
Contents
- What is microdermabrasion
- Microdermabrasion benefits
- Microdermabrasion side effects
- Microdermabrasion Preparation
- Microdermabrasion treatment
- What happens during microdermabrasion?
- What will I need to do after microdermabrasion?
- Is there downtime with microdermabrasion?
- When will I see results from microdermabrasion?
- How long will the microdermabrasion results last?
- What are the possible side effects of microdermabrasion?
- How often can I safely get another microdermabrasion treatment?
- What is the safety record for microdermabrasion?
- The Skin
- What does microdermabrasion do
What is microdermabrasion
Microdermabrasion is a nonsurgical, office‐based cosmetic procedure that uses fine crystals (usually aluminium oxide Al2O3 sodium chloride or salt) and a closed‐loop vacuum to remove dead skin cells on the face. The aim of microdermabrasion is to reduce the effect of fine lines and minor skin blemishes. Microdermabrasion works on all skin types and shouldn’t cause any skin color changes or scarring. Microdermabrasion has the advantages of low risk and rapid recovery compared with other techniques such as standard dermabrasion, chemical peeling and laser resurfacing. However, be aware that microdermabrasion can be expensive and has its limitations. Take time to find a reputable practitioner who is properly qualified and practices in a clean, safe and appropriate environment. Ask the practitioner what you should do if something were to go wrong.
Microdermabrasion is an U.S. Food and Drug Administration approved process first introduced in Italy in 1985 and is a popular method used to treat superficial scars, acne, to reduce the appearance of large pores, fine lines, wrinkles, tattoos, severe sun damage, pigmentation disorders and other cosmetic-dermatologic conditions 1.
Microdermabrasion works for:
- Dull complexion.
- Uneven skin tone or texture.
- Fine lines and wrinkles.
- Age spots.
- Dark spots that can appear when acne starts to clear.
- Melasma.
The disadvantages of microdermabrasion are that multiple treatments are needed and there may be minimal improvement in appearance.
Microdermabrasion is now possible using home kits that use virbating foam applicator to massage a moisturizing cream containing aluminium oxide crystals on the surface of the skin. However, the microdermabrasion that a dermatologist performs differs from the one that you can do at home with a kit. A dermatologist treatment goes a bit deeper into the skin. Still, the procedure is safe for all skin colors.
Dermatologists also use microdermabrasion to improve the results gained from using anti-aging products and skin-bleaching products. Microdermabrasion allows these products to penetrate the skin more easily. Because stratum corneum is the skin’s main permeability barrier, controlled microdermabrasion offers a novel approach to increasing rates of transdermal drug delivery. By using microdermabrasion on the skin, topical therapeutics can be applied at the conclusion of the treatment, which will reach levels much deeper than when typically applied to the surface of the skin, as the skin barrier function of the stratum corneum is temporarily compromised 2. Therefore, slightly greater improvements in the histological features of photoaging can be achieved with the combination of microdermabrasion followed by a 5% retinoic acid chemical peel versus a 5% retinoic acid chemical peel administered alone 3. The established clinical safety record and the non-invasive nature of microdermabrasion suggest that this approach should be safe, painless, cosmetically acceptable and effective to deliver a broad range of pharmaceutical compounds.
This study 4 showed that controlled microdermabrasion can be used to selectively remove stratum corneum (outermost layer of the skin) in a targeted fashion without removing viable epidermis. Crystal flow rate and exposure time were the most important parameters in controlling stratum corneum removal, whereas suction pressure and handpiece movement had lesser effects. Notably, this study 4 added the use of a mask (see Figure 3 C below) to limit tissue removal to an array of micron-scale pores rather than one large region of stratum corneum removal. The study authors found that the mask also influenced the depth of tissue removal; the 125 μm-hole mask limited tissue removal to the stratum corneum in a self-limiting manner independent of exposure time to microdermabrasion.
Although microdermabrasion is a gentle, non-invasive treatment, you should see a dermatologist before getting this treatment at a spa or using an at-home microdermabrasion kit if you:
- Have a mole or other spot on your skin that is growing, bleeding, or changing in any way. This spot could be a skin cancer.
- Are taking (or have taken) the acne medicine, isotretinoin, which is prescribed to treat severe acne. If you have taken this medicine within the past 6 months, you have a higher risk for complications, including scarring. You may need to wait before having microdermabrasion.
- Scar easily.
Microdermabrasion benefits
Microdermabrasion is similar to dermabrasion but as its name suggests, it uses tiny crystals to remove the surface skin layers. It is promoted for correcting fine lines and more superficial scars.
Microdermabrasion advantages include:
- Anaesthesia is not required
- It is almost painless
- Facial redness is minimized
- Simple and quick to perform
- Can be repeated at short intervals
- Does not disrupt the patient’s life greatly
Microdermabrasion side effects
The side effects of microdermabrasion, such as redness and swelling, tend to be short-lived.
Your skin may be dry and flaky for a few days after the procedure, and the suction may temporarily bruise your skin.
Your face would be more sensitive to the sun afterwards, so you should avoid sun exposure for a few days and use broad-spectrum SPF30+ sunscreen.
If you’re not happy with the results or are experiencing problems, take up the matter with your practitioner through the clinic where you were treated.
If there are any complications that require medical attention, it is best that you go back to the practitioner who treated you. If this is not possible, you can go to your doctor or local accident and emergency (A&E) department.
Microdermabrasion Preparation
To protect your health and find out what results you want, a dermatologist always offers a consultation before performing microdermabrasion. To help you get the most benefit from this consultation, you should:
- Ask questions.
- Gather important information before your consultation.
Asking questions will help you know what to expect so that you can make an informed decision.
Before having microdermabrasion, the American Academy of Dermatology recommends that you ask the following questions:
- Who will perform the microdermabrasion?
- What results can I expect?
- How many treatments will I need to get these results?
- What are the potential side effects?
- Do I have a higher risk for any side effects?
- May I see before-and-after photos or speak with patients who have been treated with microdermabrasion?
- How much will the treatment cost?
During the consultation, your dermatologist will examine your skin. This helps to determine whether microdermabrasion can diminish the signs of aging that concern you. You may learn that another cosmetic treatment is more appropriate.
Vital information to tell your dermatologist
Before having microdermabrasion, you should tell your dermatologist about all your medical conditions and medicines that you take. It is especially important for your dermatologist to know if you have:
- Cold sores breakouts.
- Skin that scars easily.
- Taken isotretinoin, a medicine prescribed to treat severe acne.
When your dermatologist asks about your medications, be sure to tell your dermatologist about all medicines that you take, even ones that do not require a prescription. Be sure to mention all vitamins, minerals, and herbal remedies.
If microdermabrasion is appropriate, your dermatologist will tell you what you can expect.
Microdermabrasion treatment
You may be given medication to relax you before the procedure begins. Local anaesthetic isn’t necessary.
The practitioner uses a handheld device to direct a fine stream of tiny crystals across the skin to loosen any dead cells and vacuum them away.
The procedure usually takes less than 40 minutes. A course of four to six sessions may be recommended.
Microdermabrasion shouldn’t be painful.
Insurance does not cover microdermabrasion treatment that reduces signs of aging or only improves a person’s appearance.
What happens during microdermabrasion?
The dermatologist uses a handheld device that gently removes the top layer of skin. You may feel a sanding sensation, but this is not painful. It takes about 30 to 40 minutes to treat the entire face and about 20 minutes to treat the neck.
After the treatment, a moisturizer is applied.
What will I need to do after microdermabrasion?
You may need to apply a moisturizer or other skin care product at home.
You will be given a skin-care plan that includes sun protection. Protecting your skin form the sun helps ensure the best possible results and reduces the risk of side effects.
Is there downtime with microdermabrasion?
You will not have downtime or a recovery period. Some patients’ skin turns pink or red. The skin can swell a bit. These side effects are similar to having a sunburn or windburn for a day or two. During this time, some patients feel uncomfortable returning to work or being in public.
When will I see results from microdermabrasion?
Most patients need a series of treatments to see results. To treat signs of aging, a dermatologist may treat a patient weekly, every two weeks, or monthly. Most patients receive between 5 and 16 treatments.
After a series of treatments, patients usually say they have smoother skin and a more-radiant complexion.
How long will the microdermabrasion results last?
The microdermabrasion results tend to be temporary. Patients who protect their skin from the sun and follow the recommended skin-care plan will maintain their results for a longer time. Yet, no matter what you do, your skin continues to age. Follow-up treatments are usually necessary to help retain smoother skin and a more radiant complexion.
What are the possible side effects of microdermabrasion?
After microdermabrasion, your treated skin may be pink or red and slightly swollen. This tends to disappear within a day.
In some cases, the skin can bruise, burn, sting, or become extremely sensitive to sunlight. These will go away without treatment.
If your skin tends to develop dark spots after acne clears or a skin injury heals, you may have a greater risk of developing more dark spots. When microdermabrasion is performed by a dermatologist, this risk is minor.
How often can I safely get another microdermabrasion treatment?
Microdermabrasion treats only the top layer of the skin, so the skin recovers quickly. Most people can safely have another treatment a week later. Some patients, however, need several weeks to recover.
What is the safety record for microdermabrasion?
When performed by a dermatologist, microdermabrasion has an excellent safety record.
Microdermabrasion also is performed in salons and non-medical spas. You can reduce your risk for side effects by having microdermabrasion performed by a dermatologist.
The Skin
The skin (integument) is the body’s largest and heaviest organ. In adults, the skin covers an area of 1.5 to 2.0 m2 and accounts for about 15% of the body weight.
The skin consists of two layers:
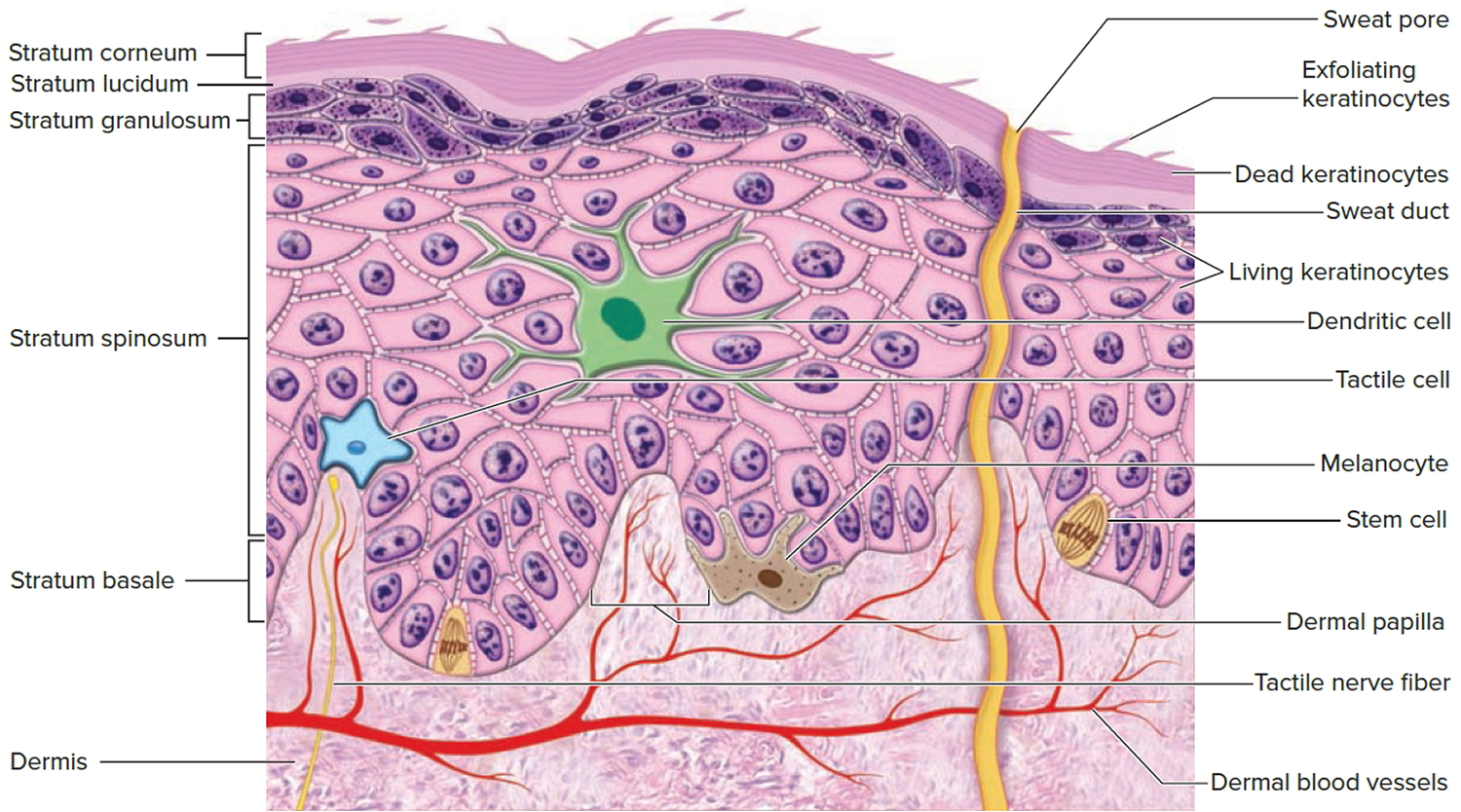
- a stratified squamous epithelium called the Epidermis (Figure 2) and
- a deeper connective tissue layer called the Dermis (Figure 1).
Figure 1. Skin structure

Below the dermis is another connective tissue layer, the hypodermis, which is not part of the skin but is customarily studied in conjunction with it. Most of the skin is 1 to 2 mm thick, but it ranges from less than 0.5 mm on the eyelids to 6 mm between the shoulder blades. The difference is due mainly to variation in thickness of the dermis, although skin is classified as thick or thin based on the relative thickness of the epidermis alone.
Thick skin covers the palms, soles, and corresponding surfaces of the fingers and toes. Its epidermis alone is about 0.5 mm thick, due to a very thick surface layer of dead cells called the stratum corneum (see Figure 2). Thick skin has sweat glands but no hair follicles or sebaceous (oil) glands. The rest of the body is covered with thin skin, which has an epidermis about 0.1 mm thick, with a thin stratum corneum. It possesses hair follicles, sebaceous glands, and sweat glands.
The accessory structures include hair, nails, and a variety of multicellular exocrine glands. These structures are located in the dermis and protrude through the epidermis to the surface.
Figure 2. Structure and skin cells of the Epidermis
What does microdermabrasion do
Microdermabrasion damages the stratum corneum by bombarding it with abrasive particles, such as alumina or sodium chloride, under vacuum 5. Damaging stratum corneum induces an inflammatory response that results in increased collagen remodeling and proliferation, which produces the positive cosmetic results seen after microdermabrasion treatment, such as noticeably firmer skin 6.
The microdermabrasion machine works by placing a handpiece on the skin, which occludes the opening of the plastic tip to create a vacuum. Upon tip occlusion, the crystals flow from the machine into the inlet port and abrade the skin. At the same time, the skin debris and used crystals are shunted back through the outlet port to the machine and collected in a waste container. This closed-loop system prevents cross-contamination between patients and exposure of medical personnel. Typically, patients undergo several sessions of microdermabrasion, depending on the severity of the skin condition, to improve the skin’s appearance 7. The microdermabrasion procedure is noninvasive, painless, and short, and requires no down time for recovery. Typically, microdermabrasion is performed at spas or by cosmetic surgeons or dermatologists. A picture of a microdermabrasion machine tip and the alumina crystals are shown in Figure 3A and 3B.
This study 4 showed the effect of crystal flow rate, suction pressure, exposure time, and handpiece movement on stratum corneum (outer most layer of the skin) removal and found that crystal flow rate and exposure time had the greatest impact on stratum corneum removal. Over the range of conditions studied, suction pressure had no significant effect. Both static and dynamic handpiece movements were effective 4. The study authors believe that the crystal flow rate was important because the crystals shear and tear the stratum corneum and, therefore, the number of times crystals impact the skin should correlate with the degree of tissue removal 8. The exposure time was also an important parameter for similar reasons; increased exposure time increased the number of crystal-skin impacts. The suction pressure, in contrast, had no significant effect on the crystal flow rate or velocity and, correspondingly, no significant effect on tissue removal. The study authors believe that the suction pressure serves to help remove skin debris and crystals from the skin surface and into the refuse canister of the microdermabrasion machine. In this way, suction is important to proper function of the microdermabrasion method, but it does not control the tissue removal process.
The importance of crystals in microdermabrasion has been shown in a previous study in which inclusion of crystals increased the expression of proteins needed for dermal remodeling, which is the primary purpose of conventional cosmetic microdermabrasion, as compared to suction pressure alone 9. However, suction pressure alone (i.e., without crystals) has been shown to remove stratum corneum at pressures of −20 to −40 kPa when the skin was exposed for 24 seconds 10. Although similar suction pressures were applied in this study 4 for up to similar periods of time (≤ 45 seconds static mode and ≤ 50 seconds dynamic mode), no stratum corneum removal was observed without significant crystal flow. While the different exposure times may play a role, the fact that a study used pig skin in laboratory setting and the study that removed stratum corneum with suction alone used human skin in vivo may also be relevant. Consistent with this expectation, a previous study with human skin in vivo found that static mode microdermabrasion at conditions that removed stratum corneum also caused microblisters (i.e., localized separation of epidermis from the underlying dermis) 11 but this was not observed in another study using pig skin in laboratory setting. This suggests that human skin in vivo may be more susceptible to suction-induced damage than pig skin in laboratory setting.
Both handpiece abrasion modes resulted in selective stratum corneum removal, however the dynamic mode appears to offer advantages [in addition to the lack of microblisters found previously 11]. For example, stratum corneum removal in the static experiments was not as uniform as in the dynamic experiments and the area of tissue removal is limited to that of the microdermabrasion tip (0.4 cm²). The dynamic mode enabled a larger area of removal (3 cm² in this study) and the results were more consistent 4. Additionally, the dynamic mode is typically used in the clinical setting for cosmetic microdermabrasion.
Use of a mask in combination with microdermabrasion limited both the area and depth of tissue removal. As discussed above, generating an array of small pores using a mask may be preferable from a safety, cosmetic and patient preference perspective compared to removing stratum corneum from large, continuous areas of skin. By selecting a mask hole diameter that was slightly smaller than the size of the crystal particles, the mask further served to limit the depth of tissue remove, such that 125-μm holes provided a self-limiting feature that achieved selective removal of stratum corneum independent of exposure time and using aggressive microdermabrasion operating parameters. In this way, the use of a mask was critically important, and arguably more important than the microdermabrasion operating parameters, to enable three-dimensional control over pore formation on the micron scale localized to the stratum corneum.
Figure 3. Microdermabrasion machine

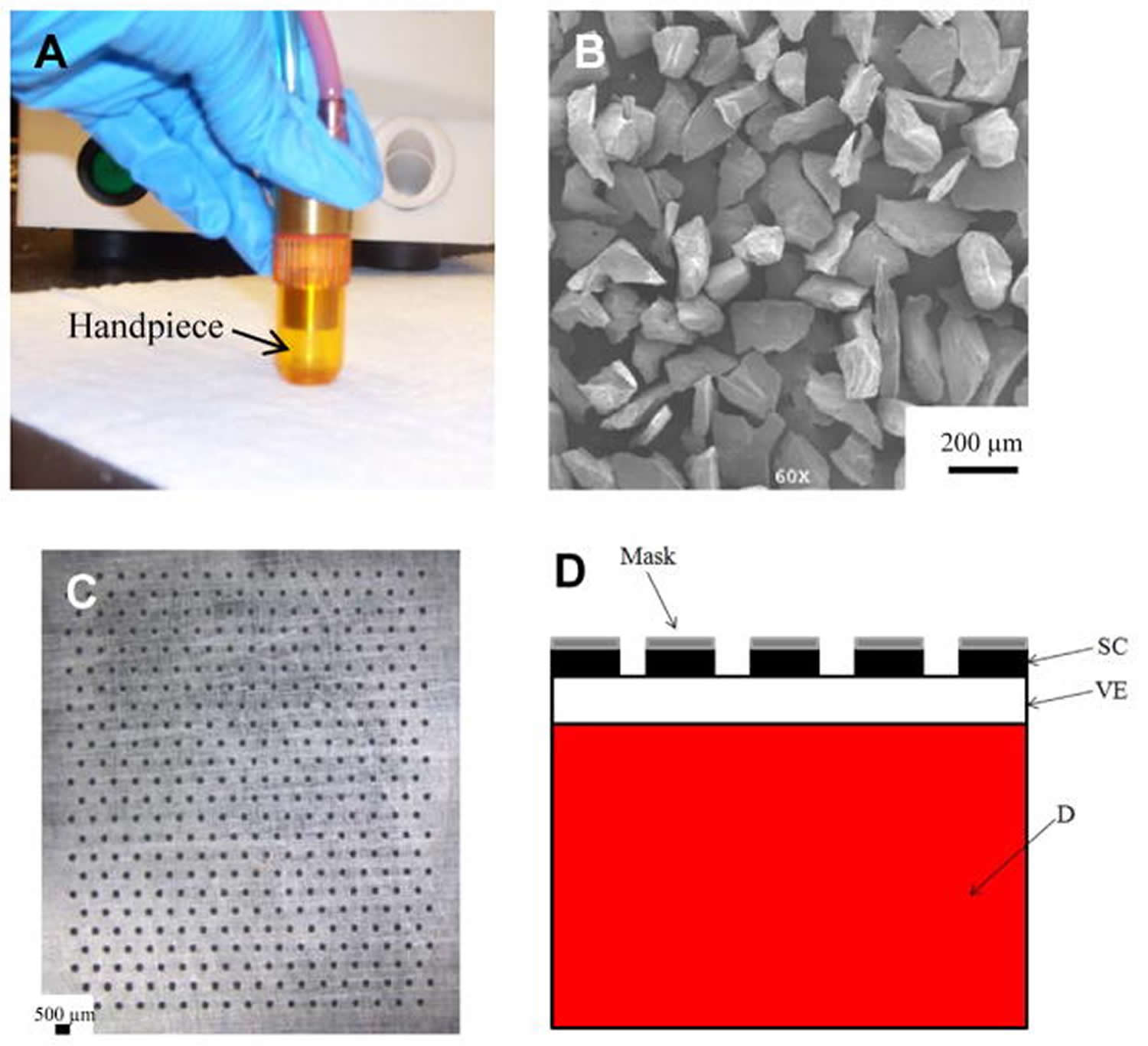 Footnotes: Microdermabrasion device and mask. (A) Microdermabrasion machine handpiece and (B) the alumina abrasion crystals (~100 μm in diameter). (C) Stainless steel mask with 408 holes (125 μm diameter). (D) Schematic diagram of the skin after abrasion with the mask, where the stratum corneum is selectively removed and the underlying layers are intact. SC = stratum corneum, VE = viable epidermis, and D = dermis.
Footnotes: Microdermabrasion device and mask. (A) Microdermabrasion machine handpiece and (B) the alumina abrasion crystals (~100 μm in diameter). (C) Stainless steel mask with 408 holes (125 μm diameter). (D) Schematic diagram of the skin after abrasion with the mask, where the stratum corneum is selectively removed and the underlying layers are intact. SC = stratum corneum, VE = viable epidermis, and D = dermis.
- Microdermabrasion: Reappraisal and brief review of literature. Bhalla M, Thami GP. Dermatol Surg. 2006 Jun; 32(6):809-14. https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1524-4725.2006.32165.x[↩]
- Microdermabrasion: an evidence-based review. Karimipour DJ, Karimipour G, Orringer JS. Plast Reconstr Surg. 2010 Jan; 125(1):372-7. https://www.ncbi.nlm.nih.gov/pubmed/20048628/[↩]
- Microdermabrasion followed by a 5% retinoid acid chemical peel vs. a 5% retinoid acid chemical peel for the treatment of photoaging – a pilot study. Hexsel D, Mazzuco R, Dal’Forno T, Zechmeister D. J Cosmet Dermatol. 2005 Jun; 4(2):111-6. https://www.ncbi.nlm.nih.gov/pubmed/17166209/[↩]
- Andrews SN, Zarnitsyn V, Brian B, Prausnitz MR. Optimization of Microdermabrasion for Controlled Removal of Stratum Corneum. International journal of pharmaceutics. 2011;407(1-2):95-104. doi:10.1016/j.ijpharm.2011.01.034. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3050026/[↩][↩][↩][↩][↩][↩]
- Skin barrier changes induced by aluminum oxide and sodium chloride microdermabrasion. Rajan P, Grimes PE. Dermatol Surg. 2002 May; 28(5):390-3. https://www.ncbi.nlm.nih.gov/pubmed/12030870/[↩]
- The epidermal and dermal changes associated with microdermabrasion. Freedman BM, Rueda-Pedraza E, Waddell SP. Dermatol Surg. 2001 Dec; 27(12):1031-3; discussion 1033-4. https://www.ncbi.nlm.nih.gov/pubmed/11849265/[↩]
- Microdermabrasion: a clinical and histopathologic study. Shim EK, Barnette D, Hughes K, Greenway HT. Dermatol Surg. 2001 Jun; 27(6):524-30. https://www.ncbi.nlm.nih.gov/pubmed/11442587/[↩]
- Bhalla M, Thami Gurvinder P. Microdermabrasion: Reappraisal and Brief Review of Literature. Am Soc of Dermatol Surg. 2006;32:809–814. https://www.ncbi.nlm.nih.gov/pubmed/16792646[↩]
- Karimipour DJ, KS, Johnson TM, Orringer JS, Hamilton T, Hammerberg C, Voorhees JJ, Fisher G. Microdermabrasion with and without aluminum oxide crystal abrasion: A comparative molecular analysis of dermal remodeling. J Am Acad of Derm. 2006;54:405–410. https://www.ncbi.nlm.nih.gov/pubmed/16488289[↩]
- Pedersen L, Jemec GBE. Mechanical properties and barrier function of healthy human skin. Acta Dermatol Venereol. 2006;86:308–311 https://www.ncbi.nlm.nih.gov/pubmed/16874414[↩]
- Gill HS, Andrews SN, Sakthivel SK, Fedanov A, Williams IR, Garber DA, Priddy FH, Yellin S, Feinberg MB, Staprans SI, Prausnitz MR. Selective removal of stratum corneum by microdermabrasion to increase skin permeability. Eur J Pharm Sci. 2009;38:95–103. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2731013/[↩][↩]





{kind=link}