
Contents
What is marasmus
Marasmus is known as the wasting syndrome (malnutrition without edema). Marasmus is one of the 3 forms of serious protein-energy malnutrition. The other 2 forms are kwashiorkor and marasmic kwashiorkor 1. These forms of serious protein-energy malnutrition represent a group of pathologic conditions associated with a nutritional and energy deficit occurring mainly in young children from developing countries at the time of weaning. Children typically have a depletion of body fat stores, low weight for height, and reduced mid-upper arm circumference 2. Other features of marasmus can include thin, dry skin; a head that appears large relative to the body; an emaciated, weak appearance; bradycardia; hypotension; hypothermia; and thin, shrunken arms, thighs, and buttocks with redundant skin folds 2.
Marasmus is a condition primarily caused by a deficiency in calories and energy, whereas kwashiorkor indicates an associated protein deficiency, resulting in an edematous appearance. Marasmic kwashiorkor indicates that, in practice, separating these entities conclusively is difficult; this term indicates a condition that has features of both 3. These conditions are frequently associated with infections, mainly gastrointestinal. The reasons for a progression of nutritional deficit into marasmus rather than kwashiorkor are unclear and cannot be solely explained by the composition of the deficient diet (i.e, a diet deficient in energy for marasmus and a diet deficient in protein for kwashiorkor) 1. The study of these phenomena is considerably limited by the lack of an appropriate animal model. Unfortunately, many authors combine these entities into one, thus precluding a better understanding of the differences between these clinical conditions.
Marasmus is rarely reported in American children. In 1995, 228 deaths were attributed to marasmus in the United States. Most of these deaths were in elderly adults, and only 3 occurred in children. However, these data do not include deaths associated with marasmus complicating anorexia nervosa.
According to the UNICEF 2016 Global Nutrition Report 4, the United States had a 0.5% overall prevalence of marasmus. Incidence of nonfatal marasmus is unclear in the United States because most patients have an underlying condition, and marasmus is not reported as an admission or discharge diagnosis. However, among hospitalized children, especially those with chronic illnesses, the prevalence is certainly higher. A report from a tertiary care center in Massachusetts reported prevalence rates of severe (1.3%), moderate (5.8%), and mild (17.4%) acute protein-energy malnutrition in hospitalized children, based on the Waterlow criteria 5. In the same cohort, chronic protein-energy malnutrition (deficits in height for age) was found to be severe (5.1%), moderate (7.7%), and mild (14.5%).
Acute (33%) and chronic (64%) malnutrition, based on comparing weight and height with controls, was found among a cohort of 160 children hospitalized with congenital heart disease in a regional pediatric cardiothoracic center at the University of Michigan 6. Malnutrition was inversely correlated with age and was present in 80% of the hospitalized infants. These studies, as well as reports from Western Europe, suggest that marasmus is underappreciated amongst chronically ill children in the United States 7.
Marasmus is more frequent in children younger than 5 years because this period is characterized by increased energy needs and increased susceptibility to viral and bacterial infections. Weaning, which occurs during this period, is often complicated by factors such as geography (eg, drought, poor soil productivity), economy (eg, illiteracy, unemployment), hygiene (eg, access to quality water), public health (eg, number of nurses is more than number of physicians), and culture and dietetics (eg, intrafamily distribution of high-nutrition foods).
According to 2015 World Health Organization data, 92 million children under five years old (15%) were underweight in less developed regions. Recent data provides a relatively small degree of optimism as the WHO reports that worldwide, the percentage of children under five years old who were underweight declined from 25% to 14% between 1990 and 2015. A 2013 guideline by the WHO reported that severe acute malnutrition affects nearly 20 million preschool-age children, mostly from the WHO African Region and South-East Asia Region and that malnutrition is a significant factor in approximately one third of the 8 million deaths in children who are under 5 years of age worldwide 8.
What causes marasmus
Several factors can lead to marasmus. Their relative importance varies between children and between parts of the world. For example, undernutrition associated with war, inappropriate weaning by a young mother, and precipitating infections can influence incidence of marasmus.
- Nutrition: In many low-income countries, food variety is limited and results in mineral and vitamin insufficiencies. In cases of anorexia, which are generally associated with infection, the total energy intake becomes insufficient. Therefore, any nutrient deficiency can lead to marasmus because appropriate growth can only be ensured by a balanced diet. Therefore, marasmus can be described as multiple-deficiency malnutrition.
- Infections: Associated infections often trigger, aggravate, or combine with marasmus. However, evidence exists that this association may have been overestimated. For example, in rural Senegal, the growth of children with or without infections, such as pertussis and measles, was similar. In contrast, the importance of diarrhea in triggering malnutrition through anorexia and weight loss has been well established. Infectious diseases more frequently associated with energy-protein malnutrition are gastroenteritis, respiratory infections, measles, and pertussis. HIV also plays an increasingly significant role in some countries.
- Socioeconomic factors: Frequently, malnutrition appears during weaning, especially if weaning is suboptimal, as can occur with a low-variety diet, or if weaning foods are introduced only in children older than 8-10 months. The WHO recommends exclusive breastfeeding until age 6 months; then, the introduction of various additional foods is recommended. The socioeconomic environment is often critical in the choice of the weaning food used. For example, in northern Senegal, available foods are often limited to grains, vegetables, and a small amount of fish. Milk and meat are rare. In this region, malnutrition and diarrhea are frequent. In contrast, in the nearby Sahelien pastures where milk and meat are the main foods, diarrhea is less frequent, and malnutrition is rare.
- Other socioeconomic factors: Other factors, such as the famines associated with climatic disasters or more often with political events and war (as has been the case in east Africa), can play a critical role. The sociofamilial environment can also be important, and children of young or inexperienced mothers, twins, or female infants can be at a higher risk in some parts of the world.
Summary: Marasmus, and malnutrition in general, represents multiple deficiencies, and multiple etiologies. Therefore, epidemiological, public health, and therapeutic approaches must be comprehensive. Population-based interventions limited to the supplementation of one nutrient have often been unsuccessful.
Marasmus is most frequently associated with acute infections (e.g., gastroenteritis, respiratory illnesses, measles), chronic illnesses (e.g., tuberculosis, HIV infection) or drastic natural or man made conditions (e.g., floods, droughts, civil war). Socioeconomic factors including access to a kitchen/toilet and parental education are also significantly associated with the rate of malnutrition. Specifically, poverty and hygiene related issues contribute to stunting and to being underweight 9.
The clinical consequences of marasmus can be considered as an evolving adaptation in a child facing an insufficient energy intake. Marasmus always results from a negative energy balance. The imbalance can result from a decreased energy intake, an increased loss of ingested calories (e.g., vomiting, diarrhea, burns), an increased energy expenditure, or combinations of these factors, such as is observed in acute or chronic diseases. Children adapt to an energy deficiency with a decrease in physical activity, lethargy, a decrease in basal energy metabolism, slowing of growth, and, finally, weight loss.
Pathophysiological changes associated with nutritional and energy deficits can be described as (1) body composition changes, (2) metabolic changes, and (3) anatomic changes.
Body Composition
- Body mass: Body mass is significantly decreased in a heterogeneous way.
- Fat mass: Fat stores can decrease to as low as 5% of the total body weight and can be macroscopically undetectable. The remaining fat is usually stored in the liver, giving a paradoxical appearance of a fatty liver. Although this is often observed in kwashiorkor, it also occurs to a lesser extent in marasmus. A study from Nigeria examined serum lipids in malnourished children 10. These authors found that total cholesterol, low density lipoprotein cholesterol, and high density lipoprotein cholesterol levels were significantly higher in children with kwashiorkor than in those with marasmus.
- Total body water: The proportion of water content in the body increases with the increased seriousness of protein-energy malnutrition (marasmus or kwashiorkor) and is associated with the loss of fat mass, which is poor in water. The proportion of extracellular water also increases, often resulting in edema. Edema is significant in kwashiorkor but can also be present in marasmus or in the frequently encountered mixed forms of protein-energy malnutrition. The increase in extracellular water is proportional to the increase in the total body water. During the first days of therapy, part of the extracellular water shifts to the intracellular compartment and part of it is lost in the urine, resulting in the observed initial weight loss with treatment.
- Protein mass: Mainly represented by muscle and some organs (e.g., heart), protein mass can decrease as much as 30% in the most serious forms. The muscle fibers are thin with loss of striation. Muscle cells are atrophic, and muscle tissue is infiltrated with fat and fibrous tissue. Total recovery is long but appears to be possible.
- Other organ mass: The brain, skeleton, and kidney are preserved, whereas the liver, heart, pancreas, and digestive tract are first affected.
- Pediatric and adult physiologic change: Finally, physiologic changes are different in infants and children when compared with adults. For example, infants with marasmus have an increased tendency to hypothermia and hypoglycemia, requiring the frequent administration of small meals. This can be explained by the body composition imbalance of children with marasmus in favor of high-energy–consuming organs, such as the brain and kidney, compared with energy-storage organs, such as muscle and fat.
- Assessment of fat and muscle mass: As described below, assessment of the fat and muscle mass loss can be clinically performed by measuring arm circumference or skinfold thickness, such as triceps skinfold. The diagram illustrates the validity of this assessment method. Mid-arm circumference is still an accurate way of measuring severity of malnutrition, although there is not a linear correlation with fat/muscle mass. Because arm circumference is relatively constant in healthy children aged 1-5 years, it roughly represents a general assessment of nutritional status. Mid-arm circumference of < 11cm indicates severe malnutrition in infants from 1-6 months of age 11.
Minerals and Vitamins
- Potassium: Potassium is the electrolyte most studied in marasmus. Total body potassium deficit is associated with decreased muscle mass, poor intake, and digestive losses. This potassium deficit, which can reach 15 mEq/kg, contributes to hypotonia, apathy, and impaired cardiac function.
- Other electrolytes: Plasma sodium concentration is generally within the reference range, but it can be low, which is then a sign of a poor prognosis. However, intracellular sodium level is elevated in the brain, muscle, and red and white blood cells, explaining the sodium excretion in the first days of recovery.
- Other minerals: A deficit in calcium, phosphorus, and magnesium stores is also observed. Iron deficiency anemia is consistently observed in marasmus. However, in the most serious forms, iron accumulates in the liver, most likely because of the deficit in transport protein. These patients are at higher risk of mortality; therefore, iron is supplemented only after the acute recovery phase is completed. Zinc, selenium, and magnesium are more significantly reduced in kwashiorkor but are also constantly deficient in marasmus. Several studies have shown improved recovery from malnutrition and decreased mortality with supplementation of these 3 micronutrients. A Cochrane review 12 concluded that zinc supplementation is clearly of benefit in children aged 6 months or older with diarrheal diseases in areas where these conditions are an important cause of childhood mortality.
- Vitamins: Both fat-soluble vitamins (ie, A, D, E, K) and water-soluble vitamins (eg, B-6, B-12, folic acid) must be systematically administered. Vitamin A is essential to retinal function, has a trophic effect on epithelial tissues, and plays a major role as an antioxidant agent. Vitamin A deficit affects visual function (eg, conjunctivitis, corneal ulcer, night blindness, total blindness) and digestive, respiratory, and urinary functions. Furthermore, vitamin A supplementation programs have resulted in decreased mortality and morbidity, in particular, during diarrheal disease and measles.
Vitamin and micronutrient deficiencies can be differentiated in 2 categories listed below. Patients with deficiencies of type 1 nutrients present with late and specific clinical signs. In contrast, patients with deficiencies of type 2 nutrients are difficult to identify because blood levels are unreliable and the clinical signs are nonspecific, such as the growth retardation with mild deficiency and weight loss with significant deficiency. Furthermore, type 2 nutrient deficiencies are often combined. Therefore, these deficiencies are global and require a global nutritional rehabilitation, such as WHO standardized solution. UNICEF’s report indicates the three vitamin/micronutrient deficiencies of largest international public health significance are iodine, iron, and vitamin A 13.
Below are characteristics of type 1 and type 2 deficiencies, according to Golden from a 1991 report.
Type 1 deficiencies
- Specific clinical signs
- Clinical signs appear after a latency period
- Used in specific metabolic pathways
- Are independent of one another
- Variable tissue concentration
Type 2 deficiencies
- Nonspecific clinical signs
- Nutrient status related to daily intake
- Used in various organs and metabolic pathways
- Nutrient interaction
- Constant tissue concentration
Below are lists of nutrient classification according to the clinical response to deficiency in type 1, with reduction of tissue concentration, and type 2 with growth deficit.
Type 1 nutrients
- Selenium
- Iodine
- Iron
- Copper
- Calcium
- Manganese
- Thiamin
- Riboflavin
- Ascorbic acid
- Retinol
- Tocopherol
- Calciferol
- Folic acid
- B-12 vitamin
- Pyridoxine
Type 2 nutrients
- Sodium
- Sulfur
- Essential amino acids
- Potassium
- Sodium
- Magnesium
- Zinc
- Phosphorus
- Water
Metabolic Changes
The overall metabolic adaptations that occur during marasmus are similar to those in starvation, which have been more extensively investigated. The primary goal is to preserve adequate energy to the brain and other vital organs in the face of a compromised supply. Early on, a rise in gluconeogenesis leads to a perceived increased metabolic rate. As fasting progresses, gluconeogenesis is suppressed to minimize muscle protein breakdown, and ketones derived from fat become the main fuel for the brain.
With chronic underfeeding, the basal metabolic rate decreases. One of the main adaptations to long-standing energy deficiency is a decreased rate of linear growth, yielding permanent stunting. The energy saving is partially attenuated by the diversion of energy from muscle to the more metabolically active organs. Further adaptations to crisis situations, such as significant infections, may have some parallels to those that are observed in a stressed, malnourished animal model 12. The rise in energy expenditure and urinary nitrogen excretion following surgery were significantly less in malnourished rats. This suggests that malnutrition can impair the ability of the organism to mobilize substrates to respond to stress. However, the healing process in these animals remained normal, indicating the ability to prioritize this biological activity.
Energy metabolism
- With reduced energy intake, a decrease in physical activity occurs followed by a progressively slower rate of growth. Weight loss initially occurs due to a decrease in fat mass, and afterwards by a decrease in muscle mass, as clinically measured by changes in arm circumference.
- Muscle mass loss results in a decrease of energy expenditure. Reduced energy metabolism can impair the response of patients with marasmus to changes in environmental temperature, resulting in an increased risk of hypothermia. Furthermore, during infection, fever is reduced compared to a well-nourished patient. In case of nutrient deficiency, the metabolism is redirected to vital function (requiring 80-100 kcal/kg/d). During recovery, the energy cost of catch-up growth has to be added (up to 100 kcal/kg/d). At this stage, energy needs can be massive.
Protein metabolism: Intestinal absorption of amino acids is maintained, despite the atrophy of the intestinal mucosa. Protein turnover is decreased (as much as 40% in severe forms), and protein-sparing mechanisms regulated by complex hormonal controls redirect amino acids to vital organs. Amino acids liberated from catabolism of muscle are recycled by the liver for the synthesis of essential proteins. Total plasma proteins, including albumin, are decreased, whereas gamma globulins are often increased by the associated infections.
Albumin: An albumin concentration lower than 30 g/L is often considered as the threshold below which edema develops from decreased oncotic pressure. However, in marasmus, albumin concentration can occasionally be below this value without edema. Prealbumin concentration is a sensitive index of protein synthesis. It decreases with decreased protein intake and rapidly increases in a few days with appropriate nutritional rehabilitation. Insulinlike growth factor 1 (IGF-1) is another sensitive marker of nutritional status.
Carbohydrate metabolism: This has mainly been studied in order to explain the serious and often fatal hypoglycemia that occurs in the initial renutrition phase of children with marasmus. The glucose level is often initially low, and the glycogen stores are depleted. Also, a certain degree of glucose intolerance of unclear etiology is observed, possibly associated with a peripheral resistance to insulin or with hypokalemia. One 2012 study 14, showed reactive hyperglycemia with reintroduction of carbohydrate indicating insulin impairment. Impaired glucose clearance in both kwashiorkor and marasmus may be related to dysfunctional pancreatic beta cell function without evidence of hepatic or peripheral insulin resistance. The reputed mechanism in kwashiorkor, and possibly marasmus, is related to pancreatic atrophy, fatty infiltration, and increased oxidative stress in beta cells. In the initiation of renutrition or in association with diarrhea or infection, a significant risk of profound and even fatal hypoglycemia occurs. Small and frequent meals are recommended, including during the night, to avoid death in the early morning. Furthermore, the digestion of starch is impaired by the decreased production of pancreatic amylase. Lactose malabsorption is frequent but is generally without clinical consequences. In most cases, renutrition using milk is possible.
Fat metabolism: Dietary fats are often malabsorbed in the initial phase of marasmus renutrition. The mobilization of fat stores for energy metabolism takes place under hormonal control by adrenaline and growth hormone. Blood lipid levels are usually low, and serious dysregulation of lipid metabolism can occur, mainly during kwashiorkor and rarely during marasmus.
Anatomic Changes
Digestive tract
The entire digestive tract from mouth to rectum is affected. The mucosal surface becomes smooth and thin, and secretory functions are impaired. A decrease in gastric hydrochloric acid (HCl) excretion and a slowing of peristalsis is observed, yielding bacterial overgrowth in the duodenum. Proportionally, the digestive tract is the organ system that loses the largest mass during marasmus. However, these important alterations of the digestive tract interfere only moderately with normal nutrient absorption. Therefore, early enteral renutrition is not contraindicated but is encouraged because some of the nutrients necessary for the recovery of the intestinal mucosa are used directly from the lumen.
In addition to the anatomic changes associated with protein-energy malnutrition, the frequent intestinal infections by viruses and bacteria and the toxins they produce also contribute to the changes in the digestive tract. Liver volume usually decreases, as do other organ volumes. An enlarged liver suggests the possibility of other diagnoses, such as kwashiorkor or hepatitis. Liver synthetic function is usually preserved, although protein synthesis is decreased, as reflected by the decreased albumin and prealbumin levels. Glycogen synthesis is decreased, further increasing the risk for hypoglycemia. The detoxifying function of the liver is impaired with structural changes in the liver cells. Therefore, drugs that are metabolized by the liver should be administered with caution, and liver function should be monitored.
Endocrine system
Many of the adaptations seen in marasmus are mediated by thyroid hormones, insulin, and growth hormone. As in any stressed state, the adrenergic response is activated.
This response is functional in marasmus but less so in kwashiorkor. Muscle proteins are converted into amino acids and are used for the hepatic synthesis of lipoproteins. These lipoproteins contribute to the mobilization of triglycerides from the liver. In contrast, during kwashiorkor, this function is impaired, resulting in liver steatosis, which is not usually present in marasmus. However, any precipitating factor, such as gastroenteritis or inappropriate renutrition, can disrupt this fragile adaptive mechanism.
Furthermore, in serious marasmus, a significant degree of hypothyroidism, with a decrease in the size of the thyroid gland and repercussions on the brain function and psychomotor development exists. In less severe forms, the impaired thyroid function has fewer clinical consequences. Insulin levels are low and contribute to a certain degree of glucose intolerance, especially during kwashiorkor. Therefore, high-carbohydrate diets are inappropriate. Growth hormone levels are initially within the reference range, but they progressively decrease with time, explaining the halt in linear growth observed with marasmus.
After initiation of renutrition, the hormonal milieu is reversed allowing for substantial anabolism and a rapid linear growth spurt. However, if the marasmic state has gone on too long, then the adult height is less than the genetic potential. Recently, investigators have obtained data that suggest a role for additional hormones in protein-energy malnutrition. Levels of serum ghrelin (an appetite stimulating peptide) were increased 15 and serum levels of leptin (a satiety hormone) and IGF-1 were decreased in children with protein-energy malnutrition compared with healthy controls 16. Fatty acid metabolism plays an important role in adaptation to acute malnutrition. Low adipose tissue leptin levels associate with mortality prior to and during treatment 17.
Hematopoietic system
A moderate normochromic or slightly hypochromic anemia is usually present, with normal red blood cell size. Iron and folate deficiencies, intestinal parasites, malaria, and other chronic infections exacerbate the anemia. However, iron stores are present in the liver. Therefore, iron supplementation should not be initially implemented. Oral iron is poorly tolerated by the digestive tract. The other blood cells (eg, thrombocytes, white blood cells) are also affected, but with generally limited clinical consequences. Blood clotting mechanisms are usually preserved, except in the case of serious vitamin K deficiency.
Immune system
Immune impairment and infections are usually associated with marasmus. Thymus atrophy is a characteristic manifestation of marasmus, but all T lymphocyte–producing tissues are affected. However, B-lymphocyte tissues, such as Peyer patches, the spleen, and the tonsils, are relatively preserved. Cellular immunity is most affected, with a characteristic tuberculin anergy. However, antibody production is maintained. In marasmus, a general acquired immunodeficiency occurs, with a decrease in secretory immunoglobulin A (IgA) and an impairment of the nonspecific local defense system, such as mucosal integrity and lymphokine production. Bacteriemia, candidiasis, and Pneumocystis carinii infection are frequently present. Immune impairment is less frequent with moderate malnutrition. Immunological recovery is generally rapid, except if measles is associated. Early malnutrition could create alterations in initial colonization of gut microbiota and the normal flora may not be restored even with therapeutic diet and antimicrobial medications. Future studies are needed to understand the gut microbiota in patients with severe or refractory disease 18.
Brain and nervous system
Cerebral tissue is usually preserved during marasmus. Brain atrophy with impairment of cerebral functions is only present in severe forms of marasmus. Effects on the brain are more important if malnutrition takes place during the first year of life or during fetal life. Irritability and apathy are characteristic of marasmus but improve rapidly with recovery. The permanent developmental consequences of marasmus are difficult to evaluate. Ongoing studies are evaluating these long-term consequences, as well as the benefit of nutritional supplementation with various vitamins and minerals.
Cardiovascular system
Cardiac muscle fiber is thin, and the contractility of the myofibrils is impaired. Cardiac output, especially systolic function, is decreased in the same proportion as the weight loss. Bradycardia and hypotension commonly occur in severe forms of malnutrition. Electrolyte imbalances present during marasmus modify the ECG findings. With this impaired cardiac function, any increase of intravascular volume during rehydration or blood transfusion can result in a significant cardiac insufficiency. With the rapid metabolic, energy, and electrolyte changes of the initial phase of renutrition, this period is also a period of high risk for arrhythmia or cardiac arrest. Therefore, close clinical monitoring is critical in children with circulatory compromise.
Marasmus symptoms
Signs and symptoms of marasmus vary with the importance and duration of the energy deficit, age at onset, associated infections (eg, GI infections), and associated nutritional deficiencies (eg, iron deficiency, iodine deficiency). Diets and deficiencies may vary considerably between different geographical regions and even within a country. The AIDS epidemic has also significantly changed the clinical course of classic marasmus. Marasmus is typically observed in infants who are breastfeeding when the amount of milk is markedly reduced or, more frequently, in those who are artificially fed. Failure to thrive is the earliest manifestation, associated with irritability or apathy. Chronic diarrhea is the most frequent symptom, and infants generally present with feeding difficulties. Presentation may be accelerated by an acute infection.
A shrunken wasted appearance is the classic presentation of marasmus. Anthropometric measurements are critical to rapidly assess the type and severity of the malnutrition. The Wellcome Classification of Malnutrition in Children was generally used, but the WHO has revised this classification. This simple classification allows a clear presentation of the clinical cases and allows comparisons between countries. Stunted children are usually considered to have a milder chronic form of malnutrition, but their condition can rapidly worsen with the onset of complications such as diarrhea, respiratory infection, or measles.
The most perceptible and frequent clinical feature in marasmus is the loss of muscle mass and subcutaneous fat mass. Some muscle groups, such as buttocks and upper limb muscles, are more frequently affected than others. Facial muscles are usually spared longer. Facial fat mass is the last to be lost, resulting, in severe cases, in the characteristic elderly appearance of children with marasmus. Anorexia is frequent and interferes with renutrition. An irritable and whining child who cannot be comforted or separated from the mother demonstrates behaviors often observed with marasmus. Apathy is a sign of serious forms of marasmus: children are increasingly motionless and seem to “let themselves die.” In contrast, during rehabilitation, even the slightest smile is a positive sign of recovery. Children’s behavior is probably one of the best clinical signs of the severity and evolution of marasmus.
Table 1. WHO Classification of Malnutrition
| Evidence of Malnutrition | Moderate | Severe (type) |
| Symmetric edema | No | Yes (edema protein-energy malnutrition [PEM])* |
| Weight for height† | Standard deviation (SD)‡ score -3 SD score < -2 (70-90%)§ | SD score < -3 (ie, severe wasting) || (< 70%) |
| Height for age | SD score– 3 SD score < -2 (85-89%) | SD score < -3 (ie, severe stunting) (< 85%) |
Footnote:
* This includes kwashiorkor (KW) and kwashiorkor marasmus (presence of edema always indicates serious PEM = protein-energy malnutrition).
† Standing height should be measured in children taller than 85 cm, and supine length should be measured in children shorter than 85 cm or in children who are too sick to stand. Generally, the supine length is considered to be 0.5 cm longer than the standing height; therefore, 0.5 cm should be deducted from the supine length measured in children taller than 85 cm who are too sick to stand.
‡ Below the median National Center for Health Statistics (NCHS)/WHO reference: The SD score is defined as the deviation of the value for an individual from the median value of the reference population divided by the standard deviation of the reference population (ie, SD score = [observed value – median reference value]/standard deviation of reference population).
§ This is the percentage of the median NCHS/WHO reference.
|| This corresponds to marasmus (without edema) in the Wellcome clinical classification and to grade III malnutrition in the Gomez system. However, to avoid confusion, the term severe wasting is preferred.
Marasmus diagnosis
Generally, for diagnosis and treatment of marasmus, no further evaluation is necessary other than the clinical evaluation. Most laboratory results are within the reference range despite significant changes in body composition and physiology. Furthermore, in regions where malnutrition is frequent, health structures are poorly equipped, and laboratory evaluations are either impossible to obtain or unreliable.
If they are available, some laboratory results can be useful to monitor treatment or to diagnose specific complications.
Laboratory tests adapted from the WHO include the following:
- Blood glucose: Hypoglycemia is present if the level is lower than 3 mmol/L.
- Examination of blood smears by microscopy or direct detection test: Presence of parasites is indicative of infection. Direct test is suitable but expensive.
- Hemoglobin: A level lower than 40 g/L is indicative of severe anemia.
- Urine examination and culture, Multistix: More than 10 leukocytes per high-power field is indicative of infection. Nitrites and leukocytes are tested on Multistix also.
- Stool examination by microscopy: Parasites and blood are indicative of dysentery.
- Albumin: Although not useful for diagnosis, it is a guide to prognosis; if albumin is lower than 35 g/L, protein synthesis is massively impaired.
- HIV test: HIV test should not be routinely performed; if completed, it should be accompanied by counseling of the child’s parents and the result should be confidential.
- Electrolytes: Measuring electrolytes is rarely helpful and it may lead to inappropriate therapy. Hyponatremia is a significant finding.
- Skin test results for tuberculosis are often negative in children who are undernourished with tuberculosis or those previously vaccinated with Bacille Calmette-Guérin (BCG) vaccine.
Marasmus treatment
Management of moderate marasmus can be performed on an outpatient basis, but severe marasmus or marasmus complicated by a life-threatening condition generally requires inpatient treatment. In these cases, management is divided into an initial intensive phase followed by a consolidation phase (rehabilitation), preparing for outpatient follow-up management. The WHO has developed guidelines 19 to help improve the quality of hospital care for malnourished children and has prioritized the widespread implementation of these guidelines.
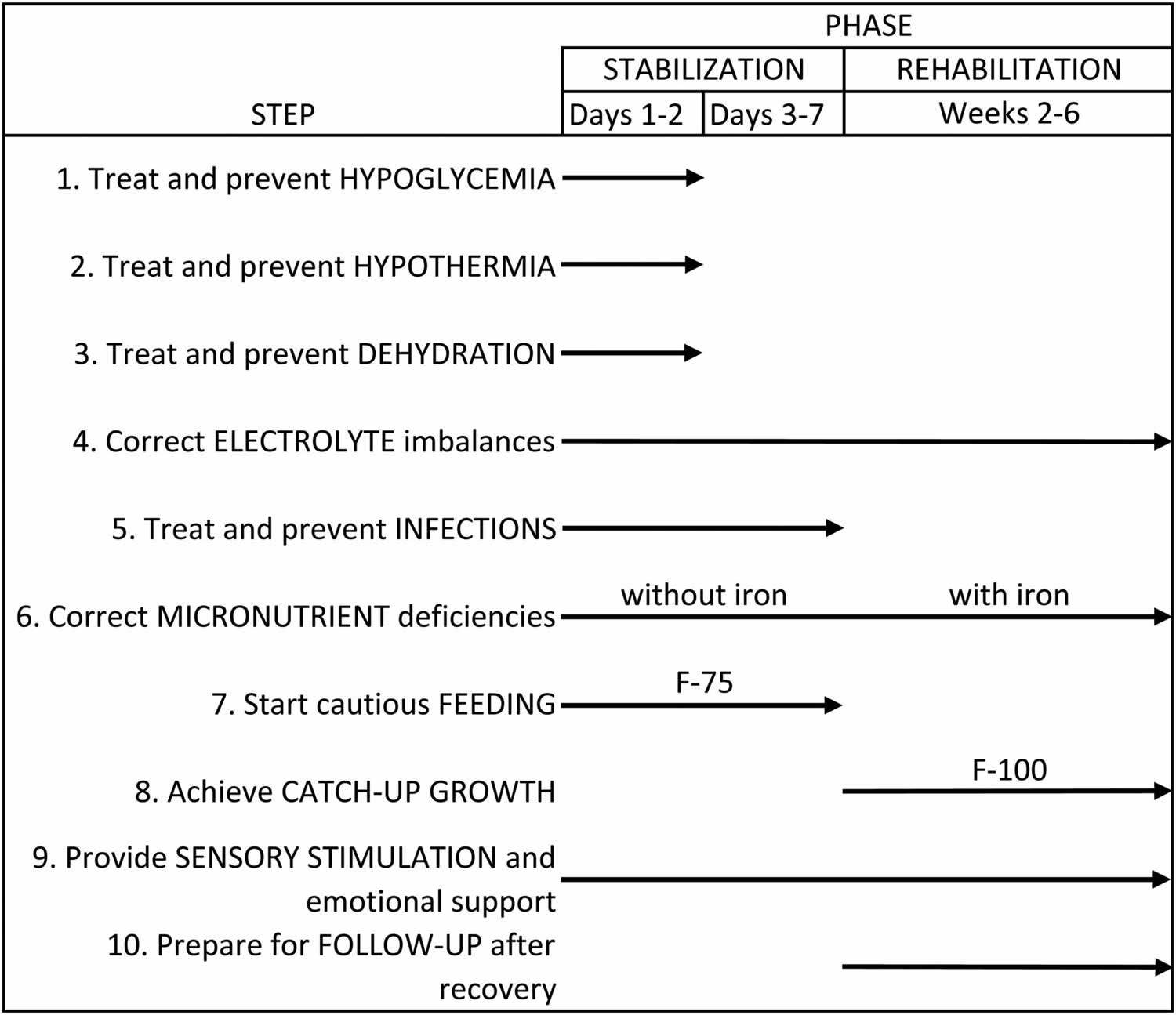
The following are ten primary principles used universally for treatment of patients who are admitted for Kwashiorkor 19. These principles are done in different phases from the time the child arrives requiring emergency stabilization through eventual rehabilitation.
- Treating/preventing hypocalcemia,
- Treating/preventing hypothermia
- Treating/preventing dehydration
- Correcting electrolyte imbalance
- Treating/preventing infection
- Correcting micronutrient deficiencies
- Starting cautious feeding
- Achieving catch-up growth
- Providing sensory stimulation and emotional support and
- Preparing for follow up after recovery.
It is important to highlight how critical it is to address the fluid imbalance in kwashiorkor. In the past, there was concern about aggressive rehydration causing acute heart failure. However, this was proven to be exaggerated. At the same time, severe hypovolemia could cause hypovolemic shock and death. So, medical staff had to proceed cautiously. The standard normal saline solution contains too much sodium and too little potassium. However, ReSoMal (Rehydration Solution of Malnutrition) is a customized solution that can be given orally or via nasogastric tubes that contains the exact amount of mineral/electrolytes, sugar, and water that the WHO recommends.
Figure 1. Marasmus WHO feeding guidelines
Because most patients with moderate cases of marasmus can be treated as outpatients, the optimal environment is a pediatric nutrition rehabilitation center. Nutritional rehabilitation should include appropriate foods for an intake up to 100-150 kcal/kg/d. Other therapeutic and preventive actions should include rehydration using the WHO solution (see below) in case of associated diarrhea, micronutrient supplementation (eg, iron, vitamin A), context-appropriate screening, and review of immunization status. This management should also incorporate nutritional and sociocultural education adapted to the local conditions. Family-based management is preferred with the child’s mother as the key player.
One key aspect of marasmus management is the potential role for routine antibiotics. The WHO has made formal recommendations for the use of oral antibiotics for children with uncomplicated severe acute malnutrition, not requiring to be admitted and who are managed as outpatients 21. Two meta-analyses found a paucity of evidence to support this recommendation 22. However, a double-blind, placebo controlled study of more than 2600 Malawian children concluded that the addition of antibiotics to therapeutic regimens for uncomplicated severe acute malnutrition was associated with a significant improvement in recovery and mortality rates 23. An even more recent 2016 meta-analysis concluded Amoxicillin should remain recommended in children with uncomplicated severe acute malnutrition 24.
Marasmus malnutrition prognosis
While recovery rates from outpatient therapeutic programmes are generally as good as or better than inpatient programmes 25, there have, in fact, not been the most stringent prospective blinded randomized controlled trials that directly test the efficacy of ready-to-use therapeutic food 26. Nevertheless, more than a decade of operational clinical experience with millions of children has rightly made outpatient management of uncomplicated severe acute malnutrition the de facto standard of care 27, and it is unlikely that such a trial could now ethically be conducted.
In the best circumstances, some 90% of children can be expected to recover from severe acute malnutrition and <5% mortality should be achievable 28. Untreated episodes of severe wasting typically have a mortality rate of 10%–15% per month; while many will recover spontaneously, their cognitive and physical development likely remains stunted. However, the success of current therapies for severe acute malnutrition underestimates overall mortality as those who recover are at continued risk for relapse and death in the long term, especially those who are HIV-infected 29.
Further work needs to be done to improve surveillance and case-finding of children with severe acute malnutrition and additional efforts need to be made to treat severe acute malnutrition as a medical emergency, integrating it into the routine delivery of healthcare. This is particularly important in the context of linkage to HIV testing and treatment efforts 30.
- Marasmus. https://emedicine.medscape.com/article/984496-overview[↩][↩]
- Benjamin O, Lappin SL. Kwashiorkor. [Updated 2019 Mar 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507876[↩][↩]
- Spoelstra MN, Mari A, Mendel M, Senga E, van Rheenen P, van Dijk TH, et al. Kwashiorkor and marasmus are both associated with impaired glucose clearance related to pancreatic ß-cell dysfunction. Metabolism. 2012 Mar 2[↩]
- International Food Policy Research Institute, Washington, DC. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. 2016.[↩]
- Hendricks KM, Duggan C, Gallagher L, et al. Malnutrition in hospitalized pediatric patients. Current prevalence. Arch Pediatr Adolesc Med. 1995 Oct. 149(10):1118-22[↩]
- Cameron JW, Rosenthal A, Olson AD. Malnutrition in hospitalized children with congenital heart disease. Arch Pediatr Adolesc Med. 1995 Oct. 149(10):1098-102[↩]
- Joosten KF, Hulst JM. Prevalence of malnutrition in pediatric hospital patients. Curr Opin Pediatr. 2008 Oct. 20(5):590-6[↩]
- Guideline] GUIDELINE: UPDATES ON THE MANAGEMENT OF SEVERE ACUTE MALNUTRITION IN INFANTS AND CHILDREN. 2013.[↩]
- Jeyaseelan V, Jeyaseelan L, Yadav B. INCIDENCE OF, AND RISK FACTORS FOR, MALNUTRITION AMONG CHILDREN AGED 5-7 YEARS IN SOUTH INDIA. J Biosoc Sci. 2016 May. 48 (3):289-305[↩]
- Akuyam SA, Isah HS, Ogala WN. Serum lipid profile in malnourished nigerian children in zaria. Niger Postgrad Med J. September 2008. 15 (3):192-6[↩]
- Chand S, Shah D. Mid upper Arm Circumference for Detection of Severe Acute Malnutrition in Infants Aged Between One and Six Months. Indian Pediatr. 2015 Jun. 52 (6):528-9.[↩]
- Lazzerini M, Ronfani L. Oral zinc for treating diarrhoea in children. Cochrane Database Syst Rev. 2008. (3):CD005436[↩][↩]
- Malnutrition. https://data.unicef.org/topic/nutrition/malnutrition/[↩]
- Spoelstra MN, Mari A, Mendel M, Senga E, van Rheenen P, van Dijk TH, et al. Kwashiorkor and marasmus are both associated with impaired glucose clearance related to pancreatic β-cell dysfunction. Metabolism. 2012 Sep. 61 (9):1224-30[↩]
- Altinkaynak S, Selimoglu MA, Ertekin V, Kilicarslan B. Serum ghrelin levels in children with primary protein-energy malnutrition. Pediatr Int. 2008 Aug. 50(4):429-31[↩]
- Kilic M, Taskin E, Ustundag B, Aygun AD. The evaluation of serum leptin level and other hormonal parameters in children with severe malnutrition. Clin Biochem. 2004 May. 37(5):382-7[↩]
- Bartz S, Mody A, Hornik C, Bain J, Muehlbauer M, Kiyimba T, et al. Severe acute malnutrition in childhood: hormonal and metabolic status at presentation, response to treatment, and predictors of mortality. J Clin Endocrinol Metab. 2014 Jun. 99 (6):2128-37[↩]
- Million M, Diallo A, Raoult D. Gut microbiota and malnutrition. Microb Pathog. 2016 Feb 4.[↩]
- Ahmed S, Ejaz K, Mehnaz A, Adil F. Implementing WHO feeding guidelines for inpatient management of malnourished children. J Coll Physicians Surg Pak. 2014 Jul;24(7):493-7[↩][↩]
- Trehan I, Manary MJ. Management of severe acute malnutrition in low-income and middle-income countries. Archives of Disease in Childhood 2015;100:283-287. https://adc.bmj.com/content/100/3/283[↩]
- [Guideline] GUIDELINE: UPDATES ON THE MANAGEMENT OF SEVERE ACUTE MALNUTRITION IN INFANTS AND CHILDREN. 2013.[↩]
- Alcoba G, Kerac M, Breysse S, et al. Do children with uncomplicated severe acute malnutrition need antibiotics? A systematic review and meta-analysis. PLoS One. 2013. 8(1):e53184[↩]
- Trehan I, Goldbach HS, LaGrone LN, et al. Antibiotics as part of the management of severe acute malnutrition. N Engl J Med. 2013 Jan 31. 368(5):425-35[↩]
- World Health Organization. WHO Global Database on Child Growth and Malnutrition. Geneva: WHO. 1996.[↩]
- Bahwere P, Mtimuni A, Sadler K, et al. Long term mortality after community and facility based treatment of severe acute malnutrition: Analysis of data from Bangladesh, Kenya, Malawi and Niger. J Pub Health Epid 2012;4:215–25[↩]
- Schoonees A, Lombard M, Musekiwa A, et al. Ready-to-use therapeutic food for home-based treatment of severe acute malnutrition in children from six months to five years of age. Cochrane Database Syst Rev 2013;6:CD009000[↩]
- WHO. Guideline: updates on the management of severe acute malnutrition in infants and children. Geneva: World Health Organization, 2013[↩]
- Trehan I, Goldbach HS, LaGrone LN, et al. Antibiotics as part of the management of severe acute malnutrition. N Engl J Med 2013;368:425–35[↩]
- Kerac M, Bunn J, Chagaluka G, et al. Follow-up of post-discharge growth and mortality after treatment for severe acute malnutrition (FuSAM study): a prospective cohort study. PLoS ONE 2014;9:e96030[↩]
- Trehan I, O’Hare BA, Phiri A, et al. Challenges in the management of HIV-infected malnourished children in Sub-Saharan Africa. AIDS Res Treat 2012;2012:790786[↩]





{kind=link}