Contents
What is labia minora
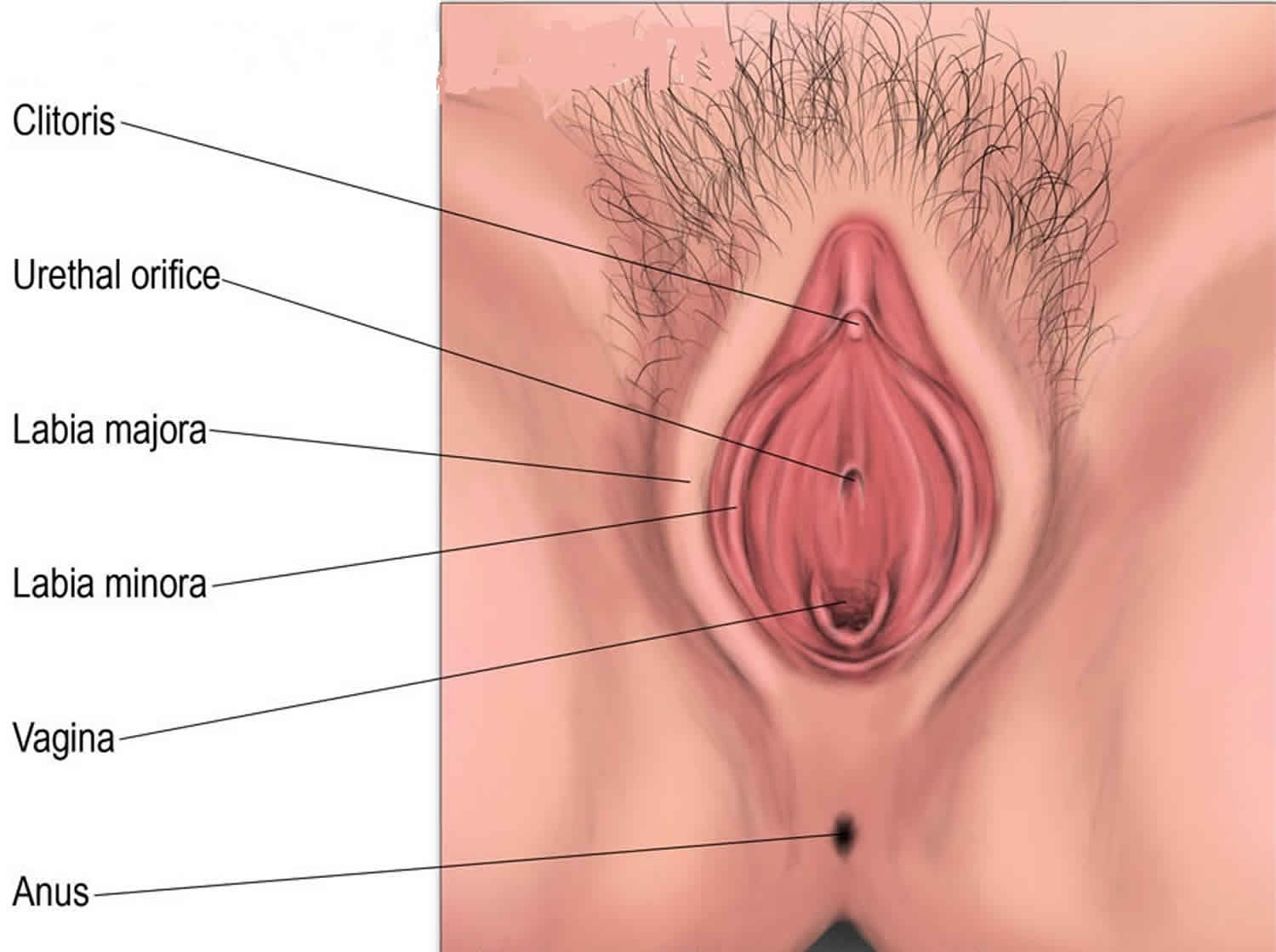
The labia minora (“smaller lips”) is hairless folds of skin which enclose a recess called the vestibule (“entrance hall”) housing the external openings of the urethra
and vagina. The labia minora are homologous to the spongy (penile) urethra in males. Within the vestibule are the hymen (if still present), the vaginal orifice, the external urethral orifice, and the openings of the ducts of several glands. The vaginal orifice, the opening of the vagina to the exterior, occupies the greater portion of the vestibule and is bordered by the hymen.
It is important to note that the labia minora are naturally not perfectly symmetrical, and that one of the labia minora is normally larger than the other, perhaps playing a role in sealing the vaginal introitus and protecting against vaginitis (Figure 1) 1. In the Joani Blank Atlas 2 there are 32 photos of genitalia of women from different ethnicities, all having one labia minora larger than the other.
Figure 1. Labia minora
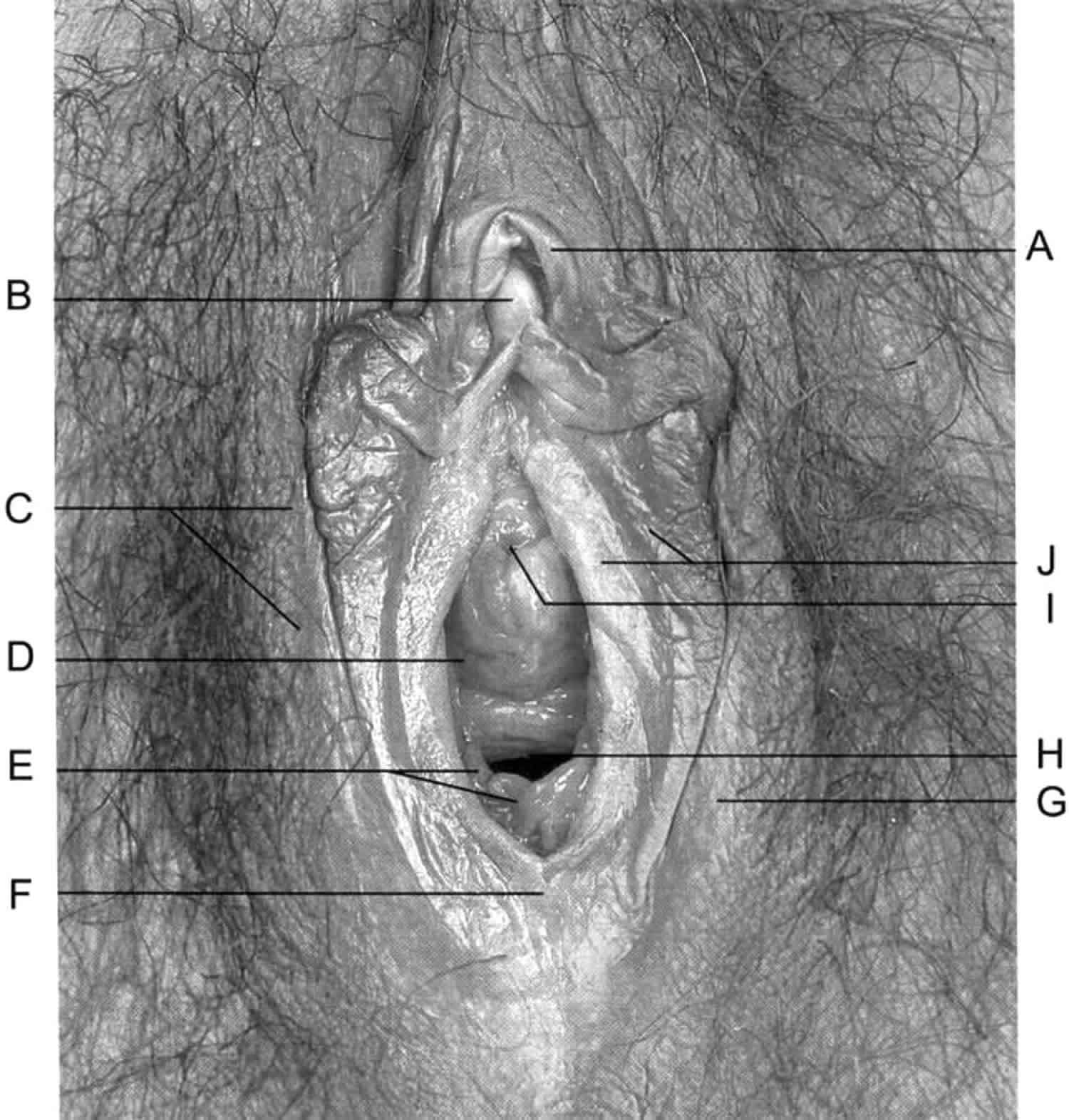
Footnote: Female anatomy. A =Prepuce of clitoris. B= Glans of clitoris. C = Labia majora. D = Vestibule of vagina. E = Hymen. F= Posterior commissure of the labia. G = Labia majora. H = Vaginal orifice. I= Urethral orifice. J = Labia minora.
[Source 3 ]Labia minora function
The labia minora contain many sebaceous glands which produce antimicrobial substances and provide some lubrication during sexual intercourse.
What causes labia minora to grow?
The labia minora grow and widen during puberty in response to an increase in estrogen and other hormones. Pubic hair begins to grow. Pubic hair increases in amount over time and becomes thicker and curlier. The vulva also may change in color. In adults, the color can range from light pink to dark brown-red or black. Color also can vary with different ethnicities. Th e vulva is the term for women’s external genital (sexual) organs. The vulva is the whole area from the pubic mons (the pad of tissue covered by hair) to the anus. The vulva includes the labia majora (outer lips), labia minora (inner lips), the clitoris, the urethral and vaginal openings, and the area between the vagina and the anus called the perineum.
There is a wide range of normal genitalia and the appearance varies from woman to woman. The labia majora can range in width from one fourth of an inch to 2 inches. The labia minora often extend past the labia majora, but it also is normal if they do not. Some women have labia that are uneven in size. All of these differences are normal.
Labia minora hypertrophy
Labia minora hypertrophy may be classified as follows 4:
- Type I Less than 2 cm
- Type II From 2 cm to 4 cm
- Type III From 4 cm to 6 cm
- Type IV Greater than 6 cm
Labia minora surgery
Labia minora surgery or labiaplasty is a surgical procedure to both the labia minora and majora. The popularity of the labia minora surgery has increased dramatically since women realized that redundancies and excesses in their vulva could be managed surgically and produce aesthetically pleasing results 5. Satisfaction has been reported to exceed 90%. Patient motivation for this procedure can vary widely, including symptoms with clothing or intimacy, including visibility or irritation of the vulva with today’s fashions. Regardless of motivation, the primary indication continues to be driven by patient choice as Hamori 6 concluded that males predominantly are unconcerned about the appearance of the female vulva. Labia minora surgery technically should not be expected to improve sexual function, although it can make a woman more confident during intimacy. Labia minora surgery does bring potential risks and complications including scarring and irregular edges, hematoma, bleeding, over-resection or amputation, wound separation, shortened introitus, and even discomfort. Also, there could be subsequent dryness, tightness, painful intercourse, and persistent asymmetry. Over-resection is the most problematic as reconstruction options are limited 7.
Normal labia minora anatomy encompasses a broad range of sizes, thickness, and color. Felicio in 2007 3 defined degrees of labial hypertrophy from type 1 (< 2cm) through type 6 (> 6cm), but since this is rarely a medically necessary procedure, when excess can be removed, a labiaplasty can be done. Ancillary procedures such as clitoral hood reduction need to be considered when planning a labioplasty minora reduction as unaddressed hood redundancies can result in unsightly bumps and bulges. Labia majora reductions or filling also can be considered if the patient is bothered by her perceived deficiencies or excesses as well. There are two reliable methods for reducing labia minora: (1) the trim method, also known as the edge method and (2) the wedge method pioneered by Alter. Technique selection should be based on the anatomy, patient goals, and patient preferences.
It is not unusual, however, for patients to request the reduction of only the larger labia minora because they believe that the asymmetry is abnormal. Usually, the asymmetry is only a matter of degree, and in most cases the asymmetry is normal. In these patients, experts recommend that corrective surgery is not necessary.
For the first 15 days after surgery, discomfort is great. Your surgeon will prescribe antiinflammatory drugs and instruct you to intermittently apply ice packs to increase comfort and minimize edema. Meticulous local wound hygiene is important to prevent infection, and patients are told to avoid immersing themselves in a bathtub or engaging in sexual relations for the first 40 days 3.
Labia minora surgery technique
There are two primary ways to reduce the labia minora: the wedge excision or the trim technique.
The trim technique involves excising excess labia along its edge, preserving at least one cm of minora from the interlabial sulcus to avoid amputation and preserve theoretical functions of the labia for ‘sealing’ the introitus. Excessive removal with this technique will produce an amputation outcome that is difficult to impossible to reconstruct. This technique is best for marked redundancies, excessive thicknesses, and where the patient is accepting of a potential change in the color of the minora edge. This procedure is simpler, can be used in any situation, and wound issues usually resolve on their own. The downside includes poor scarring on the wound edge, scalloping, prominent dog ears near the clitoral hood, and over-resection. Using a w-plasty or zig-zag along the edge can help avoid the scalloping and other potential scar issues and is routine when surgeons employ this technique. Attention must be given toward meticulous excision and closure of the superior and inferior ends of the incisions to prevent dog ears.
The wedge technique, championed by Gary Alter, MD, preserves the natural edge of the labia, resecting a wedge of minora where the redundancies are removed within the wedge. It requires meticulous, layered suturing, realignment of the edge, and avoidance of over-resection that would result in constriction of the introitus. Wedges can be multiple on one side if the conditions merit using more than one. In unique situations, wedges can be combined with trim techniques in attempts to achieve the best outcome possible from one procedure. Healing can be compromised by wound separation resulting in holes in the labia or notching of the edge that would require a revision. Cysts can form in the scar. Variations of wedges have been described where extensions of the resection are directed superiorly along the prepuce to address lateral hood redundancies at the same time.
Other variations of the above techniques as well as de-epithelialization and pedicled flap methods have been described but have failed to produce the consistent and desired outcomes that the trim or wedge methods produce. It is recommended that neophytes start with conservative resections to avoid the dreaded amputation or shortened introitus outcome that seems so common with surgeons thinking of this as a simple procedure.
Sutures used are quick dissolving types, such as Vicryl Rapide, Monocryl, or Chromic, and they are allowed to dissolve over the ensuing weeks. There is a preference for a running vertical mattress closure to oppose the edges and contibute to hemostasis in the deeper tissues. With wedge procedures, the closure is in layers with interrupted, buried 5-0 Vicryl. Patients often are seen at 3 weeks post-op to remove any retained sutures and to evaluate the healing. Itching can be intense as sutures dissolve, and patients should be prepared. Post-operative restrictions include no penetration sex for at least six weeks, avoidance of any pressures on the suture lines, and refraining from any activities that could lead to tension on the incisions. Patients must be tolerant of the impressive swelling that can follow as it may take weeks for resolution. Revisions can be considered once full healing has occurred with the prevailing opinions for complete healing is 6 months from surgery. Patient opinions of the outcomes should be respected and if something is fixable, patients should be offered the opportunity to have a revision done. A quite common complaint is of persistent, albeit less, asymmetry of the labia.
This procedure is a very gratifying one to perform as it produces dramatic results that are easy to appreciate and reproduce. Patients feel much better about themselves and are more confident with intimacy and activities.
Labia minora surgery complications
Complications include scarring and irregular edges, hematoma, bleeding, over-resection or amputation, wound separation, shortened introitus, and even discomfort. In addition, there could be dryness, tightness, painful intercourse. and persistent asymmetry.
Labia minora irritation
The labia minora and vagina can be very sensitive to many products that women commonly use. These include some soaps, shower and bath products, laundry products, panty liners and pads, and feminine hygiene washes and sprays. Over-the-counter and even prescription medications can cause labia minora or vulvar itching and burning that may feel like a vaginal infection. If you already have a vulvar or vaginal problem, using these products may make the pain or itching worse.
Women with vaginal infections or labia minora conditions often use over-the-counter products to stop itching, burning, or pain. Although for some women these products may be helpful at times, for many women they often don’t help and may worsen the pain or itching. Many over-the-counter products for vulvovaginal problems have ingredients that can cause pain or itching. The medicines women buy to treat yeast infections can cause pain or burning, especially the 1-day products. Women often scratch or rub when they feel itchy or irritated, and this makes them feel more uncomfortable. Frequent washing with soap and other cleansing products also can increase pain or itching.
What helps or prevents labia minora irritation?
Stopping the use of everything that can cause or worsen pain or itching is the first step in allowing the skin to heal. If you have a vaginal infection or labia minora skin problem, especially one that does not get better easily or keeps coming back, avoiding all things that might cause pain or itching is an important part of your care. The recommendations that follow will be helpful to women with vaginal and vulvar discomfort. They also will improve vaginal and vulvar health for all women.
Talk to your health care provider about your specific problem and recommended treatment.
Bathing and Hygiene
- Use your hands only to wash. Do not use washcloths, loofahs, puffs, and such. Pat dry after bathing.
- Use an unscented bar soap (examples: Dove, Cetaphil, Basis, Vanicream).
- Avoid bubble baths, bath salts, and scented oils.
- Use soft, white, unscented toilet paper.
- Do not use baby wipes, personal wipes, douches, sprays, perfumes, or other feminine hygiene products. These can cause pain or itching.
- Do not douche. It is not helpful or necessary and sometimes can lead to vaginal infections.
- If you have a problem cleaning aft er a bowel movement, do not rub! Try using mineral oil or an unscented liquid soap (examples: Dove, Cetaphil, Basis, Vanicream). A make up remover that contains mineral oil, petroleum jelly, and paraffin also can be used (example: Albolene moisturizing cleanser).
- Urine leaking can cause the vulva to have a rash or become painful. If this is a problem, try to avoid using pads when you are at home and rinse the vulva with plain water when you can.
During Your Periods
- Avoid wearing panty liners or pads every day. If that is not possible, try to wear them as little as possible and not when you are at home. Use unscented panty liners or pads. Avoid any panty liners or pads that say they retain moisture. Some women find that organic panty liners or pads are helpful
Clothing and Laundry
- Always use the same brand of unscented laundry detergent. Do not use bleach, liquid fabric softeners, or fabric softener sheets that you put in the dryer.
- Wear all cotton underwear, not just cotton-crotch underwear. Do not wear girdles or thongs, and try to keep underwear loose. Pantyhose also can increase moisture and heat that can worsen pain, itching, or rashes. Try knee-high or thigh-high hose.
- Do not sit in a wet bathing suit or stay in sweaty exercise clothes.
- Leaving the vulva uncovered at night (not wearing underwear) to allow the vulvar area to be open to air can be helpful.
Over-the-counter Vulvar and Vaginal Products and Medicines
- Do not use any over-the-counter products for vulvar or vaginal itching. Avoid all products that include benzocaine (examples: Vagisil, Lanacane, Vagicaine). Over-the-counter medicines for yeast infections also can cause pain or itching, especially the 1-day products.
For Comfort
- Do not scratch! Scratching and rubbing will make your symptoms worse. If you cannot stop scratching, contact your health care provider to be evaluated.
- Keep a freezer gel pack in the refrigerator; wrap the pack in a washcloth and put it against your vulva. Refrigerated petroleum jelly (Vaseline) and cold plain yogurt put on a maxi-pad and placed next to the vulva can be soothing.
- Petroleum jelly is a wonderful moisturizer to use on the vulva aft er bathing and can be used anytime for comfort. Do not use petroleum jelly with condoms—it can break down the condom so it gets holes in it.
- A lukewarm or warm bath can be soothing. Do not put any soaps, bubble bath, or oils in the water. Check with your pharmacy for a plastic sitz bath that fi ts into the toilet and use that to sit in for soaking.
- For vulvar skin that is painful from scratching, try a “soak and seal.” Soak in a lukewarm tub or use a compress for 5 to 10 minutes, pat dry, and then apply a layer of petroleum jelly. Th e water soothes the painful skin, and the petroleum jelly keeps the area moist and soft.
For Sexual Activity
- Some birth control products you can get over-the-counter (examples: foam, film, creams, sponges) cause pain or itching for some women. If this happens to you, try a different brand or talk to your health care provider about a different type of birth control.
- A lubricant may be helpful during sex, especially for women who are postmenopausal. Use an unscented lubricant (examples: KY jelly, Astroglide, Slippery Stuff ). Do not use lubricants that will heat on contact. Do not use oils or oil-based lubricants like petroleum jelly with condoms.
- Women who are postmenopausal may find that a vaginal moisturizer is helpful (example: Replens). This is not used as a lubricant when having sex but may make sex more comfortable.
Labia minora pain
Vulvodynia is chronic pain or discomfort around the opening of your vagina (vulva) for which there’s no identifiable cause and which lasts at least three months or longer. Vulvodynia is not caused by an infection, skin disorder, or other medical condition. The pain, burning or irritation associated with vulvodynia can make you so uncomfortable that sitting for long periods or having sex becomes unthinkable. The condition can last for months to years.
If you have vulvodynia, don’t let the absence of visible signs or embarrassment about discussing the symptoms keep you from seeking help. Treatment options are available to lessen your discomfort. And your doctor might be able to determine a cause for your vulvar pain, so it’s important to have an examination.
Researchers and health care providers currently know little about why and how vulvodynia occurs—the condition and the pain have no known cause or cure. Therapies can help relieve symptoms of vulvodynia, but the condition can have some serious effects on women’s reproductive health and day-to-day life.
Although women often don’t mention vulvodynia to their doctors, the condition is fairly common.
If you have pain in your genital area, discuss it with your doctor or ask for a referral to a gynecologist. It’s important to have your doctor rule out more easily treatable causes of vulvar pain — for instance, yeast or bacterial infections, herpes, precancerous skin conditions, genitourinary syndrome of menopause, and medical problems such as diabetes.
It’s also important not to repeatedly use over-the-counter treatments for yeast infections without seeing your doctor. Once your doctor has evaluated your symptoms, he or she can recommend treatments or ways to help you manage your pain.
Vulvodynia causes
Doctors don’t know what causes vulvodynia, but possible contributing factors include:
- Injury to or irritation of the nerves surrounding your vulvar region
- Past vaginal infections
- Allergies or sensitive skin
- Hormonal changes
- Muscle spasm or weakness in the pelvic floor, which supports the uterus, bladder and bowel
Vulvodynia symptoms
The main vulvodynia symptom is pain in your genital area, which can be characterized as:
- Burning
- Soreness
- Stinging
- Rawness
- Painful intercourse (dyspareunia)
- Throbbing
- Itching
Your pain might be constant or occasional. It might occur only when the sensitive area is touched (provoked). You might feel the pain in your entire vulvar area (generalized), or the pain might be localized to a certain area, such as the opening of your vagina (vestibule).
Vulvar tissue might look slightly inflamed or swollen. More often, your vulva appears normal.
A similar condition, vestibulodynia, causes pain only when pressure is applied to the area surrounding the entrance to your vagina.
Vulvodynia complications
Because it can be painful and frustrating and can keep you from wanting sex, vulvodynia can cause emotional problems. For example, fear of having sex can cause spasms in the muscles around your vagina (vaginismus). Other complications might include:
- Anxiety
- Depression
- Sleep disturbances
- Sexual dysfunction
- Altered body image
- Relationship problems
- Decreased quality of life
Vulvodynia diagnosis
Before diagnosing vulvodynia, your doctor will ask you questions about your medical, sexual and surgical history and to understand the location, nature and extent of your symptoms.
Your doctor might also perform a:
- Pelvic exam. Your doctor visually examines your external genitals and vagina for signs of infection or other causes of your symptoms. Even if there’s no visual evidence of infection, your doctor might take a sample of cells from your vagina to test for an infection, such as a yeast infection or bacterial vaginosis.
- Cotton swab test. Your doctor uses a moistened cotton swab to gently check for specific, localized areas of pain in your vulvar region.
Vulvodynia treatment
Vulvodynia treatments focus on relieving symptoms. No one treatment works for every woman. For many, a combination of treatments works best. It can take time to find the right treatments, and it can take time after starting a treatment before you notice relief.
Treatment options include:
- Medications. Steroids, tricyclic antidepressants or anticonvulsants can help lessen chronic pain. Antihistamines might reduce itching.
- Biofeedback therapy. This therapy can help reduce pain by teaching you how to relax your pelvic muscles and control how your body responds to the symptoms.
- Local anesthetics. Medications, such as lidocaine ointment, can provide temporary symptom relief. Your doctor might recommend applying lidocaine 30 minutes before sexual intercourse to reduce your discomfort. Using lidocaine ointment can cause your partner to have temporary numbness after sexual contact.
- Nerve blocks. Women who have long-standing pain that doesn’t respond to other treatments might benefit from local nerve block injections.
- Pelvic floor therapy. Many women with vulvodynia have tension in the muscles of the pelvic floor, which supports the uterus, bladder and bowel. Exercises to relax those muscles can help relieve vulvodynia pain.
- Surgery. In cases of localized vulvodynia or vestibulodynia, surgery to remove the affected skin and tissue (vestibulectomy) relieves pain in some women.
Lifestyle and home remedies
The following tips might help you manage vulvodynia symptoms:
- Try cold compresses or gel packs. Place them directly on your external genital area to ease pain and itching.
- Soak in a sitz bath. Two to three times a day, sit in comfortable, lukewarm (not hot) or cool water with Epsom salts or colloidal oatmeal for five to 10 minutes.
- Avoid tightfitting pantyhose and nylon underwear. Tight clothing restricts airflow to your genital area, often leading to increased temperature and moisture that can cause irritation. Wear white, cotton underwear to increase ventilation and dryness. Try sleeping without underwear at night.
- Avoid hot tubs and soaking in hot baths. Spending time in hot water can cause discomfort and itching.
- Don’t use deodorant tampons or pads. The deodorant can be irritating. If pads are irritating, switch to 100 percent cotton pads.
- Avoid activities that put pressure on your vulva, such as biking or horseback riding.
- Wash gently. Scrubbing the affected area harshly or washing too often can increase irritation. Instead, use plain water to gently clean your vulva with your hand and pat the area dry. After bathing, apply a preservative-free emollient, such as plain petroleum jelly, to create a protective barrier.
- Use lubricants. If you’re sexually active, apply a lubricant before having sex. Don’t use products that contain alcohol, flavor, or warming or cooling agents.
Alternative medicine
Stress tends to worsen vulvodynia and having vulvodynia increases stress. Although there’s little evidence that alternative techniques work, some women get some relief from yoga, meditation, massage and other stress reducers.
Coping and support
You might find talking to other women who have vulvodynia helpful because it can provide information and make you feel less alone. If you don’t want to join a support group, your doctor might be able to recommend a counselor in your area who has experience helping women cope with vulvodynia.
Sex therapy or couples therapy might help you and your partner cope with vulvodynia’s affect on your relationship.
- Rohen JW Yokochi C Drecoll EL Anatomia Humana, Manole LTDA4th ed. São Paulo, Brasil: Manola Ltda. 1998:340[↩]
- Blank J Femalia1 ed. San Francisco: Down There Press; 1993.[↩]
- Yhelda de Alencar Felicio, Labial Surgery, Aesthetic Surgery Journal, Volume 27, Issue 3, May 2007, Pages 322–328, https://doi.org/10.1016/j.asj.2007.03.003[↩][↩][↩]
- Felicio Y Chirurgie Intime La Rev Chir Esth Lang Franc 1992;XVII67:37–43.[↩]
- Willis RN, Wong CS, Patel BC. Labiaplasty Labia Minora Reduction. [Updated 2019 Apr 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448086[↩]
- Aesthetic surgery of the female genitalia: labiaplasty and beyond. Plast Reconstr Surg. 2014 Oct;134(4):661-73. doi: 10.1097/PRS.0000000000000516. https://www.ncbi.nlm.nih.gov/pubmed/25357028[↩]
- Surroca MM, Miranda LS, Ruiz JB. Labiaplasty: A 24-Month Experience in 58 Patients: Outcomes and Statistical Analysis. Ann Plast Surg. 2018 Apr;80(4):316-322[↩]





{kind=link}