Contents
What is oxytocin
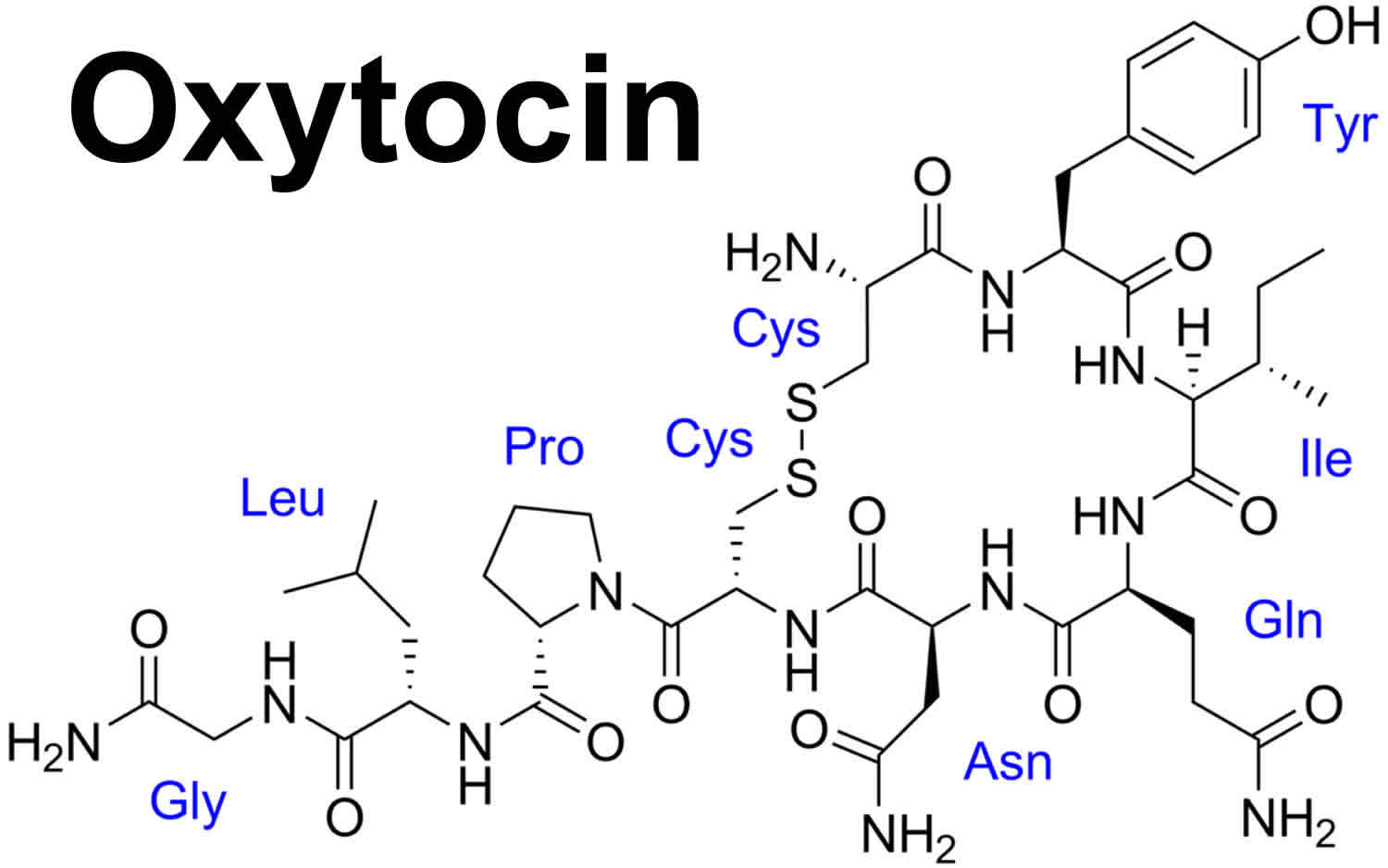
Oxytocin is a nonapeptide hormone released in high levels during childbirth from the posterior pituitary gland at the base of your brain 1. Oxytocin is in a class of medications called oxytocic hormones. Oxytocin acts on smooth muscle cells, such as stimulating uterine contractions during labor and milk ejection during breastfeeding. The oxytocin hormone is also released during sex, and is thought to be involved in helping people to form bonds. Oxytocin’s role in these areas has led to it being called various things in the mass media, such as the “oxytocin bonding hormone” or “oxytocin love hormone”. However, there is also evidence that oxytocin is associated with less “cuddly” emotions such as envy and hostility to strangers.
The hormone also has effects on appetite, and fear and reward pathways in the brain, so the researchers wanted to test whether the hormone might have a beneficial effect on anorexia.
Drugs based on oxytocin hormone are already used medically to help induce labor or strengthen labor contractions during childbirth, and to control bleeding after childbirth. Oxytocin is also used to stimulate uterine contractions in a woman with an incomplete or threatened miscarriage. Recombinant oxytocin is a synthetic cyclic peptide form of the naturally occurring posterior pituitary hormone oxytocin. Oxytocin injection is used to begin or improve contractions during labor. Oxytocin also is used to reduce bleeding after childbirth. Oxytocin also may be used along with other medications or procedures to end a pregnancy.
In recent years, the neuropeptide oxytocin, known to play a key role in bonding and social behavior, has been heralded as an important player in the etiology, symptom severity, and possible treatment of schizophrenia 2. Interest in this area of research stems from numerous studies suggesting pro-social effects of intranasal oxytocin in both non-clinical and clinical human populations. However, initial enthusiasm about oxytocin has now given way to doubt and controversy. Mounting evidence suggests that the oxytocin system is highly complex and has multifaceted influences on behavior.
Oxytocin hormone has been tested as a possible treatment in some mental health conditions, such as generalized anxiety disorder, postnatal depression and autistic spectrum disorder.
Research involving administration of oxytocin has increased dramatically over the last decade, and studies in rhesus macaques demonstrating that intranasal oxytocin can elevate oxytocin concentrations in the cerebrospinal fluid (CSF) 3 have supported the widespread adoption of intranasal administration in human populations. Administration of a single dose of oxytocin to healthy individuals has been shown to improve retention of social information 4, reduce anxiety associated with social threat 5, facilitate interpretation of faces expressing complex mental states and social emotions 6, and promote trust during interpersonal economic transactions with human (versus computer) partners 7. Neuroimaging studies have implicated oxytocin in a variety of social brain processes and shown that the amygdala, medial prefrontal cortex, anterior cingulate cortex, insula, and temporal regions are modulated by exogenous oxytocin 8. Oxytocin has also been linked with non-social cognitive processes, such as spatial and episodic memory and cognitive flexibility (Chini et al., 2014). These promising findings have generated enthusiasm for oxytocin’s potential as a therapeutic in multiple psychiatric disorders.
A dramatic rise in the number of oxytocin studies in clinical populations over the past decade reflects this enthusiasm 9. In addition to targeting deficits in schizophrenia, oxytocin has been investigated as a treatment for deficits in autism 10, alexithymia 11, Prader-Willi Syndrome 12 and social anxiety 13. Results of these clinical studies have been notably inconsistent, however. A growing body of evidence now suggests that oxytocin’s effects are more complex than previously thought: rather than being simply “pro-social,” it appears to modulate social interaction in a context-specific manner 14 that is impacted by individual differences 15. In addition, there is debate about intranasal oxytocin’s ability to consistently reach neural targets, lack of clarity about its pharmacodynamics 16, and incomplete understanding of oxytocin receptor distribution in the human brain 17. Perhaps not surprisingly, there have been recent failures to replicate some of the early oxytocin findings in healthy humans 18.
Figure 1. The pituitary gland location

Figure 2. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs

Where is oxytocin produced
Oxytocin is produced and stored in the posterior pituitary gland, where the peptide is thought to remain in vesicles until released as the nine amino acid form. However, the molecule also may be released from axons within the brain and spinal cord (central nervous system) 19, as well as from the neuronal soma and dendrites or by diffusion within the brain 20. In addition, oxytocin is made throughout the body with local effects on diverse tissues, including the uterus, testes, digestive system, kidney, and thymus 21.
There are very few sex differences in the sites of oxytocin synthesis. Oxytocin and arginine vasopressin are primarily synthesized in brain regions that are critical to behavioral and physiological homeostasis. Different cells in specific brain regions produce these two peptides, vasopressin and oxytocin, including the supraoptic nucleus (SON) and paraventricular nucleus (PVN) of the hypothalamus 19. Anatomical studies in rodents indicate that oxytocin and vasopressin are synthesized in discrete areas and in separate cells within the paraventricular nucleus (PVN) and supraoptic nucleus (SON); these cells also produce a network of neural projections reaching throughout the brain and spinal cord 20.
Research using brain slices 22 indicates that in other brain regions, including the amygdala and the bed nucleus of the stria terminalis, both oxytocin and vasopressin containing cells and projections lie adjacent to each other. These oxytocin–vasopressin associations form local functional units, capable of rapid and often opposite interactions—for example, in brain regions associated with fear versus fear reduction. Fear responses are mediated by V1aRs in the amygdala, while oxytocin may act to inhibit fear, depending on context (Figure 2) and gender 23.
Oxytocin hormone function
Oxytocin binds to oxytocin receptors in the uterine myometrium (muscles of the uterus), which triggers the G-protein coupled receptor signal transduction cascade that causes increased intracellular calcium concentrations. Increased calcium concentration levels activate myosin light chain kinase which, in turn, induces the formation of the contractile protein actomyosin. This stimulates uterine smooth muscle contractions. Oxytocin also stimulates smooth muscles which surround the alveoli of the mammary glands (lactiferous glands in breast), thereby causing lactation.
Suckling stimulates the production of oxytocin, which causes the myoepithelial cells to contract. This contraction causes milk to move from the alveoli to large sinuses for ejection (i.e., the milk letdown reflex of nursing mothers). Oxytocin stimulates contraction of uterine smooth muscle cells, and uterine sensitivity to oxytocin increases throughout pregnancy. However, plasma levels do not increase sharply during childbirth, and the role of oxytocin in the initiation of labor is unclear.
In males, oxytocin may play a role in the sexual response, including erection of the penis and movement of sperm. In addition, oxytocin is an antidiuretic, but it is much weaker than antidiuretic hormone (ADH). Men have extremely low levels of oxytocin.
Antepartum
Oxytocin injection (synthetic) is indicated for the initiation or improvement of uterine contractions, where this is desirable and considered suitable, in order to achieve early vaginal delivery for fetal or maternal reasons. It is indicated for (1) induction of labor in patients with a medical indication for the initiation of labor, such as Rhesus problems, maternal diabetes, pre-eclampsia at or near term, when delivery is in the best interest of mother and fetus or when membranes are prematurely ruptured and delivery is indicated; (2) stimulation or reinforcement of labor, as in selected cases of uterine inertia; (3) adjunctive therapy in the management of incomplete or inevitable abortion. In the first trimester, curettage is generally considered primary therapy. In second trimester abortion, oxytocin infusion will often be successful in emptying the uterus. Other means of therapy, however, may be required in such cases.
Postpartum
Oxytocin injection (synthetic) is indicated to produce uterine contractions during the third stage of labor and to control postpartum bleeding or hemorrhage.
Oxytocin and lactation
In the rat, stimulation of vagal sensory afferents in the nipple by the act of suckling triggers reflex synchronized firing of oxytotic magnocellular neurons in the neurohypophysis, and corresponding pulsatile oxytocin release 24. oxytocin acts on oxytocin-receptors on smooth muscle cells lining the milk ducts of the breast, initiating milk ejection. Oxytocin is essential for completion of this milk ejection reflex in rodent. Mice lacking oxytocin fail to transfer milk to their suckling young. This deficit is corrected by injection of oxytocin. In contrast, women lacking posterior pituitary function can breast-feed normally, illustrating that oxytocin is not necessary for lactation in man. Pituitary lactotrophs express oxytocin-receptor mRNA, and oxytocin released into the hypophyseal portal blood supply from the median eminence can stimulate prolactin release. However, the role of oxytocin in the physiology of prolactin release remains unclear 24.
Oxytocin and parturition
Oxytocin is a uterotonic agent. In many mammals, there is both an increase in oxytocin secretion and an increase in uterine responsiveness to oxytocin during childbirth 25. These data suggest a key role for oxytocin hormone in the initiation and progression of labor. Falling progesterone concentrations toward the end of pregnancy lead to up-regulation of uterine myometrial oxytocin-receptors, enhanced contractility, and increased sensitivity to circulating oxytocin. Stretching of the ‘birth canal’ during childbirth leads to the stimulation of specific autonomic afferents, reflex firing of oxytotic neurons and oxytocin release. A positive feedback loop is formed, oxytocin stimulating uterine contraction further and enhancing the production of additional local uterotonic mediators such as prostaglandins. The difficulties of analyzing pulsatile release, and the short circulating half-life of the hormone (due to placental cysteine aminopeptidase), have made it difficult to demonstrate increased circulating oxytocin levels in women during labor 24.. Mice lacking oxytocin have normal childbirth. Moreover, women with absent posterior pituitary function can have a normal labor. However, the importance of oxytocin in the birth process is highlighted by the effectiveness of oxytocin antagonists in the management of pre-term labor 26. The role of oxytocin in childbirth is not limited to maternal responses. Maternal oxytocin produces a switch to inhibitory GABAergic signaling in the fetal CNS (central nervous system). This, in turn, increases fetal neuronal resistance to damage that may occur during delivery. Oxytocin therefore mediates direct adaptive mother-fetal signaling during childbirth in line with a wider-ranging role in maternal-fetal physiology 27.
Oxytocin hormone and behavior
Oxytocin-receptor expression is widespread in the central nervous system (brain and spinal cord) of many species and oxytocin has widespread roles as a neurotransmitter, including neural networks that mediate a range of complex behaviors. In some cases, these overlap those involving vasopressin 28.
One of the most fascinating aspects of oxytocin hormone and its homologues are their fairly conserved role in the neural regulation of social behaviors 29. Oxytocin-related peptides act to modulate behavior, primarily promoting plasticity in innate behaviors 30. However, the nuances of how oxytocin acts to affect behavior are highly varied. This is ucularly true in the context of oxytocin’s sex-specific effects, which, due in part to oxytocin’s species-specific actions, makes it challenging to determine the ‘when’ and ‘where’ of oxytocin’s action. In fact, definitive statements about oxytocin’s effects with regard to the modulation of female versus male behavior are very difficult to make. Where in the brain oxytocin may function in sex-specific ways must first be considered, sex differences in neuroanatomy are often not clearly related to sex differences in behavior 31. It is also important to note that there has not been a lot of direct testing of sex differences in oxytocin’s behavioral effects, largely due to the fact that each sex is often studied in isolation, rather than at the same time with the same tests.
When sex differences are detected, females are reported as having more oxytocin immunoreactive fibers than males 32. These studies may indicate that sex differences in oxytocin function are due to its rate of axonal transport or secretion in response to physiological challenges, rather than to absolute amounts.
Oxytocin receptor expression, on the other hand, varies widely in its distribution and density between species. Two brain regions in which sex differences in the oxytocin receptor are regularly reported are the bed nucleus of the stria terminalis (BNST) and the the medial amygdala, with males typically having more oxytocin receptors in these brain regions than females 33. Though, there are studies which have found sex differences in the other direction (female > male) within other brain regions 34. Generally speaking, what is lacking, is scientific agreement on where there are consistently observed sex differences in oxytocin receptors. In almost all of the studies, oxytocin receptor binding only differs in a few brain areas and there is considerable species variation. Uncovering oxytocin’s contributions to sex differences in behavior is a challenge, possibly due to differential evolution of this system in the two sexes 35.
Oxytocin has important influences on reproductive behavior in rat; facilitating both lordosis and the development of maternal behavior patterns 25. However, mice lacking oxytocin exhibit normal sexual and maternal behavior, suggesting behavioral effects may be species-specific or the potential for considerable redundancy in neural pathways 24. Central oxytotic transmission reduces anxiety behavior and hypothalamo-pituitary-adrenal stress responses in female rats 24. It may be that oxytocin has a complex role in the stress response, with context-dependent differential effects 24.
Central oxytocin pathways have been implicated in social recognition, affiliative behavior and social bonding 24. This clustering has raised interest in the role of oxytocin and oxytocin-pathways in the development of autism spectrum disorder (ASD) 24. A number of association studies have demonstrated linkage between autistism spectrum disorder and Oxytocin-receptor polymorphisms. However, to date the effect size is inconsistent 24.
The neuropeptides vasopressin and oxytocin are involved in the regulation of diverse social behaviors such as social recognition, pair-bonding, and social cognition in mammals, including humans 36. Oxytocin and vasopressin are evolutionarily conserved, differing from each other by only two amino acids. Importantly, oxytocin and vasopressin often regulate social behavior in sex-specific ways.
At the core of positive social behaviors are neurobiological systems that regulate fear and threats versus safety (Figures 3 and 4). Oxytocin typically supports immobilization without fear, necessary in interactions with family and friendly associates 37. Vasopressin supports mobilization, and in some cases defensive aggression and protection of social boundaries. By contrast, vasopressin, in conjunction with corticotropin-releasing hormone (CRH), dopamine and many other molecules, may support active and mobilized coping strategies 38. However, as with many features of the oxytocin–vasopressin pathway, exceptions exist—possibly because of the capacity of oxytocin and vasopressin to interact with each other’s receptors (Figure 4).
Increasing evidence suggests that the actions of oxytocin on the vasopressin 1a receptor (V1aR), versus the oxytocin receptor (OTR), vary depending on the behavior and context being examined 39 (Figure 4). In hamsters, fear-based or aggressive effects of oxytocin rely on the vasopressin 1a receptor (V1aR) and social reward on the oxytocin receptor (OTR) 40. The capacity of oxytocin and vasopressin to bind to each other’s receptors adds complexity to attempts to understand both peptides. However, oxytocin–vasopressin interactions also are adaptive, increasing the capacity for a small number of peptides and receptors to regulate various processes across different tissues.
Both oxytocin and vasopressin are responsive to environmental and social demands, although in somewhat different ways 41. These peptides—presumably via interactions with their receptors—may have diverse physiological and behavioral properties. Regional effects of oxytocin and vasopressin are expected and need to be investigated to fully understand the functional consequences for these peptides. Dynamic interactions either on specific receptors, due to brain region-specific actions, or due to relative availability of the peptides to a receptor 19 could help to explain the behavioral properties of these two molecules. In addition, refined behavioral studies are necessary, since the effects of oxytocin and vasopressin on various behaviors change across time and as behavioral context changes.
Figure 3. Oxytocin and vasopressin hypothetical functions
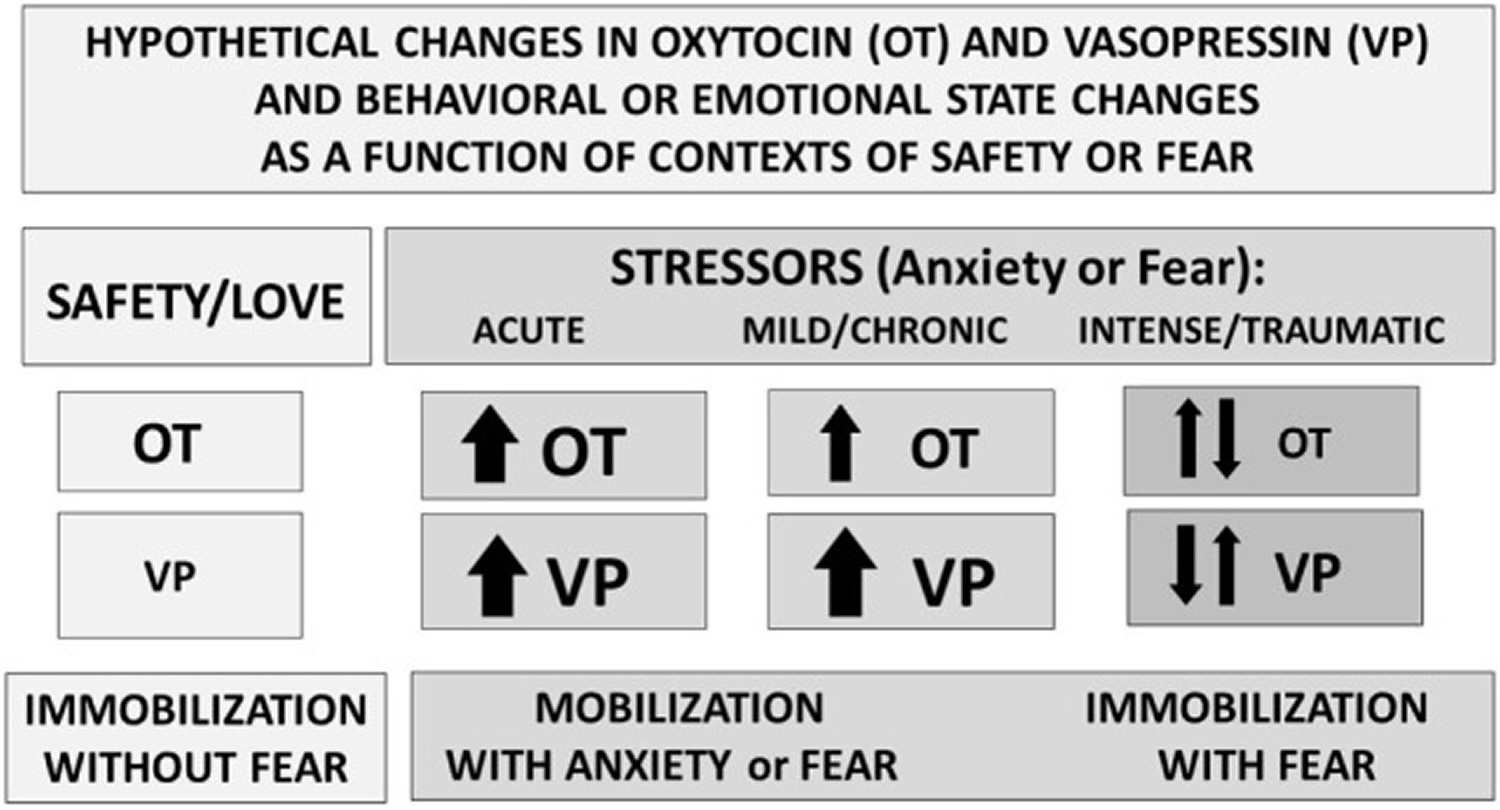
Footnotes: Perceived context and the intensity of challenge can regulate the release or effects of oxytocin (OT) and vasopressin (VP). Under conditions of safety, the actions of oxytocin (OT) may dominate, supporting high levels of sociality. In response to an acute stressor, both oxytocin (OT) and vasopressin (VP) increase, supporting mobilization and escape, followed in some cases by increases in social behavior especially toward “safe” conspecifics. Following intense or traumatic stressors, initial responses would include mobilization and anxiety. However, following a traumatic experience, individuals may vacillate between mobilization and immobilization with fear or revert to the more primitive response of shutting down. These patterns differ between males and females and as a function of individual life histories.
[Source 42]Figure 4. Oxytocin and vasopressin in human behavior
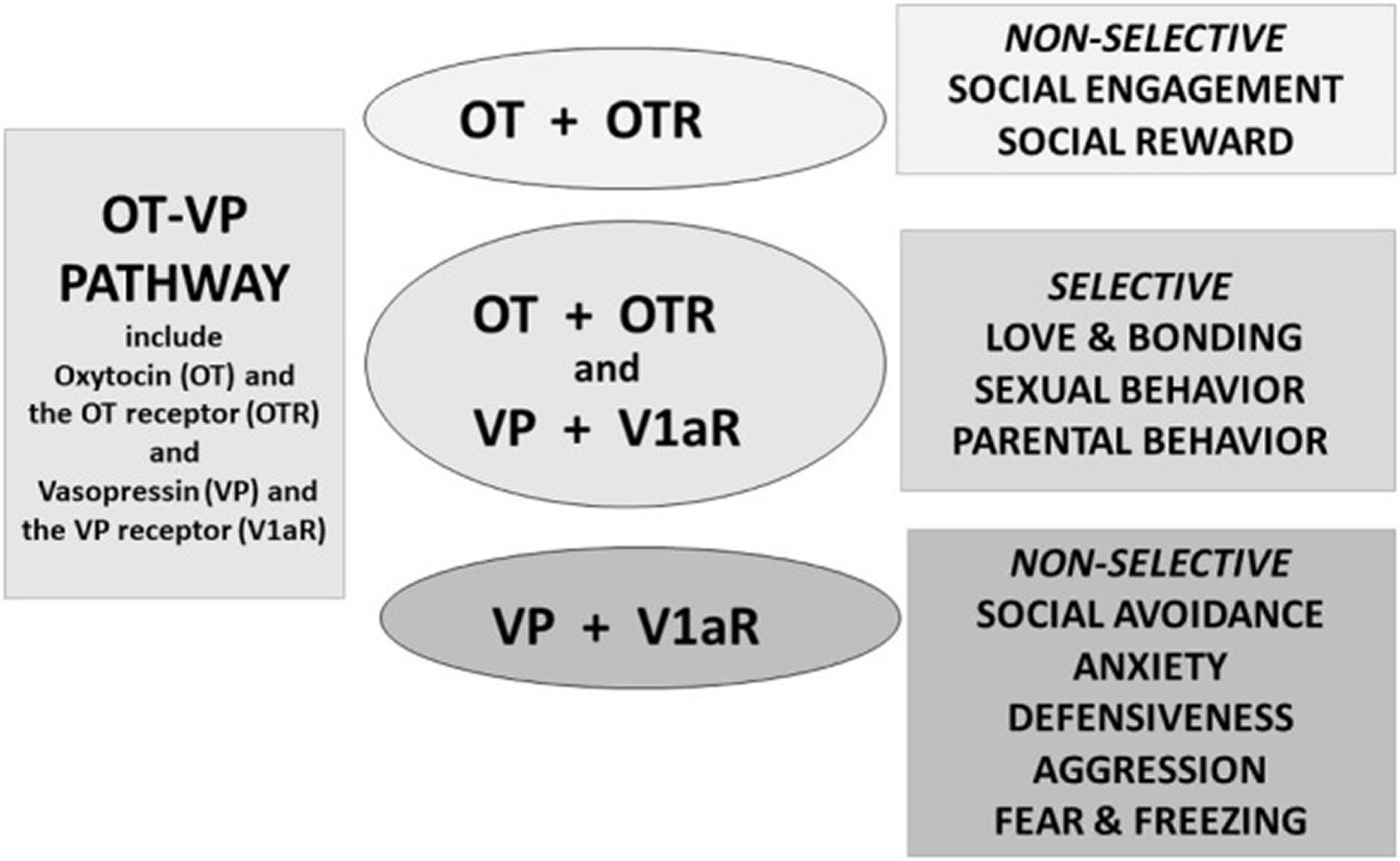
Footnotes: Oxytocin (OT) and vasopressin (VP) are components of an integrated pathway. Oxytocin (OT) and vasopressin (VP) interact dynamically with receptors [including the oxytocin receptor (OTR) or vasopressin 1a receptor (V1aR)] to influence social engagement and defensive behaviors. In many cases, oxytocin (OT) acts in conjunction with vasopressin (VP), via the V1aR or through effects on both the oxytocin receptor (OTR) and vasopressin 1a receptor (V1aR), thus regulating the capacity to form selective social behaviors. Oxytocin (OT) rarely acts alone but, especially under nonthreatening or “safe” conditions, may facilitate features of “love,” including social engagement, and social reward, and “immobility without fear”.
[Source 42]Oxytocin side effects
Oxytocin injection (synthetic oxytocin) acts on the smooth muscle of the uterus to stimulate contractions; response depends on the uterine threshold of excitability. It exerts a selective action on the smooth musculature of the uterus, particularly toward the end of pregnancy, during labor and immediately following delivery. Oxytocin stimulates rhythmic contractions of the uterus, increases the frequency of existing contractions and raises the tone of the uterine musculature. Synthetic oxytocin does not possess the cardiovascular effects, such as elevation of blood pressure, as exhibited by vasopressin found in posterior pituitary injection.
Oxytocin injection (synthetic oxytocin) is a sterile, clear, colorless solution of oxytocin in water for injection prepared by synthesis. Each mL of oxytocin injection, USP (synthetic), intended for intravenous infusion or intramuscular injection, possesses an oxytocic activity equivalent to 10 USP oxytocin units and contains chlorobutanol anhydrous (chloral derivative) 0.5%. This product may contain up to 12.5% decomposition products/impurities.
Oxytocin injection may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
Common oxytocin side effects may include:
- nausea and vomiting;
- runny nose, sinus pain or irritation;
- memory problems; or
- more intense or more frequent contractions (this is an expected effect of oxytocin).
Some oxytocin side effects can be serious. Get emergency medical help if you have signs of an allergic reaction: hives; difficult breathing; swelling of your face, lips, tongue, or throat.
- rash
- hives
- itching
- difficulty breathing or swallowing
- swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs
- fast heartbeat
- unusual bleeding
Rare oxytocin side effects
- confusion
- convulsions (seizures)
- difficulty in breathing
- dizziness
- fast or irregular heartbeat
- headache (continuing or severe)
- hives
- pelvic or abdominal pain (severe)
- skin rash or itching
- vaginal bleeding (increased or continuing)
- weakness
- weight gain (rapid)
Incidence not known
- abdominal pain or cramping
- blood clotting problem that causes prolonged bleeding
- chest pain or discomfort
- cough
- difficulty swallowing
- extra heartbeats
- fainting
- lightheadedness
- pounding or rapid pulse
- puffiness or swelling of the eyelids or around the eyes, face, lips, or tongue
- severe bleeding after giving birth
- shortness of breath
- tightness in the chest
- unusual tiredness or weakness
- wheezing
Get emergency help immediately if any of the following symptoms of overdose occur while taking oxytocin:
Symptoms of oxytocin overdose
- restlessness
- shakiness
- sleepiness
- slow to respond
- slurred speech
- unconsciousness
Oxytocin injection may cause other side effects. Call your doctor if you have any unusual problems while receiving this medication.
Contraindications
Oxytocin injection (synthetic) is contraindicated in any of the following conditions:
- Significant cephalopelvic disproportion;
- Unfavorable fetal positions or presentations which are undeliverable without conversion prior to delivery, i.e., transverse lies;
- In obstetrical emergencies where the benefit-to-risk ratio for either the fetus or the mother favors surgical intervention;
- In cases of fetal distress where delivery is not imminent;
- Prolonged use in uterine inertia or severe toxemia;
- Hypertonic uterine patterns;
- Patients with hypersensitivity to the drug;
- Induction or augmentation of labor in those cases where vaginal delivery is contraindicated, such as cord presentation or prolapse, total placenta previa, and vasa previa.
- 173 – Pathophysiology of Preterm Birth. Fetal and Neonatal Physiology (Fifth Edition). Volume 2, 2017, Pages 1732-1737.e2. https://doi.org/10.1016/B978-0-323-35214-7.00173-6[↩]
- Bradley ER, Woolley JD. Oxytocin effects in schizophrenia: Reconciling mixed findings and moving forward. Neurosci Biobehav Rev. 2017;80:36-56. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5682229/[↩]
- Aerosolized oxytocin increases cerebrospinal fluid oxytocin in rhesus macaques. Modi ME, Connor-Stroud F, Landgraf R, Young LJ, Parr LA. Psychoneuroendocrinology. 2014 Jul; 45():49-57.[↩]
- A critical review of the influence of oxytocin nasal spray on social cognition in humans: evidence and future directions. Guastella AJ, MacLeod C. Horm Behav. 2012 Mar; 61(3):410-8. https://www.ncbi.nlm.nih.gov/pubmed/22265852/[↩]
- Oxytocin and vasopressin in the human brain: social neuropeptides for translational medicine. Meyer-Lindenberg A, Domes G, Kirsch P, Heinrichs M. Nat Rev Neurosci. 2011 Aug 19; 12(9):524-38.[↩]
- Oxytocin enhances pupil dilation and sensitivity to ‘hidden’ emotional expressions. Leknes S, Wessberg J, Ellingsen DM, Chelnokova O, Olausson H, Laeng B. Soc Cogn Affect Neurosci. 2013 Oct; 8(7):741-9.[↩]
- Oxytocin increases trust in humans. Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E. Nature. 2005 Jun 2; 435(7042):673-6.[↩]
- Neurophysiological effects of acute oxytocin administration: systematic review and meta-analysis of placebo-controlled imaging studies. Wigton R, Radua J, Allen P, Averbeck B, Meyer-Lindenberg A, McGuire P, Shergill SS, Fusar-Poli P. J Psychiatry Neurosci. 2015 Jan; 40(1):E1-22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4275335/[↩]
- Low-dose oxytocin delivered intranasally with Breath Powered device affects social-cognitive behavior: a randomized four-way crossover trial with nasal cavity dimension assessment. Quintana DS, Westlye LT, Rustan ØG, Tesli N, Poppy CL, Smevik H, Tesli M, Røine M, Mahmoud RA, Smerud KT, Djupesland PG, Andreassen OA. Transl Psychiatry. 2015 Jul 14; 5():e602.[↩]
- Beyond the hype and hope: Critical considerations for intranasal oxytocin research in autism spectrum disorder. Alvares GA, Quintana DS, Whitehouse AJ. Autism Res. 2017 Jan; 10(1):25-41. https://www.ncbi.nlm.nih.gov/pubmed/27651096/[↩]
- Personality-dependent effects of oxytocin: greater social benefits for high alexithymia scorers. Luminet O, Grynberg D, Ruzette N, Mikolajczak M. Biol Psychol. 2011 Jul; 87(3):401-6.[↩]
- A double-blind randomized controlled trial of oxytocin nasal spray in Prader Willi syndrome. Einfeld SL, Smith E, McGregor IS, Steinbeck K, Taffe J, Rice LJ, Horstead SK, Rogers N, Hodge MA, Guastella AJ. Am J Med Genet A. 2014 Sep; 164A(9):2232-9.[↩]
- Oxytocin, but not vasopressin, impairs social cognitive ability among individuals with higher levels of social anxiety: a randomized controlled trial. Tabak BA, Meyer ML, Dutcher JM, Castle E, Irwin MR, Lieberman MD, Eisenberger NI. Soc Cogn Affect Neurosci. 2016 Aug; 11(8):1272-9.[↩]
- Social effects of oxytocin in humans: context and person matter. Bartz JA, Zaki J, Bolger N, Ochsner KN. Trends Cogn Sci. 2011 Jul; 15(7):301-9. https://www.ncbi.nlm.nih.gov/pubmed/21696997/[↩]
- Oxytocin and social salience: a call for gene-environment interaction research. Tabak BA. Front Neurosci. 2013; 7:199.[↩]
- Intranasal Oxytocin: Myths and Delusions. Leng G, Ludwig M. Biol Psychiatry. 2016 Feb 1; 79(3):243-50. https://www.ncbi.nlm.nih.gov/pubmed/26049207/[↩]
- Plasma and CSF oxytocin levels after intranasal and intravenous oxytocin in awake macaques. Freeman SM, Samineni S, Allen PC, Stockinger D, Bales KL, Hwa GG, Roberts JA. Psychoneuroendocrinology. 2016 Apr; 66():185-94.[↩]
- Does Oxytocin Increase Trust in Humans? A Critical Review of Research. Nave G, Camerer C, McCullough M. Perspect Psychol Sci. 2015 Nov; 10(6):772-89.[↩]
- Chini B, Verhage M, Grinevich V. The action radius of oxytocin release in the mammalian CNS: from single vesicles to behavior. Trends Pharmacol Sci (2017) 38(11):982–91.10.1016/j.tips.2017.08.005[↩][↩][↩]
- Grinevich V, Knobloch-Bollmann HS, Eliava M, Busnelli M, Chini B. Assembling the puzzle: pathways of oxytocin signaling in the brain. Biol Psychiatry (2016) 79:155–64.10.1016/j.biopsych.2015.04.013[↩][↩]
- Geenen V. Thymus-dependent T cell tolerance of neuroendocrine functions: principles, reflections, and implications for tolerogenic/negative self-vaccination. Ann N Y Acad Sci (2006) 1088:284–96.10.1196/annals.1366.009[↩]
- Stoop R, Hegoburu C, Van Den Burg E. New opportunities in vasopressin and oxytocin research: a perspective from the amygdala. Annu Rev Neurosci (2015) 38:369–88.10.1146/annurev-neuro-071714-033904[↩]
- Dumais KM, Veenema AH. Vasopressin and oxytocin receptor systems in the brain: sex differences and sex-specific regulation of social behavior. Front Neuroendocrinol (2016) 40:1–23.10.1016/j.yfrne.2015.04.003[↩]
- PhD PSGB. The Neurohypophysis: Endocrinology of Vasopressin and Oxytocin. [Updated 2017 Apr 22]. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279157[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Russell JA, Leng G 1998. Sex, parturition and motherhood without oxytocin? Journal of Endocrinology 157, 343-359.[↩][↩]
- Goodwin TM, Valenzuela GJ, Silver H, Creasy G 1996. Dose ranging study of the oxytocin antagonist atosiban in the treatment of preterm labor. Atosiban Study Group. Obstetrics and Gynecology 88, 331-336.[↩]
- Tyzio R, Cossart R, Khalilov I et al. 2006. Maternal Oxytocin triggers a transient Inhibitory switch in GABA signaling in the fetal brain during delivery. Science 15, 1788-1792.[↩]
- Dumais KM, Veenema AH 2016. Vasopressin and oxytocin receptor systems in the brain: sex differences and sex-specidic regualtion of social behavior. Frontiers in Neuroendocrinology 40, 1-23.[↩]
- Oxytocin and sex differences in behavior. Current Opinion in Behavioral Sciences Volume 23, October 2018, Pages 13-20. https://doi.org/10.1016/j.cobeha.2018.02.002[↩]
- Caldwell HK: Oxytocin and vasopressin: powerful regulators of social behavior. Neuroscientist 2017. 1073858417708284.[↩]
- McCarthy MM: Multifaceted origins of sex differences in the brain. Philos Trans R Soc Lond B Biol Sci 2016, 371:20150106.[↩]
- Qiao X, Yan Y, Wu R, Tai F, Hao P, Cao Y, Wang J: Sociality and oxytocin and vasopressin in the brain of male and female dominant and subordinate mandarin voles. J Comp Physiol A Neuroethol Sens Neural Behav Physiol 2014, 200:149-159.[↩]
- Rice MA, Hobbs LE, Wallace KJ, Ophir AG: Cryptic sexual dimorphism in spatial memory and hippocampal oxytocin receptors in prairie voles (Microtus ochrogaster). Horm Behav 2017, 95:94-102.[↩]
- Dumais KM, Bredewold R, Mayer TE, Veenema AH: Sex differences in oxytocin receptor binding in forebrain regions: correlations with social interest in brain region- and sexspecific ways. Horm Behav 2013, 64:693-701.[↩]
- Gao S, Becker B, Luo L, Geng Y, Zhao W, Yin Y, Hu J, Gao Z, Gong Q, Hurlemann R, Yao D, Kendrick KM: Oxytocin, the peptide that bonds the sexes also divides them. Proc Natl Acad Sci U S A 2016, 113:7650-7654.[↩]
- Albers, H.E., 2014. Species, sex and individual differences in the vasotocin/vasopressin system: relationship to neurochemical signaling in the social behavior neural network. Frontiers in Neuroendocrinology Volume 36, January 2015, Pages 49-71. https://doi.org/10.1016/j.yfrne.2014.07.001[↩]
- Porges SW. Love: an emergent property of the mammalian autonomic nervous system. Psychoneuroendocrinology (1998) 23:837–61.10.1016/S0306-4530(98)00057-2[↩]
- Herman JP, Tasker JG. Paraventricular hypothalamic mechanisms of chronic stress adaptation. Front Endocrinol (2016) 7:137.10.3389/fendo.2016.00137[↩]
- Albers HE. Species, sex and individual differences in the vasotocin/vasopressin system: relationship to neurochemical signaling in the social behavior neural network. Front Neuroendocrinol (2015) 36:49–71.10.1016/j.yfrne.2014.07.001[↩]
- Song Z, Larkin TE, Malley MO, Albers HE. Oxytocin (OT) and arginine-vasopressin (Avp) act on OT receptors and not Avp V1a receptors to enhance social recognition in adult Syrian hamsters (Mesocricetus auratus). Horm Behav (2016) 81:20–7.10.1016/j.yhbeh.2016.02.004[↩]
- Neumann ID, Slattery DA. Oxytocin in general anxiety and social fear: a translational approach. Biol Psychiatry (2016) 79:213–21.10.1016/j.biopsych.2015.06.004[↩]
- Carter CS. The Oxytocin–Vasopressin Pathway in the Context of Love and Fear. Frontiers in Endocrinology. 2017;8:356. doi:10.3389/fendo.2017.00356. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5743651/[↩][↩]





{kind=link}