
Contents
What is myringitis
Myringitis also called bullous myringitis, is an infection of the eardrum that causes painful blisters to form on the eardrum (tympanic membrane). Patients may collect fluid behind their the eardrum (tympanic membrane) or have a concomitant middle ear infection (acute otitis media). Bullous myringitis probably is not a separate clinical entity, but merely acute otitis media with blisters on the eardrum 1. Historically, Mycoplasma pneumoniae was described as causing bullous myringitis characterized by the presence of blistering or vesicles on the tympanic membrane 2. Recent data suggests that bullous myringitis is not specific for Mycoplasma and it is caused by common organisms of otitis media. A critical review of the literature concerning bullous myringitis has found one case of possible mycoplasma, one of possible viral, and 43 of bacterial, cause. The bacteria were Streptococcus pneumoniae, Haemophilus influenzae, and beta-hemolytic Streptococcus, in the same percentages as found in (nonbullous) otitis media 1.
Figure 1. Middle ear anatomy
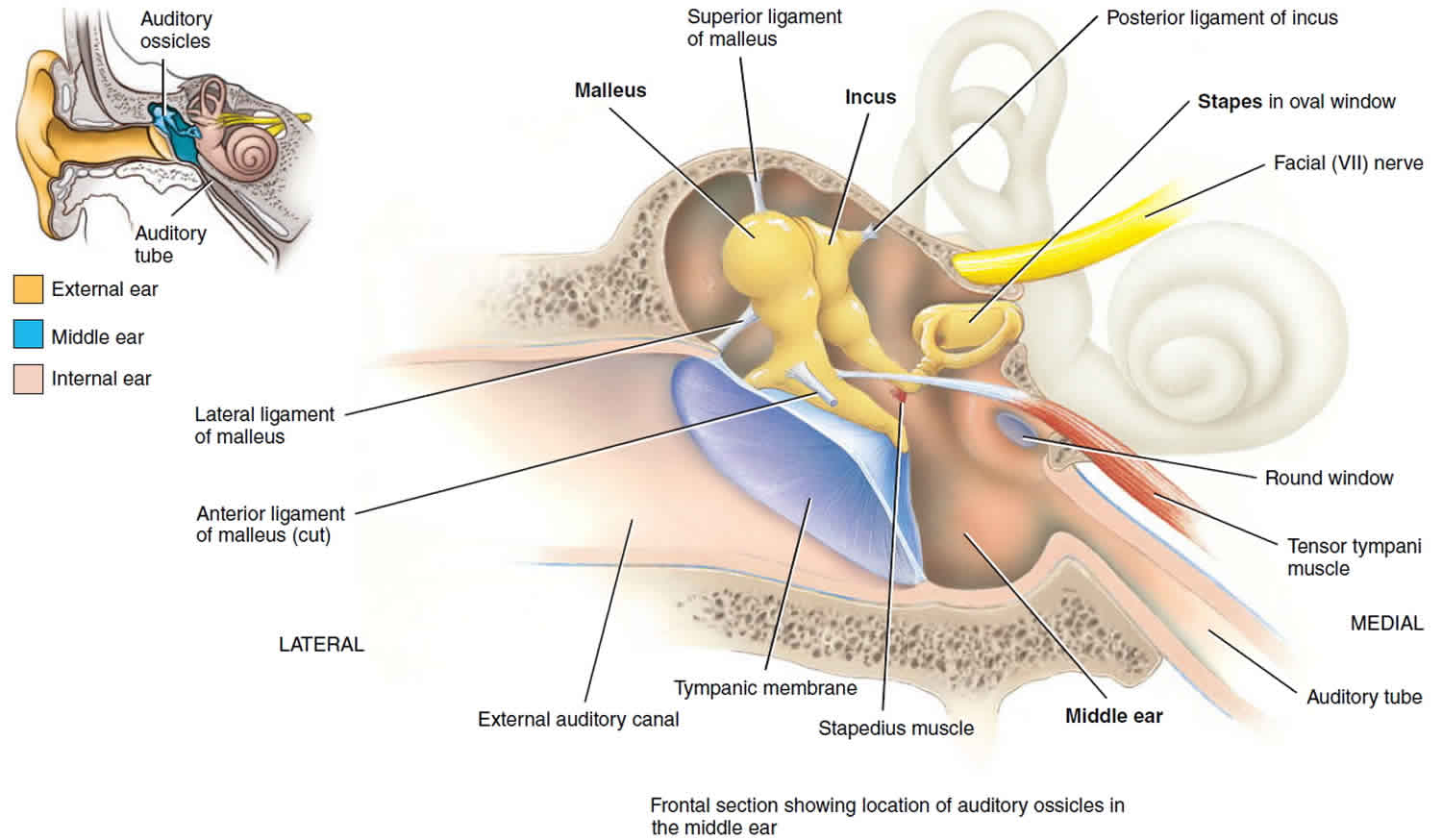
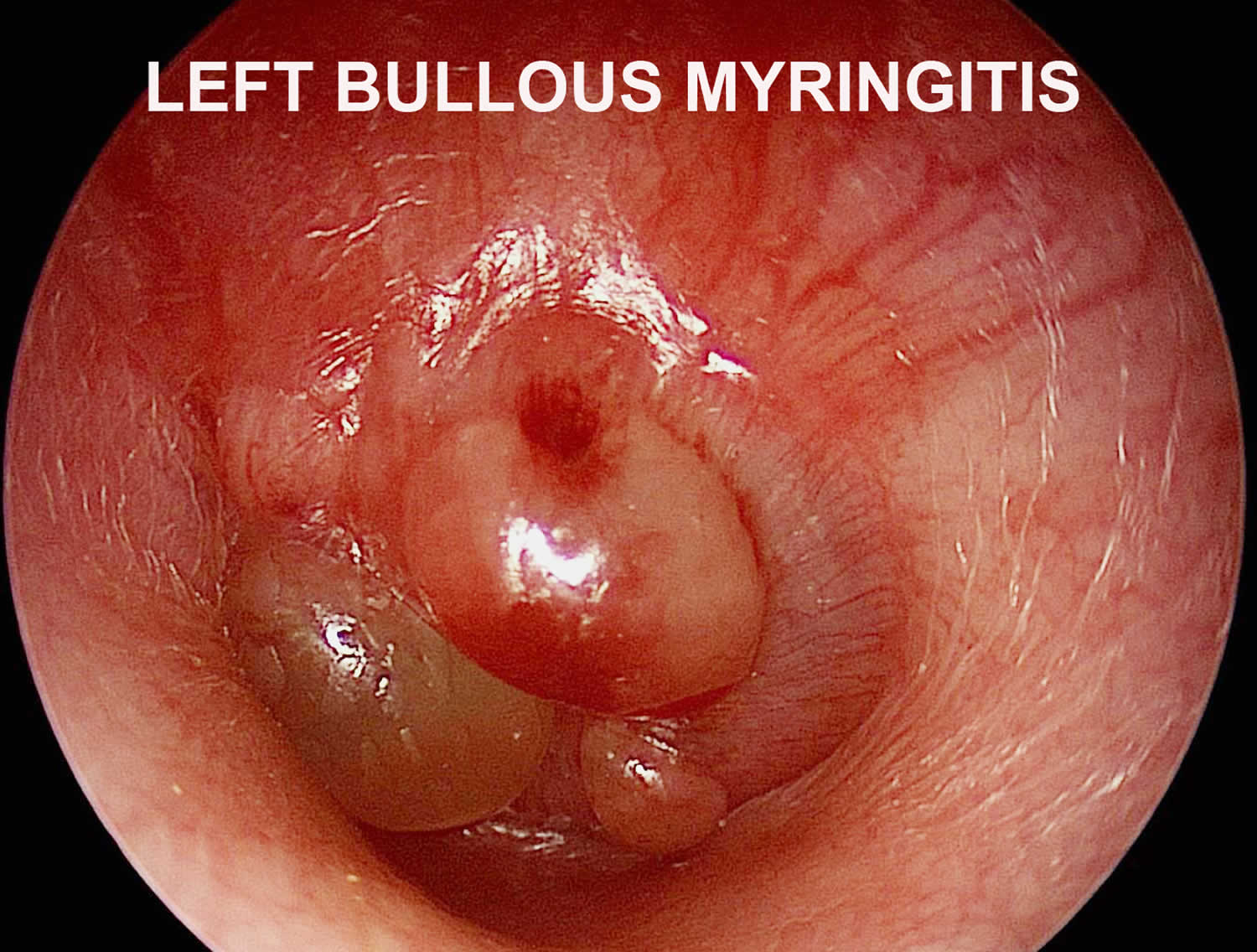
Figure 2. Bullous myringitis
Bullous myringitis causes
Bullous myringitis is caused by the same viruses or bacteria that cause middle ear infections (acute otitis media). The most common of these is mycoplasma. It is often found along with the common cold or other similar infections. Cutaneous lesions have been reported in 25–33 % of patients with Mycoplasma pneumoniae infection 3. A wide array of skin manifestations has been reported regardless of the stage and location of the Mycoplasma pneumoniae infection. The most common of these is the exanthematous or ‘maculopapular’ eruption 4. Erythema multiforme is a common form of this type of skin lesion. Stevens–Johnson syndrome is a severe form of erythema multiforme and it represents 1–5 % of cutaneous disease 5.
Thrombocytopenia is not a common manifestation of Mycoplasma pneumoniae infection and it may occur in the setting of thrombotic thrombocytopenic purpura and disseminated intravascular coagulation 6. Aviner and colleagues 7 described eight cases of M. pneumoniae-related immune thrombocytopenia purpura (ITP) that occurred concomitantly with the infection.
Bullous myringitis is most often seen in children, but it may also occur in adults.
Risk factors for bullous myringitis
Risk factors for myringitis bullosa include:
- Age. Children between the ages of 6 months and 2 years are more susceptible to ear infections because of the size and shape of their eustachian tubes and because of their poorly developed immune systems.
- Group child care. Children cared for in group settings are more likely to get colds and ear infections than are children who stay home because they’re exposed to more infections, such as the common cold.
- Infant feeding. Babies who drink from a bottle, especially while lying down, tend to have more ear infections than do babies who are breast-fed.
- Seasonal factors. Ear infections are most common during the fall and winter when colds and flu are prevalent. People with seasonal allergies may have a greater risk of ear infections during seasonal high pollen counts.
- Poor air quality. Exposure to tobacco smoke or high levels of air pollution can increase the risk of ear infection.
Can bullous myringitis be prevented or avoided?
Although an infectious myringitis is not contagious, the bacteria or virus that causes it is often passed from person to person like most germs. It’s important to:
- Vaccinate your child with a pneumococcal conjugate vaccine to protect against several types of pneumococcal bacteria. This type of bacteria is the most common cause of ear infections. Get your child’s vaccinations on time. It is recommended that you vaccinate your child with the 13-valent pneumococcal conjugate vaccine (PCV13). The PCV13 protects against more types of infection-causing bacteria than the previous vaccine, the PCV7. If your child already has begun PCV7 vaccination, consult your physician about how to transition to PCV13. The Centers for Disease Control and Prevention (CDC) recommends that children under age 2 be vaccinated, starting at 2 months of age. Studies have shown that vaccinated children get far fewer ear infections than children who aren’t vaccinated. The vaccine is strongly recommended for children in daycare.
- Practice routine hand washing and avoid sharing food and drinks, especially if your child is exposed to large groups of kids in day care or school settings.
- Avoid second-hand smoke.
- Don’t allow sick children to spend time together. As much as possible, limit your child’s exposure to other children when your child or your child’s playmates are sick.
- Breastfeed your baby exclusively for the first 6 months and continue breastfeeding for at least 1 year. Place your baby at an angle while feeding.
- Common allergy and cold medicines do not protect against ear infections.
Myringitis symptoms
The main symptom of infectious myringitis is ear pain that lasts for 24 to 48 hours. Other symptoms include:
- Draining from the ear
- Hearing loss in the painful ear
Rarely, the hearing loss will continue after the infection has cleared.
If your child isn’t old enough to say “My ear hurts,” here are a few things to look for
- Tugging or pulling at an ear
- Crying more than usual
- Acting more irritable than usual
- Drainage of fluid from the ear
- Trouble sleeping
- Loss of balance
- Difficulty hearing or responding to sounds
- Ear pain, especially when lying down
- Fever of 100 °F (38 °C) or higher
- Headache
- Loss of appetite
Bullous myringitis complications
Most bullous myringitis don’t cause long-term complications. Frequent or persistent infections and persistent fluid buildup can result in some serious complications:
- Impaired hearing. Mild hearing loss that comes and goes is fairly common with an ear infection, but it usually returns to what it was before the infection after the infection clears. Persistent infection or persistent fluids in the middle ear may result in more significant hearing loss. If there is some permanent damage to the eardrum or other middle ear structures, permanent hearing loss may occur.
- Speech or developmental delays. If hearing is temporarily or permanently impaired in infants and toddlers, they may experience delays in speech, social and developmental skills.
- Spread of infection. Untreated infections or infections that don’t respond well to treatment can spread to nearby tissues. Infection of the mastoid, the bony protrusion behind the ear, is called mastoiditis. This infection can result in damage to the bone and the formation of pus-filled cysts. Rarely, serious middle ear infections spread to other tissues in the skull, including the brain or the membranes surrounding the brain (meningitis).
- Tearing of the eardrum. Most eardrum tears heal within 72 hours. In some cases, surgical repair is needed.
Bullous myringitis diagnosis
Your health care provider will diagnose bullous myringitis by looking inside the ear with an instrument called an otoscope.
Bullous myringitis treatment
Infectious myringitis is usually treated with antibiotics. These may be given by mouth or as drops in the ear. If the pain is severe, small cuts may be made in the eardrum blisters so they can drain. Pain-killing medicines may be prescribed, as well.
Many doctors will prescribe an antibiotic, such as amoxicillin, to be taken over seven to 10 days. Your doctor also may recommend over-the-counter pain relievers such as acetaminophen or ibuprofen, or eardrops, to help with fever and pain. (Because aspirin is considered a major preventable risk factor for Reye’s syndrome, a child who has a fever or other flu-like symptoms should not be given aspirin unless instructed to by your doctor.)
You or your child should start feeling better within a few days after visiting the doctor. If it’s been several days and you or your child still seems sick, call your doctor. You or your child might need a different antibiotic. Once the infection clears, fluid may still remain in the middle ear but usually disappears within three to six weeks.
- The Etiology of Bullous Myringitis and the Role of Mycoplasmas in Ear Disease: A Review. Donald B. Roberts. Pediatrics Apr 1980, 65 (4) 761-766 https://pediatrics.aappublications.org/content/65/4/761[↩][↩]
- Roberts DB. The etiology of bullous myringitis and the role of mycoplasmas in ear disease: a review. Pediatrics. 1980;65:761–766[↩]
- Murray HW, Masur H, Senterfit LB, Roberts RB. The protean manifestations of Mycoplasma pneumoniae infection in adults. Am J Med. 1975;58:229–242. doi: 10.1016/0002-9343(75)90574-4[↩]
- Schalock PC, Dinulos JG. Mycoplasma pneumoniae-induced cutaneous disease. Int J Dermatol. 2009;48:673–681. doi: 10.1111/j.1365-4632.2009.04154.x[↩]
- Ferwerda A, Moll HA, de Groot R. Respiratory tract infections by Mycoplasma pneumoniae in children: a review of diagnostic and therapeutic measures. Eur J Pediatr. 2001;160:483–491. doi: 10.1007/s004310100775[↩]
- Eaton MD, van Herick W, Meiklejohn G. Studies on the etiology of primary atypical pneumonia: III. Specific neutralization of the virus by human serum. J Exp Med. 1945;82:329–342. doi: 10.1084/jem.82.5.329[↩]
- Aviner S, Miskin H, London D, Horowitz S, Schlesinger M. Mycoplasma pneumonia infection: a possible trigger for immune thrombocytopenia. Indian J Hematol Blood Transfus. 2011;27:46–50. doi: 10.1007/s12288-011-0054-6[↩]




{kind=link}