
Contents
What are neurological disorders
Neurological disorders and diseases are those that affect the brain, spinal cord and all the nervous system, includes Parkinson’s Disease and Alzheimer’s Disease. Structural, biochemical or electrical abnormalities in the brain, spinal cord or other nerves can result in a range of symptoms. Examples of symptoms include paralysis, muscle weakness, poor coordination, loss of sensation, seizures, confusion, pain and altered levels of consciousness. There are many recognized neurological disorders, some relatively common, but many rare. They may be assessed by neurological examination, and studied and treated within the specialities of neurology and clinical neuropsychology.
Environmental factors are suspected of playing a large role in both the onset and severity of both neurological disorders and diseases, in addition to genetics, aging, and other factors. Interventions for neurological disorders include preventative measures, lifestyle changes, physiotherapy or other therapy, neurorehabilitation, pain management, medication, operations performed by neurosurgeons or a specific diet.
Neurological disorders impact the quality of life for both the sufferer and the caregiver as well as places healthcare stresses on the economy and workforce. Neurological disorders are the leading cause of disability and the second leading cause of death worldwide 1. Globally, in 2016, neurological disorders were the leading cause of disability-adjusted life-years (276 million) and second leading cause of deaths (9·0 million) 2. The absolute number of deaths and disability-adjusted life-years from all neurological disorders combined increased (deaths by 39% and disability-adjusted life-years by 15%) whereas their age-standardized rates decreased (deaths by 28% and disability-adjusted life-years by 27%) between 1990 and 2016 2. The only neurological disorders that had a decrease in rates and absolute numbers of deaths and disability-adjusted life-years were tetanus, meningitis, and encephalitis 2.
Globally, the burden of neurological disorders, as measured by the absolute number of disability-adjusted life-years, continues to increase 2. As populations are growing and ageing, and the prevalence of major disabling neurological disorders steeply increases with age, governments will face increasing demand for treatment, rehabilitation, and support services for neurological disorders.
The bulk of the burden from neurological disorders continues to be in low-income and middle-income countries 2. The scarcity of established modifiable risks for most of the neurological disorders demonstrates that new knowledge is required to develop effective prevention and treatment strategies.
Types of neurological disorders
Neurological disorders can be categorized according to the primary location affected, the primary type of dysfunction involved, or the primary type of cause. The broadest division is between central nervous system disorders and peripheral nervous system disorders. The Merck Manual lists brain, spinal cord and nerve disorders in the following overlapping categories 3:
Brain:
- Brain damage according to cerebral lobe (see also ‘lower’ brain areas such as basal ganglia, cerebellum, brainstem):
- Frontal lobe damage
- Parietal lobe damage
- Temporal lobe damage
- Occipital lobe damage
- Brain infections:
- Brain abscess
- Encephalitis
- Intracranial Epidural Abscess and Subdural Empyema
- Parasitic Brain Infections
- Progressive Multifocal Leukoencephalopathy (PML)
- Rabies
- Brain dysfunction according to type:
- Aphasia (language)
- Dysgraphia (writing)
- Dysarthria (speech)
- Apraxia (patterns or sequences of movements)
- Agnosia (identifying things or people)
- Amnesia (memory)
- Transient Global Amnesia
- Wernicke-Korsakoff Syndrome
- Coma and Impaired Consciousness
- Consciousness
- Stupor and Coma
- Vegetative State
- Minimally Conscious State
- Locked-In Syndrome
- Brain Death
- Delirium and Dementia
- Delirium
- Dementia
- Alzheimer Disease
- Chronic Traumatic Encephalopathy (CTE)
- Frontotemporal Dementia (FTD)
- HIV-Associated Dementia
- Lewy Body Dementia and Parkinson Disease Dementia
- Normal-Pressure Hydrocephalus
- Vascular Dementia
- Spinal cord disorders (spinal pathology, injury, inflammation)
- Peripheral neuropathy and other Peripheral nervous system disorders
- Cranial nerve disorders:
- Trigeminal neuralgia
- Internuclear Ophthalmoplegia
- Conjugate Gaze Palsies
- Third Cranial Nerve (Oculomotor Nerve) Palsy
- Fourth Cranial Nerve (Trochlear Nerve) Palsy
- Sixth Cranial Nerve (Abducens Nerve) Palsy
- Bell Palsy
- Hemifacial Spasm
- Glossopharyngeal Neuralgia
- Hypoglossal Nerve Disorders
- Headaches
- Cluster Headaches
- Idiopathic Intracranial Hypertension (pseudotumour cerebri)
- Low-Pressure Headache
- Migraines
- Short-Lasting Unilateral Neuralgiform Headache With Conjunctival Injection and Tearing (SUNCT)
- Tension-Type Headaches
- Meningitis
- Acute Bacterial Meningitis
- Viral Meningitis
- Noninfectious Meningitis
- Recurrent Meningitis
- Subacute and Chronic Meningitis
- Autonomic nervous system disorders such as dysautonomia, Multiple System Atrophy
- Seizure disorders such as epilepsy
- Movement disorders of the central and peripheral nervous system:
- Parkinson’s disease,
- Essential tremor,
- Amyotrophic lateral sclerosis (ALS),
- Tourette’s syndrome
- Chorea, Athetosis, and Hemiballismus
- Coordination Disorders
- Dystonia
- Cervical Dystonia
- Fragile X–Associated Tremor/Ataxia Syndrome
- Huntington Disease
- Myoclonus
- Parkinsonism
- Progressive Supranuclear Palsy (PSP)
- Tremor
- various types of Peripheral Neuropathy
- Multiple Sclerosis (MS) and Related Disorders
- Multiple Sclerosis (MS)
- Neuromyelitis Optica Spectrum Disorder (NMOSD)
- Other Primary Demyelinating Diseases
- Pain
- Chronic Pain
- Neuropathic Pain
- Complex Regional Pain Syndrome
- Nociceptive Pain
- Psychologic Factors That Contribute to Pain
- Lower back and neck pain (see back pain)
- Peripheral Nerve Disorders
- Amyotrophic Lateral Sclerosis (ALS) and Other Motor Neuron Diseases (MNDs)
- Neuromuscular Junction Disorders
- Myasthenia Gravis
- Eaton-Lambert Syndrome
- Isaacs Syndrome
- Stiff-Person Syndrome
- Plexus Disorders
- Thoracic Outlet Syndromes (TOS)
- Mononeuropathy
- Multiple Mononeuropathy
- Polyneuropathy
- Guillain-Barré Syndrome (GBS)
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Hereditary Neuropathies
- Charcot-Marie-Tooth Disease
- Hereditary Neuropathy With Liability to Pressure Palsies (HNPP)
- Spinal Muscular Atrophies (SMAs)
- Prion Diseases
- Creutzfeldt-Jakob Disease (CJD)
- Fatal Insomnia
- Gerstmann-Sträussler-Scheinker Disease (GSS)
- Kuru
- Prion Disease Associated With Diarrhea and Autonomic Neuropathy
- Variably Protease-Sensitive Prionopathy
- Seizure Disorders and Epilepsies:
- Focal Seizures
- Generalized Seizures
- Absence Seizure (Petit Mal Seizure)
- Frontal Lobe Seizures
- Grand Mal Seizure
- Temporal Lobe Seizure
- Todd’s Paralysis
- Sleep disorders:
- Narcolepsy
- Snoring
- Insomnia and Excessive Daytime Sleepiness (EDS)
- Circadian Rhythm Sleep Disorders
- Narcolepsy
- Periodic Limb Movement Disorder (PLMD) and Restless Legs Syndrome (RLS)
- Parasomnias
- Sleep Disorders in Dementia
- Spinal Cord Disorders
- Acute Transverse Myelitis
- Blockage of the Spinal Cord’s Blood Supply
- Cervical Spondylosis
- Compression of the Spinal Cord
- Hereditary Spastic Paraparesis
- Subacute Combined Degeneration
- Syrinx of the Spinal Cord and Brain Stem
- Tropical Spastic Paraparesis/HTLV-1–Associated Myelopathy
- Stroke (CVA)
- Ischemic Stroke
- Transient Ischemic Attacks (TIAs)
- Overview of Hemorrhagic Stroke
- Intracerebral Hemorrhage
- Subarachnoid Hemorrhage
- Tumors of the Nervous System
- Brain Tumors
- Some Specific Brain Tumors
- Spinal Cord Tumors
- Damage to the Nervous System Due to Radiation Therapy
- Neuropsychiatric illnesses (diseases and/or disorders with psychiatric features associated with known nervous system injury, underdevelopment, Biochemical, anatomical, or electrical malfunction, and/or disease pathology e.g. Attention deficit hyperactivity disorder, Autism, Tourette’s syndrome and Some cases of obsessive compulsive disorder as well as the neurobehavioral associated symptoms of degeneratives of the nervous system such as Parkinson’s disease, essential tremor, Huntington’s disease, Alzheimer’s disease, multiple sclerosis and organic psychosis.
Many of the diseases and disorders listed above have neurosurgical treatments available (e.g. Tourette’s Syndrome, Parkinson’s disease, Essential tremor and Obsessive compulsive disorder).
- Delirium and dementia such as Alzheimer’s disease
- Dizziness and vertigo
- Stupor and coma
- Head injury
- Stroke (CVA, cerebrovascular attack)
- Tumors of the nervous system (e.g. cancer)
- Multiple sclerosis and other demyelinating diseases
- Infections of the brain or spinal cord (including meningitis)
- Prion diseases (a type of infectious agent)
- Complex regional pain syndrome (a chronic pain condition)
Common neurological disorders
There are more than 600 neurological disorders. Major types include
- Diseases caused by faulty genes, such as Huntington’s disease and muscular dystrophy
- Problems with the way the nervous system develops, such as spina bifida
- Degenerative diseases, where nerve cells are damaged or die, such as Parkinson’s disease and Alzheimer’s disease
- Diseases of the blood vessels that supply the brain, such as stroke
- Injuries to the spinal cord and brain
- Seizure disorders, such as epilepsy
- Cancer, such as brain tumors
- Infections, such as meningitis
The four largest contributors of neurological disability-adjusted life-years were stroke (42·2%), migraine (16·3%), Alzheimer’s disease and other dementias (10·4%), and meningitis (7·9%) 2. For the combined neurological disorders, age-standardized disability-adjusted life-year rates were significantly higher in males than in females (male-to-female ratio 1·12), but migraine, multiple sclerosis, and tension-type headache were more common and caused more burden in females, with male-to-female ratios of less than 0·7. The 84 risks quantified in Global Burden of Disease explain less than 10% of neurological disorder disability-adjusted life-year burdens, except stroke, for which 88·8% of disability-adjusted life-years are attributable to risk factors, and to a lesser extent Alzheimer’s disease and other dementias (22·3% of disability-adjusted life-years are risk attributable) and idiopathic epilepsy (14·1% of disability-adjusted life-years are risk attributable).
Figure 1. Common neurological disorders (ranking of age-standardized disability-adjusted life-year rates for all neurological disorders by region, 2016)
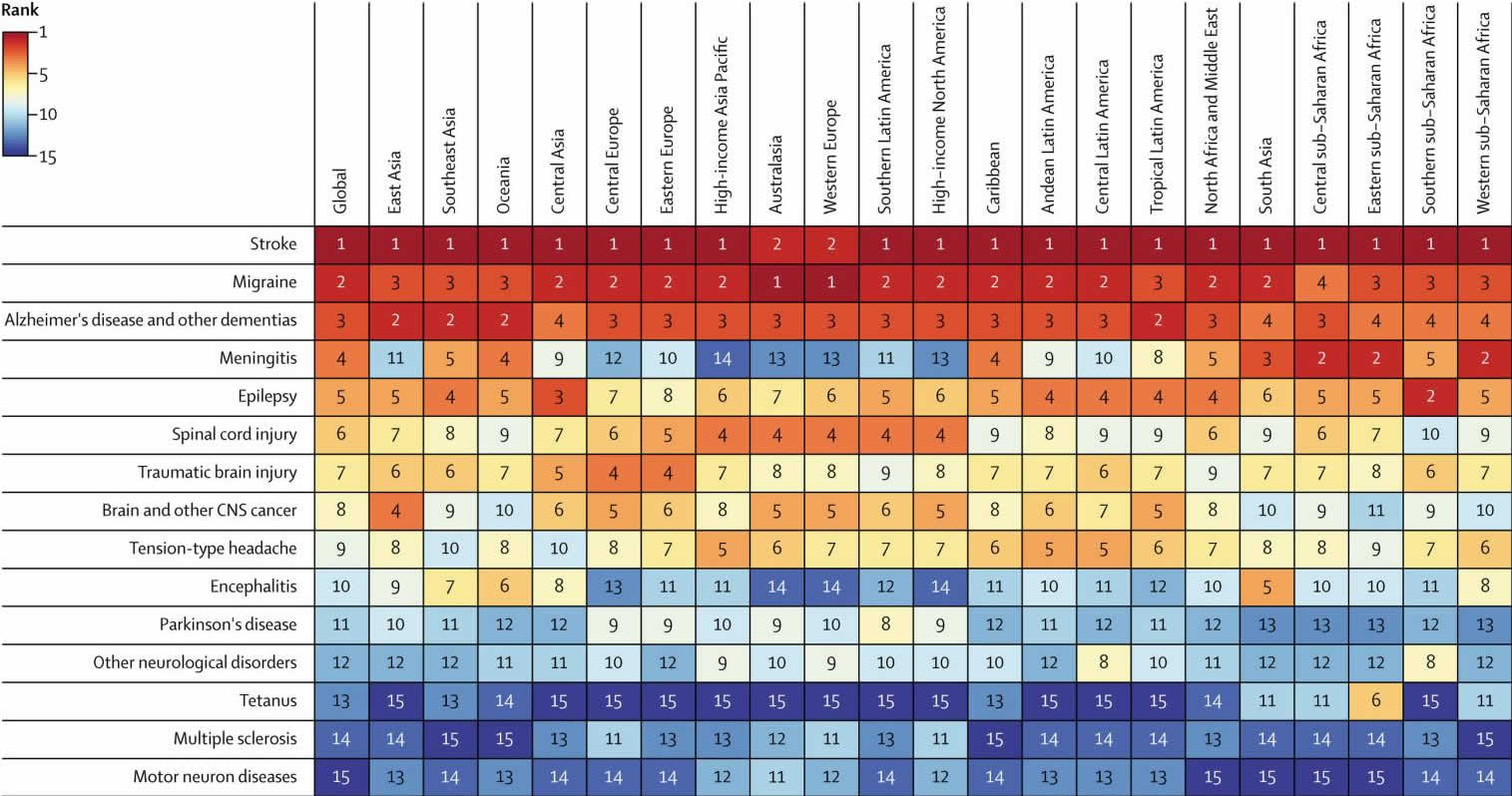
Figure 2. Neurological disorders by sex and age
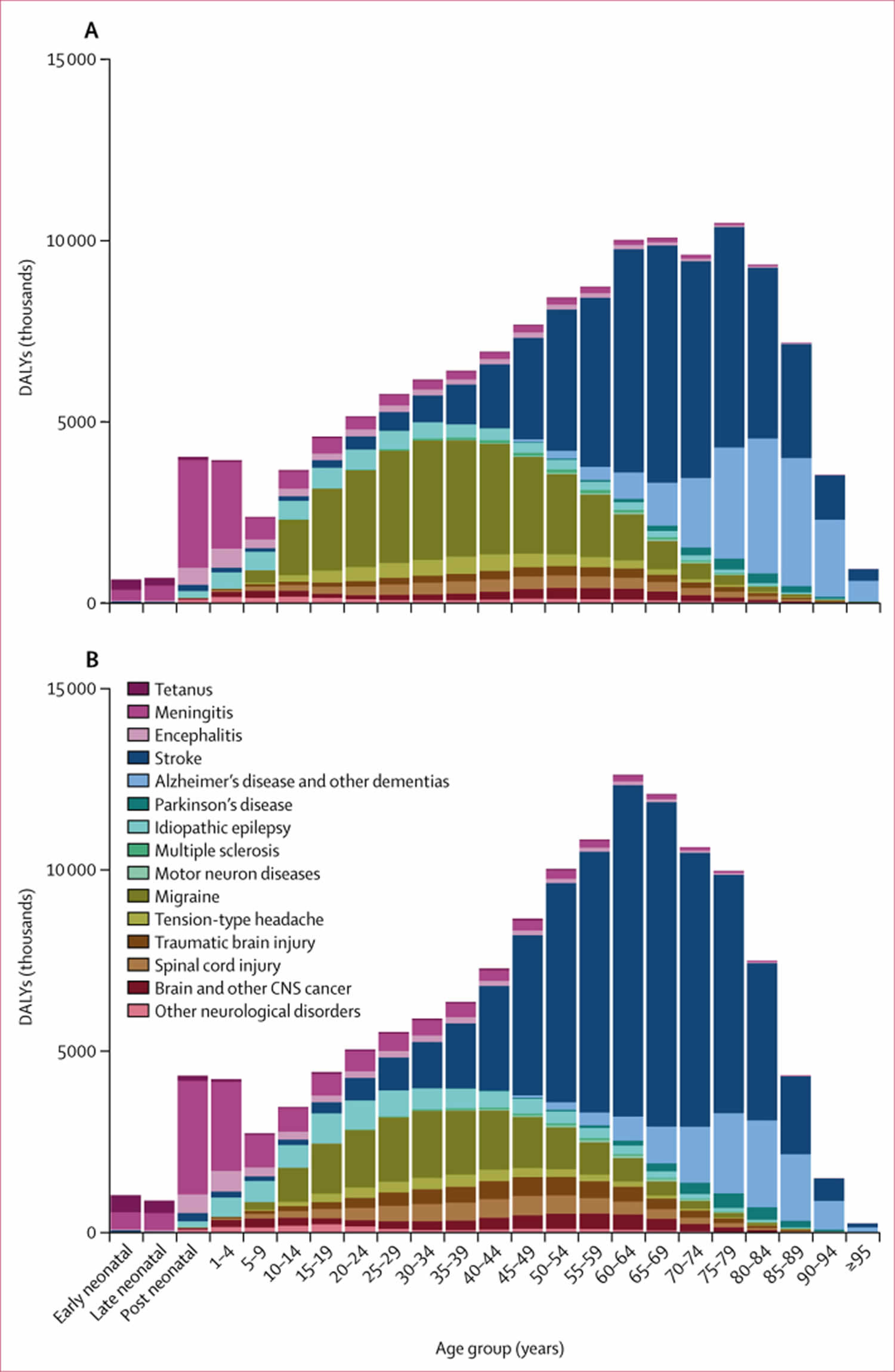
Footnote: Early neonatal is 0–7 days; late neonatal is 7–28 days; and post-neonatal is 28 days to 1 year. (A) Females. (B) Males. DALY=disability-adjusted life-year.
[Source 2 ]Neurological disorders symptoms
Neurological disorders symptoms caused by a disorder that affects part or all of the nervous system—can vary greatly because the nervous system controls so many different body functions. Symptoms can include all forms of pain, including headache and back pain. Muscles, skin sensation, the special senses (vision, taste, smell, and hearing), and other senses depend on nerves to function normally. Thus, neurologic symptoms can include muscle weakness or lack of coordination, abnormal sensations in the skin, and disturbances of vision, taste, smell, hearing, sleep, awareness (consciousness), and mental function (cognition).
Neurologic disorders can interfere with sleep, making a person anxious or excited at bedtime and thus tired and sleepy during the day.
Neurologic symptoms may be minor (such as a foot that has fallen asleep) or life threatening (such as coma due to stroke).
The following are some relatively common neurologic symptoms:
Pain
- Back pain
- Neck pain
- Headache
- Pain along a nerve pathway (as in sciatica or shingles)
Muscle malfunction
- Weakness
- Tremor (rhythmic shaking of a body part)
- Paralysis
- Involuntary (unintended) movements (such as tics)
- Abnormalities in walking
- Clumsiness or poor coordination
- Muscle spasms
- Rigidity, stiffness, and spasticity (muscle spasms resulting from muscle stiffness)
- Slowed movements
Changes in sensation
- Numbness of the skin
- Tingling or a pins-and-needles sensation
- Increased sensitivity (hypersensitivity) to light touch
- Loss of sensation for touch, cold, heat, or pain
- Loss of position sense (knowing where parts of the body are in space)
Changes in the special senses
- Disturbances of smell and taste
- Visual hallucinations
- Partial or complete loss of vision
- Double vision
- Deafness
- Ringing or other sounds originating in the ears (tinnitus)
Other symptoms
- Vertigo
- Loss of balance
- Difficulty swallowing
- Slurred speech (dysarthria)
Sleep problems
- Difficulty falling or staying asleep
- Uncontrollable leg movements during sleep
- Falling asleep uncontrollably (as in narcolepsy) or sleeping too much
Changes in consciousness
- Fainting
- Confusion or delirium
- Seizures (ranging from brief lapses in consciousness to severe muscle contractions and jerking throughout the body)
- Coma
- Stupor
Changes in cognition (mental ability)
- Difficulty understanding language or using language to speak or write (aphasia)
- Poor memory
- Difficulty with common motor skills, such as striking a match or combing hair, despite normal strength (apraxia)
- Inability to recognize familiar objects (agnosia) or familiar faces (prosopagnosia)
- Inability to sustain concentration when doing a task
- Inability to distinguish right from left
- Inability to do simple arithmetic (acalculia)
- Difficulty understanding spatial relationships (for example, being unable to draw a clock or becoming lost driving in a familiar neighborhood)
- Dementia (dysfunction of several cognitive functions)
- Neglect of one side of the body or denial that it exists (often due to a brain injury)
The characteristics and pattern of symptoms help doctors diagnose the neurologic disorder. Doctors also do a neurologic examination, which can detect disorders of the brain, spinal cord, and nerves in other parts of the body (peripheral nerves).
Peripheral nerves include:
- The nerves that connect the head, face, eyes, nose, muscles, and ears to the brain (cranial nerves)
- The nerves that connect the spinal cord to the rest of the body: 31 pairs of spinal nerves
- Nerves that run throughout the body
Some peripheral nerves (sensory nerves) carry sensory information (about such things as pain, temperature, vibration, smells, and sounds) to the spinal cord and then to the brain. Others (motor nerves) carry impulses that control muscle movement from the brain through the spinal cord to the muscles. Still others (called the autonomic nerves) carry information about the body and external environment to the internal organs, such as the blood vessels, stomach, intestine, liver, kidneys, and bladder. In response to this information, autonomic nerves stimulate or inhibit the organs they supply. These nerves work automatically (autonomously), without a person’s conscious effort.
If motor nerves are damaged, muscles may weaken or become paralyzed. If sensory nerves are damaged, abnormal sensations may be felt or sensation, sight, or another sense may be impaired or lost. If autonomic nerves are damaged, the organ they regulate may malfunction. For example, blood pressure may not increase as it normally does when a person stands, and the person may feel light-headed.
Neurological disorders diagnosis
Based on the result of a neurological exam, physical exam, patient history, x-rays of the patient’s chest and skull, and any previous screening or testing, physicians may order one or more of the following diagnostic tests to determine the specific nature of a suspected neurological disorder or injury. These diagnostics generally involve either nuclear medicine imaging, in which very small amounts of radioactive materials are used to study organ function and structure, ordiagnostic imaging, which uses magnets and electrical charges to study human anatomy.
The following list of available procedures—in alphabetical rather than sequential order—includes some of the more common tests used to help diagnose a neurological condition.
Angiography
Angiography is a test used to detect blockages of the arteries or veins. A cerebral angiogram can detect the degree of narrowing or obstruction of an artery or blood vessel in the brain, head, or neck. It is used to diagnose stroke and to determine the location and size of a brain tumor, aneurysm, or vascular malformation. This test is usually performed in a hospital outpatient setting and takes up to 3 hours, followed by a 6- to 8-hour resting period. The patient, wearing a hospital or imaging gown, lies on a table that is wheeled into the imaging area. While the patient is awake, a physician anesthetizes a small area of the leg near the groin and then inserts a catheter into a major artery located there. The catheter is threaded through the body and into an artery in the neck. Once the catheter is in place, the needle is removed and a guide wire is inserted. A small capsule containing a radiopaque dye (one that is highlighted on x-rays) is passed over the guide wire to the site of release. The dye is released and travels through the bloodstream into the head and neck. A series of x-rays is taken and any obstruction is noted. Patients may feel a warm to hot sensation or slight discomfort as the dye is released.
Biopsy
Biopsy involves the removal and examination of a small piece of tissue from the body. Muscle or nerve biopsies are used to diagnose neuromuscular disorders and may also reveal if a person is a carrier of a defective gene that could be passed on to children. A small sample of muscle or nerve is removed under local anesthetic and studied under a microscope. The sample may be removed either surgically, through a slit made in the skin, or by needle biopsy, in which a thin hollow needle is inserted through the skin and into the muscle. A small piece of muscle or nerve remains in the hollow needle when it is removed from the body. The biopsy is usually performed at an outpatient testing facility. A brain biopsy, used to determine tumor type, requires surgery to remove a small piece of the brain or tumor. Performed in a hospital, this operation is riskier than a muscle biopsy and involves a longer recovery period.
Cerebrospinal fluid analysis
Cerebrospinal fluid analysis involves the removal of a small amount of the fluid that protects the brain and spinal cord. The fluid is tested to detect any bleeding or brain hemorrhage, diagnose infection to the brain and/or spinal cord, identify some cases of multiple sclerosis and other neurological conditions, and measure intracranial pressure.
The procedure is usually done in a hospital. The sample of fluid is commonly removed by a procedure known as a lumbar puncture, or spinal tap. The patient is asked to either lie on one side, in a ball position with knees close to the chest, or lean forward while sitting on a table or bed. The doctor will locate a puncture site in the lower back, between two vertebrate, then clean the area and inject a local anesthetic. The patient may feel a slight stinging sensation from this injection. Once the anesthetic has taken effect, the doctor will insert a special needle into the spinal sac and remove a small amount of fluid (usually about three teaspoons) for testing. Most patients will feel a sensation of pressure only as the needle is inserted.
A common after-effect of a lumbar puncture is headache, which can be lessened by having the patient lie flat. Risk of nerve root injury or infection from the puncture can occur but it is rare. The entire procedure takes about 45 minutes.
Brain scans
Brain scans are imaging techniques used to diagnose tumors, blood vessel malformations, or hemorrhage in the brain. These scans are used to study organ function or injury or disease to tissue or muscle. Types of brain scans include computed tomography, magnetic resonance imaging, and positron emission tomography (see descriptions, below).
Computed tomography, also known as a CT scan, is a noninvasive, painless process used to produce rapid, clear two-dimensional images of organs, bones, and tissues. Neurological CT scans are used to view the brain and spine. They can detect bone and vascular irregularities, certain brain tumors and cysts, herniated discs, epilepsy, encephalitis, spinal stenosis (narrowing of the spinal canal), a blood clot or intracranial bleeding in patients with stroke, brain damage from head injury, and other disorders. Many neurological disorders share certain characteristics and a CT scan can aid in proper diagnosis by differentiating the area of the brain affected by the disorder.
Scanning takes about 20 minutes (a CT of the brain or head may take slightly longer) and is usually done at an imaging center or hospital on an outpatient basis. The patient lies on a special table that slides into a narrow chamber. A sound system built into the chamber allows the patient to communicate with the physician or technician. As the patient lies still, x-rays are passed through the body at various angles and are detected by a computerized scanner. The data is processed and displayed as cross-sectional images, or “slices,” of the internal structure of the body or organ. A light sedative may be given to patients who are unable to lie still and pillows may be used to support and stabilize the head and body. Persons who are claustrophobic may have difficulty taking this imaging test.
Occasionally a contrast dye is injected into the bloodstream to highlight the different tissues in the brain. Patients may feel a warm or cool sensation as the dye circulates through the bloodstream or they may experience a slight metallic taste.
Although very little radiation is used in CT, pregnant women should avoid the test because of potential harm to the fetus from ionizing radiation.
Discography is often suggested for patients who are considering lumbar surgery or whose lower back pain has not responded to conventional treatments. This outpatient procedure is usually performed at a testing facility or a hospital. The patient is asked to put on a metal-free hospital gown and lie on an imaging table. The physician numbs the skin with anesthetic and inserts a thin needle, using x-ray guidance, into the spinal disc. Once the needle is in place, a small amount of contrast dye is injected and CT scans are taken. The contrast dye outlines any damaged areas. More than one disc may be imaged at the same time. Patient recovery usually takes about an hour. Pain medicine may be prescribed for any resulting discomfort.
An intrathecal contrast-enhanced CT scan (also called cisternography) is used to detect problems with the spine and spinal nerve roots. This test is most often performed at an imaging center. The patient is asked to put on a hospital or imaging gown. Following application of a topical anesthetic, the physician removes a small sample of the spinal fluid via lumbar puncture. The sample is mixed with a contrast dye and injected into the spinal sac located at the base of the lower back. The patient is then asked to move to a position that will allow the contrast fluid to travel to the area to be studied. The dye allows the spinal canal and nerve roots to be seen more clearly on a CT scan. The scan may take up to an hour to complete. Following the test, patients may experience some discomfort and/or headache that may be caused by the removal of spinal fluid.
Electroencephalography (EEG)
Electroencephalography or EEG, monitors brain activity through the skull. EEG is used to help diagnose certain seizure disorders, brain tumors, brain damage from head injuries, inflammation of the brain and/or spinal cord, alcoholism, certain psychiatric disorders, and metabolic and degenerative disorders that affect the brain. EEGs are also used to evaluate sleep disorders, monitor brain activity when a patient has been fully anesthetized or loses consciousness, and confirm brain death.
This painless, risk-free test can be performed in a doctor’s office or at a hospital or testing facility. Prior to taking an EEG, the person must avoid caffeine intake and prescription drugs that affect the nervous system. A series of cup-like electrodes are attached to the patient’s scalp, either with a special conducting paste or with extremely fine needles. The electrodes (also called leads) are small devices that are attached to wires and carry the electrical energy of the brain to a machine for reading. A very low electrical current is sent through the electrodes and the baseline brain energy is recorded. Patients are then exposed to a variety of external stimuli—including bright or flashing light, noise or certain drugs—or are asked to open and close the eyes, or to change breathing patterns. The electrodes transmit the resulting changes in brain wave patterns. Since movement and nervousness can change brain wave patterns, patients usually recline in a chair or on a bed during the test, which takes up to an hour. Testing for certain disorders requires performing an EEG during sleep, which takes at least 3 hours.
In order to learn more about brain wave activity, electrodes may be inserted through a surgical opening in the skull and into the brain to reduce signal interference from the skull.
Electromyography (EMG)
Electromyography or EMG, is used to diagnose nerve and muscle dysfunction and spinal cord disease. It records the electrical activity from the brain and/or spinal cord to a peripheral nerve root (found in the arms and legs) that controls muscles during contraction and at rest.
During an EMG, very fine wire electrodes are inserted into a muscle to assess changes in electrical voltage that occur during movement and when the muscle is at rest. The electrodes are attached through a series of wires to a recording instrument. Testing usually takes place at a testing facility and lasts about an hour but may take longer, depending on the number of muscles and nerves to be tested. Most patients find this test to be somewhat uncomfortable.
An EMG is usually done in conjunction with a nerve conduction velocity (NCV) test, which measures electrical energy by assessing the nerve’s ability to send a signal. This two-part test is conducted most often in a hospital. A technician tapes two sets of flat electrodes on the skin over the muscles. The first set of electrodes is used to send small pulses of electricity (similar to the sensation of static electricity) to stimulate the nerve that directs a particular muscle. The second set of electrodes transmits the responding electrical signal to a recording machine. The physician then reviews the response to verify any nerve damage or muscle disease. Patients who are preparing to take an EMG or NCV test may be asked to avoid caffeine and not smoke for 2 to 3 hours prior to the test, as well as to avoid aspirin and non-steroidal anti-inflammatory drugs for 24 hours before the EMG. There is no discomfort or risk associated with this test.
Electronystagmography (ENG)
Electronystagmography (ENG) describes a group of tests used to diagnose involuntary eye movement, dizziness, and balance disorders, and to evaluate some brain functions. The test is performed at an imaging center. Small electrodes are taped around the eyes to record eye movements. If infrared photography is used in place of electrodes, the patient wears special goggles that help record the information. Both versions of the test are painless and risk-free.
Evoked potentials
Evoked potentials (also called evoked response) measure the electrical signals to the brain generated by hearing, touch, or sight. These tests are used to assess sensory nerve problems and confirm neurological conditions including multiple sclerosis, brain tumor, acoustic neuroma (small tumors of the inner ear), and spinal cord injury. Evoked potentials are also used to test sight and hearing (especially in infants and young children), monitor brain activity among coma patients, and confirm brain death.
Testing may take place in a doctor’s office or hospital setting. It is painless and risk-free. Two sets of needle electrodes are used to test for nerve damage. One set of electrodes, which will be used to measure the electrophysiological response to stimuli, is attached to the patient’s scalp using conducting paste. The second set of electrodes is attached to the part of the body to be tested. The physician then records the amount of time it takes for the impulse generated by stimuli to reach the brain. Under normal circumstances, the process of signal transmission is instantaneous.
Auditory evoked potentials (also called brain stem auditory evoked response) are used to assess high-frequency hearing loss, diagnose any damage to the acoustic nerve and auditory pathways in the brainstem, and detect acoustic neuromas. The patient sits in a soundproof room and wears headphones. Clicking sounds are delivered one at a time to one ear while a masking sound is sent to the other ear. Each ear is usually tested twice, and the entire procedure takes about 45 minutes.
Visual evoked potentials detect loss of vision from optic nerve damage (in particular, damage caused by multiple sclerosis). The patient sits close to a screen and is asked to focus on the center of a shifting checkerboard pattern. Only one eye is tested at a time; the other eye is either kept closed or covered with a patch. Each eye is usually tested twice. Testing takes 30-45 minutes.
Somatosensory evoked potentials measure response from stimuli to the peripheral nerves and can detect nerve or spinal cord damage or nerve degeneration from multiple sclerosis and other degenerating diseases. Tiny electrical shocks are delivered by electrode to a nerve in an arm or leg. Responses to the shocks, which may be delivered for more than a minute at a time, are recorded. This test usually lasts less than an hour.
Magnetic resonance imaging (MRI)
Magnetic resonance imaging (MRI) uses computer-generated radio waves and a powerful magnetic field to produce detailed images of body structures including tissues, organs, bones, and nerves. Neurological uses include the diagnosis of brain and spinal cord tumors, eye disease, inflammation, infection, and vascular irregularities that may lead to stroke. MRI can also detect and monitor degenerative disorders such as multiple sclerosis and can document brain injury from trauma.
The equipment houses a hollow tube that is surrounded by a very large cylindrical magnet. The patient, who must remain still during the test, lies on a special table that is slid into the tube. The patient will be asked to remove jewelry, eyeglasses, removable dental work, or other items that might interfere with the magnetic imaging. The patient should wear a sweat shirt and sweat pants or other clothing free of metal eyelets or buckles. MRI scanning equipment creates a magnetic field around the body strong enough to temporarily realign water molecules in the tissues. Radio waves are then passed through the body to detect the “relaxation” of the molecules back to a random alignment and trigger a resonance signal at different angles within the body. A computer processes this resonance into either a three-dimensional picture or a two-dimensional “slice” of the tissue being scanned, and differentiates between bone, soft tissues and fluid-filled spaces by their water content and structural properties. A contrast dye may be used to enhance visibility of certain areas or tissues. The patient may hear grating or knocking noises when the magnetic field is turned on and off. (Patients may wear special earphones to block out the sounds.) Unlike CT scanning, MRI does not use ionizing radiation to produce images. Depending on the part(s) of the body to be scanned, MRI can take up to an hour to complete. The test is painless and risk-free, although persons who are obese or claustrophobic may find it somewhat uncomfortable. (Some centers also use open MRI machines that do not completely surround the person being tested and are less confining. However, open MRI does not currently provide the same picture quality as standard MRI and some tests may not be available using this equipment). Due to the incredibly strong magnetic field generated by an MRI, patients with implanted medical devices such as a pacemaker should avoid the test.
Functional MRI (fMRI) uses the blood’s magnetic properties to produce real-time images of blood flow to particular areas of the brain. An fMRI can pinpoint areas of the brain that become active and note how long they stay active. It can also tell if brain activity within a region occurs simultaneously or sequentially. This imaging process is used to assess brain damage from head injury or degenerative disorders such as Alzheimer’s disease and to identify and monitor other neurological disorders, including multiple sclerosis, stroke, and brain tumors.
Myelography
Myelography involves the injection of a water- or oil-based contrast dye into the spinal canal to enhance x-ray imaging of the spine. Myelograms are used to diagnose spinal nerve injury, herniated discs, fractures, back or leg pain, and spinal tumors.
The procedure takes about 30 minutes and is usually performed in a hospital. Following an injection of anesthesia to a site between two vertebrae in the lower back, a small amount of the cerebrospinal fluid is removed by spinal tap (seecerebrospinal fluid analysis, above) and the contrast dye is injected into the spinal canal. After a series of x-rays is taken, most or all of the contrast dye is removed by aspiration. Patients may experience some pain during the spinal tap and when the dye is injected and removed. Patients may also experience headache following the spinal tap. The risk of fluid leakage or allergic reaction to the dye is slight.
Positron emission tomography (PET)
Positron emission tomography (PET) scans provide two- and three-dimensional pictures of brain activity by measuring radioactive isotopes that are injected into the bloodstream. PET scans of the brain are used to detect or highlight tumors and diseased tissue, measure cellular and/or tissue metabolism, show blood flow, evaluate patients who have seizure disorders that do not respond to medical therapy and patients with certain memory disorders, and determine brain changes following injury or drug abuse, among other uses. PET may be ordered as a follow-up to a CT or MRI scan to give the physician a greater understanding of specific areas of the brain that may be involved with certain problems. Scans are conducted in a hospital or at a testing facility, on an outpatient basis. A low-level radioactive isotope, which binds to chemicals that flow to the brain, is injected into the bloodstream and can be traced as the brain performs different functions. The patient lies still while overhead sensors detect gamma rays in the body’s tissues. A computer processes the information and displays it on a video monitor or on film. Using different compounds, more than one brain function can be traced simultaneously. PET is painless and relatively risk-free. Length of test time depends on the part of the body to be scanned. PET scans are performed by skilled technicians at highly sophisticated medical facilities.
Polysomnogram
A polysomnogram measures brain and body activity during sleep. It is performed over one or more nights at a sleep center. Electrodes are pasted or taped to the patient’s scalp, eyelids, and/or chin. Throughout the night and during the various wake/sleep cycles, the electrodes record brain waves, eye movement, breathing, leg and skeletal muscle activity, blood pressure, and heart rate. The patient may be videotaped to note any movement during sleep. Results are then used to identify any characteristic patterns of sleep disorders, including restless legs syndrome, periodic limb movement disorder, insomnia, and breathing disorders such as obstructive sleep apnea. Polysomnograms are noninvasive, painless, and risk-free.
Single photon emission computed tomography (SPECT)
Single photon emission computed tomography (SPECT), a nuclear imaging test involving blood flow to tissue, is used to evaluate certain brain functions. The test may be ordered as a follow-up to an MRI to diagnose tumors, infections, degenerative spinal disease, and stress fractures. As with a PET scan, a radioactive isotope, which binds to chemicals that flow to the brain, is injected intravenously into the body. Areas of increased blood flow will collect more of the isotope. As the patient lies on a table, a gamma camera rotates around the head and records where the radioisotope has traveled. That information is converted by computer into cross-sectional slices that are stacked to produce a detailed three-dimensional image of blood flow and activity within the brain. The test is performed at either an imaging center or a hospital.
Thermography
Thermography uses infrared sensing devices to measure small temperature changes between the two sides of the body or within a specific organ. Also known as digital infrared thermal imaging, thermography may be used to detect vascular disease of the head and neck, soft tissue injury, various neuromusculoskeletal disorders, and the presence or absence of nerve root compression. It is performed at an imaging center, using infrared light recorders to take thousands of pictures of the body from a distance of 5 to 8 feet. The information is converted into electrical signals which results in a computer-generated two-dimensional picture of abnormally cold or hot areas indicated by color or shades of black and white. Thermography does not use radiation and is safe, risk-free, and noninvasive.
Ultrasound
Ultrasound imaging, also called ultrasound scanning or sonography, uses high-frequency sound waves to obtain images inside the body. Neurosonography (ultrasound of the brain and spinal column) analyzes blood flow in the brain and can diagnose stroke, brain tumors, hydrocephalus (build-up of cerebrospinal fluid in the brain), and vascular problems. It can also identify or rule out inflammatory processes causing pain. It is more effective than an x-ray in displaying soft tissue masses and can show tears in ligaments, muscles, tendons, and other soft tissue masses in the back. Transcranial Doppler ultrasound is used to view arteries and blood vessels in the neck and determine blood flow and risk of stroke.
During ultrasound, the patient lies on an imaging table and removes clothing around the area of the body to be scanned. A jelly-like lubricant is applied and a transducer, which both sends and receives high-frequency sound waves, is passed over the body. The sound wave echoes are recorded and displayed as a computer-generated real-time visual image of the structure or tissue being examined. Ultrasound is painless, noninvasive, and risk-free. The test is performed on an outpatient basis and takes between 15 and 30 minutes to complete.
Neurological disorders treatment
neurological disorders treatment involves treating the underlying cause(s) of the neurological disorders.
- GBD 2015 Neurological Disorders Collaborator Group Global, regional, and national burden of neurological disorders during 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017;16:877–897 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5641502[↩]
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6459001[↩][↩][↩][↩][↩][↩][↩][↩]
- Brain, Spinal Cord, and Nerve Disorders. https://www.merckmanuals.com/home/brain-spinal-cord-and-nerve-disorders[↩]





{kind=link}