
Contents
What is pleomorphic adenoma
Pleomorphic adenoma also known as benign mixed tumor, is the most common benign salivary tumor, which predominantly affect the superficial lobe of the parotid gland and are usually slow growing 1. The “pleomorphic” nature of the tumor can be explained on the basis of its epithelial and connective tissue origin. Pleomorphic adenoma has a female predilection between 30–50 years of age. Slowly progressing asymptomatic swelling is the usual presentation of the tumor. Your doctor is likely to suggest surgery to remove pleomorphic adenomas with utmost care taken to preserve the facial nerve, as there is a small risk of a cancer developing within the tumor. You might have a course of radiotherapy if your benign pleomorphic adenomas is likely to come back again.
It is not uncommon for pleomorphic adenomas to recur and though benign, a subset will undergo malignant transformation or carcinoma ex pleomorphic adenoma. Malignant changes in pleomorphic adenoma have been associated with a long duration, tumor recurrence, radiation therapy, an advanced age, and tumor size. Because the incidence of malignancy is correlated with the duration of pleomorphic adenoma, the risk of developing malignancy is only about 1.5% for a duration of <5 years but increases to 9.5% for a duration of >15 years 2.
There are two main types of salivary glands called the:
- major salivary glands
- minor salivary glands
You have 3 main pairs of major salivary glands (see Figure 1), the:
- Parotid glands – just under the lobes of your ears
- Sublingual glands – under your tongue
- Submandibular glands – under each side of your jawbone
As well as the 3 major pairs of salivary glands you have over 600 smaller, minor salivary glands throughout the lining of the mouth and throat.
Pleomorphic adenoma is located in the parotid glands (85%), minor salivary glands (10%), and the submandibular glands (5%) 3. In the majority of cases, the tumors originate in the superficial lobe. However, occasional pleomorphic adenoma cases may involve the deep lobe of the parotid gland 4 and the parapharyngeal space. Minor salivary gland pleomorphic adenomas are frequently encountered on the palate, followed by the lip, cheek, tongue and floor of the mouth 5.
Pleomorphic adenoma mostly presents as a solitary mobile slow-growing, painless mass or parotid gland swelling without facial nerve involvement, which may be present for many years 6. Symptoms and signs mainly depend on size, location, and potential to undergo malignant transformation. In the parotid gland, signs of facial nerve weakness occur when the tumor is large or if it undergoes malignant change. Pleomorphic adenoma in the deep lobe of the parotid gland may present as an oral retro tonsillar or para-pharyngeal mass which is visible or usually palpable. Rapid enlargement of a tumor nodule should raise a concern of malignant change. Minor salivary gland tumors may present with a variety of symptoms, including dysphagia, hoarseness, dyspnea, difficulty in chewing, and epistaxis dependent on the site of the tumor.
Pleomorphic adenomas are best treated by a wide local excision with good safety margins and follow-up for at least 3–4 years 7.
Figure 1. Major salivary glands
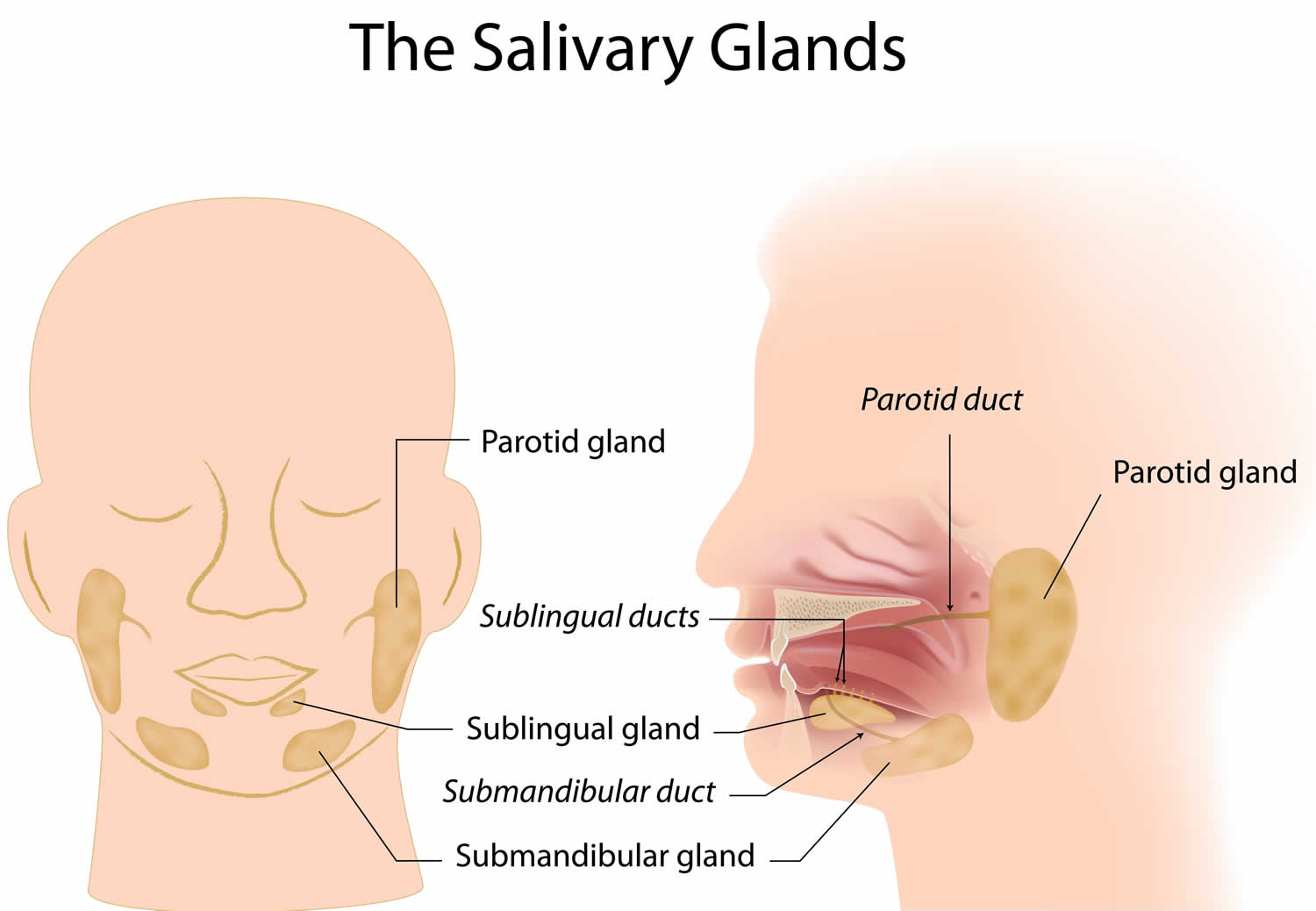
Figure 2. Pleomorphic adenoma post-op

Footnote: (A) Post- operative facial view. (B) Lateral view showing no recurrence of lesion after follow-up of 3 years.
[Source 1 ]Carcinoma ex pleomorphic adenoma
Carcinoma ex pleomorphic adenoma is an infrequent aggressive cancer but is the most common of three malignant mixed tumors of salivary glands, and are thought to arise from pre-existing pleomorphic adenomas (or benign mixed tumors) 2. Carcinoma ex pleomorphic adenoma accounts for 3.6% (range, 0.9%–14%) of all salivary neoplasms and for 11.7% (range, 2.8%–42.4%) of salivary malignancies 8.
Carcinoma ex pleomorphic adenomas usually occur in older patients (6th to 8th decade), who have had a pleomorphic adenoma in situ for many years (typically 10-15 years) 2. Because the incidence of malignancy is correlated with the duration of pleomorphic adenoma, the risk of developing malignancy is only about 1.5% for a duration of <5 years but increases to 9.5% for a duration of >15 years 9.
The typical clinical presentation in a patient with carcinoma ex pleomorphic adenoma is a longstanding history (average, 10–15 years) of pleomorphic adenoma and a sudden period of rapid growth (average, 3–6 months). Pain and facial nerve paralysis are often present due to tumor infiltration 2. Carcinoma ex pleomorphic adenoma usually is a more poorly circumscribed mass than benign pleomorphic adenoma; is most likely to occur within the major salivary glands, especially the parotid gland; and typically occurs in patients in the sixth-to-eighth decades of life.
Carcinoma ex pleomorphic adenomas have a high rate of metastasis at the time of diagnosis (25-76%) typically to brain, bone, lungs and of course local lymph nodes 10.
Carcinoma ex pleomorphic adenomas are associated with a 5-year survival rate of about 50% 11. The development of associated metastatic disease is considered preterminal 11.
Pleomorphic adenoma causes
The exact cause of pleomorphic adenoma is obscure although the incidence has been increasing in the last 15–20 years in relation to the exposure of radiation 1. Prior head and neck irradiation is also a risk factor for the development of pleomorphic adenomas 12. Few studies have suggested an association of the tumor with simian virus 40 (SV 40) 13.
Pleomorphic adenoma symptoms
Pleomorphic adenoma usually presents as a slow-growing, painless mass, which may be present for many years. Symptoms and signs depend on the location 14.
When pleomorphic adenoma occurs in the parotid gland, signs of facial nerve weakness are seldom encountered; however, if the tumor is large and has been neglected, facial nerve weakness is likely to arise as the result of malignant change. Pleomorphic adenoma in the deep lobe of the parotid gland may present as an oral retrotonsillar mass or parapharyngeal space tumor; indeed, tumors arising at this site are the source of the most common parapharyngeal space tumors. Rapid enlargement of a tumor nodule should raise concern about the development of malignant change.
Patients with minor salivary gland pleomorphic adenomas may present with a variety of symptoms, depending on the site of the tumor; such symptoms include dysphagia, dyspnea, hoarseness, difficulty in chewing, and epistaxis.
Pleomorphic adenoma diagnosis
On gross examination, a pleomorphic adenoma is a single firm, mobile, well-circumscribed mass. Its color may vary from whitish-tan to gray to bluish, and its size may range from a few millimeters to quite large or even giant 15. Pleomorphic adenomas are irregularly shaped and have a bosselated surface. Recurrent tumors characteristically tend to present as multiple nodules of variable size.
The diagnosis is made both on tissue sampling and radiographic studies. Tissue sampling procedures including fine needle aspiration (FNA) and core needle biopsy which can be done in an outpatient setting. These procedures are associated with very low tumor seeding rates 16.
Fine needle aspiration (FNA) can determine whether the tumor is malignant in nature with an approximate sensitivity of 90%. Core needle biopsy is more invasive but provides more accurate histological typing of the tumor with a diagnostic accuracy of around 97%. Immunohistochemistry may prove to be supportive in delineating the different cell components.
Pleomorphic adenoma radiology
X-rays
If you have a lump or swelling near your jaw, your doctor may order x-rays of your jaws and teeth to look for a tumor.
If you’ve been diagnosed with cancer, an x-ray of your chest may be done to see if the cancer has spread to your lungs. This also provides other information about your heart and lungs that might be useful if surgery is planned.
Computed tomography (CT or CAT) scan
A CT scan uses x-rays to produce detailed cross-sectional images of your body. Unlike a regular x-ray, CT scans can show the detail in soft tissues (such as internal organs). A CT scan can show the size, shape, and position of a tumor and can help find enlarged lymph nodes that might contain cancer. If needed, CT scans can also be used to look for tumors in other parts of the body.
Before the scan, you may be asked to drink 1 to 2 pints of a liquid called oral contrast. This helps outline the structures in your head and neck so that certain areas are not mistaken for tumors. You may also receive an IV (intravenous) line through which a different kind of contrast dye (IV contrast) is injected. This helps better outline structures in your body.
CT examination a pleomorphic adenoma usually appears as smoothly marginated or lobulated homogeneous soft tissue density globular mass. Necrosis can be seen in larger masses. Few foci of calcification are common. Smaller tumors show early homogenous prominent enhancement while in the case of larger tumors enhancement is less marked and delayed.
Magnetic resonance imaging (MRI) scan
Like CT scans, MRI scans make detailed images of soft tissues in the body. But MRI scans use radio waves and strong magnets instead of x-rays. The energy from the radio waves is absorbed and then released in a pattern formed by the type of body tissue and by certain diseases. A computer translates the pattern into very detailed images of parts of the body. A contrast material called gadolinium is often injected into a vein before the scan to better see details.
MRI scans can help determine the exact location and extent of a tumor. They can also show any lymph nodes that are enlarged or if other organs have suspicious spots, which might be due to the spread of cancer.
MRI is similar to CT; smaller masses appear well-circumscribed and homogeneous whereas larger tumors appear heterogeneous.
- T1: usually of low intensity.
- T2: usually of very high intensity (especially myxoid type) 6 often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule.
- T1 C+ (Gd): usually demonstrates homogeneous enhancement.
- The presence of either T2 hypointensity or ill-defined margins after contrast administration can be a simple MR imaging malignancy test for parotid tumors, with a sensitivity and specificity of 0.70 and 0.73, respectively.
- Post contrast STIR images help the delineate the perineural spread of tumor in case of malignant change.
Ultrasound
Ultrasound pleomorphic adenomas characteristically appear hypoechoic in texture. They usually show a lobulated distinct border with or without posterior acoustic enhancement. Ultrasound guided biopsy or FNA are minimally invasive and cost effective procedures.
Angiography (DSA) can also be considered.
Positron emission tomography (PET) scan
A PET scan looks for areas of high cellular activity (which might be a sign of cancer), rather than just showing if areas look abnormal based on their size or shape. This test can help show whether an abnormal lump or tumor seen on another imaging test may be cancer. If you have been diagnosed with cancer, your doctor may use this test to see if the cancer has spread to lymph nodes or other parts of the body. A PET scan can also be useful if your doctor thinks the cancer might have spread but doesn’t know where.
Biopsy
Symptoms and the results of exams or imaging tests may strongly suggest you have salivary gland cancer, but the actual diagnosis is made by removing cells from an abnormal area and looking at them under a microscope. This is known as a biopsy. Different types of biopsies might be done, depending on the situation.
Fine needle aspiration (FNA) biopsy
An FNA biopsy is used to remove a small amount of cells and fluid from a lump or tumor for testing. This type of biopsy can be done in a doctor’s office or clinic. It’s done with a thin, hollow needle much like those used for routine blood tests.
Your doctor may first numb the area over the tumor. The doctor then puts the needle right into the tumor and pulls cells and a few drops of fluid into a syringe. The sample is then sent to a lab, where it’s checked under a microscope to look for cancer cells.
Doctors may use FNA if they are not sure whether a lump is a salivary gland cancer. The FNA might show the lump is due to an infection, a benign (non-cancerous) salivary tumor, or a salivary gland cancer. In some cases this type of biopsy can help a person avoid unnecessary surgery.
An FNA biopsy is only helpful if enough cells are taken out to be able to tell for certain what a tumor is made of. But sometimes not enough cells are removed, or the biopsy is read as negative (normal) even when the tumor is cancer. If the doctor is not sure about the FNA results, a different type of biopsy might be needed.
Incisional biopsy
This type of biopsy may sometimes be done if the FNA biopsy didn’t get a large enough sample. In this procedure, the surgeon numbs the area over the tumor, makes a small incision (cut) with a scalpel and takes out a tiny part of the tumor. The specimen is sent to the lab to be looked at by the pathologist. These types of biopsies are not done often for salivary gland tumors.
Surgery
As mentioned above, FNA biopsy of a suspected salivary gland cancer may not always provide a clear answer. If this is the case but the physical exam and imaging tests suggest that it is cancer, the doctor may advise surgery to remove the tumor completely. This can both provide enough of a sample for a diagnosis and treat the tumor at the same time.
In some cases if the exams and tests suggest cancer is likely, the doctor may skip the FNA biopsy altogether and go directly to surgery to remove the tumor. The specimen is then sent to the lab to confirm the diagnosis.
Pleomorphic adenoma cytology
World Health Organization (1972) defined pleomorphic adenoma as a well-defined tumor characterized by its pleomorphic or mixed appearance. There is intermixing of the clearly recognizable epithelial component with mucoid, myxoid and chondroid component 17. Although the lesion presents several histological features due to the different compounds with a myxoid or chondroid matrix, it is generally considered to be a benign neoplasm 18.
Microscopic (histologic) description of pleomorphic adenoma:
- Not as well circumscribed as may grossly appear, with tongue like protrusions into surrounding salivary gland
- Thick capsule if present in deep parotid lobe
- Biphasic population of epithelial and mesenchymal cells
- Epithelial cells are glandular or occasionally squamous; may be spindled or oval, have large hyperchromatic nuclei
- Myoepithelial basal layer or overlying pseudoepitheliomatous hyperplasia; tumor may be very cellular
- Stroma is myxoid, hyaline, chondroid, rarely adipose tissue or osseous; mucin often present
- Occasional angiolymphatic invasion
- May have adenoid cystic pattern
- No mitotic figures, no necrosis
Figure 3. Pleomorphic adenoma CT scan and cytology
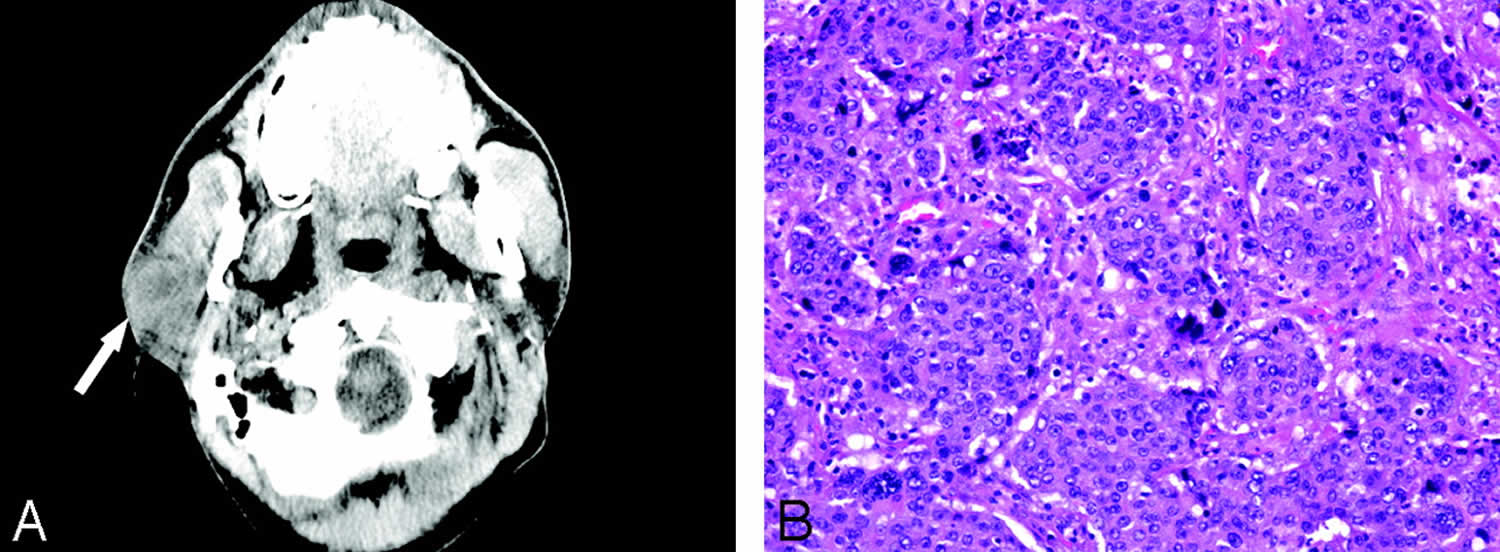
Footnote: A, Axial image from noncontrast CT examination of the head demonstrates a heterogeneous mass involving the superficial right parotid gland (arrow).B, Photomicrograph of tumor in A demonstrates nests of basophilic tumor cells arising from a pleomorphic adenoma. (H&E stain × 100).
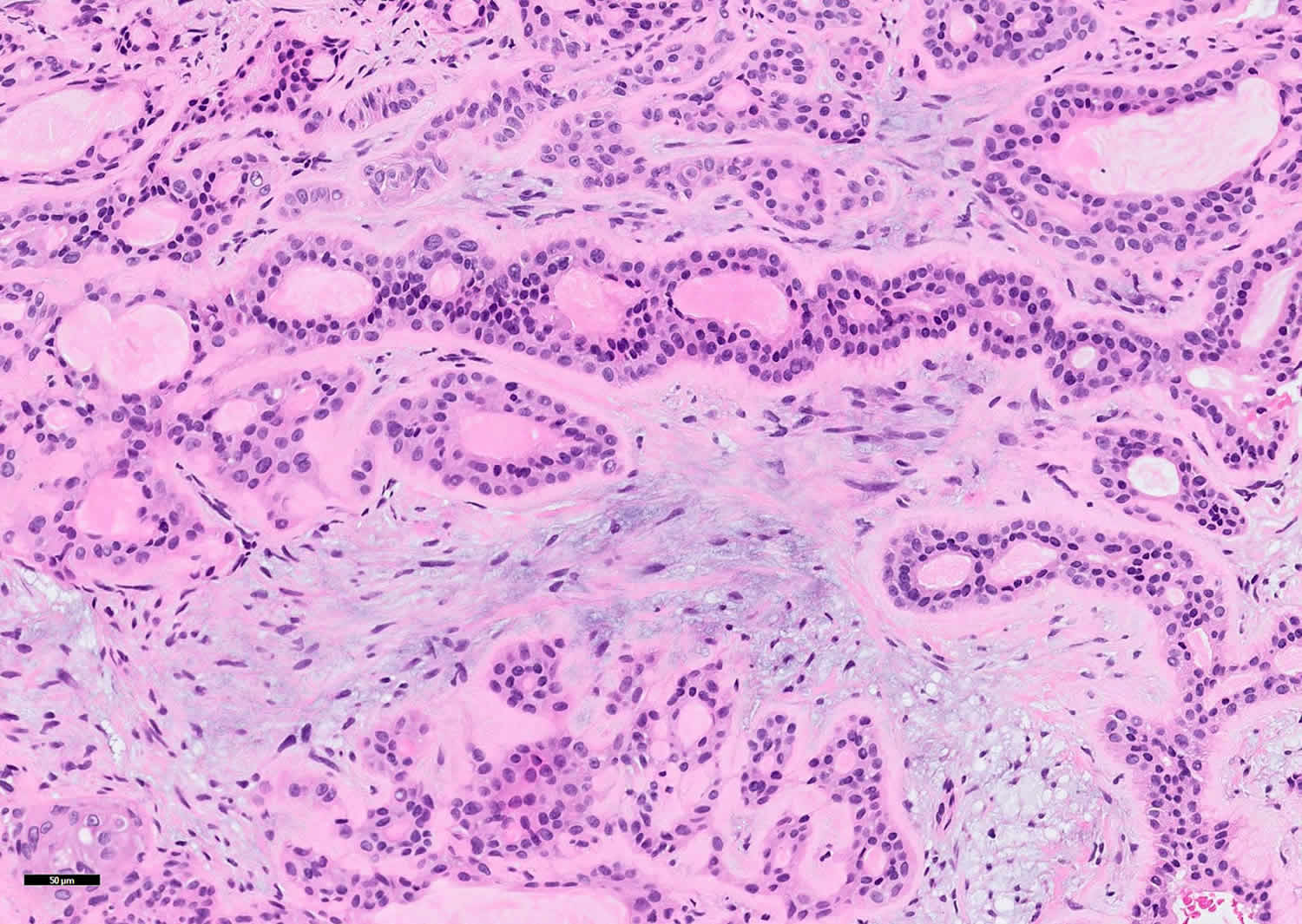
[Source 19 ]Figure 4. Pleomorphic adenoma cytology
Pleomorphic adenoma treatment
Pleomorphic adenomas harbor a small risk of malignant transformation. The malignant potential is proportional to the time the lesion is in situ (1.5% in the first five years, 9.5% after 15 years). Therefore, excision is warranted in almost all cases. Other risk factors for malignancy include advanced age, radiation therapy, large size, and recurrent tumors.
Because of the potential for malignant transformation, surgical excision is currently the most widely accepted treatment of pleomorphic adenomas 20. Benign pleomorphic adenomas have a tendency to recur at a rate of 1%–50%, depending largely on the surgical technique of excision 11. Enucleation of pleomorphic adenoma results in a higher rate of recurrence versus superficial or total parotidectomy. Enucleation procedure has been abandoned because of high associated rates of recurrence.
Presently pleomorphic adenoma of the parotid gland is treated either with superficial (Patey’s operation) or total parotidectomy with the latter being the more frequently performed procedure due to lower incidence of recurrence 21. Meticulous technique is required to preserve the facial nerve. Pleomorphic adenomas of the submandibular glands are treated with simple excision procedure with preservation of adjacent nerve including the mandibular branch of the trigeminal nerve, the hypoglossal nerve, and the lingual nerve 22.
When pleomorphic adenoma is in the minor salivary glands, a five mm margin should be obtained. These tumors do not invade into periosteum. Thus, the bone need not be resected. When tumor bed recurrences occur, they show significant resistance to treatment, with management options including monitoring only, surgery, and radiotherapy 21.
In addition, pleomorphic adenomas have a false-capsule composed of compressed surrounding normal salivary tissue. Recurrence (or residual tumor) tends to be more likely in patients in whom capsular rupture occurs at the time of surgical resection and in patients in whom the podlike extensions of tumor extend beyond the capsule 20. Similarly, if a focus of malignant transformation is confined within the fibrous capsule, it tends to behave in a more benign manner and carry a better prognosis, which is similar to that of a benign mixed tumor 8. Conversely, malignancies extending beyond the tumor capsule tend to behave more aggressively and are associated with a poor prognosis with the 5-year survival rate of 25%–65% 23. According to LiVolsi and Perzin 24 and Tortoledo et al 25, the extent of tumor infiltration beyond the capsule is the most reliable prognostic marker. Although containment within the tumor capsule has been found to be an indicator of benign clinical behavior, Felix et al 26 recently reported a case in which a completely encapsulated carcinoma ex pleomorphic adenoma presented with regional lymph node metastatic dissemination.
Pleomorphic adenoma prognosis
For most patients with benign, well-circumscribed pleomorphic adenomas, the prognosis is excellent after surgical resection. However, recurrence can be a problem with pleomorphic adenomas, particularly those occurring in the parotid gland 27. Recurrence has been related to many factors, including an incomplete capsule, extension of tumor nodules beyond the capsule, and intraoperative tumor rupture 28, in which tumor contents spill into the operative field.
Recurrence usually occurs in a multinodular fashion 29. In some cases, it involves microscopic elements, which render operative control extremely difficult and increase the risk of multiple further recurrences, as well as the risk of future malignant transformation. Recurrences have been related to tumors with high mesenchymal content, particularly chondroid and myxoid stroma. In some series, recurrences seem to be more common in younger patients than in older ones 30.
Malignant change occurs in 2-7% of cases and shows some association with multiple recurrences, deep lobe tumors, male gender, and older age.
A pleomorphic adenoma may undergo a malignant change that is not fully appreciated, because the malignant tumor is well differentiated and has a bland cellular morphology at a level indistinguishable from its benign counterpart, particularly with a small biopsy specimen or fine-needle aspiration (FNA). As a result, a malignant recurrence may be erroneously presumed to be benign.
An example of this mistaken presumption that is becoming increasingly recognized in the literature is a well-differentiated myoepithelial carcinoma ex pleomorphic adenoma with mild cytologic atypia that is presumed to be a cellular pleomorphic adenoma 31. In these cases, the malignant change can be recognized only after careful assessment of the resected specimen and the discovery of evidence of malignancy (which is sometimes subtle) 32.
- Jain S, Hasan S, Vyas N, Shah N, Dalal S. Pleomorphic Adenoma of the Parotid Gland: Report of a Case With Review of Literature. Ethiop J Health Sci. 2015;25(2):189–194. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478272[↩][↩][↩]
- Kato H, Kanematsu M, Mizuta K et-al. Carcinoma ex pleomorphic adenoma of the parotid gland: radiologic-pathologic correlation with MR imaging including diffusion-weighted imaging. AJNR Am J Neuroradiol. 2008;29 (5): 865-7. doi:10.3174/ajnr.A0974[↩][↩][↩][↩]
- Luna MA. Salivary glands. In: Pilch BZ, editor. Head and neck surgical pathology. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 284–349.[↩]
- Pleomorphic adenoma in the parapharyngeal space: report of three cases. Morita N, Miyata K, Sakamoto T, Wada T. J Oral Maxillofac Surg. 1995 May; 53(5):605-10.[↩]
- Minor salivary gland tumors: A clinicopathological study of 18 cases. Pons Vicente O, Almendros Marqués N, Berini Aytés L, Gay Escoda C. Med Oral Patol Oral Cir Bucal. 2008 Sep 1; 13(9):E582-8.[↩]
- Giant deep lobe parotid gland pleomorphic adenoma involving the parapharyngeal space. Report of three cases and review of the diagnostic and therapeutic approaches. Sergi B, Limongelli A, Scarano E, Fetoni AR, Paludetti G. Acta Otorhinolaryngol Ital. 2008 Oct; 28(5):261-5.[↩]
- Aggarwal A, Singh R, Sheikh S, Pallagatti S, Singla I. Pleomorphic adenoma of minor salivary gland: A case report. RSBO Revista Sul-Brasileira de Odontologia. 2012;9:97–101[↩]
- Olsen KD, Lewis JE. Carcinoma ex pleomorphic adenoma: a clinicopathologic review. Head Neck 2001;23:705–12[↩][↩]
- Seifert G. Histopathology of malignant salivary gland tumours. Eur J Cancer B Oral Oncol 1992;28:49–56[↩]
- Thoeny HC. Imaging of salivary gland tumours. Cancer Imaging. 2007;7 : 52-62. doi:10.1102/1470-7330.2007.0008[↩]
- Som PM, Brandwein MS. Salivary glands: anatomy and pathology. In: Som PM, Curtin HD, eds. Head and neck imaging. St Louis: Mosby;2003 :2067–76[↩][↩][↩]
- Gündüz AK, Yeşiltaş YS, Shields CL. Overview of benign and malignant lacrimal gland tumors. Curr Opin Ophthalmol. 2018 Sep;29(5):458-468.[↩]
- Simian virus 40 sequences and expression of the viral large T antigen oncoprotein in human pleomorphic adenomas of parotid glands. Martinelli M, Martini F, Rinaldi E, Caramanico L, Magri E, Grandi E, Carinci F, Pastore A, Tognon M. Am J Pathol. 2002 Oct; 161(4):1127-33.[↩]
- Spiro RH. Salivary neoplasms: overview of a 35-year experience with 2,807 patients. Head Neck Surg. 1986 Jan-Feb. 8(3):177-84.[↩]
- Takahama A Jr, da Cruz Perez DE, Magrin J, de Almeida OP, Kowalski LP. Giant pleomorphic adenoma of the parotid gland. Med Oral Patol Oral Cir Bucal. 2008 Jan 1. 13(1):E58-60.[↩]
- Kato H, Kawaguchi M, Ando T, Mizuta K, Aoki M, Matsuo M. Pleomorphic adenoma of salivary glands: common and uncommon CT and MR imaging features. Jpn J Radiol. 2018 Aug;36(8):463-471[↩]
- Traiger J, Rosen MB. Mixed tumor of the cheek; report of a case. Oral Surg Oral Med Oral Pathol. 1965;19:711–714.[↩]
- Carr RJ, Bowerman JE. A review of tumors of the deep lobe of the parotid salivary gland. Br J Oral Maxillofac Surg. 1986;24:155–168.[↩]
- CNS Metastases of Carcinoma ex Pleomorphic Adenoma of the Parotid Gland. S.P. Sheedy, K.M. Welker, D.R. DeLone, J.R. Gilbertson. American Journal of Neuroradiology Aug 2006, 27 (7) 1483-1485. http://www.ajnr.org/content/27/7/1483[↩]
- Buchman C, Stringer SP, Mendenhall WM, et al. Pleomorphic adenoma: effect of tumor spill and inadequate resection on tumor recurrence. Laryngoscope 1994;104:1231–34[↩][↩]
- Bokhari MR, Greene J. Pleomorphic Adenoma. [Updated 2019 Jan 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430829[↩][↩]
- Gleave EN, Whittaker JS, Nicholson A. Salivary tumours–experience over thirty years. Clin Otolaryngol Allied Sci. 1979 Aug;4(4):247-57[↩]
- Gnepp DR. Malignant mixed tumors of the salivary glands: a review. Pathol Annu 1993;28:279–328[↩]
- LiVolsi VA, Perzin KH. Malignant mixed tumors arising in salivary glands. I. Carcinomas arising in benign mixed tumors: a clinicopathologic study. Cancer 1977;39:2209–230[↩]
- Tortoledo, ME, Luna MA, Batsakis JG. Carcinoma ex pleomorphic adenoma and malignant mixed tumors: histomorphologic indexes. Arch Otolaryngol 1984;110:172–76[↩]
- Felix A, Rosa-Santos J, Mendonca ME, et al. Intracapsular carcinoma ex pleomorphic adenoma: report of a case with unusual metastatic behaviour. Oral Oncol 2002;38:107–110[↩]
- Laskawi R, Schott T, Schroder M. Recurrent pleomorphic adenomas of the parotid gland: clinical evaluation and long-term follow-up. Br J Oral Maxillofac Surg. 1998 Feb. 36(1):48-51.[↩]
- Riad MA, Abdel-Rahman H, Ezzat WF, Adly A, Dessouky O, Shehata M. Variables related to recurrence of pleomorphic adenomas: outcome of parotid surgery in 182 cases. Laryngoscope. 2011 Jul. 121(7):1467-72[↩]
- Wittekindt C, Streubel K, Arnold G, Stennert E, Guntinas-Lichius O. Recurrent pleomorphic adenoma of the parotid gland: analysis of 108 consecutive patients. Head Neck. 2007 Sep. 29(9):822-8[↩]
- McGregor AD, Burgoyne M, Tan KC. Recurrent pleomorphic salivary adenoma–the relevance of age at first presentation. Br J Plast Surg. 1988 Mar. 41(2):177-81.[↩]
- Antony J, Gopalan V, Smith RA, Lam AK. Carcinoma ex pleomorphic adenoma: a comprehensive review of clinical, pathological and molecular data. Head Neck Pathol. 2011 Jul 9[↩]
- Sedassari BT, Rodrigues MF, Mariano FV, Altemani A, Nunes FD, Sousa S. The Stem Cell Marker Bmi-1 Is Sensitive in Identifying Early Lesions of Carcinoma ex Pleomorphic Adenoma. Medicine (Baltimore). 2015 Jul. 94 (27):e1035[↩]





{kind=link}