
Contents
- What is obsessive compulsive disorder
- Obsessive compulsive disorder in children
- What might parents notice?
- How is obsessive compulsive disorder diagnosed in children?
- How is obsessive compulsive disorder treated in children?
- When should medicine be considered for children with obsessive compulsive disorder?
- What kinds of medicines help obsessive compulsive disorder in children?
- How long does it take for obsessive compulsive disorder medicines to work?
- How helpful are these medicines for children with obsessive compulsive disorder?
- Are there permanent side effects from using obsessive compulsive disorder medicines?
- Will medicine ‘Cure’ my Child’s obsessive compulsive disorder?
- Will my child need to take these medicines forever?
- What can parents do?
- What is obsessive compulsive personality disorder
- Obsessive compulsive disorder signs and symptoms
- Obsessive compulsive disorder complications
- Obsessive compulsive disorder causes
- Obsessive compulsive disorder prevention
- Obsessive compulsive disorder diagnosis
- Obsessive compulsive disorder treatment
What is obsessive compulsive disorder
Obsessive-compulsive disorder also known as OCD, is a type of anxiety disorder. If you have obsessive compulsive disorder, you have frequent, upsetting thoughts called obsessions. To try to control the thoughts, you feel an overwhelming urge to repeat certain rituals or behaviors. These are called compulsions. Examples of obsessions are a fear of germs or a fear of being hurt. Compulsions include washing your hands, counting, checking on things, or cleaning. With obsessive compulsive disorder, the thoughts and rituals cause distress and get in the way of your daily life. You probably recognize that your obsessive thoughts and compulsive behaviors are irrational—but even so, you feel unable to resist them and break free.
Obsessive compulsive disorder usually develops in late childhood or early teenage years and without proper treatment can become a chronic condition. Symptoms usually begin gradually and tend to vary in severity throughout life. Symptoms generally worsen when you experience greater stress. obsessive compulsive disorder, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling.
According to International OCD Foundation best estimates, there are that about 1 in 100 adults – or between 2 to 3 million adults in the United States – currently have obsessive compulsive disorder 1. This is roughly the same number of people living in the city of Houston, Texas. There are also at least 1 in 200 – or 500,000 – children and teens that have obsessive compulsive disorder 2. This is about the same number of children who have diabetes. That means four or five children with obsessive compulsive disorder are likely to be enrolled in any average size elementary school. In a medium to large high school, there could be 20 students struggling with the challenges caused by obsessive compulsive disorder 3. Obsessive compulsive disorder affects men, women and children of all races and backgrounds equally.
There are 2 kinds of obsessive compulsive disorder symptoms:
- Obsessions – irrational thoughts and fears. Obsessions are involuntary thoughts, images, or impulses that occur over and over again in your mind. You don’t want to have these ideas, but you can’t stop them. Unfortunately, these obsessive thoughts are often disturbing and distracting.
- Compulsions – repetitive behaviors or rituals, which are carried out to reduce anxiety. Compulsions are behaviors or rituals that you feel driven to act out again and again. Usually, compulsions are performed in an attempt to make obsessions go away.
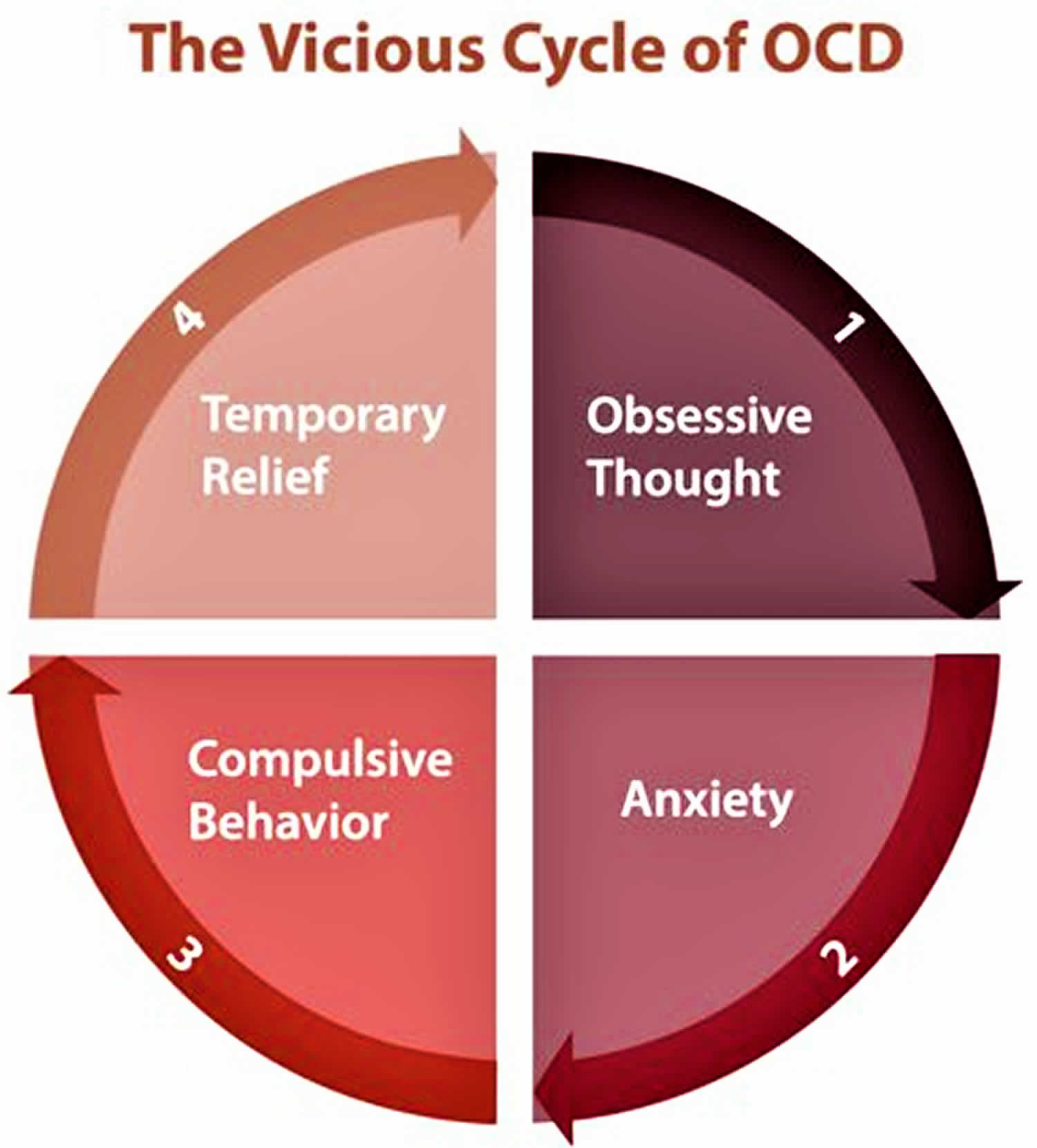
It’s normal, on occasion, to go back and double-check that the iron is unplugged or your car is locked. But if you suffer from obsessive-compulsive disorder (OCD), obsessive thoughts and compulsive behaviors become so consuming they interfere with your daily life. The compulsions can take considerable time, impacting on normal day-to-day activities. No matter what you do, you can’t seem to shake them. For example, a person with obsessive compulsive disorder may need to check the iron is turned off 20 times to make sure it’s really turned off, or wash your hands until they’re scrubbed raw. While you don’t derive any sense of pleasure from performing these repetitive behaviors, they may offer some passing relief for the anxiety generated by the obsessive thoughts.
You may try to ignore or stop your obsessions, but that only increases your distress and anxiety. Ultimately, you feel driven to perform compulsive acts to try to ease your stress. Despite efforts to ignore or get rid of bothersome thoughts or urges, they keep coming back. This leads to more ritualistic behavior — the vicious cycle of OCD.
Most people with obsessive compulsive disorder fall into one of the following categories:
- Washers are afraid of contamination. They usually have cleaning or hand-washing compulsions.
- Checkers repeatedly check things (oven turned off, door locked, etc.) that they associate with harm or danger.
- Doubters and sinners are afraid that if everything isn’t perfect or done just right something terrible will happen, or they will be punished.
- Counters and arrangers are obsessed with order and symmetry. They may have superstitions about certain numbers, colors, or arrangements.
- Hoarders fear that something bad will happen if they throw anything away. They compulsively hoard things that they don’t need or use. They may also suffer from other disorders, such as depression, PTSD, compulsive buying, kleptomania, ADHD, skin picking, or tic disorders.
Other conditions can be closely related to obsessive compulsive disorder, such as:
- body dysmorphic disorder – excessive concern over a body part, and believing it is abnormal in some way
- trichotillomania – compulsive hair pulling
- hypochondriasis – fear and preoccupation with developing a physical illness
- compulsive hoarding
- anorexia nervosa.
People who suffer from obsessive compulsive disorder are also more likely to develop depression or other anxiety disorders, such as panic disorder or social anxiety.
People suffering from obsessive compulsive disorder are usually aware of their behaviors and know they are excessive. This can cause shame, forcing people to keep their condition secret. You may try to avoid situations that trigger or worsen your symptoms or self-medicate with alcohol or drugs. But while it can seem like there’s no escaping your obsessions and compulsions, there are plenty of things you can do to help yourself and regain control of your thoughts and actions.
The sooner people with obsessive compulsive disorder seek effective treatment, the closer they are to regaining control of their lives.
Researchers think brain circuits may not work properly in people who have obsessive compulsive disorder. OCD tends to run in families. The symptoms often begin in children or teens. But help is available. With treatment and self-help strategies, you can break free of the unwanted thoughts and irrational urges and take back control of your life. Treatments include psychotherapy, medicines, or both. One type of psychotherapy, cognitive behavioral therapy (CBT), is useful for treating obsessive compulsive disorder.
Most studies show that, on average, about 70% of patients with obsessive compulsive disorder will benefit from either medicine or cognitive behavior therapy (CBT). Patients who respond to medicine usually show a 40 to 60% reduction in obsessive compulsive disorder symptoms, while those who respond to CBT often report a 60 to 80% reduction in obsessive compulsive disorder symptoms.
However, medicines have to be taken on a regular basis and patients must actively participate in cognitive behavioral therapy (CBT) for the treatments to work. Unfortunately, studies show that at least 25% of obsessive compulsive disorder patients refuse cognitive behavioral therapy (CBT), and as many as half of obsessive compulsive disorder patients discontinue medicines due to side effects or for other reasons.
There’s a difference between being a perfectionist — someone who requires flawless results or performance, for example — and having obsessive compulsive disorder. obsessive compulsive disorder thoughts aren’t simply excessive worries about real problems in your life or liking to have things clean or arranged in a specific way.
If your obsessions and compulsions are affecting your quality of life, see your doctor or mental health professional.
At what age does obsessive compulsive disorder begin?
Obsessive compulsive disorder can start at any time from preschool to adulthood. Although obsessive compulsive disorder does occur at earlier ages, there are generally two age ranges when obsessive compulsive disorder first appears. The first range is between ages 10 and 12 and the second between the late teens and early adulthood.
What are common obstacles to effective obsessive compulsive disorder treatment?
Studies find that it takes an average of 14 to 17 years from the time obsessive compulsive disorder begins for people to obtain appropriate treatment.
- Some people choose to hide their symptoms, often in fear of embarrassment or stigma. Therefore, many people with obsessive compulsive disorder do not seek the help of a mental health professional until many years after the onset of symptoms.
- Until recently, there was less public awareness of obsessive compulsive disorder, so many people were unaware that their symptoms represented an illness that could be treated.
- Lack of proper training by some health professionals often leads to the wrong diagnosis. Some patients with obsessive compulsive disorder symptoms will see several doctors and spend several years in treatment before receiving a correct diagnosis.
- Difficulty finding local therapists who can effectively treat obsessive compulsive disorder.
- Not being able to afford proper treatment.
Obsessive compulsive disorder in children
At least 1 in 200 children and teens in the United States have obsessive compulsive disorder. Understanding the special impact that the disorder has on their lives is important in helping them get the right treatment.
Children don’t always talk about the fears and behaviors obsessive compulsive disorder causes. They may feel embarrassed or confused about their fear and keep it to themselves. They may try to hide rituals they do. They may worry that others will tease them about their fears and rituals.
Children with obsessive compulsive disorder feel unable to stop focusing on their obsessions. They feel like they have to do the rituals to guard against bad things they worry could happen. For some kids, doing a ritual is the only way they feel “everything’s OK.”
What might parents notice?
Many children have obsessive compulsive disorder for a while before parents, teachers, or doctors realize it. Parents might only learn about the obsessive compulsive disorder if their child tells them, or if they notice the child seems overly worried or is doing behaviors that seem like rituals.
Sometimes, parents may notice other difficulties that can be a result of obsessive compulsive disorder. For example, obsessive compulsive disorder can cause children to:
- have trouble concentrating on schoolwork, or enjoying activities
- feel and act irritable, upset, sad, or anxious
- seem unsure of whether things are OK
- have trouble deciding or choosing
- take much too long to do everyday tasks, like getting dressed, organizing a backpack, completing homework, or taking a shower
- get upset and lose their temper if they can’t make something perfect or if something is out of place
- insist that a parent say or do something an exact way
- anger management problems — this is because the parents have become unwilling (or are unable) to comply with the child’s obsessive compulsive disorder related demands. Even when parents set reasonable limits, kids and teens with obsessive compulsive disorder can become anxious and angry.
How is obsessive compulsive disorder diagnosed in children?
To diagnose obsessive compulsive disorder, you’ll meet with a child psychologist or psychiatrist, who will interview you and your child to learn more details. You and your child also may fill out checklists and questionnaires. These will help the psychologist or psychiatrist make a diagnosis. There are no lab tests to diagnose obsessive compulsive disorder.
When obsessive compulsive disorder is diagnosed, it can be a relief to children and parents. obsessive compulsive disorder can get better with the right attention and care.
How is obsessive compulsive disorder treated in children?
Obsessive compulsive disorder is treated with medicine and psychotherapy. For children who need medicines, doctors give SSRIs (selective serotonin reuptake inhibitors), like Zoloft, Prozac, and Luvox.
Therapists treat obsessive compulsive disorder with cognitive behavioral therapy (CBT). During this kind of talk-and-do therapy, children learn about obsessive compulsive disorder and begin to understand it better. They learn that doing rituals keeps obsessive compulsive disorder going strong, and that not doing rituals helps to weaken obsessive compulsive disorder. They learn ways to face fears, cope with them, and resist doing rituals. Learning these skills helps stop the cycle of obsessive compulsive disorder.
Part of treatment is coaching parents on how they can help children get better. Parents learn how to respond to obsessive compulsive disorder situations, and how to support their child’s progress without giving in to rituals.
When should medicine be considered for children with obsessive compulsive disorder?
Both cognitive behavioral therapy (CBT) and medicine effectively treat obsessive compulsive disorder in children and adolescents. Their use is supported by the treatment guidelines of the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry. Medicines should only be considered when there are moderate to severe obsessive compulsive disorder symptoms.
What kinds of medicines help obsessive compulsive disorder in children?
Antidepressants are usually the first kind of medicine that a doctor will try. Your doctor might refer to these medicines as “Selective Serotonin-Reuptake Inhibitors” (SSRI’s) or “Tricyclics” (TCA’s):
Selective Serotonin-Reuptake Inhibitors (SSRI’s):
- citalopram (Celexa®)
- escitalopram (Lexapro®)
- fluvoxamine (Luvox®)
- fluoxetine (Prozac®)
- paroxetine (Paxil®)
- sertraline (Zoloft®)
Tricyclic Antidepressant (TCA):
- clomipramine (Anafranil®)
Only four obsessive compulsive disorder medicines have been approved by the FDA for use in children: clomipramine (Anafranil®), fluoxetine (Prozac®), fluvoxamine (Luvox®) and sertraline (Zoloft®), but doctors can prescribe any obsessive compulsive disorder medicines to children if they feel it is needed.
Factors that may guide the medicine choice include:
- positive response to a certain drug by other family members
- presence of other disorders
- potential for side effects
- cost or availability
How long does it take for obsessive compulsive disorder medicines to work?
All obsessive compulsive disorder medicines work slowly. It is important to not give up on a medicine until it has been taken at the right dose for 10 to 12 weeks. Studies have also shown that improvement of childhood obsessive compulsive disorder can continue for at least a year after starting medicine.
How helpful are these medicines for children with obsessive compulsive disorder?
In the largest child obsessive compulsive disorder treatment study to date (POTS) 4, remission (absence of any major symptoms) occurred in about 1 in 5 children on medicine and in more than half of those with medicine and cognitive behavior therapy (CBT). In addition, many more children had improvement (but not full remission). Some patients will have no response at all, which does not mean that other medicines will not help.
Are there permanent side effects from using obsessive compulsive disorder medicines?
These drugs appear very safe with long-term use and side effects reverse when they are stopped. There is no current evidence that they do permanent damage to the body.
Will medicine ‘Cure’ my Child’s obsessive compulsive disorder?
Obsessive compulsive disorder medicines control and decrease symptoms, but do not “cure” the disorder. obsessive compulsive disorder is usually well controlled when proper treatment is in place. Symptoms often return when the child stops taking the medicine.
Will my child need to take these medicines forever?
Many doctors suggest that obsessive compulsive disorder treatment should continue for at least one year even after symptoms have stopped. Unfortunately, obsessive compulsive disorder drugs do not ‘cure’ the illness. When medicine is stopped, symptoms often return within a few weeks to months. If they return, most patients will respond well after restarting the medicine.
What can parents do?
Talk with your child about what’s going on
Talk supportively, listen, and show love. Say something that works for your child’s situation like, “I notice you worry about your covers being smooth, your socks being even, and your shoes lined up. I notice it gets you stressed if you can’t fix things just so.”
Say that something called obsessive compulsive disorder might be causing the worry and the fixing. Tell your child that a checkup with a doctor can find out if this is what’s going on. Reassure your child that this can get better, and that you want to help.
Make an appointment with a child psychiatrist or psychologist. Your child’s doctor can help you find the right person.
Take part in your child’s therapy. Learn all you can about how parents can help when their child has obsessive compulsive disorder. Overcoming obsessive compulsive disorder is a process. There will be many therapy appointments, and it’s important to go to them all. Practice the things the therapist recommends. Encourage your child.
Get support, and give it. There are lots of resources and support for parents and families dealing with obsessive compulsive disorder. Knowing that you’re not alone can help you cope. Sharing success stories with other parents can give you hope and confidence.
What is obsessive compulsive personality disorder
Obsessive-compulsive personality disorder is characterized by a preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency.
When rules and established procedures do not dictate the correct answer, decision making may become a time-consuming, often painful process. Individuals with obsessive-compulsive personality disorder may have such difficulty deciding which tasks take priority or what is the best way of doing some particular task that they may never get started on anything.
They are prone to become upset or angry in situations in which they are not able to maintain control of their physical or interpersonal environment, although the anger is typically not expressed directly. For example, a person may be angry when service in a restaurant is poor, but instead of complaining to the management, the individual ruminates about how much to leave as a tip. On other occasions, anger may be expressed with righteous indignation over a seemingly minor matter.
People with this disorder may be especially attentive to their relative status in dominance-submission relationships and may display excessive deference to an authority they respect and excessive resistance to authority that they do not respect.
Individuals with obsessive-compulsive personality disorder usually express affection in a highly-controlled or stilted fashion and may be very uncomfortable in the presence of others who are emotionally expressive. Their everyday relationships have a formal and serious quality, and they may be stiff in situations in which others would smile and be happy (e.g., greeting a lover at the airport). They carefully hold themselves back until they are sure that whatever they say will be perfect. They may be preoccupied with logic and intellect.
A personality disorder is an enduring pattern of inner experience and behavior that deviates from the norm of the individual’s culture. The pattern is seen in two or more of the following areas: cognition; affect; interpersonal functioning; or impulse control. The enduring pattern is inflexible and pervasive across a broad range of personal and social situations. It typically leads to significant distress or impairment in social, work, or other areas of functioning. The pattern is stable and of long duration, and its onset can be traced back to early adulthood or adolescence.
Obsessive-Compulsive Personality Disorder Symptoms
A pervasive pattern of preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency, beginning by early adulthood and present in a variety of contexts, as indicated by four (or more) of the following:
- Is preoccupied with details, rules, lists, order, organization, or schedules to the extent that the major point of the activity is lost
- Shows perfectionism that interferes with task completion (e.g., is unable to complete a project because his or her own overly strict standards are not met)
- Is excessively devoted to work and productivity to the exclusion of leisure activities and friendships (not accounted for by obvious economic necessity)
- Is overconscientious, scrupulous, and inflexible about matters of morality, ethics, or values (not accounted for by cultural or religious identification)
- Is unable to discard worn-out or worthless objects even when they have no sentimental value
- Is reluctant to delegate tasks or to work with others unless they submit to exactly his or her way of doing things
- Adopts a miserly spending style toward both self and others; money is viewed as something to be hoarded for future catastrophes
- Shows significant rigidity and stubbornness
Because personality disorders describe long-standing and enduring patterns of behavior, they are most often diagnosed in adulthood. It is uncommon for them to be diagnosed in childhood or adolescence, because a child or teen is under constant development, personality changes, and maturation. However, if it is diagnosed in a child or teen, the features must have been present for at least 1 year.
Obsessive-compulsive personality disorder is approximately twice as prevalent in males than females, and occurs in between 2.1 and 7.9 percent of the general population.
Like most personality disorders, obsessive-compulsive personality disorder typically will decrease in intensity with age, with many people experiencing few of the most extreme symptoms by the time they are in their 40s or 50s.
Obsessive-Compulsive Personality Disorder Diagnosis
Personality disorders such as obsessive-compulsive personality disorder are typically diagnosed by a trained mental health professional, such as a psychologist or psychiatrist. Family physicians and general practitioners are generally not trained or well-equipped to make this type of psychological diagnosis. So while you can initially consult a family physician about this problem, they should refer you to a mental health professional for diagnosis and treatment. There are no laboratory, blood, or genetic tests that are used to diagnose obsessive-compulsive personality disorder.
Many people with obsessive-compulsive personality disorder don’t seek out treatment. People with personality disorders, in general, do not often seek out treatment until the disorder starts to significantly interfere or otherwise impact a person’s life. This most often happens when a person’s coping resources are stretched too thin to deal with stress or other life events.
A diagnosis for obsessive-compulsive personality disorder is made by a mental health professional comparing your symptoms and life history with those listed here. They will make a determination whether your symptoms meet the criteria necessary for a personality disorder diagnosis.
Obsessive-Compulsive Personality Disorder Causes
Researchers today don’t know what causes obsessive-compulsive personality disorder, however, there are many theories about the possible causes. Most professionals subscribe to a biopsychosocial model of causation — that is, the causes are likely due to biological and genetic factors, social factors (such as how a person interacts in their early development with their family and friends and other children), and psychological factors (the individual’s personality and temperament, shaped by their environment and learned coping skills to deal with stress). This suggests that no single factor is responsible — rather, it is the complex and likely intertwined nature of all three factors that are important. If a person has this personality disorder, research suggests that there is a slightly increased risk for this disorder to be “passed down” to their children.
Obsessive compulsive personality disorder treatment
Individuals who suffer from obsessive-compulsive personality disorder often are characterized by their lack of openness and flexibility in not only their daily routines, but also with interpersonal relationships and expectations. The overwhelming preoccupation with orderliness, perfectionism, and control of their lives and relationships means that most types of treatment are going to be, at best, difficult. Treatment options which do not fit within the client’s cognitive schema will likely be quickly rejected rather than attempted.
Individuals who suffer from this disorder have difficulty in incorporating new and changing information into their lives, so new learning takes place only over a great deal of time and with as much effort on both the clinician’s and client’s part. Their ability to work with others is equally affected, since they see the world as black and white— their way of doing things and the wrong way of doing things. Naturally, this faulty logic will also be translated into their therapeutic relationship with the clinician and their treatment. It is therefore unlikely the clinician will have much success in using techniques or treatment modalities which haven’t first been approved by the patient for use. Sometimes this may be done simply by stating the effectiveness of a given treatment for a specific problem, citing relevant research studies. More often, though, this technique won’t be effective.
When this disorder is combined with the presentation of a medical illness, physicians should expect a logical and coherent presentation of troubling symptoms with little emotionality attached to their physical discomfort. Treatment is most effective when the nature of the disease process is first discussed with the individual, as well as typical and accepted treatments. A physician in this instance should stick to the facts of the presenting problem and underlying disorder rather than offering vague impressions of their opinion. Since the individual with this disorder tends to be meticulous and concerned with details, the treatment regimen — once accepted — will likely be adhered to rigorously, without incident.
Psychotherapy
As with most personality disorders, individuals seek treatment for items in their life which have become overwhelming to their existing coping skills. These skills may be somewhat limited in the first place because of their disorder. While they may be generally effective enough in most instances to shield the client from stress and emotional difficulties, during times of increased stress, work pressure, family problems, etc., the underlying disorder will become more evident in day-to-day behaviors.
As with most personality disorders, treatment is often focused on short-term symptom relief and the support of existing coping mechanisms while teaching new ones. Long-term or substantive work on personality change is usually beyond most clinician’s skill levels, and patient’s budgets. Obsessive-compulsive personality disorder is especially resistant to such changes, because of the basic makeup of this disorder.
Short-term therapy will be most likely to be beneficial when the patient’s current support system and coping skills are examined. Those skills which are not currently working could be reinforced with additional skill sets. Social relationships can also be examined, reinforcing strong, positive relationships while having the client re-examine negative or harmful relationships. One important aspect is to try and have the individual examine and properly identify their feeling states, rather than just intellectualizing or distancing themselves from their emotions. This can be accomplished through a variety of techniques, such as feeling identification (e.g., the “feeling faces”) at the onset of every therapy session. Homework might include writing feelings down in a journal, especially as they notice them. Proper identification and realization of feelings can bring about much change in and of itself.
Individuals suffering from obsessive-compulsive personality disorder often are not in touch with their emotional states as much as their thoughts. Leading the client away from describing situations, events, and daily happenings and to talking about how such situations, events and daily happenings made them feel may be helpful. Sometimes the patient may complain he or she doesn’t remember or know how he or she felt at the time; the journal becomes a useful tool at this point.
Therapy with people who have this disorder can sometimes be trying, since they can see the world in a very “all-or-nothing” manner. Beck’s cognitive therapy doesn’t seem to be all that effective in treatment, and cognitive approaches in general probably aren’t useful in this case. Clinicians must be willing to undergo verbal attacks on their professionalism and knowledge, as such skepticism about a therapist’s treatment approach from the client with this disorder can be expected. Clinicians should also be careful about engaging the client within these verbal attacks or intellectual discussions, as they continue to distance the patient from his or her feelings. And take the focus off of the client and onto unrelated matters (e.g., a therapist’s professional training).
Most people who suffer from this personality disorder (and the different, but related, obsessive-compulsive disorder) lead relatively normal lives, may have a family, friends, and work regularly. Clinicians should be careful not to overgeneralize psychopathology and look to change aspects of the patient’s personality he or she is not ready or willing to change. This means, in effect, that if the way they relate to others in their environment (which a clinician might characterize as a personality disorder) is working for them, a clinician should not seek to change it 180 degrees without the client’s purposeful consent. Therapy will most often be most effective when it focuses on correcting short-term difficulties currently being experienced. It will become increasingly less effective when the goal of therapy is a complex, long-term personality change.
Although a group therapy modality may be helpful and an effective treatment option, most people who suffer from this disorder will not be able to withstand the minimum social contact necessary to gain a healthy group dynamic. They may quickly become ostracized by the group for pointing out other people’s deficits and “wrong-headed” ways of doing things.
Hospitalization
Hospitalization is rarely needed for people who suffer from this disorder, unless an extreme or severe stressor or stressful life event occurs which increases the compulsive behaviors to an extent where regular daily activities are halted or present possible risks of harm to the patient. Hospitalization may also be needed when the obsessive thoughts do not allow the individual to conduct any usual activities, paralyzing them in bed or with their accompanying compulsive behaviors.
Medications
In most cases, medication for this disorder is not indicated unless the individuals is also suffering from another psychiatric disorder. However, newer medications such as Prozac, an selective serotonin reuptake inhibitor (SSRI), have been approved for the treatment of obsessive-compulsive disorder and may provide some relief to individuals with the related personality disorder. Long-term use, though, is rarely indicated, appropriate, or beneficial.
Self-Help
Self-help methods for the treatment of this disorder are often overlooked by the medical profession because very few professionals are involved in them. Support groups, though, offer an excellent adjunct to continuing medication check-ups once a month, and a way to gain emotional and social support through the community. These groups also allow others to ensure the client is doing well and promotes the client’s independence and stability. Many support groups exist within communities throughout the world which are devoted to helping individuals with this disorder share their commons experiences and feelings.
Such support groups are recommended to individuals suffering from this disorder, especially if they have found therapy unhelpful or too expensive.
Obsessive compulsive disorder signs and symptoms
The symptoms of obsessive-compulsive disorder (OCD) are known as obsessions and compulsions. Obsessive-compulsive disorder usually includes both obsessions and compulsions. But it’s also possible to have only obsession symptoms or only compulsion symptoms. Obsessions are irrational thoughts and fears that intrude on everyday thoughts and may include inappropriate visual images. Compulsions are repetitive behaviors or rituals, which occur as a response to the obsessions and are an attempt to reduce anxiety. You may or may not realize that your obsessions and compulsions are excessive or unreasonable, but they take up a great deal of time and interfere with your daily routine and social or work functioning.
There are a variety of different symptoms involved in obsessive compulsive disorder, but often they follow certain common themes.
Obsessions (thoughts)
Obsessive compulsive disorder obsessions are repeated, persistent and unwanted thoughts, urges or images that are intrusive and cause distress or anxiety. You might try to ignore them or get rid of them by performing a compulsive behavior or ritual. These obsessions typically intrude when you’re trying to think of or do other things.
Common obsessions include:
- Fear of contamination due to germs or illness, which may lead to avoiding hand contact or toilets, and an excessive need to wash and clean
- Fear of hurting others – for example, your own children – or injuring someone in a car accident
- Preoccupation with having things in order and symmetrical (the idea that everything must line up “just right”) or with following certain patterns
- Sexual or pornographic thoughts or images
- Worrying you have forgotten to lock doors or turn off appliances
- Aggressive or horrific thoughts about harming yourself or others
- Fear of losing or not having things you might need
- Superstitions — excessive attention to something considered lucky or unlucky
- Preoccupation with religious or moral issues.
Examples of obsession signs and symptoms include:
- Fear of being contaminated by touching objects others have touched
- Doubts that you’ve locked the door or turned off the stove
- Intense stress when objects aren’t orderly or facing a certain way
- Images of hurting yourself or someone else that are unwanted and make you uncomfortable
- Thoughts about shouting obscenities or acting inappropriately that are unwanted and make you uncomfortable
- Avoidance of situations that can trigger obsessions, such as shaking hands
- Distress about unpleasant sexual images repeating in your mind
Compulsions (behaviors)
Obsessive compulsive disorder compulsions are repetitive behaviors that you feel driven to perform. These repetitive behaviors or mental acts are meant to prevent or reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
You may make up rules or rituals to follow that help control your anxiety when you’re having obsessive thoughts. These compulsions are excessive and often are not realistically related to the problem they’re intended to fix.
Common compulsions include:
- Cleaning: excessive hand washing, showering or house cleaning due to fear of germs, which may result in dermatitis of the hands
- Checking: a compulsive need to continually check things, such as taps, locks or light switches due to a fear of damage or harm or to maintain order and symmetry
- Counting items or objects such as paving stones on a walk
- Hair pulling and hair loss
- Skin picking
- Hoarding random objects, such as junk mail, old newspapers or empty food containers
- Praying excessively or engaging in rituals triggered by religious fear
- Constant demands for reassurance from others.
Examples of compulsion signs and symptoms include:
- Hand-washing until your skin becomes raw
- Spending a lot of time washing or cleaning
- Checking doors repeatedly to make sure they’re locked
- Checking the stove repeatedly to make sure it’s off
- Counting in certain patterns
- Counting, tapping, repeating certain words, or doing other senseless things to reduce anxiety
- Silently repeating a prayer, word or phrase
- Arranging your canned goods to face the same way
- Excessive double-checking of things, such as locks, appliances, and switches
- Repeatedly checking in on loved ones to make sure they’re safe
If you or someone you know displays any of the above obsessive compulsive disorder symptoms to the extent that it affects quality of life, visit a doctor for an assessment. Some behaviors not listed here may still be obsessive compulsive disorder symptoms. Obsessive compulsive disorder is characterized by the obsessive nature of the behavior as much as the behavior itself.
Obsessive compulsive disorder symptoms in children
While the onset of obsessive-compulsive disorder usually occurs during adolescence or young adulthood, younger children sometimes have symptoms that look like obsessive compulsive disorder. However, the symptoms of other disorders, such as ADHD, autism, and Tourette’s syndrome, can also look like obsessive-compulsive disorder, so a thorough medical and psychological exam is essential before any diagnosis is made.
Obsessive compulsive disorder complications
Problems resulting from OCD may include, among others:
- Health issues, such as contact dermatitis from frequent hand-washing
- Inability to attend work, school or social activities
- Troubled relationships
- Overall poor quality of life
- Suicidal thoughts and behavior
Obsessive compulsive disorder causes
It’s not clear what causes obsessive compulsive disorder. Like many mental disorders, it’s thought to develop due to a combination of genetic and environmental factors. There are several theories about the causes of obsessive compulsive disorder, including:
- Genetic – having a first-degree relative with obsessive compulsive disorder may increase the chance of someone developing it. Research shows that obsessive compulsive disorder does run in families and that genes likely play a role in the development of the disorder. Genes appear to be only partly responsible for causing the disorder though. No one really knows what other factors might be involved, perhaps an illness or even ordinary life stresses that may induce the activity of genes associated with the symptoms of obsessive compulsive disorder. Some experts think that obsessive compulsive disorder that begins in childhood may be different from the obsessive compulsive disorder that begins in adults. For example, a recent review of twin studies3 has shown that genes play a larger role when obsessive compulsive disorder starts in childhood (45-65%) compared to when it starts in adulthood (27-47%).
- Biological – functional, structural or chemical abnormalities in the brain are currently being researched. Some links have been found to irregular levels of serotonin, the chemical that sends messages to the brain.
- Environmental – some research suggests that obsessive compulsive disorder behaviors could be learned following a stressful event, such as catching a serious disease from contamination. obsessive compulsive disorder rituals may even be learned from others, such as from a parent with obsessive compulsive disorder.
Obsessive compulsive disorder usually begins in adolescence or young adulthood, and tends to appear at a younger age in boys than in girls. Researchers have found that several parts of the brain, as well as biological processes, play a key role in obsessive thoughts and compulsive behavior, as well as the fear and anxiety related to them. Researchers also know that people who have suffered physical or sexual trauma are at an increased risk for obsessive compulsive disorder.
Research suggests that obsessive compulsive disorder involves problems in communication between the front part of the brain and deeper structures. These brain structures use a chemical messenger called serotonin. Pictures of the brain at work also show that in some people, the brain circuits involved in obsessive compulsive disorder become more normal with either serotonin medicines or cognitive behavior therapy (CBT).
Some children may develop a sudden onset or worsening of obsessive compulsive disorder symptoms after a streptococcal infection; this post-infectious autoimmune syndrome is called Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections (PANDAS).
Personality traits and distressing life events may also play a role in developing obsessive compulsive disorder. Researchers are currently looking at how environmental factors and stress may play a role. They are also working on developing better treatments for obsessive compulsive disorder by studying how the functioning of the brain affects feelings such as fear and anxiety.
However, if you’re concerned that you or someone you know has obsessive compulsive disorder, it’s important to seek treatment rather than focusing on the cause.
Risk factors for obsessive compulsive disorder
Factors that may increase the risk of developing or triggering obsessive-compulsive disorder include:
- Family history. Having parents or other family members with the disorder can increase your risk of developing obsessive compulsive disorder.
- Stressful life events. If you’ve experienced traumatic or stressful events, your risk may increase. This reaction may, for some reason, trigger the intrusive thoughts, rituals and emotional distress characteristic of obsessive compulsive disorder.
- Other mental health disorders. Obsessive compulsive disorder may be related to other mental health disorders, such as anxiety disorders, depression, substance abuse or tic disorders.
Obsessive compulsive disorder prevention
There’s no sure way to prevent obsessive-compulsive disorder. However, getting treatment as soon as possible may help prevent obsessive compulsive disorder from worsening and disrupting activities and your daily routine.
Obsessive compulsive disorder diagnosis
Obsessive-compulsive disorder (OCD) symptoms can feel embarrassing or shameful. For this reason, obsessive compulsive disorder can go undiagnosed for much too long, during which time compulsive behavior can become ingrained and damaging. This may mean adults become housebound or children cannot attend school. If you or someone you know has obsessions or compulsions that are unreasonable and impact on daily life, don’t delay going to visit a doctor.
There is no single ‘test’ for obsessive compulsive disorder, but a health professional can make a diagnosis based on an assessment of the person’s behaviors, thoughts and feelings.
Steps to help diagnose obsessive compulsive disorder may include:
- Physical exam. This may be done to help rule out other problems that could be causing your symptoms and to check for any related complications.
- Lab tests. These may include, for example, a complete blood count (CBC), a check of your thyroid function, and screening for alcohol and drugs.
- Psychological evaluation. This includes discussing your thoughts, feelings, symptoms and behavior patterns. With your permission, this may include talking to your family or friends.
- Diagnostic criteria for obsessive compulsive disorder. Your doctor may use criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association.
Diagnostic criteria for obsessions include:
- recurrent, persistent, intrusive thoughts and ideas that cause distress and anguish, and thoughts that are unreasonable and excessive and which cannot be ignored.
Diagnostic criteria for compulsions include:
- rituals and patterns of behavior that take up considerable time
- repetitive physical or mental acts, such as silent counting or hand washing behaviors, or rituals performed to ease anxiety about unrealistic obsessions.
Diagnosis can sometimes take time. Health professionals need to distinguish between other similar mental health issues such as depression, schizophrenia and anxiety disorders. Beginning the assessment process is a positive step towards recovery.
Diagnostic challenges
It’s sometimes difficult to diagnose obsessive compulsive disorder because symptoms can be similar to those of obsessive-compulsive personality disorder, anxiety disorders, depression, schizophrenia or other mental health disorders. And it’s possible to have both obsessive compulsive disorder and another mental disorder. Work with your doctor so that you can get the appropriate diagnosis and treatment.
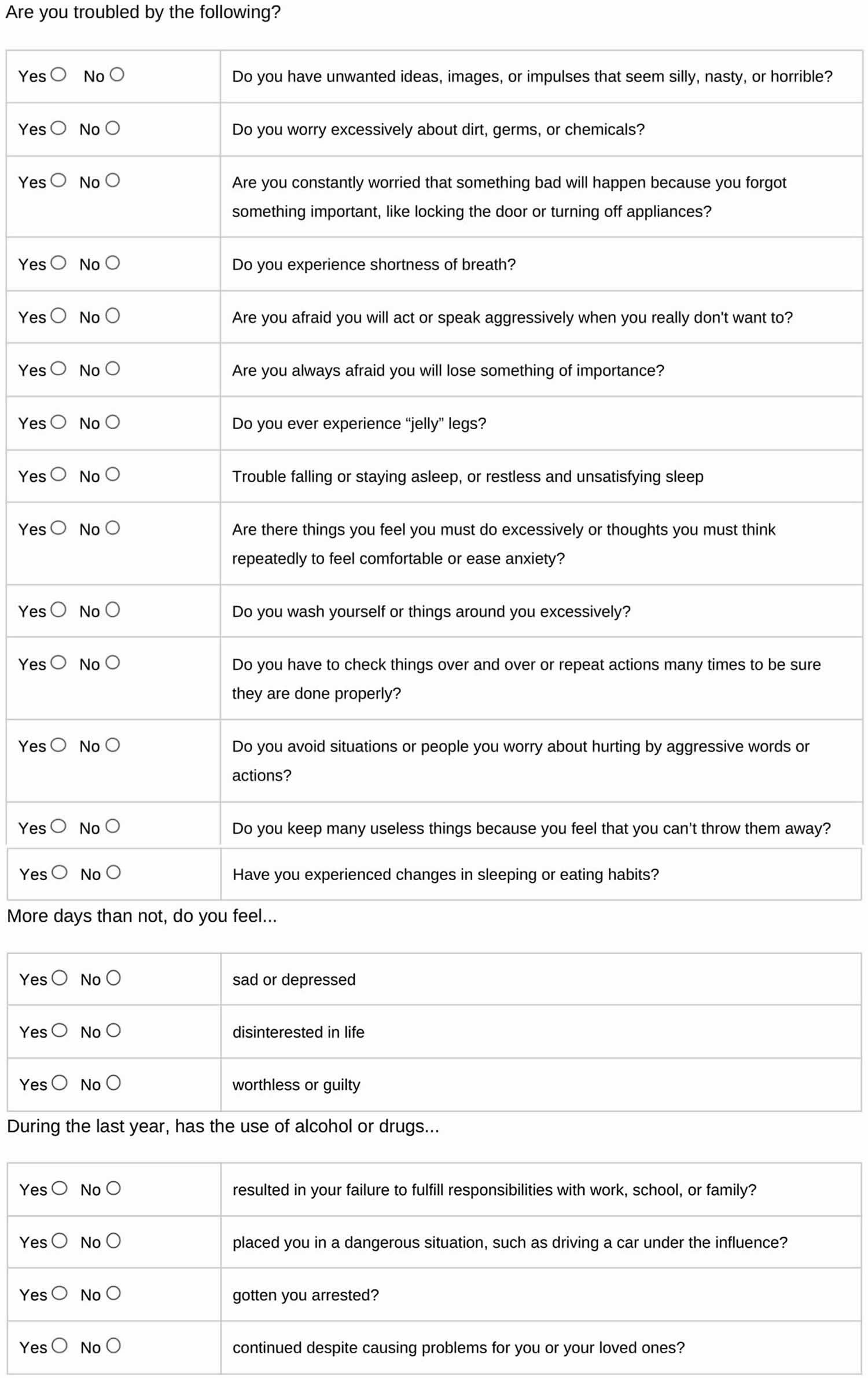
Obsessive compulsive disorder test
Use this brief screening quiz to help you determine if you might need to see a mental health professional for diagnosis and treatment of obsessive-compulsive disorder (OCD). This is a screening test to help you determine whether you might have obsessive compulsive disorder that needs professional attention. This screening tool is not designed to make a diagnosis of obsessive compulsive disorder but to be shared with your primary care physician or mental health professional to inform further conversations about diagnosis and treatment. For each item, indicate the extent to which it is true, by checking the appropriate box next to the item. Print this form in order to use it.
Obsessive compulsive disorder treatment
Obsessive-compulsive disorder (OCD) can be treated, enabling people with the disorder to live happier lives. The first step is to talk with your doctor or health care provider about your symptoms. The clinician should do an exam and ask you about your health history to make sure that a physical problem is not causing your symptoms. Your doctor may refer you to a mental health specialist, such as a psychiatrist, psychologist, social worker, or counselor for further evaluation or treatment.
Treatment can help people with obsessive compulsive disorder manage their intrusive obsessions and compulsions. It may not cure obsessive compulsive disorder, which can be a lifelong disorder, but it can help control symptoms and stop them ruling a person’s life. The best results may come from a combination of treatments.
There are some effective treatments for obsessive compulsive disorder that can help reduce the impact the condition has on your life.
The main treatments are:
- Cognitive behavior therapy (CBT): By working with a mental health professional, a person with obsessive compulsive disorder can learn new and more positive ways to cope with symptoms. The person is gently encouraged to resist their compulsive behaviors and find other ways to reduce their anxiety. Over time, this causes a reduction in the symptoms.
- Medication: Antidepressants usually a type of antidepressant medication called selective serotonin reuptake inhibitors (SSRIs) are licensed for the treatment of obsessive compulsive disorder and can be very effective. They can assist the brain in restoring a normal chemical balance.
- Community support and recovery programs: obsessive compulsive disorder can be an isolating disorder. People with obsessive compulsive disorder and their families can benefit from support groups, where people share coping strategies and develop a support network. Family therapy may also be helpful. Community support and connection can play a vital role in rebuilding lives.
Seeing a doctor, however, is the first step in the journey to wellness.
Cognitive behavioral therapy
Cognitive-behavioral therapy is the most effective treatment for obsessive-compulsive disorder and involves two components: 1) exposure and response prevention, and 2) cognitive therapy.
In general, cognitive behavioral therapy (CBT) teaches you different ways of thinking, behaving, and reacting to the obsessions and compulsions.
Exposure and Response Prevention is a specific form of cognitive behavioral therapy (CBT) which has been shown to help many patients recover from obsessive compulsive disorder. Exposure and Response Prevention involves gradually exposing you to your fears or obsessions and teaching you healthy ways to deal with the anxiety they cause. You are asked to refrain from the compulsive behavior you’d usually perform to reduce your anxiety.
- For example, if you are a compulsive hand washer, you might be asked to touch the door handle in a public restroom and then be prevented from washing up. As you sit with the anxiety, the urge to wash your hands will gradually begin to go away on its own. In this way, you learn that you don’t need the ritual to get rid of your anxiety—that you have some control over your obsessive thoughts and compulsive behaviors.
- Studies show that exposure and response prevention can actually “retrain” the brain, permanently reducing the occurrence of obsessive compulsive disorder symptoms.
Cognitive therapy focuses on the catastrophic thoughts and exaggerated sense of responsibility you feel. A big part of cognitive therapy for OCD is teaching you healthy and effective ways of responding to obsessive thoughts, without resorting to compulsive behavior.
Other therapies, such as habit reversal training, can also help you overcome compulsions.
For children, mental health professionals can also identify strategies to manage stress and increase support to avoid exacerbating obsessive compulsive disorder symptoms in school and home settings.
Obsessive compulsive disorder medications
Certain psychiatric medications can help control the obsessions and compulsions of obsessive compulsive disorder. Most commonly, antidepressants are tried first.
Antidepressants approved by the Food and Drug Administration (FDA) to treat obsessive compulsive disorder include:
- Clomipramine (Anafranil) for adults and children 10 years and older
- Fluoxetine (Prozac) for adults and children 7 years and older
- Fluvoxamine (Luvox) for adults and children 8 years and older
- Paroxetine (Paxil, Pexeva) for adults only
- Sertraline (Zoloft) for adults and children 6 years and older
- Citalopram (Celexa)
- Escitalopram (Lexapro)
- Venlafaxine (Effexor)
However, your doctor may prescribe other antidepressants and psychiatric medications.
Anafranil (clomipramine) has been around the longest and is the best studied. There is growing evidence that the other drugs are also effective. In addition to these carefully studied drugs, there are hundreds of case reports of other drugs being helpful. For example, duloxetine (Cymbalta) has been reported to help obsessive compulsive disorder patients who have not responded to these other medicines. It seems that for most people, high doses of these drugs are required to work. The studies done to date suggest that the following doses may be needed:
- Fluvoxamine (Luvox) (up to 300 mg/day)
- Fluoxetine (Prozac) (40-80 mg/day)
- Sertraline (Zoloft) (up to 200 mg/day)
- Paroxetine (Paxil, Pexeva) (40-60 mg/day)
- Citalopram (Celexa) (up to 80 mg/day)
- Clomipramine (Anafranil) (up to 250 mg/day)
- Escitalopram (Lexapro) (up to 40 mg/day)
- Venlafaxine (Effexor) (up to 375 mg/day)
It remains unclear why these particular drugs help OCD. Experts do know that each of these medicines affect a chemical in the brain called serotonin. Serotonin is used by the brain as a messenger. If your brain does not have enough serotonin, your brain isn’t working quite right. Adding these medicines to your system can help boost your serotonin and get your brain back on track.
Who should not take these medicines?
- Women who are pregnant or are breastfeeding. If severe obsessive compulsive disorder cannot be controlled any other way, these medicines seem to be safe. Many pregnant women have taken them without difficulty. Some obsessive compulsive disorder patients use exposure and response prevention to minimize medicine use during the first or last trimester of pregnancy.
- Very elderly patients should avoid Anafranil as the first drug tried since it has side effects that can interfere with thinking and can cause or worsen confusion.
- Patients with heart problems should use special caution if taking Anafranil.
What to consider
Here are some issues to discuss with your doctor about medications for obsessive compulsive disorder:
- Choosing a medication. In general, the goal is to effectively control symptoms at the lowest possible dosage. It’s not unusual to try several drugs before finding one that works well. Your doctor might recommend more than one medication to effectively manage your symptoms. It can take weeks to months after starting a medication to notice an improvement in symptoms.
- Side effects. All psychiatric medications have potential side effects. Talk to your doctor about possible side effects and about any health monitoring needed while taking psychiatric drugs. And let your doctor know if you experience troubling side effects.
- Suicide risk. Most antidepressants are generally safe, but the FDA requires that all antidepressants carry black box warnings, the strictest warnings for prescriptions. In some cases, children, teenagers and young adults under 25 may have an increase in suicidal thoughts or behavior when taking antidepressants, especially in the first few weeks after starting or when the dose is changed. If suicidal thoughts occur, immediately contact your doctor or get emergency help. Keep in mind that antidepressants are more likely to reduce suicide risk in the long run by improving mood.
- Interactions with other substances. When taking an antidepressant, tell your doctor about any other prescription or over-the-counter medications, herbs or other supplements you take. Some antidepressants can cause dangerous reactions when combined with certain medications or herbal supplements.
- Stopping antidepressants. Antidepressants aren’t considered addictive, but sometimes physical dependence (which is different from addiction) can occur. So stopping treatment abruptly or missing several doses can cause withdrawal-like symptoms, sometimes called discontinuation syndrome. Don’t stop taking your medication without talking to your doctor, even if you’re feeling better — you may have a relapse of obsessive compulsive disorder symptoms. Work with your doctor to gradually and safely decrease your dose.
Talk to your doctor about the risks and benefits of using specific medications. Don’t stop taking your medication without talking to your doctor first. Your doctor will work with you to find the best medication and dose for you.
How long does it take for these medicines to work?
It is important not to give up on a medicine until you have been taking it as prescribed for 10 to 12 weeks. Many patients feel no positive effects for the first few weeks of treatment but then improve greatly.
The main problem with solely using medicines to treat obsessive compulsive disorder is that you may not even know if the medicine is helping if you are not doing CBT. Some people have a noticeable response to medicine without cognitive behavioral therapy (CBT)/Exposure and Response Prevention, but most patients can be better and not even know it if their obsessive compulsive disorder has become a habit or a way of life. One way of looking at it is that the medicine may help correct the chemical or neurological problem in the brain, but you need behavior therapy to help correct the behaviors that have become ingrained in your lifestyle. Therefore, most obsessive compulsive disorder experts usually recommend that all obsessive compulsive disorder patients get cognitive behavioral therapy (CBT)/Exposure and Response Prevention, and most patients use a combination of cognitive behavioral therapy (CBT)/Exposure and Response Prevention and medicines. This maximizes the chances for a good response.
Other treatment
Sometimes, medications and psychotherapy aren’t effective enough to control obsessive compulsive disorder symptoms. Research continues on the potential effectiveness of deep brain stimulation (DBS) for treating obsessive compulsive disorder that doesn’t respond to traditional treatment approaches.
Because deep brain stimulation (DBS) hasn’t been thoroughly tested for use in treating obsessive compulsive disorder, make sure you understand all the pros and cons and possible health risks.
Obsessive compulsive disorder self-help
Learn how to resist obsessive compulsive disorder rituals
No matter how overwhelming your obsessive compulsive disorder symptoms seem, there are many ways you can help yourself. One of the most powerful strategies is to eliminate the compulsive behaviors and rituals that keep your obsessions going.
Don’t avoid your fears
It might seem smart to avoid the situations that trigger your obsessive thoughts, but the more you avoid them, the scarier they feel. Instead, expose yourself to your obsessive compulsive disorder triggers, then try to resist or delay the urge to complete your relief-seeking compulsive ritual. If resistance gets to be too hard, try to reduce the amount of time you spend on your ritual. Each time you expose yourself to your trigger, your anxiety should lessen and you’ll start to realize that you have more control (and less to fear) than you think.
Anticipate obsessive compulsive disorder urges
By anticipating your compulsive urges before they arise, you can help to ease them. For example, if your compulsive behavior involves checking that doors are locked, windows closed, or appliances turned off, try to lock the door or turn off the appliance with extra attention the first time.
- Create a solid mental picture and then make a mental note. Tell yourself, “The window is now closed,” or “I can see that the oven is turned off.”
- When the urge to check arises later, you will find it easier to re-label it as “just an obsessive thought.”
Refocus your attention
When you’re experiencing obsessive compulsive disorder thoughts and urges, try shifting your attention to something else. You could exercise, jog, walk, listen to music, read, surf the web, play a video game, make a phone call, or knit. The important thing is to do something you enjoy for at least 15 minutes, in order to delay your response to the obsessive thought or compulsion.
At the end of the delaying period, reassess the urge. In many cases, the urge will no longer be quite as intense. Try delaying for a longer period. The longer you can delay the urge, the more it will likely change.
Challenge obsessive thoughts
Everyone has troubling thoughts or worries from time to time. But obsessive-compulsive disorder causes the brain to get stuck on a particular anxiety-provoking thought, causing it to play over and over in your head. The following strategies can help you get unstuck.
Write down your obsessive thoughts or worries
Keep a pad and pencil on you, or type on a laptop, smartphone, or tablet. When you begin to obsess, write down all your thoughts or compulsions.
- Keep writing as the obsessive compulsive disorder urges continue, aiming to record exactly what you’re thinking, even if you’re repeating the same phrases or the same urges over and over.
- Writing it all down will help you see just how repetitive your obsessions are.
- Writing down the same phrase or urge hundreds of times will help it lose its power.
- Writing thoughts down is much harder work than simply thinking them, so your obsessive thoughts are likely to disappear sooner.
Create an obsessive compulsive disorder worry period
Rather than trying to suppress obsessions or compulsions, develop the habit of rescheduling them.
- Choose one or two 10-minute “worry periods” each day, time you can devote to obsessing. Choose a set time and place (e.g. in the living room from 8:00 to 8:10 a.m. and 5:00 to 5:10 p.m.) that’s early enough it won’t make you anxious before bedtime.
- During your worry period, focus only on negative thoughts or urges. Don’t try to correct them. At the end of the worry period, take a few calming breaths, let the obsessive thoughts or urges go, and return to your normal activities. The rest of the day, however, is to be designated free of obsessions and compulsions.
- When thoughts or urges come into your head during the day, write them down and “postpone” them to your worry period. Save it for later and continue to go about your day.
- Go over your “worry list” during the worry period. Reflect on the thoughts or urges you wrote down during the day. If the thoughts are still bothering you, allow yourself to obsess about them, but only for the amount of time you’ve allotted for your worry period.
Create a tape of your obsessive compulsive disorder obsessions
Focus on one specific worry or obsession and record it to a tape recorder, laptop, or smartphone.
- Recount the obsessive phrase, sentence, or story exactly as it comes into your mind.
- Play the tape back to yourself, over and over for a 45-minute period each day, until listening to the obsession no longer causes you to feel highly distressed.
- By continuously confronting your worry or obsession you will gradually become less anxious. You can then repeat the exercise for a different obsession.
Four Steps for Conquering Obsessive Thoughts
Psychiatrist Jeffrey Schwartz, author of Brain Lock: Free Yourself from Obsessive-Compulsive Behavior, offers the following four steps for dealing with obsessive thoughts:
- RELABEL – Recognize that the intrusive obsessive thoughts and urges are the result of OCD. For example, train yourself to say, “I don’t think or feel that my hands are dirty. I’m having an obsession that my hands are dirty.” Or, “I don’t feel that I have the need to wash my hands. I’m having a compulsive urge to perform the compulsion of washing my hands.”
- REATTRIBUTE – Realize that the intensity and intrusiveness of the thought or urge is caused by OCD; it is probably related to a biochemical imbalance in the brain. Tell yourself, “It’s not me—it’s my OCD,” to remind you that OCD thoughts and urges are not meaningful, but are false messages from the brain.
- REFOCUS – Work around the OCD thoughts by focusing your attention on something else, at least for a few minutes. Do another behavior. Say to yourself, “I’m experiencing a symptom of OCD. I need to do another behavior.”
- REVALUE – Do not take the OCD thought at face value. It is not significant in itself. Tell yourself, “That’s just my stupid obsession. It has no meaning. That’s just my brain. There’s no need to pay attention to it.” Remember: You can’t make the thought go away, but neither do you need to pay attention to it. You can learn to go on to the next behavior.
Make lifestyle changes to ease obsessive compulsive disorder
A healthy, balanced lifestyle plays a big role in easing anxiety and keeping obsessive compulsive disorder compulsions, fears, and worry at bay.
Exercise regularly
Exercise is a natural and effective anti-anxiety treatment that helps to control obsessive compulsive disorder symptoms by refocusing your mind when obsessive thoughts and compulsions arise. For maximum benefit, try to get 30 minutes or more of aerobic activity on most days. Ten minutes several times a day can be as effective as one longer period especially if you pay mindful attention to the movement process.
Get enough sleep
Not only can anxiety and worry cause insomnia, but a lack of sleep can also exacerbate anxious thoughts and feelings. When you’re well rested, it’s much easier to keep your emotional balance, a key factor in coping with anxiety disorders such as obsessive compulsive disorder.
Avoid alcohol and nicotine
Alcohol temporarily reduces anxiety and worry, but it actually causes anxiety symptoms as it wears off. Similarly, while it may seem that cigarettes are calming, nicotine is actually a powerful stimulant. Smoking leads to higher, not lower, levels of anxiety and obsessive compulsive disorder symptoms.
Practice relaxation techniques
While stress doesn’t cause obsessive compulsive disorder, it can trigger symptoms or make them worse. Mindful meditation, yoga, deep breathing, and other relaxation techniques can help lower your overall stress and tension levels and help you manage your urges. For best results, practice a relaxation technique regularly.
Reach out for support
Obsessive compulsive disorder can get worse when you feel powerless and alone, so it’s important to build a strong support system. The more connected you are to other people, the less vulnerable you’ll feel. Just talking about your worries and urges can make them seem less threatening.
Stay connected to family and friends
Obsessions and compulsions can consume your life to the point of social isolation. In turn, social isolation will aggravate your obsessive compulsive disorder symptoms. It’s important to invest in relating to family and friends. Talking face-to-face about your worries and urges can make them feel less real and less threatening.
Join an obsessive compulsive disorder support group
You’re not alone in your struggle with obsessive compulsive disorder, and participating in a support group can be an effective reminder of that. obsessive compulsive disorder support groups enable you to both share your own experiences and learn from others who are facing the same problems.
- International OCD Foundation (https://iocdf.org/)
Helping someone with obsessive compulsive disorder
The way you react to your loved one’s obsessive compulsive disorder symptoms can have a big impact on their outlook and recovery. Negative comments or criticism can make obsessive compulsive disorder worse, while a calm, supportive environment can help improve the outcome of treatment.
- Avoid making personal criticisms. Remember, your loved one’s obsessive compulsive disorder behaviors are symptoms, not character flaws.
- Don’t scold someone with obsessive compulsive disorder or tell them to stop performing rituals. They can’t comply, and the pressure to stop will only make the behaviors worse.
- Be as kind and patient as possible. Each sufferer needs to overcome problems at their own pace. Praise any successful attempt to resist obsessive compulsive disorder, and focus attention on positive elements in the person’s life.
- Do not play along with your loved one’s rituals. Helping with rituals will only reinforce the behavior. Support the person, not their rituals.
- Keep communication positive and clear. Communication is important so you can find a balance between supporting your loved one and standing up to the obsessive compulsive disorder symptoms and not further distressing your loved one.
- Find the humor. Laughing together over the funny side and absurdity of some obsessive compulsive disorder symptoms can help your loved one become more detached from the disorder. Just make sure your loved one feels respected and in on the joke.
- Don’t let obsessive compulsive disorder take over family life. Sit down as a family and decide how you will work together to tackle your loved one’s symptoms. Try to keep family life as normal as possible and the home a low-stress environment.
Learn to recognize and reduce “Family Accommodation Behaviors”
Family Accommodation Behaviors are things families do that enable obsessive compulsive disorder symptoms. Families are constantly affected by the demands of obsessive compulsive disorder. Research shows that how a family responds to the obsessive compulsive disorder may help fuel obsessive compulsive disorder symptoms. The more that family members can learn about their responses to obsessive compulsive disorder and the impact they have on the person with obsessive compulsive disorder, the more the family becomes empowered to make a difference!
Here are some examples of these problematic behaviors:
- Participating in the behavior: You participate in your family member’s obsessive compulsive disorder behavior along with them. Example: washing your hands whenever they wash their hands.
- Assisting in avoiding: You help your family member avoid things that upset them. Example: doing their laundry for them so that it is cleaned the “right” way.
- Helping with the behavior: You do things for your family member that lets them do obsessive compulsive disorder behaviors. For example, buying large amounts of cleaning products for them.
- Making changes in family routine: you change the time of day that you shower, or when you change your clothes.
- Taking on extra responsibilities: going out of your way to drive them places when they could otherwise drive themselves.
- Making changes in leisure activities: your family member gets you to not leave the house without them. This affects your interests in movies, dinners out, time with friends, etc.
- Making changes at your job: you cut back on hours at your job in order to take care of your family member.
- Ruscio AM, Stein DJ, Chiu WT, Kessler RC. “The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication.” Molecular Psychiatry. 2008 Aug 26.[↩]
- International OCD Foundation.What You Need to Know about Obsessive Compulsive Disorder. https://iocdf.org/wp-content/uploads/2014/10/What-You-Need-To-Know-About-OCD.pdf[↩]
- March, J. & Benton, C. (2007). Talking Back to OCD. (pp.10-11). The Guilford Press.[↩]
- The Pediatric OCD Treatment Study (POTS) Team. “Cognitive-Behavior Therapy, Sertraline, and Their Combination for Children and Adolescents with Obsessive-Compulsive Disorder: The Pediatric OCD Treament Study (POTS) Randomized Controlled Trial.” JAMA 2004;292(16):1969-1976[↩]





{kind=link}