Contents
What is parathyroid adenoma
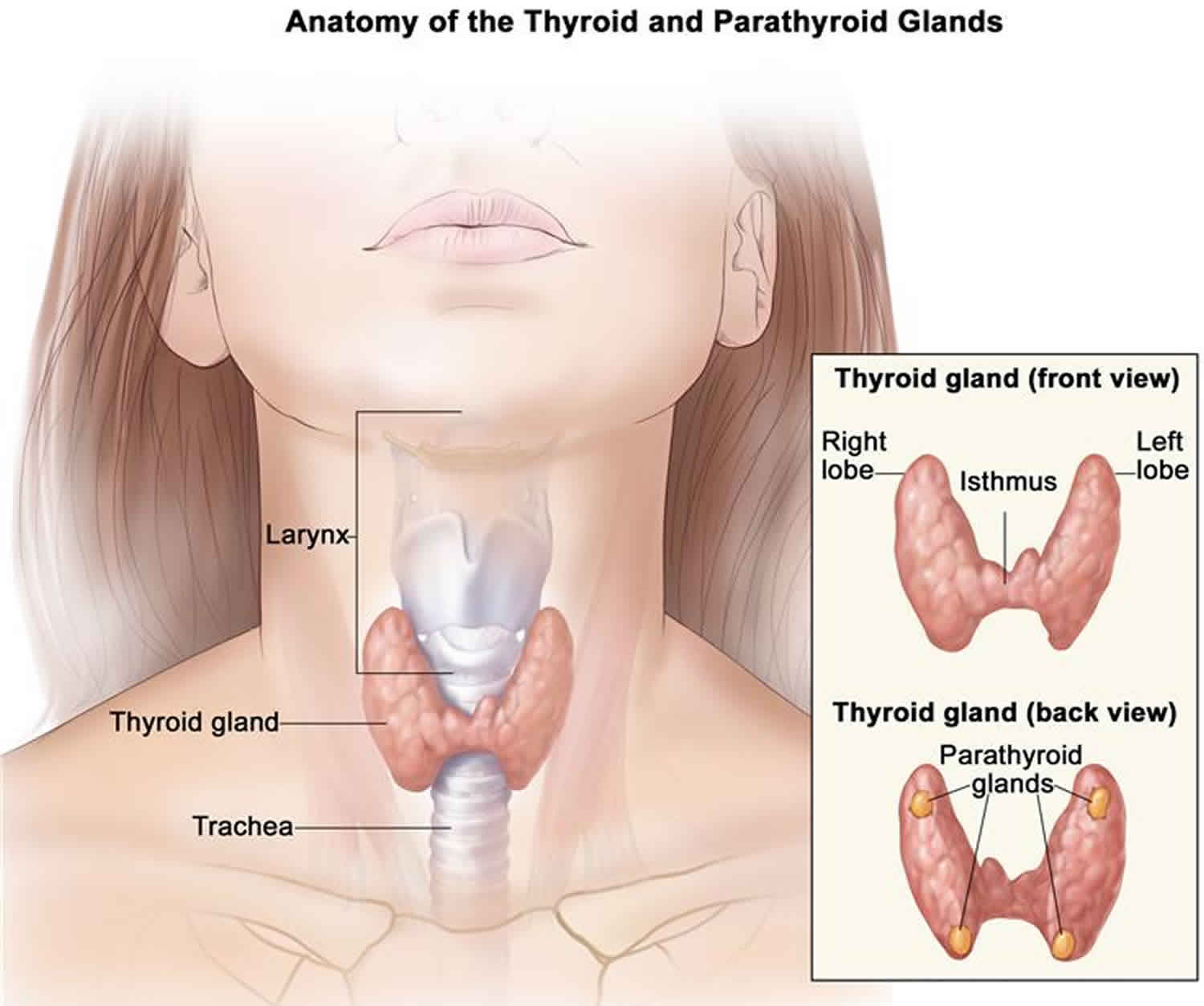
A parathyroid adenoma is a noncancerous (benign) tumor of the parathyroid glands. The parathyroid glands are located in the neck, near or attached to the back side of the thyroid gland. The parathyroid glands in the neck help control calcium use and removal by the body. The parathyroid glands do this by producing parathyroid hormone (PTH). Parathyroid hormone (PTH) helps control calcium, phosphorus, and vitamin D levels in the blood and is important for healthy bones.
A single parathyroid adenoma is responsible for 80% to 85% of hyperparathyroidism, with double adenomas the culprit in 4% to 5%, and parathyroid hyperplasia in 10% to 12% 1. Parathyroid adenomas are most common in patients 50 to 70 years old; however, they can occur at any age. Women are affected 3-times as often as men 2.
Many patients with a parathyroid adenoma are asymptomatic, with hypercalcemia incidentally discovered on routine lab work. Symptomatic parathyroid disease will most commonly manifest as symptoms of hypercalcemia such as bone pain, abdominal pain, fatigue, polyuria, nephrolithiasis, constipation, mental changes and depression. More extreme elevations in calcium can cause complications such as cardiac arrhythmias, coma, and death. A patient is unlikely to have outward physical signs of a parathyroid adenoma.
Parathyroid adenoma diagnosis is often made by the presence of hypercalcemia in blood, followed by an imaging test of the neck.
Most parathyroid adenomas do not have an identified cause. Sometimes a genetic problem is the cause. This is more common if the diagnosis is made when you are young.
Conditions that stimulate the parathyroid glands to get bigger can also cause an adenoma. These include:
- Genetic disorders
- Taking the drug lithium
- Chronic kidney disease
Women over age 60 have the highest risk for developing this condition. Radiation to the head or neck also increases risk.
Parathyroid adenoma causes
The cause of a parathyroid adenoma remains unknown for most patients 1. The most common genetic mutation associated with sporadic parathyroid adenomas is the cyclin D1/PRAD1 gene. Alteration in the normal function of this gene affects parathyroid hormone (PTH) secretion. Approximately 20% to 40% of sporadic parathyroid adenomas have overexpression of cyclin D1. Regarding environmental factors, some data suggest that a history radiation therapy predisposes a patient to parathyroid disease later in life. Long-term calcium deficiency may also result in parathyroid disease due to chronic stimulation of parathyroid hormone (PTH) 3.
A parathyroid adenoma is primarily composed of chief cells, but it can also include oxyphil cells, oncocytes, transitional oncocytes, or a mixture of these cell types. There may also be a rim of normal parathyroid tissue surrounding the adenoma. Microadenomas tend to be unencapsulated; however, larger tumors may have a thin fibrous capsule present with cystic degeneration seen within the tumor. Characteristics such as thick fibrous capsule, adherence to surrounding tissues, vascular and capsular invasion, tumor necrosis, and increased mitotic activity should not be seen in benign adenoma and are more suggestive of carcinoma.
Parathyroid adenoma symptoms
Many people with parathyroid adenoma have no symptoms. Parathyroid adenoma is often discovered when blood tests are done for another medical reason.
Parathyroid adenomas are the most common cause of hyperparathyroidism (overactive parathyroid glands), which leads to an increased blood calcium level. Symptoms may include any of the following:
- Confusion
- Constipation
- Lack of energy (lethargy)
- Muscle pain
- Nausea or decreased appetite
- Urinating more often at night
- Weak bones or fractures
The pathologic gland itself is rarely palpable, and an obvious neck mass is more suggestive of thyroid pathology or parathyroid carcinoma.
Parathyroid adenoma complications
An untreated parathyroid adenoma could cause complications related to hypercalcemia. A rare clinical phenomenon is a parathyroid crisis, which is characterized by extremely high calcium levels, usually more than 15 mg/dL. Symptoms include changes in mental status leading to nervous system failure and coma.
Osteoporosis and the increased risk for bone fractures is the most common concern.
Other complications are less common, but may include:
- Nephrocalcinosis (calcium deposits in the kidneys that can reduce kidney function)
- Osteitis fibrosa cystica (softened, weak areas in the bones)
Complications from surgery include:
- Damage to a nerve that controls your voice
- Damage to the parathyroid glands, which causes hypoparathyroidism (lack of enough parathyroid hormone) and low calcium level
Complications can also arise with resection of the parathyroid adenoma. Injury to the recurrent laryngeal nerve is a serious complication of endocrine surgery and has consequences of hoarseness (unilateral damage) or airway occlusion (bilateral damage). Direct trauma to the nerve due to clipping, grasping, or stretching can cause damage. Indirect deleterious effects on the nerve include skeletonization, thermal injury, or compression. The damage may be transient in cases of compression or stretching, and may resolve in 4 to 6 weeks. However, if improvement in function is not seen after 6 to 12 months, the damage should be presumed to be permanent. If the damage is recognized intra-operatively, immediate primary repair or grafting should be performed.
Parathyroid adenoma diagnosis
Blood tests may be done to check levels of:
- Parathyroid hormone (PTH)
- Calcium
- Phosphorus
- Vitamin D
A 24-hour urine test may be done to check for increased calcium in the urine.
Other tests include:
- Bone density exam
- Kidney ultrasound or CT scan (may show kidney stones)
- Kidney x-rays (may show kidney stones)
- MRI
- Neck ultrasound
- Sestamibi neck scan (to check for swelling of the parathyroid glands)
Hypercalcemia seen on routine lab work performed for other purposes is the most common initial sign of hyperparathyroidism. In most patients, this hypercalcemia is mild and may even be intermittent, and is usually less than 1.0 mg/dL above normal upper limits. Unexplained hypercalcemia on a repeated set of lab work warrants further investigation. PTH level should be subsequently measured, and it may be elevated or even within normal limits, although inappropriately so given the patient’s hypercalcemia. Twenty-four-hour urinary calcium may also be measured, but it is not essential for diagnosis 4.
The next step in evaluation is radiographic imaging. Imaging is essential because it not only guides operative planning but distinguishes a single adenoma from a multi-gland hyperplastic disease.
Normal parathyroids are generally too small to be seen on ultrasound; therefore, visualization of this gland should raise suspicion for a pathologic process. If an adenoma identifiable on ultrasound, it should appear as homogeneously hypoechoic extrathyroidal oval mass with a fat plane separating it from normal thyroid tissue. A feeding artery may also be visualized entering the superior or inferior pole of the adenoma. Ultrasound alone has a sensitivity of only 60% to 80% because it is operator dependent. It may be used as an adjunct nuclear imaging.
The gold standard of parathyroid localization is single-radioisotope scintigraphy with technetium-99m (99mTc) combined with single photon emission computed tomography (SPECT) imaging. SPECT is a 3-dimensional sestamibi scan which improves the visualization of parathyroid glands. The combination of these methods has a 91% to 98% sensitivity for identifying parathyroid adenomas.
An alternative is dual-radioisotope imaging, in which both 99mTc pertechnetate and thallium-201 (201Tl) are given. Thallium is taken up by both the thyroid and parathyroid, while pertechnetate only has avidity for the thyroid. Subtraction imaging is then used to visualize the glands. Drawbacks to this method include the necessity of a subtraction program, long imaging times, and limited views.
Four-dimensional CT and MRI have also been used in parathyroid imaging. However, they are only 75% and 40% to 85% sensitive respectively. For that reason, nuclear imaging for preoperative localization. Four-dimensional CT and MRI may have a more beneficial role in localizing ectopic glands after failed parathyroidectomy. In a study of 45 patients who had undergone previous neck exploration, 4-dimensional CT had 88% sensitivity for abnormal parathyroid glands compared with sestamibi SPECT or neck ultrasound (54% and 21%, respectively).
Figure 1. Parathyroid adenoma ultrasound
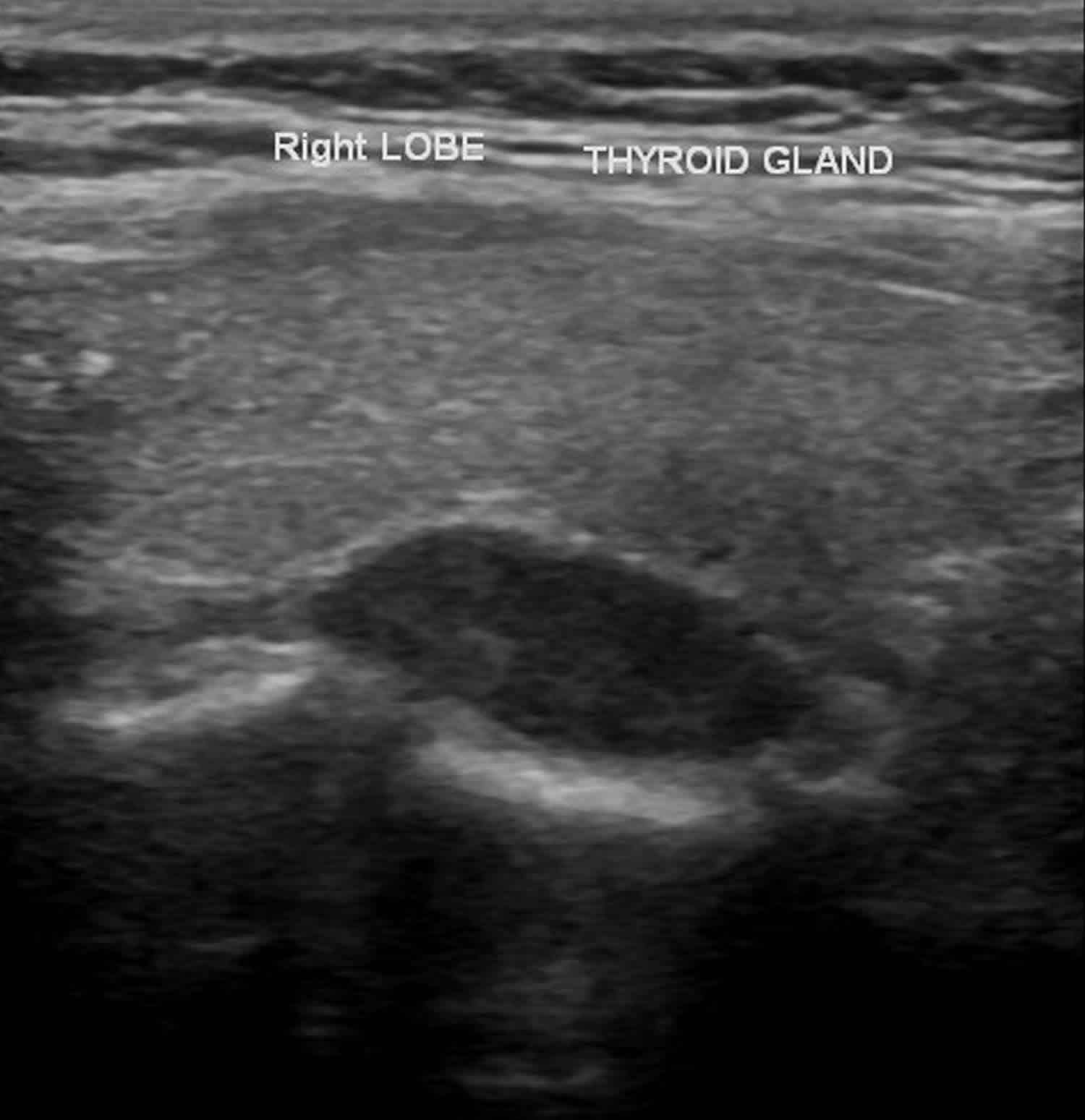
Figure 2. Parathyroid adenoma SPECT scan
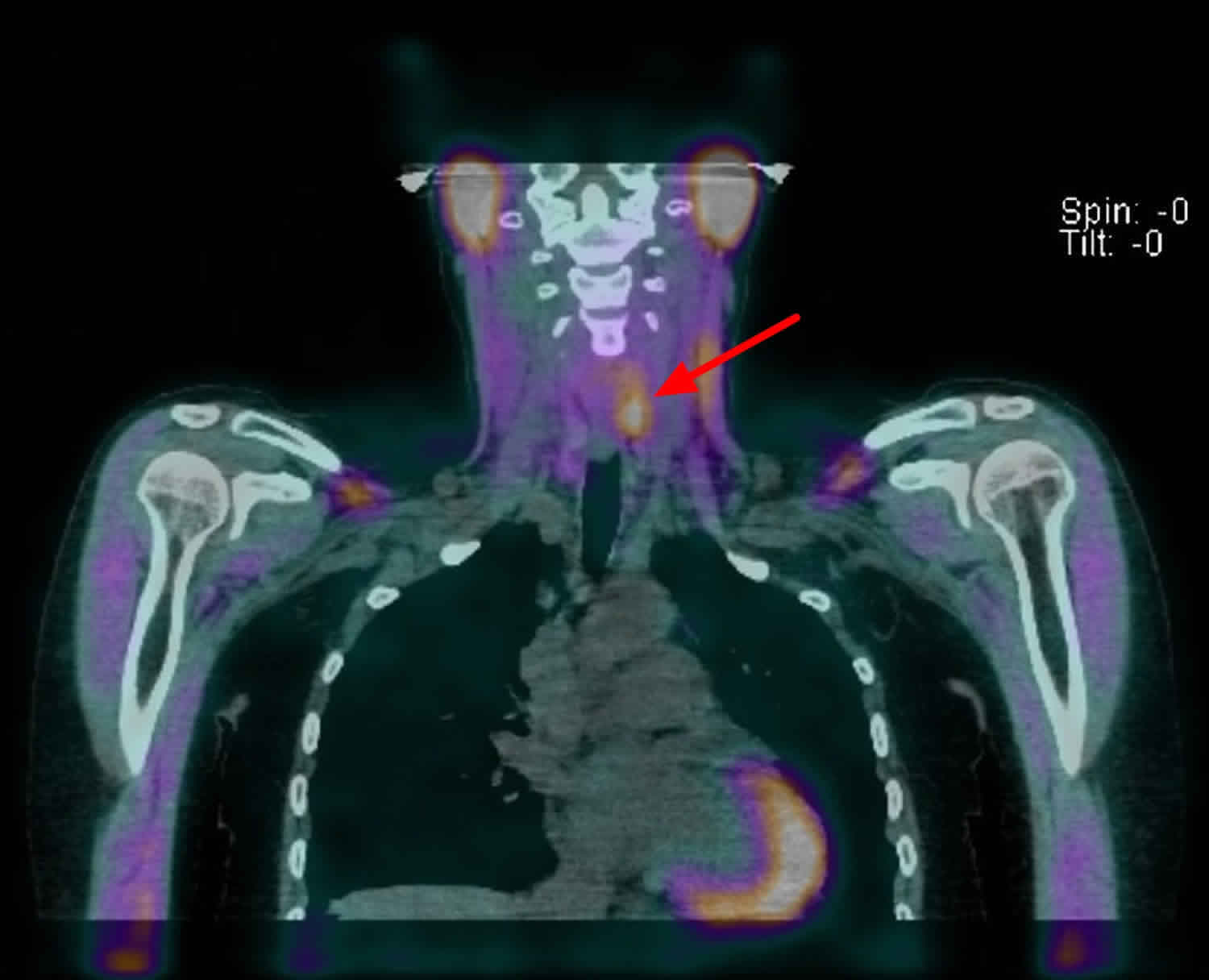
Footnote: Static and SPECT images were acquired at 15 min and 3 hours. Delayed CT- SPECT was performed. Initial images show mild focal uptake in the region of the thyroid left upper and right lower poles. No other abnormal extra-thyroid uptake is detected in the rest of the neck or mediastinum. Delayed images show locally retained uptake corresponding to a soft tissue nodule posterior to the left upper pole and another little nodule posterior to the right lower pole. Mild uptake in sub centimeter left supraclavicular lymph nodes is non-specific. Mild uptake in the left anterior mediastinum is probably within physiological limits.
Parathyroid adenoma treatment
Surgery is the most common treatment, and it often cures the parathyroid adenoma. But, some people choose to only have regular checkups with their health care provider if the hyperparathyroidism (overactive parathyroid glands) is mild.
To help improve hyperparathyroidism (overactive parathyroid glands), your doctor may ask you to stop taking calcium and vitamin D supplements. Women who have gone through menopause may want to discuss treatment with estrogen.
Parathyroid adenoma surgery
Traditionally, bilateral 4-gland exploration was the procedure of choice for hyperparathyroidism. However, because a single parathyroid adenoma causes 85% of the disease, minimally invasive parathyroidectomy is emerging as the gold standard for a parathyroid adenoma 5.
After parathyroidectomy, the calcium levels will drop for the next 2-4 days but few patients will develop symptoms. However, if symptoms appear, treatment with calcium gluconate may be required. if the hypocalcemic state persists, one will need to supplement with oral calcium.
Due to the short half-life of PTH, the Miami criteria dictates that the PTH level should decrease by at least 50% within 10 minutes of parathyroid adenoma removal. If this value is not met, further exploration is warranted. Missing parathyroid glands can be found in the retropharyngeal or retro- esophageal planes, posterior mediastinum, thymus, mediastinum, inside the thyroid capsule or gland, or in the carotid sheath 6.
Persistent hyperparathyroidism after parathyroid surgery is most likely due to a missed parathyroid adenoma. The thymus has been reported as the most common ectopic site for parathyroid adenomas, followed by the thyroid gland, undescended glands, carotid sheath and the retroesophageal space.
Parathyroid adenoma prognosis
When treated, parathyroid adenoma outlook is generally good.
- Wolfe SA, Sharma S. Parathyroid Adenoma. [Updated 2019 Mar 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507870[↩][↩]
- Edafe O, Collins EE, Ubhi CS, Balasubramanian SP. Current predictive models do not accurately differentiate between single and multi gland disease in primary hyperparathyroidism: a retrospective cohort study of two endocrine surgery units. Ann R Coll Surg Engl. 2018 Feb;100(2):140-145[↩]
- Sahli ZT, Karipineni F, Zeiger MA. A garden of parathyroid adenomas. BMJ Case Rep. 2017 Aug 03;2017[↩]
- Raruenrom Y, Theerakulpisut D, Wongsurawat N, Somboonporn C. Diagnostic accuracy of planar, SPECT, and SPECT/CT parathyroid scintigraphy protocols in patients with hyperparathyroidism. Nucl Med Rev Cent East Eur. 2018;21(1):20-25.[↩]
- Komarowska H, Bromińska B, Luftmann B, Ruchała M. Primary hyperparathyroidism in pregnancy – a review of literature. Ginekol. Pol. 2017;88(5):270-275[↩]
- Mourad M, Buemi A, Darius T, Maiter D. Surgical options for primary hyperparathyroidism. Ann. Endocrinol. (Paris). 2015 Oct;76(5):638-42.[↩]





{kind=link}