
Contents
What is paronychia
Paronychia is also called whitlow, is a skin infection around the fingernails or toenails from which the nail plate originates, which is called the proximal nail fold. Paronychia usually affects the skin at the base (cuticle) or up the sides of the nail. There are two types of paronychia:
- Acute paronychia – comes on suddenly and may not last long (< 6 weeks); it usually occurs on fingers. Acute paronychia is often caused by the Staphylococcus aureus bacteria, although any number of germs such as candida (yeast) or the cold sore virus (herpes simplex virus [HSV]) can be involved (see Figure 6 below). Acute paronychia usually starts after a minor injury to the nail fold, such as from nail biting, picking or manicures. Acute paronychia presents as a red, warm, tender swelling, most commonly of the lateral nail folds, with erythema (redness) and sometimes pus may be seen, which can form around the nail and may lift the nail. Acute paronychia can occasionally evolve into an abscess.
- Chronic paronychia – lasts longer (persisting > 6 weeks) and may occur on your fingers or toes. Chronic paronychia either doesn’t get better or keeps coming back. Chronic paronychia is caused by a mixture of yeasts (candida, herpes simplex and bacteria Staphylococcus aureus). Chronic paronychia is most common in people who often have their hands in water, detergents or chemicals, have poor circulation (cold hands and feet) or diabetes. Women get chronic paronychia more often than men. In chronic paronychia the nail plate thickens and is distorted, often with transverse ridges (see Figure 8 below).
Paronychia can happen to adults and children. Usually paronychia isn’t serious and can be treated at home.
Paronychia treatment at home
- Try soaking the nails in warm water for acute paronychia.
- Avoid water and chemical exposure to prevent symptoms of chronic paronychia.
Treatments your physician may prescribe
The optimal treatment is different for acute verus chronic paronychia. For acute paronychia, optimal treatment is systemic/topical treatment or surgery. For chronic paronychia, optimal treatment is prevention and treatment of the chronic inflammation.
For acute paronychia, your doctor may:
- Puncture and drain the affected area and test for bacteria or viral infection.
- Prescribe antibiotics for a bacterial infection or an antiviral medication for a herpes infection.
For chronic paronychia, your doctor may:
- Prescribe a topical steroid.
- Prescribe a topical antifungal medication.
- Prescribe an oral antifungal medicine or antibiotics.
Treatment of chronic paronychia includes avoiding exposure to contact irritants and appropriate management of underlying inflammation or infection 1. A broad-spectrum topical antifungal agent can be used to treat the condition and prevent recurrence 2 Application of emollient lotions to lubricate the nascent cuticle and the hands is usually beneficial. One randomized controlled trial assigned 45 adults with chronic paronychia to treatment with a systemic antifungal agent (itraconazole [Sporanox] or terbinafine [Lamisil]) or a topical steroid cream (methylprednisolone aceponate [Advantan, not available in the United States]) for three weeks 3. After nine weeks, more patients in the topical steroid group were improved or cured (91 versus 49 percent; number needed to treat = 2.4).
The presence or absence of Candida seems to be unrelated to the effectiveness of treatment. Given their lower risks and costs compared with systemic antifungals, topical steroids should be the first-line treatment for patients with chronic paronychia 3. Alternatively, topical treatment with a combination of steroid and antifungal agents may also be used in patients with simple chronic paronychia, although data showing the superiority of this treatment to steroid use alone are lacking 4. Intralesional corticosteroid administration (triamcinolone [Amcort]) may be used in refractory cases.8,19 Systemic corticosteroids may be used for treatment of inflammation and pain for a limited period in patients with severe paronychia involving several fingernails.
If patients with chronic paronychia do not respond to topical therapy and avoidance of contact with water and irritants, a trial of systemic antifungals may be useful before attempting invasive approaches. Commonly used medications for chronic paronychia are listed in Table 2 below.
In patients with recalcitrant chronic paronychia, en bloc excision of the proximal nail fold is effective. Simultaneous avulsion of the nail plate (total or partial, restricted to the base of the nail plate) improves surgical outcomes 5. Alternatively, an eponychial marsupialization, with or without nail removal, may be performed 6. This technique involves excision of a semicircular skin section proximal to the nail fold and parallel to the eponychium, expanding to the edge of the nail fold on both sides 6. Paronychia induced by the epidermal growth factor receptor inhibitor cetuximab can be treated with an antibiotic such as doxycycline (Vibramycin) 7. In patients with paronychia induced by indinavir, substitution of an alternative antiretroviral regimen that retains lamivudine and other protease inhibitors can resolve retinoid-like manifestations without recurrences (Garcia-Silva J, Almagro M, Peña-Penabad C, Fonseca E. Indinavir-induced retinoid-like effects: incidence, clinical features and management. Drug Saf. 2002;25(14):993–1003.()).
Preventive measures for chronic paronychia are described in paronychia prevention below.
Figure 1. Paronychia finger

Figure 2. Paronychia toe

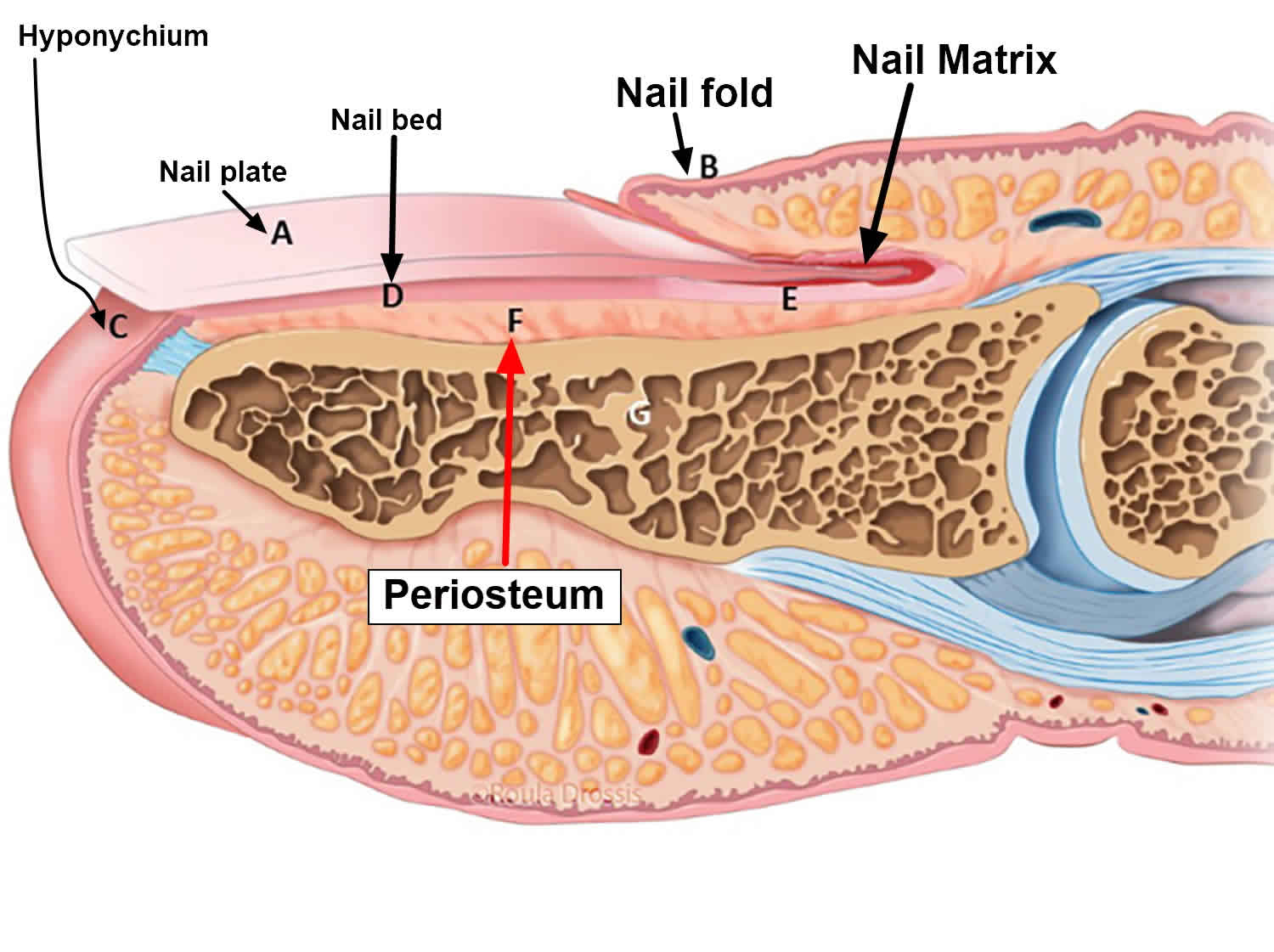
Figure 3. Fingernail
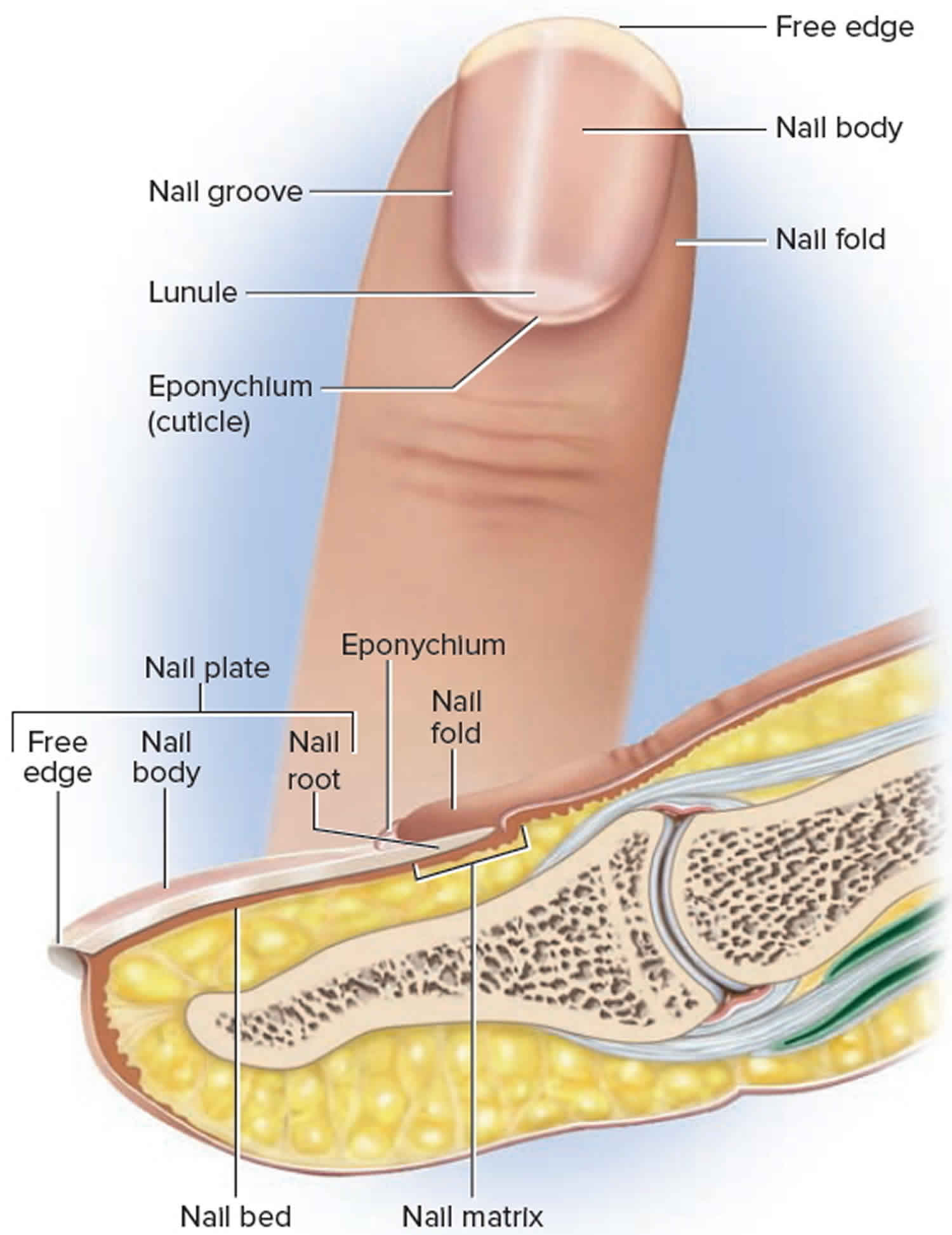
Figure 4. Toenail
Acute paronychia
Acute paronychia develops along a break in the skin and is usually seen at the side of the nail (see Figure 5). Acute paronychia usually develops rapidly over a few hours, and usually affects a single nail fold. Symptoms are pain, redness and swelling. Sometimes yellow pus appears under the cuticle and can evolve to abscess. The nail plate may lift up (onycholysis). Acute paronychia due to Streptococcus pyogenes may be accompanied by fever, lymphangiitis and tender lymphadenopathy. Acute candida more commonly infects the proximal nail fold.
Acute paronychia nail infection is often caused by a bacterial infection but may also be caused by herpes simplex virus (HSV), a type of viral infection. If herpes simplex virus (HSV) is the cause, multiple tender vesicles may be observed (see Figure 6).
- Acute paronychia mainly affects children and adolescents
- The causative organisms are usually Staphylococcus aureus or streptococci, and, less commonly, pseudomonas or proteus species
- Organisms enter through a break in the epidermis resulting from trauma to a nail fold, loss of the cuticle, or chronic irritation (eg, resulting from water and detergents). Biting or sucking fingers can also predispose to infection. In toes, infection often begins in an ingrown toenail
- Occasionally the infection can be viral, due to either the herpes simplex virus (HSV), or orf virus. In cases of herpes simplex virus (HSV) infection (a herpetic whitlow), the presentation is that of vesicles, often grouped together. Such episodes can be recurrent.
Figure 5. Acute paronychia

Figure 6. Herpetic whitlow (herpes simplex virus (HSV) infection)

Chronic paronychia
Chronic paronychia is a gradual process. Chronic paronychia may start in one nail fold, particularly the proximal nail fold, but often spreads laterally and to several other fingers. Each affected nail fold is swollen and lifted off the nail plate. This allows entry of organisms and irritants.The affected skin may be red and tender from time to time, and sometimes a little pus (white, yellow or green) can be expressed from under the cuticle.
Chronic paronychia is an inflammatory dermatosis of the nail folds that results from irritant dermatitis rather than an infection 8, which causes retraction of the periungual tissues with resultant secondary effects on the nail matrix, nail growth and soft‐tissue attachments. Chronic paronychia occurs most often in people whose hands are constantly or often exposed to moisture. Common irritants include acids, alkalis, or other chemicals commonly used by housekeepers, dishwashers, bartenders, laundry workers, florists, bakers, and swimmers. Once the protective nail barrier is disrupted, repeated exposure to irritants may result in chronic inflammation.
Although uncomfortable, chronic paronychia is generally less painful than acute paronychia. Chronic paronychia often results from contact dermatitis, a type of skin inflammation caused by exposure to chemicals that are irritating to the skin. People with chronic paronychia may have periodic, painful flare-ups. This type of nail infection may be complicated by the addition of a fungal infection, commonly due to a type of yeast called Candida, or bacterial infection, and this may lead to abnormal nail growth.
Chronic paronychia distribution
- Any finger may be involved, although it is most frequently the index and middle fingers of the right hand and the middle finger of the left
- Toenails can also be affected
Chronic paronychia morphology
- Chronic paronychia begins as a slight erythematous swelling of the nail folds
- The cuticle is lost and pus may collect beneath the nail fold
- Repeated acute exacerbations impact on the nail matrix, which leads to the development of numerous irregular transverse nail ridges
- The nail may become discolored
- In longstanding cases the nail may reduce in size
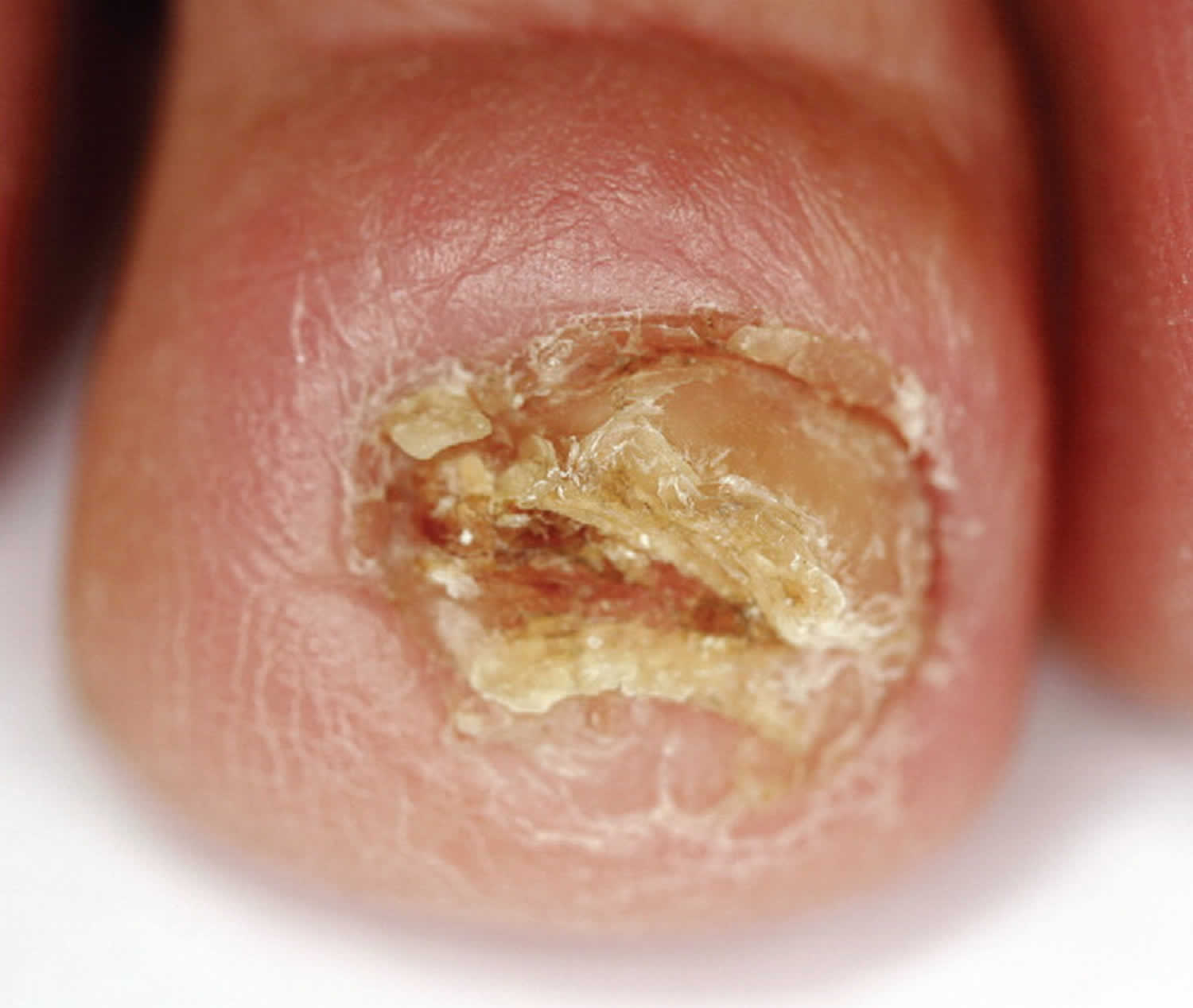
Figure 7. Chronic paronychia

Figure 8. Chronic paronychia with typical loss of cuticle and transverse ridges (Beau lines)

Chronic paronychia causes
- Chronic paronychia is predominantly a disease of domestic and catering workers, bar staff and fishmongers, where water and/or chemicals cause a contact irritant dermatitis. Handling of wet foods represents a particular hazard, as these often combine several predisposing factors including wet working conditions, a cold environment and irritation from the food itself
- Other causes include an underling inflammatory dermatosis such as atopic eczema or psoriasis, and finger or thumb sucking in children.
- Yeast infections, such as candida, can be associated as either a primary or secondary event. Dermatophytic paronychia is rare.
- Several classes of medications can cause chronic paronychia: retinoids, protease inhibitors (4% of users), antiepidermal growth factor receptor antibodies (17% of users), and several classes of chemotherapeutic agents (35% of users) 9. The effect can be immediate or delayed up to 12 months.
Is chronic paronychia hereditary?
No
Chronic paronychia symptoms
- the skin may be red and shiny around the nail
- tenderness of the skin around the nail
- swelling at the base or sides of one or more nails
- pus-filled blisters, white, yellow or even greenish
- changes in nail shape, color, or texture (ridges). This can be apparent for many months after the paronychia has cleared as the nail slowly grows out.
- detachment of the nail
How is chronic paronychia diagnosed?
Chronic paronychia is diagnosed clinically based on symptom duration of at least six weeks, a positive exposure history, and clinical findings consistent with nail dystrophy 10. The red swollen nail folds of chronic paronychia give it a characteristic look so your doctor will be able to make the diagnosis without laboratory tests. The cuticle may be totally absent, and Beau lines (deep side-to-side grooves in the nail that represent interruption of nail matrix maturation) may be present 11 (see Figure 8). Multiple digits typically are involved. If only a single digit is affected, the possibility of malignancy, such as squamous cell cancer, must be considered (see Figure 9) 10. The presence of pus and redness may indicate an acute exacerbation of a chronic process.
Chronic paronychia should not be confused with ringworm (tinea) infection, which causes whitish thicken-ing of the nail and nailbed, nail thickening and discoloration. Other conditions such as psoriasis and lichen planus can also affect the nails and cause ridging and discoloration.
Your doctor may check your urine for sugar to make sure you are not diabetic and also take a swab from the infected nail fold to be tested in the laboratory, which will often grow a mixture of bacteria and yeasts, rather than just a single type.
Acute and chronic paronychia are largely distinguished from each other by the speed of onset and the duration of the infection.
Figure 9. Squamous cell carcinoma of the nail
Can chronic paronychia be cured?
Yes – but remember that just as chronic paronychia starts slowly, it also clears slowly.
Who gets paronychia?
Acute paronychia can affect anyone. However, it is more likely to follow a break in the skin, especially between the proximal nail fold/cuticle and the nail plate. For example:
- If the nail is bitten (onychophagia) or the nail-fold is habitually picked
- In infants that suck their fingers or thumbs
- Following manicuring
- Ingrown toenails (onychocryptosis)
- On application of sculptured or artificial fingernails
- Treatment with oral retinoid that dries the skin (acitretin, isotretinoin)
- Other drugs, including epidermal growth factor receptor and BRAF inhibitors (vemurafenib, dabrafenib)
Chronic paronychia mainly occurs in people with hand dermatitis, or who have constantly cold and wet hands, such as:
- Dairy farmers
- Fishermen
- Bar tenders
- Cleaners
- Housewives
- People with poor circulation
Acute and chronic skin infections tend to be more frequent and aggressive in patients with diabetes or chronic debility, or that are immune suppressed by drugs or disease.
Paronychia causes
Paronychia happens when the skin around the nail gets irritated or injured. Germs get into the skin and cause an infection. These germs can be bacteria or a fungus. Paronychia is more common in adult women and in people who have diabetes. People who have weak immune systems are also at higher risk of getting paronychia. This includes people who must take medicine after having an organ transplant or people who are infected with HIV.
Acute paronychia is usually due to bacterial infection with Staphylococcus aureus (which may be multiresistant), Streptococcus pyogenes, pseudomonas, or other bacterial pathogens. It can also be due to the cold sore virus, Herpes simplex, and the yeast, Candida albicans.
Often, the skin is injured because of biting, chewing, or picking at the nails. It can also be caused by pulling hangnails or sucking on fingers. An ingrown toenail can also cause paronychia.
The cause or causes of chronic paronychia are not fully understood. In many cases, it is due to dermatitis of the nail fold. Often several different micro-organisms can be cultured, particularly Candida albicans and the Gram negative bacilli, pseudomonas.
Moisture allows certain germs, such as candida (a type of fungus) and bacteria to grow. People whose hands may be wet for long periods of time are at higher risk for chronic paronychia. These may include bartenders, dishwashers, food handlers, or housecleaners. Chronic paronychia may also be caused by irritant dermatitis, a condition that makes skin red and itchy. Once the skin is irritated, germs can take hold and cause an infection.
Risk factors for paronychia
- Accidental trauma
- Artificial nails
- Manicures
- Manipulating a hangnail (i.e., shred of eponychium)
- Occupational trauma (e.g., bartenders, housekeepers, dishwashers, laundry workers)
- Onychocryptosis (i.e., ingrown nails)
- Onychophagia (nail biting)
Paronychia prevention
The best away to avoid acute paronychia is to take good care of your nails 12.
- Avoid nail trauma, biting, picking, and manipulation, and finger sucking.
- Don’t bite or pick your nails.
- Keep your nails trimmed and smooth.
- Keep nails short.
- Avoid cutting nails too short.
- Don’t scrape or trim your cuticles, as this can injure the skin.
- Use clean nail clippers or scissors.
- Apply moisturizing lotion after hand washing.
- Avoid chronic prolonged exposure to contact irritants and moisture (including detergent and soap).
- Improve glycemic control in patients with diabetes mellitus.
- Keep affected areas clean and dry.
- Use rubber gloves, preferably with inner cotton glove or cotton liners when exposed to moisture and/or irritants.
You can avoid chronic paronychia by keeping your hands dry and free from chemicals. Wear gloves when working with water or harsh chemicals. Change socks at least every day, and do not wear the same shoes for two days in a row. This allows them to dry out completely.
Paronychia symptoms
Bacterial nail infection most often affects the proximal nail fold of the fingers and less commonly affects the toes.
- Acute paronychia: The proximal nail fold is red, swollen, painful, and may contain pus. Usually one nail is affected.
- Chronic paronychia: The proximal nail fold is swollen, red, and has no cuticle (the strip of hardened skin at the base and sides of a fingernail or toenail). One or more nails may be affected.
Typically, paronychia begins with pain, swelling and redness around the base or the sides of the nail. Acute paronychia can cause pus-filled pockets (abscesses) to form.
Chronic paronychia may cause the cuticle to break down. This type of paronychia may eventually cause the nail to separate from the skin. The nail may become thick, hard, and deformed.
Paronychia caused by bacteria can get worse quickly. Fungus-caused paronychia typically gets worse slowly over time.
What are the complications of paronychia?
Acute paronychia can spread to cause a serious hand infection (cellulitis) and may involve underlying tendons (infectious tendonitis).
Systemic complications of acute paronychia are rare but may include
- Abscess formation
- Permanent deformation of the nail plate
- Systemic fever/chills
- Development of red streaks along the skin
- Development of cellulitis or erysipelas
- Joint pain
- General ill feeling
- Flu-like symptoms
- Osteomyelitis
- Flexor tenosynovitis
The main complication of chronic paronychia is nail dystrophy. It is often associated with distorted, ridged nail plates. They may become yellow or green/black and brittle. After recovery, it takes up to a year for the nails to grow back to normal.
How is paronychia diagnosed?
Paronychia is a clinical diagnosis, often supported by laboratory evidence of infection. Your doctor can diagnose paronychia with a simple physical exam. Special tests aren’t usually necessary. Your doctor may want to send a sample of fluid or pus to a laboratory. There they can identify the bacteria or fungus that is causing the infection.
- Gram stain microscopy may reveal bacteria
- Potassium hydroxide microscopy may reveal fungi
- Bacterial culture
- Viral swabs
- Tzanck smears
- Nail clippings for culture (mycology).
How to treat paronychia
Treatment for paronychia depends on how severe the infection is. If you have acute paronychia, soaking the infected nail in warm water 3 to 4 times a day can help reduce pain and swelling. It should heal up in a few days. If the infection is very painful, doesn’t get better with home care, or has a pus-filled abscess, you may need to see your doctor. Your doctor may prescribe antibiotics if your paronychia is caused by bacteria. He or she may prescribe antifungal medicines if your infection is caused by a fungus.
If you have an abscess, your doctor may need to drain it. Your doctor will numb the area, separate the skin from the base or sides of the nail, and drain the pus.
If you have chronic paronychia, it is important to keep your nails dry and protect them from harsh chemicals. You may need to wear gloves or use a skin-drying cream to protect skin from moisture. You may need an antifungal medicine or antibiotic, depending on what is causing the infection.
Paronychia caused by a fungus can be hard to get rid of. Be patient and follow your doctor’s recommendations. If the infection does not clear up, be sure to tell your doctor.
Most of the time, paronychia responds well to treatment. But sometimes complications can happen.
Rarely, paronychia can cause permanent damage to your nail. If you have diabetes, there’s a risk that paronychia could spread to deeper tissues and bones, or into the bloodstream and other parts of the body. In extreme cases of deep infection, paronychia can result in the loss of fingers, toes, or limbs.
Be sure to contact your doctor if:
- Treatment doesn’t help your symptoms
- You have a fever or chills
- Red streaks appear on your skin, running from the infected area toward your body (for example, up your foot from your toes or up your hand or wrist from your fingers)
- You have joint or muscle pain
Acute paronychia treatment
Treatment of acute paronychia is based on the severity of inflammation and the presence of an abscess. If only mild inflammation is present and there is no overt cellulitis, treatment consists of warm soaks, topical antibiotics with or without topical steroids, or a combination of topical therapies. Warm soaks have been advocated to assist with spontaneous drainage.14 Although they have not been extensively studied, Burow solution (aluminum acetate solution) and vinegar (acetic acid) combined with warm soaks have been used for years as a topical treatment. Burow solution has astringent and antimicrobial properties and has been shown to help with soft tissue infections.15 Similarly, 1% acetic acid has been found effective for treating multidrug-resistant pseudomonal wound infections because of its antimicrobial properties.16 Soaking can lead to desquamation, which is normal.17 Topical antibiotics for paronychia include mupirocin (Bactroban), gentamicin, or a topical fluoroquinolone if pseudomonal infection is suspected. Neomycin-containing compounds are discouraged because of the risk of allergic reaction (approximately 10%).18 The addition of topical steroids decreases the time to symptom resolution without additional risks.19
If an abscess is present, it should be opened to facilitate drainage. Soaking combined with other topical therapies can be tried, but if no improvement is noted after two to three days or if symptoms are severe, the abscess must be mechanically drained5 (Figure 44). No randomized controlled trials have compared methods of drainage, and treatment should be individualized according to the clinical situation and skill of the physician. An instrument such as a nail elevator or hypodermic needle can be inserted at the junction of the affected nail fold and nail.20
- The affected digit should be soaked in warm water several times daily
- Topical antiseptics, e.g., Fucidin cream, may be used for localized, minor infection
- An oral antistaphylococcal antibiotic may be necessary for more severe or prolonged bacterial infection; often a tetracycline such as doxycycline is prescribed.
- Surgical incision and drainage may be required for abscess followed by irrigation and packing with gauze.
- Rarely, the nail must be removed to allow pus to drain.
Paronychia antibiotics
The use of oral antibiotics should be limited 13. Patients with overt cellulitis and possibly those who are immunocompromised or severely ill may warrant oral antibiotics 14. When antibiotics are required, therapy should be directed against the most likely pathogens. If there are risk factors for oral pathogens, such as thumb-sucking or nail biting, medications with adequate anaerobic coverage should be used. Table 1 lists common pathogens and suggested antibiotic options 8, but local community resistance patterns should be considered when choosing specific agents 15.
Recurrent acute paronychia can progress to chronic paronychia. Therefore, patients should be counseled to avoid trauma to the nail folds. Systemic diseases such as psoriasis and eczema can cause acute paronychia; in these cases, treatment should be directed at the underlying cause.
Table 1. Treatment Options for Typical Pathogens Associated with Acute Paronychia
| Pathogen | Antibiotic options |
|---|---|
Gram-negative aerobes | |
Fusobacterium | Amoxicillin/clavulanate (Augmentin), clindamycin, fluoroquinolones |
Pseudomonas | Ciprofloxacin |
Gram-negative anaerobe | |
Bacteroides | Amoxicillin/clavulanate, clindamycin, fluoroquinolones |
Gram-negative facultative anaerobes | |
Eikenella | Cefoxitin |
Enterococcus | Amoxicillin/clavulanate |
Klebsiella | Trimethoprim/sulfamethoxazole, fluoroquinolones |
Proteus | Amoxicillin/clavulanate, fluoroquinolones |
Gram-positive aerobes | |
Staphylococcus | Cephalexin (Keflex) |
For suspected methicillin-resistant Staphylococcus aureus (MRSA) infections: clindamycin, doxycycline, trimethoprim/sulfamethoxazole | |
Streptococcus | Cephalexin |
Footnote: Local community resistance patterns should always be considered when choosing antibiotics.
[Source 16 ]Table 2. Commonly Used Medications for Acute and Chronic Paronychia
| Drug | Typical dosage | Comments | ||
|---|---|---|---|---|
Antibiotics (oral) | ||||
Amoxicillin/clavulanate (Augmentin)* | 500 mg/125 mg orally three times daily for seven days | Dosage adjustment may be necessary in patients with renal impairment; cross-sensitivity documented with cephalosporins; diarrhea may occur | ||
or | ||||
875 mg/125 mg orally twice daily for seven days | ||||
Clindamycin (Cleocin)* | 150 to 450 mg orally three or four times daily (not to exceed 1.8 g daily) for seven days | Adjust dosage in patients with severe hepatic dysfunction; associated with severe and possibly fatal colitis; inform patient to report severe diarrhea immediately | ||
Trimethoprim/sulfamethoxazole (TMP/SMX; Bactrim, Septra)* | 160 mg/800 mg orally twice daily for seven days | High doses may cause bone marrow depression; discontinue therapy if significant hematologic changes occur; caution in folate or glucose-6-phosphate dehydrogenase deficiency | ||
Antibiotics (topical) | ||||
Bacitracin/neomycin/polymyxin B ointment (Neosporin) | Three times daily for five to 10 days | Overgrowth of nonsusceptible organisms with prolonged use | ||
Gentamicin ointment | Three or four times daily for five to 10 days | — | ||
Mupirocin ointment (Bactroban) | Two to four times daily for five to 10 days | Avoid contact with eyes; may irritate mucous membranes; resistance may result with prolonged use | ||
Antifungal agents (oral) | ||||
Fluconazole (Diflucan) | 100 mg orally once daily for seven to 14 days | Hepatotoxicity and QT prolongation may occur | ||
Itraconazole (Sporanox) | 200 mg orally twice daily for seven days | Antacids may reduce absorption; edema may occur with coadministration of calcium channel blockers; rhabdomyolysis may occur with coadministration of statins; inhibition of cytochrome P450 hepatic enzymes may cause increased levels of many drugs | ||
Nystatin (Mycostatin) 200,000-unit pastilles | One or two pastilles four times daily for seven to 14 days | Adverse effects include nausea, vomiting, and diarrhea | ||
Antifungal agents (topical) | ||||
Ciclopirox topical suspension (Loprox TS) | Twice daily until clinical resolution (one month maximum) | Avoid contact with eyes and mucous membranes | ||
Clotrimazole cream (Lotrimin) | Three times daily until clinical resolution (one month maximum) | Avoid contact with eyes; if irritation or sensitivity develops, discontinue use and begin appropriate therapy | ||
Econazole cream (Spectazole) | Three or four times daily until clinical resolution (one month maximum) | Avoid contact with eyes; if irritation or sensitivity develops, discontinue use and begin appropriate therapy | ||
Ketoconazole cream (Nizoral; brand no longer available in the United States) | Once or twice daily until clinical resolution (one month maximum) | Avoid contact with eyes; if irritation or sensitivity develops, discontinue use and begin appropriate therapy | ||
Nystatin cream | Three times daily until clinical resolution (one month maximum) | Avoid contact with eyes; if irritation or sensitivity develops, discontinue use and begin appropriate therapy | ||
Antiviral agents for herpetic whitlow | ||||
Acyclovir (Zovirax) † | 200 mg orally five times daily for 10 days | Nausea, vomiting, rash, deposition in renal tubules, and central nervous system symptoms may occur | ||
Famciclovir (Famvir)† | 250 mg orally twice daily for 10 days | Dosage adjustment recommended in patients with renal impairment | ||
Valacyclovir (Valtrex)† | 500 mg orally twice daily for 10 days | Associated with onset of hemolytic uremic syndrome | ||
Corticosteroids (topical) | ||||
Betamethasone 0.05% cream (Diprolene) | Twice daily for one to two weeks | If infection develops and is not responsive to antibiotic treatment, discontinue use until infection is controlled | ||
Betamethasone valerate 0.1% solution or lotion (Beta-Val) | Once or twice daily for one to two weeks | Prolonged therapy over large body surface areas may suppress adrenal function; if infection develops, discontinue use until infection is controlled | ||
Combination antifungal agent and corticosteroid | ||||
Nystatin and triamcinolone cream (Mytrex; brand no longer available in the United States) | Two or three times daily until the cuticle has regrown | Check precautions for both components | ||
Footnote:
*— Active against non-multiresistant methicillin-resistant Staphylococcus aureus strains.
†— Use with caution in patients with renal failure and in those taking other nephrotoxic drugs.
[Source 17 ]Chronic paronychia treatment
Usually an antibacterial and/or antifungal cream or lotion improves the condition within a few weeks. In addition, a steroid cream may be prescribed to speed up improvement.
Treatment of chronic paronychia consists of stopping the source of irritation, controlling inflammation, and restoring the natural protective barrier 18. Topical anti-inflammatory agents, steroids, or calcineurin inhibitors are the mainstay of therapy 19. In a randomized, unblinded, comparative study, tacrolimus 0.1% (Protopic) was more effective than betamethasone 17-valerate 0.1% 19. In severe or refractory cases, more aggressive treatments may be required to stop the inflammation and restore the barrier. If the Swiss roll technique is used, the nail bed will need to be exposed for a longer duration (seven to 14 days) than for acute cases (two to three days) 20.
If a medication is the cause, the physician and patient must decide whether the adverse effects are acceptable for the therapeutic effect of the drug. Discontinuing the medication should reverse the process and allow healing. Doxycycline has been found effective for treatment of paronychia caused by antiepidermal growth factor receptor antibodies 10. A case report describes successful treatment with twice-daily application of a 1% solution of povidone/iodine in dimethyl sulfoxide until symptom resolution in patients with chemotherapy-induced chronic paronychia 21. Zinc deficiency is known to cause nail plate abnormalities and chronic paronychia; treatment with 20 mg of supplemental zinc per day is helpful 22. It is important to inform the patient that the process can take weeks to months to restore the natural barrier.
Manage predisposing factors:
- Avoid any manipulation of the nail such as manicuring, or finger sucking.
- Avoid frequent hand-wetting, manicures and irritating sub-stances.
- Patients involved in wet work should be advised to wear rubber or plastic gloves, preferably with inner cotton gloves or cotton liners.
- Avoid the use of soaps and detergents, instead use a soap-substitute eg Dermol Wash ® Cutaneous Emulsion
- Emollient creams should be applied on a regular basis.
- Underlying conditions such as diabetes and poor circulation must also be treated to help improve paronychia.
Treatment should focus on the dermatitis and any microbes grown on culture 23.
- Trimovate ® cream applied twice daily can be useful during a flare-up as it combines a topical steroid with antiseptic and antifungal therapies. Other options include Daktacort ® cream, which contains a weaker steroid than Trimovate ® cream, or, occasionally a more potent topical steroid may be required for a short duration if the inflammation is more marked.
- Topical corticosteroid ointment is applied for 2–4 weeks and repeated for flares.
- Tacrolimus ointment is an alternative when dermatitis is not responding to routine management 24.
- Intralesional steroid injections are sometimes used in resistant cases.
- Antiseptics or antifungal lotions or solutions may be applied for several months.
- If creams or lotions are not successful antibiotic or antifungal tablets by mouth may be needed.
- In more troublesome cases, where a swab confirms Candida albicans then a short course of an oral antifungal therapy, such as itraconazole or fluconazole, may be required
Surgery is not usually needed, but sometimes a doctor may make a small cut and drain the area to help clear the condition if medication treatment fails.
Other management
- Patients with diabetes and vascular disease with toenail paronychia infections should be examined for signs of cellulitis.
- Surgical excision of the proximal nail fold may be necessary.
- Eponychial marsupialisation involves surgical removal of a narrow strip of skin next to the nail, to reduce the risk of infection 25.
- Swiss roll technique has the advantage of retaining the nail plate and quicker recovery 26.
Chronic paronychia finger self-care
- You should keep your hands as warm and dry as possible; you will not get better until you do this.
- Avoid wet work, or wear gloves for any tasks using water, irritants and chemicals, including shampooing and washing up.
- Keep fingernails scrupulously clean.
- Wash after dirty work with soap and water, rinse off and dry carefully.
- Apply emollient hand cream frequently – dimeticone barrier creams may help.
- Avoid biting your nails, manicuring your nail folds, and pushing back the cuticles.
- Do not use nail varnish until the condition has been treated.
- Occasionally a change of occupation may be worth thinking about.
- Do not apply false nails until the condition is resolved.
Paronychia prognosis
- Acute paronychia usually clears completely in a few days, and rarely recurs in healthy individuals.
- Chronic paronychia may persist for months or longer, and can recur in predisposed individuals. Chronic paronychia responds slowly to treatment. Resolution usually takes several weeks or months, but the slow improvement rate should not discourage physicians and patients. In mild to moderate cases, nine weeks of drug treatment usually is effective. In recalcitrant cases, en bloc excision of the proximal nail fold with nail avulsion may result in significant cure rates. Successful treatment outcomes also depend on preventive measures taken by the patient (e.g., having a water barrier in the nail fold). If the patient is not treated, sporadic, self-limiting, painful episodes of acute inflammation should be expected as the result of continuous penetration of various pathogens.
- Habif TP. Nail diseases. In: Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 4th ed. Edinburgh, UK: Mosby; 2004:871–872.[↩]
- Daniel CR, Daniel MP, Daniel J, Sullivan S, Bell FE. Managing simple chronic paronychia and onycholysis with ciclopirox 0.77% and an irritant-avoidance regimen. Cutis. 2004;73(1):81–85.[↩]
- Tosti A, Piraccini BM, Ghetti E, Colombo MD. Topical steroids versus systemic antifungals in the treatment of chronic paronychia: an open, randomized double-blind and double dummy study. J Am Acad Dermatol. 2002;47(1):73–76.[↩][↩]
- Baran R. Common-sense advice for the treatment of selected nail disorders. J Eur Acad Dermatol Venereol. 2001;15(2):97–102.[↩]
- de Berker D, Baran R, Dawber RP. Disorders of the nails. In: Burns T, Breathnach S, Cox N, Griffiths S, eds. Rook’s Textbook of Dermatology. 7th ed. Oxford, UK: Black-well Science; 2005:62.1.[↩]
- Bednar MS, Lane LB. Eponychial marsupialization and nail removal for surgical treatment of chronic paronychia. J Hand Surg [Am]. 1991;16(2):314–317.[↩][↩]
- Shu KY, Kindler HL, Medenica M, Lacouture M. Doxycycline for the treatment of paronychia induced by the epidermal growth factor receptor inhibitor cetuximab. Br J Dermatol. 2006;154(1):191–192.[↩]
- Chang P. Diagnosis using the proximal and lateral nail folds. Dermatol Clin. 2015;33(2):207–241.[↩][↩]
- Capriotti K, Capriotti JA, Lessin S, et al. The risk of nail changes with taxane chemotherapy: a systematic review of the literature and meta-analysis. Br J Dermatol. 2015;173(3):842–845.[↩]
- Rigopoulos D, Larios G, Gregoriou S, Alevizos A. Acute and chronic paronychia. Am Fam Physician. 2008;77(3):339–346.[↩][↩][↩][↩]
- Tully AS, Trayes KP, Studdiford JS. Evaluation of nail abnormalities. Am Fam Physician. 2012;85(8):779–787[↩]
- Rigopoulos D, Larios G, Gregoriou S, Alevizos A. Acute and chronic paronychia. Am Fam Physician. 2008;77(3):343.[↩]
- Raff AB, Kroshinsky D. Cellulitis: a review. JAMA. 2016;316(3):325–337.[↩]
- Duong M, Markwell S, Peter J, Barenkamp S. Randomized, controlled trial of antibiotics in the management of community-acquired skin abscesses in the pediatric patient. Ann Emerg Med. 2010;55(5):401–407.[↩]
- Daum RS. Clinical practice. Skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus [published correction appears in N Engl J Med. 2007;357(13):1357]. N Engl J Med. 2007;357(4):380–390.[↩]
- Acute and Chronic Paronychia. Am Fam Physician. 2017 Jul 1;96(1):44-51. https://www.aafp.org/afp/2017/0701/p44.html[↩]
- Acute and Chronic Paronychia. Am Fam Physician. 2008 Feb 1;77(3):339-346. https://www.aafp.org/afp/2008/0201/p339.html[↩]
- Shafritz AB, Coppage JM. Acute and chronic paronychia of the hand. J Am Acad Orthop Surg. 2014;22(3):165–174.[↩]
- Rigopoulos D, Gregoriou S, Belyayeva E, Larios G, Kontochristopoulos G, Katsambas A. Efficacy and safety of tacrolimus ointment 0.1% vs. betamethasone 17-valerate 0.1% in the treatment of chronic paronychia: an unblinded randomized study. Br J Dermatol. 2009;160(4):858–860.[↩][↩]
- Pabari A, Iyer S, Khoo CT. Swiss roll technique for treatment of paronychia. Tech Hand Up Extrem Surg. 2011;15(2):75–77.[↩]
- Capriotti K, Capriotti JA. Chemotherapy-associated paronychia treated with a dilute povidone-iodine/dimethylsulfoxide preparation. Clin Cosmet Investig Dermatol. 2015;8:489–491.[↩]
- Iorizzo M. Tips to treat the 5 most common nail disorders: brittle nails, onycholysis, paronychia, psoriasis, onychomycosis. Dermatol Clin. 2015;33(2):175–183.[↩]
- Relhan, Vineet, et al. Management of chronic paronychia. Indian journal of Dermatology 59.1 (2014): 15.[↩]
- Rigopoulos D, Gregoriou S, Belyayeva E, Larios G, Kontochristopoulos G, Katsambas A. Efficacy and safety of tacrolimus ointment 0.1% vs. betamethasone 17-valerate 0.1% in the treatment of chronic paronychia: An unblinded randomized study. Br J Dermatol. 2009;160:858–60.[↩]
- Bednar MS, Lane LB. Eponychial marsupialization and nail removal for surgical treatment of chronic paronychia. J Hand Surg Am 1991;16:314-7.[↩]
- Pabari A, Iyer S, Khoo CT. Swiss roll technique for treatment of paronychia. Tech Hand Surg 2011;15:75-7[↩]





{kind=link}