What is nitric oxide
Nitric oxide also called mononitrogen monoxide or nitrogen monoxide, is a colorless gas with the formula NO. Nitric oxide is an unstable free-radical gas which reacts rapidly with oxygen to form nitrogen oxides. Water soluble, nitric oxide (NO) is produced normally in numerous tissues and is considered to be a mediator of cell-to cell communication; nitric oxide (NO) functions in numerous processes including vasodilation, inflammation, and neurotransmission. Nitric oxide is a free radical gas, i.e., it has an unpaired electron, which is sometimes denoted by a dot in its chemical formula, i.e., ·NO. Although nitric oxide (NO) was identified as a gas in late eighteenth century, its role as a biological agent was confirmed only in 1980 1. Nitric oxide (NO) was identified as the known as an endothelium-derived relaxing factor (EDRF) or vasodilator in 1987 2. Nitric oxide (NO) also inhibits platelet aggregation, induces disaggregation of aggregated platelets, and inhibits platelet adhesion to the vascular endothelium. Nitric oxide activates cytosolic guanylate cyclase and thus elevates intracellular levels of cyclic GMP.
In the U.S., the Occupational Safety and Health Administration (OSHA) has set the legal limit (permissible exposure limit) for nitric oxide exposure in the workplace as 25 ppm (30 mg/m³) over an 8-hour workday. The National Institute for Occupational Safety and Health (NIOSH) has set a recommended exposure limit (REL) of 25 ppm (30 mg/m³) over an 8-hour workday. At levels of 100 ppm, nitric oxide is immediately dangerous to life and health 3.
Nitric oxide (NO) is formed from guanidine nitrogen of L-arginine by the action of 3 isoforms of the enzyme nitric oxide synthase (NOS), namely, endothelial nitric oxide synthase (eNOS), inducible nitric oxide synthase (iNOS), and neuronal nitric oxide synthase (nNOS) 4.
This enzymatic conversion of arginine to nitric oxide (NO) by endothelial nitric oxide synthase (eNOS) requires oxygen and the reduced cofactors, tetrahydrobiopterin (BH4) and nicotinamide adenine dinucleotide phosphate (NADPH) 5. Increased intracellular calcium in response to vasodilator agonists such as acetylcholine and bradykinin leads to activation of endothelial nitric oxide synthase (eNOS) and increased production of nitric oxide (NO) in endothelial cells. Nitric oxide (NO) diffuses into vascular smooth muscle cells where it activates soluble guanylyl cyclase, in turn forming cyclic guanosine monophosphate (cGMP) to elicit vasorelaxation, as shown in Figure 1. This nitric oxide/ soluble guanylyl cyclase/cGMP pathway has shown a spatial distribution in the kidney, and its importance in this organ is supported by many studies 6. The level of cGMP is determined by the balance between the synthesizing enzyme soluble guanylyl cyclase (sGC) and catabolizing enzyme phosphodiestrase (PDE), which metabolizes cGMP to its biologically inactive metabolite, 5′-GMP, as shown in Figure 1. In most cells, the rate of synthesis of cGMP is 10-fold lower than its rate of hydrolysis by phosphodiestrase (PDE) 7. Therefore, inhibition of phosphodiestrase (PDE) is considered a therapeutic target in many pathological conditions such as erectile dysfunction 8, in which an elevated levels of nitric oxide is desired. Another interaction of cGMP is with protein kinase G (PKG), which is activated upon CGMP stimulation to phosphorylate different target proteins upon cGMP stimulation. These proteins are involved in vasodilation, neutrophil activation, smooth muscle tone modulator, and matrix expansion 9 as shown in Figure 1.
Figure 1. Nitric oxide synthesis
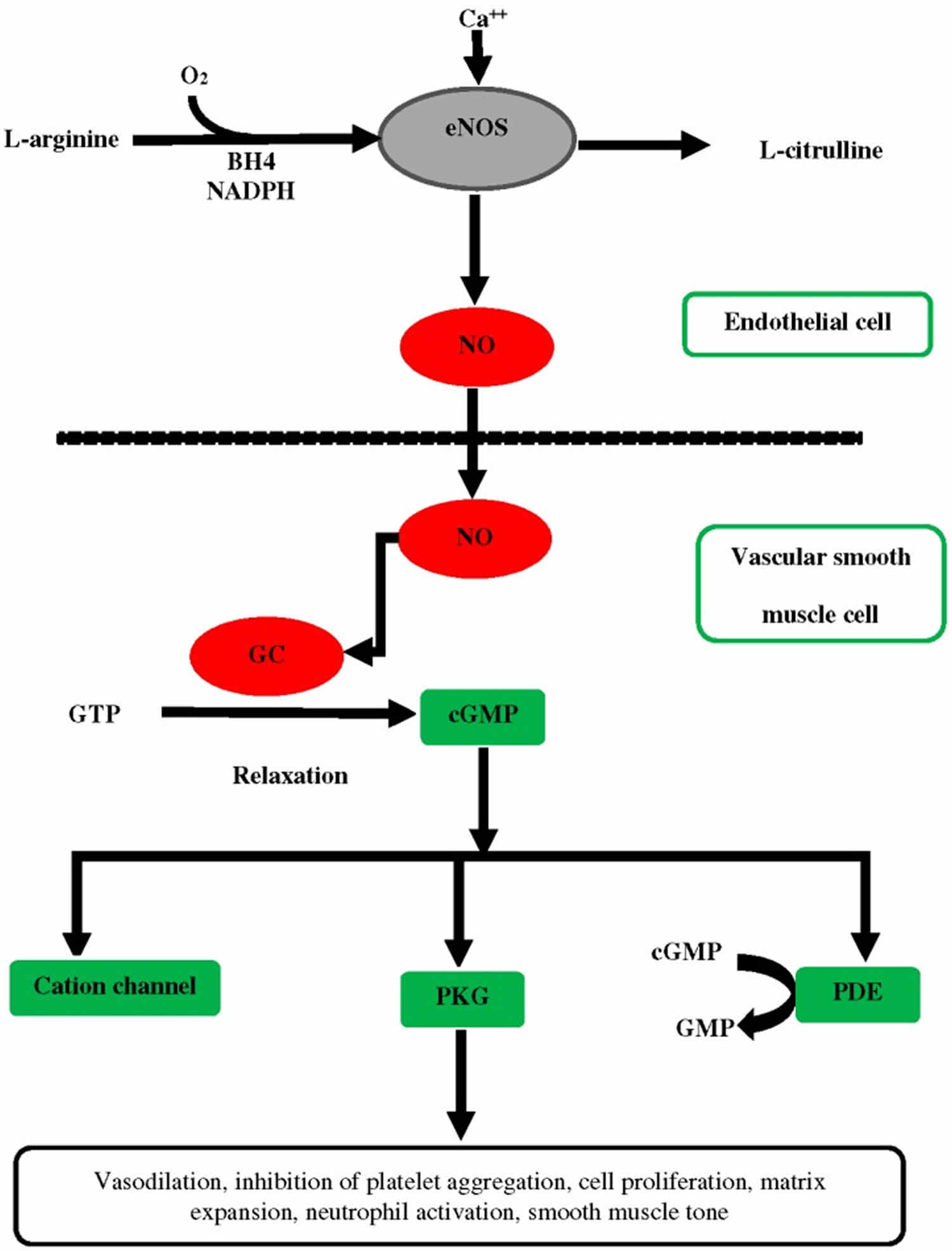
Abbreviations: NO = Nitric oxide; endothelial nitric oxide synthase = eNOS; BH4 = tetrahydrobiopterin; NADPH = nicotinamide adenine dinucleotide phosphate; cGMP = cyclic guanosine monophosphate; GMP = guanosine monophosphate; GC = Guanylate cyclase; PDE = phosphodiesterase; PKG = protein kinase G;
[Source 4 ]What does nitric oxide do?
Nitric oxide is a vasodilator. The physiologic effect of nitric oxide is by means of vasodilation. A large body of evidence supports that the nitric oxide system plays a critical role in blood pressure regulation 4. The data obtained in the cardiovascular system are consistent, and the literature has described in detail the role of L-arginine (nitric oxide donor) in hypertension 10. Reduced concentrations of nitric oxide in plasma have been observed in patients with essential hypertension 11 and endothelium dependent vasodilation is impaired in patients with essential hypertension 12. The endothelium (inner lining) of blood vessels uses nitric oxide to signal the surrounding smooth muscle to relax, thus resulting in vasodilation and increasing blood flow. Sildenafil (Viagra) is a common example of a drug that uses the nitric oxide pathway. Sildenafil does not produce nitric oxide, but enhances the signals that are the downstream of the nitric oxide pathway by protecting cyclic guanosine monophosphate (cGMP) from degradation by cGMP-specific phosphodiesterase type 5 (PDE5) in the corpus cavernosum, allowing for the signal to be enhanced, and thus vasodilation 13.
Figure 2. Interactions of nitric oxide with different systems and modulation of their functions in cardiovascular and renovascular systems
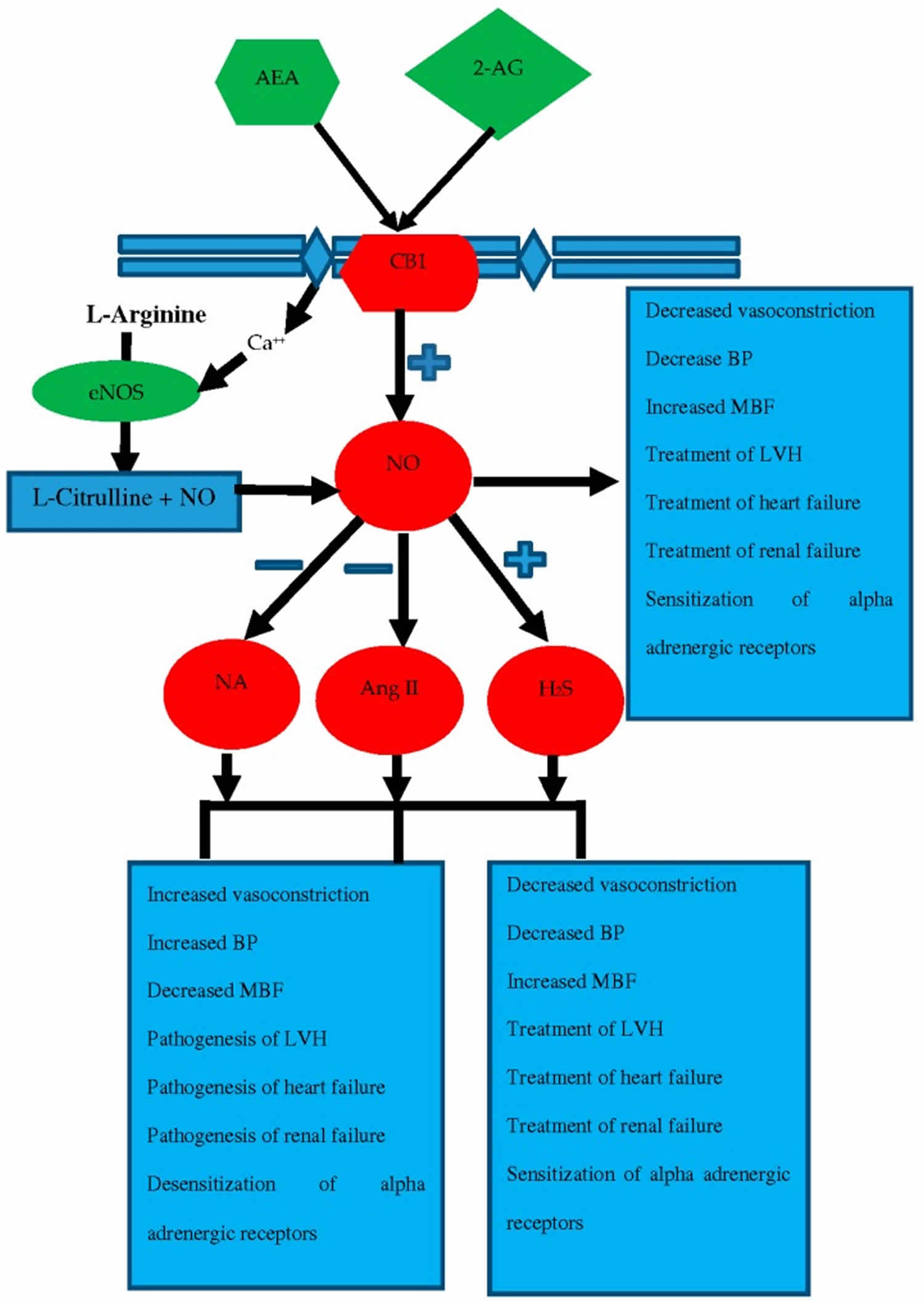
Abbreivations: AEA = anandamide; 2-AG = 2-arachidonylglycerol; CB1 = cannabinoid receptor 1; BP = blood pressure; MBF = myocardial blood flow; LVH = left ventricular hypertrophy; H2S = hydrogen sulfide; Ang2 = angiotensin 2; NA = noradrenaline
[Source 4 ]Nitric oxide bioavailability can be improved by both nonpharmacological and pharmacological approaches. Physical exercise is a nonpharmacological approach to enhance nitric oxide bioavailability and improve endothelial function in hypertensive patients 14. Restoration of eNOS function through augmentation of its substrate, L-arginine, or cofactors for its synthesis has been demonstrated to have beneficial effects. For example, chronic oral supplementation of tetrahydrobiopterin prevented the blood pressure increase in rats with 5/6 nephrectomy 15 and arterial stiffness in fructose-fed insulin-resistant rats 16. The critical role of eNOS and nitric oxide in the prevention of hypertension is supported by the finding that mice lacking a functional eNOS gene develop hypertension 17. NG-monomethyl-l-arginine (l-NMMA) has been frequently employed to block the nitric oxide production pathway to study the importance of this mechanism in hypertension. Intra-arterial infusion of this inhibitor in untreated hypertensive patients resulted in an abnormal basal nitric oxide-induced vasodilation in the forearm arteriolar bed 18. Intravenous injection of a low dose of l-NMMA in Sprague-Dawley rats affected the renal excretions of sodium and water without altering blood pressure, but at a high dose it induced hypertension 19.
Supplementation with L-arginine has been a common approach for testing the effect of nitric oxide enhancement on hypertension. By providing a source of nitrogen for synthesis of nitric oxide by NOS, L-arginine is thought to lower pressure by enhancing vasodilation of resistance vessels indirectly by augmenting the production of nitric oxide from NOS. This vasodilator action of nitric oxide (endothelium-derived relaxing factor; EDRF) depends on activation of sGC which converts guanosine triphosphate to its product, cyclic 3′, 5′-guanosine monophosphate (cGMP). It has been reported that the impaired nitric oxide production pathway may lead to the onset of essential hypertension 20. L-arginine and L-citrulline, which is converted to L-arginine, increased the production of nitric oxide and prevented the development of salt-sensitive hypertension in Dahl/Rapp rats 21. In patients with hypertension, the oral administration of l-arginine was an effective therapeutic option 22. In some studies, vasorelaxation in response to nitroglycerin was also blunted 23, indicating associated changes in responsiveness to nitric oxide either supplied exogenously or produced endogenously. Despite several lines of evidence, demonstrating antihypertensive actions of L-arginine, there is a paucity of evidence regarding the role of l-arginine in hypertension. It has been reported that newly diagnosed, mild to moderate hypertensive patients given l-arginine (2 g three times per day) had reduced blood pressure and improved vascular function after one week of treatment 24. Similarly in patients with mild hypertension, the infusion of l-arginine (500 mg/kg for 30 min) lowered the mean blood pressure by 8% and reduced the renovascular resistance 25. L-arginine reduced serum endothelin-1 and angiotensin 2 levels 26 which may be contributory factors in the lowering of blood pressure. Overall, these data support the idea that the endothelium plays an important role in the modulation of blood pressure and that nitric oxide is a key component responsible for this modulation and is generally known as endothelium-derived relaxing factor (EDRF). It may be possible to pharmacologically modulate the endogenous production of nitric oxide by exogenous agents to reduce blood pressure.
The upregulation of the nitric oxide/sGC/cGMP pathway in arterial hypertension has been identified as a promising therapeutic goal for lowering blood pressure and reducing associated complications related to heart and kidney function based on experimental models of hypertension and NOS-inhibition without causing tolerance 27.
Summary
A large body of evidence supports nitric oxide roles as a vasodilator, as an antihypertensive, antihypertrophic, and renoprotective agent 4. The linkage of a single molecule with such a diverse number of physiological systems in the human body underscores its promising therapeutic potential in cardiovascular and renovascular complications 4. As a sympatholytic agent, nitric oxide not only contributes to the regulation of blood pressure, but also plays a renoprotective role in hypertensive patients by antagonizing the deleterious effects of norepinephrine (noradrenaline) and angiotensin and by mediating the release of another promising gasotransmitter, hydrogen sulfide (H2S). In conclusion, studies have highlighted the beneficial roles of nitric oxide in the cardiovascular system and kidney, but also emphasized the link between nitric oxide and different physiological systems whose effects are either mediated by nitric oxide or antagonized by nitric oxide.
Nitric oxide supplements
Focusing on vasodilation, several sources 28 have suggested that nitric oxide (NO) is a prime solicitor in the process. Nitric oxide (NO) is not ingested directly, rather it is derived from substances endogenously manufactured or ingested. Nitric oxide (NO) is synthesized via at least two physiological pathways: nitric oxide synthase (NOS)-dependent and NOS-independent. Research pertaining to the nitric oxide synthase (NOS)-dependent nitric oxide donors pathway have consistently shown to not affect on VO2max 29. Thus, further research on the effects of nitric oxide (NO) on VO2max should shift its focus on investigating the nitric oxide synthase (NOS)-independent pathway instead.
Research on supplementation through the nitric oxide synthase (NOS)-independent pathway involves sodium nitrate and beetroot 30. The nitric oxide synthase (NOS)-independent donors have shown mixed results. Sodium nitrate decreased VO2 peak in two studies 31, 32, while beetroot juice increased VO2max in one study 33 and did not affect VO2peak or VO2max in three others 34, 35, 36.
Nitrates, like those found in beetroot juice, have garnered interest due to their effects on lowering blood pressure at rest 34, however there is also a line of research investigating their effects on performance. The current literature regarding the ergogenic effects of nitrates is mostly concentrated on four different nitric oxide donors: L-arginine, L-citrulline, sodium nitrate, and beetroot juice. These nitric oxide donors are categorized into two groups, based on whether they are oxidized in the nitric oxideS-dependent physiological pathway, or reduced in the nitric oxideS independent physiological pathway. L-arginine and L-citrulline pertain to the former, while sodium nitrate and beetroot juice pertain to the latter. The purpose of this study 30 was to investigate the effects of beetroot juice compared to placebo on VO2max and blood pressure during submaximal exercise on recreationally trained college-aged males. VO2max, respiratory exchange ratio, systolic blood pressure, and diastolic blood pressure were analyzed for differences between the supplement and the placebo. There were no significant differences in any of these variables after beetroot juice supplementation compared to placebo 30. At rest, beetroot juice has been shown to decrease resting systolic blood pressure 36 as well as diastolic blood pressure 33. Systolic and diastolic blood pressure at 70% of max heart rate calculated using the Karvonen formula did not show a significant change after beetroot juice supplementation. A study by Miyai et al. 37 investigated the blood pressure response to heart rate during exercise in 1033 normotensive men. The blood pressure mean values at 70% max heart rate from the present study were comparable to those found the study. The diastolic blood pressure means from the present study fell into the 50th percentile values of those 1033 men at 70% of heart rate reserve, while the systolic blood pressure means fell into the 25th percentile.
In a study by Larsen et al. 38, supplementation with sodium nitrate (0.1 mmol /kg of body mass/day for 3 days) in moderately trained subjects showed a decrease in VO2 at submaximal intensities, indicating a beneficial reduced oxygen cost during exercise. Gross efficiency, which was defined as work rate divided by energy expenditure, was also significantly improved. A later study by Larsen et al. 32 on moderately trained subjects used the same loading scheme for 2 days and also showed a significantly lower VO2 peak after sodium nitrate ingestion without any effect on time to exhaustion. A study done on welltrained subjects showed a similar significantly reduced VO2 peak compared to placebo, but with no effects on VO2 at submaximal intensities. The dosage in this study was more acute (3 hours pre-exercise) compared to previous studies and used 10 mg/kg of body mass of sodium nitrate 31.
In a study done on physically active individuals, beetroot supplementation for 15 days showed a significant increase in peak power and VO2max. Additionally, steady-state VO2 at moderate-intensity exercise was significantly reduced 2.5 hours after ingestion 33. In other studies, it has been shown to increase power output 35, delay time to exhaustion, and increase efficiency not only at the onset of exercise, but also in moderate (80% of gas exchange threshold) and severe intensity exercise (70% of the difference between the power output at gas exchange threshold and VO2 peak) 36.
Nitric oxide supplements have been shown to increase mitochondrial efficiency by improving the amount of oxygen reduced per ATP produced, otherwise known as the mitochondrial P/O ratio 39. Theoretically, this would explain the suggested benefits that previous studies have shown on the cardiorespiratory components of aerobic exercise. Keeping this in consideration, along with all the aforementioned results, it could be hypothesized that a nitric oxide supplement would help increase VO2max. With respect to the NOS-independent pathway, results are contradicting between two forms of NO donor. There are two studies using sodium nitrate that showed a significantly reduced VO2peak and VO2max following supplementation 31, while there is one study using beetroot juice that showed an increase in VO2max 33. Furthermore, the study that used beetroot juice used a ramp cycle ergometer test to gather VO2 data, while it has been shown that an individualized ramp treadmill protocol elicits higher, more valid values and is more likely to bring an individual to a true VO2max due to the increased volume of muscle mass used 40. In addition, it is widely accepted that typical blood pressure responses during incremental cardiorespiratory endurance exercise include an increase in systolic pressure and a maintenance of diastolic pressure. It is also known that NO is effective at reducing blood pressure at rest 33. However, there appear to be no studies that have investigated the effect of supplementation on blood pressure values during exercise. The purpose of this study was to investigate the effects beetroot juice on VO2max and on blood pressure during submaximal exercise in recreationally trained, college-aged males.
- The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Furchgott RF, Zawadzki JV. Nature. 1980 Nov 27; 288(5789):373-6.[↩]
- Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Ignarro LJ, Buga GM, Wood KS, Byrns RE, Chaudhuri G. Proc Natl Acad Sci U S A. 1987 Dec; 84(24):9265-9.[↩]
- Nitric oxide. The National Institute for Occupational Safety and Health (NIOSH). https://www.cdc.gov/niosh/npg/npgd0448.html[↩]
- Ahmad A, Dempsey SK, Daneva Z, et al. Role of Nitric Oxide in the Cardiovascular and Renal Systems. Int J Mol Sci. 2018;19(9):2605. Published 2018 Sep 3. doi:10.3390/ijms19092605 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6164974[↩][↩][↩][↩][↩][↩]
- Recoupling the cardiac nitric oxide synthases: tetrahydrobiopterin synthesis and recycling. Alkaitis MS, Crabtree MJ. Curr Heart Fail Rep. 2012 Sep; 9(3):200-10.[↩]
- Interaction between nitric oxide and renal α1-adrenoreceptors mediated vasoconstriction in rats with left ventricular hypertrophyin Wistar Kyoto rats. Ahmad A, Sattar MA, Azam M, Khan SA, Bhatt O, Johns EJ. PLoS One. 2018; 13(2):e0189386.[↩]
- Cyclic GMP and regulation of cyclic nucleotide hydrolysis. Sonnenburg WK, Beavo JA. Adv Pharmacol. 1994; 26():87-114.[↩]
- Santillo M.F., Mapa M.S.T. Phosphodiesterase (PDE5) inhibition assay for rapid detection of erectile dysfunction drugs and analogs in sexual enhancement products. Drug Test. Anal. 2018 doi: 10.1002/dta.2375[↩]
- NO signaling through cGMP in renal tissue fibrosis and beyond: key pathway and novel therapeutic target. Wang-Rosenke Y, Neumayer HH, Peters H. Curr Med Chem. 2008; 15(14):1396-406.[↩]
- Arginase upregulation and eNOS uncoupling contribute to impaired endothelium-dependent vasodilation in a rat model of intrauterine growth restriction. Grandvuillemin I, Buffat C, Boubred F, Lamy E, Fromonot J, Charpiot P, Simoncini S, Sabatier F, Dignat-George F, Peyter AC, Simeoni U, Yzydorczyk C. Am J Physiol Regul Integr Comp Physiol. 2018 Sep 1; 315(3):R509-R520.[↩]
- Reduced plasma concentrations of nitrogen oxide in individuals with essential hypertension. Node K, Kitakaze M, Yoshikawa H, Kosaka H, Hori M. Hypertension. 1997 Sep; 30(3 Pt 1):405-8.[↩]
- Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. Panza JA, Quyyumi AA, Brush JE Jr, Epstein SE. N Engl J Med. 1990 Jul 5; 323(1):22-7.[↩]
- Sildenafil in Term and Premature Infants: A Systematic Review. Clin Ther. 2015 Nov 1;37(11):2598-2607.e1. doi: 10.1016/j.clinthera.2015.07.019. Epub 2015 Oct 19. https://www.ncbi.nlm.nih.gov/pubmed/26490498[↩]
- Regular aerobic exercise augments endothelium-dependent vascular relaxation in normotensive as well as hypertensive subjects: role of endothelium-derived nitric oxide. Higashi Y, Sasaki S, Kurisu S, Yoshimizu A, Sasaki N, Matsuura H, Kajiyama G, Oshima T. Circulation. 1999 Sep 14; 100(11):1194-202.[↩]
- Effect of chronic tetrahydrobiopterin supplementation on blood pressure and proteinuria in 5/6 nephrectomized rats. Podjarny E, Hasdan G, Bernheim J, Rashid G, Green J, Korzets Z, Bernheim J. Nephrol Dial Transplant. 2004 Sep; 19(9):2223-7.[↩]
- Oral administration of tetrahydrobiopterin prevents endothelial dysfunction and vascular oxidative stress in the aortas of insulin-resistant rats. Shinozaki K, Nishio Y, Okamura T, Yoshida Y, Maegawa H, Kojima H, Masada M, Toda N, Kikkawa R, Kashiwagi A. Circ Res. 2000 Sep 29; 87(7):566-73.[↩]
- Hypertension in mice lacking the gene for endothelial nitric oxide synthase. Huang PL, Huang Z, Mashimo H, Bloch KD, Moskowitz MA, Bevan JA, Fishman MC. Nature. 1995 Sep 21; 377(6546):239-42.[↩]
- Effect of local intra-arterial NG-monomethyl-L-arginine in patients with hypertension: the nitric oxide dilator mechanism appears abnormal. Calver A, Collier J, Moncada S, Vallance P. J Hypertens. 1992 Sep; 10(9):1025-31.[↩]
- Effects of NG-nitro-L-arginine methyl ester on renal function and blood pressure. Lahera V, Salom MG, Miranda-Guardiola F, Moncada S, Romero JC. Am J Physiol. 1991 Dec; 261(6 Pt 2):F1033-7.[↩]
- Defective L-arginine-nitric oxide pathway in offspring of essential hypertensive patients. Taddei S, Virdis A, Mattei P, Ghiadoni L, Sudano I, Salvetti A. Circulation. 1996 Sep 15; 94(6):1298-303.[↩]
- L-arginine abrogates salt-sensitive hypertension in Dahl/Rapp rats. Chen PY, Sanders PW. J Clin Invest. 1991 Nov; 88(5):1559-67.[↩]
- Effect of oral L-arginine on blood pressure and symptoms and endothelial function in patients with systemic hypertension, positive exercise tests, and normal coronary arteries. Palloshi A, Fragasso G, Piatti P, Monti LD, Setola E, Valsecchi G, Galluccio E, Chierchia SL, Margonato A. Am J Cardiol. 2004 Apr 1; 93(7):933-5.[↩]
- Effects of race and hypertension on flow-mediated and nitroglycerin-mediated dilation of the brachial artery. Gokce N, Holbrook M, Duffy SJ, Demissie S, Cupples LA, Biegelsen E, Keaney JF Jr, Loscalzo J, Vita JA. Hypertension. 2001 Dec 1; 38(6):1349-54.[↩]
- The effects of sustained-release-L-arginine formulation on blood pressure and vascular compliance in 29 healthy individuals. Miller AL. Altern Med Rev. 2006 Mar; 11(1):23-9.[↩]
- Effects of L-arginine infusion on renal hemodynamics in patients with mild essential hypertension. Higashi Y, Oshima T, Ozono R, Watanabe M, Matsuura H, Kajiyama G. Hypertension. 1995 Apr; 25(4 Pt 2):898-902.[↩]
- Intravenous administration of L-arginine inhibits angiotensin-converting enzyme in humans. Higashi Y, Oshima T, Ono N, Hiraga H, Yoshimura M, Watanabe M, Matsuura H, Kambe M, Kajiyama G. J Clin Endocrinol Metab. 1995 Jul; 80(7):2198-202.[↩]
- Protective effects of BAY 41-2272 (sGC stimulator) on hypertension, heart, and cardiomyocyte hypertrophy induced by chronic L-NAME treatment in rats. Zanfolin M, Faro R, Araujo EG, Guaraldo AM, Antunes E, De Nucci G. J Cardiovasc Pharmacol. 2006 Mar; 47(3):391-5.[↩]
- Role of nitric oxide and adenosine in the onset of vasodilation during dynamic forearm exercise. Casey DP, Mohamed EA, Joyner MJ. Eur J Appl Physiol. 2013 Feb; 113(2):295-303.[↩]
- VO2max and ventilatory threshold of trained cyclists are not affected by 28-day L-arginine supplementation. Sunderland KL, Greer F, Morales J. J Strength Cond Res. 2011 Mar; 25(3):833-7[↩]
- Perez JM, Dobson JL, Ryan GA, Riggs AJ. The Effects of Beetroot Juice on VO2max and Blood Pressure during Submaximal Exercise. Int J Exerc Sci. 2019;12(2):332–342. Published 2019 Mar 1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6413851[↩][↩][↩]
- Bescós R, Rodríguez FA, Iglesias X, Ferrer MD, Iborra E, Pons A. Acute administration of inorganic nitrate reduces VO2peak in endurance athletes. Med Sci Sports Exerc. 2011;43(10):1979–1986[↩][↩][↩]
- Larsen FJ, Weitzberg E, Lundberg JO, Ekblom B. Dietary nitrate reduces maximal oxygen consumption while maintaining work performance in maximal exercise. Free Radic Biol Med. 2010;48(2):342–347[↩][↩]
- Vanhatalo A, Bailey SJ, Blackwell JR, DiMenna FJ, Pavey TG, Wilkerson DP, Benjamin N, Winyard PG, Jones AM. Acute and chronic effects of dietary nitrate supplementation on blood pressure and the physiological responses to moderate-intensity and incremental exercise. Am J Physiol Regul Integr Comp Physiol. 2010;299(4):R1121–R1131[↩][↩][↩][↩][↩]
- Bailey SJ, Winyard P, Vanhatalo A, Blackwell JR, DiMenna FJ, Wilkerson DP, Tarr J, Benjamin N, Jones AM. Dietary nitrate supplementation reduces the O2 cost of low-intensity exercise and enhances tolerance to high-intensity exercise in humans. J Appl Physiol. 2009;107(4):1144–1155[↩][↩]
- Lansley KE, Winyard PG, Bailey SJ, Vanhatalo A, Wilkerson DP, Blackwell JR, Gilchrist M, Benjamin N, Jones AM. Acute dietary nitrate supplementation improves cycling time trial performance. Med Sci Sports Exerc. 2011a;43(6):1125–1131[↩][↩]
- Lansley KE, Winyard PG, Fulford J, Vanhatalo A, Bailey SJ, Blackwell JR, DiMenna FJ, Gilchrist M, Benjamin N, Jones AM. Dietary nitrate supplementation reduces the O2 cost of walking and running: a placebo-controlled study. J Appl Physiol. 2011b;110(3):591–600[↩][↩][↩]
- Miyai N, Arita M, Miyashita K, Morioka I, Shiraishi T, Nishio I. Blood pressure response to heart rate during exercise test and risk of future hypertension. Hypertension. 2002;39(3):761–766[↩]
- Larsen FJ, Weitzberg E, Lundberg JO, Ekblom B. Effects of dietary nitrate on oxygen cost during exercise. Acta Physiol. 2007;191(1):59–66[↩]
- Larsen FJ, Schiffer TA, Borniquel S, Sahlin K, Ekblom B, Lundberg JO, Weitzberg E. Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell Metab. 2011;13(2):149–159[↩]
- Myers J, Buchanan N, Smith D, Neutel J, Bowes E, Walsh D, Froelicher VF. Individualized ramp treadmill: observations on a new protocol. Chest. 1992;101(5):236S–241S[↩]





{kind=link}