
Contents
- What is PCOS
- Who gets PCOS?
- Getting pregnant with PCOS
- Treatment options for PCOS if you want to get pregnant
- You desire fertility and you have normal weight
- You desire fertility and you are overweight
- How do I know if I’m overweight or obese?
- What effect can weight loss have on women with PCOS?
- What can be done to increase the chances of pregnancy for women with PCOS?
- How IVF as a treatment for infertility procedure works
- How does PCOS affect pregnancy?
- Treatment options for PCOS if you want to get pregnant
- PCOS signs and symptoms
- PCOS causes
- PCOS diagnosis
- PCOS treatment
- PCOS diet
What is PCOS
PCOS also known as polycystic ovary syndrome or polycystic ovarian syndrome, is a common hormonal condition that affects up to 1 in 5 to 10 girls and women in their reproductive years or of childbearing age. PCOS may cause disruptions to the menstrual cycle, skin and hair changes, as well as cysts on your ovaries. Women with PCOS have a hormonal imbalance and metabolism problems that may affect their overall health and appearance. PCOS is also a common and treatable cause of infertility.
PCOS is one of the leading causes of infertility, yet many women do not know they have it – up to 70% of women with PCOS remain undiagnosed.
Women with PCOS produce high levels of male hormones (androgens) from their ovaries. These male hormones affect the menstrual cycle and many other parts of your body. Women with PCOS often have enlarged ovaries. Their ovaries may have many cysts on them, which is where the name comes from. With PCOS, the egg in your ovaries may not develop as it should or it may not be released during ovulation as it should be.
PCOS can cause missed or irregular menstrual periods. Irregular periods can lead to:
- Infertility (inability to get pregnant). In fact, PCOS is one of the most common causes of infertility in women.
- Development of cysts (small fluid-filled sacs) in the ovaries
Women with PCOS can also have a wide range of symptoms. The most visible polycystic ovary syndrome symptoms are acne, excessive hair on the upper lip, stomach and back, thinning hair on the head and even baldness. Problems which are not so visible include diabetes, high cholesterol levels, heart disease, difficulty falling pregnant and a tendency to gain weight.
PCOS diagnosis is based on your doctor talking to you, examining you and possibly asking you to have blood tests and an ultrasound of the pelvis, ovaries and uterus.
The cause of PCOS is unknown but there appears to be connections with family history, insulin resistance and lifestyle (e.g., obesity or being overweight) or environment. PCOS is related to abnormal hormone levels in the body, including high levels of insulin. Insulin is a hormone that controls sugar levels in the body. Many women with PCOS are resistant to the action of insulin in their body and produce higher levels of insulin to overcome this. This contributes to the increased production and activity of hormones such as testosterone. Being overweight or obese also increases the amount of insulin your body produces.
Polycystic ovarian syndrome (PCOS) can’t be cured, but you and your doctor can manage many of the symptoms.
The treatment you will have depends on the main problems you face. It can involve medicines, cosmetic treatments and having a healthy lifestyle with a healthy diet and regular exercise.
The first step in managing PCOS when you are overweight is to get regular exercise and eat heart-healthy foods. This can help lower blood pressure and cholesterol and reduce the risk of diabetes and heart disease. Try to fit in moderate activity and/or vigorous activity on a regular basis. Walking is a great exercise that most people can do. Eat a heart-healthy diet. In general, this diet has lots of vegetables, fruits, nuts, beans, and whole grains. It also limits foods that are high in saturated fat, such as meats, cheeses, and fried foods. If you have blood sugar problems, try to eat about the same amount of carbohydrate at each meal. A registered dietitian can help you make a meal plan.
Most women who have PCOS can benefit from losing weight. Even losing 10 lb (4.5 kg) may help get your hormones in balance and regulate your menstrual cycle. PCOS can make it hard to lose weight, so work with your doctor to make a plan that can help you succeed. Additionally, if you smoke, consider quitting. Women who smoke have higher androgen levels that may contribute to PCOS symptoms. Smoking also increases the risk for heart disease.
Will my PCOS symptoms go away at menopause?
Yes and no. PCOS affects many systems in your body. Many women with PCOS find that their menstrual cycles become more regular as they get closer to menopause. However, their PCOS hormonal imbalance does not change with age, so they may continue to have symptoms of PCOS.
Also, the risks of PCOS-related health problems, such as diabetes, stroke, and heart attack, increase with age. These risks may be higher in women with PCOS than those without.
Who gets PCOS?
Between 5% and 10% of women between 15 and 44, or during the years you can have children, have PCOS 1. Most women find out they have PCOS in their 20s and 30s, when they have problems getting pregnant and see their doctor. But PCOS can happen at any age after puberty 2.
Women of all races and ethnicities are at risk of PCOS. Your risk of PCOS may be higher if you have obesity or if you have a mother, sister, or aunt with PCOS.
Getting pregnant with PCOS
Having PCOS does not mean you can’t get pregnant. PCOS is one of the most common, but treatable, causes of infertility in women. In women with PCOS, the hormonal imbalance interferes with the growth and release of eggs from the ovaries (ovulation). If you don’t ovulate, you can’t get pregnant.
Your doctor can talk with you about ways to help you ovulate and to raise your chance of getting pregnant.
“Infertility” is a term used to describe the inability of a couple to get pregnant or the inability of a woman to carry a pregnancy to term.
Infertility is defined clinically as not being able to achieve pregnancy after 1 year of having regular, unprotected intercourse, or after 6 months if the woman is older than 35 years of age 3.
The term “infertility” also is used to describe the condition of women who are able to get pregnant but unable to carry a pregnancy to term because of miscarriage (sometimes called clinical spontaneous abortion), recurrent pregnancy loss, stillbirth, or other problems 4.
Recurrent pregnancy loss is considered distinct from infertility. Although there may be some overlap, the causes of pregnancy loss, recurrent pregnancy loss, and stillbirth are often different from the causes of infertility.
Treatment options for PCOS if you want to get pregnant
You have several options to help your chances of getting pregnant if you have PCOS:
- Losing weight. If you have overweight or obesity, losing weight through healthy eating, including eating the right amount of calories for you, and regular physical activity can help make your menstrual cycle more regular and improve your fertility. Women with PCOS who lose weight are more likely to have restored ovulation and improved pregnancy rates 5.
- Medicine. After ruling out other causes of infertility in you and your partner, your doctor might prescribe medicine to help you ovulate, such as clomiphene (Clomid). Clomifene encourages the monthly release of an egg from the ovaries (ovulation). Studies have shown that in women with PCOS, those who took clomiphene were six times more likely to get pregnant than those who did not.
- If clomiphene (Clomid) is unsuccessful in encouraging ovulation, another medication called metformin may be recommended. Metformin is often used to treat type 2 diabetes, but it can also lower insulin and blood sugar levels in women with PCOS. As well as stimulating ovulation, encouraging regular monthly periods and lowering the risk of miscarriage, metformin can also have other, long-term health benefits, such as lowering high cholesterol levels and reducing the risk of heart disease. Metformin isn’t FDA approved for treating PCOS in the US, but because many women with PCOS have insulin resistance, it can be used “off-label” to encourage fertility and control the symptoms of PCOS, but so far there is no evidence that metformin treatment increases the rate of pregnancy in women with PCOS. Possible side effects of metformin include nausea, vomiting, stomach pain, diarrhea and loss of appetite.
- A combination of clomiphene and metformin. In women with PCOS who do not respond to clomiphene by itself, adding metformin may slightly increase the rate of pregnancy.
- Letrozole and tamoxifen are sometimes used to stimulate ovulation instead of clomiphene. These medications can also be used for treating breast cancer. Use of letrozole, also known as Femara, for fertility treatment is “off-label” to improve the receptivity of the uterus lining in women with PCOS 6. In other words, although letrozole is licensed for treating breast cancer, it doesn’t have a license for treating PCOS. Doctors sometimes use an unlicensed medication if they think it’s likely to be effective and the benefits of treatment outweigh any associated risks.
- If you’re unable to get pregnant despite taking oral medications, a different type of medication called gonadotrophins may be recommended. Gonadotropins and hCG (human chorionic gonadotropin) are given by injection and there’s a higher risk that they may overstimulate your ovaries and lead to multiple pregnancies. An alternative to gonadotrophins is a surgical procedure called laparoscopic ovarian drilling (see below). This treatment can be as effective as using gonadotrophins, but it doesn’t increase your risk of multiple pregnancies.
- In vitro fertilization (IVF). IVF may be an option if medicine does not work. In IVF, your egg is fertilized with your partner’s sperm in a laboratory and then placed in your uterus to implant and develop. Compared to medicine alone, IVF has higher pregnancy rates and better control over your risk of having twins and triplets (by allowing your doctor to transfer a single fertilized egg into your uterus).
- Surgery. A minor surgical procedure called laparoscopic ovarian drilling may be a treatment option for fertility problems associated with PCOS, usually only if the other options do not work. The outer shell (called the cortex) of ovaries is thickened in women with PCOS and thought to play a role in preventing spontaneous ovulation. Ovarian drilling is a surgery in which the doctor makes a few holes in the surface of your ovary using lasers or a fine needle heated with electricity, it can stimulate ovulation in women with PCOS. Surgery usually restores ovulation, but only for 6 to 8 months. The procedure is usually done through a small incision near the belly button, with the woman under general anesthesia. A laser or electrocautery (a process that destroys tissue using heat current) is used to destroy parts of the ovaries. This surgery is not commonly used. But it can be an option for women who are still not ovulating after losing weight and trying fertility medicines. Laparoscopic ovarian drilling has been found to lower levels of testosterone and luteinising hormone (LH) and raise levels of follicle-stimulating hormone (FSH). This corrects your hormone imbalance and can restore the normal function of your ovaries. Studies of women with PCOS have shown that ovarian drilling results in an 80% ovulation rate and a 50% pregnancy rate 7.
PCOS treatment depends on the specific goals and characteristics of the patient
You desire fertility and you have normal weight
Ovulation induction using fertility drugs are indicated if you are infertile due to polycystic ovary syndrome and are of normal weight. These medications are used to regulate or induce ovulation. In general, they are designed to work like your own hormones. Fertility drugs are either used alone or in combinations depending on the reason for your ovulatory problem. Currently used fertility medications may include clomiphene citrate (Clomid®, Serophene®), gonadotropins, letrozole (Femara®, Amiridex®), bromocriptine (Parlodel®) or cabergoline (Dostinex®).
You desire fertility and you are overweight
As in the women who do not desire fertility, the first step is weight loss. The same recommendations hold true and the same approach is used. The main difference is with the time frame with which the treatment is completed. If you are young (<33 years old), then it makes logical sense to proceed with aggressive weight loss and achieve a more healthy BMI (Ideally < 30). If your BMI (body mass index) indicates morbid obesity (>40), then consideration should be given to aggressive weight loss to achieve a BMI of <35 and then proceeding with ovulation induction and pregnancy.
There is not an “ideal weight.” Complications from PCOS can affect the ensuing pregnancy regardless of the weight. However, miscarriage, gestational diabetes mellitus, hypertension (high blood pressure) are all significantly increased in patients with a BMI (body mass index) of >40. It is common practice to strongly recommend that no attempts with ovulation induction occur when the BMI is >40 (even with patients older than 35). There has been improved results with patients who undergo weight loss surgery (bariatric surgery). However, the best strategy should be determined after a honest dialogue where the patient is open about her dietary and lifestyle habits.
After weight loss, it is recommended to proceed directly with ovulation induction. Some patients may start to ovulate on their own and provided there are no other fertility factors (low sperm count, blocked tubes, advanced reproductive age of the women), it is reasonable to consider waiting for spontaneous conception with timed intercourse.
How do I know if I’m overweight or obese?
You can use the body mass index (BMI) to find out whether your weight is in a healthy or unhealthy range. BMI is a tool to estimate body fat. Type your height and weight into this BMI calculator (https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html)
- Women with a BMI of 25 to 29.9 are considered overweight.
- Women with a BMI of 30 or more have obesity.
BMI gives you a good idea of how healthy your weight is. But it doesn’t tell the whole story. BMI is less accurate in some people than in others. For example, if you are very muscular, you may be healthy even if your BMI is above 25. This is because muscle weighs more than fat.
Another way to figure out if you have a healthy weight is to measure your waist circumference (the distance around your waist). Researchers and doctors have agreed that women with a waist circumference larger than 35 inches are at higher risk for many health problems caused by overweight or obesity 8.
What effect can weight loss have on women with PCOS?
For overweight women, weight loss alone often regulates the menstrual cycle. Even a loss of 10–15 pounds can be helpful in making menstrual periods more regular. Weight loss also has been found to improve cholesterol and insulin levels and relieve symptoms such as excess hair growth and acne.
What can be done to increase the chances of pregnancy for women with PCOS?
Successful ovulation is the first step toward pregnancy. For overweight women, weight loss often accomplishes this goal. Medications also may be used to cause ovulation. Surgery on the ovaries has been used when other treatments do not work. However, the long-term effects of these procedures are not clear.
How IVF as a treatment for infertility procedure works
- Step 1 – Ovulation induction. You will start daily injections of an ovulation induction medication. These medications stimulate the growth of multiple follicles in both ovaries. These medications are given by injection for 8 to 14 days. A health care provider closely monitors the development of the eggs using transvaginal ultrasound and blood tests to assess follicle growth and estrogen production by the ovaries. When the eggs are mature—as determined by the size of the ovarian follicles and the level of estrogen—an injection of the hormone human chorionic gonadotropin (hCG) initiates the ovulation process. A health care provider takes out (egg retrieval) the eggs 34 to 36 hours after the hCG injection.
- Step 2 – Egg retrieval. This is the process used to remove the eggs from the ovaries so they can be fertilized. The procedure is performed in a physician’s office as an outpatient procedure. A mild sedative and painkiller are often used during the procedure, and it normally takes about 30 minutes. The steps for egg retrieval are as follows:
- An ultrasound probe is inserted into the vagina to visualize the ovaries and the follicles, which contain the eggs.
- A needle is inserted through the wall of the vagina to the ovaries. Generally, ultrasound is used to guide the placement of the needle.
- Suction is used to pull the eggs from the ovaries into the needle.
- Step 3 – Fertilization. After egg retrieval, your eggs will be combined with your partner’s sperm or donor sperm in the lab. A man provides a semen sample. If the sperm are healthy, they are centrifuged to concentrate them and reduce the volume, placed in a dish with the egg, and left overnight in an incubator. Fertilization usually occurs on its own. However, sometimes sperm are not able to fertilize the egg on their own. When this is the case, a single sperm is injected into an egg using a needle. This process is called intracytoplasmic sperm injection (ICSI). About 60% of IVF in the Unites States is performed with ICSI 9. The pregnancy rate is about the same for IVF using natural fertilization or intracytoplasmic sperm injection (ICSI). If sperm cannot fertilize the egg without assistance, couples should consider genetic testing. This testing can determine whether the sperm have chromosome problems that might cause development problems in the resulting embryos. Embryos that develop from IVF are placed into the uterus 1 to 6 days after retrieval. An embryologist will check for signs of fertilization and will monitor the growing embryos over the next 5 to 6 days.
- Step 4 – Embryo transfer. This procedure is performed in a physician’s office. The procedure is normally painless, but some women may experience cramping. A health care provider inserts a long, thin tube through the vagina and into the uterus and injects the embryo into the uterus. The embryo should implant into the lining of the uterus 6 to 10 days after retrieval. Sometimes the embryos are frozen and thawed at a later date for embryo transfer. This is often done when fresh embryos fail to implant or when a woman wants to preserve her eggs in order to become pregnant years later. Women either time implantation with their ovulation cycle or receive estrogen and progesterone medications to prepare their uterine linings for implantation. Implantation of the embryo into the uterine lining usually occurs over the next 5 to 7 days.
- Step 5 – Cryopreservation. Often patients will produce more viable embryos than they need in one IVF cycle. Additional embryos can be frozen, or cryopreserved, to be used later in a frozen embryo transfer.
- Step 6 – Pregnancy test. You can expect your physician to order a pregnancy test about 2 weeks after transfer.
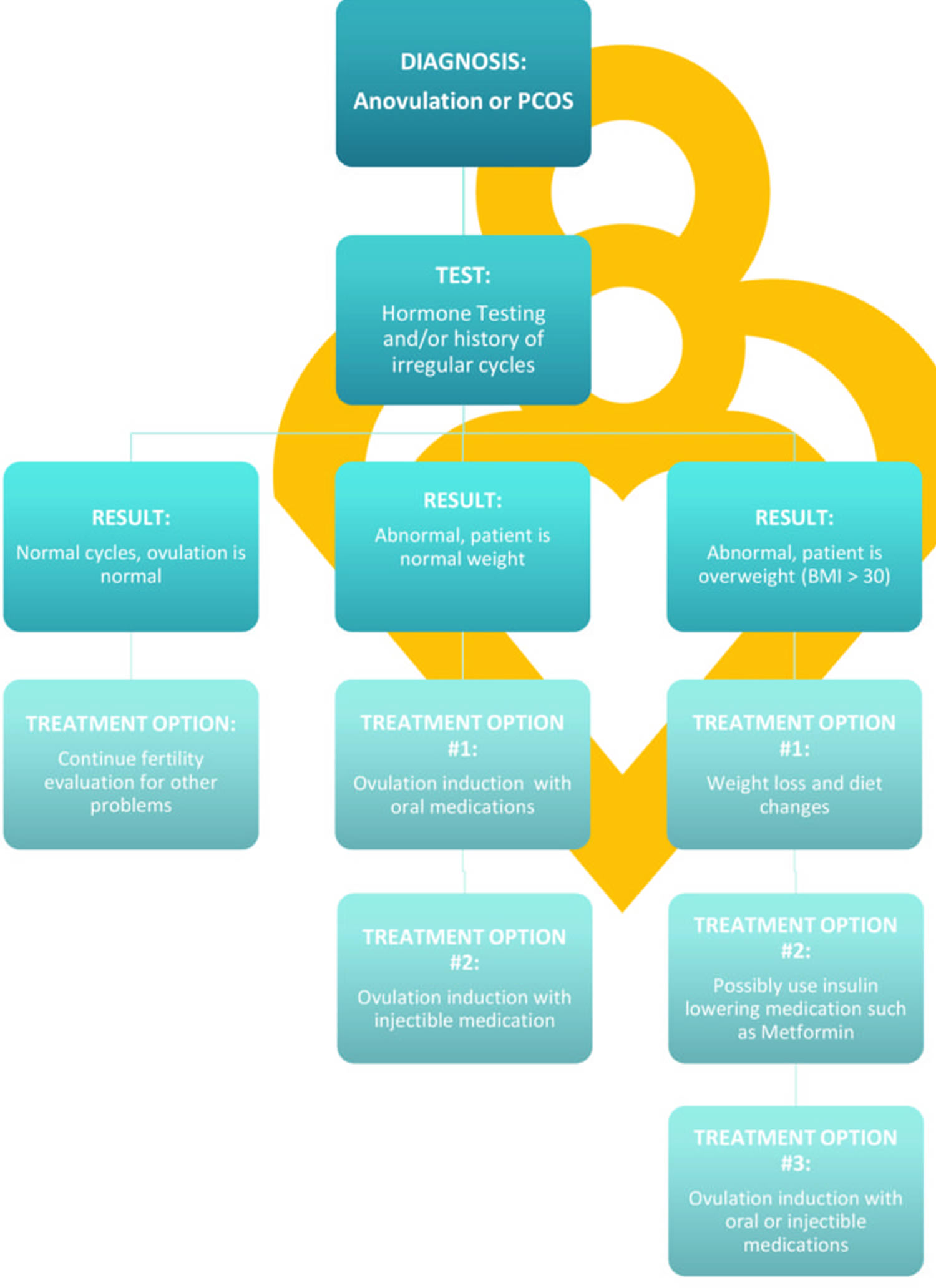
Figure 1. Getting Pregnant with PCOS Treatment Algorithm
How does PCOS affect pregnancy?
PCOS can cause problems during pregnancy for you and for your baby. Women with PCOS have higher rates of 11:
- Miscarriage
- Gestational diabetes
- High blood pressure (hypertension)
- Preeclampsia
- Cesarean section (C-section)
Your baby also has a higher risk of being heavy (macrosomia) and of spending more time in a neonatal intensive care unit (NICU).
If you’re overweight or obese, you can lower your risk by losing weight before trying for a baby.
How can I prevent problems from PCOS during pregnancy?
You can lower your risk of problems during pregnancy by:
- Reaching a healthy weight before you get pregnant. Use this interactive tool (link is external) to see your healthy weight before pregnancy and what to gain during pregnancy.
- Reaching healthy blood sugar levels before you get pregnant. You can do this through a combination of healthy eating habits, regular physical activity, weight loss, and medicines such as metformin.
- Taking folic acid. Talk to your doctor about how much folic acid you need.
PCOS signs and symptoms
A diagnosis of PCOS can usually be made if other rare causes of the same symptoms have been ruled out and you meet at least two of the following three criteria.
The three main features of PCOS are:
- Irregular periods – which means your ovaries don’t regularly release eggs (ovulation)
- Excess androgen – high levels of “male hormones” in your body, which may cause physical signs such as excess facial or body hair (see signs and symptoms below)
- Polycystic ovaries – your ovaries become enlarged and contain many fluid-filled sacs (follicles) which surround the eggs
As only two of these need to be present to diagnose PCOS, you won’t necessarily need to have an ultrasound scan before the condition can be confirmed.
If you have PCOS (polycystic ovarian syndrome), you may have some or all of the following symptoms:
- Excess hair growing on your face, chin, chest, stomach or back (hirsutism). Hirsutism affects up to 70% of women with PCOS 12.
- Thinning hair or hair loss on the scalp; male-pattern baldness (alopecia)
- Irregular periods (menstrual cycle) or no periods at all. Women with PCOS may miss periods or have fewer periods (fewer than eight in a year). Or, their periods may come every 21 days or more often. Some women with PCOS stop having menstrual periods.
- Abnormal vaginal bleeding
- Difficulty falling pregnant or not falling pregnant at all
- Acne on the face, chest, and upper back
- Easy weight gain or difficulty losing weight
- Swollen belly
- Mental health problems such as depression and anxiety
- Darkening of skin, particularly along neck creases, in the groin, and underneath breasts
- Skin tags, which are small excess flaps of skin in the armpits or neck area
It’s important to talk to your doctor if you have any or all of these symptoms.
Your doctor may also look for:
- high blood pressure
- symptoms and signs of diabetes.
PCOS and other health problems
Studies have found links between PCOS and other health problems, including:
- Type 2 Diabetes. More than half of women with PCOS will have diabetes or prediabetes (glucose intolerance) before the age of 40 13.
- High blood pressure. Women with PCOS are at greater risk of having high blood pressure compared with women of the same age without PCOS. High blood pressure is a leading cause of heart disease and stroke. Learn more about heart disease and stroke.
- Unhealthy cholesterol. Women with PCOS often have higher levels of LDL (bad) cholesterol and low levels of HDL (good) cholesterol. High cholesterol raises your risk of heart disease and stroke.
- Sleep apnea. This is when momentary and repeated stops in breathing interrupt sleep. Many women with PCOS have overweight or obesity, which can cause sleep apnea. Sleep apnea raises your risk of heart disease and diabetes.
- Depression and anxiety. Depression and anxiety are common among women with PCOS.
- Endometrial cancer. Problems with ovulation, obesity, insulin resistance, and diabetes (all common in women with PCOS) increase the risk of developing cancer of the endometrium (lining of the uterus or womb).
Researchers do not know if PCOS causes some of these problems, if these problems cause PCOS, or if there are other conditions that cause PCOS and other health problems.
PCOS causes
The exact cause of PCOS is not known. Most experts think that several factors, including genetics, play a role:
- High levels of androgens. Androgens are sometimes called “male hormones,” although all women make small amounts of androgens. Androgens control the development of male traits, such as male-pattern baldness. Women with PCOS have more androgens than normal. Higher than normal androgen levels in women can prevent the ovaries from releasing an egg (ovulation) during each menstrual cycle, and can cause extra hair growth and acne, two signs of PCOS.
- High levels of insulin. Insulin is a hormone that controls how the food you eat is changed into energy. Insulin resistance is when the body’s cells do not respond normally to insulin. As a result, your insulin blood levels become higher than normal. Many women with PCOS have insulin resistance, especially those who have overweight or obesity, have unhealthy eating habits, do not get enough physical activity, and have a family history of diabetes (usually type 2 diabetes). Over time, insulin resistance can lead to type 2 diabetes.
Insulin Resistance
Recent studies have demonstrated that Polycystic Ovary Syndrome (PCOS) is due to an underlying metabolic problem known as insulin resistance.
Insulin is a hormone produced by the pancreas to control the amount of sugar in your blood. Insulin helps to move glucose from blood into cells, where it’s broken down to produce energy. Insulin resistance means the body’s tissues are resistant to the effects of insulin. The body therefore has to produce extra insulin to compensate.
When the body’s muscles and fat tissues become resistant to insulin action, the pancreas produces increased amounts insulin, leading to high insulin levels. In a woman with PCOS, these high insulin levels can set into play a vicious cycle that makes weight loss extremely difficult. Because the high insulin levels tend to produce food cravings, particularly in the form of carbohydrates, the woman often finds herself in a state of overnourishment. These high insulin levels also drive the ovary to produce high amounts of male hormones, testosterone, which interferes with the development of the follicles (the sacs in the ovaries where eggs develop) and prevents normal ovulation, leading to Ovarian Confusion. This unhealthy environment in the ovary causes follicles to literally die before they release mature eggs resulting in Ovulation Disruption.
Hormone Imbalance
Many women with PCOS are found to have an imbalance in certain hormones, including:
- raised levels of testosterone – a hormone often thought of as a male hormone, although all women usually produce small amounts of it
- raised levels of luteinising hormone (LH) – this stimulates ovulation, but may have an abnormal effect on the ovaries if levels are too high
- low levels of sex hormone-binding globulin (SHBG) – a protein in the blood, which binds to testosterone and reduces the effect of testosterone
- raised levels of prolactin (only in some women with PCOS) – hormone that stimulates the breast glands to produce milk in pregnancy
The exact reason why these hormonal changes occur isn’t known. It’s been suggested that the problem may start in the ovary itself, in other glands that produce these hormones, or in the part of the brain that controls their production. The changes may also be caused by the resistance to insulin.
Genetic factor
PCOS sometimes runs in families. If any relatives, such as your mother, sister or aunt, have PCOS, then the risk of you developing it is often increased.
This suggests there may be a genetic link to PCOS, although specific genes associated with the condition haven’t yet been identified.
If you have the syndrome, your sisters and daughters have a 50% chance of developing PCOS. Abnormal insulin production and metabolic problems may contribute to the development of PCOS. If you do not ovulate normally for any length of time, you may develop multiple cysts on your ovaries (polycystic ovaries).
You may have more regular menstrual cycles as you near menopause. The reason for this is not known. However, your history of PCOS may still increase your long-term risk of high blood pressure (hypertension), heart disease, diabetes, or endometrial cancer.
The main risk factor for polycystic ovary syndrome (PCOS) is a family history of PCOS. If you have the syndrome, your sisters and daughters have a 50% chance of developing PCOS. A family history of diabetes may increase your risk for PCOS because of the strong relationship between diabetes and PCOS. Research is ongoing on this risk factor.
The long-term use of the anti-seizure medication valproate has been related to an increased risk of developing PCOS.
Insulin resistance is a condition in which the body’s cells do not respond to the effects of insulin. When the body does not respond to insulin, the level of glucose in the blood increases. This may cause more insulin to be produced as the body tries to move glucose into cells. Insulin resistance can lead to diabetes mellitus. It also is associated with acanthosis nigricans.
PCOS diagnosis
The diagnosis of polycystic ovarian syndrome (PCOS) is usually difficult. There is no single test to diagnose PCOS. To help diagnose PCOS and rule out other causes of your symptoms, your doctor may talk to you about your medical history and do a physical exam and different tests.
You should see your doctor if you are feeling unwell and have any of the symptoms that could be caused by PCOS.
Your doctor will talk to you to try to understand your symptoms. He or she will examine you.
- Physical exam. Your doctor will measure your blood pressure, body mass index (BMI), and waist size. They will also look at your skin for extra hair on your face, chest or back, acne, or skin discoloration. Your doctor may look for any hair loss or signs of other health conditions (such as an enlarged thyroid gland).
- Pelvic exam. Your doctor may do a pelvic exam for signs of extra male hormones (for example, an enlarged clitoris) and check to see if your ovaries are enlarged or swollen.
- Pelvic ultrasound (sonogram). This test uses soundwaves to examine your ovaries for the presence of multiple, fluid-filled sacs (cysts) and check the endometrium (lining of the uterus or womb). Polycystic ovaries contain a large number of harmless follicles that are up to 8mm (approximately 0.3in) in size. The follicles are under-developed sacs in which eggs develop. In PCOS, these sacs are often unable to release an egg, which means that ovulation doesn’t take place.
- Blood tests. Blood tests check your androgen hormone levels (such as testosterone), sometimes called “male hormones.” Your doctor will also check for other hormones related to other common health problems that can be mistaken for PCOS, such as thyroid disease. Your doctor may also test your cholesterol levels and test glucose levels in your blood for diabetes.
Once other conditions are ruled out, you may be diagnosed with PCOS if you have at least two of the following symptoms 14:
- Irregular periods, including periods that come too often, not often enough, or not at all
- Signs that you have high levels of androgens:
- Extra hair growth on your face, chin, and body (hirsutism)
- Acne
- Thinning of scalp hair
- Higher than normal blood levels of androgens
- Multiple cysts on one or both ovaries
PCOS treatment
PCOS (polycystic ovarian syndrome) can’t be cured, but you and your doctor can manage many of the symptoms. The treatment you will have depends on the main problems you have.
If you are worried about your fertility (falling pregnant), your plans for having children or about irregular periods, then speak to your doctor about the many different approaches you can take.
If you are worried about acne and excess hair, there are cosmetic treatments and medical treatments that can help.
No matter what the issue, being healthy is important. Eating a healthy diet and getting some regular exercise can help many of the physical and emotional problems caused by PCOS.
Exercise can improve your mental health, and losing even a small amount of weight can help regulate your periods, improve your chance of becoming pregnant and reduce your risk of diabetes and heart disease.
It’s important to have regular health checks because of your increased risk of developing health problems later in life.
Talk to your doctor if you need help to control your weight. Your doctor can refer you to the right health professional for your situation, such as a dietitian or exercise specialist.
You can take steps at home to help your PCOS symptoms, including:
- Losing weight. Healthy eating habits and regular physical activity can help relieve PCOS-related symptoms. Losing weight may help to lower your blood glucose levels, improve the way your body uses insulin, and help your hormones reach normal levels. Even a 10% loss in body weight (for example, a 150-pound woman losing 15 pounds) can help make your menstrual cycle more regular and improve your chances of getting pregnant 15. Learn more about healthy weight.
- Removing hair. You can try facial hair removal creams, laser hair removal, or electrolysis to remove excess hair. You can find hair removal creams and products at drugstores. Procedures like laser hair removal or electrolysis must be done by a doctor and may not be covered by health insurance.
- Slowing hair growth. A prescription skin treatment (eflornithine HCl cream) can help slow down the growth rate of new hair in unwanted places.
Medicines treat PCOS
The types of medicines that treat PCOS and its symptoms include:
- Hormonal birth control, including the pill, patch, shot, vaginal ring, and hormone intrauterine device (IUD). For women who don’t want to get pregnant, hormonal birth control can:
- Make your menstrual cycle more regular
- Lower your risk of endometrial cancer
- Help improve acne and reduce extra hair on the face and body (Ask your doctor about birth control with both estrogen and progesterone.)
- Anti-androgen medicines. These medicines block the effect of androgens and can help reduce scalp hair loss, facial and body hair growth, and acne. They are not approved by the Food and Drug Administration (FDA) to treat PCOS symptoms. These medicines can also cause problems during pregnancy.
- Metformin. Metformin is often used to treat type 2 diabetes and may help some women with PCOS symptoms. It is not approved by the FDA to treat PCOS symptoms. Metformin improves insulin’s ability to lower your blood sugar and can lower both insulin and androgen levels (to encourage fertility). After a few months of use, metformin may help restart ovulation, but it usually has little effect on acne and extra hair on the face or body. As metformin can stimulate fertility, if you’re considering using it for PCOS and aren’t trying to get pregnant, make sure you use suitable contraception if you’re sexually active. Recent research shows that metformin may have other positive effects, including lowering body mass and improving cholesterol levels and reducing the risk of heart disease. Possible side effects of metformin include nausea, vomiting, stomach pain, diarrhoea and loss of appetite.
If you do not desire pregnancy and you are not overweight or insulin resistant, a very common approach is to begin treatment with oral contraceptive pills (OCP’s) and specific treatments for the excess hair growth. Birth control pills can help your periods be regular and can reduce symptoms such as excess facial hair and acne. An androgen-lowering medicine, spironolactone, may be used with birth control pills to help reduce symptoms even more. These medicines are not used if you are trying to get pregnant.
It is important to see your doctor for follow-up to make sure treatment is working and to adjust it if needed. You may also need regular tests to check for diabetes, high blood pressure, and other possible problems. In addition, it may take a while for treatments to help with symptoms such as facial hair or acne. In the meantime, over-the-counter or prescription acne medicines may help with skin problems as well as waxing, tweezing, and shaving are easy ways to get rid of unwanted hair. Electrolysis or laser treatments can permanently remove the hair but are more expensive. Your doctor can also prescribe a skin cream that slows hair growth for as long as you use it regularly.
Medications can also be used to treat some of the other problems associated with PCOS, including:
- weight-loss medication, such as orlistat, if you’re overweight
- cholesterol-lowering medication (statins), if you have high levels of cholesterol in your blood
- acne treatments
Unwanted hair growth and hair loss
Medications to control excessive hair growth (hirsutism) and hair loss (alopecia) include:
- particular types of combined oral contraceptive tablets (such as co-cyprindiol, Dianette, Marvelon and Yasmin)
- cyproterone acetate
- spironolactone
- flutamide
- finasteride
These medications work by blocking the effects of “male hormones”, such as testosterone, and some also suppress production of these hormones by the ovaries.
A cream called eflornithine can also be used to slow down the growth of unwanted facial hair. This cream doesn’t remove hair or cure unwanted facial hair, so you may wish to use it alongside a hair-removal product. Improvement may be seen four to eight weeks after treatment with this medication.
If you have unwanted hair growth, you may also want to remove the excess hair (by methods such as plucking, shaving, threading, creams or laser removal). Laser removal of facial hair is an option.
PCOS diet
Around half of all women with polycystic ovary syndrome (PCOS), are overweight or obese. Because PCOS sufferers have higher than normal insulin levels, controlling insulin, a hormone that’s produced in your pancreas, through a PCOS diet can have many benefits. The wrong kind of diet, one high in refined carbohydrates, can make insulin resistance, and therefore weight loss, more difficult to control.
Many women with PCOS find they are able to manage their symptoms and reduce their risk of other medical concerns by controlling their diet and lifestyle choices with a PCOS diet. Women who thrive with PCOS know that food is medicine. The right PCOS diet foods can heal your most challenging symptoms. The essence of eating to heal with PCOS is to consume food in its most natural state. Processed and refined foods wreak havoc with hormone levels, so “clean” eating will actually help you begin to balance your hormones. As insulin, cortisol, testosterone, progesterone, estrogen, and thyroid become more in balance, PCOS symptoms will be alleviated
PCOS Diet Rules
- No Processed Foods: Avoid processed and refined foods such as white flour, sugar, breads and pasta. Instead eat whole gluten-free grains like oatmeal, brown rice, millet, amaranth and quinoa.
- Increase Fiber: Eat more foods that are high in fiber. Because fiber slows down digestion it is effective at combating insulin resistance.
- Drink More Water: Drink two liters of water per day, flavoring with cut-up fresh citrus, cucumber, mint or berries.
- No Refined Sugar: Avoid foods with refined sugar, high-fructose corn-syrup, artificial sweeteners, artificial colors, MSG, trans-fats and high saturated fat.
- Less Ingredients: Eat packaged foods with 5 or less all-natural ingredients. Any product with a long ingredient list is usually highly processed.
- Limit Alcohol: Make alcohol an occasional indulgence – not an everyday occurrence. A glass of red wine is fine once in awhile, but after one glass, the benefits are reversed.
- Balance Carbs and Proteins: Always combine a lean protein and complex carb at every meal/snack. For example, a slice of turkey and a handful of nuts with a half of banana. Or yogurt with a small piece of cheese.
- Take the Right Foods With You: Take the right foods with you. Pack your own lunches for work or play. Make sure you bring along snacks so you have healthy choices wherever you go and don’t eat whatever is available because you are starving.
It’s important to understand that there is no cure for PCOS and no magical formula or pill that will make the symptoms better. But, by making these diet and lifestyle changes, many of PCOS patients are able to manage their symptoms, improve their fertility, and lead fulfilled lives where they are happy with their bodies and the way they look.
- Trivax, B., & Azziz, R. (2007). Diagnosis of polycystic ovary syndrome. Clinical Obstetrics and Gynecology, 50(1), 168–177. https://www.ncbi.nlm.nih.gov/pubmed/17304034[↩]
- Bremer AA. Polycystic Ovary Syndrome in the Pediatric Population. Metabolic Syndrome and Related Disorders. 2010;8(5):375-394. doi:10.1089/met.2010.0039. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3125559/[↩]
- Infertility and Fertility. https://www.nichd.nih.gov/health/topics/infertility[↩]
- Practice Committee of American Society for Reproductive Medicine. (2013). Definitions of infertility and recurrent pregnancy loss: A committee opinion. Fertility and Sterility, 99(1), 63.[↩]
- Moran, L. J., Hutchison, S. K., Norman, R. J., & Teede, H. J. (2011). Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database of Systematic Reviews, 2, CD007506.[↩]
- Wallace, K. L., Johnson, V., Sopelak, V., & Hines, R. (2011). Clomiphene citrate versus letrozole: Molecular analysis of the endometrium in women with polycystic ovary syndrome. Fertility and Sterility, 96(4), 1051–1056. https://www.ncbi.nlm.nih.gov/pubmed/21851939[↩]
- American College of Obstetricians and Gynecologists (2002, reaffirmed 2008). Management of infertility caused by ovulatory dysfunction. ACOG Practice Bulletin No. 34. Obstetrics and Gynecology, 99(2), 347–358.[↩]
- Flint, A.J., Rexrode, K.M., Hu, F.B., Glynn, R.J., Caspard, H., Manson, J.E., et al. (2010). Body mass index, waist circumference, and risk of coronary heart disease: a prospective study among men and women. Obesity Research and Clinical Practice; 4(3): e171-e181. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2992336/[↩]
- American Society for Reproductive Medicine. (2015). Assisted reproductive technologies: A guide for patients. http://www.fertilityanswers.com/wp-content/uploads/2016/04/assisted-reproductive-technologies-booklet.pdf[↩]
- Anovulation & PCOS. QuickView Treatment Plan. https://www.fertilityanswers.com/fertility-treatments/anovulation-pcos/[↩]
- Boomsma, C. M., Fauser, B. C., & Macklon, N.S. (2008). Pregnancy complications in women with polycystic ovary syndrome. Seminars in Reproductive Medicine, 26, 72–84. https://www.ncbi.nlm.nih.gov/pubmed/18181085[↩]
- Polycystic Ovary Syndrome (PCOS). American College of Obstetricians and Gynecologists. https://www.acog.org/Patients/FAQs/Polycystic-Ovary-Syndrome-PCOS[↩]
- Lorenz, L. B., & Wild, R. A. (2007). Polycystic ovarian syndrome: an evidence-based approach to evaluation and management of diabetes and cardiovascular risks for today’s clinician. Clinical Obstetrics and Gynecology, 50, 226–243. https://www.ncbi.nlm.nih.gov/pubmed/17304038[↩]
- Goodman, N. F., Cobin, R. H., Futterweit, W., Glueck, J. S., Legro, R. S., & Carmina, E. (2015). American Association of Clinical Endocrinologists, American College of Endocrinology, and Androgen Excess and PCOS Society disease state clinical review: guide to the best practices in the evaluation and treatment of polycystic ovary syndrome – part 1. Endocrine Practice, 11, 1291–300. http://journals.aace.com/doi/pdf/10.4158/EP15748.DSC[↩]
- Polycystic Ovary Syndrome (PCOS). https://www.acog.org/Patients/FAQs/Polycystic-Ovary-Syndrome-PCOS[↩]





{kind=link}