.
- Organic acids are secreted into the urine.
- Albumin is generally reabsorbed within the tubules.
Damaged kidneys allow albumin to cross the filtration barrier into the urine
- Increased glomerular permeability allows albumin (and other proteins) to cross the glomerulus into the urine.
- Higher levels of protein within the tubule may exacerbate kidney damage by exceeding tubules’ ability to reabsorb the proteins.
- An elevated urine albumin-to-creatinine ratio (UACR) is used to identify damaged kidneys. Urine albumin (UACR) results are used for screening, diagnosing, and treating chronic kidney disease. Forty percent of people are identified with chronic kidney disease on the basis of urine albumin alone.
The kidneys have several other important functions:
- Produce Erythropoietin which stimulates marrow production of red blood cells.
- Playing a role in the activation of vitamin D [activate 25(OH)D to 1,25 (OH)2D (active vitamin D)].
- Helping to maintain blood volume and blood pressure by secreting the enzyme Renin.
- Metabolize drugs and endogenous substances (e.g., insulin).
In patients with kidney failure:
- Kidneys cannot maintain homeostasis.
- Kidney failure is associated with fluid, electrolyte, and hormonal imbalances and metabolic abnormalities.
- End stage kidney failure means the patient is on dialysis or has a kidney transplant.
Ultrafiltration of plasma is the main function of the glomeruli
Filtration is based on size and charge.
- Small solutes cross readily.
- Larger substances are generally restricted.
- Negatively charged molecules are restricted.
Volume of ultrafiltrate = 135–180 liters(L)/day
- 99% water reabsorbed 1–1.5 L urine excreted
- Glomerular filtration rate (GFR) provides an estimate of how much blood is filtered by the kidneys each minute. In normal kidneys are GFR > 60 ml/minute
- The formula used to estimate GFR uses serum creatinine, age, gender, and race.
- eGFR (mL/min/1.73 m2) = 175 x (serum creatinine)–1.154 x (Age)–0.203 x (0.742 if female) x (1.212 if African American)
- Kidney failure is an eGFR < 15 ml/minute.
- eGFR is not reliable for patients with rapidly changing creatinine levels, extremes in muscle mass and body size, or altered diet patterns.
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/communication-programs/nkdep/laboratory-evaluation/glomerular-filtration-rate-calculators
Table 1. Reference Table for Population Mean eGFR from NHANES III
Age (years) | Mean eGFR (mL/min/1.73 m²) |
20–29 | 116 |
30–39 | 107 |
40–49 | 99 |
50–59 | 93 |
60–69 | 85 |
70 | 75 |
How to test kidney function
Urine Albumin and Albumin/Creatinine Ratio
Urine Albumin and Albumin/Creatinine Ratio test is also known as microalbumin, ACR or UACR.
Albumin is a major protein normally present in your blood. A healthy kidney does not let albumin pass into the urine. A damaged kidney lets some albumin pass into the urine. The less albumin in your urine, the better. Normal urine protein elimination is less than 150 mg/day and less than 30 mg of albumin/day. Elevated levels may be seen temporarily with conditions such as infections, stress, pregnancy, diet, cold exposure, or heavy exercise. Persistent protein in the urine suggests possible kidney damage or some other condition that requires additional testing to determine the cause.
The urine albumin test detects and measures the amount of albumin in the urine. The presence of a small amount of albumin in the urine may be an early indicator of kidney disease. A small amount of albumin in the urine is sometimes referred to as urine microalbumin or microalbuminuria. “Microalbuminuria” is slowly being replaced with the term “albuminuria,” which refers to any elevation of albumin in the urine.
Plasma, the liquid portion of blood, contains many different proteins, including albumin. One of the many functions of the kidneys is to conserve plasma proteins so that they are not released along with waste products when urine is produced. There are two mechanisms that normally prevent protein from passing into urine: (1) the glomeruli provide a barrier that keeps most large plasma proteins inside the blood vessels and (2) the smaller proteins that do get through are almost entirely reabsorbed by the tubules.
Protein in the urine (proteinuria) most often occurs when either the glomeruli or tubules in the kidney are damaged. Inflammation and/or scarring of the glomeruli can allow increasing amounts of protein to leak into the urine. Damage to the tubules can prevent protein from being reabsorbed.
Albumin is a plasma protein that is present in high concentrations in the blood, and when the kidneys are functioning properly, virtually no albumin is present in the urine. If a person’s kidneys become damaged or diseased, however, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension, with increasing amounts of protein in the urine reflecting increasing kidney dysfunction.
Albumin is one of the first proteins to be detected in the urine with kidney damage. People who have consistently detectable small amounts of albumin in their urine (albuminuria) have an increased risk of developing progressive kidney failure and cardiovascular disease in the future.
A urine albumin test is used to screen for kidney disease in people with chronic conditions such as diabetes and high blood pressure. It can detect small amounts of albumin that escape from the blood through the kidneys into the urine several years before significant kidney damage becomes apparent. Most of the time, tests for albumin and creatinine are done on a urine sample collected randomly (not timed) and an albumin-to-creatinine ratio is calculated. This is done to provide a more accurate indication of the how much albumin is being released into the urine.
How is the urine sample collected for testing?
A random sample of urine, a timed urine sample (such as 4 hours or overnight), or a complete 24-hour urine sample is collected in a clean container. The health practitioner or laboratory will provide a container and instructions for properly collecting the sample that is needed.
How is urine albumin/creatinine ratio test used?
The urine albumin test or albumin/creatinine ratio (ACR) is used to screen people with chronic conditions, such as diabetes and high blood pressure (hypertension) that put them at an increased risk of developing kidney disease. Studies have shown that identifying individuals in the very early stages of kidney disease helps people and healthcare providers adjust treatment. Controlling diabetes and hypertension by maintaining tight glycemic control and reducing blood pressure delay or prevent the progression of kidney disease.
Albumin is a protein that is present in high concentrations in the blood. Virtually no albumin is present in the urine when the kidneys are functioning properly. However, albumin may be detected in the urine even in the early stages of kidney disease.
If albumin is detected in a urine sample collected at random, over 4 hours, or overnight, the test may be repeated and/or confirmed with urine that is collected over a 24-hour period (24-hour urine).
Most of the time, both albumin and creatinine are measured in a random urine sample and an albumin/creatinine ratio (ACR) is calculated. This may be done to more accurately determine how much albumin is escaping from the kidneys into the urine. The concentration (or dilution) of urine varies throughout the day with more or less liquid being released in addition to the body’s waste products. Thus, the concentration of albumin in the urine may also vary.
Creatinine, a byproduct of muscle metabolism, is normally released into the urine at a constant rate and its level in the urine is an indication of the urine concentration. This property of creatinine allows its measurement to be used to correct for urine concentration in a random urine sample. The American Diabetes Association has stated a preference for the albumin/creatinine ratio (ACR) for screening for albuminuria indicating early kidney disease. Since the amount of albumin in the urine can vary considerably, an elevated albumin/creatinine ratio (ACR) should be repeated twice within 3 to 6 months to confirm the diagnosis.
Studies have shown that elevated levels of urinary albumin in people with diabetes or hypertension are associated with increased risk of developing cardiovascular disease. More recently, research has been focused on trying to determine if increased levels of albumin in the urine are also indicative of cardiovascular disease risk in those who do not have diabetes or high blood pressure.
When is urine albumin/creatinine ratio ordered?
According to the American Diabetes Association and National Kidney Foundation, everyone with type 1 diabetes should get tested annually, starting 5 years after onset of the disease, and all those with type 2 diabetes should get tested annually, starting at the time of diagnosis. If albumin in the urine (albuminuria) is detected, it should be confirmed by retesting twice within a 3 to 6 month period. People with hypertension may be tested at regular intervals, with the frequency determined by their healthcare provider.
What does abnormal urine albumin/creatinine ratio test result mean?
Moderately increased albumin levels found in both initial and repeat urine tests indicate that a person is likely to have early kidney disease. Very high levels are an indication that kidney disease is present in a more severe form. Undetectable levels are an indication that kidney function is normal.
The presence of blood in the urine, a urinary tract infection, vigorous exercise, and other acute illnesses may cause a positive test result that is not related to kidney disease. Testing should be repeated after these conditions have resolved.
What is the difference between serum/plasma albumin, prealbumin, and urine albumin tests?
Although the names are similar, albumin and prealbumin are completely different molecules. They are both proteins made by the liver, however, and both have been used historically to evaluate nutritional status. Serum/plasma (or blood) albumin is now more often used to screen for and help diagnose liver or kidney disease and is tested on a blood sample. The urine albumin test (also called a microalbumin test) detects and measures albumin in the urine as an early indicator of kidney damage.
Is there anything I can do to prevent microalbuminuria?
Yes, if you are diabetic, follow your healthcare provider’s instructions for maintaining tight control over your blood glucose level. Keeping high blood pressure under control is also effective in preventing kidney damage that leads to microalbuminuria. Some studies have shown that those who have albuminuria can prevent it from worsening or may reverse it with good glycemic and blood pressure control, or by quitting smoking.
Are there other reasons for having increased urine albumin levels?
Yes, albuminuria is not specific for diabetes. It may also be associated with hypertension (high blood pressure), some lipid abnormalities, and several immune disorders. Elevated results may also be caused by vigorous exercise, blood in the urine, urinary tract infection, dehydration, and some drugs.
What blood test for kidney function
Blood Creatinine
Creatinine is a waste product produced by muscles from the breakdown of a compound called creatine. Creatinine is removed from the body by the kidneys, which filter almost all of it from the blood and release it into the urine, so blood levels are usually a good indicator of how well the kidneys are working. Blood creatinine test measures the amount of creatinine in the blood and/or urine.
Creatine is part of the cycle that produces energy needed to contract muscles. Both creatine and creatinine are produced by the body at a relatively constant rate. Since almost all creatinine is filtered from the blood by the kidneys and released into the urine, blood levels are usually a good indicator of how well the kidneys are working. The quantity produced depends on the size of the person and their muscle mass. For this reason, creatinine concentrations will be slightly higher in men than in women and children.
A normal blood creatinine result is 0.7 to 1.3 mg/dL (61.9 to 114.9 µmol/L) for men and 0.6 to 1.1 mg/dL (53 to 97.2 µmol/L) for women.
Women usually have a lower creatinine level than men. This is because women usually have less muscle mass than men. Creatinine level varies based on a person’s size and muscle mass.
The examples above are common measurements for results of creatinine tests. Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor about the meaning of your specific test results.
Results from a blood creatinine test may be used in combination with results from other tests, such as a 24-hour urine creatinine test, to perform calculations that are used to evaluate kidney function.
A blood sample is drawn from a vein in the arm. A 24-hour urine sample may also be collected, in which all urine produced during 24 hours is saved. Sometimes a single, random urine sample may be collected and tested.
When is creatinine blood test ordered?
Creatinine may be ordered routinely as part of a comprehensive or basic metabolic panel during a health examination. It may be ordered when someone is acutely ill and/or when a health practitioner suspects that a person’s kidneys are not working properly. Some signs and symptoms of kidney dysfunction include:
- Fatigue, lack of concentration, poor appetite, or trouble sleeping
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure
The creatinine blood test may be ordered, along with a BUN (blood urea nitrogen) test and urine albumin, at regular intervals when someone has a known kidney disorder or has a disease that may affect kidney function. Both blood urea nitrogen (BUN) and creatinine may be ordered when a CT scan is planned, prior to and during certain drug therapies, and before and after dialysis to monitor the effectiveness of treatments.
How is creatinine blood test used?
The creatinine blood test is used to assess kidney function. It is frequently ordered along with a BUN (blood urea nitrogen) test or as part of a basic or comprehensive metabolic panel, groups of tests that are performed to evaluate the function of the body’s major organs. Basic or comprehensive metabolic panel tests are used to screen healthy people during routine physical exams and to help evaluate acutely or chronically ill people in the emergency room and/or hospital. Sometimes, creatinine may be performed as part of a renal panel to evaluate kidney function.
If the creatinine and blood urea nitrogen (BUN) tests are found to be abnormal or if someone has an underlying disease that is known to affect the kidneys, such as diabetes or high blood pressure, then creatinine and blood urea nitrogen (BUN) tests may be used to monitor for kidney dysfunction and the effectiveness of treatment. Blood creatinine and blood urea nitrogen (BUN) tests may also be ordered to evaluate kidney function prior to some procedures, such as a CT (computed tomography) scan, that may require the use of drugs that can damage the kidneys.
Results from creatinine tests may be used in calculations that help assess kidney function:
- Blood creatinine measurements, along with age, weight, and sex, are used to calculate the estimated glomerular filtration rate (eGFR), which is used as a screening test to look for evidence of early kidney damage.
- Blood and urine creatinine levels may be used to calculate a creatinine clearance. This test measures how effectively the kidneys are filtering small molecules like creatinine out of the blood.
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/communication-programs/nkdep/laboratory-evaluation/glomerular-filtration-rate-calculators
Urine creatinine may also be used with a variety of other urine tests as a correction factor. The concentration (or dilution) of urine varies throughout the day, with more or less liquid being released in addition to the body’s waste products. Since creatinine is produced and removed at a relatively constant rate, the amount of urine creatinine can be compared to the amount of another substance being measured. This stable excretion rate is useful when evaluating both 24-hour urine samples and random urine samples. Examples include:
- Urine albumin/creatinine ratio (ACR). This more accurately determines how much albumin is escaping from the kidneys into the urine. It is used to screen people with chronic conditions, such as diabetes and high blood pressure (hypertension) that put them at an increased risk of developing kidney disease.
- Urine protein/creatinine ratio (UP/CR). This may be used to monitor a person with known kidney disease or damage or to screen people on a regular basis when they are taking a medication that may affect their kidney function.
Is any test preparation needed to ensure the quality of the sample?
You may be instructed to fast overnight or refrain from eating cooked meat; some studies have shown that eating cooked meat prior to testing can temporarily increase the level of creatinine. If a 24-hour urine sample is being collected, it is important to save all of the urine produced during that time period.
The health care provider may also tell you to temporarily stop taking certain medicines that can affect the test. These medicines include:
- Cimetidine, famotidine, and ranitidine
- Certain antibiotics, such as trimethoprim
Tell your provider about all the medicines you take.
What does a high creatinine blood test mean?
Increased creatinine levels in the blood suggest kidney disease or other conditions that affect kidney function. These can include:
- Damage to or swelling of blood vessels in the kidneys (glomerulonephritis) caused by, for example, infection or autoimmune diseases
- Bacterial infection of the kidneys (pyelonephritis)
- Death of cells in the kidneys’ small tubes (acute tubular necrosis) caused by, for example, drugs or toxins
- Prostate disease, kidney stone, or other causes of urinary tract obstruction
- Reduced blood flow to the kidney due to shock, dehydration, congestive heart failure, atherosclerosis, or complications of diabetes
Creatinine blood levels can also increase temporarily as a result of muscle injury and are generally slightly lower during pregnancy.
Some drugs may cause increased creatinine levels. Inform your healthcare provider of any drugs you are taking.
Note: Blood creatinine levels are evaluated with 24-hour urine creatinine levels as part of a creatinine clearance test.
Single, random urine creatinine levels have no standard reference ranges. They are usually used with other tests to reference levels of other substances measured in the urine. Some examples include the urine albumin test and urine albumin/creatinine ratio and the urine protein test.
What does a low creatinine blood test mean?
Low blood levels of creatinine are not common, but they are also not usually a cause for concern. They can be seen with conditions that result in decreased muscle mass.
What can I do to make my creatinine level normal?
Creatinine is a reflection of processes that are going on in your body and of kidney function. It is not generally responsive to lifestyle changes. If you have an elevated creatinine that is due to a temporary condition, such as a kidney infection, then it should normalize as the infection resolves. If it is elevated due to an underlying chronic condition that can affect kidney function, such as diabetes, then it will reflect changes in kidney function and is likely to stabilize if/when the condition is under control.
How does diet affect creatinine levels?
Some studies have shown that eating cooked meat prior to testing can temporarily increase the level of creatinine. Creatinine levels may be 10%-30% higher in people who eat a diet that is very high in meat.
What is creatine? If I take creatine, will my creatinine levels go up?
Creatine is a compound that is made primarily in the liver and then transported to your muscles, where it is used as an energy source for muscle activity. Once in the muscle, some of the creatine is spontaneously converted to creatinine. The amount of both creatine and creatinine depend on muscle mass, so men usually have higher levels than women. Creatine is now available as a dietary supplement. If you take creatine, your creatinine levels may be higher than when you do not take the supplement. You should tell your healthcare provider about all of the dietary supplements you are taking to help in the evaluation of your lab results.
Will exercise affect my creatinine levels?
In general, moderate exercise will not affect your creatinine levels. As you continue to exercise and build muscle mass, your creatinine levels may increase slightly but not to abnormal levels.
Do creatinine levels change with age?
Creatinine levels relate to both muscle mass and to kidney function. As you age, your muscle mass decreases but your kidneys tend to function less effectively. The net result is not much change in creatinine levels in the blood as you get older.
What is a BUN/Creatinine ratio?
Occasionally, a health practitioner will look at the ratio between a person’s blood urea nitrogen (BUN) and blood creatinine to help determine what is causing these concentrations to be higher than normal. The ratio of blood urea nitrogen (BUN) to creatinine is usually between 10:1 and 20:1. An increased ratio may be due to a condition that causes a decrease in the flow of blood to the kidneys, such as congestive heart failure or dehydration. It may also be seen with increased protein, from gastrointestinal bleeding, or increased protein in the diet. The ratio may be decreased with liver disease (due to decrease in the formation of urea) and malnutrition.
Besides measuring blood creatinine, are there other ways of estimating GFR?
Yes, a set of new Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) calculators was published in 2012. One uses the measure of a substance called cystatin C instead of creatinine to calculate eGFR (estimated GFR) while the other uses measures of both blood creatinine and cystatin C to estimate GFR. Cystatin C is a relatively small protein that is produced throughout the body by all cells that contain a nucleus and is found in a variety of body fluids, including the blood. It is produced, filtered from the blood by the kidneys, and broken down at a constant rate. Unlike creatinine, cystatin C is not significantly affected by muscle mass.
According to the National Kidney Foundation, the newer Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations may be useful for assessing kidney function in people who have differences in diet, such as vegans, very high or very low muscle mass (e.g., body builders or those with muscle-wasting diseases), or for those who have changing muscle mass. They also may be useful for identifying people diagnosed with chronic kidney disease who have the highest risk of complications.
Urine creatinine test
The creatinine urine test measures the amount of creatinine in urine. This test is done to see how well your kidneys are working.
This creatinine urine test is done to see how well your kidneys work. Creatinine is removed by the body entirely by the kidneys. If kidney function is not normal, creatinine level in your urine decreases.
Normal urine creatinine (24-hour sample) values can range from 500 to 2000 mg/day (4420 to 17680 mmol/day). Results depend on your age and amount of lean body mass.
Another way of expressing the normal range for test results is:
- 14 to 26 mg per kg of body mass per day for men ( 123.8 to 229.8 µmol/kg/day)
- 11 to 20 mg per kg of body mass per day for women (97.2 to 176.8 µmol/kg/day)
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor about the meaning of your specific test results.
Creatinine urine test can be used for the following:
- To evaluate how well the kidneys are working
- As part of the creatinine clearance test
- To provide information on other chemicals in the urine, such as albumin or protein
How the urine creatinine test is performed
After you provide a urine sample, it is tested in the lab. If needed, your doctor may ask you to collect your urine at home over 24 hours. Your health care provider will tell you how to do this. Follow instructions exactly so that the results are accurate.
How to prepare for the urine creatinine test
Your health care provider may tell you to temporarily stop taking certain medicines that may affect test results. Be sure to tell your provider about all the medicines you take. These include:
- Antibiotics such as cefoxitin or trimethoprim
- Cimetidine
DO NOT stop taking any medicine before talking to your provider.
How the creatinine urine test will feel
The test involves only normal urination. There is no discomfort.
Creatinine clearance test
The creatinine clearance test helps provide information about how well the kidneys are working. The test compares the creatinine level in urine with the creatinine level in blood.
By comparing the creatinine level in urine with the creatinine level in blood, this test estimates the glomerular filtration rate (GFR). GFR (glomerular filtration rate) is a measure of how well the kidneys are working, especially the kidneys’ filtering units. These filtering units are called glomeruli.
Creatinine is removed, or cleared, from the body entirely by the kidneys. If kidney function is abnormal, creatinine level increases in the blood because less creatinine is released through the urine.
How the creatinine clearance test is performed
Creatinine clearance test test requires both a urine sample and blood sample. You will collect your urine for 24 hours and then have blood taken. Follow instructions exactly. This ensures accurate results.
How to prepare for the creatinine clearance test
Your health care provider may ask you to temporarily stop any medicines that may affect the test results. These include some antibiotics and stomach acid medicines. Be sure to tell your provider about all the medicines you take.
DO NOT stop taking any medicine before talking to your provider.
How the creatinine clearance test will feel
The urine test involves only normal urination. There is no discomfort.
When the needle is inserted to draw blood, some people feel moderate pain. Others feel only a prick or stinging. Afterward, there may be some throbbing or a slight bruise. This soon goes away.
Glomerular filtration rate
Glomerular filtration rate (GFR) is a measure of the function of the kidneys. This test measures the level of creatinine in the blood and uses the result in a formula to calculate a number that reflects how well the kidneys are functioning, called the estimated GFR or eGFR.
- eGFR (mL/min/1.73 m2) = 175 x (serum creatinine)–1.154 x (Age)–0.203 x (0.742 if female) x (1.212 if African American)
- For a free Glomerular Filtration Rate (GFR) Calculators please go here: https://www.niddk.nih.gov/health-information/communication-programs/nkdep/laboratory-evaluation/glomerular-filtration-rate-calculators
Glomeruli are tiny filters in the kidneys that allow waste products to be removed from the blood, while preventing the loss of important constituents, including proteins and blood cells. Every day, healthy kidneys filter about 200 quarts of blood and produce about 2 quarts of urine. The GFR refers to the amount of blood that is filtered by the glomeruli per minute. As a person’s kidney function declines due to damage or disease, the filtration rate decreases and waste products begin to accumulate in the blood.
Chronic kidney disease (CKD) is associated with a decrease in kidney function that is often progressive. Chronic kidney disease (CKD) can be seen with a variety of conditions, including diabetes and high blood pressure. Early detection of kidney dysfunction can help to minimize the damage. This is important as symptoms of kidney disease may not be noticeable until as much as 30-40% of kidney function is lost.
Measuring glomerular filtration rate directly is considered the most accurate way to detect changes in kidney status, but measuring the GFR directly is complicated, requires experienced personnel, and is typically performed only in research settings and transplant centers. Because of this, the estimated GFR (eGFR) is usually used.
The eGFR (estimated GFR) is a calculation based on a serum creatinine test. Creatinine is a muscle waste product that is filtered from the blood by the kidneys and released into the urine at a relatively steady rate. When kidney function decreases, less creatinine is eliminated and concentrations increase in the blood. With the creatinine test, a reasonable estimate of the actual GFR can be determined.
Different equations may be used to calculate eGFR. The following two are most common and require a person’s blood creatinine result, age, and assigned values based upon sex and race.
- Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation (2009)—recommended by the National Kidney Foundation for calculating eGFR in adults
- Modification of Diet in Renal Disease Study (MDRD) equation—some laboratories continue to use this equation
The results reported using one equation versus the other will not be identical but should give a healthcare practitioner similar information.
A different set of Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) calculators was published in 2012. These equations use the result of a cystatin C test. There is also a modified equation for people 18 and under that takes the blood urea nitrogen (BUN) level into consideration along with the factors listed above.
How is estimated glomerular filtration rate used?
The estimated glomerular filtration rate (eGFR) is used to screen for and detect early kidney damage, to help diagnose chronic kidney disease (CKD), and to monitor kidney status. It is a calculation based on the results of a blood creatinine test along with other variables such as age, sex, and race (e.g., African-American, non-African American), depending on the equation used.
The National Kidney Disease Education Program, American Society of Nephrology, and the National Kidney Foundation all recommend that an eGFR be calculated every time a creatinine blood test is done. The creatinine test is ordered frequently as part of a routine comprehensive metabolic panel (CMP) or basic metabolic panel (BMP), or along with a blood urea nitrogen (BUN) test to evaluate the status of a person’s kidneys.
Creatinine, along with estimated glomerular filtration rate (eGFR), is often used to monitor people with known chronic kidney disease and those with conditions such as diabetes and high blood pressure (hypertension) that may lead to kidney damage.
Other tests that may be done at the same time to help detect kidney damage and/or evaluate kidney function are:
- Urine albumin (microalbumin) and albumin/creatinine ratio (ACR)—used to screen people with chronic conditions, such as diabetes and hypertension, that put them at an increased risk of developing kidney disease; increased levels of albumin in the urine may indicate kidney damage.
- Urinalysis—may be used to help detect signs of kidney damage, such as the presence of blood or casts in the urine
When is estimated glomerular filtration rate ordered?
A creatinine test and estimated glomerular filtration rate (eGFR) may be ordered when a healthcare practitioner wants to evaluate a person’s kidney function as part of a health checkup or if kidney disease is suspected. Signs and symptoms of kidney disease may include:
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs, or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure (hypertension)
As kidney disease worsens, symptoms may include:
- Urinating more or less often
- Feeling itchy
- Tiredness, loss of concentration
- Loss of appetite, nausea and/or vomiting
- Swelling and/or numbness in hands and feet
- Darkened skin
- Muscle cramps
An estimated glomerular filtration rate (eGFR) may be repeated if the initial result is abnormal to see if it persists.
The test is usually ordered periodically when a person has a chronic kidney disease (CKD) or a condition such as diabetes or hypertension that is associated with an increased risk of kidney damage.
How can actual glomerular filtration rate be determined?
The best method for directly determining the GFR is a procedure called an “inulin clearance.” It involves introducing a fluid containing the marker molecule inulin (NOT insulin) into your veins (IV – intravenous infusion) and then collecting timed urines over a period of hours. The urine volumes are noted and the inulin in each sample is measured to allow determination of the GFR. This test and other methods of determining GFR, such as those that use radioactive markers, are not routinely ordered and are primarily performed in research settings.
Could I calculate my own eGFR?
If you have had a recent creatinine or cystatin C measurement, you can calculate the eGFR by using one of the calculators for people 19 years of age or older on the National Kidney Foundation (https://www.kidney.org/professionals/KDOQI/gfr) web site. If you have questions about the interpretation of your results, it is best to consult with your healthcare provider. For children and teens younger than 19, see the pediatric eGFR calculator on the National Kidney Foundation website here (https://www.kidney.org/professionals/KDOQI/gfr_calculatorPed).
What does abnormal glomerular filtration rate test result mean?
Estimated GFR results are reported as milliliters/minute/1.73m² (mL/min/1.73m²). Because some laboratories do not collect information on a patient’s race when the sample is collected for testing, they may report calculated results for both African Americans and non-African Americans. The healthcare practitioner uses the result that applies to the particular patient in order to interpret the results correctly.
A normal eGFR for adults is greater than 90 mL/min/1.73m², according to the National Kidney Foundation. (Because the calculation works best for estimating reduced kidney function, actual numbers are only reported once values are less than 60 mL/min/1.73m²).
An eGFR below 60 mL/min/1.73m² suggests that some kidney damage has occurred. The test may be repeated to see if the abnormal result persists. Chronic kidney disease is diagnosed when a person has an eGFR less than 60 mL/min/1.73m² for more than three months.
A person may have some kidney damage even with an eGFR greater than 90 mL/min/1.73m². Other evidence, such as increased urine albumin, may indicate some degree of kidney damage. Thus, a person’s eGFR should be interpreted in relation to the person’s clinical history and presenting conditions.
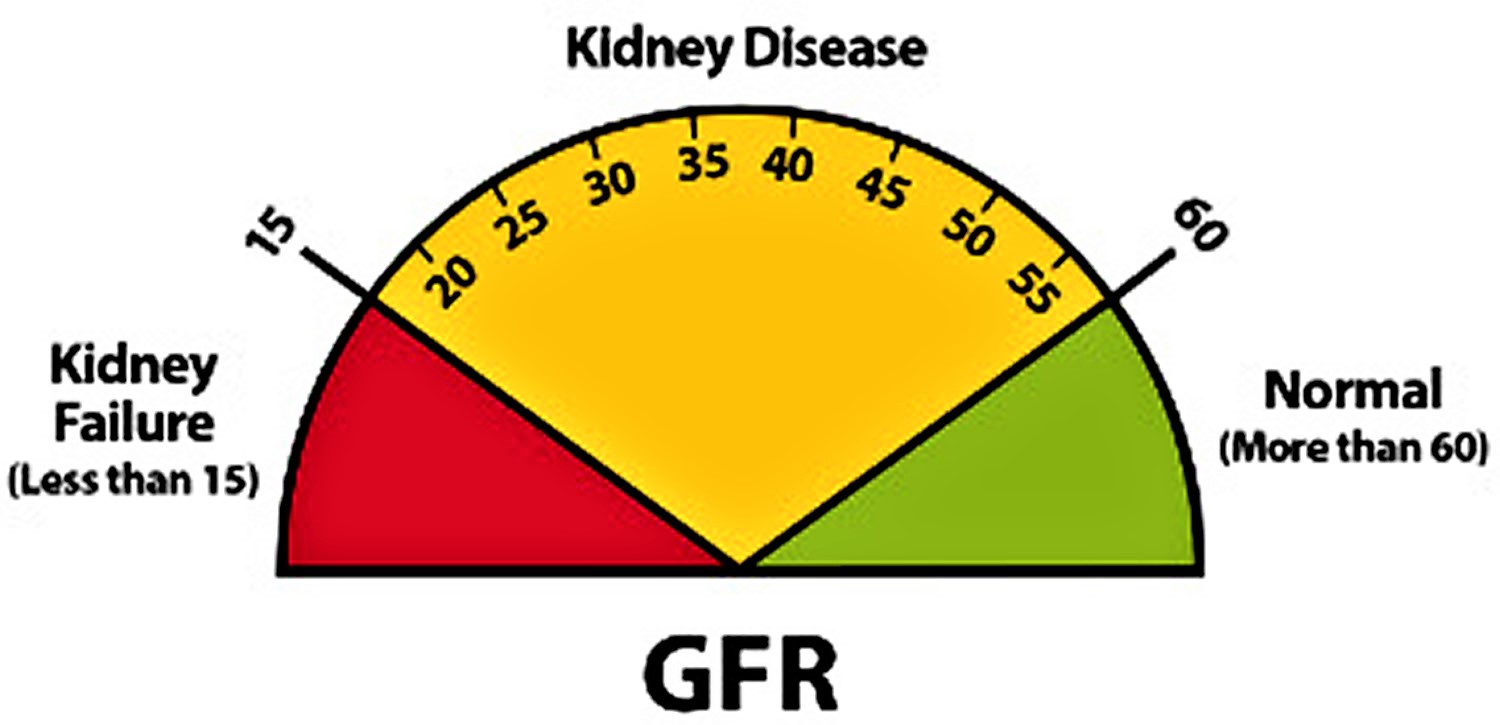
GFR is a measure of how well your kidneys filter blood.
- A GFR of 60 ml/min/1.73 m2 or higher is in the normal range.
- A GFR below 60 ml/min/1.73 m2 may mean kidney disease.
- A GFR of 15 ml/min/1.73 m2 or lower may mean kidney failure.
Figure 6. Kidney function test results
Another method of evaluating kidney function and potentially estimating GFR involves the measurement of the blood level of cystatin C. There is increasing interest in the use of this test for these purposes and several studies have been performed comparing calculations of eGFR using creatinine, cystatin C, or both. According to the National Kidney Foundation (NKF), two meta-analyses concluded that cystatin C is superior to creatinine as a marker of kidney function. The NKF also states that a formula for calculating eGFR that includes both blood creatinine and cystatin C values may improve that estimate (see below).
The creatinine clearance test also provides an estimate of kidney function and of the actual GFR. However, in addition to the serum creatinine, this test requires a timed urine collection (24 hours) for urine creatinine measurement in order to compare blood and urine creatinine concentrations and to calculate the clearance.
The actual amount of creatinine that a person produces and excretes is affected by their muscle mass and by the amount of protein in their diet. Men tend to have higher creatinine levels than women and children.
A person’s GFR decreases with age and some illnesses and usually increases during pregnancy.
A slightly different equation should be used to calculate the eGFR for those under the age of 18 (see below). The eGFR equations are not valid for those who are 70 years of age or older because muscle mass normally decreases with age.
An eGFR may not be as useful for those who differ from normal creatinine concentrations. This may include people who have significantly more muscle (such as a body builder) or less muscle (such as a muscle-wasting disease) than the norm, those who are extremely obese, malnourished, follow a strict vegetarian diet, ingest little protein, or who take creatine dietary supplements.
The eGFR may also be affected by a variety of drugs, such as gentamicin, cisplatin, and cefoxitin that increase creatinine levels, and by any condition that decreases blood flow to the kidneys.
The calculation for eGFR is intended to be used when kidney function and creatinine production are stable. If a creatinine level is measured when the kidney function is changing rapidly, such as with acute kidney failure, then it will not give a useful estimate of the filtration rate.
Why might my healthcare provider repeat my eGFR test?
Besides for periodic monitoring, the eGFR might be repeated if your healthcare provider feels that a temporary condition may be affecting your results.
What other findings might suggest kidney dysfunction?
Diabetics and others at risk for developing kidney disease may be monitored for small amounts of albumin in their urine by performing a urine albumin test. The presence of albumin and other plasma proteins as well as blood in the urine can all be signs of potential kidney damage.
Why are factors such as age, sex, and race used in eGFR calculations?
This is because these factors are known to affect the level of creatinine in the blood. Creatinine is a waste product produced by muscles from the breakdown of a compound called creatine. According to the National Kidney Foundation, men tend to have more muscle mass than women so their creatinine levels tend to be higher. African Americans have a higher average muscle mass and generate more creatinine. As we age, we lose muscle mass and thus have lower blood creatinine levels for the same kidney function the older we get.
Blood Urea Nitrogen (BUN)
Urea is a waste product formed in the liver when protein is metabolized into its component parts (amino acids) . This process produces ammonia, which is then converted into the less toxic waste product urea. Blood urea nitrogen (BUN) test measures the amount of urea nitrogen in your blood.
Nitrogen is a component of both ammonia and urea. Urea and urea nitrogen are referred to somewhat interchangeably because urea contains nitrogen and because urea/urea nitrogen is the “transport method” used by the body to rid itself of excess nitrogen. Urea is released by the liver into the blood and is carried to the kidneys, where it is filtered out of the blood and released into the urine. Since this is an ongoing process, there is usually a small but stable amount of urea nitrogen in the blood. However, when the kidneys cannot filter wastes out of the blood due to disease or damage, then the level of urea in the blood will rise.
Most diseases or conditions that affect the kidneys or liver have the potential to affect the amount of urea present in the blood. If increased amounts of urea are produced by the liver or if the kidneys are not working properly and have difficulty filtering wastes out of the blood, then urea concentrations will rise in the blood. If significant liver damage or disease inhibits the production of urea, then blood urea nitrogen (BUN) concentrations may fall.
The blood urea nitrogen (BUN) test is primarily used, along with the creatinine test, to evaluate kidney function in a wide range of circumstances, to help diagnose kidney disease, and to monitor people with acute or chronic kidney dysfunction or failure. It also may be used to evaluate a person’s general health status when ordered as part of a renal panel, basic metabolic panel or comprehensive metabolic panel.
If the creatinine and BUN tests are found to be abnormal or if someone has an underlying disease that is known to affect the kidneys, such as diabetes or high blood pressure, then creatinine and blood urea nitrogen (BUN) tests may be used to monitor for kidney dysfunction and the effectiveness of treatment. Blood creatinine and BUN tests may also be ordered to evaluate kidney function prior to some procedures, such as a CT (computed tomography) scan, that may require the use of drugs that can damage the kidneys.
Blood urea nitrogen (BUN) levels increase with age. Blood urea nitrogen levels in very young babies are about 2/3 of the levels found in healthy young adults, while levels in adults over 60 years of age are slightly higher than younger adults.
When is blood urea nitrogen (BUN) ordered?
Blood urea nitrogen (BUN) is part of both the basic metabolic panel and comprehensive metabolic panel, groups of tests that are widely used:
- As part of a routine health checkup
- To check how the kidneys are functioning before starting to take certain drug therapies
- When an acutely ill person comes to the emergency room and/or is admitted to the hospital
- During a hospital stay
Although early kidney disease usually does not have any signs or symptoms, certain factors can put you at a higher risk. These include:
- Family history of kidney problems
- Diabetes
- High blood pressure
- Heart disease
Blood urea nitrogen (BUN) is often ordered with creatinine or renal panel when kidney problems are suspected. Some signs and symptoms of kidney dysfunction include:
- Fatigue, lack of concentration, poor appetite, or trouble sleeping
- Swelling or puffiness (edema), particularly around the eyes or in the face, wrists, abdomen, thighs, or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure
- Needing to go the bathroom (urinate) frequently or infrequently
- Itching
- Recurring fatigue
- Muscle cramps
- Trouble sleeping
Blood urea nitrogen (BUN) also may be ordered:
- At regular intervals to monitor kidney function in those with chronic diseases or conditions such as diabetes, congestive heart failure, and myocardial infarction (heart attack)
- At regular intervals to monitor kidney function and treatment in people with known kidney disease
- Prior to and during certain drug treatments to monitor kidney function
- Along with a creatinine when a CT scan is planned
- At regular intervals to monitor the effectiveness of dialysis
What happens during a blood urea nitrogen (BUN) test?
A health care professional will take a blood sample from a vein in your arm, using a small needle. After the needle is inserted, a small amount of blood will be collected into a test tube or vial. You may feel a little sting when the needle goes in or out. This usually takes less than five minutes.
Will I need to do anything to prepare for the blood urea nitrogen (BUN) test?
You don’t need any special preparations for a BUN test. If your health care provider has also ordered other blood tests, you may need to fast (not eat or drink) for several hours before the test. Your health care provider will let you know if there are any special instructions to follow.
What do the blood urea nitrogen (BUN) results mean?
Normal blood urea nitrogen (BUN) levels can vary, but generally a high level of blood urea nitrogen is a sign that your kidneys are not working correctly. However, abnormal results don’t always indicate that you have a medical condition needing treatment. Higher than normal blood urea nitrogen (BUN) levels can also be caused by dehydration, burns, certain medications, a high protein diet, or other factors. To learn what your results mean, talk to your health care provider.
Blood Urea Nitrogen (BUN) levels can increase with the amount of protein in the diet. High-protein diets may cause abnormally high blood urea nitrogen (BUN) levels while very low-protein diets can cause an abnormally low blood urea nitrogen (BUN).
A wide variety of drugs can cause an increase in blood urea nitrogen (BUN). Drugs that can decrease blood urea nitrogen (BUN) include chloramphenicol and streptomycin. Inform your healthcare provider of any medications you are taking.
Both decreased and increased blood urea nitrogen (BUN) concentrations may be seen during a normal pregnancy.
What is a BUN/Creatinine ratio?
Occasionally, a health practitioner will look at the ratio between a person’s blood urea nitrogen (BUN) and blood creatinine to help determine what is causing these concentrations to be higher than normal. The ratio of BUN to creatinine is usually between 10:1 and 20:1. An increased ratio may be due to a condition that causes a decrease in the flow of blood to the kidneys, such as congestive heart failure or dehydration. It may also be seen with increased protein, from gastrointestinal bleeding, or increased protein in the diet. The ratio may be decreased with liver disease (due to decrease in the formation of urea) and malnutrition.
What other tests are used with the blood urea nitrogen test to check how my kidneys are functioning?
BUN and creatinine are the primary tests used to check how well the kidneys are able to filter waste products from your blood. Your healthcare provider may also order a renal panel or electrolyte tests, such as sodium and potassium, or calcium to help understand how your kidneys are functioning.
Cystatin C
Cystatin C is a relatively small protein that is produced throughout the body by all cells that contain a nucleus and is found in a variety of body fluids, including the blood. It is produced, filtered from the blood by the kidneys, and broken down at a constant rate. Cystatin C blood test measures the amount of cystatin C in blood to help evaluate kidney function.
Cystatin C is filtered out of the blood by the glomeruli, clusters of tiny blood vessels in the kidneys that allow water, dissolved substances, and wastes to pass through their walls while retaining blood cells and larger proteins. What passes through the walls of the glomeruli forms a filtrate fluid. From this fluid, the kidneys reabsorb cystatin C, glucose, and other substances. The remaining fluid and wastes are carried to the bladder and excreted as urine. The reabsorbed cystatin C is then broken down and is not returned to the blood.
The rate at which the fluid is filtered is called the glomerular filtration rate (GFR). A decline in kidney function leads to decreases in the GFR and to increases in cystatin C and other measures of kidney function, such as creatinine and urea in the blood. The increases in these levels occur because the kidneys are not able to properly filter the blood at a normal rate, causing their accumulation in the blood. On the other hand, improvement in kidney function is expected to lead to increases in GFR, which would cause cystatin C, creatinine, and urea to decline as a result of the kidneys being able to effectively clear them from the blood.
When the kidneys are functioning normally, concentrations of cystatin C in the blood are stable. However, as kidney function deteriorates, the concentrations begin to rise. This increase in cystatin C occurs as the GFR falls and is often detectable before there is a measurable decrease in kidney function (GFR).
Because cystatin C levels fluctuate with changes in GFR, there has been interest in the cystatin C test as one method of evaluating kidney function. Tests currently used include creatinine, a byproduct of muscle metabolism that is measured in the blood and urine, blood urea nitrogen (BUN), and eGFR (an estimate of the GFR usually calculated from the blood creatinine level). Unlike creatinine, cystatin C is not significantly affected by muscle mass (hence, sex or age), race, or diet, which has led to the idea that it could be a more reliable marker of kidney function and potentially used to generate a more precise estimate of GFR.
While there are growing data and literature supporting the use of cystatin C, there is still a degree of uncertainty about when and how it should be used. However, testing is becoming increasingly more available and steps are being taken toward standardizing the calibration of cystatin C results.
How is cystatin C blood test used?
A cystatin C test may be used as an alternative to creatinine and creatinine clearance to screen for and monitor kidney dysfunction in those with known or suspected kidney disease. Cystatin C test is most useful in special cases where creatinine measurement could be misleading.
For example, in those who have liver cirrhosis, are very obese, are malnourished, practice a vegetarian diet, have amputated limbs, or have reduced muscle mass (elderly and children), creatinine measurements may not be reliable. Since creatinine depends on muscle mass, assessment of kidney function may therefore not be accurate in these individuals with abnormally high or low body mass. Cystatin C is not affected by body mass or diet, and hence is a more reliable marker of kidney function than creatinine.
Measuring cystatin C may also be useful in the early detection of kidney disease when other test results (eGFR, creatinine or urine albumin) may still be normal or borderline and an affected person may have few, if any, symptoms. In this case, the healthcare practitioner may want to confirm if chronic kidney disease is present by measuring cystatin C.
Although cystatin C is less variable and less affected by age, body mass, and diet than creatinine in some individuals, it is not a perfect test and can be affected by a number of drugs and other medical conditions.
Some studies have reported increased cystatin C levels associated with higher levels of C-reactive protein (CRP) or body mass index (BMI), hyperthyroidism, steroid use, malignant diseases, HIV/AIDS, rheumatic diseases, and certain metabolic conditions such as hyperhomocysteinemia (increased homocysteine). In addition, other studies suggest that cystatin C can be cleared by non-kidney pathways, such as in the gut, and that its levels tend to fluctuate among patients with kidney transplants.
Researchers are exploring other uses of cystatin C, such as using it alone or in combination with blood creatinine for estimating the glomerular filtration rate (GFR). A recent study found that an equation for eGFR that includes both creatinine and cystatin C was more accurate than one that uses either of these alone and could be used to confirm chronic kidney disease (CKD) in people with an eGFR near 60, the threshold for CKD. In addition to kidney dysfunction, it has been associated with an increased risk of mortality, cardiovascular disease and heart failure in older adults. These equations are currently being validated in different patient populations prior to it being fully implemented into clinical practice.
Lastly, there is some research suggesting that cystatin C returns to a normal level more quickly than creatinine and could be used to assess kidney function and severity of illness when GFR is rapidly changing in critically ill hospitalized patients.
When is cystatin C ordered?
Cystatin C is gaining acceptance as studies confirm and define its usefulness, especially as an early, sensitive marker for chronic kidney disease (CKD). It may be ordered when a person has a known or suspected disease that affects or potentially affects kidney function and reduces the rate at which the kidneys filter impurities from the blood, the glomerular filtration rate (GFR).
It may be ordered when a healthcare practitioner is not satisfied with the results of other tests, such as a creatinine or creatinine clearance, or wants to check for early kidney dysfunction, particularly in the elderly or in sick babies, and/or wants to monitor known impairment over time.
Research is ongoing to learn more about cystatin C as an indicator of risk of end stage renal disease, heart failure, and death. Studies have also found that, in diverse populations, cystatin C may improve the estimate of GFR when combined in an equation with blood creatinine.
Can cystatin C be measured in my urine?
No. Unlike creatinine, cystatin C is reabsorbed from the glomerular filtrate and then metabolized in the kidneys. Under normal conditions, cystatin C is not found at detectable levels in the urine.
Kidney function test results
Glomerular filtration rate (GFR)
The following table summarizes estimated GFR (eGFR) and the stages of kidney damage
Table 2. Estimated GFR (eGFR) and the stages of kidney damage
| Kidney damage stage | description | estimated gfr (ml/min/1.73M2) | other findings |
|---|---|---|---|
| 1 | Normal or minimal kidney damage with normal GFR | 90+ | Protein or albumin in urine may be high, cells or casts rarely seen in urine |
| 2 | Mild decrease in GFR | 60-89 | Protein or albumin in urine may be high, cells or casts rarely seen in urine |
| 3 | Moderate decrease in GFR | 30-59 | |
| 4 | Severe decrease in GFR | 15-29 | |
| 5 | Kidney failure | <15 |
What does abnormal blood creatinine results mean
A normal blood creatinine result is 0.7 to 1.3 mg/dL (61.9 to 114.9 µmol/L) for men and 0.6 to 1.1 mg/dL (53 to 97.2 µmol/L) for women.
Women usually have a lower creatinine level than men. This is because women usually have less muscle mass than men. Creatinine level varies based on a person’s size and muscle mass.
A higher than normal blood creatinine level may be due to:
- Blocked urinary tract
- Kidney problems, such as kidney damage or failure, infection, or reduced blood flow
- Loss of body fluid (dehydration)
- Muscle problems, such as breakdown of muscle fibers (rhabdomyolysis)
- Problems during pregnancy, such as seizures caused by eclampsia or high blood pressure caused by preeclampsia
A lower than normal blood creatinine level may be due to:
- Conditions involving the muscles and nerves that lead to decreased muscle mass
- Malnutrition
There are many other conditions for which the test may be ordered, such as high blood pressure, diabetes, or medicine overdose. Your provider will tell you more, if needed.
What does abnormal urine creatinine results mean
Normal urine creatinine (24-hour sample) values can range from 500 to 2000 mg/day (4420 to 17680 mmol/day). Results depend on your age and amount of lean body mass.
Another way of expressing the normal range for test results is:
- 14 to 26 mg per kg of body mass per day for men ( 123.8 to 229.8 µmol/kg/day)
- 11 to 20 mg per kg of body mass per day for women (97.2 to 176.8 µmol/kg/day)
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor about the meaning of your specific test results.
Abnormal results of urine creatinine may be due to any of the following:
- High meat diet
- Kidney problems, such as damage to the tubule cells
- Kidney failure
- Too little blood flow to the kidneys, damage to filtering units
- Kidney infection (pyelonephritis)
- Muscle breakdown (rhabdomyolysis), or loss of muscle tissue (myasthenia gravis)
- Urinary tract obstruction
Creatinine clearance test
Normal creatinine clearance test results
Clearance is often measured as milliliters per minute (mL/min) or milliliters per second (mL/s). Normal values are:
- Male: 97 to 137 mL/min (1.65 to 2.33 mL/s).
- Female: 88 to 128 mL/min (14.96 to 2.18 mL/s).
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your doctor to know about the meaning of your specific test results.
What abnormal creatinine clearance test results mean
Abnormal results (lower than normal creatinine clearance) may indicate:
- Kidney problems, such as damage to the tubule cells
- Kidney failure
- Too little blood flow to the kidneys
- Damage to the filtering units of the kidneys
- Loss of body fluids (dehydration)
- Bladder outlet obstruction
- Heart failure
What does abnormal blood urea nitrogen (BUN) test result mean?
Increased blood urea nitrogen (BUN) levels suggest impaired kidney function. This may be due to acute or chronic kidney disease, damage, or failure. It may also be due to a condition that results in decreased blood flow to the kidneys, such as congestive heart failure, shock, stress, recent heart attack, or severe burns, to conditions that cause obstruction of urine flow, or to dehydration.
Blood urea nitrogen (BUN) concentrations may be elevated when there is excessive protein breakdown (catabolism), significantly increased protein in the diet, or gastrointestinal bleeding (because of the proteins present in the blood).
Low blood urea nitrogen (BUN) levels are not common and are not usually a cause for concern. They may be seen in severe liver disease, malnutrition, and sometimes when a person is overhydrated (too much fluid volume), but the BUN test is not usually used to diagnose or monitor these conditions.
If one kidney is fully functional, blood urea nitrogen (BUN) concentrations may be normal even when significant dysfunction is present in the other kidney.
What does abnormal cystatin C test result mean?
A high level of cystatin C in the blood corresponds to a decreased glomerular filtration rate (GFR) and hence to kidney dysfunction.
Since cystatin C is produced throughout the body at a constant rate and removed and broken down by the kidneys, it should remain at a steady level in the blood if the kidneys are working efficiently and the GFR is normal.
Recent studies suggest that increased levels of cystatin C may also indicate an increased risk of heart disease, heart failure, and mortality.
What causes kidney failure
Kidneys can become damaged from a physical injury or a disease like diabetes, high blood pressure, or other disorders.
Diabetes is the most common cause of kidney failure. High blood pressure is the second most common cause of kidney failure.
Other problems that can cause kidney failure include 3:
- Autoimmune diseases, such as lupus and IgA nephropathy
- Genetic diseases (diseases you are born with), such as polycystic kidney disease
- Nephrotic syndrome
- Urinary tract problems
Sometimes the kidneys can stop working very suddenly (within two days). This type of kidney failure is called acute kidney injury or acute renal failure. Common causes of acute renal failure include:
- Heart attack
- Illegal drug use and drug abuse
- Not enough blood flowing to the kidneys
- Urinary tract problems
This type of kidney failure is not always permanent. Your kidneys may go back to normal or almost normal with treatment and if you do not have other serious health problems.
Having one of the health problems that can lead to kidney failure does not mean that you will definitely have kidney failure.
Kidney failure does not happen overnight. It is the end result of a gradual loss of kidney function. In fact, some people do not even know they have kidney disease until their kidneys fail. Why not? Because people with early kidney disease may not have any symptoms. Symptoms usually show up late in the progression of the disease.
Types of Kidney Disease
Kidney disease occurs when the kidneys are damaged and cannot function properly. Numerous conditions and diseases can result in damage to the kidneys, thus affecting their ability to filter waste from the blood while reabsorbing important substances. Generally, kidney disease may present or develop in a few different ways:
- Acute kidney injury (AKI) is the rapid loss of kidney function. It may be recognized when a person suddenly produces urine much less frequently and/or has a dramatic increase in the level of waste products in the blood that the kidneys normally filter out. Acute kidney injury (AKI) is often the result of trauma, illness, or a medication that damages the kidneys. It is most common in people who are already hospitalized, such as those who are critically ill and in the intensive care unit. If the damage caused by acute kidney injury persists, it can eventually progress to chronic kidney disease.
- Chronic kidney disease (CKD) occurs over time and is usually defined as lasting over 3 months. The most common causes are diabetes and high blood pressure (hypertension). According to the National Kidney Foundation, 26 million American adults have chronic kidney disease (CKD) and many more are at risk. However, in some cases, it is preventable or, if detected early enough, treatable to prevent or delay progression to kidney failure.
- Nephrotic syndrome is characterized by the loss of too much protein in the urine. It is caused by damage to the glomeruli and can be a primary disorder of the kidney or secondary to an illness or other condition, such as cancer or lupus. Along with a high amount of protein in the urine, signs and symptoms of nephrotic syndrome include a low amount of albumin in the blood, higher than normal lipid levels in the blood, and swelling (edema) in the legs, feet, and ankles. The condition may be acute or chronic, and the outcome can vary.
- Kidney failure, also called end-stage renal disease or ESRD, is the total or near total loss of kidney function and is permanent. Treatment with hemodialysis or kidney transplant is the only option at this stage of kidney disease to sustain life.
Various factors can cause different patterns of injury to the kidneys and can affect kidney function. Some factors affect the blood-filtering units, the nephrons, or parts of the nephrons, such as the glomeruli or the tubules. Some factors affect the passage of urine from the kidney while others cause damage to the kidney(s) as a whole.
The most common causes of and main risk factors for kidney disease are:
- Diabetes: a sustained high level of blood glucose from uncontrolled diabetes can over time damage the nephrons in the kidneys. This can be avoided by maintaining good glucose control.
- High blood pressure (hypertension): can damage blood vessels within the kidneys, preventing them from filtering wastes from the blood as they should. Hypertension can therefore cause chronic kidney disease (CKD), but having chronic kidney disease (CKD) can cause high blood pressure as well.
- Family history of kidney disease: for example, polycystic kidney disease (PKD) is an inherited disorder in which cysts grow in the kidneys, reducing kidney function over time and eventually leading to kidney failure.
Some other examples of factors affecting the kidneys or patterns of kidney disease include:
- Glomerulonephritis (also called chronic nephritis or nephritic syndrome): a group of diseases that cause inflammation and damage to the blood filtering units of the kidneys (glomeruli) and the third most common type of kidney disease. As blood filtering becomes impaired, urine output decreases, water and waste products accumulate in the blood, and blood appears in the urine. Because the blood cells break down, urine often becomes brown instead of red. Certain body tissues swell with the excess water (a condition called edema). Outcomes can vary: the condition may go away in a few weeks, permanently reduce kidney function, or progress to end-stage renal disease.
- Obstruction: the urinary tract can become blocked, or obstructed, from such things as a kidney stone or tumor. The blockage can lead to infection and injury of the kidney.
- Autoimmune disease: sometimes an autoimmune disorder such as systemic lupus erythematosus or Goodpasture syndrome can lead to glomerular disease and affect the kidneys. In autoimmune diseases, the body’s immune system mistakenly attacks and damages its own tissue and organs, including the kidneys.
- Infections: certain bacteria and viruses can infect the kidneys and cause damage. Repeated urinary tract infections (UTIs) that spread to the kidneys is an example.
- Immune response: infections in other parts of the body can stimulate an immune response that has an adverse effect on the kidneys. Examples include strep infection of the throat or skin, the skin infection impetigo, an infection inside the heart (endocarditis), or a viral infection such as HIV, hepatitis B, or hepatitis C.
- Congenital defects: defects present at birth, such as those that impede the normal flow of urine.
- Injury: trauma to the kidneys can cause AKI that can lead to chronic kidney disease.
- Toxins: some contrast dyes used for imaging procedures and certain medications can have toxic effects on the kidneys.
- Drugs: use and/or overuse of non-steroidal anti-inflammatory drugs (NSAIDS), such as over-the-counter ibuprofen, and various prescription drugs can damage the kidneys. Use of analgesics (pain killers) has been associated with two different forms of kidney damage: acute renal failure and a type of chronic kidney disease called analgesic nephropathy. Certain antibiotics can be directly toxic to the kidneys if their levels are too high. Other drugs may trigger an immune response by the body that subsequently causes kidney damage.
- Pre-renal azotemia: any situation in which there is severe blood loss or reduced blood flow may prevent the kidneys from working properly, such as a blood clot, severe burn, severe dehydration, or septic shock.
- Interstitial nephritis: a kidney disorder in which the spaces between the kidney tubules become inflamed and swollen. It may be acute or chronic. Causes include side effects of certain medications, certain autoimmune disorders, and having a low blood potassium level or a high blood level of calcium or uric acid. It is associated with decreased urine output, blood in the urine, and edema. Usually, this is a short-term condition.
- Acute tubular necrosis (ATN): a kidney disorder involving damage to the tubules in the kidneys. It is one of the most common causes of kidney failure in hospitalized patients. It is caused by a lack of oxygen to the kidney tissues or from damage to the kidneys by toxic substances such as contrast dyes used for x-ray studies and certain medications. In most cases, acute tubular necrosis is reversible.
According to the National Kidney Foundation 4:
- 26 million American adults are estimated to have chronic kidney disease (CKD), although most don’t know it because early signs are often missed
- 2,941,360 Medicare patients are diagnosed with chronic kidney disease (CKD), but not kidney failure
- 548,000 Americans have irreversible kidney failure, or end-stage renal disease (ESRD), and require dialysis or a kidney transplant to survive
- 382,343 End-stage renal disease (ESRD) patients receive dialysis at least 3 times per week to replace kidney function
- 158,739 Americans live with a functioning kidney transplant
- 87,812 People die annually due to end-stage renal disease (ESRD), the ninth leading cause of death
- 15,430 Americans received a kidney transplant in 2010
- 83,621 Americans were on the kidney transplant waiting list on March 3, 2010
- 72% Of new dialysis patients have diabetes and/or hypertension as cause of end-stage renal disease (ESRD)
- 76.3% Of new end-stage renal disease (ESRD) patients apply for Medicare for their primary health insurance
What are signs and symptoms of kidney failure
Healthy kidneys remove wastes and extra fluid from your blood. But when your kidneys fail, wastes and extra fluid can build up in your blood and make you feel sick.
Chronic kidney disease (CKD) can progress silently over many years, with no signs or symptoms or with ones that are too general for a person to suspect as related to kidney function. For that reason, routine blood and urine tests are especially important. They detect blood or protein in the urine and abnormal levels of certain waste products in the blood, such as creatinine and urea (blood urea nitrogen or BUN), which are early signs of kidney dysfunction. The following problems may, however, be warning signs of kidney disease and should not be ignored.
Prompt medical attention is required when any of these are present:
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure (hypertension)
As kidney disease worsens, symptoms may include:
- Urinating more or less often
- Feeling itchy
- Tiredness, loss of concentration
- Loss of appetite, nausea and/or vomiting
- Swelling and/or numbness in hands and feet
- Darkened skin
- Muscle cramps
Acute kidney injury (AKI) is a sudden loss of kidney function and can be fatal. It requires prompt treatment. Symptoms may include:
- Urinating less frequently
- Fluid retention, causing swelling in the legs, ankles or feet
- Drowsiness, fatigue
- Shortness of breath
- Nausea
- Confusion
- Seizures or coma
- Chest pain
When these conditions occur, you need treatment to replace the work your damaged kidneys have stopped doing. Left untreated, kidney failure will lead to coma, seizures, and death.
Once you begin treatment for kidney failure, your symptoms will improve and you will begin to feel much better.
Stages of kidney failure
Chronic kidney disease progresses in stages.
Each stage of chronic kidney disease is related to the level of kidney function and kidney damage.
- Stage 1 – a normal eGFR greater than or equal to 90 ml per minute per 1.73 m2, and albuminuria, hematuria, a pathological abnormality or a structural abnormality.
- Stage 2 – a slightly decreased eGFR between 60 and 89 ml per minute per 1.73 m2, and albuminuria, haematuria, a pathological abnormality or a structural abnormality.
Note: If your kidney function is at stage 1 or 2, you only have chronic kidney disease if you have albuminuria, hematuria, a pathological abnormality or a structural abnormality.
- Stage 3a – a mild to moderate decrease in eGFR between 45 and 59 millilitres per minute per 1.73 m2.
- Stage 3b – a moderate to severe decrease in eGFR between 30 and 44 millilitres per minute per 1.73 m2.
- Stage 4 – a severe decrease in eGFR between 15 and 29 millilitres per minute per 1.73 m2.
- Stage 5 – end stage kidney disease, as eGFR decreases to less than 15 millilitres per minute per 1.73 m2 or dialysis is started.
Figure 7. Stages of Chronic Kidney Disease
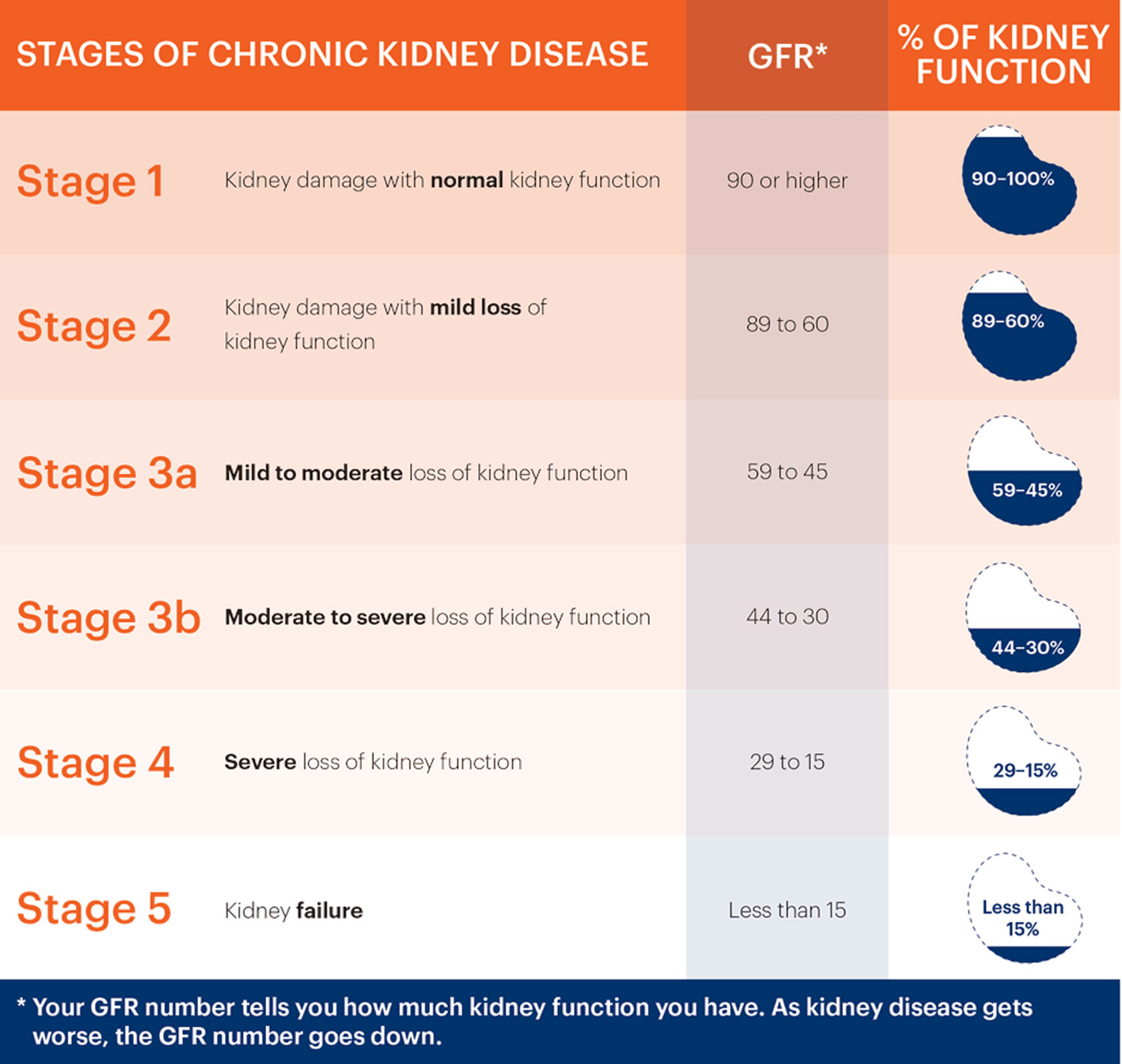
What is chronic kidney disease?
Chronic kidney disease (CKD) is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health.
Chronic kidney disease (CKD) can be slowed and progression halted, but it generally cannot be reversed.
Chronic kidney disease (CKD) means that there has been irreversible loss of kidney function and glomeruli. This is not reversible with present existing medical technology. With treatment, however, you may see an improvement in the glomerular filtration rate (eGFR) and stabilization of kidney function. This is the goal of medical treatment of CKD.
Over 30 million American adults have chronic kidney disease (CKD). It is the ninth leading cause of death in the U.S., yet most people are not aware they have this illness or are at risk.
Table 3. Criteria for chronic kidney disease (CKD)
| Either of the following present for > 3 months | |
|---|---|
| Markers of kidney damage (one or more) |
|
| Decreased GFR | GFR <60 ml/min/1.73 m2 |
| Abbreviations: GFR, glomerular filtration rate. | |
How will kidney failure affect your life ?
Kidney failure will affect your life in many ways. You may find you cannot do all the things you used to do at home or at work. You may have less energy and may feel depressed. Physical problems may include:
- ankle or belly swelling
- stomach sickness
- throwing up
- loss of appetite
- feeling tired
- weakness
- confusion
- headaches
Having kidney failure does not have to take over your life. Having kidney failure does not have to mean giving up hobbies, work, social activities, or time with family.
Kidney disorder and failure treatment
Appropriate treatment will vary, depending on the cause of the kidney disorder. In general, the earlier kidney disease is recognized, the more likely it is to be treatable, and sometimes – as may occur with acute kidney disease – the damage may be reversible. Goals of treatment are to treat underlying conditions, minimize kidney dysfunction, control symptoms, and prevent the progression of kidney disease to the extent possible.
In the case of diabetics, monitoring and controlling blood glucose levels are paramount. For people with hypertension, lowering blood pressure, sometimes through the use of medications, can help protect the kidneys from damage.
Other medications may be used to relieve some of the symptoms of kidney disease, such as anemia and edema, or to lower cholesterol in order to reduce the risk of heart disease. Dietary changes may also be recommended.
Some kidney conditions, such as infections and some acute kidney injuries, can be resolved without causing permanent kidney damage. In many cases, however, the damage cannot be reversed. If the damage is severe and end-stage renal disease has been reached, treatment involves dialysis – a machine used several times a week to take over kidney filtration – or kidney transplant surgery.
You have three treatment options to choose from to filter your blood if you have kidney failure or end-stage renal disease. A fourth option offers care without replacing the work of the kidneys. None of these treatments helps the kidneys get better. However, they all can help you feel better.
- Hemodialysis uses a machine to move your blood through a filter outside your body, removing wastes.
- Peritoneal dialysis uses the lining of your belly to filter your blood inside your body, removing wastes.
- Kidney transplantation is surgery to place a healthy kidney from a person who has just died or a living person, usually a family member, into your body to take over the job of filtering your blood.
- Conservative management is the choice not to treat kidney failure with dialysis or a transplant. Instead, the focus is on using medicines to keep you comfortable, preserving kidney function through diet, and treating the problems of kidney failure, such as anemia—a shortage of red blood cells that can make you tired—and weak bones.
- Lindeman RD, TobinJ, ShockNW. Longitudinal studies on the rate of decline in renal function with age, J Am Geriatr Soc, 1985, vol. 33, pg. 278-85[↩]
- http://nkdep.nih.gov/professionals/gfr_calculators/gfr_faq.htm[↩]
- Kidney failure. American Kidney Fund. http://www.kidneyfund.org/kidney-disease/kidney-failure/[↩]
- Kidney Disease by Numbers. National Kidney Foundation. https://www.kidney.org/sites/default/files/docs/kidney_disease_by_the_numbers.pdf[↩]





{kind=link}