
Contents
What is odynophagia
Odynophagia means having pain while swallowing. Odynophagia is any pain or discomfort while swallowing. You may feel pain when swallowing high in your throat or lower down behind the breastbone in your chest. Most often, pain when swallowing feels like a strong sensation of squeezing or burning. Painful swallowing may be a symptom of a serious disorder.
Swallowing involves many nerves and muscles in the mouth, throat area, and food pipe (esophagus). Part of swallowing is voluntary. This means you are aware of controlling the action. However, much of swallowing is involuntary.
Problems at any point in the swallowing process (including chewing, moving food to the back of the mouth, or moving it to the stomach) as food and liquid move from the mouth, down the back of the throat, through the esophagus and into the stomach can result in painful swallowing.
Swallowing problems can cause symptoms such as:
- Chest pain
- Feeling of food stuck in the throat
- Heaviness or pressure in the neck or upper chest while eating
Figure 1. Esophagus
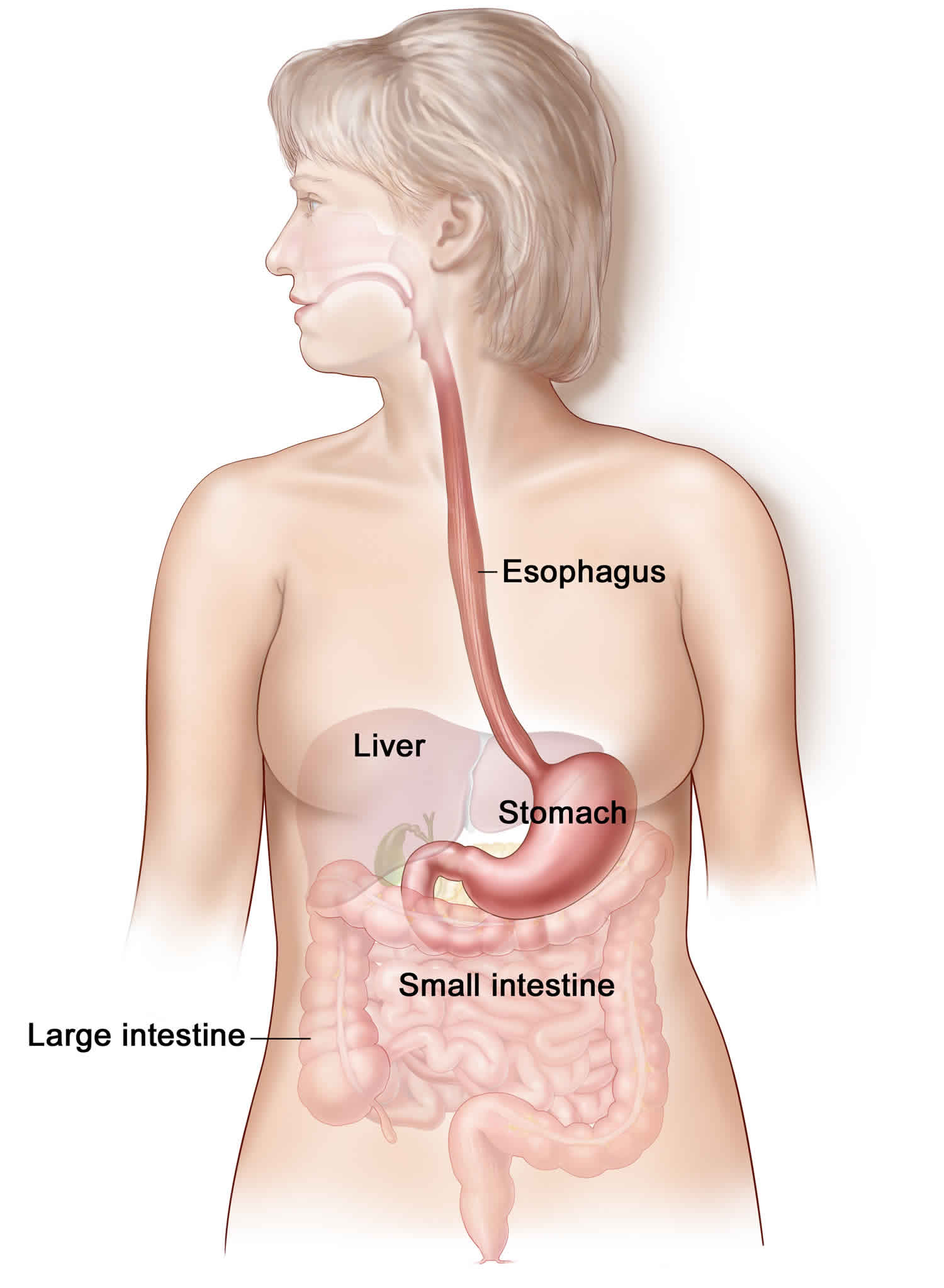 Figure 2. Pharynx and larynx anatomy
Figure 2. Pharynx and larynx anatomy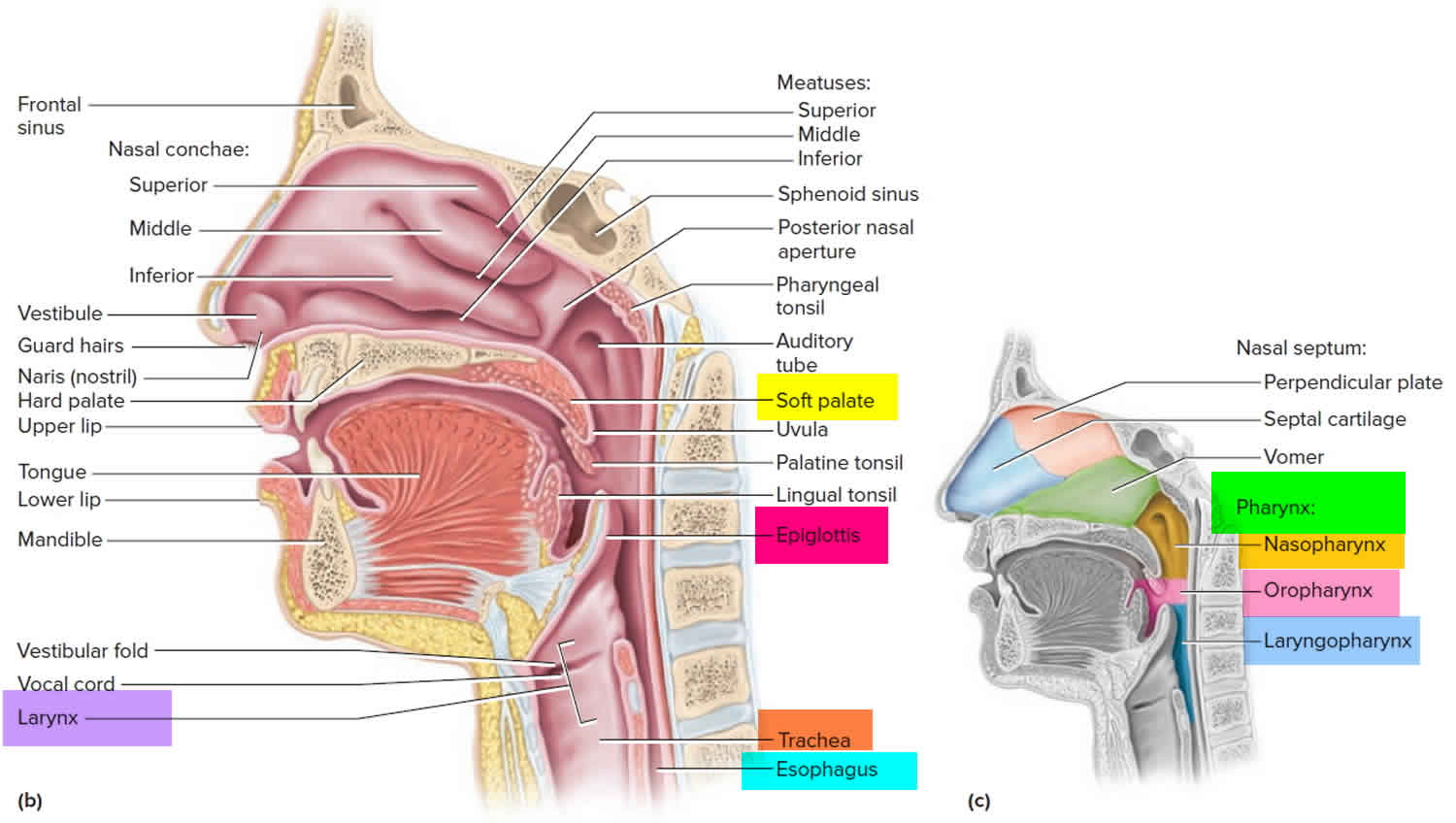
See your doctor if you have painful swallowing and:
- Blood in your stools or your stools appear black or tarry
- Shortness of breath or lightheadedness
- Weight loss
See your doctor if you regularly have difficulty swallowing or if weight loss, regurgitation or vomiting accompanies your pain when swallowing.
If an obstruction interferes with breathing, call for emergency help immediately. If you’re unable to swallow because you feel that the food is stuck in your throat or chest, go to the nearest emergency department.
Tell your doctor about any other symptoms that occur with pain when swallowing, including:
- Abdominal pain
- Chills
- Cough
- Fever
- Heartburn
- Nausea or vomiting
- Sour taste in the mouth
- Wheezing
Odynophagia vs Dysphagia
Dysphagia is difficulty swallowing, which means it takes more time and effort to move food or liquid from your mouth to your stomach. Dysphagia may also be associated with pain. In some cases, swallowing may be impossible.
Occasional difficulty swallowing, which may occur when you eat too fast or don’t chew your food well enough, usually isn’t cause for concern. But persistent dysphagia (difficulty swallowing) may indicate a serious medical condition requiring treatment.
Dysphagia can occur at any age, but it’s more common in older adults. The causes of swallowing problems vary, and treatment depends on the cause.
Dysphagia causes
Swallowing is complex, and a number of conditions can interfere with this process. Sometimes the cause of dysphagia can’t be identified. However, dysphagia generally falls into one of the following categories.
Esophageal dysphagia
Esophageal dysphagia refers to the sensation of food sticking or getting hung up in the base of your throat or in your chest after you’ve started to swallow. Some of the causes of esophageal dysphagia include:
- Achalasia. When your lower esophageal muscle (sphincter) doesn’t relax properly to let food enter your stomach, it may cause you to bring food back up into your throat. Muscles in the wall of your esophagus may be weak as well, a condition that tends to worsen over time.
- Diffuse spasm. This condition produces multiple high-pressure, poorly coordinated contractions of your esophagus, usually after you swallow. Diffuse spasm affects the involuntary muscles in the walls of your lower esophagus.
- Esophageal stricture. A narrowed esophagus (stricture) can trap large pieces of food. Tumors or scar tissue, often caused by gastroesophageal reflux disease (GERD), can cause narrowing.
- Esophageal tumors. Difficulty swallowing tends to get progressively worse when esophageal tumors are present.
- Foreign bodies. Sometimes food or another object can partially block your throat or esophagus. Older adults with dentures and people who have difficulty chewing their food may be more likely to have a piece of food become lodged in the throat or esophagus.
- Esophageal ring. A thin area of narrowing in the lower esophagus can intermittently cause difficulty swallowing solid foods.
- Gastroesophageal reflux disease (GERD). Damage to esophageal tissues from stomach acid backing up into your esophagus can lead to spasm or scarring and narrowing of your lower esophagus.
- Eosinophilic esophagitis. This condition, which may be related to a food allergy, is caused by an overpopulation of cells called eosinophils in the esophagus.
- Scleroderma. Development of scar-like tissue, causing stiffening and hardening of tissues, can weaken your lower esophageal sphincter, allowing acid to back up into your esophagus and cause frequent heartburn.
- Radiation therapy. This cancer treatment can lead to inflammation and scarring of the esophagus.
Oropharyngeal dysphagia
Certain conditions can weaken your throat muscles, making it difficult to move food from your mouth into your throat and esophagus when you start to swallow. You may choke, gag or cough when you try to swallow or have the sensation of food or fluids going down your windpipe (trachea) or up your nose. This may lead to pneumonia.
Causes of oropharyngeal dysphagia include:
- Neurological disorders. Certain disorders — such as multiple sclerosis, muscular dystrophy and Parkinson’s disease — can cause dysphagia.
- Neurological damage. Sudden neurological damage, such as from a stroke or brain or spinal cord injury, can affect your ability to swallow.
- Pharyngoesophageal diverticulum (Zenker’s diverticulum). A small pouch that forms and collects food particles in your throat, often just above your esophagus, leads to difficulty swallowing, gurgling sounds, bad breath, and repeated throat clearing or coughing.
- Cancer. Certain cancers and some cancer treatments, such as radiation, can cause difficulty swallowing.
Risk factors for dysphagia
The following are risk factors for dysphagia:
- Aging. Due to natural aging and normal wear and tear on the esophagus and a greater risk of certain conditions, such as stroke or Parkinson’s disease, older adults are at higher risk of swallowing difficulties. But, dysphagia isn’t considered a normal sign of aging.
- Certain health conditions. People with certain neurological or nervous system disorders are more likely to experience difficulty swallowing.
Dysphagia prevention
Although swallowing difficulties can’t be prevented, you can reduce your risk of occasional difficulty swallowing by eating slowly and chewing your food well. Early detection and effective treatment of GERD can lower your risk of developing dysphagia associated with an esophageal stricture.
Dysphagia symptoms
Signs and symptoms associated with dysphagia may include:
- Having pain while swallowing (odynophagia)
- Being unable to swallow
- Having the sensation of food getting stuck in your throat or chest or behind your breastbone (sternum)
- Drooling
- Being hoarse
- Bringing food back up (regurgitation)
- Having frequent heartburn
- Having food or stomach acid back up into your throat
- Unexpectedly losing weight
- Coughing or gagging when swallowing
- Having to cut food into smaller pieces or avoiding certain foods because of trouble swallowing
Dysphagia complications
Difficulty swallowing can lead to:
- Malnutrition, weight loss and dehydration. Dysphagia can make it difficult to take in adequate nourishment and fluids.
- Aspiration pneumonia. Food or liquid entering your airway when you try to swallow can cause aspiration pneumonia, because the food can introduce bacteria to the lungs.
- Choking. When food becomes impacted, choking can occur. If food completely blocks the airway, and no one intervenes with a successful Heimlich maneuver, death can occur.
Dysphagia treatment
Treatment for dysphagia depends on the type or cause of your swallowing disorder.
Oropharyngeal dysphagia
For oropharyngeal dysphagia, your doctor may refer you to a speech or swallowing therapist, and therapy may include:
- Learning exercises. Certain exercises may help coordinate your swallowing muscles or restimulate the nerves that trigger the swallowing reflex.
- Learning swallowing techniques. You may also learn ways to place food in your mouth or to position your body and head to help you swallow. You may be taught exercises and new swallowing techniques to help compensate for dysphagia caused by neurological problems such as Alzheimer’s disease or Parkinson’s disease.
Esophageal dysphagia
Treatment approaches for esophageal dysphagia may include:
- Esophageal dilation. For a tight esophageal sphincter (achalasia) or an esophageal stricture, your doctor may use an endoscope with a special balloon attached to gently stretch and expand the width of your esophagus or pass a flexible tube or tubes to stretch the esophagus (dilation).
- Surgery. For an esophageal tumor, achalasia or pharyngoesophageal diverticulum, you may need surgery to clear your esophageal path.
- Medications. Difficulty swallowing associated with GERD can be treated with prescription oral medications to reduce stomach acid. You may need to take these medications for an extended period. If you have eosinophilic esophagitis, you may need corticosteroids. If you have esophageal spasm, smooth muscle relaxants may help.
Severe dysphagia
If difficulty swallowing prevents you from eating and drinking adequately, your doctor may recommend:
- A special liquid diet. This may help you maintain a healthy weight and avoid dehydration.
- A feeding tube. In severe cases of dysphagia, you may need a feeding tube to bypass the part of your swallowing mechanism that isn’t working normally.
Surgery
Surgery may be recommended to relieve swallowing problems caused by throat narrowing or blockages, including bony outgrowths, vocal cord paralysis, pharyngoesophageal diverticulum, GERD and achalasia, or to treat esophageal cancer. Speech and swallowing therapy is usually helpful after surgery.
The type of surgical treatment depends on the cause for dysphagia. Some examples are:
- Laparoscopic Heller myotomy, which is used to cut the muscle at the lower end of the esophagus (sphincter) when it fails to open and release food into the stomach in people who have achalasia.
- Esophageal dilation. Your doctor inserts a lighted tube (endoscope) into your esophagus and inflates an attached balloon to gently stretch and expand its width (dilation). This treatment is used for a tight sphincter muscle at the end of the esophagus (achalasia), a narrowing of the esophagus (esophageal stricture), an abnormal ring of tissue located at the junction of the esophagus and stomach (Schatzki’s ring) or a motility disorder. Alternatively, your doctor may pass a flexible tube or tubes of different diameters instead of a balloon.
- Stent placement. The doctor can also insert a metal or plastic tube (stent) to prop open a narrowing or blockage in your esophagus. Some stents are permanent, such as those for people with esophageal cancer, while others are temporary and are removed later.
Odynophagia causes
Swallowing is complex, and a number of conditions can interfere with this process. Sometimes the cause of pain when swallowing can’t be identified. However, odynophagia generally falls into one of the following categories.
Odynophagia may be due to infections, such as:
- Cytomegalovirus
- Gum disease (gingivitis)
- Herpes simplex virus
- Human immunodeficiency virus (HIV)
- Pharyngitis (sore throat)
- Thrush
Odynophagia may be due to a problem with the esophagus, such as:
- Achalasia. When your lower esophageal muscle (sphincter) doesn’t relax properly to let food enter your stomach, it may cause you to bring food back up into your throat. Muscles in the wall of your esophagus may be weak as well, a condition that tends to worsen over time.
- Esophageal spasms. This condition produces multiple high-pressure, poorly coordinated contractions of your esophagus, usually after you swallow. Diffuse spasm affects the involuntary muscles in the walls of your lower esophagus.
- Gastroesophageal reflux disease (GERD). Damage to esophageal tissues from stomach acid backing up into your esophagus can lead to spasm or scarring and narrowing of your lower esophagus.
- Inflammation of the esophagus (esophagitis).
- Nutcracker esophagus
- Esophageal stricture. A narrowed esophagus (stricture) can trap large pieces of food. Tumors or scar tissue, often caused by gastroesophageal reflux disease (GERD), can cause narrowing.
- Esophageal tumors. Difficulty swallowing tends to get progressively worse when esophageal tumors are present.
- Foreign bodies. Sometimes food or another object can partially block your throat or esophagus. Older adults with dentures and people who have difficulty chewing their food may be more likely to have a piece of food become lodged in the throat or esophagus.
- Esophageal ring. A thin area of narrowing in the lower esophagus can intermittently cause difficulty swallowing solid foods.
- Ulcer in the esophagus, especially due to the antibiotic doxycycline, aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, naproxyn.
- Eosinophilic esophagitis. This condition, which may be related to a food allergy, is caused by an overpopulation of cells called eosinophils in the esophagus.
- Scleroderma. Development of scar-like tissue, causing stiffening and hardening of tissues, can weaken your lower esophageal sphincter, allowing acid to back up into your esophagus and cause frequent heartburn.
- Radiation therapy. This cancer treatment can lead to inflammation and scarring of the esophagus.
Certain conditions can weaken your throat muscles, making it difficult to move food from your mouth into your throat and esophagus when you start to swallow. You may choke, gag or cough when you try to swallow or have the sensation of food or fluids going down your windpipe (trachea) or up your nose. This may lead to pneumonia.
Causes of oropharyngeal dysphagia include:
- Neurological disorders. Certain disorders — such as multiple sclerosis, muscular dystrophy and Parkinson’s disease — can cause dysphagia.
- Neurological damage. Sudden neurological damage, such as from a stroke or brain or spinal cord injury, can affect your ability to swallow.
- Pharyngoesophageal diverticulum (Zenker’s diverticulum). A small pouch that forms and collects food particles in your throat, often just above your esophagus, leads to difficulty swallowing, gurgling sounds, bad breath, and repeated throat clearing or coughing.
- Cancer. Certain cancers and some cancer treatments, such as radiation, can cause difficulty swallowing.
Other causes of odynophagia include:
- Mouth or throat ulcers
- Esophageal cancer (advanced stage)
- Something stuck in the throat (for example, fish or chicken bones)
- Tooth infection or abscess
Risk factors for odynophagia
The following are risk factors for odynophagia:
- Aging. Due to natural aging and normal wear and tear on the esophagus and a greater risk of certain conditions, such as stroke or Parkinson’s disease, older adults are at higher risk of swallowing difficulties. But, dysphagia isn’t considered a normal sign of aging.
- Certain health conditions. People with certain neurological or nervous system disorders are more likely to experience difficulty swallowing.
- Neurological conditions that can cause swallowing difficulties are: stroke (the most common cause of dysphagia); traumatic brain injury; cerebral palsy; Parkinson disease and other degenerative neurological disorders such as amyotrophic lateral sclerosis (ALS, also known as Lou Gehrig’s disease), multiple sclerosis, progressive supranuclear palsy, Huntington disease, and myasthenia gravis.
- Muscular dystrophy and myotonic dystrophy are accompanied by pain when swallowing, which is also the cardinal symptom of oculopharyngeal muscular dystrophy, a rare, progressive genetic disorder.
Odynophagia diagnosis
Your doctor will examine you and ask about your medical history and symptoms, including:
- Do you have pain when swallowing solids, liquids, or both?
- Is the pain constant or does it come and go?
- Is the pain getting worse?
- Do you have difficulty swallowing?
- Do you have a sore throat?
- Does it feel like there is a lump in your throat?
- Have you inhaled or swallowed any irritating substances?
- What other symptoms do you have?
- What other health problems do you have?
- What medicines do you take?
The following tests may be done:
- A visual examination of your esophagus with biopsy (endoscopy). A thin, flexible lighted instrument (endoscope) is passed down your throat so that your doctor can see your esophagus. Your doctor may also take biopsies of the esophagus to look for inflammation, eosinophilic esophagitis, narrowing or a tumor.
- Fiber-optic endoscopic swallowing evaluation. Your doctor may examine your throat with a special camera and lighted tube (endoscope) as you try to swallow.
- Dynamic swallowing study. You swallow barium-coated foods of different consistencies. This test provides an image of these foods as they travel through your mouth and down your throat. The images may show problems in the coordination of your mouth and throat muscles when you swallow and determine whether food is going into your breathing tube.
- Barium swallow and upper GI series. You drink a barium solution that coats your esophagus, allowing it to show up better on X-rays. Your doctor can then see changes in the shape of your esophagus and can assess the muscular activity. Your doctor may also have you swallow solid food or a pill coated with barium to watch the muscles in your throat as you swallow or to look for blockages in your esophagus that the liquid barium solution may not identify.
- Chest x-ray
- Esophageal pH monitoring (measures acid in the esophagus)
- Esophageal manometry (measures pressure in the esophagus). In manometry, a small tube is inserted into your esophagus and connected to a pressure recorder to measure the muscle contractions of your esophagus as you swallow.
- Esophagogastroduodenoscopy (EGD)
- HIV testing
- Imaging scans. These may include a CT scan, which combines a series of X-ray views and computer processing to create cross-sectional images of your body’s bones and soft tissues; an MRI scan, which uses a magnetic field and radio waves to create detailed images of organs and tissues.
- Throat culture
Odynophagia treatment
Treatment for odynophagia depends on the type or cause of your swallowing disorder.
Home remedies
If you have trouble swallowing, be sure to see a doctor and follow his or her advice.
Some tips that may help you to ease swallowing pain at home include:
- Eat slowly and chew your food well.
- Eat pureed foods or liquids if solid foods are hard to swallow.
- Avoid very cold or very hot foods if they make your symptoms worse.
- Avoiding alcohol, tobacco and caffeine. These can make heartburn worse.
- Trying foods with different textures to see if some cause you more trouble. Thin liquids, such as coffee and juice, are a problem for some people, and sticky foods, such as peanut butter or caramel, can make swallowing difficult. Avoid foods that cause you trouble.
- Changing your eating habits. Try eating smaller, more-frequent meals. Be sure to cut your food into smaller pieces, chew food thoroughly and eat more slowly.
Oropharyngeal dysphagia
For oropharyngeal dysphagia, your doctor may refer you to a speech or swallowing therapist, and therapy may include:
- Learning exercises. Certain exercises may help coordinate your swallowing muscles or restimulate the nerves that trigger the swallowing reflex.
- Learning swallowing techniques. You may also learn ways to place food in your mouth or to position your body and head to help you swallow. You may be taught exercises and new swallowing techniques to help compensate for dysphagia caused by neurological problems such as Alzheimer’s disease or Parkinson’s disease.
Esophageal dysphagia
Treatment approaches for esophageal dysphagia may include:
- Esophageal dilation. For a tight esophageal sphincter (achalasia) or an esophageal stricture, your doctor may use an endoscope with a special balloon attached to gently stretch and expand the width of your esophagus or pass a flexible tube or tubes to stretch the esophagus (dilation).
- Surgery. For an esophageal tumor, achalasia or pharyngoesophageal diverticulum, you may need surgery to clear your esophageal path.
- Medications. Difficulty swallowing associated with GERD can be treated with prescription oral medications to reduce stomach acid. You may need to take these medications for an extended period. If you have eosinophilic esophagitis, you may need corticosteroids. If you have esophageal spasm, smooth muscle relaxants may help.
Severe dysphagia
If difficulty swallowing prevents you from eating and drinking adequately, your doctor may recommend:
- A special liquid diet. This may help you maintain a healthy weight and avoid dehydration.
- A feeding tube. In severe cases of dysphagia, you may need a feeding tube to bypass the part of your swallowing mechanism that isn’t working normally.
Surgery
Surgery may be recommended to relieve swallowing problems caused by throat narrowing or blockages, including bony outgrowths, vocal cord paralysis, pharyngoesophageal diverticulum, GERD and achalasia, or to treat esophageal cancer. Speech and swallowing therapy is usually helpful after surgery.
The type of surgical treatment depends on the cause for dysphagia. Some examples are:
- Laparoscopic Heller myotomy, which is used to cut the muscle at the lower end of the esophagus (sphincter) when it fails to open and release food into the stomach in people who have achalasia.
- Esophageal dilation. Your doctor inserts a lighted tube (endoscope) into your esophagus and inflates an attached balloon to gently stretch and expand its width (dilation). This treatment is used for a tight sphincter muscle at the end of the esophagus (achalasia), a narrowing of the esophagus (esophageal stricture), an abnormal ring of tissue located at the junction of the esophagus and stomach (Schatzki’s ring) or a motility disorder. Alternatively, your doctor may pass a flexible tube or tubes of different diameters instead of a balloon.
- Stent placement. The doctor can also insert a metal or plastic tube (stent) to prop open a narrowing or blockage in your esophagus. Some stents are permanent, such as those for people with esophageal cancer, while others are temporary and are removed later.





{kind=link}