What is MCV
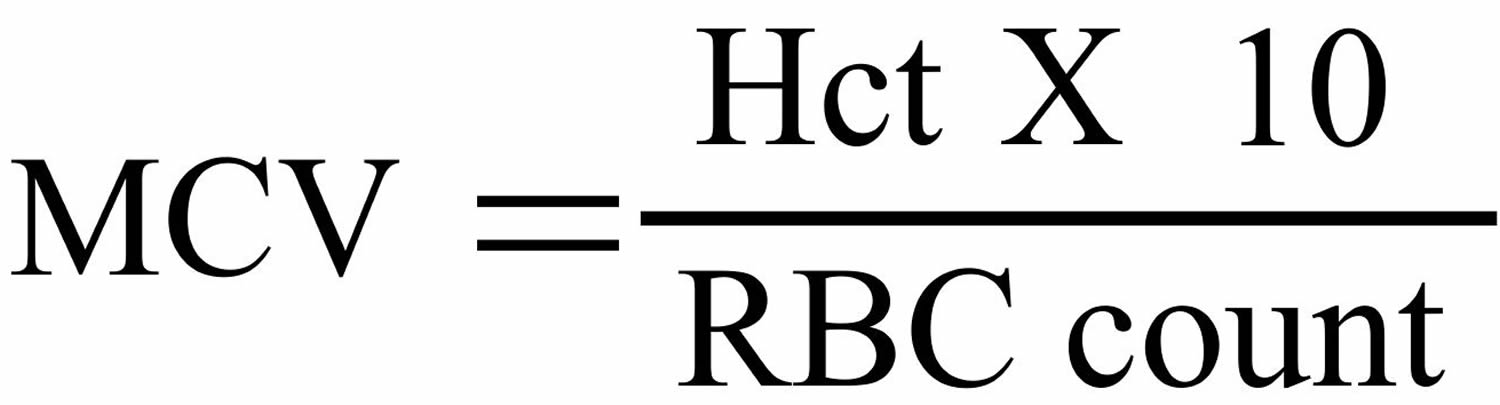
MCV is short for mean cell volume or mean corpuscular volume (MCV), which is a measurement of the average size of a single red blood cell. MCV defines the size of the red blood cells and is expressed as femtoliters (10−15; fl) or as cubic microns (μm3). Mean corpuscular volume (MCV) is the best index of classifying anemia. Arithmetically, MCV is Hematocrit (Hct) divided by red blood cell (RBC) count.
Figure 1. MCV calculation
 The normal values for MCV are 87 ± 7 fl.
The normal values for MCV are 87 ± 7 fl.MCV normal range
- Adult (all ages) = 80 to 95 mm³ (87 ± 7 fl.)
- Newborn = 96 to 108 mm³
On the basis of MCV blood test
- Macrocytes when MCV value is high (larger than normal red blood cells), e.g. in Megaloblastic anemia (due to vitamin B and folic acid deficiency).
- Microcytes when the MCV is decreased (smaller than normal red blood cells) as seen in iron deficiency anemia and thalassemia.
- In microcytic anemia (MCV less than the lower limit of normal), MCV is 50 to 82 mm³
- In normocytic normochromic anemia (MCV within normal range), MCV is 82 to 98 mm³
- In macrocytic anemia (MCV greater than the upper limit of normal), MCV is 100 to 150 mm³
The following are the types of anemia and their causes:
- Microcytic/hypochromic anemia e.g. from iron deficiency, lead poisoning, or thalassemia.
- Microcytic/normochromic anemia e.g. lack (deficiency) of the hormone erythropoietin from kidney failure.
- Macrocytic/normochromic anemia e.g.from chemotherapy, folate deficiency, or vitamin B12 deficiency.
- Normocytic/normochromic anemia e.g.from blood loss, prosthetic heart valves, sepsis, tumor, or aplastic anemia.
Mean corpuscular hemoglobin (MCH) measures the mean of the average amount of hemoglobin in red blood cells. Generally, macrocytes will have more hemoglobin and microcytes will have less hemoglobin. So the values resemble those of MCV.
Mean corpuscular hemoglobin concentration (MCHC) is the average concentration of or percentage of hemoglobin in the red cells. This is calculated by dividing the hemoglobin concentration by hematocrit. Mean corpuscular hemoglobin concentration (MCHC) is the most useful in monitoring the treatment of anemia.
Red blood cell distribution width (RDW) indicates variation in the size of red blood cell.
Table 1. What MCV mean in a blood test
| Red cell size as defined by MCV | |||
|---|---|---|---|
| RDW | Decreased (microcytic; low MCV) | Normal (normocytic; MCV = normal) | Increased (macrocytic; high MCV) |
| Normal (little or no anisocytosis) | Heterozygous thalassemias | Poor iron utilization | Liver disease |
| Acute blood loss | Aplastic anemia | ||
| Anemia of chronic disease (hypoproliferative) | Enzyme defects (e.g., G6PD deficiency) | Myelodysplastic syndrome | |
| Acute hemolysis | |||
| Liver disease | |||
| Increased (anisocytosis) | Iron deficiency | Early iron deficiency | Megaloblastic |
| Red cell fragmentation | Early megaloblastic | Sideroblastic | |
| Sideroblastic | Myelodysplastic syndrome | ||
| Myelophthisis | Secondary to chemotherapy | ||
| Combined deficiency | |||
| Sickle cell anemia | |||
| Immune hemolysisa | |||
| Secondary to chemotheraphy | |||
- a MCV may be falsely elevated due to cell agglutination, usually with cold agglutinins.
- Red blood cell distribution width (RDW) indicates variation in the size of red blood cell.
What is anemia?
Anemia is the most common blood disorder in the United States. It affects your red blood cells and hemoglobin. This is the protein in red blood cells that carries oxygen from your lungs to the rest of your body. You need iron in order to make hemoglobin. Most people who have anemia have a shortage of iron. This condition is called iron deficiency anemia.
There are a few other types of anemia, including:
- Aplastic anemia. This occurs when your bone marrow has damaged stem cells. Your body fails to produce enough new blood cells. The condition affects your red blood cells, white blood cells, and platelets. Sometimes it is called bone marrow failure.
- Hemolytic anemia. This occurs when your body destroys red blood cells before they should. The normal lifespan of red blood cells is 120 days.
- Normocytic anemia. This occurs when your red blood cells are normal in size, but low in count.
- Pernicious anemia. This occurs when your body lacks vitamin B12. It causes a shortage of healthy red blood cells.
- Sickle cell anemia (a form of sickle cell disease). This is a genetic disease that affects your red blood cells. It occurs when you are born with 2 abnormal hemoglobin genes.
Symptoms of anemia
Mild forms of anemia may not cause any symptoms. Fatigue, or feeling tired, is a common symptom. This is because the hemoglobin in red blood cells carries oxygen. A lack of oxygen reduces energy. It can cause your heart to work harder to pump oxygen. Anemia can produce other symptoms, such as:
- paleness
- shortness of breath
- cold hands and feet
- headaches
- dizziness
- fast, slow, or uneven heartbeat
- brittle nails or hair loss
- strange food cravings (known as pica).
Contact your doctor if you have any of these symptoms. They can diagnose the type and cause of the condition.
What causes anemia?
There are three main reasons why anemia occurs.
1) Your body can’t produce enough red blood cells.
Diet
Your body may not produce enough red blood cells if you lack certain nutrients. Low iron is a common problem. People who don’t eat meat or follow “fad” diets are more at risk of low iron. Infants and toddlers are at risk of getting anemia from a low-iron diet. Low vitamin B12 and folic acid can cause anemia as well.
Unable to absorb
Certain diseases affect your small intestine’s ability to absorb nutrients. For example, Crohn’s disease and celiac disease can cause low iron levels in your body. Some foods, like milk, can prevent your body from absorbing iron. Taking vitamin C can help this. Medicines, such as antacids or prescriptions to reduce acid in your stomach, can affect it as well.
Pregnancy
Women who are pregnant or breastfeeding can get anemia. When you’re pregnant, you need more blood (up to 30%) to share with the baby. If your body lacks iron or vitamin B12, your body can’t produce enough red blood cells.
The following factors may increase your risk of anemia during pregnancy.
- Vomiting a lot from morning sickness.
- Having a diet low in nutrients.
- Having heavy periods before pregnancy.
- Having 2 pregnancies close together.
- Being pregnant with multiple babies at once.
- Becoming pregnant as a teenager.
- Losing a lot of blood from an injury or surgery.
Growth spurts
Children younger than 3 years of age are prone to anemia. Their bodies grow so fast that they can have a hard time getting or keeping enough iron.
Normocytic anemia
Normocytic anemia can be congenital (from birth) or acquired (from a disease or infection). The most common cause of the acquired form is a chronic (long-term) disease. Examples include kidney disease, cancer, rheumatoid arthritis, and thyroiditis. Some medicines can cause normocytic anemia, but this is rare.
2) Your body destroys red blood cells early and faster that they can be replaced
Treatments, such as chemotherapy, can damage your red blood cells and/or bone marrow. Infection caused by a weakened immune system can lead to anemia. You may be born with a condition that destroys or remove red blood cells. Examples include sickle cell disease, thalassemia, and a lack of certain enzymes. Having an enlarged or diseased spleen can cause anemia, too.
3) You have blood loss that creates a shortage of red blood cells
Heavy periods may cause low iron levels in women. Internal bleeding, such as in your digestive or urinary tract, can cause blood loss. This can be caused by conditions such as a stomach ulcer or ulcerative colitis. Other reasons for blood loss include:
- cancer
- surgery
- trauma
- taking aspirin or a similar medicine for a long time.
Anemia diagnosis
Talk to your doctor if you think you or your child might have anemia. They will do a physical exam and review your health history and symptoms. To diagnose anemia, your doctor will test your blood. This test is called a complete blood count (CBC). Based on the results, they may need to do other tests, such as testing your bone marrow. This can help confirm the cause of anemia or another health condition.
Can anemia be prevented or avoided?
You cannot avoid anemia caused by a genetic disease. You often cannot avoid it due to blood loss. If your blood loss is from heavy periods, receiving treatment can help prevent anemia. If your body can’t absorb certain nutrients, such as iron or vitamin B12, talk to your doctor about taking a supplement. This can help manage your levels and prevent anemia.
A balanced diet can help prevent some types of anemia. Eat the foods below to prevent a deficiency.
Foods high in iron include:
- red meat
- seafood
- organ meats, such as liver
- whole grains
- dried fruits
- nuts
- beans, especially lima beans
- dark green leafy vegetables, such as spinach and broccoli
- iron-fortified foods, such as breads and cereals (check the label).
Vitamin C can help your body absorb iron. Try eating foods, such as citrus fruits or juice. Some foods can make it harder for your body to absorb iron. These include coffee, tea, milk, egg whites, fiber, and soy protein. Try to avoid these foods if you have iron deficiency anemia.
Foods high in vitamin B12 include:
- meat and poultry
- organ meats, such as liver
- fish and shellfish
- eggs, milk, and dairy products
- some fortified cereals, grains, and yeasts (check the label).
Foods high in folic acid (folate) include:
- dark green leafy vegetables, such as spinach and broccoli
- asparagus
- beans
- peas
- lentils
- bananas, oranges, and orange juice.
Pregnant women may be tested for anemia or take an iron supplement to help prevent it. However, the American Academy of Family Physicians has insufficient evidence to assess the benefits and risks of screening pregnant women for iron deficiency anemia or having them take an iron supplement.
Evidence also is lacking to measure the benefits and risks of screening children ages 6 to 24 months. To help prevent your child from getting iron deficiency anemia, you can:
- use iron-fortified formula
- use iron-fortified cereal starting around 4 months of age
- limit your child to less than 24 oz. (3 cups) of cow’s milk per day (after 12 months of age)
- introduce foods high in iron starting around 12 months of age.
Warning: Keep all products with iron stored out of reach of your child. Iron can be toxic if taken in large amounts.
Anemia treatment
There are many treatment options for anemia. They vary based on the type, cause, and severity, as well as your overall health. The first goal of treatment is to create more healthy red blood cells that can carry enough oxygen to your body. Often this is achieved by increasing your red blood cell count and/or hemoglobin. The other goal is to treat the cause, if possible. For example, if anemia results from losing too much blood, your doctor will need to treat the cause of your blood loss.
If you have a type of anemia caused by a deficiency, make changes to your diet. This can increase your nutrient levels or help your body absorb nutrients.
In some cases, your doctor can prescribe medicine to help your body produce more red blood cells. Examples include:
- Erythropoietin shots to treat normocytic anemia. These can help your bone marrow produce more red blood cells.
- Hormone medicines to treat heavy periods.
- Antibiotic medicines to treat infections.
- Medicines to help prevent your body from damaging or destroying red blood cells.
Other forms of anemia require intense treatment. You may need surgery to stop blood loss or have your spleen removed. Other treatments include a blood transfusion or a blood and bone marrow stem cell transplant.
Talk to your doctor about how to manage a chronic disease or other health problem that causes anemia.
Living with anemia
Following treatment, most people go on to live normal, healthy lives. However, anemia can have lasting, or life-threatening, effects. These are more common if the condition is chronic, severe, or left untreated. They include:
- Arrhythmia. This is an issue with your heartbeat. It can be too fast, too slow, or uneven. Over time, this can lead to heart disease or heart failure.
- Organ damage. This can occur if an organ doesn’t get enough oxygen.
- Weakened immune system. This can be fatal if your immune system already is weak from cancer, disease (such as HIV/AIDS), or an infection.
Children who have iron deficiency anemia have a higher risk of lead poisoning. They also can develop mental, motor, or behavioral problems over a long time.
Pregnant women who have iron deficiency anemia may have their baby premature or at a low birth weight. There also is a risk of needing a blood transfusion if you lose a lot of blood during delivery. Anemia may be associated with postpartum depression.
What are red blood cells
Blood transports a variety of materials between interior body cells and those that exchange substances with the external environment. In this way, blood helps maintain stable internal environmental conditions. Blood is composed of formed elements suspended in a fluid extracellular matrix called blood plasma. The “formed elements” include red blood cells, white blood cells, and cell fragments called platelets. Most blood cells form in red marrow within the hollow parts of certain long bones.
Most blood samples are roughly 37% to 49% red blood cells by volume – adult females is 38–46% (average = 42%) and for adult males, it is 40–54% (average = 47). This percentage is called the hematocrit. The white blood cells and platelets account for less than 1% of blood volume. The remaining blood sample, about 55%, is the plasma, a clear, straw-colored liquid. Blood plasma is a complex mixture of water, gases, amino acids, proteins, carbohydrates, lipids, vitamins, hormones, electrolytes, and cellular wastes.
Blood volume varies with body size, percent adipose tissue, and changes in fluid and electrolyte concentrations. An average-size adult has a blood volume of about 5 liters (5.3 quarts), 4–5 liters in a female and 5–6 liters in a male.
Red blood cell (also called erythrocyte) is biconcave disc without a nucleus. This biconcave shape is an adaptation for transporting the gases oxygen and carbon dioxide. It increases the surface area through which oxygen and carbon dioxide can diffuse into and out of the cell. The characteristic shape of a red blood cell also places the cell membrane closer to oxygen-carrying hemoglobin molecules in the cell reducing the distance for diffusion.
Each red blood cell is about one-third hemoglobin by volume. This protein imparts the color of blood. When hemoglobin binds oxygen, the resulting oxyhemoglobin is bright red, and when oxygen is released, the resulting deoxyhemoglobin is darker.
Prolonged oxygen deficiency (hypoxia) causes cyanosis, in which the skin and mucous membranes appear bluish due to an abnormally high blood concentration of deoxyhemoglobin in the superficial blood vessels. Exposure to low temperature may also result in cyanosis by constricting superficial blood vessels. This response to environmental change slows skin blood flow. As a result, more oxygen than usual is removed from the blood flowing through the vessels, increasing the concentration of deoxyhemoglobin.
Note: Blood is a complex mixture of formed elements in a liquid extracellular matrix, called blood plasma. Note that water and proteins account for 99% of the blood plasma.
Figure 2. Blood composition


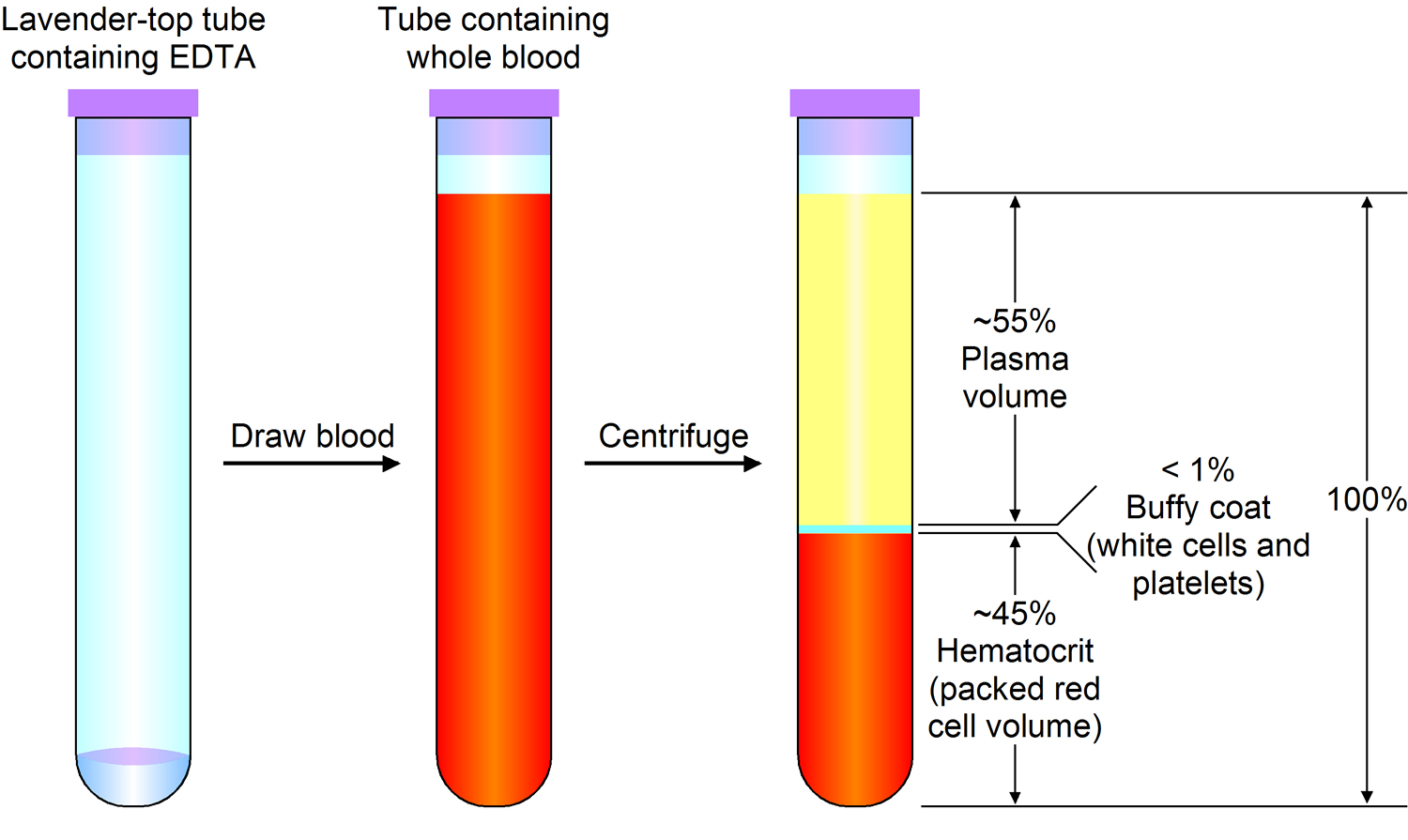
Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
Blood Cell Formation
The process of blood cell formation, called hematopoiesis, begins in the yolk sac, which lies outside the human embryo. Later in the fetal development, red blood cells are manufactured (erythropoiesis) in the liver and spleen, and still later they form in bone marrow. After birth, these cells are produced in the red bone marrow.
Bone marrow is a soft, netlike mass of connective tissue within the medullary cavities of long bones, in the irregular spaces of spongy bone, and in the larger central canals of compact bone tissue. It is of two kinds: red and yellow. Red bone marrow functions in the formation of red blood cells (erythrocytes), white blood cells (leukocytes), and blood platelets. The color comes from the oxygen-carrying pigment hemoglobin in the red blood cells.
In an infant, red marrow occupies the cavities of most bones. As a person ages, yellow bone marrow, which stores fat, replaces much of the red marrow. Yellow marrow is not active in blood cell production. In an adult, red marrow is primarily found in the spongy bone of the skull, ribs, breastbone (sternum), collarbones (clavicles), backbones (vertebrae), and hip bones. If the supply of blood cells is deficient, some yellow marrow may become red marrow, which then reverts to yellow marrow when the deficiency is corrected.
Figure 4 illustrates the stages in the formation of red blood cells from hematopoietic stem cells (blood-forming cells), which are also called hemocytoblasts.
Red blood cells have nuclei during their early stages of development but lose their nuclei as the cells mature. Losing the nuclei provides more space for hemoglobin. Because mature red blood cells do not have nuclei, they cannot divide. They use none of the oxygen they carry because they do not have mitochondria. Mature red blood cells produce ATP through glycolysis only.
The average life span of a red blood cell is 120 days. Many of these cells are removed from the circulation each day, and yet the number of cells in the circulating blood remains relatively stable. This observation suggests a homeostatic control of the rate of red blood cell production.
The hormone erythropoietin (EPO) controls the rate of red blood cell formation through negative feedback. The kidneys, and to a lesser extent the liver, release erythropoietin in response to prolonged oxygen deficiency (Figure 6). At high altitudes, for example, where the amount of oxygen in the air is reduced, the blood oxygen level initially decreases. This drop in the blood oxygen level triggers the release of erythropoietin, which travels via the blood to the red bone marrow and stimulates red blood cell production.
After a few days of exposure to high altitudes, many newly formed red blood cells appear in the circulating blood. The increased rate of production continues until the number of erythrocytes in the circulation is sufficient to supply tissues with oxygen. When the availability of oxygen returns to normal, erythropoietin release decreases, and the rate of red blood cell production returns to normal as well. An excessive increase in red blood cells is called polycythemia. This condition increases blood viscosity, slowing blood flow and impairing circulation.
Figure 3. Bone marrow anatomy

Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
What does MCV mean in a blood test?
During erythropoiesis (formation of red blood cells), the process of erythroid maturation involves a progressive condensation of nuclear chromatin (termed nuclear maturation) and finally its extrusion from the cell, the synthesis of hemoglobin in the cytoplasm (termed cytoplasmic maturation), and a concomitant reduction in cell size due to division and water loss.
Defects in nuclear maturation, as seen in megaloblastic anemias due to folate or vitamin B12 deficiency, result in large oval erythrocytes (macroovalocytes) with a normal hemoglobin content. The MCV (mean corpuscular volume) and mean corpuscular hemoglobin (MCH) are increased, while the mean corpuscular hemoglobin concentration (MCHC) remains normal. There is anisocytosis, and RDW is often increased. In the macrocytosis of liver disease, where there is no defect in nuclear maturation, the cells are large due to an excess red cell membrane. These cells are round, rather than oval, and the RDW is normal.
Defective hemoglobin synthesis results in small cells (low MCV) with or without anisocytosis. In heterozygous β-thalassemias, the cells are uniformly small (low MCV; RDW tends to be normal), whereas in iron deficiency, anisocytosis (increased RDW) may be the first laboratory abnormality, even before anemia and microcytosis are seen.
In abnormalities involving nuclear maturation, hemoglobin production proceeds normally, while cell division lags behind, ultimately leading to a larger than normal cell. In contrast, when there is defective and delayed synthesis of hemoglobin, the continued cell division leads to microcytosis.
Figure 4. Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell

Figure 5. Blood cells
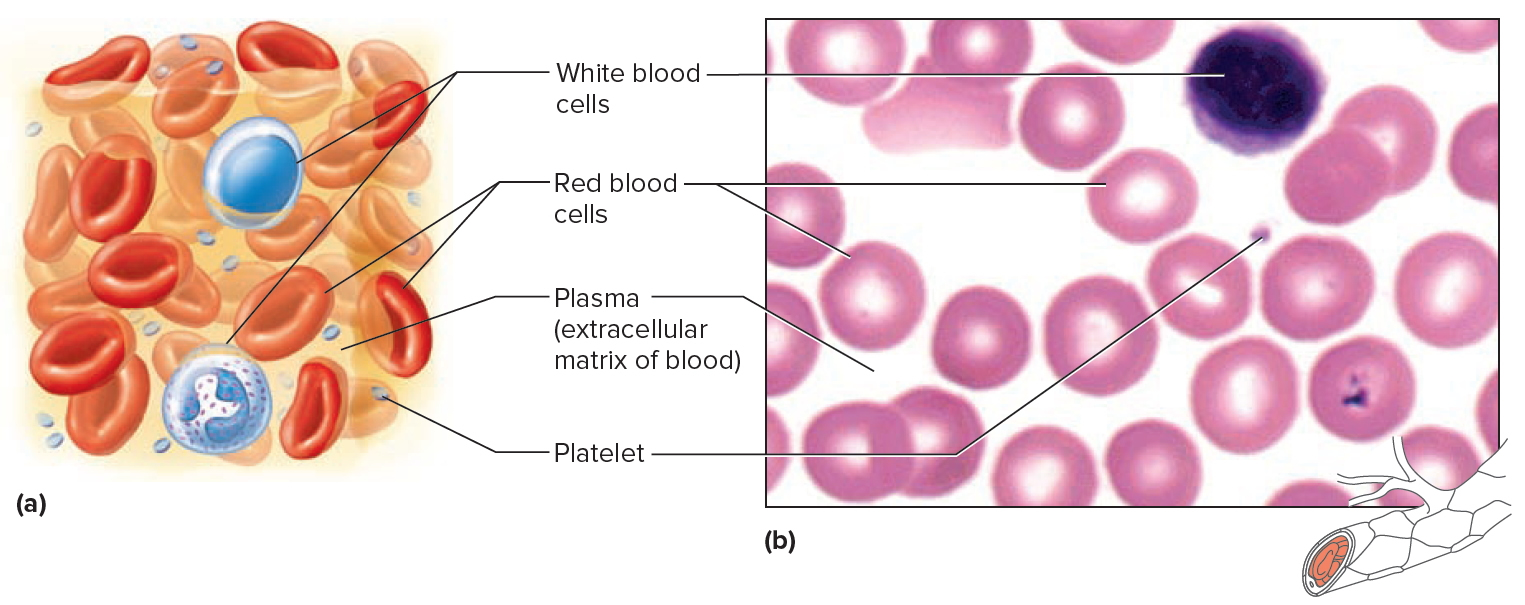
Note: Blood tissue consists of red blood cells, white blood cells, and platelets suspended in plasma. (a) Idealized representation of a sample of blood. (b) Micrograph of a sample of blood (1,000x).
Figure 6. Red blood cells
MCV high
Macrocytosis (high MCV) is 100 to 150 mm³
Macrocytosis (high MCV) is found in megaloblastic, aplastic, dyserythropoietic and sideroblastic anaemias; Myelodysplastic syndromes, myeloma; Liver disease, alcohol excess; chronic hypoxic lung disease; myxoedema; following renal transplant; cytotoxic drug therapy particularly hydroxyurea, therapy with Zidovudine (AZT); and some rare metabolic disorders.
High MCV common causes
- Pernicious anemia (vitamin B12 deficiency).
- Folic acid deficiency (vitamin B-9 deficiency).
- Antimetabolite treatment.
- Chronic liver disease.
- Alcoholism.
Pernicious anemia
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia.
Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.
Causes of vitamin B-12 deficiency
Pernicious anemia is a type of vitamin B12 anemia. The body needs vitamin B12 to make red blood cells. You get this vitamin from eating foods such as meat, poultry, shellfish, eggs, and dairy products.
A special protein, called intrinsic factor (IF), helps your intestines absorb vitamin B12. This protein is released by cells in the stomach. When the stomach does not make enough intrinsic factor, the intestine cannot properly absorb vitamin B12.
Common causes of pernicious anemia include:
- Weakened stomach lining (atrophic gastritis)
- An autoimmune condition in which the body’s immune system attacks the actual intrinsic factor protein or the cells in the lining of your stomach that make it.
Very rarely, pernicious anemia is passed down through families. This is called congenital pernicious anemia. Babies with this type of anemia do not make enough intrinsic factor. Or they cannot properly absorb vitamin B12 in the small intestine.
In adults, symptoms of pernicious anemia are usually not seen until after age 30. The average age of diagnosis is age 60.
You are more likely to develop this disease if you:
- Are Scandinavian or Northern European
- Have a family history of the condition
Certain diseases can also raise your risk. They include:
- Addison disease
- Chronic thyroiditis
- Graves disease
- Hypoparathyroidism
- Hypopituitarism
- Myasthenia gravis
- Secondary amenorrhea
- Type 1 diabetes
- Testicular dysfunction
- Vitiligo
Possible complications of pernicious anemia
People with pernicious anemia may have gastric polyps. They are also more likely to develop gastric cancer and gastric carcinoid tumors.
Brain and nervous system problems may continue or be permanent if treatment is delayed.
A woman with a low B12 level may have a false positive Pap smear. This is because vitamin B12 deficiency affects the way certain cells (epithelial cells) in the cervix look.
Symptoms
Some people do not have symptoms. Symptoms may be mild.
They can include:
- Desire to eat ice or other non-food things (pica)
- Diarrhea or constipation
- Fatigue, lack of energy, or lightheadedness when standing up or with exertion
- Loss of appetite
- Pale skin
- Problems concentrating
- Shortness of breath, mostly during exercise
- Swollen, red tongue or bleeding gums
If you have a low vitamin B12 level for a long time, you can have nervous system damage. Symptoms can include:
- Confusion
- Depression
- Loss of balance
- Numbness and tingling in the hands and feet
Exams and Tests
The health care provider will perform a physical exam. Tests that may be done include:
- Bone marrow examination (only needed if diagnosis is unclear)
- Complete blood count (CBC)
- Reticulocyte count
- Schilling test
- LDH level
- Methylmalonic acid (MMA) level
- Vitamin B12 level
- Levels of antibodies against IF or the cells which make IF
Treatment
The goal of treatment is to increase your vitamin B12 level:
- Treatment involves a shot of vitamin B12 once a month. People with severely low levels of B12 may need more shots in the beginning.
- Some people may also need to take vitamin B12 supplements by mouth.
- A certain type of vitamin B12 may be given through the nose.
Your provider will also recommend eating a variety of foods.
Outlook (Prognosis)
Most people often do well with treatment.
It is important to start treatment early. Nerve damage can be permanent if treatment does not start within 6 months of symptoms.
Folic acid deficiency anemia
Folate, also known as vitamin B-9, is a nutrient found mainly in fruits and leafy green vegetables. A diet consistently lacking in these foods can lead to a deficiency. Folate deficiency means you have a lower-than-normal amount of folic acid, in your blood.
An inability to absorb folate from food also can lead to a deficiency. Most nutrients from food are absorbed in your small intestine. People with diseases of the small intestine, such as celiac disease, or those who have had a large part of the small intestine surgically removed or bypassed may have difficulty absorbing folate or its synthetic form, folic acid. Alcohol decreases absorption of folate, so drinking alcohol to excess may lead to a deficiency. Certain prescription drugs, such as some anti-seizure medications, can interfere with absorption of this nutrient.
Pregnant women and women who are breast-feeding have an increased demand for folate, as do people undergoing hemodialysis for kidney disease. Failure to meet this increased demand can result in a deficiency.
Causes of folic acid deficiency
Folic acid (vitamin B9) works with vitamin B12 and vitamin C to help the body break down, use, and make new proteins. The vitamin helps form red and white blood cells. It also helps produce DNA, the building block of the human body, which carries genetic information.
Folic acid is a water-soluble type of vitamin B. This means it is not stored in the fat tissues of the body. Leftover amounts of the vitamin leave the body through the urine.
Because folate is not stored in the body in large amounts, your blood levels will get low after only a few weeks of eating a diet low in folate. Folate is found in green leafy vegetables and liver.
Contributors to folate deficiency include:
- Diseases in which folic acid is not well absorbed in the digestive system (such as Celiac disease or Crohn disease)
- Drinking too much alcohol
- Eating overcooked fruits and vegetables. Folate can be easily destroyed by heat.
- Hemolytic anemia
- Certain medicines (such as phenytoin, sulfasalazine, or trimethoprim-sulfamethoxazole)
- Eating an unhealthy diet that does not include enough fruits and vegetables
- Kidney dialysis
Prevention
The best way to get vitamins your body needs is to eat a balanced diet. Most people in the United States eat enough folic acid because it is plentiful in the food supply.
Folate occurs naturally in the following foods:
- Beans and legumes
- Citrus fruits and juices
- Dark green leafy vegetables such as spinach, asparagus, and broccoli
- Liver
- Mushrooms
- Poultry, pork, and shellfish
- Wheat bran and other whole grains
The Institute of Medicine Food and Nutrition Board recommends that adults get 400 µg of folate daily. Women who may become pregnant should take folic acid supplements to ensure that they get enough each day.
Specific recommendations depend on a person’s age, gender, and other factors (such as pregnancy and lactation). Many foods, such as fortified breakfast cereals, now have extra folic acid added to help prevent birth defects.
Symptoms
Folic acid deficiency may cause:
- Fatigue, irritability, or diarrhea
- Poor growth
- Smooth and tender tongue
Diagnosis
Folate deficiency can be diagnosed with a blood test. Pregnant women commonly have this blood test at prenatal checkups.
Possible complications
Complications include:
- Anemia (low red blood cell count)
- Low levels of white blood cells and platelets (in severe cases)
In folate-deficiency anemia, the red blood cells are abnormally large (megaloblastic).
Pregnant women need to get enough folic acid. The vitamin is important to the growth of the fetus’s spinal cord and brain. Folic acid deficiency can cause severe birth defects known as neural tube defects. The Recommended Dietary Allowance (RDA) for folate during pregnancy is 600 micrograms (µg)/day.
Treatment
Treatment involves eating a healthy diet and taking folic acid supplements as prescribed by your doctor. In most cases, folic acid supplements are taken orally. Once your body’s level of folate increases to normal, you may be able to stop taking the supplements. But if the cause of your folate deficiency can’t be corrected, you may need to take folic acid supplements indefinitely.
Aplastic Anemia
Aplastic anemia is a rare disease caused by a decrease in the number of all types of blood cells that bone marrow produces. Normally, the bone marrow produces a sufficient number of new red blood cells (red blood cells), white blood cells (WBCs), and platelets for normal body function. Each type of cell enters the blood, circulates, and then dies within a certain time frame. For example, the normal lifespan of red blood cells is about 120 days. If the bone marrow is not able to produce enough blood cells to replace those that die, a number of symptoms, including those due to anemia, may result. This form of anemia can be severe or even fatal.
Symptoms of aplastic anemia can appear abruptly or can develop more slowly. Some general symptoms that are common to different types of anemia may appear first and are due to the decrease in number of red blood cells.
Some additional signs and symptoms that occur with aplastic anemia include those due to decreased platelets (thrombocytopenia):
- Prolonged bleeding
- Frequent nosebleeds and bleeding gums
- Easy bruising
- Pinpoint red spots on skin
- Blood in the stool
- Heavy menstrual bleeding
There may also be signs and symptoms due to a low white blood cell (WBC) count:
- Increased frequency and severity of infections
- Fever
Aplastic anemia causes
Causes of aplastic anemia usually have to do with damage to the stem cells in the bone marrow that are responsible for blood cell production. Some factors that may be involved with bone marrow damage and that can lead to aplastic anemia include:
- Exposure to toxic substances like arsenic, benzene (found in gasoline), or pesticides
- Cancer therapy (radiation or chemotherapy)
- Autoimmune disorders such as lupus or rheumatoid arthritis
- Viral infections such as hepatitis, HIV, EBV, or CMV
- Medicines such as chloramphenicol (an antibiotic rarely used in the U.S.)
Rarely, aplastic anemia is due to an inherited (genetic) disorder such as Fanconi anemia. Other genetic disorders leading to aplastic anemia include Shwachman-Diamond syndrome and dyskeratosis congenita.
Laboratory Tests
The initial test for anemia, the complete blood count (CBC), may reveal many abnormal results.
- Hemoglobin and/or hematocrit may be low.
- Red blood cell and white blood cell (WBC) counts are low.
- Platelet count is low.
- Red blood cell indices are usually normal.
- The differential white blood count shows a decrease in most types of cells but not lymphocytes.
Some additional tests that may be performed to help determine the type and cause of anemia include:
- Reticulocyte count—result is low
- Erythropoietin—usually increased in aplastic anemia
- Bone marrow aspiration or biopsy will show a decrease in the number of all types of cells.
- Tests for infections such as hepatitis, HIV, EBV, CMV help to determine the cause.
- Tests for arsenic (a heavy metal) and other toxins
- Iron tests or tests for vitamin B12 may be done to rule out other causes.
- ANA (antinuclear antibody) —to determine if the cause is autoimmune disease
Aplastic anemia treatment
A physical examination or complete medical history may reveal possible causes for aplastic anemia, such as exposure to toxins or certain drugs (e.g., chloramphenicol) or prior treatment for cancer. Some cases of aplastic anemia are temporary while others have lasting damage to the bone marrow. Therefore, the treatment depends on the cause. Reducing or eliminating exposure to certain toxins or drugs may help resolve the condition. Medications may be given to stimulate bone marrow production, to treat infections, or to suppress the immune system in cases of autoimmune disorders. Blood transfusions and a bone marrow transplant may be needed in severe cases.
MCV low
Microcytosis (low MCV) is 50 to 82 mm³
Microcytosis (low MCV) is found in iron deficiency anaemia, some cases of anaemia of chronic disease, haemoglobinopathies (especially the Thalassaemias), lead toxicity, congenital sideroblastosis and rare red cell enzyme deficiencies.
Low MCV common causes
- Iron deficiency anemia.
- Thalassemia.
- Chronic diseases.
Iron deficiency anemia
Iron deficiency anemia occurs when your body does not have enough iron. Iron helps make red blood cells. Iron deficiency anemia is the most common form of anemia.
Causes
Red blood cells bring oxygen to the body’s tissues. Healthy red blood cells are made in your bone marrow. Red blood cells circulate through your body for 3 to 4 months. Parts of your body, such as your spleen, remove old blood cells.
Iron is a key part of red blood cells. Without iron, the blood cannot carry oxygen effectively. Your body normally gets iron through your diet. It also reuses iron from old red blood cells.
Iron deficiency anemia develops when your body’s iron stores run low. This can occur because:
- You lose more blood cells and iron than your body can replace
- Your body does not do a good job of absorbing iron
- Your body is able to absorb iron, but you are not eating enough foods that contain iron
- Your body needs more iron than normal (such as if you are pregnant or breastfeeding)
Bleeding can cause iron loss. Common causes of bleeding are:
- Heavy, long, or frequent menstrual periods
- Cancer in the esophagus, stomach, small bowel, or colon
- Esophageal varices, often from cirrhosis
- The use of aspirin, ibuprofen, or arthritis medicines for a long time, which can cause gastrointestinal bleeding
- Peptic ulcer disease
The body may not absorb enough iron in your diet due to:
- Celiac disease
- Crohn disease
- Gastric bypass surgery
- Taking too many antacids that contain calcium
You may not get enough iron in your diet if:
- You are a strict vegetarian
- You are an older adult and do not eat a balanced diet
Prevention
A balanced diet should include enough iron. Red meat, liver, and egg yolks are high sources of iron. Flour, bread, and some cereals are fortified with iron. If advised by your provider, take iron supplements if you are not getting enough iron in your diet.
Symptoms
You may have no symptoms if the anemia is mild.
Most of the time, symptoms are mild at first and develop slowly. Symptoms may include:
- Feeling weak or tired more often than usual, or with exercise
- Headaches
- Problems concentrating or thinking
As the anemia gets worse, symptoms may include:
- Brittle nails
- Desire to eat ice or other non-food things (pica)
- Feeling lightheaded when you stand up
- Pale skin color
- Shortness of breath
- Sore tongue
Symptoms of the conditions that cause iron deficiency anemia include:
- Dark, tar-colored stools or blood in the stool
- Heavy menstrual bleeding (women)
- Pain in the upper belly (from ulcers)
- Weight loss (in people with cancer)
Diagnosis
To diagnose anemia, your health care provider may order these blood tests:
- Hematocrit and hemoglobin (red blood cell measures)
- RBC indices
- To check iron levels, your provider may order:
- Bone marrow biopsy (rarely done)
- Iron binding capacity (TIBC) in the blood
- Serum ferritin
- Serum iron level
To check for cause of iron deficiency, your provider may order:
- Colonoscopy
- Fecal occult blood test
- Upper endoscopy
Treatment
Treatment may include taking iron supplements and eating iron-rich foods.
Iron supplements (most often ferrous sulfate) build up the iron stores in your body. Most of the time, your provider will measure your iron level before you start supplements.
If you cannot take iron by mouth, you may need to take it through a vein (intravenous) or by an injection into the muscle.
Pregnant and breastfeeding women will need to take extra iron because they often cannot get enough iron from their normal diet.
Your hematocrit should return to normal after 2 months of iron therapy. You will need to keep taking iron for another 6 to 12 months to replace the body’s iron stores in the bone marrow.
Iron-rich foods include:
- Chicken and turkey
- Dried lentils, peas, and beans
- Fish
- Meats (liver is the highest source)
- Peanut butter
- Soybeans
- Whole-grain bread
Other sources include:
- Oatmeal
- Raisins, prunes, and apricots
- Spinach, kale, and other greens
Outlook (Prognosis)
With treatment, the outcome is likely to be good, but it does depend on the cause.
Thalassemia
Thalassemia is a name for a group of inherited blood disorders. When you have thalassemia, your body makes fewer healthy red blood cells and less hemoglobin than normal. Hemoglobin is an iron-rich protein in red blood cells. It allows the red blood cells to carry oxygen from your lungs to the rest of your body. Having not enough red blood cell hemoglobin is anemia. Anemia interferes with your body’s ability to move oxygen from your lungs to all of your organs and limbs. Thalassemias occur most often among people of Italian, Greek, Middle Eastern, Southern Asian, and African descent.
Thalassemias can be mild or severe. Some people have no symptoms or mild anemia. The most common severe type in the United States is called Cooley’s anemia. It usually appears during the first two years of life. People with it may have severe anemia, slowed growth and delayed puberty, and problems with the spleen, liver, heart, or bones.
Doctors diagnose thalassemias using blood tests. Treatments include blood transfusions and treatment to remove excess iron from the body. If you have mild symptoms or no symptoms, you may not need treatment. In some severe cases, you may need a bone marrow transplant.
Symptoms of thalassemia
Thalassemia symptoms depend on the type of thalassemia you have and how severe the anemia becomes. Some people have little or even no symptoms. Other people have mild to severe symptoms. Symptoms of thalassemia may include one or more of the following:
- Paleness
- Tiredness, low energy, or muscle weakness (also called fatigue)
- Lightheadedness or shortness of breath
- Lack of appetite
- Dark urine
- Jaundice (yellowing of the skin and the whites of the eyes)
- In children, slow growth and delayed puberty
- Bone deformities in the face
- Abdominal swelling
Children who are born with thalassemia may show signs of the disease right away, or symptoms may appear later. Most signs and symptoms usually show up within the first 2 years of life. If your child has delayed growth, it’s important to find out if he or she might have thalassemia. Untreated thalassemia can cause heart failure and infection.
Causes of thalassemia
You get thalassemia when you inherit gene mutations from one or both parents. These gene mutations cause you to lose red blood cells at a higher than normal rate and cause you to produce less hemoglobin.
The type of thalassemia you have depends on which mutated genes you inherit from your parents, and how many genes you inherit. There are 2 main types of thalassemia: alpha thalassemia and beta thalassemia. These are named after alpha-globin and beta-globin, the proteins that make up normal hemoglobin.
- Alpha thalassemia: This type of thalassemia involves 4 genes (you get 2 of these genes from your mother and 2 of these genes from your father). If you only get 1 mutated gene, you will have no signs or symptoms of thalassemia, but you can still pass on the gene mutation to your children (this is called being a “carrier”. If you get 2 mutated genes, you will have mild symptoms. If you get 3, you’ll have moderate to severe symptoms. A baby who inherits all 4 mutated genes will be very sick, and probably won’t live long after birth.
- Beta thalassemia: This type of thalassemia involves 2 genes (you get 1 gene from your mother and 1 gene from your father). If you get only 1 mutated gene, you’ll have mild signs or symptoms of thalassemia. If you get 2 mutated genes, you’ll have moderate to severe symptoms that usually develop in the first 2 years of life.
Who is at risk for thalassemia?
You are at risk for thalassemia if you have a family history of it. Thalassemia can affect both men and women. Certain ethnic groups are at greater risk:
Alpha thalassemia most often affects people who are of Southeast Asian, Indian, Chinese, or Filipino descent.
Beta thalassemia most often affects people who are of Mediterranean (Greek, Italian and Middle Eastern), Asian, or African descent.
Thalassemia diagnosis
If your doctor thinks you or your child might have thalassemia, he’ll do a physical exam and ask about your medical history. Thalassemia can only be diagnosed with blood tests. Doctors use several different types of blood tests to look for thalassemia. Some tests measure the number and size of red blood cells, or the amount of iron in the blood. Others look at the hemoglobin within the red blood cells. DNA testing helps doctors identify which genes are missing or damaged.
Treatment
Treatment for thalassemia depends on which type of thalassemia you have and the severity of your symptoms. If you have no or only mild symptoms, you may need little or no treatment.
Treatment for moderate to severe forms of thalassemia often includes regular blood transfusions and folate supplements. Folate (also called folic acid) helps your body make healthy blood cells. Alpha thalassemia can sometimes be mistaken for low-iron anemia, and iron supplements may be recommended as a treatment. But iron supplements have no effect on thalassemia.
If you have many blood transfusions, too much iron may build up in your blood. If this happens, you will need chelation therapy to remove extra iron from your body. You shouldn’t take iron supplements if you receive blood transfusions.
In the most severe cases, bone marrow or stem cell transplants may help by replacing damaged cells with healthy ones from a donor (usually a relative such as a brother or sister).
How can I cope with thalassemia?
Although you can’t prevent inheriting thalassemia, you can manage the disease so you can have the best quality of life possible. Key steps include:
- Follow your treatment plan. Get blood transfusions as often as your doctor recommends. Make sure to take your iron chelation medicine and/or folic acid supplements.
- Get ongoing medical care. Have regular medical checkups and get the medical tests your doctor suggests. These may include tests relating to thalassemia, as well as your overall health. Be sure to get any vaccinations for flu, pneumonia, hepatitis B and meningitis that your doctor recommends.
- Take care of yourself. Follow a healthy eating plan. Lower your chance of getting an infection by washing your hands often, and avoiding crowds during flu and cold season. Keep the area around your transfusion site clean. Call your doctor if you develop a fever or other signs of infection.
- Look for information and support. Join a support group or talk with others who have the disease to learn coping strategies. Be sure to discuss any changes in your treatment plan with your doctor.
Complications of thalassemia
Thalassemia can lead to other health problems:
- An enlarged spleen. Your spleen helps your body fight infections and filters out damaged blood cells. If you have thalassemia, your spleen may have to work harder than normal, which can cause it to enlarge. If your spleen becomes too large, it may have to be removed.
- Infections. People who have thalassemia are more likely to get blood infections, especially if they have a lot of blood transfusions. Some types of infection can be worse if you’ve had your spleen removed.
- Bone problems. Thalassemia can cause bone deformities in the face and skull. People who have thalassemia may also have severe osteoporosis (brittle bones).
- Too much iron in your blood. This can cause damage to the heart, liver, or endocrine system (glands in the body that make hormones, like the thyroid gland and adrenal glands).
What should I do if I’m a carrier of thalassemia and I want to get pregnant?
Some severe types of thalassemia can cause babies to die before they are born or soon after. If you or your partner knows you are a carrier for thalassemia, you may want to talk to your doctor or a genetic counselor before getting pregnant. Certain tests may be able to show which type of thalassemia you are carrying. Once you are pregnant, prenatal testing can show whether or not your baby has thalassemia.
Anemia of chronic disease
Some chronic (long-term) illnesses can cause anemia. Often, anemia caused by chronic diseases goes undetected until a routine test such as a complete blood count (CBC) reveals abnormal results. Several follow-up tests may be used to determine the underlying cause. There are many chronic conditions and diseases that can result in anemia. Some examples of these include:
- Kidney disease—red blood cells are produced by the bone marrow in response to a hormone called erythropoietin, made primarily by the kidneys. Chronic kidney disease can cause anemia resulting from too little production of this hormone; the anemia can be treated by giving erythropoietin injections.
- Anemia of chronic disease—whenever there are chronic diseases that stimulate the body’s inflammatory response, the ability of the bone marrow to respond to erythropoietin is decreased, mainly due to impairment in body iron regulation. For example, rheumatoid arthritis (a severe form of joint disease caused by the body attacking its own joints, called an autoimmune disease) can cause anemia by this mechanism. Other diseases that can produce anemia in the same way include chronic infections such as HIV or tuberculosis (TB).
Anemia of chronic disease laboratory tests
A number of tests may be used as follow up to abnormal results of initial tests such as a CBC and blood smear to determine the underlying cause of chronic anemia. Some of these may include:
- Reticulocyte count—will typically be low
- Comprehensive metabolic panel—used to detect evidence of chronic disorders
Tests for anemia of chronic disease may include:
- Tests for inflammation such as C-Reactive Protein (CRP)
- Erythropoietin—is typically mildly increased
- Tests for infections such as HIV and TB
- Iron and transferrin (TIBC)—are typically both low
- Soluble transferrin receptor (sTfR)—is typically normal or low
Anemia of chronic disease treatment
Treatment of anemia due to chronic conditions usually involves determining and/or resolving the underlying disease. Blood transfusions may be used to treat the condition in the short term.
Normal MCV Anemia
Rarely, anemia is due to problems that cause the red blood cells (RBCs) to die or be destroyed prematurely. Normally, red blood cells live in the blood for about four months. In hemolytic anemia, this time is shortened, sometimes to only a few days. The bone marrow is not able to produce new red blood cells quickly enough to replace those that have been destroyed, leading to a decreased number of red blood cells in the blood, which in turn leads to a diminished capacity to supply oxygen to tissues throughout the body. This results in the typical symptoms of anemia.
Depending on the cause, hemolytic anemia can be chronic, developing and lasting over a long period or lifetime, or may be acute. The various forms can have a wide range of signs and symptoms. See the discussions of the various types below for more on this.
The different causes of hemolytic anemia fall into two main categories:
- Inherited forms in which a gene or genes are passed from one generation to the next that result in abnormal red blood cells or hemoglobin
- Acquired forms in which some factor results in the early destruction of red blood cells
Inherited Hemolytic Anemia
Two of the most common causes of inherited hemolytic anemia are sickle cell anemia and thalassemia:
Sickle cell anemia is a disorder where the body makes abnormal hemoglobin, which in turn causes red blood cells to become crescent-shaped, sickle cells under certain conditions. The “trait” (when you carry one mutated gene from one of your parents) can cause minor difficulties; the “disease” (when you carry two mutated genes, one from each of your parents) causes severe clinical problems. Misshapen blood cells are unstable (leading to hemolysis) and can block blood vessels, causing pain and anemia. Newborns are usually screened for sickle cell anemia, particularly those of African descent, because they are more likely to possess the inherited trait. Sometimes screening is done prenatally on a sample of amniotic fluid. Follow-up tests for hemoglobin variants may be performed to confirm a diagnosis. Treatment is usually based on the type, frequency, and severity of symptoms.
Other less common types of inherited forms of hemolytic anemia include:
- Hereditary spherocytosis—results in abnormally shaped red blood cells (so called spherocytes) that may be seen on a blood smear. These cells are very rigid, cannot pass through the spleen as normal red cells would, and thus get destroyed prematurely.
- Hereditary elliptocytosis—another cause of abnormally oval-shaped red blood cells seen on a blood smear.
- Glucose-6-phospate dehydrogenase (G6PD) deficiency—G6PD is an enzyme that is necessary for red blood cell survival and, if deficient, red blood cells come into contact with certain substances in the blood, the cells rupture and get destroyed. Those substances could include naphthalene, antimalarial medications, or fava beans. G6PD deficiency may be diagnosed with a test for its activity.
- Pyruvate kinase deficiency—pyruvate kinase is another enzyme important for red blood cell survival and its deficiency causes significant anemia. It is a rare disease that may be diagnosed with a test for the enzyme activity.
Inherited Hemolytic Anemia Laboratory Tests
Since some of these inherited forms may have mild symptoms, they may first be detected on a routine complete blood count (CBC) and blood smear, which can reveal various abnormal results that give clues as to the cause. Follow-up tests are then usually performed to make a diagnosis. Some of these include:
- Hemoglobinopathy evaluation
- DNA analysis—not routinely done but can be used to help diagnose hemoglobin variants, thalassemia, and to determine carrier status
- Glucose-6-phospate dehydrogenase (G6PD) test—to detect deficiency in this enzyme
- Osmotic fragility test—detects red blood cells that are more fragile than normal, which may be found in hereditary spherocytosis
These genetic disorders cannot be cured, but often the symptoms resulting from the anemia may be alleviated with treatment as necessary.
Acquired Hemolytic Anemia
Some of the conditions or factors involved in acquired forms of hemolytic anemia include:
- Autoimmune disorders—conditions in which the body produces antibodies against its own red blood cells; it is not well understood why this may happen, but it accounts for about half of all cases of hemolytic anemia. Certain diseases such as lupus, HIV and hepatitis can increase a person’s risk for it.
- Transfusion reaction—result of blood donor-recipient incompatibility; this occurs very rarely, but when it does, it can have some serious complications.
- Infections, such as malaria and infectious mononucleosis (mono)
- Mother-baby blood group incompatibility—may result in hemolytic disease of the newborn
- Medications—certain medications such as penicillin can trigger the body to produce antibodies directed against red blood cells or cause the direct destruction of red blood cells.
- Physical destruction of red blood cells by, for example, an artificial heart valve or cardiac bypass machine used during open-heart surgery
- Paroxysmal Nocturnal Hemoglobinuria (PNH)—a rare condition in which the different types of blood cells including red blood cells, white blood cells, and platelets are abnormal due to lack of certain surface proteins; because the red blood cells are defective, the body destroys them earlier than the normal lifespan. This disease occurs due to a change or mutation in a gene called PIGA in the stem cells that make blood. Though it is a genetic disorder, it is not passed from one generation to the next (it is not an inherited condition). Those affected will often pass dark urine due to the hemoglobin released by destroyed red blood cells being cleared from the body by the kidneys. This is most noticeable first thing in the morning when urine is most concentrated.
Acquired Hemolytic Anemia Laboratory Tests
Hemolytic anemias are often first identified by signs and symptoms, during physical examination, and by medical history. A medical history can reveal, for example, a recent transfusion, treatment with penicillin, or cardiac surgery. A complete blood count (CBC) and/or blood smear may show various abnormal results. Depending on those findings, additional follow-up tests may be performed. Some of these may include:
- Tests for autoantibodies for suspected autoimmune disorders
- Direct antiglobulin test in the case of transfusion reaction, mother-baby blood type incompatibility, or autoimmune hemolytic anemia
- Haptoglobin—usually low
- Reticulocyte count—typically high
- Flow cytometry for suspected Paroxysmal Nocturnal Hemoglobinuria (PNH)
Hemolytic anemia treatment
Treatments for hemolytic anemia are as varied as the causes. However, the goals are the same: to treat the underlying cause of the anemia, to decrease or stop the destruction of red blood cells, and to increase the red blood cell count and/or hemoglobin level to alleviate symptoms. This may involve, for example:
- Drugs used to suppress production of autoantibodies that destroy red blood cells
- Blood transfusions to increase the number of healthy red blood cells
- Bone marrow transplant—to increase production of normal red blood cells
- Avoiding triggers that cause the anemia such as the cold in some forms of autoimmune hemolytic anemia or fava beans, naphthalene and certain medicines for those with G6PD deficiency.
- Sarma PR. Red Cell Indices. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 152. Available from: https://www.ncbi.nlm.nih.gov/books/NBK260[↩]





{kind=link}