Contents
Lipoprotein-A
Lipoprotein-A also known as Lp(a) or lipoprotein(a) is a molecule that has two protein components, apolipoprotein(a) [apo(a)] and apolipoprotein B100 (apo-B100) 1, 2, 3. Lipoprotein-A or Lp(a) is large lipoprotein made by the liver a lot like LDL cholesterol (‘bad cholesterol’) but it’s more ‘sticky’ 4. Lipoproteins are particles made of protein and fats (lipids). Their job is to carry fats also called lipids around your body in your blood. The two main groups of lipoproteins are called HDL or high-density lipoprotein also known as “good” cholesterol and LDL or low-density lipoprotein also known as “bad” cholesterol. Lipoprotein-a or lipoprotein(a) is a type of LDL (“bad” cholesterol). Lipoprotein-a or lipoprotein(a) carry cholesterol to the cells in your arteries. If you have high levels of LDL in your blood, cholesterol can build up in your arteries and form blockages called plaques. This condition is known as atherosclerosis or “hardening of the arteries”. It can lead many serious medical conditions such as coronary artery disease (narrow or blocked arteries in your heart), heart attack (myocardial infarction), stroke, peripheral arterial disease (blocked arteries in your legs or arms) and other blood vessel diseases. Lipoprotein-a or Lp(a) particles are stickier than other types of LDL particles, so they may be more likely to cause blockages and blood clots in your arteries. As a result, if you have high levels of lipoprotein-a or Lp(a) in your blood, it can stick to your artery walls and clog them up, leading to heart disease, stroke and other serious conditions related to blockages and blood clots in your arteries at a young age 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20.
Lipoprotein-a or Lp(a) concentration ranges between less than 0.1 milligrams per deciliter (mg/dL) and greater than 300 mg/dL (less than 0.2 to 750 nanomoles per liter [nmol/L]) and is predominantly (>90%) determined by genetic variability at the LPA gene 21, 22, 23, 24, 25, 26. A 100-mg/dL difference in lipoprotein-a or Lp(a) concentration had the same association with coronary heart disease risk as a 38.67-mg/dL difference in low-density lipoprotein cholesterol (LDL “bad” cholesterol) level 27. The results of this 3 to 5 year randomized trial 27 suggest that lowering lipoprotein-a or Lp(a) level by approximately 100 mg/dL should reduce the risk of coronary heart disease (coronary heart disease death or nonfatal myocardial infarction) by approximately 22% to 25%, which is similar to the association that has been observed for a 38.67-mg/dL reduction in low-density lipoprotein cholesterol (LDL “bad” cholesterol) level during treatment with a statin drug 28, 29, 30. Therefore, it follows that lowering lipoprotein-a or Lp(a) concentration by 80 mg/dL might be expected to reduce the risk of coronary heart disease events by approximately 18% to 20%, while lowering lipoprotein-a or Lp(a) concentration by 50 mg/dL might reduce coronary heart disease events by 10% to 12%, assuming that there are no unrecognized competing risks associated with lowering Lp(a) concentration 27. Therefore, only persons with very high lipoprotein-a or Lp(a) concentrations are likely to benefit substantially from therapies that reduce Lp(a) concentration 27.
In general, Lipoprotein-a or Lp(a) levels above 50 milligrams per deciliter (mg/dL) or 125 nanomoles per liter (nmol/L) are considered high risk for cardiovascular disease, heart attack and stroke. Today, about 20-30% of people (more than 2 billion people) worldwide are estimated to have elevated levels of lipoprotein(a), which are generally thought to start between 30-50 mg/dL 31, 32. Currently, if a person has elevated Lipoprotein-a or Lp(a) levels, they would likely work with their cardiologist to create a plan to take steps to support heart-healthy living and minimize any risks, such as having high blood pressure or high cholesterol 33, 34, 35, 20. Some patients may also consider taking LDL cholesterol-lowering treatments, such as statins or PCSK9 inhibitors 36, 37, 38, 39. In some cases, PCSK9 inhibitors have been shown to lower Lp(a) levels by about 20-30%. Lipoprotein apheresis, which removes excess Lp(a) and LDL cholesterol from the body, is another option, but for people with higher risks 40, 41. According to the Food and Drug Administration (FDA), patients qualified for lipoprotein apheresis present with familial hypercholesterolemia, coronary artery disease and LDL-C >100 mg/dL and Lp(a) > 60 mg/dL. Lipoprotein apheresis procedure is typically performed every two weeks (in some countries weekly). During the one course (3–4 hour) the Lp(a) concentration can be lowered by 50% to 85%. Additionally, lipoprotein apheresis reduces LDL levels by 60% to 85% 42. It is expected that such Lipoprotein-a or Lp(a) lowering reduces the risk of atherosclerotic cardiovascular disease events. For clinical practice, lipoprotein(a) should be measured at least once in adults and results interpreted in the context of a patient’s absolute global cardiovascular risk, with recommendations on intensified early risk factor management by lifestyle modification 20.
However, recent meta-analysis of prospective studies shows that very low lipoprotein-a or Lp(a) levels are associated with increased risk of type 2 diabetes mellitus 43, 44, 45, 46, 47, 48, 49, 50, 51, 50.
Currently there is no expert consensus about when to get a lipoprotein-a or Lp(a) test. Different medical organizations have distinct recommendations, but lipoprotein-a or Lp(a) test is more likely to be recommended if you have risk factors for cardiovascular disease such as 52:
- Past diagnosis of cardiovascular disease
- Very high levels of low-density lipoprotein (LDL) cholesterol (“bad” cholesterol)
- Family history of cardiovascular disease, especially if it occurred early in life (<60 years of age) and in more than one first-degree relatives
- First degree relatives with raised serum lipoprotein(a) levels (>200 nmol/l)
- High potential of having familial hypercholesterolemia (FH), a hereditary disorder causing high levels of “bad” LDL cholesterol or other genetic dyslipidemias.
- Calcific aortic valve stenosis
- A borderline increased (but <15%) 10-year risk of a cardiovascular event
In the U.S., lipoprotein-a or Lp(a) blood test is recommended for people younger than age 65 who have had a heart attack, those with a family history of premature heart disease, and those with elevated LDL cholesterol who haven’t responded to statins, which are cholesterol-lowering drugs that can lower LDL levels by about 30% 53, 54. Since elevated lipoprotein-a or Lp(a) levels are largely due to genetic risks and don’t fluctuate much in response to modifiable risks, such as exercise, a one-time screening would be sufficient for most people 54, 38, 39.
In Europe and Canada, lipoprotein-a or Lp(a) screenings are recommended for everyone 38, 39.
Your doctor or cardiologist may order lipoprotein(a) test if you have certain signs or health conditions that mean you have a high risk for blockages in your arteries, such as 55:
- A family health history of early heart or blood vessel disease (before age 55 for a father or brother and before age 65 for a mother or sister)
- High LDL cholesterol, even though you take medicine to lower it
- Heart or blood vessel disease, especially if your cholesterol and triglyceride levels are normal without taking medicine to lower them
- Signs of an inherited condition called familial hypercholesterolemia
- Had more than one heart attack or more than one procedure to open up narrow or blocked arteries in your heart (angioplasty)
The lipoprotein-a test may also be used to help make decisions about the risks and benefits of taking cholesterol medicine to lower your chance of developing heart and blood vessel disease.
If you are found to have elevated lipoprotein-a or Lp(a) levels (greater than 36 mg/dL [greater than 90 nmol/l]), your cardiologist will create a plan for heart-healthy lifestyle changes to minimize any risks you may have such as having high blood pressure, high cholesterol or diabetes 38, 39. Your cardiologist, after reviewing your risk factors for heart disease, may also consider putting you on LDL cholesterol-lowering drugs such as statins or PCSK9 inhibitors. In some cases, PCSK9 inhibitors have been shown to lower lipoprotein-a levels by about 20-30%. PCSK9 inhibitors (e.g., Alirocumab [Praluent] and evolocumab [Repatha]) are a type of medicine that you inject under your skin every few weeks and are expensive. By stopping the PCSK9 protein, PCSK9 inhibitors (e.g., Alirocumab [Praluent] and evolocumab [Repatha]) can reduce LDL cholesterol levels. Your cardiologist may prescribe a PCSK9 inhibitor and a statin if you are at high risk of complications like heart attack or stroke, or if you have familial hypercholesterolemia. In 2021, the United States Food and Drug Administration (FAD) approved another the PCSK9 inhibitor called inclisiran (Leqvio), joining the already approved alirocumab, for patients with familial hypercholesterolemia 56. The most common side effects of PCSK9 inhibitors are itching, pain, or swelling at the place where you injected it. Lipoprotein apheresis, which removes excess lipoprotein-a and LDL cholesterol from the body to lower blood cholesterol levels, is another option, but is reserved for people with progressive cardiovascular disease despite optimal management of risk factors. Lipoprotein apheresis uses a filtering machine to remove “bad” LDL cholesterol from your blood. Then the machine returns the rest of your blood back to your body.
Lipoprotein(a) key points 20, 52, 57, 58, 59, 60, 24, 25, 26, 61, 62, 63, 64:
- There are strong evidence for a causal relationship between high concentrations of lipoprotein-a and increased risk of cardiovascular disease in different ethnicities.
- This association is continuous even at low levels of low-density lipoprotein (LDL “bad” cholesterol) cholesterol.
- Lipoprotein-a or Lp(a) is a new risk factor for aortic valve stenosis.
- Evidence does not support lipoprotein-a or Lp(a) as a risk factor for venous thromboembolism and impaired fibrinolysis.
- Lifelong very low lipoprotein-a or Lp(a) concentrations may associate with type 2 diabetes mellitus.
- The amount of lipoprotein-a or Lp(a) in your blood is determined by your genes. Lipoprotein-a or Lp(a) concentration is predominantly determined by genetics (>90%), more than any other lipoprotein.
- Lipoprotein(a) levels are genetically determined with an autosomal co-dominant inheritance.
- The Kringle-IV (K-IV) repeat polymorphism explains ∼30–70% of the variability in lipoprotein(a) concentration.
- Lipoprotein-a or Lp(a) level varies with ethnicity (in increasing order: Chinese, White, South Asian, and Black individuals).
- Lipoprotein(a) or Lp(a) levels also differ between men and women, with Lp(a) concentration generally ∼5–10% higher in women than men, in both Black and White individuals. In men, lipoprotein(a) remains relatively constant, whereas in women lipoprotein-a levels tend to increase at menopause
- Lipoprotein-a or Lp(a) should be measured at least once in adults.
- A high lipoprotein-a or Lp(a) concentration should be interpreted in the context of other risk factors and absolute global cardiovascular risk, and addressed through intensified lifestyle and risk factor management.
- Many aspects of the genetic regulation of lipoprotein-a are not fully understood. Identification of causal variants and the mechanisms by which they modulate lipoprotein-a concentration or enhance lipoprotein-a pathogenicity require further research.
- Better understanding of the pathogenicity of the various moieties of lipoprotein-a particles is a priority.
- Investigation of the mechanisms underlying the link between very low lipoprotein-a concentration and the development of diabetes mellitus is needed.
- Standardization and harmonization of lipoprotein-a measurement needs to be improved.
- Studies in larger samples of different ethnicities are needed.
- Whether lipoprotein-a lowering reverses accelerated atherogenesis and aortic valve stenosis progression and reduces cardiovascular events has to be tested.
- The extent of lipoprotein-a lowering required for clinical benefit is also not known.
Figure 1. Lipoprotein-a structure
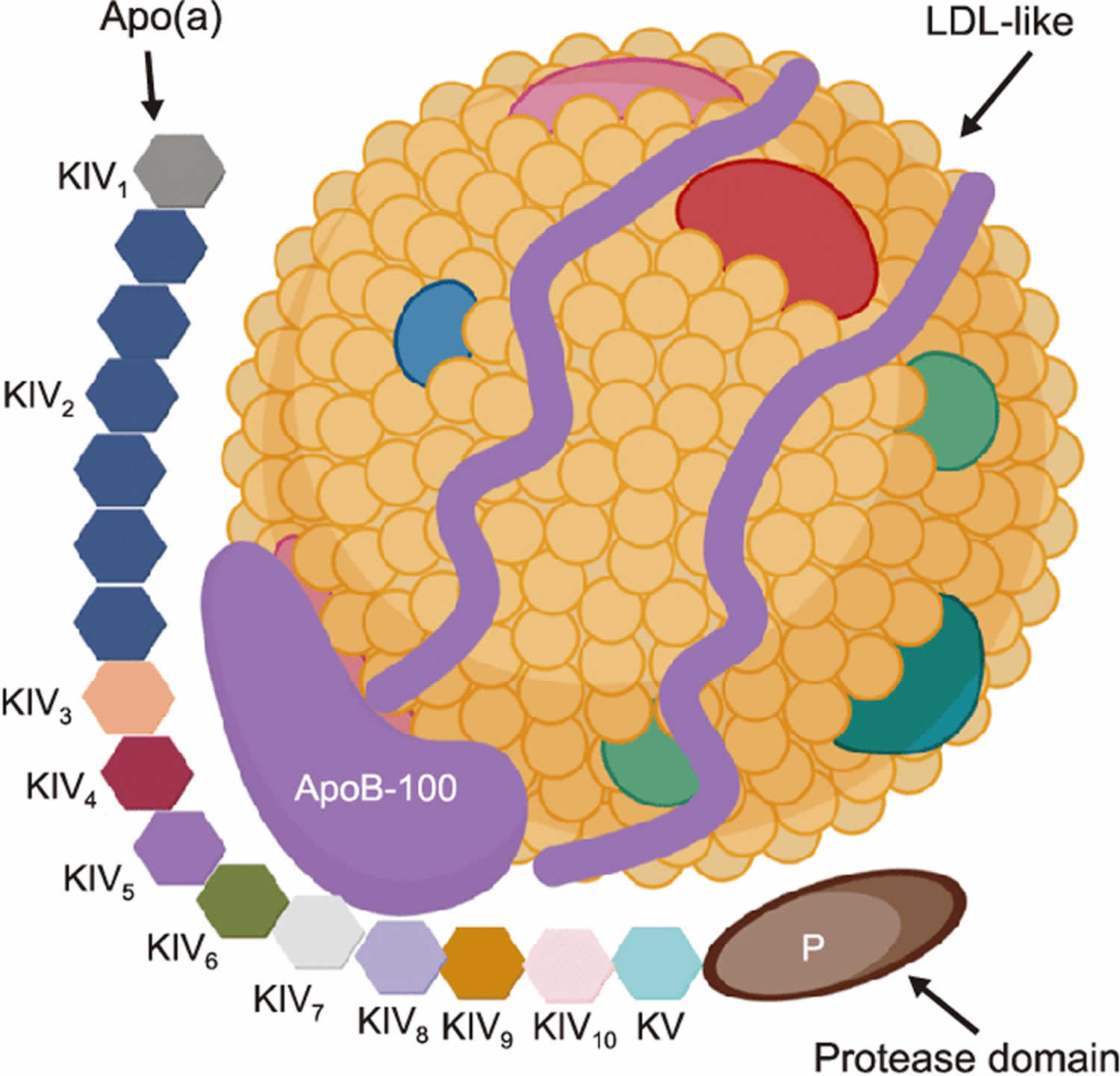
Footnotes: The structure of Lipoprotein(a) [Lp(a)]. Lp(a) is composed of two parts: one part is low-density lipoprotein (LDL)-like particles with apolipoprotein B100 (apo-B100) (blue ribbon) which forms a ribbon and bow-like structure around the cholesteryl-ester core of the LDL component of this particle and the other part is apolipoprotein a [apo(a)] covalently bound by disulfide bonds. Apo(a) contains 10 types (colored hexagons) of kringle IV (KIV) subtypes; one copy of both KIV1 and KIV3-10, and variable KIV2 repetition. In addition, apo(a) is composed of kringle V (KV) and an inactive protease-like domain (P). Only KIV2 is repeated in the apo(a) sequence and the number of KIV2 repetitions is determined by the Lp(a) gene 65, 24. Genetic polymorphism of apo(a) by variable KIV2 repetition determines the level of plasma Lipoprotein(a) [Lp(a)] 66, 31, 67, 68. Both Kringle V and the protease-like domains in apo(a) are highly similar to the plasminogen 69, 70.
[Source 71 ]Figure 2. Lipoprotein-a clinical outcomes
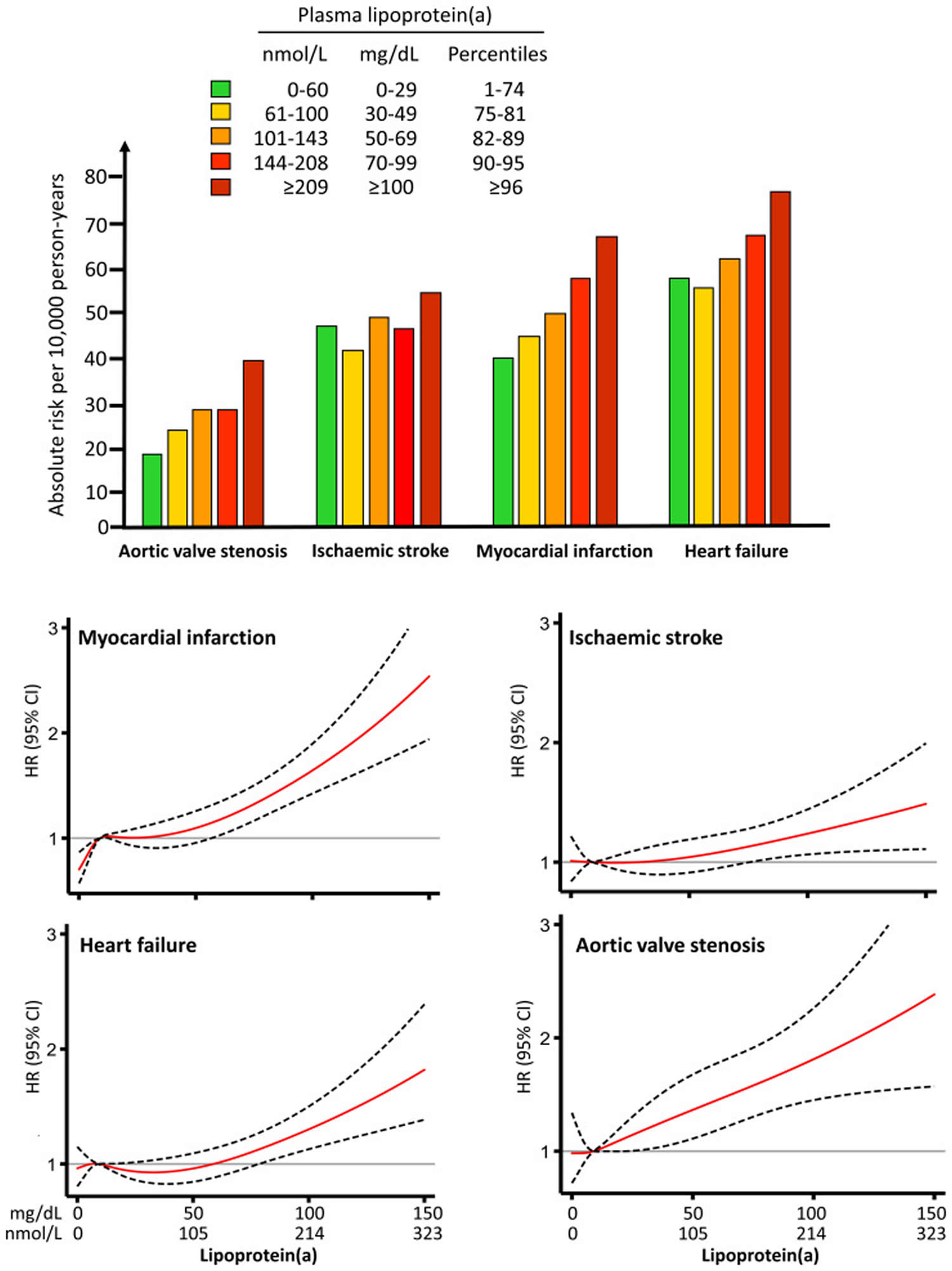
Footnotes: Risk of clinical outcomes with lipoprotein-a or Lp(a) concentration, based on data from 70,286 White individuals in the Copenhagen General Population Study with a median 7.4 years of follow-up. Absolute and relative risks of aortic valve stenosis, ischemic stroke, myocardial infarction and heart failure as a function of increasing plasma lipoprotein-a concentration in the general population. Top panel shows the absolute risk per 10000 person-years, and the lower panel shows hazard ratios as solid red line with 95% confidence intervals as dotted black lines; when the lower 95% confidence interval no longer overlap the hazard ratios reference value of 1.0 for the median lipoprotein-a concentration, risk is significantly elevated.
[Source 20 ]Figure 3. Effect of increasing lipoprotein-A levels and estimated baseline absolute risk for major cardiovascular events
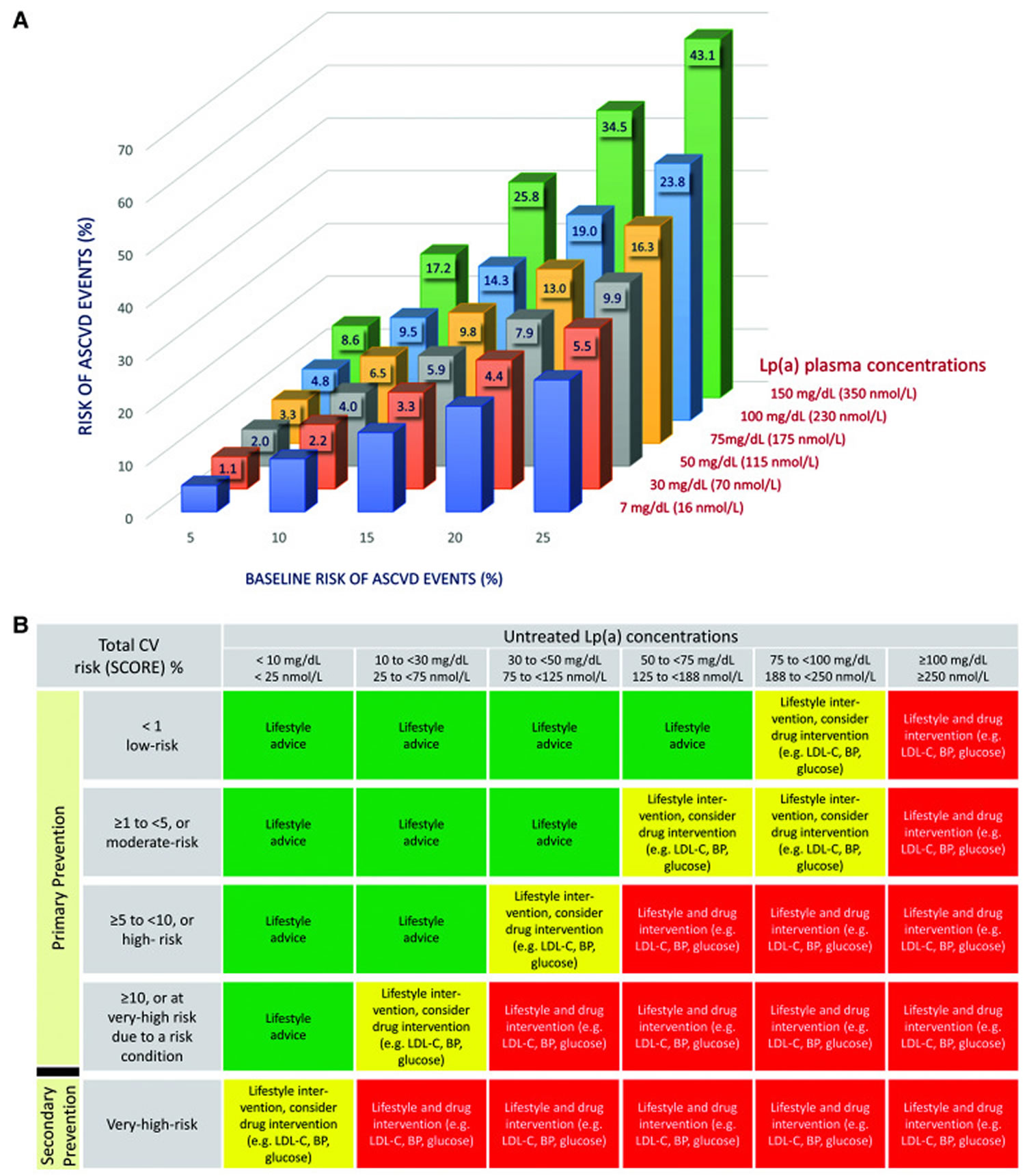
Footnotes: Panel A shows the estimated remaining lifetime risk of a major cardiovascular event [defined as the composite of the first occurrence of fatal or non-fatal myocardial infarction, fatal or non-fatal ischaemic stroke, or coronary revascularization (percutaneous coronary intervention or coronary artery bypass graft surgery)] among 415 274 participants of European ancestry in the UK Biobank for whom measured lipoprotein-a values were available. Participants are divided into categories of baseline estimated lifetime risk (5%, 10%, 15%, 20%, and 25%) calculated using the Joint British Societies (JBS3) Lifetime Risk Estimating algorithm (derived from a similar UK population). Within each baseline risk category, participants are then further divided into categories defined by baseline measured lipoprotein-a concentration. The incremental increase in risk caused by higher lipoprotein-a concentrations from 30 to 150 mg/dL (70 from 350 nmol/L) was estimated by adding lipoprotein-a as an independent exposure to the JBS3 risk estimating algorithm. The numbers at the upper end of each bar represent the increment of increased absolute risk above the estimated baseline risk caused by lipoprotein-a. For example, for a person with a baseline risk of 5%, an lipoprotein-a concentration of 30 mg/dL increases the absolute remaining lifetime risk of a major cardiovascular event by 1.1% to 6.1% (vs. a person with an lipoprotein-a of 7 mg/dL). By contrast, for a person with a baseline risk of 25%, an lipoprotein-a concentration of 30 mg/dL increases the absolute risk of a major cardiovascular event by 5.5% to 30.5% (vs. a person with an lipoprotein-a of 7 mg/dL). For individuals with an lipoprotein-a concentration of 75 mg/dL, the corresponding absolute increases in risk are 3.3% and 16.3%, respectively. The figure illustrates that failure to consider a person’s lipoprotein-a level can lead to a substantial underestimate of their absolute risk of a major cardiovascular event. Panel B provides the intervention strategies as a function of total cardiovascular risk and untreated lipoprotein-a concentration. In the absence of specific lipoprotein-a-lowering therapy, these focus on management of other cardiovascular risk factors.
[Source 20 ]How much should lipoprotein-A be lowered for benefit?
Although estimates vary, several randomization studies suggested that large absolute reductions in lipoprotein-a concentration (greater than 50–100 mg/dL) are needed for a clinically meaningful reduction in the risk of atherosclerotic cardiovascular disease events in a ‘short-term’ (<5 years) clinical trial 37, 27, 72. How much lipoprotein-a needs to be lowered to produce a clinically meaningful benefit remains uncertain. Data are awaited from the lipoprotein-aHORIZON trial in patients with ASCVD and elevated lipoprotein-a (>70 mg/dL) 73.
What is cholesterol?
Cholesterol is a waxy, fat-like substance that’s found in all the cells in your body. Cholesterol is produced by your body and also found in some foods. Your body needs some cholesterol to make hormones, vitamin D and substances that help you digest foods. Cholesterol comes from two sources. Your liver makes all of the cholesterol your body needs to form cell membranes and to make certain hormones. Cholesterol is also found in foods from animal sources, such as egg yolks, meat, and cheese, which is called dietary cholesterol. Although we often blame the cholesterol found in foods that we eat for raising blood cholesterol, the main culprit is actually saturated fat. Foods rich in saturated fat include butter fat in milk products, fat from red meat, and tropical oils such as coconut oil.
Cholesterol travels to cells through your bloodstream in special carriers called lipoproteins. Two of the most important lipoproteins are low-density lipoprotein (LDL) and high-density lipoprotein (HDL).
There are different types of cholesterol:
- HDL stands for high-density lipoprotein or HDL-C (high-density lipoprotein cholesterol). HDL is sometimes called “good cholesterol” because it carries harmful cholesterol from other parts of your body including your arteries back to your liver. Your liver then removes the cholesterol from your body and helps protect you from heart attack and stroke. A healthy HDL-cholesterol level may protect against heart attack and stroke. If you have low HDL levels, you have a greater heart disease risk, even if your total cholesterol is below 200 mg/dL. Your doctor will evaluate your HDL and other cholesterol levels and other factors to assess your risk for heart attack or stroke. People with high blood triglycerides usually also have lower levels of HDL. Genetic factors, Type 2 diabetes, smoking, being overweight and being sedentary can all lower HDL cholesterol. Women tend to have higher levels of HDL cholesterol than men do, because the female hormone estrogen raises HDL, but this can change after menopause.
- LDL stands for low-density lipoprotein or LDL-C (low-density lipoprotein cholesterol). LDL is sometimes called “bad cholesterol” because a high LDL level leads to the buildup of plaque in your arteries. LDL is the most important lipid for predicting your heart disease risk. Low-density lipoprotein (LDL or ‘bad’) cholesterol can join with fats and other substances to build up (also known as plaque) in the inner walls of your arteries, which starts a disease process called atherosclerosis. The arteries can become clogged and narrow, and blood flow is reduced. When plaque builds up in your coronary arteries that supply blood to your heart, you are at greater risk of having a heart attack. Since LDL is the bad kind of cholesterol, a low LDL level is considered good for your heart health. A diet high in saturated and trans fat is unhealthy because it tends to raise LDL cholesterol levels. Your LDL levels may be high if you eat a diet with a lot of saturated fat, cholesterol, or both. Sometimes, an under-active thyroid called hypothyroidism may also increase LDL levels.
- VLDL stands for very low-density lipoprotein or VLDL-C (very low-density lipoprotein cholesterol). Some people also call VLDL a “bad cholesterol” because it too contributes to the buildup of plaque in your arteries. But VLDL and LDL are different; VLDL mainly carries triglycerides and LDL mainly carries cholesterol. VLDL particles are released into the blood by the liver and circulate in the bloodstream, ultimately being converted into LDL as they lose triglyceride, having carried it to other parts of the body. According to the National Heart, Lung and Blood Institute’s National Cholesterol Education Program Guidelines ATP III, there is growing evidence that VLDL plays an important role in atherogenesis, in which plaques form on the interior walls of arteries, narrowing these passageways and restricting blood flow, which can lead to heart disease and increase the risk of stroke. Currently, direct measurement of VLDL cholesterol requires specialized testing. However, since VLDL-C contains most of the circulating triglyceride (if a person is fasting) and since the composition of the different particles is relatively constant, it is possible to estimate the amount of VLDL-C based on the triglyceride value. To estimate VLDL-C, divide the triglyceride value by 5 if the value is in mg/dL or divide by 2.2 if the value is in mmol/L. In most cases, this formula provides a good estimate of VLDL-C. However, this formula becomes less accurate with increased triglyceride levels when, for example, a person has not fasted before having blood drawn. The calculation is not valid when the triglyceride level is greater than 400 mg/dl (4.5 mmol/L) because other lipoproteins are usually present. In this situation, VLDL-C may be measured directly using specialized testing.
- Triglycerides. Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. Triglycerides are fats that provide energy for your muscles. If you eat foods with a lot of saturated fat or carbohydrates, you will raise your triglyceride levels. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels. Elevated triglycerides levels are thought to lead to a greater risk of heart disease, but scientists do not agree that high triglycerides alone are a risk factor for heart disease. Normal triglyceride levels vary by age and sex. People with high triglycerides often have a high total cholesterol level, including a high LDL (bad) cholesterol level and a low HDL (good) cholesterol level. Many people with metabolic syndrome or diabetes also have high triglyceride levels. Extremely high triglyceride levels (more than 1000 mg/dL) can lead to abdominal pain and a life-threatening disorder of the pancreas called pancreatitis. Factors that can contribute to elevated triglyceride levels:
- Overweight or obesity
- Insulin resistance or metabolic syndrome
- Diabetes mellitus, especially with poor glucose control
- Alcohol consumption, especially in excess
- Excess sugar intake, especially from processed foods
- High saturated fat intake
- Hypothyroidism
- Chronic kidney disease
- Physical inactivity
- Pregnancy (especially in the third trimester)
- Inflammatory diseases (such as rheumatoid arthritis, systemic lupus erythematosus
- Some medications may also increase triglycerides.
High cholesterol usually has no symptoms. You can find out the levels of these in your blood and also your total cholesterol level with a cholesterol or lipid profile blood test. If you are concerned about your cholesterol level, talk to your doctor. You will need to stop eating for 10 to 12 hours before a cholesterol or lipid profile blood test, and the only liquid you may drink is water.
According to the National Heart, Lung and Blood Institute, a person’s first cholesterol screening should occur between the ages of 9 and 11 and then be repeated every five years after that 74. The National Heart, Lung and Blood Institute recommends that cholesterol screenings occur every 1 to 2 years for men ages 45 to 65 and for women ages 55 to 65. People over 65 should receive cholesterol tests annually 74. More-frequent cholesterol testing might be needed if your initial cholesterol test results were abnormal or if you already have coronary artery disease, you’re taking cholesterol-lowering medications or you’re at higher risk of coronary artery disease because you:
- Have a family history of high cholesterol or heart attacks
- Are overweight
- Are physically inactive
- Have diabetes
- Eat an unhealthy diet
- Smoke cigarettes
People undergoing treatment for high cholesterol require regular cholesterol testing to monitor the effectiveness of their treatments.
Your doctor can best help you understand what your specific test results mean for your health. Some doctors may set a specific target level when prescribing medication to lower cholesterol. Factors like diet, age, smoking, physical activity, weight, sex, genetics, medicines, and other medical conditions can all affect your LDL cholesterol level.
Lifestyle changes such as exercising and eating a healthy diet are the first line of defense against high cholesterol. But, if you’ve made these important lifestyle changes and your cholesterol levels remain high, your doctor might recommend medication.
Lipoprotein-a causes
Lipoprotein(a) or Lp(a) levels are largely driven by genes that can be passed down through families with up to ≈90% heritability 75, 76. Lipoprotein-a or Lp(a) levels is predominantly (>90%) determined by genetic variability at the LPA gene (genetic polymorphism of apo(a) by variable KIV2 repetition) 66, 31, 67, 68, 21, 22, 23, 24, 25, 26. Your genes control how much lipoprotein(a) or Lp(a) you make 77. The LPA gene encodes for apolipoprotein(a) (apo[a]), a dominant and a rate-limiting component in the hepatic synthesis of the lipoprotein(a) particle 78. The Kringle-IV (K-IV) repeat polymorphism explains ∼30–70% of the variability in lipoprotein(a) concentration 24, 25, 26. By age 5, you usually have your “adult level” of lipoprotein-a and it tends to remain about the same for the rest of your life 77. For that reason, diet and exercise may not change your lipoprotein-a levels.
Lipoprotein(a) or Lp(a) levels also differ between men and women, with Lp(a) concentration generally ∼5–10% higher in women than men, in both Black and White individuals 61, 62, 63. In men, lipoprotein(a) remains relatively constant, whereas in women lipoprotein-a levels tend to increase at menopause 64.
Lipoprotein-a or Lp(a) levels vary significantly among different ethnic groups 79, 80. Lipoprotein-a or Lp(a) distribution is highly right-skewed in Whites with medians of ≈10–12 mg/dL 24. The inter-individual lipoprotein-a concentrations extend for about three orders of magnitude (<0.1 mg/dL to >300 mg/dL) 24 and show considerable cross-ancestry variance 81, 82. In Black populations, the distribution is more Gaussian and median concentrations are markedly higher 81, 83, 84. It has been suggested that genetic variability might be responsible for some of the cross-ancestry differences in lipoprotein-a concentrations 85, 86. Scientists do not completely understand why lipoprotein-a concentrations vary across different ethnic groups. There is evidence that single nucleotide polymorphisms (SNPs) with a strong influence on lipoprotein-a concentrations show a wide frequency variability across ancestries 86, 87, 88, 89. Others also suggested a role of environmental factors 90, 91. Identifying the unknowns might bring us closer to the full picture of cross-ancestry genetic regulation of the Lp(a) concentration differences, helping to dissect the relative contribution of genetics and environment in determining the lipoprotein-a trait across ancestries.
Secondary causes of high lipoprotein-A levels
Although less well-characterized, non-genetic factors may also affect lipoprotein-a concentration (see Table 1 below) 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 64, 108. Lifestyle interventions have minimal impact, but a low carbohydrate/high fat diet may decrease levels by 10–15% 64, 108.
Several hormones, particularly those affecting lipoprotein metabolism, influence lipoprotein-a concentration 97, 98, 99, 100, 101. Impaired kidney function may increase lipoprotein-a levels, possibly due to increased liver lipoprotein-a synthesis triggered by protein loss in urine (nephrotic syndrome) or peritoneal dialysate or impaired catabolism 102, 103, 109, 110, 111, 112. As lipoprotein-a production occurs in the liver, liver disease may decrease lipoprotein-a levels 113. Pre-clinical models showed that inflammation impacts lipoprotein-a level 114, but the effects in population studies were small or negligible 95. Clinically, lipoprotein-a was lower in severe, life-threatening acute-phase conditions, but higher in several acute and chronic inflammatory conditions 105, 106. Increase lipoprotein-a concentration was related to interleukin-6 (IL-6) concentration were reported 115 and decrease lipoprotein-a concentration after treatment of rheumatoid arthritis patients with the IL-6 receptor antibody Tocilizumab 107.
Table 1. Risk factors affecting lipoprotein-A levels
| Condition or intervention | Effect on lipoprotein-A levels |
|---|---|
| Lifestyle | |
| Replacement of dietary saturated fat with carbohydrate or unsaturated fat 108 | ∼10%–15% increase |
| Low carbohydrate diet high in saturated fat 92 | ∼15% decrease |
| Fasting 95 | None |
| Physical activity 96 | None/minimal |
| Hormones and related conditions | |
| Hyperthyroidism (overactive thyroid) 97 | Decrease; 20%–25% increase with thyrostatic treatment or radioactive iodine therapy |
| Hypothyroidism (underactive thyroid) 97 | Increase; 5%–20% decrease with replacement therapy |
| Growth hormones 98 | 2x increase with therapy |
| Endogenous sex hormones 64 | None/minimal |
| Pregnancy 99, 100 | 2x increase |
| Menopause 64 | None/minimal |
| 101Postmenopausal hormonal replacement therapy | ∼25% decrease |
| Surgical or biochemical castration in males 116 | Small increase |
| Ovariectomy, oestrogen receptor antagonist 117 | Small increase |
| Chronic kidney disease 102, 103 | |
| Nephrotic syndrome 109, 111 | 3–5 x increase (vs. control) |
| Peritoneal dialysis patients 110Peritoneal dialysis patients | 2 x increase (vs. control) |
| Hemodialysis treatment and chronic kidney disease 110, 118, 112 | Increases in large apo(a) isoform carriers |
| Kidney transplantation 104Kidney transplantation | ∼Normalization of levels |
| Liver impairment 119, 113 | Decrease, depending on cause |
| Liver transplantation 120 | Changes of apo(a) isoform to that of the donor, with corresponding changes in Lp(a) levels |
| Inflammation and related conditions 121, 114 | |
| Severe, life-threatening acute-phase conditions (sepsis, severe burns) 106 | Decrease |
| Several inflammatory conditions 105 | Increase |
| 107, 115Tocilizumab (interleukin-6 inhibitor) | ∼30%–40% decrease |
| Protease inhibitors or antiretroviral therapy 122, 123 | Increase |
| Statins 124, 125, 54, 126 | May slightly increase Lp(a) (but reports are heterogeneous) |
| Air pollution (fine particulate, PM2.5) 127 | Slight increase |
Lipoprotein-a symptoms
Lipoprotein-a or Lp(a) is thought to speed up the narrowing of the arteries because it is held in the artery walls more readily than LDL cholesterol due to the “sticky” Apo(a) protein. Lipoprotein-a or Lp(a) is thought to increase the development of blood clots. A high level of lipoprotein-a or Lp(a) in the blood has now been identified as a risk factor for diseases of the heart and blood vessels – known as cardiovascular disease 128. Numerous epidemiological and clinical studies have showed a strong association between increased lipoprotein-a or Lp(a) and atherosclerosis, calcific aortic valve disease, aortic stenosis, heart attacks, strokes, peripheral arterial disease (PAD), and heart failure 129, 4, 10, 11, 27, 6, 7, 8, 9, 15, 16, 17, 18, 19.
Lipoprotein-a diagnosis
A lipoprotein-a or Lp(a) blood test can give you a more accurate understanding of your risk than a routine cholesterol test that only measures your total LDL cholesterol level. That’s because a routine cholesterol test may show that your LDL cholesterol level is “healthy,” but if a large percentage of your LDL cholesterol is carried by lipoprotein(a) particles, your risk for heart disease, stroke, and other blood vessel diseases could still be high.
However, lipoprotein-a or Lp(a) blood test is not a routine screening test. Researchers are still studying how lipoprotein(a) levels affect your health and when the test should be used.
In the U.S., lipoprotein-a or Lp(a) blood test is recommended for people younger than age 65 who have had a heart attack, those with a family history of premature heart disease, and those with elevated LDL cholesterol who haven’t responded to statins, which are cholesterol-lowering drugs that can lower LDL levels by about 30% 53, 54. Since elevated lipoprotein-a or Lp(a) levels are largely due to genetic risks and don’t fluctuate much in response to modifiable risks, such as exercise, a one-time screening would be sufficient for most people 54, 38, 39.
In Europe and Canada, lipoprotein-a or Lp(a) screenings are recommended for everyone 38, 39.
Your doctor or cardiologist may order lipoprotein(a) test if you have certain signs or health conditions that mean you have a high risk for blockages in your arteries, such as:
- A family health history of early heart or blood vessel disease (before age 55 for a father or brother and before age 65 for a mother or sister)
- High LDL cholesterol, even though you take medicine to lower it
- Heart or blood vessel disease, especially if your cholesterol and triglyceride levels are normal without taking medicine to lower them
- Signs of an inherited condition called familial hypercholesterolemia
- Had more than one heart attack or more than one procedure to open up narrow or blocked arteries in your heart (angioplasty)
The lipoprotein-a test may also be used to help make decisions about the risks and benefits of taking cholesterol medicine to lower your chance of developing heart and blood vessel disease.
HEART UK’s 2019 Consensus statement for lipoprotein-a and the recently established Lipoprotein(a) Taskforce recommend that lipoprotein-a should be measured in nmol/L of lipoprotein-a particles. Risk of atherosclerotic cardiovascular disease and aortic valve stenosis is determined according to the following thresholds 130:
- 12.8 to 36 mg/dL [32-90 nmol/L] (minor risk)
- 36 to 80 mg/dL [90-200 nmol/L] (moderate risk)
- 80 to 160 mg/dL [200-400 nmol/L] (high risk)
- More than 160 mg/dL [greater than 400nmol/L] (very high risk)
Lipoprotein-a test
Lipoprotein-a test measures the amount of lipoprotein-a or Lp(a) in the blood. The purpose of a lipoprotein-a or Lp(a) test is to evaluate whether you have high levels of lipoprotein-a or Lp(a) that can contribute to cardiovascular diseases like heart attack and stroke. Lipoprotein-a test is not a routine type of cholesterol test, and it is usually reserved if you have already been determined to be at higher risk of cardiovascular problems. Lipoprotein-a or Lp(a) test is not recommended as a screening test in the healthy population without other cardiovascular risks.
Currently there is no expert consensus about when to get a lipoprotein-a or Lp(a) test. Different medical organizations have distinct recommendations, but lipoprotein-a or Lp(a) test is more likely to be recommended if you have risk factors for cardiovascular disease such as:
- Past diagnosis of cardiovascular disease
- Very high levels of low-density lipoprotein (LDL) cholesterol (“bad” cholesterol)
- Family history of cardiovascular disease, especially if it occurred early in life and in more than one first-degree relatives
- High potential of having familial hypercholesterolemia, a hereditary disorder causing high levels of “bad” LDL cholesterol
A test for lipoprotein-a or Lp(a) can also inform treatment decisions related to lowering cholesterol and reducing the risk of heart problems. For example, a doctor and patient may consider lipoprotein-a or Lp(a) levels when deciding whether to use cholesterol-lowering medications. In addition, lipoprotein-a or Lp(a) testing may be recommended if low-density lipoprotein (LDL) cholesterol levels do not decrease as much as expected when taking cholesterol-lowering medications.
Preparations for a lipoprotein-a or Lp(a) test depend on the lab doing the test. Usually, you need to fast (not eat or drink) for 9 to 12 hours before your blood is drawn. Your doctor will let you know if there are any special instructions to follow.
Certain substances can affect your test results. Before you get a lipoprotein-a or Lp(a) test, tell your doctor if you have been drinking alcohol or taking niacin (vitamin B3) supplements, aspirin, or oral estrogen hormones.
Labcorp – lipoprotein-a test
Labcorp’s lipoprotein-a test involves a simple blood test performed at one of the Labcorp’s patient centers. You don’t need to fast or otherwise prep prior to Labcorp’s lipoprotein-a test. You can schedule your appointment online. Labcorp operates more than 2,000 locations nationwide, and you can find the nearest center using a zip code aggregator on the test’s primary webpage.
When purchasing the lipoprotein-a test, you’ll register an account with Labcorp’s online portal. The company takes measures to ensure your information remains secure and confidential. Most people receive their results within one to two business days after their sample is collected. You must have a registered account to view your full report. If your results indicate high lipoprotein-a test levels, you should chat with your doctor about the next steps.
Although Labcorp does not accept insurance as payment, you may purchase the test with an HSA or FSA card. Anyone 18 or older is eligible for the test.
Let’s Get Checked Cholesterol Test
The Let’s Get Checked Cholesterol Test is comprehensive, relatively inexpensive, and easy to administer in the comfort of your own home. Using a blood sample extracted through a finger prick, the test measures the following:
- Lipoprotein-a or Lp(a): Lipoprotein-a or Lp(a) levels are genetically determined, but since this is a type of LDL, you don’t want them to be too high.
- Triglycerides: The most common fats in your body, triglycerides can be a sign of high caloric intake. Your body converts calories into triglycerides when you consume more calories than your body is able to burn, and they are then stored as fat in your body.
- Total Cholesterol: Cholesterol is important for creating vitamin D and digesting fat, but too much can lead to health problems such as heart disease.
- High-Density Lipoprotein (HDL): This type of lipoprotein (a) is often considered “good cholesterol” because it removes “bad” cholesterol from your blood. High HDL levels are generally considered healthy.
- Low-Density Lipoprotein (LDL): LDL is “bad cholesterol,” though it typically makes up most of a person’s total cholesterol. Too much LDL increases your risk of heart attack and stroke.
HDL Percentage of Total Cholesterol: The ratio of HDL to LDL in your total cholesterol count can help you and your doctor explore options if there’s too much of the latter.
You’ll need to fast for this test, meaning it needs to be administered before you eat your first meal of the day — many choose to take the test in the morning before breakfast. Follow the detailed instructions included with your sample collection kit.
Most people receive results within five business days of the lab receiving your specimen. Based on your results, you can pay an additional fee and schedule a virtual consultation with a healthcare provider. You may receive a prescription based on the test, though this also costs extra and is not covered under your initial purchase. There are some state restrictions, so make sure you qualify for the test based on where you live. Adults 18 or older are eligible. Those who sign up for a subscription with Let’s Get Checked receive a 30% discount on their order.
How much does the lipoprotein-a test cost?
The cost of lipoprotein-a or Lp(a) testing depends on many factors such as where the test is done, whether any other measurements are included, and whether testing is covered by health insurance. Complete lipoprotein-a or Lp(a) testing can include charges for the blood draw, office visits, and laboratory analysis of the test sample.
At-home lipoprotein-a or Lp(a) tests vary in costs depending on the lab being used and the type of sample collected.
Because lipoprotein-a or Lp(a) is not part of routine cholesterol testing, some insurance plans may not pay for testing even if your doctor prescribes it. For that reason, you should talk to your insurance company before having a lipoprotein-a or Lp(a) testing.
Cholesterol levels
Your cholesterol levels show how much cholesterol is circulating in your blood. Your blood cholesterol levels tell you how much lipid or fat is in your blood and your cholesterol levels are expressed in milligrams per deciliter (mg/dL).
Total blood or serum cholesterol is a composite of different measurements. Your “total blood cholesterol” is calculated by adding your HDL (“good” cholesterol) and LDL (“bad” cholesterol) cholesterol levels, plus 20% of your triglyceride level. Here’s the formula for calculating your “total blood cholesterol”: Total cholesterol = HDL + LDL + 20% triglycerides.
- “Total cholesterol” is the total amount of cholesterol that’s circulating in your blood. Your “Total cholesterol” should be below 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L.
- Your HDL “good” cholesterol is the one number you want to be high, ideally above 60 mg/dL (1.55 mmol/L) or higher.
- Your LDL “bad” cholesterol should be below 100 mg/dL (less than 2.59 mmol/L).
- Your triglycerides should be below 150 mg/dL (less than 1.70 mmol/L). Triglycerides are the most common type of fat in your blood. Triglycerides come from food, and your body also makes them. When you eat, your body converts calories it doesn’t need into triglycerides, which are stored in fat cells. High triglyceride levels are associated with several factors, including being overweight, eating too many sweets or drinking too much alcohol, smoking, being sedentary, or having diabetes with elevated blood sugar levels.
- Talk with your doctor about what your results mean for you and how to manage your cholesterol.
“Normal cholesterol levels” are less important than your overall cardiovascular risk. Like HDL and LDL cholesterol levels, your total blood cholesterol level should be considered in context with your other known risk factors. To determine your cardiovascular risk, your doctor will consider your cholesterol test results in context with your age, sex and family history. Other risk factors, such as smoking, diabetes and high blood pressure, will be considered as well. If your risk remains uncertain, and treatment options are unclear, your doctor may consider other factors and/or request a coronary artery calcium measurement to provide greater insight into your risk and help in decision-making.
In general, you want to have a total cholesterol level below 200 mg/dL or 5.18 mmol/L. Between 200 mg/dL and 239 mg/dL, your cholesterol level is elevated or borderline-high and should be lowered if you can. With a total cholesterol level of 240 mg/dL or above, your cholesterol level is high, and there is a need for action. For example, changing your diet, beginning an exercise program, and taking statins or other cholesterol-lowering medicines are all ways to lower your cholesterol level.
Figure 2. Cholesterol levels
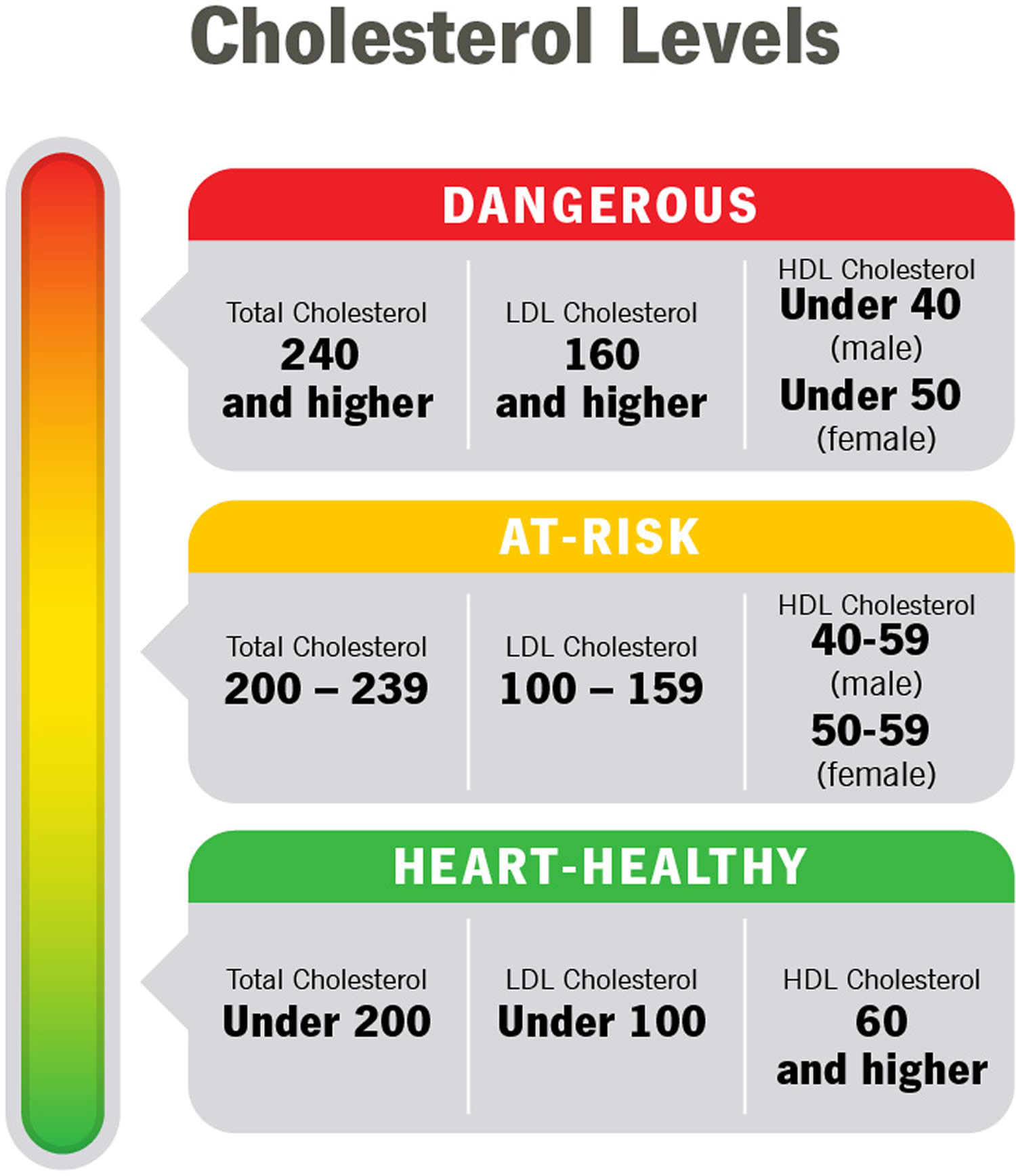
Table 2. Normal Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) | HDL (“good” cholesterol) |
|---|---|---|---|---|
| 19 and younger | Below 170 milligrams per deciliter of blood (mg/dL) | Below 120 mg/dL | Below 110 mg/dL | Above 45 mg/dL |
| 20 and older Male | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 40 mg/dL or higher |
| 20 and older Female | 125 to 200 milligrams per deciliter of blood (mg/dL) | Below 130 mg/dL | Below 100 mg/dL | 50 mg/dL or higher |
Footnotes: As you review your results, remember that you want your LDL to be low and your HDL to be high. Ideally, your HDL should be above 60 mg/dL (1.55 mmol/L). It’s the helpful cholesterol. An HDL above 60 mg/dL (greater than 1.55 mmol/L) offers you protection against heart disease.
Table 3. High Cholesterol Levels
| Age | Total cholesterol | Non-HDL cholesterol | LDL (“bad” cholesterol) |
|---|---|---|---|
| 19 and younger | Borderline high: 170-199 mg/dL High: 200 mg/dL or higher | Borderline high: 120-144 mg/dL High: 145 mg/dL or higher | Borderline high: 110-129 mg/dL High: 130 mg/dL or higher |
| 20 and older | Borderline high: 200-239 mg/dL High: 240 mg/dL or higher | High: 130 mg/dL or higher | Near-optimal: 100-129 mg/dL Borderline high: 130-159 mg/dL High: 160-189 mg/dL Very high: 190 mg/dL or higher |
Footnotes: High cholesterol generally means your total cholesterol is 200 mg/dL (greater than 5.18 mmol/L) or higher. But doctors use additional categories like “borderline high” and “near optimal” to break down your results. If your numbers are close to normal levels, they may be easier to manage through lifestyle and dietary changes.
Table 4. Desirable Cholesterol Levels
| Desirable Cholesterol Levels | |
|---|---|
| Total cholesterol | Less than 200 milligrams per deciliter of blood (mg/dL) or 5.18 mmol/L |
| LDL (“bad” cholesterol) | Less than 100 mg/dL (2.59 mmol/L) |
| HDL (“good” cholesterol) | 60 mg/dL (1.55 mmol/L) or higher |
| Triglycerides | Less than 150 mg/dL (1.70 mmol/L) |
Lipoprotein-a treatment
At the moment, the most important way to manage high lipoprotein-a or Lp(a) levels is optimizing the treatment of all other risk factors for heart disease, your cardiologist will create a plan for heart-healthy lifestyle changes to minimize any risks you may have such as having high blood pressure, high cholesterol or diabetes 52, 38, 39, 53. As other conditions can also affect your lipoprotein-a level, such as chronic kidney disease (CKD), nephrotic kidney disease, hypothyroidism (underactive thyroid), hyperthyroidism (overactive thyroid), your doctor should also aim to find out if you have any underlying conditions and begin treating those conditions as well.
Because lipoprotein-a or Lp(a) levels are determined by your genes, they do not change throughout your lifetime 52. This means once you’ve had your lipoprotein-a level measured, you won’t usually need to have it checked again. However, it is important to be aware of other things that can raise your risk of heart disease – such as being overweight, high blood pressure, not being physically active, a diet high in saturated fat, smoking and drinking too much alcohol – and make healthy lifestyle changes.
Your doctor or cardiologist may suggest that you:
- Eat a healthy diet. At the moment there is not enough evidence to know whether making changes to your diet can make a meaningful difference to your lipoprotein-a levels, but it can lower your LDL (“bad” cholesterol) as well as other types of cholesterol and risk factors for heart disease, such as your blood pressure. Eat a healthy diet to lower your risk of heart disease overall. The DASH eating plans can help you lower your “bad” LDL cholesterol. DASH eating plan encourages:
- Limiting saturated fats found in fatty cuts of meats, dairy products, and desserts
- Eating whole grains, fruits, and vegetables rather than refined carbohydrates such as sweets and other high-sugar foods
- Eating a variety of nuts
- Preparing foods with little or no salt
- Lose excess weight.
- Research has shown that adults with overweight and obesity can lower “bad” LDL cholesterol and raise “good” HDL cholesterol by losing only 3% to 5% of their weight.
- Quit smoking.
- If you smoke, quit. Smoking can raise your risk of heart disease and heart attack and worsen other heart disease risk factors. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke.
- Get regular exercise.
- Studies have shown that physical activity can lower LDL cholesterol and triglycerides and raise your “good” HDL cholesterol. For example, resistance training among postmenopausal women may decrease total cholesterol, LDL cholesterol, and triglycerides. The more active you are, the more you benefit.
- Regular physical activity can:
- Help you lose excess weight
- Improve physical fitness
- Lower many heart disease risk factors such as “bad” LDL cholesterol levels, increase “good” HDL cholesterol levels, and manage high blood pressure
- Lower stress and improve your mental health
- Lower your risk for other conditions such as type 2 diabetes, depression, and cancer
- The U.S. Department of Health and Human Services’ Physical Activity Guidelines for Americans recommends that each week, adults get at least 132:
- 150 minutes (2 hours and 30 minutes) to 300 minutes (5 hours) a week of moderate-intensity aerobic physical activity, or
- 75 minutes (1 hour and 15 minutes) to 150 minutes (2 hours and 30 minutes) a week of vigorous-intensity aerobic physical activity, or
- A combination of both moderate-intensity and vigorous-intensity activity.
- Reduce stress.
- Research has shown that chronic stress can sometimes increase LDL cholesterol levels and decrease HDL cholesterol levels.
- Research suggests that an emotionally upsetting event, particularly one involving anger, can serve as a trigger for a heart attack or angina in some people. Stress can contribute to high blood pressure and other heart disease risk factors. Some of the ways people cope with stress — drinking alcohol, using other substances, smoking, or overeating — are not healthy ways to manage stress.
- Consider healthy stress-reducing activities such as:
- Talking to a professional counselor
- Participating in a stress management program
- Practicing meditation
- Practicing yoga
- Being physically active
- Trying relaxation techniques
- Talking with friends, family, and community or religious support systems
- Lower your blood pressure.
- Changing your lifestyle can help control and manage high blood pressure:
- Eating a heart-healthy diet with less salt
- Getting regular physical activity
- Maintaining a healthy weight or losing weight
- Limiting alcohol
- Not smoking
- Getting 7 to 9 hours of sleep daily
- Changing your lifestyle can help control and manage high blood pressure:
- Limit alcohol.
- Getting enough good-quality sleep. Getting 7 to 9 hours of sleep every night lowers your risk of high LDL cholesterol and total cholesterol levels.
Lipoprotein-a medication
Lifestyle changes such as exercising and eating a healthy diet are the first line of defense against high cholesterol. But, if you’ve made these important lifestyle changes and your cholesterol levels remain high, your cardiologist, after reviewing your risk factors for heart disease, may also consider putting you on LDL cholesterol-lowering drugs such as statins or PCSK9 inhibitors. In some cases, PCSK9 inhibitors have been shown to lower lipoprotein-a levels by about 20-30%.
Statins
Statins are the most common medicine used to treat high blood cholesterol. Statins reduce the amount of cholesterol made in the liver. This causes your liver to remove cholesterol from your blood. Choices include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pitavastatin (Livalo), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor). Studies have shown that statins lower the risk of heart attack and stroke in people with high LDL cholesterol. Although statins may slightly increase lipoprotein-a levels 124, 125, 54, 126, treatment should not be discontinued as the cardiovascular benefits in patients with high lipoprotein-a far outweigh any potential risk associated with modest increases in lipoprotein-a levels 124, 133. Statins may also raise your risk of type 2 diabetes. However, this mainly happens in people already at high risk of diabetes, such as those who have prediabetes, overweight or obesity, or metabolic syndrome. Statins may also cause abnormal results on liver enzymes tests, but actual liver damage is extremely rare. Other rare side effects of statins include muscle damage and cognitive impairment.
PCSK9 inhibitors
Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors (e.g., Alirocumab [Praluent] and evolocumab [Repatha]) are a type of medicine that you inject under your skin every few weeks and are expensive. By stopping the PCSK9 protein, PCSK9 inhibitors (e.g., Alirocumab [Praluent] and evolocumab [Repatha]) can reduce LDL cholesterol levels. The most common side effects of PCSK9 inhibitors are itching, pain, or swelling at the place where you injected it. Your cardiologist may prescribe a PCSK9 inhibitor and a statin if you are at high risk of complications like heart attack or stroke, or if you have familial hypercholesterolemia. In 2021, the United States Food and Drug Administration (FAD) approved another the PCSK9 inhibitor called inclisiran (Leqvio), joining the already approved alirocumab, for patients with familial hypercholesterolemia 56. In major studies with PCSK9 inhibitors, the absolute cardiovascular risk reduction with this treatment was higher at higher baseline lipoprotein-a levels. In FOURIER, the absolute risk reduction was 2.41% vs. 1.41% with an lipoprotein-a >50 vs. <50 mg/dL 134 and in ODYSSEY OUTCOMES, 3.7% at lipoprotein-a >60 mg/dL vs. 0.5% in the lowest lipoprotein-a quartile 135. However, PCSK9 inhibitors are not registered for lipoprotein-a lowering.
Lipoprotein apheresis
Lipoprotein apheresis which removes excess lipoprotein-a and LDL cholesterol from your body to lower blood cholesterol levels, is another option, but is reserved for people with progressive cardiovascular disease despite optimal management of risk factors 136. Lipoprotein apheresis uses a filtering machine to remove “bad” LDL cholesterol from your blood. Then the machine returns the rest of your blood back to your body. Lipoprotein apheresis is a weekly-fortnightly treatment similar to kidney dialysis which can reduce lipoprotein-a levels by up to 75%.
New treatments being researched
Novel antisense and small interfering RNA (siRNA) treatments that target apo(a) production in the hepatocyte lower lipoprotein-a concentration 137. In early trials, mean decreases of 80 and 72% were reported with the antisense oligonucleotide pelacarsen [formerly TQJ230 and AKCEA-APO(a)-LRx] given 20 mg weekly and 60 mg every 4 weeks, respectively, with 98% and 81% of participants attaining lipoprotein-a levels <125 nmol/L at the end of the study 138. Reductions ranging between 71% and 97% were observed with olpasiran (formerly AMG 890), a N-acetylgalactosamine (GalNAc)-conjugated siRNA, which were sustained for over 6 months 139. Both treatments showed a favourable safety profile. Another GalNAc-conjugated siRNA (SLN360, Silence Therapeutics) is in early development 140.
Mipomersen is a 2′-O-methoxy ethyl (2′-MOE)-modified second-generation antisense oligonucleotide (ASO), which binds to the homologous apolipoprotein B-100 (apoB-100) messenger ribonucleic acid (mRNA) 141, 142, 143. Due to the inhibition of the synthesis of apolipoprotein B-100 (apoB-100), the plasma concentration of LDL, apoB and lipoprotein-a can be significantly reduced. In the existing phase 3 randomized trial, in patients with hypercholesterolemia of different causes, mipomersen continuously reduced the median plasma lipoprotein-a level by 26.4% 141. Mipomersen is approved by the FDA for lowering low-density lipoprotein (LDL) cholesterol, apo(B) and other lipoprotein in homozygous familial hypercholesterolemia. A meta-analysis found that the level of lipoprotein-a was reduced 26% from baseline 144.
- Peripheral Vascular Disease; Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2022, 42, e48–e60.[↩]
- Kronenberg F. Human genetics and the causal role of lipoprotein(a) for various diseases. Cardiovasc Drugs Ther. 2016;30(1):87–100. doi: 10.1007/s10557-016-6648-3[↩]
- Schmidt K, Noureen A, Kronenberg F, Utermann G. Structure, function, and genetics of lipoprotein (a) J Lipid Res. 2016;57:1339–1359. doi: 10.1194/jlr.R067314[↩]
- Pasławska A, Tomasik PJ. Lipoprotein(a)—60 Years Later—What Do We Know? Cells. 2023; 12(20):2472. https://doi.org/10.3390/cells12202472[↩][↩]
- Anne Langsted, Pia R Kamstrup, Børge G Nordestgaard, High lipoprotein(a) and high risk of mortality, European Heart Journal, Volume 40, Issue 33, 1 September 2019, Pages 2760–2770, https://doi.org/10.1093/eurheartj/ehy902[↩]
- Emerging Risk Factors Collaboration; Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, Thompson A, White IR, Marcovina SM, Collins R, Thompson SG, Danesh J. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009 Jul 22;302(4):412-23. doi: 10.1001/jama.2009.1063[↩][↩]
- Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009 Jun 10;301(22):2331-9. doi: 10.1001/jama.2009.801[↩][↩]
- Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, Heath SC, Parish S, Barlera S, Franzosi MG, Rust S, Bennett D, Silveira A, Malarstig A, Green FR, Lathrop M, Gigante B, Leander K, de Faire U, Seedorf U, Hamsten A, Collins R, Watkins H, Farrall M; PROCARDIS Consortium. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009 Dec 24;361(26):2518-28. doi: 10.1056/NEJMoa0902604[↩][↩]
- Nordestgaard BG, Langsted A. Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology. J Lipid Res. 2016 Nov;57(11):1953-1975. doi: 10.1194/jlr.R071233[↩][↩]
- Paré, G.; Çaku, A.; McQueen, M.; Anand, S.S.; Enas, E.; Clarke, R.; Boffa, M.B.; Koschinsky, M.; Wang, X.; Yusuf, S.; et al. Lipoprotein(a) Levels and the Risk of Myocardial Infarction Among 7 Ethnic Groups. Circulation 2019, 139, 1472–1482.[↩][↩]
- Langsted A, Kamstrup PR, Nordestgaard BG. High lipoprotein(a) and high risk of mortality. Eur Heart J. 2019 Sep 1;40(33):2760-2770. doi: 10.1093/eurheartj/ehy902[↩][↩]
- Burgess S, Ference BA, Staley JR, et al. European Prospective Investigation Into Cancer and Nutrition–Cardiovascular Disease (EPIC-CVD) Consortium. Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol. 2018 Jul 1;3(7):619-627. doi: 10.1001/jamacardio.2018.1470[↩]
- Pavanello, C.; Pirazzi, C.; Bjorkman, K.; Sandstedt, J.; Tarlarini, C.; Mosca, L.; Romeo, S.; Calabresi, L.; Mancina, R.M. Individuals with familial hypercholesterolemia and cardiovascular events have higher circulating Lp(a) levels. J. Clin. Lipidol. 2019, 13, 778–787.[↩]
- Patel AP, Wang (汪敏先) M, Pirruccello JP, Ellinor PT, Ng K, Kathiresan S, Khera AV. Lp(a) (Lipoprotein[a]) Concentrations and Incident Atherosclerotic Cardiovascular Disease: New Insights From a Large National Biobank. Arterioscler Thromb Vasc Biol. 2021 Jan;41(1):465-474. doi: 10.1161/ATVBAHA.120.315291[↩]
- Kamstrup PR, Tybjærg-Hansen A, Nordestgaard BG. Extreme lipoprotein(a) levels and improved cardiovascular risk prediction. J Am Coll Cardiol. 2013 Mar 19;61(11):1146-56. doi: 10.1016/j.jacc.2012.12.023[↩][↩]
- Kamstrup PR, Tybjærg-Hansen A, Nordestgaard BG. Elevated lipoprotein(a) and risk of aortic valve stenosis in the general population. J Am Coll Cardiol. 2014 Feb 11;63(5):470-7. doi: 10.1016/j.jacc.2013.09.038[↩][↩]
- Thanassoulis G, Campbell CY, Owens DS, et al. CHARGE Extracoronary Calcium Working Group. Genetic associations with valvular calcification and aortic stenosis. N Engl J Med. 2013 Feb 7;368(6):503-12. doi: 10.1056/NEJMoa1109034[↩][↩]
- Capoulade R, Chan KL, Yeang C, Mathieu P, Bossé Y, Dumesnil JG, Tam JW, Teo KK, Mahmut A, Yang X, Witztum JL, Arsenault BJ, Després JP, Pibarot P, Tsimikas S. Oxidized Phospholipids, Lipoprotein(a), and Progression of Calcific Aortic Valve Stenosis. J Am Coll Cardiol. 2015 Sep 15;66(11):1236-1246. doi: 10.1016/j.jacc.2015.07.020[↩][↩]
- Tsimikas S. Lipoprotein(a): novel target and emergence of novel therapies to lower cardiovascular disease risk. Curr Opin Endocrinol Diabetes Obes. 2016 Apr;23(2):157-64. doi: 10.1097/MED.0000000000000237[↩][↩]
- Kronenberg F, Mora S, Stroes ESG, Ference BA, Arsenault BJ, Berglund L, Dweck MR, Koschinsky M, Lambert G, Mach F, McNeal CJ, Moriarty PM, Natarajan P, Nordestgaard BG, Parhofer KG, Virani SS, von Eckardstein A, Watts GF, Stock JK, Ray KK, Tokgözoğlu LS, Catapano AL. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022 Oct 14;43(39):3925-3946. doi: 10.1093/eurheartj/ehac361[↩][↩][↩][↩][↩][↩]
- Kenet G, Lütkhoff LK, Albisetti M, Bernard T, Bonduel M, Brandao L, Chabrier S, Chan A, deVeber G, Fiedler B, Fullerton HJ, Goldenberg NA, Grabowski E, Günther G, Heller C, Holzhauer S, Iorio A, Journeycake J, Junker R, Kirkham FJ, Kurnik K, Lynch JK, Male C, Manco-Johnson M, Mesters R, Monagle P, van Ommen CH, Raffini L, Rostásy K, Simioni P, Sträter RD, Young G, Nowak-Göttl U. Impact of thrombophilia on risk of arterial ischemic stroke or cerebral sinovenous thrombosis in neonates and children: a systematic review and meta-analysis of observational studies. Circulation. 2010 Apr 27;121(16):1838-47. doi: 10.1161/CIRCULATIONAHA.109.913673[↩][↩]
- Strandkjær N, Hansen MK, Nielsen ST, Frikke-Schmidt R, Tybjærg-Hansen A, Nordestgaard BG, Tabor A, Bundgaard H, Iversen K, Kamstrup PR. Lipoprotein(a) Levels at Birth and in Early Childhood: The COMPARE Study. J Clin Endocrinol Metab. 2022 Jan 18;107(2):324-335. doi: 10.1210/clinem/dgab734[↩][↩]
- de Boer LM, Hof MH, Wiegman A, Stroobants AK, Kastelein JJP, Hutten BA. Lipoprotein(a) levels from childhood to adulthood: Data in nearly 3,000 children who visited a pediatric lipid clinic. Atherosclerosis. 2022 May;349:227-232. doi: 10.1016/j.atherosclerosis.2022.03.004[↩][↩]
- Kronenberg F, Utermann G. Lipoprotein(a): resurrected by genetics. J Intern Med. 2013 Jan;273(1):6-30. doi: 10.1111/j.1365-2796.2012.02592.x[↩][↩][↩][↩][↩][↩][↩]
- Kamstrup PR. Lipoprotein(a) and Cardiovascular Disease. Clin Chem. 2021 Jan 8;67(1):154-166. doi: 10.1093/clinchem/hvaa247[↩][↩][↩][↩]
- Coassin S, Kronenberg F. Lipoprotein(a) beyond the kringle IV repeat polymorphism: The complexity of genetic variation in the LPA gene. Atherosclerosis. 2022 May;349:17-35. doi: 10.1016/j.atherosclerosis.2022.04.003[↩][↩][↩][↩]
- Burgess S, Ference BA, Staley JR, Freitag DF, et al. European Prospective Investigation Into Cancer and Nutrition–Cardiovascular Disease (EPIC-CVD) Consortium. Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol. 2018 Jul 1;3(7):619-627. doi: 10.1001/jamacardio.2018.1470[↩][↩][↩][↩][↩][↩]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010 Nov 13;376(9753):1670-81. doi: 10.1016/S0140-6736(10)61350-5[↩]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012 Aug 11;380(9841):581-90. doi: 10.1016/S0140-6736(12)60367-5[↩]
- Silverman MG, Ference BA, Im K, Wiviott SD, Giugliano RP, Grundy SM, Braunwald E, Sabatine MS. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA. 2016 Sep 27;316(12):1289-97. doi: 10.1001/jama.2016.13985[↩]
- Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol. 2017 Feb 14;69(6):692-711. doi: 10.1016/j.jacc.2016.11.042[↩][↩][↩]
- Tsimikas S, Stroes ESG. The dedicated “Lp(a) clinic”: A concept whose time has arrived? Atherosclerosis. 2020 May;300:1-9. doi: 10.1016/j.atherosclerosis.2020.03.003[↩]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188.[↩]
- Wilson, D.P.; Jacobson, T.A.; Jones, P.H.; Koschinsky, M.L.; McNeal, C.J.; Nordestgaard, B.G.; Orringer, C.E. Use of Lipoprotein(a) in clinical practice: A biomarker whose time has come. A scientific statement from the National Lipid Association. J. Clin. Lipidol. 2019, 13, 374–392.[↩]
- Stone NJ, Smith SC Jr, Orringer CE, Rigotti NA, Navar AM, Khan SS, Jones DW, Goldberg R, Mora S, Blaha M, Pencina MJ, Grundy SM. Managing Atherosclerotic Cardiovascular Risk in Young Adults: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022 Mar 1;79(8):819-836. doi: 10.1016/j.jacc.2021.12.016[↩]
- Verbeek, R.; Hoogevee, R.M.; Langste, A.; Stiekema, L.; Verweij, S.; Hoving, G.K.; Wareham, N.J.; Khav, K.; Boekholdt, S.M.; Nordestgaard, B.; et al. Cardiovascular disease risk associated with elevated lipoprotein(a) attenuates at low low-density lipoprotein cholesterol levels in a primary prevention setting. Eur. Heart J. 2018, 39, 2589–2596.[↩]
- Madsen CM, Kamstrup PR, Langsted A, Varbo A, Nordestgaard BG. Lipoprotein(a)-Lowering by 50 mg/dL (105 nmol/L) May Be Needed to Reduce Cardiovascular Disease 20% in Secondary Prevention: A Population-Based Study. Arterioscler Thromb Vasc Biol. 2020 Jan;40(1):255-266. doi: 10.1161/ATVBAHA.119.312951[↩][↩]
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, Graham IM, Halliday A, Landmesser U, Mihaylova B, Pedersen TR, Riccardi G, Richter DJ, Sabatine MS, Taskinen MR, Tokgozoglu L, Wiklund O; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020 Jan 1;41(1):111-188. doi: 10.1093/eurheartj/ehz455. Erratum in: Eur Heart J. 2020 Nov 21;41(44):4255. doi: 10.1093/eurheartj/ehz826[↩][↩][↩][↩][↩][↩][↩]
- Pearson GJ, Thanassoulis G, Anderson TJ, Barry AR, Couture P, Dayan N, Francis GA, Genest J, Grégoire J, Grover SA, Gupta M, Hegele RA, Lau D, Leiter LA, Leung AA, Lonn E, Mancini GBJ, Manjoo P, McPherson R, Ngui D, Piché ME, Poirier P, Sievenpiper J, Stone J, Ward R, Wray W. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can J Cardiol. 2021 Aug;37(8):1129-1150. doi: 10.1016/j.cjca.2021.03.016[↩][↩][↩][↩][↩][↩][↩]
- Waldmann, E.; Parhofer, K.G. Apheresis for severe hypercholesterolaemia and elevated lipoprotein(a). Pathology 2019, 51, 227–232.[↩]
- Sachais, B.S.; Shaz, B.H. Apheresis to mitigate atherosclerotic vascular disease. Am. J. Hypertens. 2018, 31, 945–949.[↩]
- Pokrovsky, S.N.; Afanasieva, O.I.; Ezhov, M.V. Therapeutic apheresis for management of Lp(a) hyperlipoproteinemia. Curr. Atheroscler. Rep. 2020, 22, 68.[↩]
- Mora S, Kamstrup PR, Rifai N, Nordestgaard BG, Buring JE, Ridker PM. Lipoprotein(a) and risk of type 2 diabetes. Clin Chem. 2010 Aug;56(8):1252-60. doi: 10.1373/clinchem.2010.146779[↩]
- Gudbjartsson DF, Thorgeirsson G, Sulem P, et al. Concentration and Risks of Cardiovascular Disease and Diabetes. J Am Coll Cardiol. 2019 Dec 17;74(24):2982-2994. doi: 10.1016/j.jacc.2019.10.019[↩]
- Tolbus A, Mortensen MB, Nielsen SF, Kamstrup PR, Bojesen SE, Nordestgaard BG. Kringle IV Type 2, Not Low Lipoprotein(a), as a Cause of Diabetes: A Novel Genetic Approach Using SNPs Associated Selectively with Lipoprotein(a) Concentrations or with Kringle IV Type 2 Repeats. Clin Chem. 2017 Dec;63(12):1866-1876. doi: 10.1373/clinchem.2017.277103[↩]
- Kamstrup PR, Nordestgaard BG. Lipoprotein(a) concentrations, isoform size, and risk of type 2 diabetes: a Mendelian randomisation study. Lancet Diabetes Endocrinol. 2013 Nov;1(3):220-7. doi: 10.1016/S2213-8587(13)70064-0[↩]
- Langsted A, Nordestgaard BG, Kamstrup PR. Low lipoprotein(a) levels and risk of disease in a large, contemporary, general population study. Eur Heart J. 2021 Mar 21;42(12):1147-1156. doi: 10.1093/eurheartj/ehaa1085[↩]
- Ye Z, Haycock PC, Gurdasani D, Pomilla C, Boekholdt SM, Tsimikas S, Khaw KT, Wareham NJ, Sandhu MS, Forouhi NG. The association between circulating lipoprotein(a) and type 2 diabetes: is it causal? Diabetes. 2014 Jan;63(1):332-342. doi: 10.2337/db13-1144[↩]
- Kaya A, Onat A, Yüksel H, Can G, Yüksel M, Ademoğlu E. Lipoprotein(a)-activated immunity, insulin resistance and new-onset diabetes. Postgrad Med. 2017 Aug;129(6):611-618. doi: 10.1080/00325481.2017.1342508[↩]
- Paige E, Masconi KL, Tsimikas S, Kronenberg F, Santer P, Weger S, Willeit J, Kiechl S, Willeit P. Lipoprotein(a) and incident type-2 diabetes: results from the prospective Bruneck study and a meta-analysis of published literature. Cardiovasc Diabetol. 2017 Mar 21;16(1):38. doi: 10.1186/s12933-017-0520-z[↩][↩]
- Ding L, Song A, Dai M, Xu M, Sun W, Xu B, Sun J, Wang T, Xu Y, Lu J, Wang W, Bi Y, Ning G. Serum lipoprotein (a) concentrations are inversely associated with T2D, prediabetes, and insulin resistance in a middle-aged and elderly Chinese population. J Lipid Res. 2015 Apr;56(4):920-6. doi: 10.1194/jlr.P049015[↩]
- Cegla J, Neely RDG, France M, Ferns G, Byrne CD, Halcox J, Datta D, Capps N, Shoulders C, Qureshi N, Rees A, Main L, Cramb R, Viljoen A, Payne J, Soran H; HEART UK Medical, Scientific and Research Committee. HEART UK consensus statement on Lipoprotein(a): A call to action. Atherosclerosis. 2019 Dec;291:62-70. doi: 10.1016/j.atherosclerosis.2019.10.011. Epub 2019 Oct 14. Erratum in: Atherosclerosis. 2020 Mar;296:48. doi: 10.1016/j.atherosclerosis.2020.01.019[↩][↩][↩][↩]
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019 Jun 18;139(25):e1082-e1143. doi: 10.1161/CIR.0000000000000625 Erratum in: Circulation. 2019 Jun 18;139(25):e1182-e1186. doi: 10.1161/CIR.0000000000000698. Erratum in: Circulation. 2023 Aug 15;148(7):e5. doi: 10.1161/CIR.0000000000001172[↩][↩][↩]
- Trinder M, Paruchuri K, Haidermota S, Bernardo R, Zekavat SM, Gilliland T, Januzzi J Jr, Natarajan P. Repeat Measures of Lipoprotein(a) Molar Concentration and Cardiovascular Risk. J Am Coll Cardiol. 2022 Feb 22;79(7):617-628. doi: 10.1016/j.jacc.2021.11.055. Erratum in: J Am Coll Cardiol. 2022 Aug 9;80(6):651. doi: 10.1016/j.jacc.2022.06.014[↩][↩][↩][↩][↩][↩]
- Nurmohamed NS, Kaiser Y, Schuitema PCE, Ibrahim S, Nierman M, Fischer JC, Chamuleau SAJ, Knaapen P, Stroes ESG. Finding very high lipoprotein(a): the need for routine assessment. Eur J Prev Cardiol. 2022 May 5;29(5):769-776. doi: 10.1093/eurjpc/zwab167[↩]
- FDA approves add-on therapy to lower cholesterol among certain high-risk adults. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-add-therapy-lower-cholesterol-among-certain-high-risk-adults[↩][↩]
- Erqou S, Thompson A, Di Angelantonio E, Saleheen D, Kaptoge S, Marcovina S, Danesh J. Apolipoprotein(a) isoforms and the risk of vascular disease: systematic review of 40 studies involving 58,000 participants. J Am Coll Cardiol. 2010;55(19):2160–2167. doi: 10.1016/j.jacc.2009.10.080[↩]
- Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331–2339. doi: 10.1001/jama.2009.801[↩]
- Kraft HG, Lingenhel A, Kochl S, Hoppichler F, Kronenberg F, Abe A, Muhlberger V, Schonitzer D, Utermann G. Apolipoprotein(a) kringle IV repeat number predicts risk for coronary heart disease. Arterioscler Thromb Vasc Biol. 1996;16(6):713–719. doi: 10.1161/01.ATV.16.6.713[↩]
- Seed M, Hoppichler F, Reaveley D, McCarthy S, Thompson GR, Boerwinkle E, Utermann G. Relation of serum lipoprotein(a) concentration and apolipoprotein(a) phenotype to coronary heart disease in patients with familial hypercholesterolemia. N Engl J Med. 1990;322(21):1494–1499. doi: 10.1056/NEJM199005243222104[↩]
- Virani SS, Brautbar A, Davis BC, Nambi V, Hoogeveen RC, Sharrett AR, Coresh J, Mosley TH, Morrisett JD, Catellier DJ, Folsom AR, Boerwinkle E, Ballantyne CM. Associations between lipoprotein(a) levels and cardiovascular outcomes in black and white subjects: the Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2012 Jan 17;125(2):241-9. doi: 10.1161/CIRCULATIONAHA.111.045120[↩][↩]
- Erhart G, Lamina C, Lehtimäki T, Marques-Vidal P, Kähönen M, Vollenweider P, Raitakari OT, Waeber G, Thorand B, Strauch K, Gieger C, Meitinger T, Peters A, Kronenberg F, Coassin S. Genetic Factors Explain a Major Fraction of the 50% Lower Lipoprotein(a) Concentrations in Finns. Arterioscler Thromb Vasc Biol. 2018 May;38(5):1230-1241. doi: 10.1161/ATVBAHA.118.310865[↩][↩]
- Varvel S, McConnell JP, Tsimikas S. Prevalence of Elevated Lp(a) Mass Levels and Patient Thresholds in 532 359 Patients in the United States. Arterioscler Thromb Vasc Biol. 2016 Nov;36(11):2239-2245. doi: 10.1161/ATVBAHA.116.308011[↩][↩]
- Derby CA, Crawford SL, Pasternak RC, Sowers M, Sternfeld B, Matthews KA. Lipid changes during the menopause transition in relation to age and weight: the Study of Women’s Health Across the Nation. Am J Epidemiol. 2009 Jun 1;169(11):1352-61. doi: 10.1093/aje/kwp043[↩][↩][↩][↩][↩][↩]
- Utermann G. The mysteries of lipoprotein(a). Science. 1989 Nov 17;246(4932):904-10. doi: 10.1126/science.2530631[↩]
- Ellis KL, Boffa MB, Sahebkar A, Koschinsky ML, Watts GF. The renaissance of lipoprotein(a): Brave new world for preventive cardiology? Prog Lipid Res. 2017 Oct;68:57-82. doi: 10.1016/j.plipres.2017.09.001[↩][↩]
- Marcovina SM, Albers JJ, Gabel B, Koschinsky ML, Gaur VP. Effect of the number of apolipoprotein(a) kringle 4 domains on immunochemical measurements of lipoprotein(a). Clin Chem. 1995 Feb;41(2):246-55.[↩][↩]
- Marcovina SM, Albers JJ. Lipoprotein (a) measurements for clinical application. J Lipid Res. 2016 Apr;57(4):526-37. doi: 10.1194/jlr.R061648[↩][↩]
- Kronenberg F. Human Genetics and the Causal Role of Lipoprotein(a) for Various Diseases. Cardiovasc Drugs Ther. 2016 Feb;30(1):87-100. doi: 10.1007/s10557-016-6648-3[↩]
- Gabel BR, Koschinsky MI. Analysis of the proteolytic activity of a recombinant form of apolipoprotein(a). Biochemistry. 1995 Dec 5;34(48):15777-84. doi: 10.1021/bi00048a023[↩]
- Liu T, Yoon WS, Lee SR. Recent Updates of Lipoprotein(a) and Cardiovascular Disease. Chonnam Med J. 2021 Jan;57(1):36-43. doi: 10.4068/cmj.2021.57.1.36[↩]
- Lamina C, Kronenberg F; Lp(a)-GWAS-Consortium. Estimation of the Required Lipoprotein(a)-Lowering Therapeutic Effect Size for Reduction in Coronary Heart Disease Outcomes: A Mendelian Randomization Analysis. JAMA Cardiol. 2019 Jun 1;4(6):575-579. doi: 10.1001/jamacardio.2019.1041[↩]
- Assessing the Impact of Lipoprotein (a) Lowering With Pelacarsen (TQJ230) on Major Cardiovascular Events in Patients With CVD (Lp(a)HORIZON). https://clinicaltrials.gov/study/NCT04023552[↩]
- Blood Cholesterol Diagnosis. https://www.nhlbi.nih.gov/health/blood-cholesterol/diagnosis[↩][↩]
- Kraft HG, Köchl S, Menzel HJ, Sandholzer C, Utermann G. The apolipoprotein (a) gene: a transcribed hypervariable locus controlling plasma lipoprotein (a) concentration. Hum Genet. 1992 Nov;90(3):220-30. doi: 10.1007/BF00220066[↩]
- Boerwinkle E, Leffert CC, Lin J, Lackner C, Chiesa G, Hobbs HH. Apolipoprotein(a) gene accounts for greater than 90% of the variation in plasma lipoprotein(a) concentrations. J Clin Invest. 1992 Jul;90(1):52-60. doi: 10.1172/JCI115855[↩]
- Marcovina SM, Viney NJ, Hughes SG, Xia S, Witztum JL, et al. Temporal variability in lipoprotein(a) levels in patients enrolled in the placebo arms of IONIS-APO(a)Rx and IONIS-APO(a)-LRx antisense oligonucleotide clinical trials. J Clin Lipidol. 2018;12:122–129.:e2. doi: 10.1016/j.jacl.2017.10.024[↩][↩]
- Koschinsky ML, Marcovina SM, May LF, Gabel BR. Analysis of the mechanism of lipoprotein(a) assembly. Clin Genet. 1997;52(5):338-346. doi: 10.1111/j.1399-0004.1997.tb04351.x[↩]
- Varvel S, McConnell JP, Tsimikas S. Prevalence of Elevated Lp(a) Mass Levels and Patient Thresholds in 532 359 Patients in the United States. Arterioscler Thromb Vasc Biol. 2016 Nov;36(11):2239-2245. https://doi.org/10.1161/ATVBAHA.116.308011[↩]
- Langsted A, Kamstrup PR, Benn M, Tybjærg-Hansen A, Nordestgaard BG. High lipoprotein(a) as a possible cause of clinical familial hypercholesterolaemia: a prospective cohort study. Lancet Diabetes Endocrinol. 2016 Jul;4(7):577-87. doi: 10.1016/S2213-8587(16)30042-0[↩]
- Kraft HG, Lingenhel A, Pang RW, Delport R, Trommsdorff M, et al. Frequency distributions of apolipoprotein(a) kringle IV repeat alleles and their effects on lipoprotein(a) levels in Caucasian, Asian, and African populations: the distribution of null alleles is non-random. Eur J Hum Genet. 1996;4:74–87. doi: 10.1159/000472175[↩][↩]
- Mehta A, Jain V, Saeed A, Saseen JJ, Gulati M, et al. Lipoprotein(a) and ethnicities. Atherosclerosis. 2022;349:42–52. doi: 10.1016/j.atherosclerosis.2022.04.005[↩]
- Sandholzer C, Hallman DM, Saha N, Sigurdsson G, Lackner C, et al. Effects of the apolipoprotein(a) size polymorphism on the lipoprotein(a) concentration in 7 ethnic groups. Hum Genet. 1991;86:607–614. doi: 10.1007/BF00201550[↩]
- Lee S, Prasad A, Choi Y, Xing C, Clopton P, et al. LPA gene, ethnicity, and cardiovascular events. Circulation. 2017;135:251–263. doi: 10.1161/CIRCULATIUNAHA.116.024611[↩]
- Deo RC, Wilson JG, Xing C, Lawson K, Kao WHL, et al. Single-nucleotide polymorphisms in LPA explain most of the ancestry-specific variation in Lp(a) levels in African Americans. PLoS One. 2011;6:e14581. doi: 10.1371/journal.pone.0014581[↩]
- Mukamel RE, Handsaker RE, Sherman MA, Barton AR, Zheng Y, et al. Protein-coding repeat polymorphisms strongly shape diverse human phenotypes. Science. 2021;373:1499–1505. doi: 10.1126/science.abg8289[↩][↩]
- Coassin S, Erhart G, Weissensteiner H, Araújo MEGde, Lamina C, et al. A novel but frequent variant in LPA KIV-2 is associated with a pronounced Lp(a) and cardiovascular risk reduction. Eur Heart J. 2017;38:1823–1831. doi: 10.1093/eurheartj/ehx174[↩]
- Schachtl-Riess JF, Kheirkhah A, Grüneis R, Di Maio S, Schoenherr S, et al. Frequent LPA KIV-2 variants lower lipoprotein(a) concentrations and protect against coronary artery disease. J Am Coll Cardiol. 2021;78:437–449. doi: 10.1016/j.jacc.2021.05.037[↩]
- Kraft HG, Windegger M, Menzel HJ, Utermann G. Significant impact of the + 93 C/T polymorphism in the apolipoprotein(a) gene on Lp(a) concentrations in Africans but not in Caucasians: confounding effect of linkage disequilibrium. Hum Mol Genet. 1998;7:257–264. doi: 10.1093/hmg/7.2.257[↩]
- Enkhmaa B, Anuurad E, Berglund L. Lipoprotein (a): impact by ethnicity and environmental and medical conditions. J Lipid Res. 2016;57:1111–1125. doi: 10.1194/jlr.R051904[↩]
- Noureen A, Ronke C, Khalifa M, Halbwax M, Fischer A, et al. Significant differentiation in the apolipoprotein(a)/lipoprotein(a) trait between chimpanzees from Western and Central Africa. Am J Primatol. 2017;79:e22683. doi: 10.1002/ajp.22683[↩]
- Ebbeling CB, Knapp A, Johnson A, Wong JMW, Greco KF, Ma C, Mora S, Ludwig DS. Effects of a low-carbohydrate diet on insulin-resistant dyslipoproteinemia-a randomized controlled feeding trial. Am J Clin Nutr. 2022 Jan 11;115(1):154-162. doi: 10.1093/ajcn/nqab287. Erratum in: Am J Clin Nutr. 2022 Jan 11;115(1):310. doi: 10.1093/ajcn/nqab372[↩][↩]
- Austin MA, Sandholzer C, Selby JV, Newman B, Krauss RM, Utermann G. Lipoprotein(a) in women twins: heritability and relationship to apolipoprotein(a) phenotypes. Am J Hum Genet. 1992 Oct;51(4):829-40. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1682765/pdf/ajhg00068-0148.pdf[↩]
- Lamon-Fava S, Jimenez D, Christian JC, Fabsitz RR, Reed T, Carmelli D, Castelli WP, Ordovas JM, Wilson PW, Schaefer EJ. The NHLBI Twin Study: heritability of apolipoprotein A-I, B, and low density lipoprotein subclasses and concordance for lipoprotein(a). Atherosclerosis. 1991 Nov;91(1-2):97-106. doi: 10.1016/0021-9150(91)90191-5[↩]
- Langsted A, Kamstrup PR, Nordestgaard BG. Lipoprotein(a): fasting and nonfasting levels, inflammation, and cardiovascular risk. Atherosclerosis. 2014 May;234(1):95-101. doi: 10.1016/j.atherosclerosis.2014.01.049[↩][↩][↩]
- Enkhmaa B, Anuurad E, Berglund L. Lipoprotein (a): impact by ethnicity and environmental and medical conditions. J Lipid Res. 2016 Jul;57(7):1111-25. doi: 10.1194/jlr.R051904[↩][↩]
- Kotwal A, Cortes T, Genere N, Hamidi O, Jasim S, Newman CB, Prokop LJ, Murad MH, Alahdab F. Treatment of Thyroid Dysfunction and Serum Lipids: A Systematic Review and Meta-analysis. J Clin Endocrinol Metab. 2020 Dec 1;105(12):dgaa672. doi: 10.1210/clinem/dgaa672[↩][↩][↩][↩]
- Edén S, Wiklund O, Oscarsson J, Rosén T, Bengtsson BA. Growth hormone treatment of growth hormone-deficient adults results in a marked increase in Lp(a) and HDL cholesterol concentrations. Arterioscler Thromb. 1993 Feb;13(2):296-301. doi: 10.1161/01.atv.13.2.296[↩][↩][↩]
- Zechner R, Desoye G, Schweditsch MO, Pfeiffer KP, Kostner GM. Fluctuations of plasma lipoprotein-A concentrations during pregnancy and post partum. Metabolism. 1986 Apr;35(4):333-6. doi: 10.1016/0026-0495(86)90150-2[↩][↩][↩]
- Sattar N, Clark P, Greer IA, Shepherd J, Packard CJ. Lipoprotein (a) levels in normal pregnancy and in pregnancy complicated with pre-eclampsia. Atherosclerosis. 2000 Feb;148(2):407-11. doi: 10.1016/s0021-9150(99)00296-8[↩][↩][↩]
- Salpeter SR, Walsh JM, Ormiston TM, Greyber E, Buckley NS, Salpeter EE. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diabetes Obes Metab. 2006 Sep;8(5):538-54. doi: 10.1111/j.1463-1326.2005.00545.x[↩][↩][↩]
- Kronenberg F. Causes and consequences of lipoprotein(a) abnormalities in kidney disease. Clin Exp Nephrol. 2014 Apr;18(2):234-7. doi: 10.1007/s10157-013-0875-8[↩][↩][↩]
- Hopewell JC, Haynes R, Baigent C. The role of lipoprotein (a) in chronic kidney disease. J Lipid Res. 2018 Apr;59(4):577-585. doi: 10.1194/jlr.R083626[↩][↩][↩]
- Kronenberg F, König P, Lhotta K, Ofner D, Sandholzer C, Margreiter R, Dosch E, Utermann G, Dieplinger H. Apolipoprotein(a) phenotype-associated decrease in lipoprotein(a) plasma concentrations after renal transplantation. Arterioscler Thromb. 1994 Sep;14(9):1399-404. doi: 10.1161/01.atv.14.9.1399[↩][↩]
- Missala I, Kassner U, Steinhagen-Thiessen E. A Systematic Literature Review of the Association of Lipoprotein(a) and Autoimmune Diseases and Atherosclerosis. Int J Rheumatol. 2012;2012:480784. doi: 10.1155/2012/480784[↩][↩][↩]
- Mooser V, Berger MM, Tappy L, Cayeux C, Marcovina SM, Darioli R, Nicod P, Chioléro R. Major reduction in plasma Lp(a) levels during sepsis and burns. Arterioscler Thromb Vasc Biol. 2000 Apr;20(4):1137-42. doi: 10.1161/01.atv.20.4.1137[↩][↩][↩]
- Schultz O, Oberhauser F, Saech J, Rubbert-Roth A, Hahn M, Krone W, Laudes M. Effects of inhibition of interleukin-6 signalling on insulin sensitivity and lipoprotein (a) levels in human subjects with rheumatoid diseases. PLoS One. 2010 Dec 13;5(12):e14328. doi: 10.1371/journal.pone.0014328[↩][↩][↩]
- Enkhmaa B, Petersen KS, Kris-Etherton PM, Berglund L. Diet and Lp(a): Does Dietary Change Modify Residual Cardiovascular Risk Conferred by Lp(a)? Nutrients. 2020 Jul 7;12(7):2024. doi: 10.3390/nu12072024[↩][↩][↩]
- Kronenberg F, Lingenhel A, Lhotta K, Rantner B, Kronenberg MF, König P, Thiery J, Koch M, von Eckardstein A, Dieplinger H. The apolipoprotein(a) size polymorphism is associated with nephrotic syndrome. Kidney Int. 2004 Feb;65(2):606-12. doi: 10.1111/j.1523-1755.2004.00418.x[↩][↩]
- Kronenberg F, König P, Neyer U, Auinger M, Pribasnig A, Lang U, Reitinger J, Pinter G, Utermann G, Dieplinger H. Multicenter study of lipoprotein(a) and apolipoprotein(a) phenotypes in patients with end-stage renal disease treated by hemodialysis or continuous ambulatory peritoneal dialysis. J Am Soc Nephrol. 1995 Jul;6(1):110-20. doi: 10.1681/ASN.V61110[↩][↩][↩]
- Stenvinkel P, Berglund L, Heimbürger O, Pettersson E, Alvestrand A. Lipoprotein(a) in nephrotic syndrome. Kidney Int. 1993 Nov;44(5):1116-23. doi: 10.1038/ki.1993.357[↩][↩]
- Dieplinger H, Lackner C, Kronenberg F, Sandholzer C, Lhotta K, Hoppichler F, Graf H, König P. Elevated plasma concentrations of lipoprotein(a) in patients with end-stage renal disease are not related to the size polymorphism of apolipoprotein(a). J Clin Invest. 1993 Feb;91(2):397-401. doi: 10.1172/JCI116213[↩][↩]
- Feely J, Barry M, Keeling PW, Weir DG, Cooke T. Lipoprotein(a) in cirrhosis. BMJ. 1992 Feb 29;304(6826):545-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1881428/pdf/bmj00062-0033.pdf[↩][↩]
- Reyes-Soffer G, Westerterp M. Beyond Lipoprotein(a) plasma measurements: Lipoprotein(a) and inflammation. Pharmacol Res. 2021 Jul;169:105689. doi: 10.1016/j.phrs.2021.105689[↩][↩]
- Müller N, Schulte DM, Türk K, Freitag-Wolf S, Hampe J, Zeuner R, Schröder JO, Gouni-Berthold I, Berthold HK, Krone W, Rose-John S, Schreiber S, Laudes M. IL-6 blockade by monoclonal antibodies inhibits apolipoprotein (a) expression and lipoprotein (a) synthesis in humans. J Lipid Res. 2015 May;56(5):1034-42. doi: 10.1194/jlr.P052209[↩][↩]
- Henriksson P, Angelin B, Berglund L. Hormonal regulation of serum Lp (a) levels. Opposite effects after estrogen treatment and orchidectomy in males with prostatic carcinoma. J Clin Invest. 1992 Apr;89(4):1166-71. doi: 10.1172/JCI115699[↩]
- Walsh BW, Kuller LH, Wild RA, Paul S, Farmer M, Lawrence JB, Shah AS, Anderson PW. Effects of raloxifene on serum lipids and coagulation factors in healthy postmenopausal women. JAMA. 1998 May 13;279(18):1445-51. doi: 10.1001/jama.279.18.1445[↩]
- Kronenberg F, Kuen E, Ritz E, Junker R, König P, Kraatz G, Lhotta K, Mann JFE, Müller GA, Neyer U, Riegel W, Riegler P, Schwenger V, VON Eckardstein A. Lipoprotein(a) serum concentrations and apolipoprotein(a) phenotypes in mild and moderate renal failure. J Am Soc Nephrol. 2000 Jan;11(1):105-115. doi: 10.1681/ASN.V111105[↩]
- Jung I, Kwon H, Park SE, Park CY, Lee WY, Oh KW, Park SW, Rhee EJ. Serum lipoprotein(a) levels and insulin resistance have opposite effects on fatty liver disease. Atherosclerosis. 2020 Sep;308:1-5. doi: 10.1016/j.atherosclerosis.2020.07.020[↩]
- Kraft HG, Menzel HJ, Hoppichler F, Vogel W, Utermann G. Changes of genetic apolipoprotein phenotypes caused by liver transplantation. Implications for apolipoprotein synthesis. J Clin Invest. 1989 Jan;83(1):137-42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC303653/pdf/jcinvest00082-0149.pdf[↩]
- Holm S, Oma I, Hagve TA, Saatvedt K, Brosstad F, Mikkelsen K, Rydningen H, Risnes I, Almdahl SM, Ueland T, Aukrust P, Halvorsen B, Hollan I. Levels of Lipoprotein (a) in patients with coronary artery disease with and without inflammatory rheumatic disease: a cross-sectional study. BMJ Open. 2019 May 10;9(5):e030651. doi: 10.1136/bmjopen-2019-030651[↩]
- Enkhmaa B, Anuurad E, Zhang W, Li CS, Kaplan R, Lazar J, Merenstein D, Karim R, Aouizerat B, Cohen M, Butler K, Pahwa S, Ofotokun I, Adimora AA, Golub E, Berglund L. Effect of antiretroviral therapy on allele-associated Lp(a) level in women with HIV in the Women’s Interagency HIV Study. J Lipid Res. 2018 Oct;59(10):1967-1976. doi: 10.1194/jlr.P084517[↩]
- Enkhmaa B, Anuurad E, Zhang W, Abbuthalha A, Li XD, Dotterweich W, Pollard RB, Asmuth DM, Berglund L. HIV disease activity as a modulator of lipoprotein(a) and allele-specific apolipoprotein(a) levels. Arterioscler Thromb Vasc Biol. 2013 Feb;33(2):387-92. doi: 10.1161/ATVBAHA.112.300125[↩]
- Willeit P, Ridker PM, Nestel PJ, Simes J, Tonkin AM, Pedersen TR, Schwartz GG, Olsson AG, Colhoun HM, Kronenberg F, Drechsler C, Wanner C, Mora S, Lesogor A, Tsimikas S. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: individual patient-data meta-analysis of statin outcome trials. Lancet. 2018 Oct 13;392(10155):1311-1320. doi: 10.1016/S0140-6736(18)31652-0[↩][↩][↩]
- Tsimikas S, Gordts PLSM, Nora C, Yeang C, Witztum JL. Statin therapy increases lipoprotein(a) levels. Eur Heart J. 2020 Jun 21;41(24):2275-2284. doi: 10.1093/eurheartj/ehz310[↩][↩]
- de Boer LM, Oorthuys AOJ, Wiegman A, Langendam MW, Kroon J, Spijker R, Zwinderman AH, Hutten BA. Statin therapy and lipoprotein(a) levels: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022 May 5;29(5):779-792. doi: 10.1093/eurjpc/zwab171[↩][↩]
- Wu XM, Broadwin R, Basu R, Malig B, Ebisu K, Gold EB, Qi L, Derby C, Park SK, Green S. Associations between fine particulate matter and changes in lipids/lipoproteins among midlife women. Sci Total Environ. 2019 Mar 1;654:1179-1186. doi: 10.1016/j.scitotenv.2018.11.149[↩]
- Nordestgaard BG, Chapman MJ, Ray K, Boren J, Andreotti F, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31:2844–2853. doi: 10.1093/eurheartj/ehq386[↩]
- Koschinsky ML, Boffa MB. Oxidized phospholipid modification of lipoprotein (a): epidemiology, biochemistry and pathophysiology. Atherosclerosis. 2022;349:92–100. doi: 10.1016/j.atherosclerosis.2022.04.001[↩]
- High lipoprotein (a). https://www.heartuk.org.uk/genetic-conditions/high-lipoproteina[↩]
- National Cholesterol Education Program. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. https://www.nhlbi.nih.gov/files/docs/guidelines/atp3xsum.pdf[↩]
- Physical Activity Guidelines for Americans. https://health.gov/our-work/nutrition-physical-activity/physical-activity-guidelines[↩]
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008 Nov 20;359(21):2195-207. doi: 10.1056/NEJMoa0807646[↩]
- O’Donoghue ML, Fazio S, Giugliano RP, Stroes ESG, Kanevsky E, Gouni-Berthold I, Im K, Lira Pineda A, Wasserman SM, Češka R, Ezhov MV, Jukema JW, Jensen HK, Tokgözoğlu SL, Mach F, Huber K, Sever PS, Keech AC, Pedersen TR, Sabatine MS. Lipoprotein(a), PCSK9 Inhibition, and Cardiovascular Risk. Circulation. 2019 Mar 19;139(12):1483-1492. doi: 10.1161/CIRCULATIONAHA.118.037184[↩]
- Szarek M, Bittner VA, Aylward P, Baccara-Dinet M, Bhatt DL, Diaz R, Fras Z, Goodman SG, Halvorsen S, Harrington RA, Jukema JW, Moriarty PM, Pordy R, Ray KK, Sinnaeve P, Tsimikas S, Vogel R, White HD, Zahger D, Zeiher AM, Steg PG, Schwartz GG; ODYSSEY OUTCOMES Investigators. Lipoprotein(a) lowering by alirocumab reduces the total burden of cardiovascular events independent of low-density lipoprotein cholesterol lowering: ODYSSEY OUTCOMES trial. Eur Heart J. 2020 Nov 21;41(44):4245-4255. doi: 10.1093/eurheartj/ehaa649[↩]
- Thompson GR; HEART-UK LDL Apheresis Working Group. Recommendations for the use of LDL apheresis. Atherosclerosis. 2008 Jun;198(2):247-55. doi: 10.1016/j.atherosclerosis.2008.02.009[↩]
- Tsimikas S. Potential Causality and Emerging Medical Therapies for Lipoprotein(a) and Its Associated Oxidized Phospholipids in Calcific Aortic Valve Stenosis. Circ Res. 2019 Feb;124(3):405-415. doi: 10.1161/CIRCRESAHA.118.313864[↩]
- Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, Tardif JC, Baum SJ, Steinhagen-Thiessen E, Shapiro MD, Stroes ES, Moriarty PM, Nordestgaard BG, Xia S, Guerriero J, Viney NJ, O’Dea L, Witztum JL; AKCEA-APO(a)-LRx Study Investigators. Lipoprotein(a) Reduction in Persons with Cardiovascular Disease. N Engl J Med. 2020 Jan 16;382(3):244-255. doi: 10.1056/NEJMoa1905239[↩]
- Koren MJ, Moriarty PM, Baum SJ, Neutel J, Hernandez-Illas M, Weintraub HS, Florio M, Kassahun H, Melquist S, Varrieur T, Haldar SM, Sohn W, Wang H, Elliott-Davey M, Rock BM, Pei T, Homann O, Hellawell J, Watts GF. Preclinical development and phase 1 trial of a novel siRNA targeting lipoprotein(a). Nat Med. 2022 Jan;28(1):96-103. doi: 10.1038/s41591-021-01634-w[↩]
- Nissen SE, Wolski K, Balog C, Swerdlow DI, Scrimgeour AC, Rambaran C, Wilson RJ, Boyce M, Ray KK, Cho L, Watts GF, Koren M, Turner T, Stroes ES, Melgaard C, Campion GV. Single Ascending Dose Study of a Short Interfering RNA Targeting Lipoprotein(a) Production in Individuals With Elevated Plasma Lipoprotein(a) Levels. JAMA. 2022 May 3;327(17):1679-1687. doi: 10.1001/jama.2022.5050[↩]
- Santos RD, Raal FJ, Catapano AL, Witztum JL, Steinhagen-Thiessen E, Tsimikas S. Mipomersen, an antisense oligonucleotide to apolipoprotein B-100, reduces lipoprotein(a) in various populations with hypercholesterolemia: results of 4 phase III trials. Arterioscler Thromb Vasc Biol. 2015 Mar;35(3):689-99. doi: 10.1161/ATVBAHA.114.304549[↩][↩]
- Thomas GS, Cromwell WC, Ali S, Chin W, Flaim JD, Davidson M. Mipomersen, an apolipoprotein B synthesis inhibitor, reduces atherogenic lipoproteins in patients with severe hypercholesterolemia at high cardiovascular risk: a randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol. 2013 Dec 10;62(23):2178-84. doi: 10.1016/j.jacc.2013.07.081[↩]
- Raal FJ, Santos RD, Blom DJ, Marais AD, Charng MJ, Cromwell WC, Lachmann RH, Gaudet D, Tan JL, Chasan-Taber S, Tribble DL, Flaim JD, Crooke ST. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010 Mar 20;375(9719):998-1006. doi: 10.1016/S0140-6736(10)60284-X[↩]
- Kassner U, Schlabs T, Rosada A, Steinhagen-Thiessen E. Lipoprotein(a)–An independent causal risk factor for cardiovascular disease and current therapeutic options. Atheroscler Suppl. 2015 May;18:263-7. doi: 10.1016/j.atherosclerosissup.2015.02.039[↩]





{kind=link}