Contents
- What is photodynamic therapy
- What is photodynamic therapy used for?
- Pros and cons of photodynamic therapy
- Photodynamic therapy for psoriasis
- Photodynamic therapy for acne
- Photodynamic therapy for skin cancer
- Photodynamic therapy for cancer
- Photodynamic therapy side effects
What is photodynamic therapy
Photodynamic therapy is a non-invasive treatment that uses special drugs, called photosensitizing agents, along with high-intensity light energy, such as from lasers, to kill cancer cells and treat inflammatory and infectious skin diseases. Photodynamic therapy is also sometimes used off-label for facial rejuvenation and to treat mild to moderate acne. The drugs (photosensitizing agents) only work after they have been activated or “turned on” by certain kinds of light. Photodynamic therapy may also be called photoradiation therapy, phototherapy, or photochemotherapy.
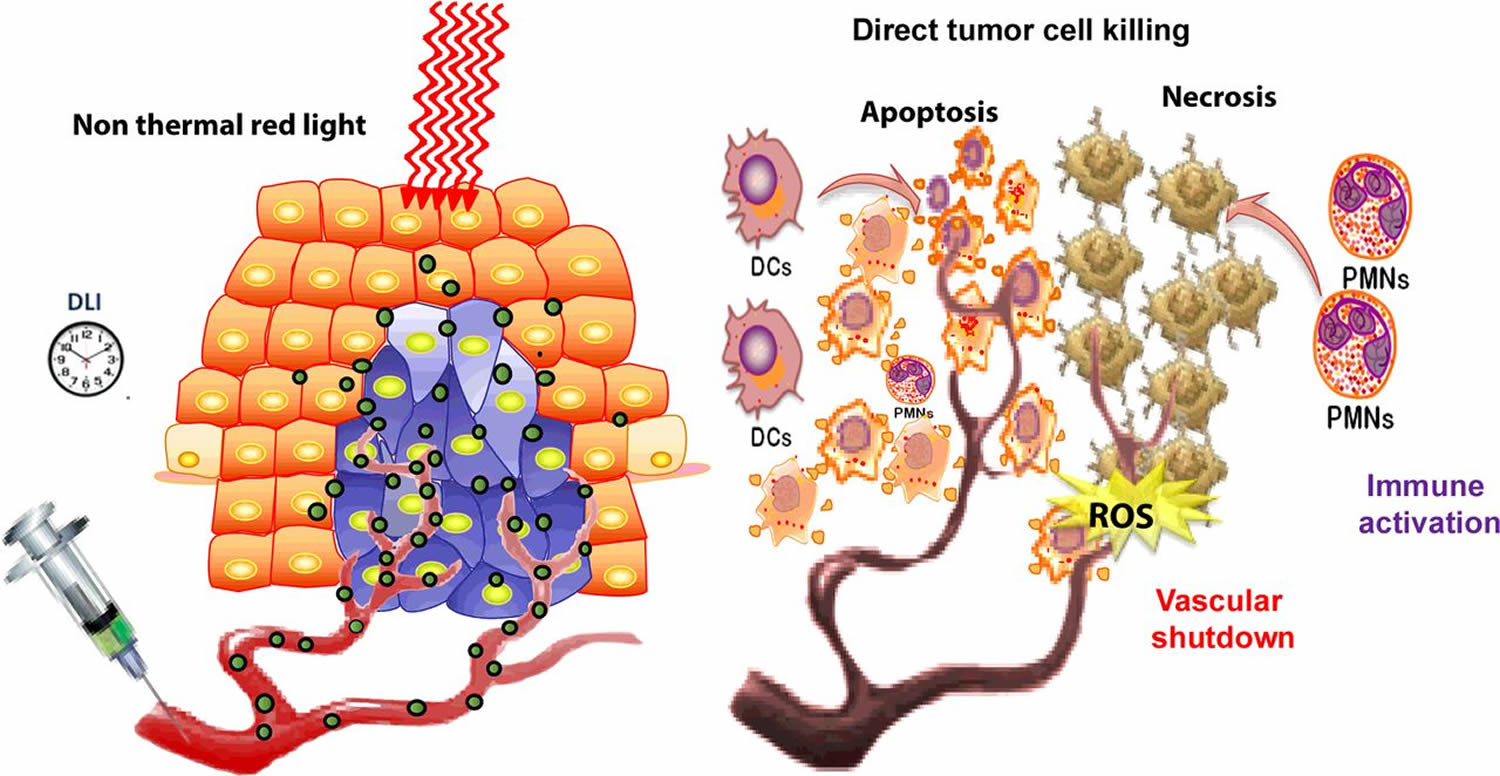
Depending on the part of the body being treated, the photosensitizing agent is either put into the bloodstream through a vein or put on your skin. Over a certain amount of time the drug is absorbed by the cancer cells. Then light is applied to the area to be treated. The light causes the drug to react with oxygen, which forms a chemical that kills the cells. Photodynamic therapy might also help by destroying the blood vessels that feed the cancer cells and by alerting the immune system to attack the cancer.
The period of time between when the drug is given and when the light is applied is called the drug-to-light interval. It can be anywhere from a couple of hours to a couple of days, depending on the drug used.
Photodynamic therapy can be done by topically applying the photosensitizer prodrug 5-aminolaevulinic acid (ALA) or its methylated ester of ALA (MAL), which are converted by the heme biosynthetic pathway predominantly to protoporphyrin IX 1. Subsequent activation by light of an appropriate wavelength produces reactive oxygen species (ROS), especially singlet oxygen, triggering both apoptosis and necrosis of target cells. Photodynamic therapy is a well-established treatment for actinic keratosis, in situ squamous cell carcinoma (Bowen’s disease), superficial and nodular basal cell carcinoma (BCC) 2. Experimental and clinical studies also demonstrated various anti-inflammatory effects and immunological activities of photodynamic therapy 3. The goal of Non Melanoma Skin Cancer treatment with photodynamic therapy is to achieve complete eradication of the tumor while preserving aesthetically and functionally important structures. Photodynamic therapy displays several major strengths: it is a non-invasive, easily repeatable, outpatient treatment that can be applied to wide areas of affected skin with an overall good profile of safety. Photodynamic therapy can be used in elderly patients in whom surgery is contraindicated, in immuno-depressed subjects, or to treat large or multiple lesions localized in poorly healing areas, i.e., lower legs. Moreover, photodynamic therapy shows superior cosmetic outcome compared with surgery and cryotherapy, with no scarring and pigmentary changes 4. Faced with the above listed advantages, photodynamic therapy is not without complications, with side effects that can be classified, according to the time of onset, in early (immediately or within days after treatment) and late (after weeks or months) onset side effects.
Photodynamic therapy drugs approved in the US to treat cancer
Several photosensitizing agents are currently approved by the US Food and Drug Administration (FDA) to treat certain cancers or pre-cancers.
Porfimer sodium (Photofrin®)
Porfimer sodium is the most widely used and studied photosensitizer. It’s activated by red light from a laser. It’s approved by the FDA to treat patients with:
- Cancer of the esophagus (the swallowing tube) to relieve symptoms when a tumor totally blocks the esophagus or partly blocks the esophagus and can’t be treated with laser therapy alone
- Barrett’s esophagus with dysplasia, a pre-cancerous condition that may lead to esophageal cancer in people who don’t have surgery
- A type of non-small cell lung cancer that affects the lining of the large breathing tubes (bronchi) called endobronchial cancer. Photodynamic therapy can help to shrink tumors that are blocking the bronchi. It’s used if there is very little spread of the cancer cells (the cancer is micro-invasive). Photodynamic therapy can help those who can’t have other types of treatment, such as surgery or radiation therapy.
Aminolevulinic acid (ALA or Levulan®)
Aminolevulinic acid (ALA) is a drug that’s put right on the skin. It’s used to treat actinic keratosis, a skin condition that can become cancer, and is used only on the face or scalp. A special blue light, rather than laser light, is used to activate this drug.
Methyl ester of ALA (Metvixia® cream)
Methyl ester of ALA (MAL) is one of several other forms of ALA that have been developed. A disadvantage of the older forms of aminolevulinic acid (ALA) is that they do not get into the cancer cells very easily. Newer ester forms, like this one, do. It is approved for treatment of some types of actinic keratoses of the face and scalp. Again, these are skin conditions that can become cancer. Methyl ester of ALA (MAL) is activated with a red light.
Newer photodynamic therapy drugs
Researchers are looking for new photodynamic therapy drugs, and many are being studied. Photodynamic therapy is also being tested for use against several other types of cancer. An example of one of these new drugs, Photochlor®, is now being used in clinical trials. Photochlor, or HPPH, is a second-generation photosensitizer. It’s being studied in the treatment of esophageal, lung, skin, and mouth and throat cancers. So far, studies have shown that photosensitivity lasts a much shorter time, and the drug is removed from the body much faster than porfimer sodium (Photofrin).
Studies are also being done to try to make photodynamic therapy work better and have fewer side effects. Scientists are looking at things like using ointments containing ferrous or cobalt ions and using hydrogen peroxide on the treated area to improve photodynamic therapy outcomes, but these studies are in their early stages and more research is needed.
What is photodynamic therapy used for?
Photodynamic therapy can be used in people with certain types of cancer to help them live longer and improve their quality of life. Although photodynamic therapy works and causes few long-term problems, it’s not widely used to treat cancer today. Still, it is offered in some treatment centers, and is being studied in many clinical trials. It’s becoming more widely recognized as a valuable treatment option for localized cancers (cancers that have not spread far from where they started).
Photodynamic therapy is also used to treat pre-cancers of the skin, and is being tested against pre-cancers in the mouth and other places.
Other light sources
Researchers are also looking at different types of lasers and other light sources. Some newer agents may respond to small doses of radiation as well as to light. This could allow doctors to use smaller amounts of radiation than the doses used in standard radiation therapy, which could lead to fewer side effects.
Combining treatments
Another exciting area of research is looking at the use of photodynamic therapy along with other therapies to make it more effective.
One example of this is to use photodynamic therapy during surgery to help keep cancer from coming back on large surface areas inside the body, such as the pleura (lining of the lung) and the peritoneum (lining of the belly or abdomen). The light treatment can be given while these areas are already exposed during the surgery. Cancers that start in the pleura or peritoneum are called mesotheliomas. These are also common sites of spread for some other types of cancer.
Interstitial treatments
Someday photodynamic therapy may be used to help treat larger solid tumors, too. A technique known as interstitial therapy involves using imaging tests (such as CT scans) to guide fiber optics directly into tumors using needles. This may be especially useful in areas that would require major surgery. Early results of studies of interstitial therapy in head and neck, prostate, and liver tumors have been promising.
Pros and cons of photodynamic therapy
Studies have shown that photodynamic therapy can work as well as surgery or radiation therapy in treating certain kinds of cancers and pre-cancers. It has some advantages, such as:
- It has no long-term side effects when used properly.
- It’s less invasive than surgery.
- It usually takes only a short time and is most often done as an outpatient.
- It can be targeted very precisely.
- Unlike radiation, photodynamic therapy can be repeated many times at the same site if needed.
- There’s usually little or no scarring after the site heals.
- It often costs less than other cancer treatments.
But photodynamic therapy has limits, too:
- photodynamic therapy can only treat areas where light can reach. This means it’s mainly used to treat problems on or just under the skin, or in the lining of organs that can be reached with a light source. Because light can’t travel very far through body tissues, photodynamic therapy can’t be used to treat large cancers or cancers that have grown deeply into the skin or other organs.
- photodynamic therapy can’t be used to treat cancers that have spread to many places.
- the drugs used for photodynamic therapy leave people very sensitive to light for some time, so special precautions must be taken after the drugs are put in or on the body.
- photodynamic therapy can’t be used in people who have certain blood diseases, such as any of the porphyrias (a rare group of diseases that affect the skin or nervous system) or people who are allergic to porphyrins. This allergy is rare, but it may happen in those who have gotten porphyrins in the past.
Photodynamic therapy for psoriasis
Psoriasis is a chronic, recurrent, and immune-mediated inflammatory disease that affects 2–3% of the world population. It is associated with genetic predisposition, autoimmune disorders, psychiatry and psychological health, environmental factors (e.g., infection, stress, trauma), and so on. The pathogenesis is closely related to abnormal interactions among innate immunity, T cells, keratinocytes, etc. Immune cells in the patients release excess proinflammatory factors, leading to uncontrollable activation of congenital and acquired immune system, such as nuclear factor-κB (NF-kB) signaling pathway and differentiation of T helper (Th) cells toward Th1 and/or Th17 cells 5. The complex pathogenesis results in tissue and organ damage over time, manifested by hyperproliferation, inflammation, and other clinical syndromes at the lesion sites. Therapeutic options for psoriasis can be divided into two aspects: systemic and topical treatments. The former involves immune inhibitors, like methotrexate, cyclosporine; retinoids (acitretin); immune modulators, such as glycyrrhizin, leflunomide 6. Additionally, newly developed biological agents have been employed to treat moderate to severe psoriasis with body surface area (BSA) greater than 10% or psoriasis area and severity index (PASI) higher than 10 7, including tumor necrosis factor α antagonists (etanercept, infliximab, etc.), alefacept, efalizumab, and ustekinumab 8. As for topical treatment that is mainly for mild or moderate psoriasis, it includes ointments (e.g., calcipotriol, calcineurin inhibitors, tretinoin, glucocorticoid), medicated bath with diastase or herbal extracts, and phototherapy. Phototherapy is an effective, safe, and accessible treatment without incurring any systemic side effects, in contrast to biologic agents or other drugs, especially for stable plaque psoriasis. Moreover, phototherapy can be combined with biologic agents for the treatment of severe psoriasis 9.
Although phototherapy is convenient to use without severe adverse events, inadequate choice of laser/light types or parameters or unnecessary laser exposure could cause erythema, skin burning, photoaging, etc. It is therefore critical for clinicians to properly choose a right light source for a special type of psoriasis.
Low-level light is also called “cold laser,” which involves ultraviolet, visible, and near infrared with much lower energy densities than those lasers used for ablation, cutting, and thermally coagulating tissues. Light sources of low-level light/laser therapy include LED, helium-neon (He-Ne, 632.8 nm), and gallium arsenide (GaAs) laser. LED is the complex semiconductor that converts electrical current into incoherent narrow spectrum light. LED or lasers at a wavelength ranging from 600 to 1070 nm have been widely applied to low-level light/laser therapy. Although longer wavelengths penetrate deeper, lasers at 700-770 nm have been found to limit biochemical activity 10. Blue light (400-480 nm) can reduce the proliferative activity of keratinocytes, modulate T cell immune responses, and safely improve plaque psoriasis 11. It is thus propitious to treat chronic hyperplastic and inflammatory dermatosis, such as psoriasis and atopic dermatitis. A prospective randomized study by comparing the efficacy of blue light (420 and 453 nm, LED) in treatment of psoriasis vulgaris once daily for 4 weeks showed significant improvement in either wavelength 12. Red light (620–770 nm) is able to deeply penetrate skin to about 6 mm 13, stimulate mitochondrial activity, and modulate cytokine release from macrophages to reduce topical inflammation 14. When patients with plaque psoriasis were treated sequentially with LED delivering continuous 830 and 633 nm in two 20-min sessions for 4 or 5 weeks, 60–100% of clearance rates were achieved without any significant side effects 15.
Low-level light is characterized by its ability to induce photobiological processes in cells. For instance, laser at 810 nm was shown to activate NF-kB in primary murine embryonic fibroblasts cells 16. In contrast, a combination of curcumin (anti-proliferation) with LED blue light, along with red light radiation in psoriasis, inhibited NF-κB activity, activated caspase-8/9, and downregulated the phosphorylation level of Akt and ERK 17. A growing number of investigations have demonstrated that low-level light can improve mitochondrial function under stress by increasing ATP synthesis, reactive oxygen species (ROS) generation, and cell redox activity 18. The beneficial functions of low-level light/laser therapy rely on its ability to activate cytochrome c oxidase at the mitochondrial respiratory chain. Cytochrome c oxidase has strong absorption of light at wavelengths ranging from 670 to 830 nm 19. Recent studies also showed that low-level light/laser therapy increased mitochondrial biogenesis in megakaryocytes, facilitating platelet biogenesis both in vivo and in vitro in preclinical studies 20. Finally, laser irradiation at green, red, or infrared wavelength with special parameters can change gene expression and release of various mediators in human and animal cells 21. low-level light/laser therapy has been also commonly used in a variety of conditions for acceleration of healing and relief of pain and inflammation, etc. 22. Its advantages of non-invasion, few side effects, and measurable benefits merit to be explored in the treatment of psoriasis.
Topical ALA-photodynamic therapy was inadequate for chronic plaque psoriasis because of variability in clinical responses and severe pain 23. Single intense pulsed light has been applied to vascular skin disease, such as facial telangiectasias and port-wine stains. At present, intense pulsed light has been widely used to photorejuvenation as non-invasive therapy either alone or in combination with the photosensitizer 24. A fewer literatures reported that intense pulsed light with 550-nm filter was effective to plaque psoriasis 25. In this regard, sunlight contains mainly UV and visible and infrared light, and UVB from the sun works the same way as UVB in phototherapy. Thus, multiple and short exposures to sunlight are recommended in psoriasis patients if they are tolerant to sunlight in the basis of clinical studies of phototherapy. Yet, natural sunbath is so unbound, rendering patients to the risks of photosensitivity and sunburn increase, and thus it should be carefully monitored. The patients should apply broad-spectrum sunscreen to all areas of unaffected skin and wear sunglasses during sunbath.
The outcome of phototherapy depends on a delicate balance between beneficial and detrimental effects of a specific laser. In comparison with other laser modalities, PUVA and UVB have the advantages of large radiation sizes, low price, and efficacy and safety that have been intensively demonstrated. In addition, PUVA has better effects than UVB on refractory psoriasis plaque and palmoplantar pustular psoriasis, but its side effects limit its broad application. Pulsed dye laser provides optimal outcomes on nail psoriasis compared with other lasers. The trails of low-level light/laser therapy are still limited, but the near infrared and visible red light with low energy show prospects for treating psoriasis due to its strong penetration and encouraging photomodulation. Intense pulsed light is rarely reported for the treatment of psoriasis, but photodynamic therapy-intense pulsed light has been found to offer a moderate effect on nail psoriasis.
Photodynamic therapy for acne
Acne vulgaris is a common adolescence disorder, affecting almost 80% of people mostly in their teens, with the most severity in females aged 14–17 and males aged 16–19 26. The prevalence is almost same for both sexes with a higher severity in males. Major factors in acne are hyperactivity of sebaceous glands and the involvement of acne proprium bacterium. Acne entails clinical manifestations and leaves scars in untreated cases and this makes it important mainly due to adverse effects on the patient’s self-confidence, social communication, and psychological functions that result in psychosocial and clinical disorders and even suicide 26. Even though various single and combinational treatments have been introduced, the best method is still controversial and this necessitates the search for less invasive, fast, more tolerable and efficient, and long-lasting options 27. Topical antibacterial agents are preferred to systemic treatments and benzoyl peroxide has distinct advantages among these topical options. Benzoyl peroxide is a nonantibiotic antibacterial agent and its keratolytic property reduces the sebaceous glands activity. Benzoyl peroxide is more effective than topical antibacterials, especially in inflamed lesions 28.
In recent decades, photodynamic therapy with the prodrug 5-aminolevulinic acid (ALA) or its ester derivative (eg, methyl ester of ALA or MAL) as a porphyrin precursor have been gaining increasing popularity and it is regarded as the most evidential treatment of all laser and light devices for acne by the U.S guidelines 29. Previous study reported that ALA is able to be absorbed and accumulated in sebaceous glands and then intracellularly converted to photosensitizer protoporphyrin IX (PpIX).4,5 When irradiated with special wavelength light, PpIX can produce reactive oxygen species (ROS) such as singlet oxygen and leads to a series of reactions. What’s more, photodynamic photorejuvenation has also been reported for this treating method 30.
A well conducted 2016 Cochrane Systematic Study 31 found high-quality evidence on the use of light therapies for people with acne is lacking. There is low certainty of the usefulness of MAL-photodynamic therapy (red light) or ALA-photodynamic therapy (blue light) as standard therapies for people with moderate to severe acne. The review authors 31 were unable to draw firm conclusions from the results of their review, as it was not clear whether the light therapies (including photodynamic therapy) assessed in their studies were more effective than the other comparators tested such as placebo, no treatment, or treatments rubbed on the skin, nor how long the possible benefits lasted. Most studies reported side-effects, but not adequately. Scarring was reported as absent, and blistering was reported in studies on intense pulsed light, infrared light and on photodynamic therapy. Three studies, with a total of 360 participants with moderate to severe acne, showed that photodynamic therapy with methyl aminolevulinate (MAL), activated by red light, had a similar effect on changes in numbers of blackheads, whiteheads and inflamed spots when compared with placebo cream with red light. The review authors judged the quality of this evidence moderate. Future well planned studies comparing the effectiveness of common acne treatments with light therapies are needed to assess the true clinical effects and side-effects of light therapies for acne.
There is a variety of light sources for photodynamic therapy of acne. Red LED arrays (∼ 635 nm) have the advantage of accuracy, intensity, robustness and it has been sufficiently the wide-area sources for facial acne photodynamic therapy 28. A study 32 previously reported that 89.61% (69/77) patients showed excellent improvement (>90% clearance of acne lesions) after three or fewer treatment sessions of ALA-photodynamic therapy conducted by red light (633 ± 6 nm). However, under the circumstance of low doses, low fluency and short exposure time, lots of cases of adverse reactions such as pain, hyperpigmentation and acute inflammatory reactions were still reported. Therefore, a method which can balance the efficacy and adverse events is urgently needed.
Intense pulsed lights (intense-pulsed light) are filtered, noncoherent, nonlaser broadband light and are reported effective and well-tolerated for photodynamic therapy of acne. Studies on ALA-intense-pulsed light-photodynamic therapy for the treatment of acne reported a reduction of lesion counts of 71.8%–87.7% after 12 weeks and side effects were mild and reversible 33.
Usefulness of intense-pulsed light in acne is controversial, especially as a single treatment 34. Intense-pulsed light has shown no superiority over benzoyl peroxide in some previous reports 35. However, intense-pulsed light could have merits over topical options in some conditions 36. Despite the single or combinational therapies with intense-pulsed light in previous studies, no study has addressed the efficacy of intense-pulsed light and benzoyl peroxide in the acne treatment. This combinational choice could reduce the treatment period and increase patient compliance. As results suggest, all severity indices, patient satisfaction, and complications patterns are clearly steeper for treatment group and the effect of combined therapy becomes much distinct by passing the time. The difference 1 month after the last therapeutic visit is remarkable and indicates more long-term benefit could be expected from intense-pulsed light.
In intense-pulsed light therapy, patients need to refer to clinic several times and this may be a disadvantage. intense-pulsed light could result in postinflammatory hyperpigmentation in dark skin patients. It also costs more than conventional treatments. Free visits in our study and lower amounts of prescribed drugs may be an explanation for patient adherence and satisfaction and this could be different in public practice.
Generally, complications following laser and light-based therapies are more frequent than topical treatments 37.
Topical treatments with benzoyl peroxide component have been shown more effective than benzoyl peroxide alone. Erythromycin 3%/benzoyl peroxide 5% combination has been shown to be effective in treating mild-to-moderate inflammatory acne by affecting the antioxidant defense enzymes 38. This combination gives more reduction in levels of superoxide dismutase, glutathione peroxidase, and catalase in leukocytes than benzoyl peroxide alone 39. It also has in vivo anti-propionibacterial activity greater than erythromycin 3% alone 38. Although benzoyl peroxide has a greater and more rapid suppressive effect on follicular population of Propionibacterium acnes than clindamycin, their combinational gel has proven clinical efficacy through both antibacterial and anti-inflammatory superior to single treatments 38. Using these combinational alternatives along with intense-pulsed light could be promising areas of the future work. Efficacy and safety of single intense-pulsed light therapy in acne treatments could be assessed in a trial framework. Increasing the number of visits and/or reducing the visit interval could give an optimal therapy policy.
Intense-pulsed light affects other normal structures of the skin and may result in local hair loss and depigmentation in treated areas. Each filter has its own features. Even though pain is common during intense-pulsed light session, patients tolerated it well because of its positive effects. One patient had postinflammatory hyperpigmentation after first intense-pulsed light session that recovered before the next intense-pulsed light session.
Intense-pulsed light could help improve results from topical agents such as benzoyl peroxide in treating mild-to-moderate acne vulgaris. Higher frequencies of complication are common in laser and light-based therapies. Future research is warranted to assess the effect of intense-pulsed light and combinational topical agents such as erythromycin/benzoyl peroxide and clindamycin/benzoyl peroxide.
Photodynamic therapy for skin cancer
Photodynamic therapy is treatment used mainly for superficial types of skin cancer. Photodynamic therapy is effective in treating actinic keratoses and superficial basal cell carcinomas.
Photodynamic therapy is currently being used or investigated as a treatment for the following skin conditions:
- Actinic keratoses on the face and scalp
- Basal cell carcinomas
- Intraepidermal squamous carcinoma (squamous cell carcinoma in situ, Bowen disease)
- Squamous cell carcinoma
- Mycosis fungoides (cutaneous T-cell lymphoma)
- Kaposi sarcoma
- Psoriasis
- Viral warts.
How does photodynamic therapy work?
Photodynamic therapy utilises photosensitizing agents, oxygen and light, to create a photochemical reaction that selectively destroys cancer cells. Photosensitising agents are drugs that are administered into the body through topical, oral or intravenous methods. In the body, they concentrate in cancer cells and only become active when light of a certain wavelength is directed onto the area where the cancer is. The photodynamic reaction between the photosensitising agent, light and oxygen kills the cancer cells.
Photosensitizing agents
Methyl aminolevulinic acid cream
- Registered for use in the treatment of actinic keratoses and superficial basal cell carcinoma
- Used with red light or daylight
- Cutaneous photosensitvity resolves within 24 hours after application
Aminolevulinic acid hydrochloride topical solution
- Registered in the treatment of actinic keratoses
- Used with blue light
BF-200 ALA gel
- Registered for the treatment of actinic keratoses
- Nanoemulsion formulation containing 10% aminolaevulinic acid hydrochloride
- Used with red light, BF-RhodoLED
Porfimer sodium
- Administered intravenously
- Causes generalised cutaneous photosenstivity that can last for months
Benzoporphyrin derivative monacid ring A
- Second-generation photosensitisers undergoing evaluation
Tin ethyl etiopurpurin and Lutetium texaphyrin
Light sources
Light sources used in photodynamic therapy include laser or nonlaser light.
Laser light has the advantages of being:
- Monochromatic (exactly one colour/wavelength that corresponds with the peak absorption of the photosensitising agent)
- Coherent (able to focus lightwaves to specific site)
- Intense (high irradiance allowing for shorter treatment times).
Laser light is suitable for small skin lesions whilst nonlaser light is better for the treatment of large skin lesions as the field of illumination is larger. Nonlaser light that emits polychromatic light is also suitable when using different photosensitisers with different absorption maxima.
Natural daylight is used successfully as a light source for the treatment of actinic keratoses.
How is photodynamic therapy given for skin cancer?
Stage 1
Photosensitizing drug is applied to the lesion. The skin may be gently scraped (curettage) or needled beforehand to increase the amount of the drug absorbed.
Waiting for a period of time (usually between 3 and 6 hours) allows the drug to concentrate in the cancer cells.
Stage 2
- Laser light or nonlaser light is shone directly on to the treated area.
- Treatment usually last between 5 and 45 minutes.
- The treated area is covered with a dressing.
- Depending on the type of lesion being treated and the photosensitizing chemical used, a 2nd cycle of treatment may be given 7–10 days later.
Stage 3
A sunburn reaction occurs, which usually heals within 4 to 8 weeks.
What are the possible side effects of photodynamic therapy for skin cancers?
Side effects from photodynamic therapy are due to the treated area being sensitive to light. The photosensitivity usually lasts about 24 hours (depending on the specific agent). Side effects may include:
- Burning/stinging sensation
- Swelling and redness
- Crusting
- Itchiness
- Peeling and blisters
- Skin infections.
The treated area should be protected from light exposure using a dressing. A local anaesthetic such as lignocaine (lidocaine) spray may be applied to the treatment area before or during Stage 2 of the procedure to help relieve pain.
The treated skin lesion may blister and ulcerate as the cancer cells die off. This may take several weeks to heal. Scarring is generally minimal (but can be moderate). Loss of pigmentation may occur sometimes and can be permanent.
Although photosensitizing drugs concentrate in cancer cells, they can also make healthy cells more sensitive to light. This is not a problem when photosensitizing creams are used as they are localised to the treatment site. It is more of a problem when photosensitizing drugs are given by mouth or injected intravenously. These patients may find all parts of their body sensitive to light and should take precautions to protect themselves from light for the necessary period of time (may be days or weeks depending on the photosensitizing drug used).
Photodynamic therapy for actinic keratosis
Photodynamic therapy is a frequently utilized treatment for actinic keratoses and, in some instances, considered the first-line treatment 40. Several studies of efficacy have been conducted for both aminolevulinic acid (ALA)/photodynamic therapy and methyl ester of ALA (MALA)/photodynamic therapy in treatment of actinic keratoses. A phase III clinical trial of ALA/photodynamic therapy for the treatment of multiple actinic keratoses of the face and scalp found 89% of patients had 75% or more of their actinic keratoses treated by week 12 41. In a phase IV clinical trial to assess longer term results, ALA/photodynamic therapy resulted in an overall lesional recurrence rate of 24% judged by clinical exam. Of the 162 lesions clinically diagnosed as recurrent actinic keratoses, 139 lesions were biopsied. The other lesions were either lost to follow-up (16) or cleared (7). 91% of biopsied lesions were confirmed histologically as actinic keratosis, 7% were found to be squamous cell carcinoma, and 0.7% basal cell carcinoma. Recurrent and non-responding lesions did not show an anatomic predilection, as they were found widely distributed on the face and scalp 42. These studies were conducted with the FDA-approved incubation regimen of illumination occurring with blue light for 14–18 hours after ALA application. Studies have suggested efficacy rates approaching those in the larger clinical trials for shortened incubation times, as short as 1 hour, which is off-label use 42. The newer gel formulation of ALA showed patient complete clearance rates of 78.2%, significantly higher than MAL cream, at the 3 month follow-up point.
MAL/photodynamic therapy has also demonstrated success in treatment of actinic keratoses. Use with red light showed an 89% complete lesion response rate compared to a 38% placebo rate at 3 months. Excellent or good cosmetic results were seen in over 90% of patients treated with MAL/photodynamic therapy 43. Tarstedt et al. 44 analyzed MAL/photodynamic therapy for treatment of thin versus thick actinic keratoses and found that a single treatment was effective for thin actinic keratoses, whereas a repeat treatment 1 week after the initial treatment was more effective for thick lesions.
Photodynamic therapy for basal cell carcinoma
A number of studies have assessed the efficacy, cosmetic results, and recurrence rates of basal cell carcinoma treated with photodynamic therapy 45. MAL/photodynamic therapy is approved in the EU for treatment of basal cell carcinoma, but remains off-label in the United States. Photodynamic therapy has shown to generally be more effective for superficial basal cell carcinoma as compared to nodular basal cell carcinoma, and also for smaller lesions <2 cm 46. However, when considering use of photodynamic therapy for treatment of larger and nodular basal cell carcinoma, MAL/photodynamic therapy specifically has shown more promise as compared to ALA/photodynamic therapy. Whereas ALA/photodynamic therapy was found to have a 30.7% recurrence rate for treatment of nodular basal cell carcinoma in one study 47, MAL/photodynamic therapy showed a 14% recurrence rate for treatment of nodular basal cell carcinoma in another study 48. Christensen et al. 49 conducted the longest follow-up of any study to date, which spanned 10 years. The overall complete response rate was 75% for all subtypes of basal cell carcinoma treated with ALA/photodynamic therapy, with a 60% complete response after one treatment and 87% response after two treatments. Further long term studies are warranted to better assess the effectiveness of photodynamic therapy on basal cell carcinoma.
Compared to surgical excision, photodynamic therapy appears to result in higher basal cell carcinoma recurrence rates [42,47,51,52,54]. Rhodes et al. 48 found the recurrence rate for primary nodular basal cell carcinoma to be 14% with photodynamic therapy and 4% with surgical excision at the 5-year follow-up point. A meta-analysis of photodynamic therapy versus surgical excision by Zou et al. 50 concluded that photodynamic therapy is comparably effective to excision for treatment of basal cell carcinoma, but with increased risk of recurrence. Multiple studies have noted that photodynamic therapy compared to excision results in better cosmetic outcomes 51.
Vinciullo et al. 52 specifically examined MAL/photodynamic therapy for “difficult-to-treat” basal cell carcinoma, defined as large lesions, lesions in the H-zone, or lesions in patients with a high risk of surgical complications. Failure rate of treatment was 18% at 12 months and 24% at 24 months, with a cosmetic outcome of excellent or good in 84% of patients at 24 months. The authors concluded that MAL/photodynamic therapy is an attractive treatment option for the subset of “difficult-to-treat” basal cell carcinomas given that surgical treatment would have been extensive and resulted in a worse cosmetic outcome.
A couple of recent small studies comparing red light LED-photodynamic therapy with Pulsed Dye Laser-photodynamic therapy for treatment of basal cell carcinoma have demonstrated slightly better clearance and recurrence rates with red light LED-photodynamic therapy. A small pilot study with 6 patients, each with 1 large superficial basal cell carcinoma (average diameter of 3.5 cm), was conducted using a split lesion design. One half of each lesion was treated with 630 nm LED-photodynamic therapy, and the other half was treated with 595 nm Pulsed Dye Laser-photodynamic therapy, both using MAL as the photosensitizer. 5 patients achieved complete response with 630 nm LED–photodynamic therapy, but an incomplete response with Pulsed Dye Laser-photodynamic therapy. 1 patient did not respond to either treatment 53. Another study with 15 patients, using an intra-individual split design, with 630 nm LED-photodynamic therapy and 585 nm Pulsed Dye Laser-photodynamic therapy on similarly sized basal cell carcinomas (nodular or superficial), showed similar clearance rates with both treatments, but higher recurrence rates with PDL-photodynamic therapy 54.
For small and superficial basal cell carcinoma, photodynamic therapy is a reasonable option for treatment, although it is not considered first line. Larger and nodular basal cell carcinoma may also be treated with MAL/photodynamic therapy, however the risk of recurrence must be weighed against the gains in cosmetic outcomes when compared to surgical excision.
Photodynamic therapy for squamous cell carcinoma of the skin
Use of MAL/photodynamic therapy for treatment of Bowen’s disease, or squamous cell carcinoma in situ, is approved in several European countries. The dosing regimen for MAL/photodynamic therapy in Europe consists of two treatments 7 days apart, repeated at 3 months, as needed 55.
Historically, there has been controversy regarding use of photodynamic therapy for Bowen’s disease, given recurrence rates and the potential for squamous cell carcinoma to metastasize. Fink-Puches et al. 56 studied ALA/photodynamic therapy for superficial squamous cell carcinoma, defined as squamous cell carcinoma confined to the papillary dermis, and projected a disease-free rate of just 8% at 36 months after treatment. These lesions were not in situ, and subsequent studies have shown better response rates. A retrospective study of 31 Bowen’s lesions (in situ squamous cell carcinoma) treated with MAL/photodynamic therapy in Brazil found 14 of 31 lesions recurrent, for a rate of 53.8%, with a mean follow-up of 43.5 months 57. Comparing MAL/photodynamic therapy to cryotherapy and 5-fluorouracil showed similar response rates with all treatments used against squamous cell carcinoma in situ at the 12 month follow-up point 58. A study comparing ALA/photodynamic therapy to MAL/photodynamic therapy with 9 and 18 Bowen’s disease lesions, respectively, showed an 89% and 78% response rate, respectively, at approximately 6 months after treatment 59.
One study using 585 nm Pulsed Dye Laser-photodynamic therapy for treatment of Bowen’s disease (in situ squamous cell carcinoma), with ALA as the photosensitizer, demonstrated a complete clinical response rate of 82% at 1-year follow-up, which is in-line with LED-photodynamic therapy response rates in other studies. Morbidity after the procedure, however, was high, as 1 patient (out of the 13 patients in the study) developed cellulitis at the site of treatment, 8 patients had prolonged crusting lasting 8 weeks, and 4 patients had prolonged discomfort lasting 6 weeks after treatment.
Photodynamic therapy shows promise for treatment of Bowen’s disease, but larger studies with longer follow-up are needed to better assess response rates. Caution should be used with this treatment, given the potential for squamous cell carcinoma to metastasize. Similar to treatment outcomes of basal cell carcinoma, cosmetic outcomes have overall been good in most patients 58.
Photodynamic therapy for Organ Transplant Recipients
Organ transplant recipients on long-term immunosuppressive therapy are at an increased risk of non-melanoma skin cancer, particularly squamous cell carcinoma. Photodynamic therapy has proven useful in reducing the incidence of actinic keratoses and squamous cell carcinomas in this special population. Willey et al. 60 carried out cyclic ALA/photodynamic therapy, defined as treatments at 4 to 8 week intervals over a 2-year period, on twelve patients who were solid organ transplant recipients. There was a 95% mean reduction in squamous cell carcinoma lesion count at 24 months post-treatment, compared to 1 month pre-treatment. Wennberg et al. 61 found that repeat MAL/photodynamic therapy treatments 1 week apart at months 0, 3, 9, and 15 reduced the occurrence of new actinic keratoses in this special population.
Photodynamic therapy for cancer
Photodynamic therapy using porfimer sodium
Porfimer sodium (Photofrin) is given through a vein (IV). It travels through the bloodstream and is absorbed by both normal and cancer cells all over the body. The normal cells get rid of most of the porfimer sodium over a couple of days. But a lot of the drug stays in the cancer cells, with less in normal cells.
Porfimer sodium alone does not destroy cancer cells. It must be activated or “turned on” with light. This is done about 2 or 3 days after the drug is given. (This gives normal cells a chance to get rid of the drug.) The doctor directs a laser light at the area of cancer cells using a very thin fiber-optic glass strand.
To treat esophageal cancer or Barrett’s esophagus, the fiber-optic strand is passed down the throat through a thin, flexible tube called an endoscope. For lung cancer treatment, the strand is passed through a bronchoscope, which is an endoscope designed to go into the lungs.
The laser used is a low-power light so it does not burn. It causes little or no pain. The light is applied for 5 to 40 minutes, depending on the size of the tumor. Any dead tissue left in the treated area is removed about 4 or 5 days later during endoscopy or bronchoscopy. The treatment can be repeated if needed.
Who should not get treated with porfimer sodium?
Porfimer sodium is NOT recommended for people with:
- A fistula (abnormal opening) between the esophagus and the windpipe (trachea) or one of the lower large breathing tubes (a bronchus)
- A tumor that’s spreading into a major blood vessel
- Enlarged veins in the stomach or esophagus, or ulcers in the esophagus
- Porphyria, or an allergy to porphyrins
Possible side effects
The major possible side effects from porfimer sodium are photosensitivity reactions (reactions triggered by light) and swelling in the treated area. Swelling may cause pain or trouble swallowing or breathing. Other minor side effects are possible, too.
Photosensitivity reactions: As soon as porfimer sodium is put into the bloodstream, it starts to collect in the cells of the body. Some of it will stay in the cells for several weeks. The skin and eyes become very sensitive to light during this time. If exposed to sunlight or other forms of bright light, the skin can quickly become swollen, sunburned, and blistered. It takes only a few minutes for this to happen, so it’s very important to protect the eyes and skin during this time.
After you get porfimer sodium, you should take precautions (see below) for at least 30 days to prevent reactions. Sensitivity to light can last as long as 3 months, but the length of time is different with each person. If you have a reaction, call your doctor right away.
You should try to avoid bright lights and direct sunlight, but you don’t have stay in dark rooms. Some indoor light is important because it will help to slowly break down the drug in your skin. As this happens, your skin becomes less sensitive to light over time. Ask your doctor when and how you should test your skin for photosensitivity. This is usually done no sooner than 30 days after you get the drug.
You can help prevent a photosensitivity reaction if you prepare before treatment and use precautions after it. Here are some ways to do this:
- Before going to your doctor’s office or hospital for treatment, close the shades and curtains on the windows in your home. Be sure windows and skylights are fully covered.
- Bring dark sunglasses, gloves, a wide brimmed hat, long pants, socks, shoes, and a long-sleeved shirt to wear after your appointment. Clothing should be light in color and the fabric should be tightly woven.
- Do not count on sunscreen to protect you. Most sunscreens only protect against ultraviolet (UV) light, and they will not prevent a photosensitivity reaction.
- For at least 30 days after you get the drug, limit your time outdoors, especially when the sun’s rays are strongest (between about 10 am and 4 pm). Cover your skin when you do go outside, even on cloudy days and when you are in the car.
- Try to do your daily errands after sundown.
- Do not expose your skin to reading lamps or exam lamps (like those used in a dentist’s office).
- Don’t use helmet-type hair dryers (such as those found in beauty salons). High heat can activate any drug left in your scalp and cause redness or burning. If you use a hand-held hair dryer, use a low heat setting.
Swelling: Swelling in the treated area can lead to pain in the chest or back. If the esophagus is treated, it may lead to narrowing (stricture) of the esophagus, which could cause problems swallowing. Treatment of the breathing tubes or lungs could lead to trouble breathing. If you notice any of these problems, let your doctor know right away.
Other possible side effects: Side effects depend on the part of the body being treated. If the esophagus is treated, possible side effects include nausea, vomiting, fever, dehydration, headache, scarring and narrowing of the esophagus, hiccups, trouble swallowing, and fluid collecting around the lungs. In people treated for lung cancer, possible side effects include shortness of breath, coughing up blood, fever, pneumonia, and bronchitis.
If you are treated with porfimer sodium, ask your doctor which side effects you might expect and which you need to report right away. Get the phone number to call if you have problems after regular office hours.
Photodynamic therapy using aminolevulinic acid (ALA)
Aminolevulinic acid (Levulan Kerastick) is a solution that’s put right on the spots (called lesions) of actinic keratosis. Unlike porfimer sodium, it does not reach other parts of the body. This means the lesions are sensitive to the light but the rest of the body is not.
The drug is left on the affected skin for about 14 to 18 hours, usually until the next day. At that time your doctor will expose the area being treated to a blue light for about 15 minutes. During the light therapy you and the doctor will wear protective eyewear. You may feel stinging or burning once the area is exposed to the blue light, but it should go away within a day or so. The treated area may get red and scale and crust for up to 4 weeks before healing. If a lesion does not completely go away after treatment, it can be treated again 8 weeks later.
Who should NOT get treated with aminolevulinic acid?
Aminolevulinic acid is NOT recommended for people with skin sensitivity to blue light, people with porphyria, or anyone with an allergy to porphyrins.
Possible side effects
Photosensitivity reactions: Reactions caused by light can show up on the skin where the drug is applied. They usually involve redness and a tingling or burning sensation. For about 2 days after the drug is used, you should take care to not expose treated areas of your face and scalp to light.
- Stay out of strong, direct light.
- Stay indoors as much as possible.
- Wear protective clothing and wide-brimmed hats to avoid sunlight when outdoors.
- Avoid beaches, snow, light colored concrete, or other surfaces where strong light may be reflected.
Sunscreens will not protect the skin from photosensitivity reactions.
Skin changes: The treated skin will likely turn red and may swell after treatment. This usually peaks about a day after treatment and gets better within a week. It should be gone about 4 weeks after treatment. The skin may also be itchy or change color after treatment.
Talk to your doctor about what you should expect your treated skin to look and feel like. Also ask about which side effects you should report right away and what phone number to call if you have problems after regular office hours.
Photodynamic therapy using methyl ester of ALA (MAL)
Methyl ester of ALA (Metvixia cream) is used very much like aminolevulinic acid. It’s a cream that’s put on the skin of the face or scalp to treat actinic keratosis lesions. The doctor will likely first scrape the area with a small, sharp blade. The lesions where the cream is applied will become sensitive to light, but the rest of the body will not. (This drug does not reach other parts of the body.) The cream should not be left on the skin for more than 4 hours.
The cream is applied and covered with a bandage. About 3 hours later the doctor will take off the bandage, wash off the cream, and expose the area to a red light source for 5 to 20 minutes. During the light therapy you and the doctor will wear protective goggles. You may feel stinging or burning when light reaches the area. Two treatment sessions are usually done 7 days apart. The treated area may turn red, blister, scale, and crust for up to 10 days before healing. The doctor will look at the lesion about 3 months after the last treatment to see whether it worked.
Who should NOT get treated with methyl ester of ALA?
Methyl ester of ALA is NOT recommended for those with:
- Skin sensitivity to light
- Allergies to peanuts or almonds (these oils are used to make the cream)
- Immunosuppression (a weakened immune system)
- Porphyria, or an allergy to porphyrins
Methyl ester of ALA cream has not been studied for more than 2 treatment sessions. Information regarding more treatments done after 3 months for remaining or new actinic keratosis lesions is not available.
Possible side effects
Photosensitivity reactions: These are reactions triggered by light. They can happen at the area where the drug was applied, and usually involve redness and stinging or burning. You should stay out of the sun, away from bright indoor lights, and avoid extreme cold after the cream is applied and before the light treatment is done. For about 2 days after the light treatment, you should take care to keep the treated area away from any light.
- Keep the treated area covered.
- Stay out of strong, direct, bright indoor light.
- Stay indoors as much as possible.
- When outdoors, wearing protective clothing and wide-brimmed hats to avoid sunlight.
- Avoid beaches, snow, light-colored concrete, or other surfaces where strong light may be reflected.
Sunscreens will not protect the skin from photosensitivity.
Skin changes: The skin being treated will likely turn red and may blister and swell after treatment. Burning and stinging are common. The skin may also be itchy, scaly, or change color after treatment. These side effects should get better with time and should be gone by 3 weeks after treatment. If they get worse or are not gone in 3 weeks, call your doctor. Ask what other side effects should be reported to the doctor and what phone number you should use if you have problems after regular office hours.
Allergic reactions: Repeated exposure to methyl ester of ALA cream can cause sensitization, or development of allergy to the cream. Rashes such as eczema and hives (raised itchy bumps) can appear at the area of contact within a few hours after exposure to the cream. Very rarely, more serious allergic reactions can happen.
Photodynamic therapy side effects
Early onset side effects
Pain and local skin reactions, including erythema, edema, desquamation, or pustulae, often in association with each other, are commonly observed in course of exposure to the light source and in the hours/days immediately after photodynamic therapy 62. More rarely, urticaria, contact dermatitis, or erosive pustular dermatosis of the scalp occur. Photodynamic therapy has also a significant effect on the immune system, with acute onset, but with a potential long-term effect on treatment-related carcinogenesis.
Pain
Pain is an issue of general concern, as it represents the most frequent and limiting side effect of conventional photodynamic therapy, with up to 58% of patients reporting severe pain 63. Painful burning sensation usually starts immediately or very early during light exposure, becoming rapidly very intense, with a peak in the first minutes of treatment. Thereafter, pain usually tends to decrease or even subside towards the end of the treatment 64. In some cases, pain can be so severe to induce the premature stop of light exposure, which results in insufficient protoporphyrin IX (PpIX) formation and inadequate therapeutic result. Pain can also induce systemic symptoms. Borroni et al. 65 reported the occurrence of post-methylated ester-photodynamic therapy acute postoperative hypertension in 8 out of 36 patients (22%); 11% of patients developed hypertensive crisis, requiring immediate treatment. Interestingly, the majority of these patients had a positive history for hypertension, which may represent an important risk factor and identify high-risk subjects 65. Photodynamic therapy has a significant temporary impact on patients’ quality of life, with a marked increase of the dermatology life quality index scores from 1.6 ± 1.7 prior to photodynamic therapy to 7.3 ± 4.9 immediately post photodynamic therapy 66. Moreover, most patients experiencing severe pain are dissatisfied about effectiveness, convenience and overall experience. Pain can negatively influence patients’ adherence, leading to refusal of further treatment 67.
The exact mechanism of photodynamic therapy-related pain is yet unknown. Reactive oxygen species (ROS) are the main mediators of pain experience during photodynamic therapy, and contribute to stimulation of sensory neurons that conduct pain to sensory cortex of the brain. Intensity of pain can be determined by the depth of singlet oxygen production in the skin, which in turn depends on the nature of the photosensitizer and on the wavelength of the stimulating light. Local hypoxia secondary to oxygen-consuming reactions, like PpIX photobleaching or tumour destruction, can cause a decrease of the pH in the tissue, and trigger pain signals due to the low oxygen level around the mitochondria-rich nerve endings 68. Pain is the result of the interplay between many intrinsic and extrinsic factors. No correlation was found with age or sex, and no studies investigated racial influence 69. Skin phototype seems to not influence pain experience, although some studies reported higher intensity of pain in fair-skinned patients. However, these patients are constitutionally more prone to develop sun-induced tumors in larger areas than dark phototypes 70.
About photosensitizer, many studies compared the pain intensity experienced using 5-aminolaevulinic acid (ALA) or methylated ester (MAL). Unfortunately, these comparisons are difficult to interpret, as clinicians use the drugs differently in clinical practice; moreover, some authors compared branded versus compounded drugs. Kasche et al. 71 evaluated 69 patients affected by multiple actinic keratoses on the scalp, and reported that ALA-photodynamic therapy caused a higher level of pain than MAL-photodynamic therapy. Similar results were obtained some years later by Steinbauer et al. 72. Gaal et al. 73 compared the pain caused by ALA-photodynamic therapy and MAL-photodynamic therapy in different body areas (head, trunk, extremities), and found that ALA-photodynamic therapy was more painful than MAL-photodynamic therapy in all cases, but the difference was statistically significant only for head lesions.
On the other hand, Ibbotson et al., in a cohort of patients affected by Bowen’s disease and basal cell carcinoma, found no significant differences in visual analogue scale (VAS) scores between ALA-photodynamic therapy and MAL-photodynamic therapy 74. Such results were confirmed by Yazdanyar et al. 75, who reported no significant difference in an intra-individual split-forehead and scalp study, where MAL-photodynamic therapy and ALA-photodynamic therapy were given to each patient in two similar areas. Some studies used measurements of fluorescence intensity to evaluate PpIX generation with both photosensitizers. Pretreatment fluorescence directly correlates with pain intensity and is a good predictor of erythema and lesion clearance 76. The redness of the actinic lesions was found to be related to photodynamic therapy-induced pain, the reduction of actinic area, and the cure rate. The redder the actinic area, the better the treatment outcome and the more pain experienced 77. It is not clear, however, whether different incubation times may influence PpIX concentration and clinical outcome.
A few studies investigated the correlation between clearance rate and different incubation times with both ALA and MAL, showing no significant differences between 1 hour vs. 3 hours regimens 78. Lerche et al. 79 recently introduced the concept of pulse–photodynamic therapy, in which MAL is applied for 30 min under occlusion before it is removed. After removal, the skin is covered with a light-impermeable dressing for 2.5 hours, followed by red light illumination. The short-time incubation should promote selective PpIX accumulation in the mitochondria and the endoplasmic reticulum (which are considered the main targets for achieving apoptosis), preventing excessive PpIX production in the surrounding tissue. This would limit death to diseased cells and decrease the severity of adverse events such as pain and erythema, with no influence on treatment efficacy 79. Fluence shows a strong positive correlation with pain, lower fluences being less painful 80. Light dose also plays an important role in modulating pain sensation. Radakovic-Fijan et al. 81 found no significant correlation between high light dose and pain intensity when total light dosage was higher than 70 J/cm². Consistent with these observations, Wang et al. 82 proposed a threshold theory for photodynamic therapy-induced pain, postulating a positive correlation with both fluence rate and dose below a certain threshold (rate of 60 mW/cm², dose of 50 J/cm²). Exceeding this threshold, no significant increase in pain is experienced 82. The link may be ROS generation. Increasing light dose and fluence rate causes a progressive increase in ROS production; when the threshold is reached, desensitization of nociceptors and/or saturation of cell capacity to produce ROS may determine a plateau of pain perception. The constant and slow dynamics of ROS production is probably the mechanism through which Daylight photodynamic therapy (DL-photodynamic therapy) is quite less painful respect to conventional photodynamic therapy, with increased patient tolerance and satisfaction. Compared to conventional photodynamic therapy, pain intensity during Daylight photodynamic therapy is significantly lower, probably due to continuous production and photoactivation of small amounts of PpIX, with decreased local concentration of ROS and, consequently, reduced stimulation of nerve endings 83. Other important factors influencing pain are lesion type, location and treatment area size. Many studies identified actinic keratosis as the most painful lesion to treat, with head and neck location having the greatest impact on pain perception, because of the high nerve density; lesions located on the limbs cause a greater degree of pain than those on the trunk 84. Nevertheless, other researchers found nodular basal cell carcinoma and squamous cell carcinoma to be the most painful lesions to treat, suggesting a role for lesion thickness 85. The treatment area size positively correlates with severe pain, with larger areas being more painful 86. The first treatment is frequently less painful than the second, as demonstrated by Lindeburg et al. 87, a patient with low pain experience during the first photodynamic therapy has a greater risk of more pain during the second photodynamic therapy, while a patient with high pain experience during the first photodynamic therapy is more likely to feel a reduction of pain during the following light exposure 87.
Pain management is a major challenge. Different strategies, including cold air analgesia, topical anesthesia, infiltration anesthesia, nerve block, hypnosis, have been studied, none of them being completely effective 88. When indicated, Daylight photodynamic therapy is the real painless alternative to conventional photodynamic therapy.
Local Skin Reactions
Erythema and edema are the main phototoxic effects of photodynamic therapy and develop in the treated area during and after light exposure 89. The often severe erythema can be followed by crusting and generally resolves in 1–2 weeks. In one large study of patients (n = 2031) receiving topical photodynamic therapy over a 5-year period, erythema and oedema occurred in 89% of subjects and 80% reported scaling and itch. Crusting (9%), pustules (6%), erosions (1.2%) and infections (0.4%) were other reported adverse effects 90. Especially during photodynamic therapy treatment of large areas on the face and scalp, patients are discomforted by the inflamed appearance that may prevent them from going to work for days 91.
Brooke and colleagues 92 studied the effects of ALA-photodynamic therapy on human skin, demonstrating that the acute inflammatory response comprises immediate stinging, followed by a more prolonged erythema, and that histamine, at least in part, mediates the acute reaction to photodynamic therapy. Post-treatment dermal histamine levels peak at 30 min after light exposure, remain stably elevated for 4 hours, and gradually return to baseline by 24 hours posttreatment. However, a recent clinical trial which evaluated the impact of oral H1 antihistamine therapy in the reduction of Local Skin Reaction showed no effects both on inflammatory response and ALA-photodynamic therapy efficacy 93. If histamine is a key mediator of the immediate urticarial response, the delayed erythema is more closely attributable to other proinflammatory mediators such as prostaglandin E2 and nitric oxide, owing to their vasodilatory properties and their involvement in apoptosis and tumorigenesis in experimental models 94. However, these data refer to human healthy skin, and may not reflect the changes induced by photodynamic therapy in damaged skin.
Urticaria
Urticarial reactions to photodynamic therapy with ALA and MAL were described in the literature 95. A 2008 study reported a 0.9% prevalence (12/1353 patients) for severe itching and wheals within the first minute of illumination 96. The patients most predisposed to reaction were those who had received more than 7 courses of treatment (3.8% prevalence). The proposed mechanism was histamine release from mast cells in the dermis. This pathogenesis is consistent with the recurrent nature of the reactions in subsequent treatments, the satisfactory control of these reactions through administration of an antihistamine, such as cetirizine, before treatment, and the immediate appearance of urticaria in areas not previously treated with photodynamic therapy. Only two pediatric cases of urticaria during photodynamic therapy were reported until now 97.
Contact Dermatitis
Allergic contact dermatitis was reported with MAL and, more rarely, with ALA 98. Despite their structural similarity, no evidence of cross-reactivity between the two agents was highlighted until now. In the twenty cases reviewed by Pastor-Nieto et al. 99, patch tests with the licensed 16% MAL preparation were positive in all patients while patch tests with the vehicle were negative, confirming the causative role of the active ingredient. A single case of systemic allergic contact dermatitis caused by MAL was recently described in a patient with keratosis–ichthyosis–deafness syndrome 100. It is likely that the incidence of sensitization to MAL is underestimated, as a number of intense inflammatory post-photodynamic therapy reactions probably reflects genuine contact dermatitis. Conversely, the use of many different ALA compounded drugs could explain the lower reported occurrence of contact dermatitis caused by this molecule.
Immunosuppression
photodynamic therapy has a significant effect on the immune system, by either stimulating or, in some circumstances, repressing innate and adaptive immune response 101. photodynamic therapy causes release or expression of various pro-inflammatory and acute phase response mediators from the treated site, with local recruitment of neutrophils and other inflammatory cells in large numbers and activation of the complement system, targeting the tumor microenvironment 102. In addition to stimulating local inflammation, photodynamic therapy can induce potent, systemic, antigen specific anti-tumor immunity 103. The other side of the coin is the ability of photodynamic therapy to cause local and systemic immunosuppression, with reduction of delayed-type hypersensitivity responses to recall antigens. By measuring Mantoux erythema and diameter, Matthews and Damian found that, at the light doses and irradiance rates in current clinical use, both ALA-photodynamic therapy and MAL-photodynamic therapy were locally immune suppressive even after one treatment session 104. Moreover, it was shown that photodynamic therapy reduces the number of Langerhans cells (epidermis-resident antigen-presenting cells) both in healthy skin and in biopsy samples from basal cell carcinoma. Such reduction can induce antigenic tolerance and can be responsible for suppression of contact hypersensitivity both at the site of irradiation (local immunosuppression) as well as at distant, non-irradiated sites (systemic immunosuppression), with potential negative impact on antitumor response 105. In this respect, Thanos et al. showed that both oral and topical nicotinamide (vitamin B3) reduce the immune suppressive effects of photodynamic therapy on delayed-type hypersensitivity responses in humans, and proposed administration of nicotinamide as a simple method to increase the effectiveness of photodynamic therapy 106. Moreover, the same authors demonstrated a synergic effect of administration of nicotinamide and low irradiance rate photodynamic therapy, with no negative impact on tumour clearance rate 107. On the basis of these considerations, we could consider the association of low light intensity daylight-photodynamic therapy and oral nicotinamide as the best strategy to achieve good therapeutic efficacy with high safety profile. The exact mechanism by which nicotinamide exerts this effect is still not fully understood. Probably is involved its ability, as an NAD precursor, to replenish cellular ATP levels decreased by photodynamic therapy, thus favoring the highly energy-dependent processes of DNA repair. Furthermore, nicotinamide does not exert antioxidant effects in vitro in human keratinocytes, and, consequently, does not decrease ROS generation, which is required for the antitumoral action of photodynamic therapy 106.
Miscellaneous
It is known that photodynamic therapy exerts a wide spectrum of antimicrobial effects, so it is not unexpected that occurrence of infections at the site of treatment is a rare complication, with only four cases of bacterial cellulitis reported over 700 treatments 108. To date, only one case of erosive pustular dermatosis of the scalp was reported, with extensive sterile pustular lesions, non-healing erosions, and crusting of the scalp 109. Interestingly, three cases of erosive pustular dermatosis of the scalp were recently reported after ingenol mebutate application, suggesting that post-treatment inflammation could act as trigger factor in highly photodamaged areas 110. The good response to both topical and systemic steroids could lead us to hypothesize a common pathogenic mechanism linked to neutrophilic infiltration, which is a key component of the inflammatory response in both treatments 111. Gemigniani et al. reported a case of complete left peripheral facial palsy occurred 1 week after topical photodynamic therapy for left hemifacial actinic keratosis 112. The authors considered it as a possible, although uncommon, complication of photodynamic therapy, on the basis of the close relation among the treated zone, the superficial localization of facial nerve branches, and the short elapsed time.
Late onset side effects
Pigmentary changes and scarring
photodynamic therapy can rarely induce hyperpigmentation and scarring. In the large experience of the Scottish photodynamic therapy Centre, pigmentary change and mild/moderate scarring accounted only for 1% and 0.8% of lesions treated, respectively, on a patient population predominantly of skin phototypes I–III [86]. Hyperpigmentation is generally transient, with slow resolution within the months following photodynamic therapy. Hypopigmentation, presumably due to phototoxic damage to melanocytes, can also occur, although this is not well documented in the literature [47].
Bullous Pemphigoid
Two cases of post-photodynamic therapy bullous pemphigoid (BP) were described, one strictly confined to the areas treated with photodynamic therapy for Bowen’s disease, the other involving other sites too [87,88]. In both cases, BP lesions were detected after 3–4 months, at follow-up visit. The pathogenetic mechanism remains unknown; Wolf’s isotopic response was suggested as possible explanation.
Carcinogenicity
In the spectrum of the possible side effects caused by photodynamic therapy, the most worrisome is certainly its potential to induce or stimulate skin carcinogenesis. Several reports showed onset of basal cell carcinoma, keratoacanthoma and invasive squamous cell carcinoma after treatment with photodynamic therapy 113. In 1997, a case of melanoma of the scalp, at a site repeatedly exposed to topical ALA-photodynamic therapy for solar keratoses and superficial squamous cell carcinomas, was reported by Wolf et al. 114. In 2009, Schreml and colleagues described another case of melanoma developed after photodynamic therapy treatment of Bowen’s disease on the right cheek 115. These reports highlight the dilemma of whether photodynamic therapy may promote tumor development and growth, and should be considered with caution. Indeed, these patients often have a great predisposition to skin cancer (immunosuppression, prior history of Non Melanoma Skin Cancer, heavily photodamaged skin, multiple treatment fields) and photodynamic therapy could have a coincidental, rather than causal, role in promoting carcinogenesis. The carcinogenic risk may be the consequence of different pathogenic mechanisms, including the previously discussed immunosuppression, mutagenesis and isotopic response. The mutagenic effect of photodynamic therapy is controversial. Some authors affirm that photodynamic therapy is not directly mutagenic on DNA, others demonstrated that ROS generated after photodynamic therapy photosensitization can cause DNA damage and oncogene activation 116. Kick et al. 117 described the photodynamic therapy-related induction of some proto-oncogenes (c-jun and c-fos) involved in the carcinogenesis of human epithelial cells. Giri et al. 118 reported a particular effect of the photosensitizer protoporphyrin in mouse skin (double dose-dependent effect), resulting in the in situ generation of ROS, and able to induce DNA damage in normal epithelial cells. They demonstrated that mice treated by photodynamic therapy face an anti-tumoral effect (destruction of tumor cells) with a high dose of haematoporphyrin (5 mg/kg) and a pro-tumoral result (DNA damage) with a lower dose (2.5 mg/kg) 118. Miyazu and colleagues evaluated telomerase protein expression in noncancerous bronchial epithelium of patients with lung cancer, and concluded that photodynamic therapy is useful to treat lung cancer, but does not destroy normal cells that express telomerase and are, for this reason, predisposed to squamous cell carcinoma development 119. This aspect turns out to be relevant when the important role of telomerase is considered in skin carcinogenesis [104]. photodynamic therapy could also modify the course of tumor. Gilaberte and colleagues 120 studied recurrences and aggressiveness of skin tumors non respondent to photodynamic therapy, reporting an increased Epidermal Growth Factor Receptor (EGFR) expression after MAL-photodynamic therapy. Some authors found high expression of Epidermal Growth Factor Receptor in tumors characterized by aggressiveness, poor prognosis, short survival of patients and development of resistence to cytotoxic agents 121. This correlation was demonstrated also in squamous cell carcinoma 122. Gilaberte and colleagues also focused on the role of mitogen-activated protein kinase (MAPK), mediated in most human cancer by fosforilation of ERK1/2. They hypothesized that photodynamic therapy may promote the selection of more aggressive tumor cells, and the MAPK/ERK signal pathway may be involved in the resistance to photodynamic therapy 120. Moreover, the activation of Epidermal Growth Factor Receptor induces stimulation of ERK, with consequent overexpression of cyclin D1, which is frequently involved in keratinocyte carcinogenesis 123. In this regard, Moreno Romero et al. reported two cases of rapidly growing squamous cell carcinoma after treatment of ingenol mebutate for actinic keratoses on the forehead (time to onset: 4 weeks) and the neck (time to onset: 5 weeks), and proposed that, in some cases, the inflammatory process induced by ingenol mebutate could accelerate the transformation of actinic keratoses into squamous cell carcinomas 124. It is interesting to highlight that the MAPK/ERK signal pathway is involved also in the mechanism of action of ingenol mebutate and could explain, at least in part, this paradoxical response, which consists of reduction of cell viability and proliferation, and, on the other hand, promotion of tumor cell growth 125.
Lastly, the role of photodynamic therapy as promoter of skin malignancies remains not completely understood and its influence on tumor development in humans requires further study. However, taking into account the cases of skin cancers after photodynamic therapy that were reported in literature, it appears crucial to perform continued and careful follow-up after this useful treatment, especially in patients with multiple risk factors for skin cancers, and to make biopsies when, in a treated area, a new suspicious lesion appears or invasion is likely.
- Borgia F, Giuffrida R, Caradonna E, Vaccaro M, Guarneri F, Cannavò SP. Early and Late Onset Side Effects of Photodynamic Therapy. Biomedicines. 2018;6(1):12. doi:10.3390/biomedicines6010012. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5874669/[↩]
- Morton C., Szeimies R.M., Sidoroff A., Wennberg A.M., Basset-Seguin N., Calzavara-Pinton P., Gilaberte Y., Hofbauer G., Hunger R., Karrer S., et al. European Dermatology Forum. European Dermatology Forum Guidelines on topical photodynamic therapy. Eur. J. Dermatol. 2015;25:296–311. doi: 10.1684/ejd.2015.2570[↩]
- Borgia F., Saitta C., Vaccaro M., Franzè M.S., Lentini M., Cannavò S.P. Nodular-cystic eruption in course of sorafenib administration for hepatocarcinoma: An unconventional skin reaction requiring unconventional treatment. Int. J. Immunopathol. Pharmacol. 2017;30:327–331. doi: 10.1177/0394632017727618 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5815258/[↩]
- Tierney E.P., Eide M.J., Jacobsen G., Ozog D. Photodynamic therapy for actinic keratoses: Survey of patient perceptions of treatment satisfaction and outcomes. J. Cosmet. Laser Ther. 2008;10:81–86. doi: 10.1080/14764170802056117 https://www.ncbi.nlm.nih.gov/pubmed/18569260[↩]
- Greb JE, Goldminz AM, Elder JT, Lebwohl MG, Gladman DD, JJ W, Mehta NN, Finlay AY, Gottlieb AB. Psoriasis. Nat Rev Dis Primers. 2016;2:16082. doi: 10.1038/nrdp.2016.82[↩]
- Goldenberg G, Lanoue J, Dong J. New oral therapies for psoriasis: a comprehensive review. J Clin Aesthet Dermatol. 2016;9(8):25–28 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5022993/[↩]
- Menter A, Korman NJ, Elmets CA, Feldman SR, Gelfand JM, Gordon KB, Gottlieb AB, Koo JY, Lebwohl M, Lim HW, Van Voorhees AS, Beutner KR, Bhushan R. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am AcadDermatol. 2009;61(3):451–485. doi: 10.1016/j.jaad.2009.03.027[↩]
- Laws PM, Warren RB. Ustekinumab for the treatment of psoriasis. Expert Rev Clin Immunol. 2011;7(2):155–164. doi: 10.1586/eci.11.4[↩]
- Calzavara-Pinton PG, Sala R, Arisi M, Rossi MT, Venturini M, Ortel B. Synergism between narrowband ultraviolet B phototherapy and etanercept for the treatment of plaque-type psoriasis. Br J Dermatol. 2013;169(1):130–136. doi: 10.1111/bjd.12277[↩]
- Avci P, Gupta A, Sadasivam M, Vecchio D, Pam Z, Pam N, Hamblin MR. Low-level laser (light) therapy (LLLT)in skin: stimulating, healing, restoring. SeminCutan Med Surg. 2013;32(1):41–52.[↩]
- Pfaff S, Liebmann J, Born M, Merk HF, von Felbert V. Prospective randomized long-term study on the efficacy and safety of UV-free blue light for treating mild psoriasis vulgaris. Dermatology. 2015;231(1):24–34. doi: 10.1159/000430495[↩]
- Weinstabl A, Hoff-Lesch S, Merk HF, von Felbert V. Prospective randomized study on the efficacy of blue light in the treatment of psoriasis vulgaris. Dermatol. 2011;223:251–259. doi: 10.1159/000333364[↩]
- Niu T, Tian Y, Ren Q, Wei L, Li X, Cai Q. Red light interferes in UVA-induced photoaging of human skin fibroblast cells. Photochem Photobiol. 2014;90(6):1349–1358. doi: 10.1111/php.12316[↩]
- Kwon HH, Lee JB, Yoon JY, Park SY, Ryu HH, Park BM, Kim YJ, Suh DH. The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: a double-blind, randomized controlled trial. Br J Dermatol. 2013;168:1088–1094. doi: 10.1111/bjd.12186[↩]
- Ablon G. Combination 830-nm and 633-nm light-emitting diode phototherapy shows promise in the treatment of recalcitrant psoriasis: preliminary findings. Photomed Laser Surg. 2010;28(1):141–146. doi: 10.1089/pho.2009.2484[↩]
- Chen AC, Arany PR, Huang YY, Tomkinson EM, Sharma SK, Kharkwal GB, Saleem T, Mooney D, Yull FE, Blackwell TS, Hamblin MR. Low level laser therapy activates NF-jB via generation of reactive oxygen species in mouse embryonic fibroblasts. PLoS One. 2011;6(7):e22453. doi: 10.1371/journal.pone.0022453[↩]
- Niu T, Tian Y, Cai Q, Ren Q, Wei L. Red light combined with blue light irradiation regulates proliferation and apoptosis in skin keratinocytes in combination with low concentrations of curcumin. PLoS One. 2015;10(9):e0138754. doi: 10.1371/journal.pone.0138754[↩]
- Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin MR. The nuts and bolts of low-level laser (light) therapy. Ann Biomed Eng. 2012;40(2):516–533. doi: 10.1007/s10439-011-0454-7[↩]
- Wong-Riley MT, Liang HL, Eells JT, Chance B, Henry MM, Buchmann E, Kane M, Whelan HT. Photobiomodulation directly benefits primary neurons functionally inactivated by toxins: role of cytochrome c oxidase. J Biol Chem. 2005;280(6):4761–4771. doi: 10.1074/jbc.M409650200[↩]
- Zhang Q, Dong T, Li P, Wu MX. Noninvasive low-level laser therapy for thrombocytopenia. Sci Transl Med. 2016;8(349):349 ra101. doi: 10.1126/scitranslmed.aaf4964[↩]
- Peplow PV, Chung TY, Ryan B, Baxter GD. Laser photobiomodulation of gene expression and release of growth factors and cytokines from cells in culture: a review of human and animal studies. Photomed Laser Surg. 2011;29(5):285–304. doi: 10.1089/pho.2010.2846[↩]
- Dong T, Zhang Q, Hamblin MR, MX W. Low-level light in combination with metabolic modulators for effective therapy of injured brain. J Cereb Blood Flow Metab. 2015;35(9):1435–1444. doi: 10.1038/jcbfm.2015.87[↩]
- Zhang P, Wu MX. A clinical review of phototherapy for psoriasis. Lasers in Medical Science. 2018;33(1):173-180. doi:10.1007/s10103-017-2360-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5756569/[↩]
- Le Pillouer-Prost A, Cartier H. Photodynamic photorejuvenation: a review. Dermatol Surg. 2016;42(1):21–30. doi: 10.1097/DSS.0000000000000528[↩]
- Tawfik AA. Novel treatment of nail psoriasis using the intense pulsed light: a one-year follow-up study. Dermatol Surg. 2014;40(7):763–768[↩]
- Williams HC, Dellavalle RP, Garner S. Acne vulgaris. The Lancet. 2012;379(9813):361–72. doi: 10.1016/S0140-6736(11)60321-8[↩][↩]
- Zhang HY, Ji J, Tan YM, Zhang LL, Wang XJ, Wang PR, Yang DG, Shi L, Huang Z, Chen SY, Wang XL. Evaluation of 5-aminolevulinic acid-mediated photorejuvenation of neck skin. Photodiagnosis Photodyn Ther. 2014;11(4):498–509. doi: 10.1016/j.pdpdt.2014.10.003. doi:10.1016/j.pdpdt.2014.10.003[↩]
- Sakamoto FH, Torezan L, Anderson RR. Photodynamic therapy for acne vulgaris: a critical review from basics to clinical practice: part II. Understanding parameters for acne treatment with photodynamic therapy. J Am Acad Dermatol. 2010;63(2):195–211; quiz -2. doi:10.1016/j.jaad.2009.09.057 10.1016/j.jaad.2009.09.056[↩][↩]
- Zaenglein AL, Pathy AL, Schlosser BJ, Alikhan A, Baldwin HE, Berson DS, Bowe WP, Graber EM, Harper JC, Kang S, et al. Guidelines of care for the management of acne vulgaris.J Am Acad Dermatol. 2016;74(5):945–73.e33. doi: 10.1016/j.jaad.2015.12.037 https://www.ncbi.nlm.nih.gov/pubmed/26897386[↩]
- Ruiz-Rodriguez R, Sanz-Sanchez T, Cordoba S. Photodynamic photorejuvenation. Dermatol Surg. 2002;28(8):742–4; discussion 744. doi:10.1097/00042728-200208000-00019 10.1046/j.1524-4725.2002.02018.x[↩]
- Barbaric J, Abbott R, Posadzki P, Car M, Gunn LH, Layton AM, Majeed A, Car J. Light therapies for acne. Cochrane Database of Systematic Reviews 2016, Issue 9. Art. No.: CD007917. DOI: 10.1002/14651858.CD007917.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD007917.pub2/full[↩][↩]
- Wang XL, Wang HW, Zhang LL, Guo MX, Huang Z. Topical ALA PDT for the treatment of severe acne vulgaris. Photodiagnosis Photodyn Ther. 2010;7(1):33–8. doi:10.1016/j.pdpdt.2010.01.003[↩]
- Mei X, Shi W, Piao Y. Effectiveness of photodynamic therapy with topical 5-aminolevulinic acid and intense pulsed light in Chinese acne vulgaris patients. Photodermatol Photoimmunol Photomed. 2013;29(2):90–6. doi:10.1111/phpp.12031[↩]
- Mokhtari F, Gholami M, Siadat AH, et al. Efficacy of Intense-pulsed Light Therapy with Topical Benzoyl Peroxide 5% versus Benzoyl Peroxide 5% Alone in Mild-to-moderate Acne Vulgaris: A Randomized Controlled Trial. Journal of Research in Pharmacy Practice. 2017;6(4):199-205. doi:10.4103/jrpp.JRPP_17_29. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5787904/[↩]
- El-Latif AA, Hassan FA, Elshahed AR, Mohamed AG, Elsaie ML. Intense pulsed light versus benzoyl peroxide 5% gel in treatment of acne vulgaris. Lasers Med Sci. 2014;29:1009–15 https://www.ncbi.nlm.nih.gov/pubmed/24114421[↩]
- Faghihi G, Isfahani AK, Hosseini SM, Radan MR. Efficacy of intense pulsed light combined with topical erythromycin solution 2% versus topical erythromycin solution 2% alone in the treatment of persistent facial erythematous acne macules. Adv Biomed Res. 2012;1:70[↩]
- Mariwalla K, Rohrer TE. Use of lasers and light-based therapies for treatment of acne vulgaris. Lasers Surg Med. 2005;37:333–42[↩]
- Tan HH. Topical antibacterial treatments for acne vulgaris: Comparative review and guide to selection. Am J Clin Dermatol. 2004;5:79–84 https://www.ncbi.nlm.nih.gov/pubmed/15109272[↩][↩][↩]
- Basak PY, Gultekin F, Kilinc I, Delibas N. The effect of benzoyl peroxide and benzoyl peroxide/erythromycin combination on the antioxidative defence system in papulopustular acne. Eur J Dermatol. 2002;12:53–7[↩]
- Cohen DK, Lee PK. Photodynamic Therapy for Non-Melanoma Skin Cancers. Hamblin MR, ed. Cancers. 2016;8(10):90. doi:10.3390/cancers8100090. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5082380/[↩]
- Piacquadio D.J., Chen D.M., Farber H.F., Fowler J.F., Glazer S.D., Goodman J.J., Hruza L.L., Jeffes E.W.B., Ling M.R., Phillips T.J., et al. Photodynamic therapy with aminolevulinic acid topical solution and visible blue light in the treatment of multiple actinic keratoses of the face and scalp. Arch. Dermatol. 2004;140:41–46. doi: 10.1001/archderm.140.1.41[↩]
- Tschen E.H., Wong D.S., Pariser D.M., Dunlap F.E., Houlihan A., Ferdon M.B., Bruce S., Jarratt M.T., Loss R.W., Weiss J., et al. Photodynamic therapy using aminolaevulinic acid for patients with nonhyperkeratotic actinic keratoses of the face and scalp: Phase IV multicentre clinical trial with 12-month follow up. Br. J. Dermatol. 2006;155:1262–1269. doi: 10.1111/j.1365-2133.2006.07520.x[↩][↩]
- Pariser D.M., Lowe N.J., Stewart D.M., Jarratt M.T., Lucky A.W., Pariser R.J., Yamauchi P.S. Photodynamic therapy with topical methyl aminolevulinate for actinic keratosis: Results of a prospective randomized multicenter trial. J. Am. Acad. Dermatol. 2003;48:227–232. doi: 10.1067/mjd.2003.49[↩]
- Tarstedt M., Rosdahl I., Berne B., Svanberg K., Wennberg A.M. A randomized multicenter study to compare two treatment regimens of topical methyl aminolevulinate (Metvix®)-PDT in actinic keratosis of the face and scalp. Acta Derm. Venereol. 2005;85:424–428. doi: 10.1080/00015550510032887[↩]
- Roozeboom M.H., Arits A.H.M.M., Mosterd K., Sommer A., Essers B.A.B., de Rooij M.J.M., Quaedvlieg P.J.F., Steijlen P.M., Nelemans P.J., Kelleners-Smeets N.W.J. Three-year follow-up results of photodynamic therapy vs. imiquimod vs. fluorouracil for treatment of superficial basal cell carcinoma: A single-blind, noninferiority, randomized controlled trial. J. Investig. Dermatol. 2016;136:1568–1574. doi: 10.1016/j.jid.2016.03.043[↩]
- Kessels J., Hendriks J., Nelemans P., Mosterd K., Kelleners-Smeets N. Two-fold illumination in topical 5-aminolevulinic acid (ALA)-mediated photodynamic therapy (PDT) for superficial basal cell carcinoma (sBCC): A retrospective case series and cohort study. J. Am. Acad. Dermatol. 2016;74:899–906. doi: 10.1016/j.jaad.2015.12.009[↩]
- Roozeboom M.H., Aardoom M.A., Nelemans P.J., Thissen M.R.T.M., Kelleners-Smeets N.W.J., Kuijpers D.I.M., Mosterd K. Fractionated 5-aminolevulinic acid photodynamic therapy after partial debulking versus surgical excision for nodular basal cell carcinoma: A randomized controlled trial with at least 5-year follow-up. J. Am. Acad. Dermatol. 2013;69:280–287. doi: 10.1016/j.jaad.2013.02.014[↩]
- Rhodes L.E., de Rie M., Enstrom Y., Groves R., Morken T., Goulden V., Wong G.A., Grob J.J., Varma S., Wolf P. Photodynamic therapy using topical methyl aminolevulinate vs. surgery for nodular basal cell carcinoma: Results of a multicenter randomized prospective trial. Arch. Dermatol. 2007;143:1131–1136. doi: 10.1001/archderm.143.9.1131[↩][↩]
- Christensen E., Mørk C., Skogvoll E. High and sustained efficacy after two sessions of topical 5-aminolaevulinic acid photodynamic therapy for basal cell carcinoma: A prospective, clinical and histological 10-year follow-up study. Br. J. Dermatol. 2012;166:1342–1348. doi: 10.1111/j.1365-2133.2012.10878.x[↩]
- Zou Y., Zhao Y., Yu J., Luo X., Han J., Ye Z., Li J., Lin H. Photodynamic therapy versus surgical excision to basal cell carcinoma: Meta-analysis. J. Cosmet. Dermatol. 2016 doi: 10.1111/jocd.12236[↩]
- Szeimies R.M., Ibbotson S., Murrell D.F., Rubel D., Frambach Y., De Berker D., Dummer R., Kerrouche N., Villemagne H. A clinical study comparing methyl aminolevulinate photodynamic therapy and surgery in small superficial basal cell carcinoma (8–20 mm), with a 12-month follow-up. J. Eur. Acad. Dermatol. Venereol. 2008;22:1302–1311. doi: 10.1111/j.1468-3083.2008.02803.x[↩]
- Vinciullo C., Elliott T., Francis D., Gebauer K., Spelman L., Nguyen R., Weightman W., Sheridan A., Reid C., Czarnecki D., et al. Photodynamic therapy with topical methyl aminolaevulinate for “difficult-to-treat” basal cell carcinoma. Br. J. Dermatol. 2005;152:765–772. doi: 10.1111/j.1365-2133.2005.06484.x[↩]
- Fernandez-Guarino M., Harto A., Jaen P. Pulsed dye laser does not seem as effective as red light in basal cell carcinoma mal-pdt: A small pilot study. J. Skin Cancer. 2012 doi: 10.1155/2012/396481[↩]
- Carija A., Puizina-Iviv N., Vukovic D., Kovacevic L.M., Capkun V. Single treatment of low-risk basal cell carcinomas with pulsed dye laser-mediated photodynamic therapy (PDL-PDT) compared with photodynamic therapy (PDT): A controlled, investigator-blinded, intra-individual prospective study. Photodiagn. Photodyn. Ther. 2016;16:60–65. doi: 10.1016/j.pdpdt.2016.08.003[↩]
- Morton C.A. Methyl Aminolevulinate: Actinic Keratoses and Bowen’s Disease. Dermatol. Clin. 2007;25:81–87. doi: 10.1016/j.det.2006.09.009[↩]
- Fink-Puches R., Soyer H.P., Hofer A., Kerl H., Wolf P. Long-term follow-up and histological changes of superficial nonmelanoma skin cancers treated with topical δ-aminolevulinic acid photodynamic therapy. Arch. Dermatol. 1998;134:821–826. doi: 10.1001/archderm.134.7.821[↩]
- Cabete J., Rafael M., Cravo M., Moura C., Sachse F., Pecegueiro M. Long-term recurrence of nonmelanoma skin cancer after topical methylaminolevulinate photodynamic therapy in a dermato-oncology department. An. Bras. Dermatol. 2015;90:846–850. doi: 10.1590/abd1806-4841.20154080[↩]
- Morton C., Horn M., Leman J., Tack B., Bedane C., Tjioe M., Ibbotson S., Khemis A., Wolf P. Comparison of topical methyl aminolevulinate photodynamic therapy with cryotherapy or fluorouracil for treatment of squamous cell carcinoma in situ—Results of a multicenter randomized trial. Arch. Dermatol. 2006;142:729–735. doi: 10.1001/archderm.142.6.729[↩][↩]
- Tarstedt M., Gillstedt M., Wennberg Larkö A.-M., Paoli J. Aminolevulinic acid and methyl aminolevulinate equally effective in topical photodynamic therapy for non-melanoma skin cancers. J. Eur. Acad. Dermatol. Venereol. 2016;30:420–423. doi: 10.1111/jdv.13558[↩]
- Willey A., Mehta S., Lee P.K. Reduction in the incidence of squamous cell carcinoma in solid organ transplant recipients treated with cyclic photodynamic therapy. Dermatologic Surg. 2010;36:652–658. doi: 10.1111/j.1524-4725.2009.01384.x[↩]
- Wennberg A.M., Stenquist B., Stockfleth E., Keohane S., Lear J.T., Jemec G., Mork C., Christensen E., Kapp A., Solvsten H., et al. Photodynamic therapy with methyl aminolevulinate for prevention of new skin lesions in transplant recipients: A randomized study. Transplantation. 2008;86:423–429. doi: 10.1097/TP.0b013e318180731e[↩]
- Borgia F, Giuffrida R, Caradonna E, Vaccaro M, Guarneri F, Cannavò SP. Early and Late Onset Side Effects of Photodynamic Therapy. Biomedicines. 2018;6(1):12. doi:10.3390/biomedicines6010012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5874669/[↩]
- Tran D.T., Salmon R. Field treatment of facial and scalp actinic keratoses with photodynamic therapy: Survey of patient perceptions of treatment satisfaction and outcomes. Australas. J. Dermatol. 2011;52:195–201. doi: 10.1111/j.1440-0960.2011.00785.x https://www.ncbi.nlm.nih.gov/pubmed/21834815[↩]
- Valentine R., Ibbotson S.H., Brown T.A., Wood K., Moseley H. A quantitative comparison of 5-aminolaevulinic acid and methyl aminolevulinate-induced fluorescence, photobleaching and pain during photodynamic therapy. Photochem. Photobiol. 2011;87:242–249. doi: 10.1111/j.1751-1097.2010.00829.x https://www.ncbi.nlm.nih.gov/pubmed/21077899[↩]
- Borroni R.G., Carugno A., Rivetti N., Arbustini E., Brazzelli V. Risk of acute postoperative hypertension after topical photodynamic therapy for non-melanoma skin cancer. Photodermatol. Photoimmunol. Photomed. 2013;29:73–77. doi: 10.1111/phpp.12019 https://www.ncbi.nlm.nih.gov/pubmed/23458390[↩][↩]
- Gholam P., Kroehl V., Enk A.H. Dermatology life quality index and side effects after topical photodynamic therapy of actinic keratosis. Dermatology. 2013;226:253–259. doi: 10.1159/000349992[↩]
- Middelburg T.A., Nijsten T., Neumann M.H., de Haas E.R., Robinson D.J. Red light ALA-PDT for large areas of actinic keratosis is limited by severe pain and patient dissatisfaction. Photodermatol. Photoimmunol. Photomed. 2013;29:276–278. doi: 10.1111/phpp.12055 https://www.ncbi.nlm.nih.gov/pubmed/24001386[↩]
- Mahmound B.H., Hexsel C.L., Hamzavi I., Lim H.W. Effects of visible light on the skin. Photochem. Photobiol. Sci. 2008;84:450–462. doi: 10.1111/j.1751-1097.2007.00286.x https://www.ncbi.nlm.nih.gov/pubmed/18248499[↩]
- Hambly R.A., Mansoor N., Quinlan C., Shah Z., Lenane P., Ralph N., Moloney F.J. Factors predicting pain and effect of oral analgesia in topical photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2017;33:176–179. doi: 10.1111/phpp.12301 https://www.ncbi.nlm.nih.gov/pubmed/28196277[↩]
- Halldin C.B., Gillstedt M., Paoli J., Wennberg A.M., Gonzalez H. Predictors of pain associated with photodynamic therapy: A retrospective study of 658 treatments. Acta Derm. Venereol. 2011;91:545–551. doi: 10.2340/00015555-1101 https://www.ncbi.nlm.nih.gov/pubmed/21611684[↩]
- Kasche A., Luderschmidt S., Ring J., Hein R. Photodynamic therapy induces less pain in patients treated with methyl aminolevulinate compared to aminolevulinic acid. J. Drugs Dermatol. 2006;5:353–356. https://www.ncbi.nlm.nih.gov/pubmed/16673803[↩]
- Steinbauer J.M., Schreml S., Babilas P., Zeman F., Karrer S., Landthaler M., Szeimies R.M. Topical photodynamic therapy with porphyrin precursors-assessment of treatment—Associated pain in a retrospective study. Photochem. Photobiol. Sci. 2009;8:1111–1116. doi: 10.1039/b823378k[↩]
- Gaál M., Otrosinka S., Baltás E., Ocsai H., Oláh J., Kemény L., Gyulai R. Photodynamic therapy of non-melanoma skin cancer with methyl aminolaevulinate is associated with less pain than with aminolaevulinic acid. Acta Derm. Venereol. 2012;92:173–175. doi: 10.2340/00015555-1223[↩]
- Ibbotson S.H., Valentine R., Hearn R. Is the pain of topical photodynamic therapy with methyl aminolevulinate any different from thatA with 5-aminolaevulinic acid? Photodermatol. Photoimmunol. Photomed. 2012;28:272–273. doi: 10.1111/j.1600-0781.2012.00684.x[↩]
- Yazdanyar S., Zarchi K., Jemec G.B.E. Pain during topical photodynamic therapy—Comparing methyl aminolevulinate (Metvix®) to aminolaevulinic acid (Ameluz®); an intra-individual clinical study. Photodiagn. Photodyn. Ther. 2017;20:6–9. doi: 10.1016/j.pdpdt.2017.07.010 https://www.ncbi.nlm.nih.gov/pubmed/28780136[↩]
- Kanick S.C., Davis S.C., Zhao Y., Sheehan K.L., Hasan T., Maytin E.V., Pogue B.W., Chapman M.S. Pre-treatment protoporphyrin IX concentration in actinic keratosis lesions may be a predictive biomarker of response to aminolevulinic-acid based photodynamic therapy. Photodiagn. Photodyn. Ther. 2015;12:561–566. doi: 10.1016/j.pdpdt.2015.10.006 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4684466/[↩]
- Sandberg C., Stenquist B., Rosdahl I., Ros A.M., Synnerstad I., Karlsson M., Gudmundson F., Ericson M.B., Larkö O., Wennberg A.M. Important factors for pain during photodynamic therapy for actinic keratosis. Acta Derm. Venereol. 2006;86:404–408. doi: 10.2340/00015555-0098 https://www.ncbi.nlm.nih.gov/pubmed/16955183[↩]
- Braathen L.R., Paredes B.E., Saksela O., Fritsch C., Gardlo K., Morken T., Frølich K.W., Warloe T., Solér A.M., Ros A.M. Short incubation with methyl aminolevulinate for photodynamic therapy of actinic keratoses. J. Eur. Acad. Dermatol. Venereol. 2009;23:550–555. doi: 10.1111/j.1468-3083.2008.03029.x https://www.ncbi.nlm.nih.gov/pubmed/19415804[↩]
- Lerche C.M., Fabricius S., Philipsen P.A., Wulf H.C. Correlation between treatment time, photobleaching, inflammation and pain after photodynamic therapy with methyl aminolevulinate on tape-stripped skin in healthy volunteers. Photochem. Photobiol. Sci. 2015;14:875–882. doi: 10.1039/C5PP00069F https://www.ncbi.nlm.nih.gov/pubmed/25812618[↩][↩]
- Cottrell W.J., Paquette A.D., Keymel K.R., Foster T.H., Oseroff A.R. Irradiance-dependent photobleaching and pain in delta-aminolevulinic acid-photodynamic therapy of superficial basal cell carcinomas. Clin. Cancer Res. 2008;14:4475–4483. doi: 10.1158/1078-0432.CCR-07-5199[↩]
- Radakovic-Fijan S., Blecha-Thalhammer U., Kittler H., Hönigsmann H., Tanew A. Efficacy of 3 different light doses in the treatment of actinic keratosis with 5-aminolevulinic acid photodynamic therapy: A randomized, observer-blinded, intrapatient, comparison study. J. Am. Acad. Dermatol. 2005;53:823–827. doi: 10.1016/j.jaad.2005.06.010 https://www.ncbi.nlm.nih.gov/pubmed/16243131[↩]
- Wang B., Shi L., Zhang Y.F., Zhou Q., Zheng J., Szeimies R.M., Wang X.L. Gain with no pain? Pain management in dermatological photodynamic therapy. Br. J. Dermatol. 2017;177:656–665. doi: 10.1111/bjd.15344 https://www.ncbi.nlm.nih.gov/pubmed/28122416[↩][↩]
- Fargnoli M.C., Ibbotson S.H., Hunger R.E., Rostain G., Gaastra M.-T.W., Eibenschutz L., Cantisani C., Venema A.W., Medina S., Kerrouche N., et al. Patient and physician satisfaction in an observational study with methyl aminolevulinate daylight-photodynamic therapy in the treatment of multiple actinic keratoses of the face and scalp in 6 European countries. J. Eur. Acad. Dermatol. Venereol. 2017 doi: 10.1111/jdv.14691 https://www.ncbi.nlm.nih.gov/pubmed/29136306[↩]
- Gholam P., Kroehl V., Enk A.H. Dermatology life quality index and side effects after topical photodynamic therapy of actinic keratosis. Dermatology. 2013;226:253–259. doi: 10.1159/000349992 https://www.ncbi.nlm.nih.gov/pubmed/23796769[↩]
- Hambly R.A., Mansoor N., Quinlan C., Shah Z., Lenane P., Ralph N., Moloney F.J. Factors predicting pain and effect of oral analgesia in topical photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2017;33:176–179. doi: 10.1111/phpp.12301[↩]
- Middelburg T.A., Nijsten T., Neumann M.H., de Haas E.R., Robinson D.J. Red light ALA-PDT for large areas of actinic keratosis is limited by severe pain and patient dissatisfaction. Photodermatol. Photoimmunol. Photomed. 2013;29:276–278. doi: 10.1111/phpp.12055[↩]
- Lindeburg K.E., Brogaard H.M., Jemec G.B. Pain and photodynamic therapy. Dermatology. 2007;215:206–208. doi: 10.1159/000106577 https://www.ncbi.nlm.nih.gov/pubmed/17823516[↩][↩]
- Fink C., Enk A., Gholam P. Photodynamic therapy—Aspects of pain management. J. Dtsch. Dermatol. Ges. 2015;13:15–22. doi: 10.1111/ddg.12546 https://www.ncbi.nlm.nih.gov/pubmed/25640485[↩]
- Ibbotson S.H. Adverse effects of topical photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2011;27:116–130. doi: 10.1111/j.1600-0781.2010.00560.x[↩]
- Lehmann P. Side effects of topical photodynamic therapy. Hautarzt. 2007;58:597–603. doi: 10.1007/s00105-007-1363-4[↩]
- Esmann S., Jemec G.B. Patients’ perceptions of topical treatments of actinic keratosis. J. Dermatol. Treat. 2014;25:375–379. doi: 10.3109/09546634.2012.757285[↩]
- Brooke R.C., Sinha A., Sidhu M.K., Watson R.E., Church M.K., Friedmann P.S., Clough G.F., Rhodes L.E. Histamine is released following aminolevulinic acid-photodynamic therapy of human skin and mediates an aminolevulinic acid dose-related immediate inflammatory response. J. Investig. Dermatol. 2006;126:2296–2301. doi: 10.1038/sj.jid.5700449[↩]
- Vanaman Wilson M.J., Jones I.T., Wu D.C., Goldman M.P. A randomized, double-blind, placebo-controlled clinical trial evaluating the role of systemic antihistamine therapy for the reduction of adverse effects associated with topical 5-aminolevulinic acid photodynamic therapy. Lasers Surg. Med. 2017;49:738–742. doi: 10.1002/lsm.22682[↩]
- Brooke R.C., Sidhu M., Sinha A., Watson R.E., Friedmann P.S., Clough G.F., Rhodes L.E. Prostaglandin E2 and nitric oxide mediate the acute inflammatory (erythemal) response to topical 5-aminolaevulinic acid therapy in human skin. Br. J. Dermatol. 2013;169:645–652. doi: 10.1111/bjd.12562[↩]
- Kerr A.C., Ferguson J., Ibbotson S.H. Acute phototoxicity with urticarial features during topical 5-aminolaevulinic acid photodynamic therapy. Clin. Exp. Dermatol. 2007;32:201–202. doi: 10.1111/j.1365-2230.2006.02327.x.[↩]
- Kaae J., Philipsen P.A., Haedersdal M., Wulf H.C. Immediate whealing urticaria in red light exposed areas during photodynamic therapy. Acta Derm. Venereol. 2008;88:480–483. doi: 10.2340/00015555-0474[↩]
- Miguélez A., Martín-Santiago A., Bauzá A., Gilaberte Y. Urticaria-like reaction secondary to photodynamic therapy in 2 pediatric patients. Actas Dermosifiliogr. 2013;104:727–729. doi: 10.1016/j.ad.2012.12.002[↩]
- Wulf H.C., Philipsen P. Allergic contact dermatitis to 5-aminolaevulinic acid methylester but not to 5-aminolaevulinic acid after photodynamic therapy. Br. J. Dermatol. 2004;150:143–145. doi: 10.1111/j.1365-2133.2004.05723.x[↩]
- Pastor-Nieto M.A., Jiménez-Blázquez E., Sánchez-Herreros C., Belmar-Flores P. Allergic contact dermatitis caused by methyl aminolevulinate. Actas Dermosifiliogr. 2013;104:168–170. doi: 10.1016/j.ad.2012.02.016[↩]
- Al Malki A., Marguery M.C., Giordano-Labadie F., Konstantinou M.P., Mokeddem L., Lamant L., Paul C., Maza A., Mazereeuw-Hautier J. Systemic allergic contact dermatitis caused by methyl aminolaevulinate in a patient with keratosis-ichthyosis-deafness syndrome. Contact Dermat. 2017;76:190–192. doi: 10.1111/cod.12703[↩]
- Mroz P., Hamblin M.R. The immunosuppressive side of PDT. Photochem. Photobiol. Sci. 2011;10:751–758. doi: 10.1039/c0pp00345j[↩]
- Korbelik M. PDT-associated host response and its role in the therapy outcome. Lasers Surg. Med. 2006;38:500–508. doi: 10.1002/lsm.20337[↩]
- Mroz P., Szokalska A., Wu M.X., Hamblin M.R. Photodynamic Therapy of Tumors Can Lead to Development of Systemic Antigen-Specific Immune Response. PLoS ONE. 2010;5:e15194 doi: 10.1371/journal.pone.0015194[↩]
- Matthews Y.J., Damian D.L. Topical photodynamic therapy is immunosuppressive in humans. Br. J. Dermatol. 2010;162:637–641. doi: 10.1111/j.1365-2133.2009.09562.x[↩]
- Evangelou G., Farrar M.D., Cotterell L., Andrew S., Tosca A.D., Watson R.B.E., Rhodes L.E. Topical photodynamic therapy significantly reduces epidermal Langerhans cells during clinical treatment of basal cell carcinoma. Br. J. Dermatol. 2012;166:1112–1115. doi: 10.1111/j.1365-2133.2012.10823.x[↩]
- Thanos S.M., Halliday G.M., Damian D.L. Nicotinamide reduces photodynamic therapy-induced immunosuppression in humans. Br. J. Dermatol. 2012;167:631–636. doi: 10.1111/j.1365-2133.2012.11109.x[↩][↩]
- Frost G.A., Halliday G.M., Damian D.L. Photodynamic therapy-induced immunosuppression in humans is prevented by reducing the rate of light delivery. J. Investig. Dermatol. 2011;131:962–968. doi: 10.1038/jid.2010.429[↩]
- Wolfe C.M., Hatfield K., Cognetta A.B. Cellulitis as a postprocedural complication of topical 5-aminolevulinic acid photodynamic therapy in the treatment of actinic keratosis. J. Drugs Dermatol. 2007;6:544–548[↩]
- Guarneri C., Vaccaro M. Erosive pustular dermatosis of the scalp following topical methylaminolaevulinate photodynamic therapy. J. Am. Acad. Dermatol. 2009;60:521–522. doi: 10.1016/j.jaad.2008.09.006[↩]
- Rongioletti F., Chinazzo C., Javor S. Erosive pustular dermatosis of the scalp induced by ingenol mebutate. J. Eur. Acad. Dermatol. Venereol. 2016;30:e110–e111. doi: 10.1111/jdv.13350[↩]
- Le T.T., Skak K., Schroder K., Schroder W.A., Boyle G.M., Pierce C.J., Suhrbier A. IL-1 Contributes to the Anti-Cancer Efficacy of Ingenol Mebutate. PLoS ONE. 2016;21:e0153975 doi: 10.1371/journal.pone.0153975[↩]
- Gemigniani F., Bodet D., González-Llavona B., García-Patos V. Peripheral facial palsy after topical photodynamic therapy for facial actinic keratoses. J. Am. Acad. Dermatol. 2014;71:e90–e92. doi: 10.1016/j.jaad.2014.03.008[↩]
- Ratour-Bigot C., Chemidling M., Montlahuc C., Abirached G., Madjlessi N., Bullier C., Battistella M., Bagot M., Lebbe C., Basset-Seguin N. Squamous Cell Carcinoma Following Photodynamic Therapy for Cutaneous Bowen’s Disease in a Series of 105 Patients. Acta Derm. Venereol. 2016;96:658–663. doi: 10.2340/00015555-2330 https://www.ncbi.nlm.nih.gov/pubmed/26714426[↩]
- Wolf P., Fink-Puches R., Reimann-Weber A., Kerl H. Development of malignant melanoma after repeated topical photodynamic therapy with 5-aminolevulinic acid at the exposed site. Dermatology. 1997;194:53–54. doi: 10.1159/000246057 https://www.karger.com/Article/Abstract/246057[↩]
- Schreml S., Gantner S., Steinbauer J., Babilas P., Landthaler M., Szeimies R.M. Melanoma promotion after photodynamic therapy of a suspected Bowen’s disease (in situ squamous cell carcinoma) lesion. Dermatology. 2009;219:279–281. doi: 10.1159/000236026[↩]
- Wolf P., Kerl H. Photodynamic therapy in patient with xeroderma pigmentosum. Lancet. 1991;337:1613–1614. doi: 10.1016/0140-6736(91)93315-Z[↩]
- Kick G., Messer G., Plewig G., Kind P., Goetz A.E. Strong and prolonged induction of c-jun and c-fos proto-oncogenes by photodynamic therapy. Br. J. Cancer. 1996;74:30–36. doi: 10.1038/bjc.1996.311[↩]
- Giri U., Iqbal M., Athar M. Porphyrin-mediated photosensitization has a weak tumor promoting activity in mouse skin: Possible role of in situ-generated reactive oxygen species. Carcinogenesis. 1996;17:2023–2028. doi: 10.1093/carcin/17.9.2023[↩][↩]
- Miyazu Y.M., Miyazawa T., Hiyama K., Kurimoto N., Iwamoto Y., Matsuura H., Kanoh K., Kohno N., Nishiyama M., Hiyama E. Telomerase expression in noncancerous bronchial epithelia is a possible marker of early development of lung cancer. Cancer Res. 2005;65:9623–9627. doi: 10.1158/0008-5472.CAN-05-0976.[↩]
- Gilaberte Y., Milla L., Salazar N., Vera-Alvarez J., Kourani O., Damian A., Rivarola V., Roca M.J., Espada J., González S., Juarranz A. Cellular intrinsic factors involved in the resistance of squamous cell carcinoma to photodynamic therapy. J. Investig. Dermatol. 2014;134:2428–2437. doi: 10.1038/jid.2014.178[↩][↩]
- Brabender J., Danenberg K.D., Metzger R., Schneider P.M., Park J., Salonga D., Hölscher A.H., Danenberg P.V. Epidermal growth factor receptor and HER2-neu mRNA expression in non-small cell lung cancer Is correlated with survival. Clin. Cancer Res. 2001;7:1850–1855[↩]
- Shimizu T., Izumi H., Oga A., Furumoto H., Murakami T., Ofuji R., Muto M., Sasaki K. Epidermal growth factor receptor overexpression and genetic aberrations in metastatic squamous-cell carcinoma of the skin. Dermatology. 2001;202:203–206. doi: 10.1159/000051637[↩]
- Alao J.P. The regulation of cyclin D1 degradation: Roles in cancer development and the potential for therapeutic invention. Mol. Cancer. 2007;6:24. doi: 10.1186/1476-4598-6-24[↩]
- Moreno Romero J.A., Campoy A., Perez N., Garcia F., Grimalt R. Rapidly-growing squamous cell carcinoma shortly after treatment with ingenol mebutate for actinic keratoses: Report of two cases. Br. J. Dermatol. 2015;173:1514–1517. doi: 10.1111/bjd.14054[↩]
- Freiberger S.N., Cheng P.F., Iotzova-Weiss G., Neu J., Liu Q., Dziunycz P., Zibert J.R., Dummer R., Skak K., Levesque M.P., et al. Ingenol Mebutate Signals via PKC/MEK/ERK in Keratinocytes and Induces Interleukin Decoy Receptors IL1R2 and IL13RA2. Mol. Cancer Ther. 2015;14:2132–2142. doi: 10.1158/1535-7163.MCT-15-0023-T[↩]





{kind=link}