
Contents
What is pediculosis
Pediculosis is the medical term for an infection or infestation with lice which are blood feeding parasites. Lice are ectoparasites that live on the body. Lice are obligate, parasitic insects that have no free-living stage in their life cycle 1. Lice feed on human blood after piercing the skin and injecting saliva, which may cause intense itch (pruritis) due to an allergic reaction 2. Lice crawl but cannot fly or hop 2.
Patients typically present with intense itch, typically from an immune-mediated hypersensitivity reaction. It may take 2 to 6 weeks to develop symptoms after the first exposure, while future intense itch can develop after 1 or 2 days after exposure. The itching induces scratching, which can lead to secondary bacterial infection. This can ultimately lead to complications such as impetigo and pyoderma 3.
Different species of lice prefer to feed on certain locations on the body of the host. Louse species include Pediculus capitis (head lice), Pediculus corporis (body lice), and Pediculosis pubis or pubic lice, sometimes called “crabs” or Pthirus pubis. Head lice (Pediculus capitis) are the most common lice 4.
Lice move from person to person through close physical contact. Spread through contact with fomites (e.g., combs, brushes, clothes, hats, scarves, coats, linens) used by an infested person is uncommon 2. Overcrowding encourages the spread of lice. The body louse can be the vector of Rickettsia prowazeki, which causes typhus; Bartonella quintana, which causes trench fever; and Borrelia recurrentis, which causes relapsing fever 5.
Body and head lice are 1 mm to 3 mm long, while the pubic louse is much shorter. The head louse (Pediculus capitis) is an obligate parasite that spends its entire life on the human host. Head lice feed exclusively on blood. Lice are unable to jump or fly, and transmission requires close contact. Transmission is thought to occur by head-to-head contact, sharing of headgear, or other direct contacts with fomites (inanimate objects that harbor the organism such as movie seats) 6. A mature female head louse lays 3-6 eggs, also called nits, per day. Nits are white and less than 1 mm long. Nymphs (immature lice) hatch from the nits after 8-9 days, reach maturity in 9-12 days, and live as adults for about 30 days 2. Lice crawl but cannot fly or hop 2.
Louse infestation remains a major problem throughout the world affecting hundreds of millions of people worldwide each year 1. They have been reported in all countries and all levels of society. It is estimated that pediculus capitis (head lice) affects six to 12 million people in the United States every year, but exact numbers are unknown as it is not a reportable disease. Outbreaks of head lice more commonly affect children three to 12 years old, with girls being affected more commonly than boys. In industrialized countries, small epidemics typically develop in schoolchildren whose tight social bonds allow for the rapid spread of the infestation. It is also common for several members of the same household to be affected. Infestations are more common in the warmer months, as well as in areas with higher humidity. Head lice cross all socioeconomic barriers, whereas body lice more commonly affect the homeless and displaced 7.
Pediculus capitis (head louse) results in significant psychological stress in children and adults and missed schooldays in children, particularly in areas with a no-nit policy 8.
Human lice have been used as a forensic tool. A mixed DNA profile of 2 hosts can be detectable in blood meals of body lice that have had close contact between an assailant and a victim 9.
The treatment of lice is very effective with high cure rates, especially when mature lice are identified. However, the current treatment does not kill eggs and repeat treatment is often required. The frequent use of lice treatment is also known to cause severe itching, which can lead to skin breakdown and secondary bacterial infections. The major problem with lice today is a social embarrassment 10.
Lotions and shampoos containing 1% permethrin (Nix) often work well. You can buy these medicines at the store without a prescription. If these products do not work, a health care provider can give you a prescription for stronger medicine. Always use the medicines exactly as directed. Using them too often or in the wrong way can cause side effects.
To use the medicine shampoo:
- Rinse and dry the hair.
- Apply the medicine to the hair and scalp.
- Wait 10 minutes, then rinse it off.
- Check for lice and nits again in 8 to 12 hours.
- If you find active lice, talk to your provider before doing another treatment.
You also need to get rid of the lice eggs (nits) to keep lice from coming back.
To get rid of nits:
- You can use products that make the nits easier to remove. Some dishwashing detergents can help dissolve the “glue” that makes the nits stick to the hair shaft.
- Remove the eggs with a nit comb. Before doing this, rub olive oil in the hair or run the metal comb through beeswax. This helps make the nits easier to remove.
- Metal combs with very fine teeth are stronger and work better than plastic nit combs. These metal combs are easier to find in pet stores or on the Internet.
- Comb for nits again in 7 to 10 days.
When treating lice, wash all clothes and bed linens in hot water with detergent. This also helps prevent head lice from spreading to others during the short period when head lice can survive off the human body.
Because lice can be present on inanimate fomites, heating infested clothing and bedding with hot water is necessary to destroy all stages of lice. The heat necessary for the destruction of lice and nits is 125.6 °F (52 °C) for 30 minutes. Lice have been found to become heat resistant through hormonal mechanisms, tolerating temperatures over 212 °F (100 °C).
What causes pediculosis?
Lice do not jump or fly from person to person but require direct contact for transfer. They cannot be transmitted via animals. They can be transferred by some objects and clothing such as hats, combs and sheets.
The three lice species that infest humans are:
- Pediculus capitis (head louse) is by far the most common infestation. It does not discriminate between socioeconomic groups and occurs most commonly in school-aged children.
- Pediculosis corporis (clothing or body louse) is commonly associated with poverty, overcrowding (e.g. refugee camps and crowded buses/trains) and poor hygiene (e.g. infrequent washing and/or changing of clothing and shared bedding and/or clothing).
- Pediculosis pubis (pubic or crab louse) is transmitted by intimate and/or sexual contact and to a lesser extent via contaminated clothing, towels and bedding. Condom use does not prevent transmission.
Pediculosis life cycle
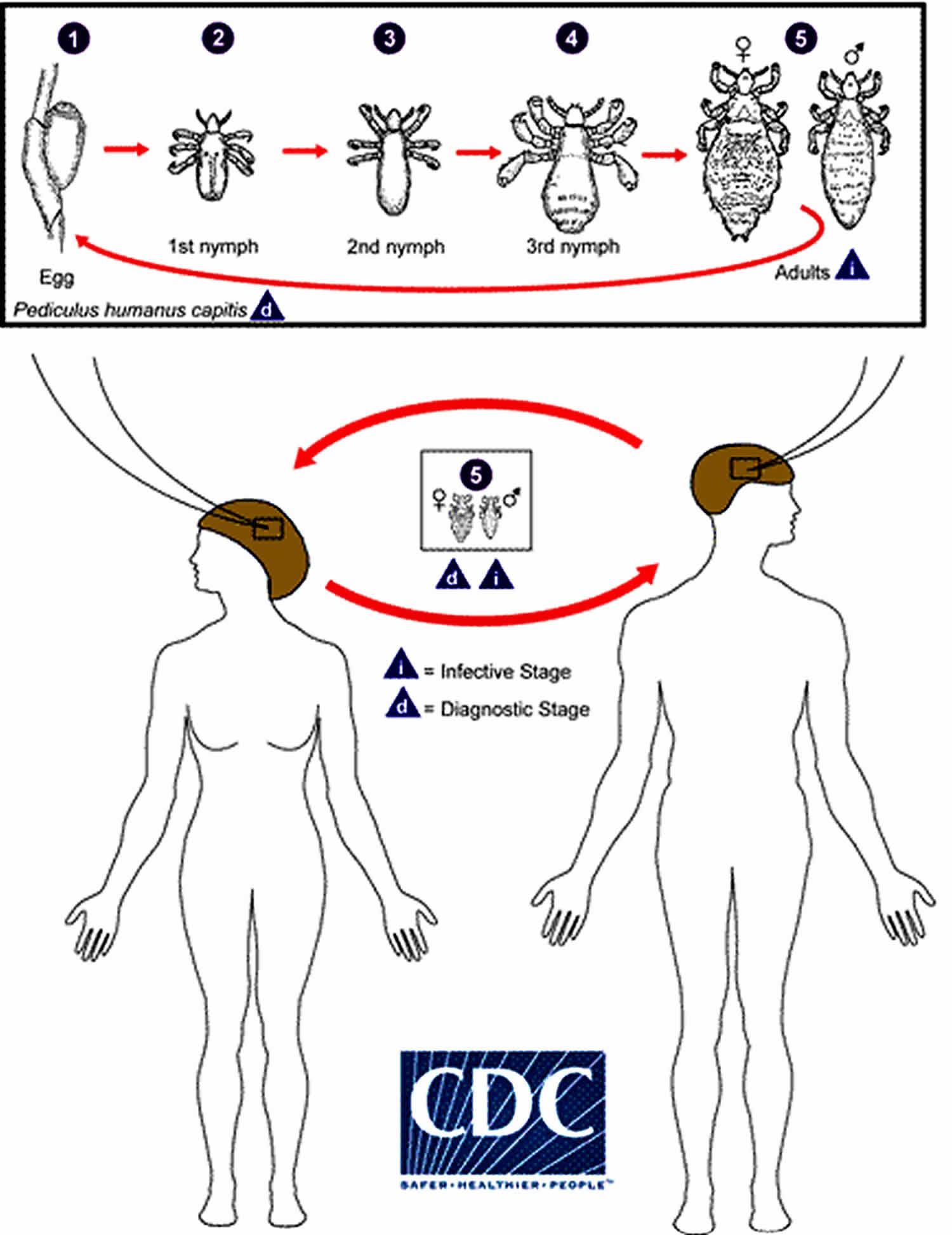
Pediculosis is infestation with the human head-and-body louse, Pediculus humanus. There are two subspecies, the head louse (Pediculus humanus capitis) and the body louse (Pediculus humanus humanus). They are ectoparasites whose only known hosts are humans. Recent molecular data suggest that the two subspecies are ecotypes of the same species and that evolution between the two populations take place continually 11.
The life cycle of the head louse has three stages: egg, nymph, and adult.
Eggs: Nits are head lice eggs. They are hard to see and are often confused for dandruff or hair spray droplets. Nits are laid by the adult female and are cemented at the base of the hair shaft nearest the scalp (number 1). They are 0.8 mm by 0.3 mm, oval and usually yellow to white. Nits take about 1 week to hatch (range 6 to 9 days). Viable eggs are usually located within 6 mm of the scalp.
Nymphs: The egg hatches to release a nymph (number 2). The nit shell then becomes a more visible dull yellow and remains attached to the hair shaft. The nymph looks like an adult head louse, but is about the size of a pinhead. Nymphs mature after three molts (number 3, number 4) and become adults about 7 days after hatching.
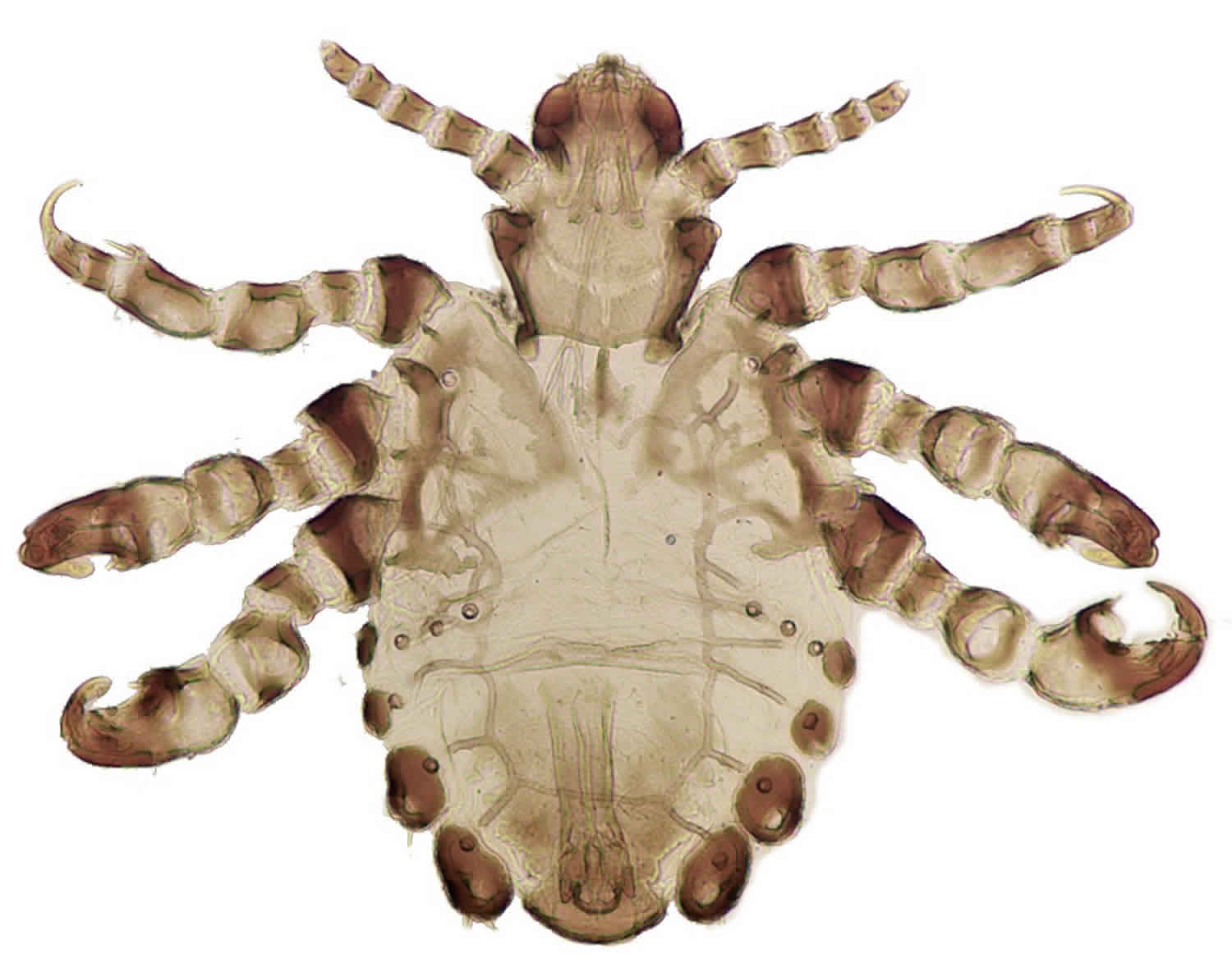
Adults: The adult louse is about the size of a sesame seed, has 6 legs (each with claws), and is tan to grayish-white (number 5). In persons with dark hair, the adult louse will appear darker. Females are usually larger than males and can lay up to 8 nits per day. Adult lice can live up to 30 days on a person’s head. To live, adult lice need to feed on blood several times daily. Without blood meals, the louse will die within 1 to 2 days off the host.
Body lice: Body lice are morphologically similar to head lice. They have a different life cycle, whereas body lice reside on and lay their eggs on the clothing and fomites of infected individuals and migrate to the human body to feed.
Figure 1. Adult head or body lice

Figure 2. Pediculosis life cycle
Pediculosis corporis
Pediculosis corporis or body lice are parasitic insects that feed on human blood. Adult body lice have 6 legs, are tan to grayish-white in color, 2.3 to 3.6 mm in length, have no wings, and are flat in shape. Body lice live and lay eggs on clothing and only move to the skin to feed. Body lice feed 1 to 5 times a day and can live up to 60 days. When separated from a human host, body lice will die within a week. Body lice are known to spread disease.
The greatest medical impact of body lice is their ability to transmit bacterial diseases, most notably trench fever caused by Bartonella quintana, relapsing fever caused by Borrelia recurrentis, and epidemic (louse-borne) typhus caused by Rickettsia prowazekii 12. Trench fever and epidemic typhus are not transmitted by louse bites but rather through infected feces. When feeding, the body louse often excretes its feces onto the skin, which can be inadvertently rubbed into the bite site, eyes, or mucous membranes. Transmission of Rickettsia prowazekii can also occur through inhalation of aerosolized fecal dust, which has been documented as a potential source of infection for clinicians. Unlike trench fever and epidemic typhus, transmission of relapsing fever, caused by Borrelia recurrentis, does not occur through contaminated feces. Infection occurs when a person crushes an infected louse, and the bacteria then invade the bite site or the skin of the fingers or hand that crushed the louse 12. In addition, a person can acquire the infection if they rub their eye or put their fingers in their mouth after crushing the louse.
Additional pathogenic bacteria found in body lice include Salmonella typhi, Serratia marcescens, and Acinetobacter baumannii. The DNA of Yersinia pestis, which causes bubonic plague, has been identified in body lice, and it is believed they may serve as supplementary vectors for the organism 13.
There has been debate amongst entomologists regarding the proper taxonomy of head and body lice, some identify them as two different species, while others group them as a single species 14. Those considering them as two distinct species identify body lice as Pediculus humanus, while those who see them as one species identify them as Pediculus humanus humanus 14. In the medical literature, body lice are often referred to as Pediculus humanus corporis, but according to the rules of the International Commission on Zoological Nomenclature, this is an improper designation 13.
Studies have identified that the head and body lice are closely related, with genetic studies demonstrating that body lice possess only one gene that is not also present in head lice 15.
Unlike head and pubic lice, body lice do not live on the skin but rather live and lay their eggs in stitchings of clothing or bedding, moving to the skin only to feed. The most significant difference between body and head lice is the distinct ability of body lice to transmit the bacterial diseases of trench fever, relapsing fever, and epidemic typhus to humans 15.
Pediculosis corporis (body lice), which have a worldwide distribution, are ectoparasites that must feed on human blood to survive. They assume 3 forms across their life cycle starting with the egg, or nit, and progressing to the nymph and adult stage. As with head lice, nits are oval and appear yellow or white. However, unlike head lice, which attach their eggs to the proximal hair shafts, body lice lay their eggs in the seams of clothing. A nymph is an immature louse, which except for its smaller size, has the same appearance as an adult louse.
As body lice cannot jump or fly, they spread primarily by direct contact, though transmission can also occur through clothing, bed linens, and towels. Body lice infestations (pediculosis) are spread most commonly by close person-to-person contact but are generally limited to persons who live under conditions of crowding and poor hygiene (for example, the homeless, refugees, etc.). Dogs, cats, and other pets do not play a role in the transmission of human lice.
Infestations are strongly correlated with poor body hygiene, lack of access to clean clothing, and crowded conditions, which facilitate spread of the lice through direct physical contact. Outbreaks most commonly occur in situations where large groups of people live in unsanitary conditions such as prisons or camps of large groups of refugees from war, famine or natural disasters. In the United States and other developed countries, body lice infestations most commonly occur in homeless populations because of the lack of access to clean clothes or showers. Outbreaks of body lice infestations and louse-borne diseases continue to occur globally and have been documented in jails and refugee camps in central and eastern Africa, rural areas in the Peruvian Andes, and amongst rural populations in Russia 15.
Body lice infestations can involve thousands of mites, each biting an average of 5 times per day. During feeding, body lice pierce the skin, inject a salivary anticoagulant, and then suck the blood meal into their digestive tract. Bites of the body louse can produce a variety of skin lesions, and severe pruritus thought to be due to an allergic and/or inflammatory reaction to the louse saliva 16. Intense scratching of pruritic bites can result in skin excoriation, potentially leading to significant secondary bacterial infections.
Improved hygiene and access to regular changes of clean clothes is the only treatment needed for body lice infestations.
Where are body lice found?
Body lice generally are found on clothing and bedding used by infested people. Sometimes body lice are be seen on the body when they feed. Body lice eggs usually are seen in the seams of clothing or on bedding. Occasionally eggs are attached to body hair.
Lice found on the head and scalp are not body lice; they are head lice.
Can body lice transmit disease?
Yes. Body lice can spread epidemic typhus, trench fever, and louse-borne relapsing fever. Although louse-borne (epidemic) typhus is no longer widespread, outbreaks of this disease still occur during times of war, civil unrest, natural or man-made disasters, and in prisons where people live together in unsanitary conditions. Louse-borne typhus still exists in places where climate, chronic poverty, and social customs or war and social upheaval prevent regular changes and laundering of clothing.
Pediculosis corporis life cycle
Pediculus humanus humanus, the body louse, is a louse insect and is an ectoparasite whose only host are humans. The louse feeds on blood several times daily and resides close to the skin to maintain its body temperature.
Life cycle:
The life cycle of the body louse has three stages: egg, nymph, and adult (see Pediculosis life cycle in Figure 2 above).
Eggs: Nits are body lice eggs. They are hard to see and are often confused for dandruff. Nits are laid by the adult female and are cemented at the base of the hair shaft nearest the skin (number 1). They are 0.8 mm by 0.3 mm, oval and usually yellow to white. Nits take about 1 week to hatch (range 6 to 9 days). Viable eggs are usually located within 6 mm of the skin.
Nymphs: The egg hatches to release a nymph (number 2). The nit shell then becomes a more visible dull yellow and remains attached to the hair shaft. The nymph looks like an adult body louse, but is about the size of a pinhead. Nymphs mature after three molts (number 3, number 4) and become adults about 7 days after hatching.
Adults: The adult louse is about the size of a sesame seed, has 6 legs (each with claws), and is tan to grayish-white (number 5). In persons with dark hair, the adult louse will appear darker. Females are usually larger than males and can lay up to 8 nits per day. Adult lice can live up to 30 days on a person’s body. To live, adult lice need to feed on blood several times daily. Without blood meals, the louse will die within 1 to 2 days off the host.
Pediculosis corporis risk factors
Body lice infestation is found worldwide but generally is limited to persons who live under conditions of crowding and poor hygiene who do not have access to regular bathing and changes of clean clothes, such as:
- the homeless,
- refugees and,
- survivors of war or natural disasters.
Infestations can spread rapidly under such conditions. Body lice infestation can occur in people of all races.
Body lice are spread through direct contact with a person who has body lice or through contact with articles such as clothing, beds, bed linens, or towels that have been in contact with an infested person. However, in the United States, actual infestation with body lice tends to be occur only in homeless, transient persons who do not have access to regular bathing and changes of clean clothes.
Body lice can transmit disease. Epidemics of typhus and louse-borne relapsing fever have been caused by body lice (typically in areas where climate, poverty, and social customs or war and social upheaval prevent regular changes and laundering of clothing).
Pediculosis corporis prevention and control
Pediculosis corporis (body lice) are spread most commonly by direct contact with an infested person or an infested person’s clothing or bedding. Body lice usually infest persons who do not launder and change their clothes regularly.
The following are steps that can be taken to help prevent and control the spread of body lice:
- Bathe regularly and change into properly laundered clothes at least once a week; launder infested clothing at least once a week.
- Machine wash and dry infested clothing and bedding using the hot water (at least 130°F [54.4 °C]) laundry cycle and the high heat drying cycle. Clothing and items that are not washable can be dry-cleaned OR sealed in a plastic bag and stored for 2 weeks.
- Do not share clothing, beds, bedding, and towels used by an infested person.
- Fumigation or dusting with chemical insecticides sometimes is necessary to control and prevent the spread of body lice for certain diseases (epidemic typhus).
Pediculosis corporis symptoms
Intense itching (“pruritus”) and rash caused by an allergic reaction to louse bites are common symptoms of body lice infestation. As with other lice infestations, intense itching leads to scratching which can cause sores and secondary bacterial infection of the skin.
When body lice infestation is long lasting, heavily bitten areas of the skin can become thickened and darkened, particularly in the mid-section of the body. This condition is called “vagabond’s disease.”
As with other lice infestations, intense itching can lead to scratching which can cause sores on the body; these sores sometimes can become infected with bacteria or fungi.
Body lice are known to transmit disease (epidemic typhus, trench fever, and epidemic relapsing fever).
Pediculosis corporis diagnosis
While body lice may occasionally be found crawling on the patient’s skin, an infestation is typically diagnosed by finding eggs and lice in seams of clothing.
A PCR assay has been developed to differentiate between head and body lice but is primarily used for research purposes rather than to support clinical decision-making.
Historical clues such as poor body hygiene, lack of access to clean clothing, homelessness, and residing in crowded, unsanitary conditions should prompt consideration for body louse infestation and louse-borne infections
The primary symptom of body lice infestations is severe pruritus.
The dermatologic findings in body lice infestation vary but include areas of pyoderma, erythematous macules, wheals, and hemorrhagic puncta. The severe pruritus associated with bites can cause intense scratching leading to excoriations and the development of secondary infections. In the setting of chronic body lice infestation, frequently bitten areas of the skin can develop notable thickening and discoloration, a condition known as “vagabond’s disease” 17. Dermatologic findings tend to be most prominent in areas where clothing seams are in contact with the skin, such as the waist, groin, thighs, and axillary folds 18. Additional physical exam findings including cervical lymphadenopathy and conjunctivitis are often present.
Unlike head and pubic lice, infestation with body lice is typically diagnosed by finding eggs and lice in seams of clothing rather than on the skin 15. Therefore, an important component of the exam in patients suspected of having body lice includes careful inspection of their clothing. In addition to lice, indirect findings such as blood stains or louse feces may be discovered.
Pediculosis corporis treatment
A body lice infestation is treated by improving the personal hygiene of the infested person, including assuring a regular (at least weekly) change of clean clothes. Clothing, bedding, and towels used by the infested person should be laundered using hot water (at least 130°F [54.4 °C]) and machine dried using the hot cycle.
Sometimes the infested person also is treated with a pediculicide, a medicine that can kill lice; however, a pediculicide generally is not necessary if hygiene is maintained and items are laundered appropriately at least once a week. A pediculicide should be applied exactly as directed on the bottle or by your physician.
If you choose to treat, guidelines for the choice of the pediculicide are the same as for head lice (see Pediculosis treatment below).
Pediculosis pubis
Pediculosis pubis also called Pthirus pubi or pubic lice or crab lice or crabs, is a louse (a type of wingless, bloodsucking insect) that can live and multiply (infest) on skin that grows pubic hair. Pediculosis pubis (pubic lice) most commonly affect the pubic hair, but other hair-bearing areas, such as the armpits and eyelashes, eyebrows, or scalp, may also be affected. Pubic lice infestations (pthiriasis) usually causes itching, but it can occur without any symptoms.
Pediculosis pubis (pubic lice) are spread through sexual contact and are most common in adults. Occasionally pubic lice may be spread by close personal contact or contact with articles such as clothing, bed linens, and towels that have been used by an infested person. Pubic lice found on the head or eyelashes of children may be an indication of sexual exposure or abuse.
Pubic lice infestations may occur with other sexually transmitted diseases. Dogs, cats, and other pets do not play a role in the transmission of human lice.
Pubic lice do not transmit disease; however, secondary bacterial infection can occur from scratching of the skin.
Adult pubic lice are 1.1–1.8 mm in length. Pubic lice typically are found attached to hair in the pubic area but sometimes are found on coarse hair elsewhere on the body (for example, eyebrows, eyelashes, beard, mustache, chest, armpits, etc.).
Men are more commonly affected by public lice, possibly because they have more coarse body hair.
This infestation is most frequent between the ages of 15–40 in people who are sexually active.
Both over-the-counter and prescription medications are available for treatment of pubic lice infestations.
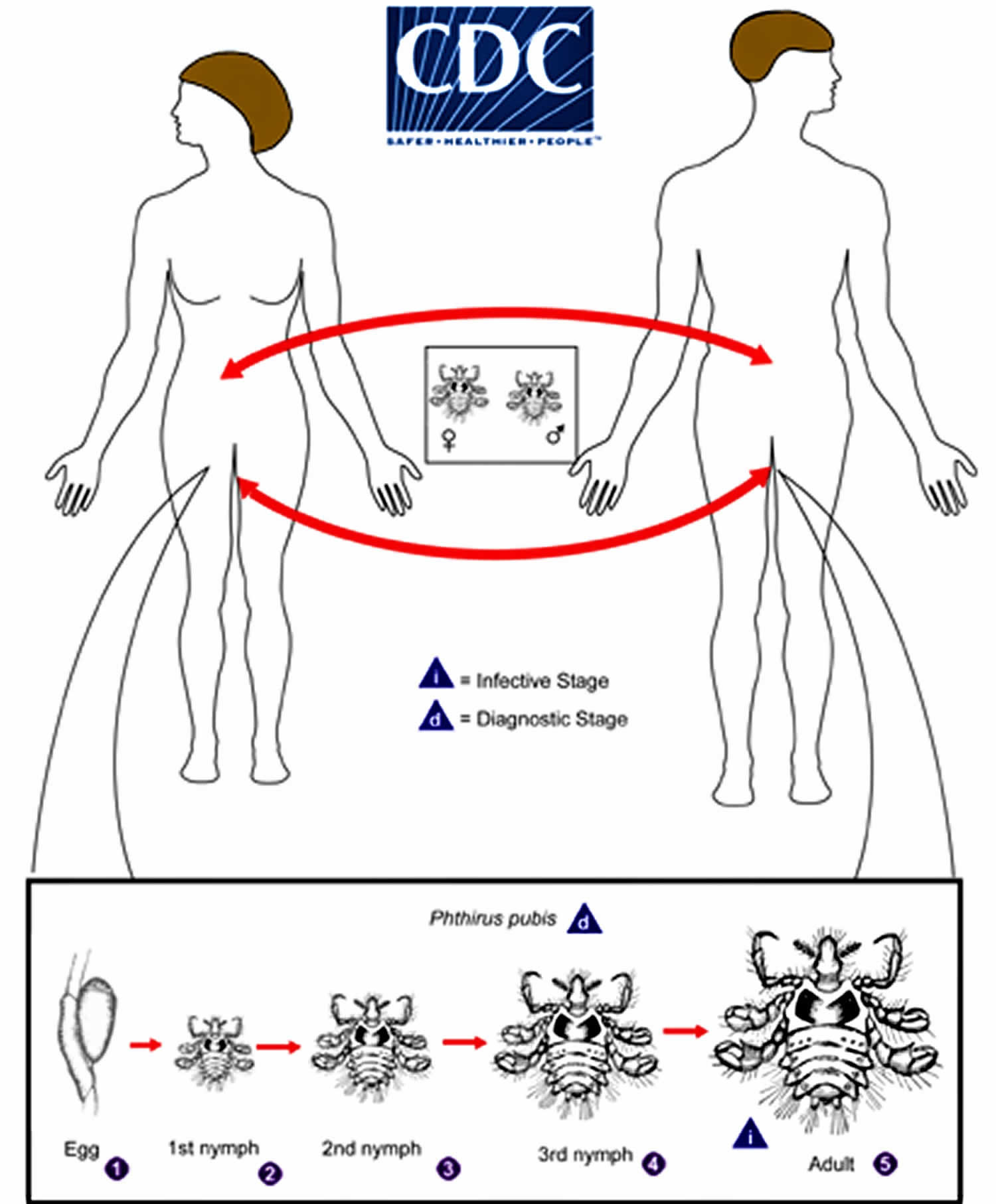
Figure 3. Pediculosis pubis
Where are pubic lice found?
Pubic lice usually are found in the genital area on pubic hair; but they may occasionally be found on other coarse body hair, such as hair on the legs, armpits, mustache, beard, eyebrows, or eyelashes. Pubic lice on the eyebrows or eyelashes of children may be a sign of sexual exposure or abuse. Lice found on the head generally are head lice, not pubic lice.
Animals do not get or spread pubic lice.
How do I get pubic lice?
Pubic lice usually are spread through sexual contact and are most common in adults. Pubic lice found on children may be a sign of sexual exposure or abuse. Occasionally, pubic lice may be spread by close personal contact or contact with articles such as clothing, bed linens, or towels that have been used by an infested person. A common misconception is that pubic lice are spread easily by sitting on a toilet seat. This would be extremely rare because lice cannot live long away from a warm human body and they do not have feet designed to hold onto or walk on smooth surfaces such as toilet seats.
Persons infested with pubic lice should be examined for the presence of other sexually transmitted diseases.
Pediculosis pubis life cycle
Phthirus pubis, the pubic or crab louse, is an insect of the order Psocodea and is an ectoparasite whose only host are humans. Pubic lice (Phthirus pubis) have three stages: egg, nymph and adult. Eggs (nits) are laid on a hair shaft (number 1). Females will lay approximately 30 eggs during their 3–4 week life span. Eggs hatch after about a week and become nymphs, which look like smaller versions of the adults. The nymphs undergo three molts (number 2, number 3 and number 4) before becoming adults (number 5). Adults are 1.5–2.0 mm long and flattened. They are much broader in comparison to head and body lice. Adults are found only on the human host and require human blood to survive. If adults are forced off the host, they will die within 24–48 hours without a blood feeding. Pubic lice are transmitted from person to person most-commonly via sexual contact, although fomites (bedding, clothing) may play a minor role in their transmission.
Figure 4. Pediculosis pubis life cycle
Pediculosis pubis risk factors
Pubic (“crab”) lice infestation is found worldwide and occurs in all races and ethnic groups and in all levels of society. Pubic lice usually are spread through sexual contact and are most common in adults. Occasionally pubic lice may be spread by close personal contact or contact with articles such as clothing, bed linens, and towels that have been used by an infested person. Pubic lice found on the head or eyelashes of children may be an indication of sexual exposure or abuse.
Pubic lice do not transmit disease; however, secondary bacterial infection can occur from scratching of the skin.
Pediculosis pubis prevention and control
Pubic (“crab”) lice most commonly are spread directly from person to person by sexual contact. Pubic lice very rarely may be spread by clothing, bedding, or a toilet seat.
The following are steps that can be taken to help prevent and control the spread of pubic (“crab”) lice:
- All sexual contacts of the infested person should be examined. All those who are infested should be treated.
- Sexual contact between the infested person(s)s and their sexual partner(s) should be avoided until all have been examined, treated as necessary, and reevaluated to rule out persistent infestation.
- Machine wash and dry clothing worn and bedding used by the infested person in the hot water (at least 130°F [54.4 °C]) laundry cycle and the high heat drying cycle.
- Clothing and items that are not washable can be dry-cleaned OR sealed in a plastic bag and stored for 2 weeks.
- Do not share clothing, bedding, and towels used by an infested person.
- Do not use fumigant sprays or fogs; they are not necessary to control pubic (“crab”) lice and can be toxic if inhaled or absorbed through the skin.
Persons with pubic lice should be examined and treated for any other sexually transmitted diseases (STDs) that may be present.
Pediculosis pubis symptoms
Pubic lice and their eggs (nits) may attach themselves to the hair in the pubic region and other areas. Lymph nodes in the groin area may be swollen. Slate blue spots may be seen at the bite sites. Itching (“pruritus”) in the pubic and groin area is the most common symptom of pubic lice infestation. As with other lice infestations, intense itching leads to scratching which can cause sores and secondary bacterial infection of the skin.
Pubic (“crab”) lice are not known to transmit any disease.
Visible lice eggs (“nits”) or lice crawling or attached to pubic hair, or less commonly other hairy areas of the body (eyelashes, eyebrows, beard, mustache, armpits, chest, back) are other signs of pubic lice infestation.
Pubic lice on the head (eyelashes or eyebrows) of a child may be an indication of sexual exposure or abuse.
Persons infested with pubic lice should be evaluated for other sexually transmitted diseases (STDs).
Pediculosis pubis diagnosis
Pubic lice are short and crab-like and appear very different from head and body lice. Pubic lice infestation is diagnosed by finding a “crab” louse or eggs on hair in the pubic region or, less commonly, elsewhere on the body (eyebrows, eyelashes, beard, mustache, armpit, perianal area, groin, trunk, scalp). Although pubic lice and nits can be large enough to be seen with the naked eye, a magnifying lens may be necessary to find lice or eggs.
Pediculosis pubis treatment
A lice-killing lotion containing 1% permethrin or a mousse containing pyrethrins and piperonyl butoxide can be used to treat pubic (“crab”) lice. These products are available over-the-counter without a prescription at a local drug store or pharmacy. These medications are safe and effective when used exactly according to the instructions in the package or on the label.
Lindane shampoo is a prescription medication that can kill lice and lice eggs. However, lindane is not recommended as a first-line therapy. Lindane can be toxic to the brain and other parts of the nervous system; its use should be restricted to patients who have failed treatment with or cannot tolerate other medications that pose less risk. Lindane should not be used to treat premature infants, persons with a seizure disorder, women who are pregnant or breast-feeding, persons who have very irritated skin or sores where the lindane will be applied, infants, children, the elderly, and persons who weigh less than 110 pounds.
Malathion* lotion 0.5% (Ovide*) is a prescription medication that can kill lice and some lice eggs; however, malathion lotion (Ovide*) currently has not been approved by the U.S. Food and Drug Administration (FDA) for treatment of pubic (“crab”) lice.
Both topical and oral ivermectin have been used successfully to treat lice; however, only topical ivermectin lotion currently is approved by the U.S. Food and Drug Administration (FDA) for treatment of lice. Oral ivermectin is not FDA-approved for treatment of lice.
How to treat pubic lice infestations:
(Warning: See special instructions for treatment of lice and nits on eyebrows or eyelashes. The lice medications described in this section should not be used near the eyes.)
- Wash the infested area; towel dry.
- Carefully follow the instructions in the package or on the label. Thoroughly saturate the pubic hair and other infested areas with lice medication. Leave medication on hair for the time recommended in the instructions. After waiting the recommended time, remove the medication by following carefully the instructions on the label or in the box.
- Following treatment, most nits will still be attached to hair shafts. Nits may be removed with fingernails or by using a fine-toothed comb.
- Put on clean underwear and clothing after treatment.
- To kill any lice or nits remaining on clothing, towels, or bedding, machine-wash and machine-dry those items that the infested person used during the 2–3 days before treatment. Use hot water (at least 130°F [54.4 °C]) and the hot dryer cycle.
- Items that cannot be laundered can be dry-cleaned or stored in a sealed plastic bag for 2 weeks.
- All sex partners from within the previous month should be informed that they are at risk for infestation and should be treated.
- Persons should avoid sexual contact with their sex partner(s) until both they and their partners have been successfully treated and reevaluated to rule out persistent infestation.
- Repeat treatment in 9–10 days if live lice are still found.
- Persons with pubic lice should be evaluated for other sexually transmitted diseases (STDs).
Special instructions for treatment of lice and nits found on eyebrows or eyelashes:
- If only a few live lice and nits are present, it may be possible to remove these with fingernails or a nit comb.
- If additional treatment is needed for lice or nits on the eyelashes, careful application of ophthalmic-grade petrolatum ointment (only available by prescription) to the eyelid margins 2–4 times a day for 10 days is effective. Regular petrolatum (e.g., Vaseline)* should not be used because it can irritate the eyes if applied.
Cutting the eyelashes is a radical technique. Physical removal of lice and nits from the eyelashes using forceps may be difficult in non-cooperative patients such as children. The use of botulinum toxin A, at the concentration of 2.5 units per 0.1 ml applied with a swab stick on the eyelashes, may be a cost-effective adjunctive treatment which facilitates physical removal since it induces paralysis of the lice preventing them from adhering to the eyelashes 19.
Several topical treatments may be used in eyelashes infestation with Pthirus pubis (phthiriasis palpebrarum). Yellow mercuric oxide ophthalmic ointment, parasympathomimetic agents (physostigmine, pilocarpine), 20% fluorescein, and liquid petrolatum ointment have been reported to be efficient on lice and nits 19. Topical antiparasitic agents such as natural pyrethrins, pyrethroids, malathion, and lindane may also be prescribed 19.
Parasite destruction may be an alternative to physical removal or topical treatment. Cryotherapy with liquid nitrogen performed under the slit lamp was reported to be efficient by some authors 19. Some authors have proposed argon laser therapy as an effective treatment for phthiriasis palpebrarum. One session using a 200-micron beam, with duration of 0.1 seconds, and a power of 0.2 W allowed the destruction of both lice and nits. However, this device necessitates a strict eye protection and may not be available on a large scale 19.
Oral ivermectin may be used as a single dose treatment; however, a second dose may be necessary after seven to 10 days to control newly hatched nits 19. Oral ivermectin is contraindicated in children younger than five years old and/or weighing less than 15 kilograms, as well as in pregnant and lactating women.
Treatment of associated body hair infestation, using antiparasitic topical and/or shaving is mandatory.
Clothing, bedding including pillowcases, and towels should be washed at least 130°F [54.4 °C] for half an hour and then heat dried for up to 10 minutes to eliminate both lice and nits. All sexual contacts and family members of a person having phthiriasis palpebrarum should be evaluated for the presence of phthiriasis pubis and phthiriasis palpebrarum, and if necessary, they have to be treated. The effect of such measures in preventing recontamination has been proven.
Pediculosis capitis
Pediculosis capitis or head lice, is a common, highly contagious infection that often occurs in nurseries, day care centers, and schools. Pediculosis capitis is caused by infestation with the human head louse, Pediculus humanus capitis, and it is usually very itchy.
Head lice are very small insects that feed on human blood. Adult head lice are roughly 2–3 mm long. The female louse attaches her eggs (nits) to the base of the hair near the scalp, and the nits hatch 7–10 days later. While the adult louse cannot survive for more than 2 days off the human head, a nit can stay alive for up to 10 days off the body (for example, on clothes, hairbrushes, or carpets). Head lice are spread from child to child by close head-to-head contact and by sharing belongings that are infested with head lice. Spread by contact with clothing (such as hats, scarves, coats) or other personal items (such as combs, brushes, or towels) used by an infested person is uncommon. Personal hygiene or cleanliness in the home or school has nothing to do with getting head lice.
Dogs, cats, and other pets do not play a role in the transmission of human lice.
Head lice move by crawling; they cannot hop or fly.
Head lice are found worldwide. In the United States, infestation with head lice is most common among pre-school children attending child care, elementary schoolchildren, and the household members of infested children. Although reliable data on how many people in the United States get head lice each year are not available, an estimated 6 million to 12 million infestations occur each year in the United States among children 3 to 11 years of age. In the United States, infestation with head lice is much less common among African-Americans than among persons of other races, possibly because the claws of the of the head louse found most frequently in the United States are better adapted for grasping the shape and width of the hair shaft of other races.
Both over-the-counter and prescription medications are available for treatment of head lice infestations.
Pediculosis capitis life cycle
Pediculus humanus capitis, the head louse, is an insect of the order Psocodea and is an ectoparasite whose only host are humans. The louse feeds on blood several times daily and resides close to the scalp to maintain its body temperature.
The life cycle of the head louse has three stages: egg, nymph, and adult (see Pediculosis life cycle in Figure 2 above).
Eggs: Nits are head lice eggs. They are hard to see and are often confused for dandruff or hair spray droplets. Nits are laid by the adult female and are cemented at the base of the hair shaft nearest the scalp (number 1). They are 0.8 mm by 0.3 mm, oval and usually yellow to white. Nits take about 1 week to hatch (range 6 to 9 days). Viable eggs are usually located within 6 mm of the scalp.
Nymphs: The egg hatches to release a nymph (number 2). The nit shell then becomes a more visible dull yellow and remains attached to the hair shaft. The nymph looks like an adult head louse, but is about the size of a pinhead. Nymphs mature after three molts (number 3 and number 4) and become adults about 7 days after hatching.
Adults: The adult louse is about the size of a sesame seed, has 6 legs (each with claws), and is tan to grayish-white (number 5). In persons with dark hair, the adult louse will appear darker. Females are usually larger than males and can lay up to 8 nits per day. Adult lice can live up to 30 days on a person’s head. To live, adult lice need to feed on blood several times daily. Without blood meals, the louse will die within 1 to 2 days off the host.
Pediculosis capitis risk factors
In the United States, infestation with head lice (Pediculus humanus capitis) is most common among preschool- and elementary school-age children and their household members and caretakers. Head lice are not known to transmit disease; however, secondary bacterial infection of the skin resulting from scratching can occur with any lice infestation.
Getting head lice is not related to cleanliness of the person or his or her environment.
Head lice are mainly spread by direct contact with the hair of an infested person. The most common way to get head lice is by head-to-head contact with a person who already has head lice. Such contact can be common among children during play at:
- school,
- home, and
- elsewhere (e.g., sports activities, playgrounds, camp, and slumber parties).
Uncommonly, transmission may occur by:
- wearing clothing, such as hats, scarves, coats, sports uniforms, or hair ribbons worn by an infested person;
- using infested combs, brushes or towels; or
- lying on a bed, couch, pillow, carpet, or stuffed animal that has recently been in contact with an infested person.
Reliable data on how many people get head lice each year in the United States are not available; however, an estimated 6 million to 12 million infestations occur each year in the United States among children 3 to 11 years of age. Some studies suggest that girls get head lice more often than boys, probably due to more frequent head-to-head contact.
In the United States, infestation with head lice is much less common among African-Americans than among persons of other races. The head louse found most frequently in the United States may have claws that are better adapted for grasping the shape and width of some types of hair but not others.
Pediculosis capitis symptoms
Head lice are not known to transmit any disease and therefore are not considered a health hazard.
Head lice infestations can be asymptomatic, particularly with a first infestation or when an infestation is light. Itching (“pruritus”) is the most common symptom of head lice infestation and is caused by an allergic reaction to louse bites. It may take 4–6 weeks for itching to appear the first time a person has head lice.
Other symptoms may include:
- a tickling feeling or a sensation of something moving in the hair;
- irritability and sleeplessness; and
- sores on the head caused by scratching. These sores caused by scratching can sometimes become infected with bacteria normally found on a person’s skin.
Pediculosis capitis diagnosis
Misdiagnosis of head lice infestation is common. The diagnosis of head lice infestation is best made by finding a live nymph or adult louse on the scalp or hair of a person.
Because adult and nymph lice are very small, move quickly, and avoid light, they may be difficult to find. Use of a fine-toothed louse comb may facilitate identification of live lice.
If crawling lice are not seen, finding nits attached firmly within ¼ inch of the base of hair shafts suggests, but does not confirm, the person is infested. Nits frequently are seen on hair behind the ears and near the back of the neck. Nits that are attached more than ¼ inch from the base of the hair shaft are almost always non-viable (hatched or dead). Head lice and nits can be visible with the naked eye, although use of a magnifying lens may be necessary to find crawling lice or to identify a developing nymph inside a viable nit. Nits are often confused with other particles found in hair such as dandruff, hair spray droplets, and dirt particles.
If no nymphs or adults are seen, and the only nits found are more than ¼ inch from the scalp, then the infestation is probably old and no longer active — and does not need to be treated.
Pediculosis symptoms
Intense itch is the usual symptom but the degree of itch does vary among individuals. With the first infestation, it may take 2 to 6 weeks before itching starts. In repeat infestations, itching develops within the first 24 to 48 hours. In some people, infestations do not produce symptoms.
- Pediculosis capitis (head lice): Evidence of head lice infestation includes scratches, redness and scaliness of the scalp and back of the neck. Head lice, eggs (nits) and empty egg cases are visible in many cases. The bites can occasionally become infected. This results in small sores with tender glands in the neck (lymphadenopathy).
- Pediculosis corporis (body lice): The body louse causes night time itch, particularly in the underarms, trunk and groin regions (i.e. areas most often covered by clothing). Nits are rarely found on the individual’s skin as the louse lives primarily on the clothing. Bites present as tiny red lumps with a red base. Crusts and scratches are occasionally complicated by bacterial infections and lymph node enlargement.
- Pediculosis pubis (pubic lice): The lice are most often found within the pubic hair. However, they can spread to other hairy parts of the body. Eyelashes or eyebrows can also be infested. Blood specks on underclothes and live lice may be seen moving in the pubic hair. Tiny bleeding spots or bite marks, scratches, secondary bacterial infection and enlarged lymph glands may be present. When the eyelashes are affected, dark flecks can form that look like mascara. Blue spots may be visible at feeding sites.
What other problems can occur with pediculosis?
- Itching commonly leads to excoriations (scratch marks) and secondary bacterial infection.
- Upon diagnosis of pubic lice a screen for other sexually transmitted infections (STIs) should be done
- In some countries the body louse transmits diseases such as epidemic typhus, trench fever and louse-borne relapsing fever.
Pediculosis diagnosis
Diagnosis of infestation requires identification of a live louse and/or a viable nit under the microscope. On physical examination, the diagnosis is confirmed by visualization of at least one louse on visual inspection. It is easier to identify and remove live lice by wet combing using a lice comb.
Use of a bright light, magnifying lens, or fine-toothed comb lice comb can aid in diagnosis. Misdiagnosis is common. Finding only nits on examination is not sufficient to confirm a current infestation, as nits can stay on hair for months after successful treatment. Additionally, dandruff, hair spray debris, and dirt particles can be confused with nits as false positives. When lice are found in one member of a family, all other family members in contact should also be examined for evidence of infestation.
Pubic lice are diagnosed by finding lice in the pubic hair, and should prompt a screening for other sexually-transmitted diseases. Presence of body lice should be considered in patients with pruritis who live in crowded conditions and/or have evidence of poor hygiene.
In most cases, one may use sticky tape over the infected area to pick up the lice and examine them under a microscope. A wood lamp examination may reveal greenish-yellow fluorescence of the nits and eggs. Sometimes the pubic hair may reveal the presence of lice and this is an indication for workup of a sexually transmitted infection 20.
Scrapings are often done to rule out a fungal infection when the diagnosis is not clear.
Pediculosis treatment
General guidelines and prevention
- All people infested with lice in a household and their infested close contacts and bedmates should be treated at the same time. Some experts believe prophylactic treatment is prudent for persons who share the same bed with actively-infested individuals. All infested persons (household members and close contacts) and their bedmates should be treated at the same time.
- Items used by the infested person must be machine washed with hot water and tumble dried.
- Items that cannot be laundered can be dry-cleaned or sealed in a plastic bag for 2 weeks.
- The floors and furniture should be vacuumed. However, the risk of getting infested by a louse that has fallen onto a rug, carpet or furniture is very small.
- Children should be taught not to share combs, brushes, hair accessories and towels.
- Soak combs and brushes in hot water (at least 130 °F [54.4 °C]) for 5 to 10 minutes.
- Dead nits may continue to adhere to hairs and this does not imply treatment failure.
- Nits can be removed with a comb designed specifically for that purpose. Use of a hair conditioner makes wet-combing easier. It is best done after treating with anti-lice insecticides. Repeat the combing at least twice more on consecutive nights if possible and then at least weekly until no lice are found on 3 consecutive occasions.
- When head lice are detected, notify the child’s school of the infestation. It is not necessary to exclude children from school after the initial treatment of head lice.
- Individuals with pubic louse infestation should be advised to avoid close body contact until they and their current sexual partner(s) have completed treatment and follow-up.
- Shaving pubic hair is beneficial as well as applying topical treatment to all hairy parts of the body apart from the eyelids and scalp. Any remaining nits should be removed by using a fine toothed comb.
- Use of a topical treatment is usually unnecessary with body louse infestation because the lice live on clothing. Treatment of clothing, bed linens and education about hygiene is most important.
Pharmacologic treatment of lice focuses on two mechanisms: neurotoxicity resulting in paralysis of the louse and suffocation of the louse from topical application. It is important to recognize that available treatments kill lice but do not reliably destroy eggs. Repeat treatment is sometimes required for complete eradication. A second treatment 7 to 10 days after the initial treatment is typically sufficient to eradicate most nonresistant lice.
Treat the infested person(s): Requires using an Over-the-counter (OTC) or prescription medication. Follow these treatment steps:
- Before applying treatment, it may be helpful to remove clothing that can become wet or stained during treatment.
- Apply lice medicine, also called pediculicide, according to the instructions contained in the box or printed on the label. If the infested person has very long hair (longer than shoulder length), it may be necessary to use a second bottle. Pay special attention to instructions on the label or in the box regarding how long the medication should be left on the hair and how it should be washed out.
- Have the infested person put on clean clothing after treatment.
- If a few live lice are still found 8–12 hours after treatment, but are moving more slowly than before, do not retreat. The medicine may take longer to kill all the lice. Comb dead and any remaining live lice out of the hair using a fine–toothed nit comb.
- If, after 8–12 hours of treatment, no dead lice are found and lice seem as active as before, the medicine may not be working. Do not retreat until speaking with your health care provider; a different pediculicide may be necessary. If your health care provider recommends a different pediculicide, carefully follow the treatment instructions contained in the box or printed on the label.
- Nit (head lice egg) combs, often found in lice medicine packages, should be used to comb nits and lice from the hair shaft. Many flea combs made for cats and dogs are also effective.
- After each treatment, checking the hair and combing with a nit comb to remove nits and lice every 2–3 days may decrease the chance of self–reinfestation.
- Continue to check for 2–3 weeks to be sure all lice and nits are gone. Nit removal is not needed when treating with spinosad topical suspension.
- Retreatment is meant to kill any surviving hatched lice before they produce new eggs. For some drugs, retreatment is recommended routinely about a week after the first treatment (7–9 days, depending on the drug) and for others only if crawling lice are seen during this period. Retreatment with lindane shampoo is not recommended.
Supplemental Measures
Head lice do not survive long if they fall off a person and cannot feed. You don’t need to spend a lot of time or money on housecleaning activities. Follow these steps to help avoid re–infestation by lice that have recently fallen off the hair or crawled onto clothing or furniture.
- Machine wash and dry clothing, bed linens, and other items that the infested person wore or used during the 2 days before treatment using the hot water (130°F [54.4 °C]) laundry cycle and the high heat drying cycle. Clothing and items that are not washable can be dry–cleaned
- OR sealed in a plastic bag and stored for 2 weeks.
- Soak combs and brushes in hot water (at least 130°F [54.4 °C]) for 5–10 minutes.
- Vacuum the floor and furniture, particularly where the infested person sat or lay. However, the risk of getting infested by a louse that has fallen onto a rug or carpet or furniture is very small. Head lice survive less than 1–2 days if they fall off a person and cannot feed; nits cannot hatch and usually die within a week if they are not kept at the same temperature as that found close to the human scalp. Spending much time and money on housecleaning activities is not necessary to avoid reinfestation by lice or nits that may have fallen off the head or crawled onto furniture or clothing.
- Do not use fumigant sprays; they can be toxic if inhaled or absorbed through the skin.
Multiple topical pediculicides are considered first-line treatments for lice infestation. These include pyrethroids, malathion, lindane, benzyl alcohol, topical ivermectin, and spinosad.
Pyrethroids are one of the most frequently used treatments for lice among topical agents. Permethrin 1% (Nix) is a synthetic pyrethroid and is widely used as a treatment and is available over-the-counter in the United States. Recent evidence suggests that resistance to permethrin has been increasing. It is retained on the hair after application and has a residual effect for up to 3 weeks, although a retreatment at 1 week is recommended. Although there is evidence of resistance, its generous safety profile with low toxicity makes it a favorable first-line agent.
Malathion 0.5% (Ovide) is an organophosphate cholinesterase inhibitor that causes respiratory paralysis in arthropods. It has a good margin of safety, but has an unappealing odor and requires an 8 to 12-hour treatment period.
Lindane 1% is an organochloride that kills lice by respiratory paralysis. It is absorbed into the blood and slowly metabolized and should not repeatedly be used. This agent has a potential for neurotoxicity and has been taken off of the market in California. It may be used as a second-line agent in adults but should be avoided in children, the elderly, or adults weighing less than 50 kg.
Benzyl alcohol 5% solution (Ulesfia) was approved in 2009 as a topical suffocation treatment that prevents lice from closing their respiratory spiracles. It appears to have an efficacy comparable to pyrethrins.
Spinosad 0.9% (Natroba) is a topical pediculicidal agent that was approved in 2011. It works by provoking hyperexcitation, causing death by paralysis. It was found to have twice the eradication rate of permethrin at 14 days and is effective after a single dose. It may be beneficial for patients not adherent to other therapies.
The only currently-used oral treatment for pediculosis is ivermectin. Ivermectin also has a risk of neurotoxicity has demonstrated effectiveness in clinical trials, but is not FDA-approved for the treatment of pediculosis. It may be an appropriate second-line therapy when the lice are resistant to topical treatments.
Body lice are eradicated through proper hygiene and laundering or application of insecticide to affected clothing. Pubic lice are commonly susceptible to agents used to treat head lice, although they vary in sensitivity.
Because lice can be present on inanimate fomites, heating infested clothing and bedding with hot water is necessary to destroy all stages of lice. The heat necessary for the destruction of lice and nits is 125.6 °F (52 °C) for 30 minutes. Lice have been found to become heat resistant through hormonal mechanisms, tolerating temperatures over 212 °F (100 °C).
Tips on treating head lice:
- Do not use extra amounts of any lice medication unless instructed to do so by your physician and pharmacist. The drugs used to treat lice are insecticides and can be dangerous if they are misused or overused.
- All the medications listed above should be kept out of the eyes. If they get onto the eyes, they should be immediately flushed away.
- Do not treat an infested person more than 2–3 times with the same medication if it does not seem to be working. This may be caused by using the medicine incorrectly or by resistance to the medicine. Always seek the advice of your health care provider if this should happen. He/she may recommend an alternative medication.
- Do not use different head lice drugs at the same time unless instructed to do so by your physician and pharmacist.
Topical agents
- It is important to read the instructions before applying the treatment to ensure that the medication has been left on for the appropriate amount of time and washed off properly.
- Not all eggs are killed with one application of topical medicine, therefore a second application is recommended 7 to10 days later (the time needed for the eggs to hatch).
- Various topical pediculicidal agents are available: Pyrethrum shampoos and permethrin 1% are available over the counter; permethrin 5%, malathion 0.5% (Ovide®), lindane, topical ivermectin (Sklice®), and spinosad are prescription agents.
- Occlusive products offer an alternative to pediculicides and include: benzyl alcohol lotion 5%, and 4% dimethicone lotion.
- Other occlusive treatments include vinegar, mayonnaise, petroleum jelly, olive oil, butter, etc. However, most of these have not been scientifically evaluated.
- The same pediculicides used for head louse infestation are also used for pubic and body louse infestation
- Eyelash infestation can be treated effectively with ophthalmic-grade petrolatum.
Over-the-counter Medications
Many head lice medications are available “Over-the-counter” without a prescription at a local drug store or pharmacy. Each Over-the-counter product approved by the FDA for the treatment of head lice contains one of the following active ingredients. If crawling lice are still seen after a full course of treatment contact your health care provider.
- Pyrethrins combined with piperonyl butoxide (brand name products: A–200*, Pronto*, R&C*, Rid*, Triple X*.)
Pyrethrins are naturally occurring pyrethroid extracts from the chrysanthemum flower. Pyrethrins are safe and effective when used as directed. Pyrethrins can only kill live lice, not unhatched eggs (nits). A second treatment is recommended 9 to 10 days after the first treatment to kill any newly hatched lice before they can produce new eggs. Pyrethrins generally should not be used by persons who are allergic to chrysanthemums or ragweed. Pyrethrin is approved for use on children 2 years of age and older.
- Permethrin lotion 1% (brand name product: Nix*)
Permethrin is a synthetic pyrethroid similar to naturally occurring pyrethrins. Permethrin lotion 1% is approved by the FDA for the treatment of head lice. Permethrin is safe and effective when used as directed. Permethrin kills live lice but not unhatched eggs. Permethrin may continue to kill newly hatched lice for several days after treatment. A second treatment often is necessary on day 9 to kill any newly hatched lice before they can produce new eggs. Permethrin is approved for use on children 2 months of age and older.
Prescription Medications
The following medications, in alphabetical order, approved by the U.S. Food and Drug Administration (FDA) for the treatment of head lice are available only by prescription. If crawling lice are still seen after a full course of treatment, contact your health care provider.
- Benzyl alcohol lotion 5% (brand name product: Ulesfia lotion*)
Benzyl alcohol is an aromatic alcohol. Benzyl alcohol lotion, 5% has been approved by the FDA for the treatment of head lice and is considered safe and effective when used as directed. It kills lice but it is not ovicidal. A second treatment is needed 7 days after the first treatment to kill any newly hatched lice before they can produce new eggs. Benzyl alcohol lotion is intended for use on persons who are 6 months of age and older and its safety in persons aged more 60 years has not been established. It can be irritating to the skin.
- Ivermectin lotion 0.5% (brand name product: Sklice*)
Ivermectin lotion, 0.5% was approved by the FDA in 2012 for treatment of head lice in persons 6 months of age and older. It is not ovicidal, but appears to prevent nymphs (newly hatched lice) from surviving. It is effective in most patients when given as a single application on dry hair without nit combing. It should not be used for retreatment without talking to a healthcare provider.
Given as a tablet in mass drug administrations, oral ivermectin has been used extensively and safely for over two decades in many countries to treat filarial worm infections. Although not FDA-approved for the treatment of lice, ivermectin tablets given in a single oral dose of 200 micrograms/kg or 400 micrograms/kg repeated in 9-10 days has been shown effective against head lice. It should not be used in children weighing less than 15 kg or in pregnant women.
- Malathion lotion 0.5% (brand name product: Ovide*)
Malathion is an organophosphate. The formulation of malathion approved in the United States for the treatment of head lice is a lotion that is safe and effective when used as directed. Malathion is pediculicidal (kills live lice) and partially ovicidal (kills some lice eggs). A second treatment is recommended if live lice still are present 7–9 days after treatment. Malathion is intended for use on persons 6 years of age and older. Malathion can be irritating to the skin. Malathion lotion is flammable; do not smoke or use electrical heat sources, including hair dryers, curlers, and curling or flat irons, when applying malathion lotion and while the hair is wet.
- Spinosad 0.9% topical suspension (brand name product: Natroba*)
Spinosad is derived from soil bacteria. Spinosad topical suspension, 0.9%, was approved by the FDA in 2011. Since it kills live lice as well as unhatched eggs, retreatment is usually not needed. Nit combing is not required. Spinosad topical suspension is approved for the treatment of children 6 months of age and older. It is safe and effective when used as directed. Repeat treatment should be given only if live (crawling) lice are seen 7 days after the first treatment.
For second–line treatment only:
- Lindane shampoo 1%
Lindane is an organochloride. The American Academy of Pediatrics (AAP) no longer recommends it as a pediculocide. Although lindane shampoo 1% is approved by the FDA for the treatment of head lice, it is not recommended as a first–line treatment. Overuse, misuse, or accidentally swallowing lindane can be toxic to the brain and other parts of the nervous system; its use should be restricted to patients for whom prior treatments have failed or who cannot tolerate other medications that pose less risk. Lindane should not be used to treat premature infants, persons with HIV, a seizure disorder, women who are pregnant or breast–feeding, persons who have very irritated skin or sores where the lindane will be applied, infants, children, the elderly, and persons who weigh less than 110 pounds. Retreatment should be avoided.
Oral agents
Ivermectin is an option for individuals whose disease is resistant to topical therapies.
What happens when head lice treatment fails?
Failure to eradicate lice is a common and frustrating problem. There may be a number of reasons for this:
- Re-infestation from another person or from contaminated clothes, hats, etc.
- Resistance of lice to insecticides or improperly applied treatment. If a course of one kind of insecticide treatment fails, a different insecticide may be selected for the next course.
- Incorrect diagnosis of inactive infection. It is important to look for active lice not just nits.
Pediculosis prognosis
Most of the time, lice are killed with the proper treatment. However, lice can come back if you do not get rid of them at the source.
- Bragg BN, Simon LV. Pediculosis Humanis (Lice, Capitis, Pubis) [Updated 2019 Jan 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470343[↩][↩]
- Head Lice Parasites. https://www.cdc.gov/parasites/lice/head[↩][↩][↩][↩][↩]
- Veraldi S, Rossi LC, Pontini P. Head lice in African children. G Ital Dermatol Venereol. 2018 Aug;153(4):580-581[↩]
- Peterson AR, Nash E, Anderson BJ. Infectious Disease in Contact Sports. Sports Health. 2019 Jan/Feb;11(1):47-58[↩]
- Pediculosis and Pthiriasis (Lice Infestation). https://emedicine.medscape.com/article/225013-overview[↩]
- Shakya M, Jayraw AK, Singh M. Pubic lice infestation in man from Mhow, Madhya Pradesh. J Parasit Dis. 2018 Sep;42(3):402-404[↩]
- Çetinkaya Ü, Şahin S, Ulutabanca RÖ. The Epidemiology of Scabies and Pediculosis in Kayseri. Turkiye Parazitol Derg. 2018 Jun;42(2):134-137[↩]
- Falagas ME, Matthaiou DK, Rafailidis PI, Panos G, Pappas G. Worldwide prevalence of head lice. Emerg Infect Dis. 2008 Sep. 14(9):1493-4.[↩]
- Mumcuoglu KY, Gallili N, Reshef A, Brauner P, Grant H. Use of human lice in forensic entomology. J Med Entomol. 2004 Jul. 41(4):803-6[↩]
- Sanchezruiz WL, Nuzum DS, Kouzi SA. Oral ivermectin for the treatment of head lice infestation. Am J Health Syst Pharm. 2018 Jul 01;75(13):937-943[↩]
- Veracz A, Raoult D. 2012. Biology and genetics of human head and body lice. Trends in Parasitology. 28: 563-571[↩]
- Bechah Y, Capo C, Mege JL, Raoult D. Epidemic typhus. Lancet Infect Dis. 2008 Jul;8(7):417-26[↩][↩]
- Bonilla DL, Durden LA, Eremeeva ME, Dasch GA. The biology and taxonomy of head and body lice–implications for louse-borne disease prevention. PLoS Pathog. 2013;9(11):e1003724[↩][↩]
- Powers J, Badri T. Pediculosis Corporis. [Updated 2019 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482148[↩][↩]
- Sangaré AK, Doumbo OK, Raoult D. Management and Treatment of Human Lice. Biomed Res Int. 2016;2016:8962685[↩][↩][↩][↩]
- Ko CJ, Elston DM. Pediculosis. J. Am. Acad. Dermatol. 2004 Jan;50(1):1-12; quiz 13-4[↩]
- Body lice parasites. https://www.cdc.gov/parasites/lice/body/index.html[↩]
- Ko CJ, Elston DM. Pediculosis. J. Am. Acad. Dermatol. 2004 Jan;50(1):1-12; quiz 13-4.[↩]
- Badri T, Hafsi W. Phthiriasis Palpebrarum. [Updated 2019 Jan 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459226[↩][↩][↩][↩][↩][↩]
- Yingklang M, Sengthong C, Haonon O, Dangtakot R, Pinlaor P, Sota C, Pinlaor S. Effect of a health education program on reduction of pediculosis in school girls at Amphoe Muang, Khon Kaen Province, Thailand. PLoS ONE. 2018;13(6):e0198599[↩]





{kind=link}