Contents
What is pleural effusion
A pleural effusion is an abnormal buildup of fluid around your lungs, between the layers of tissue that line the lungs and chest cavity. A lot of extra fluid can push the pleura against your lung until the lung, or part of it, collapses. This can make it hard for you to breathe. More than 1.5 million persons develop pleural effusions each year in the United States 1.
Normally your body produces pleural fluid in small amounts (0.1 mL per kg) to lubricate the surfaces of the pleura 2. This is the thin tissue that lines the chest cavity and surrounds the lungs. At any one time there is about 20 mL of fluid in each hemithorax giving rise to a layer of fluid 2 to 10 mm thick. Pleural effusion is an abnormal, excessive collection of this fluid. Pleural effusion can be a sign of serious illness. A pleural effusion may be malignant (caused by cancer) or nonmalignant (caused by a condition that is not cancer). The pleural effusion fluid can be watery, can contain blood (known as haemothorax) or can contain pus (known as empyema).
If you have a pleural effusion, the fluid has built up between your lungs and the inside of your chest. It sits in and expands a space known as the pleural cavity. Pleural effusion is different to pulmonary edema, which occurs when fluid collects in the air sacs in the lungs.
There are two types of pleural effusion:
- Transudative pleural effusion, where the excess pleural fluid is low in protein is caused by fluid leaking into the pleural space. This is from increased pressure in the blood vessels or a low blood protein count. Heart failure is the most common cause.
- Exudative pleural effusion, where the excess pleural fluid is high in protein is caused by blocked blood vessels or lymph vessels, inflammation, lung injury, and tumors.
Pleural effusions can be unilateral or bilateral – a large unilateral pleural effusion is more ominous since it can signify a malignancy.
A pleural effusion can be caused by many different conditions, including:
- heart failure
- infections such as pneumonia
- kidney failure
- liver disease
- low blood protein levels
- blockage of a major blood vessel
- cancer
- chest injury
Risk factors for developing pleural effusion may include:
- Smoking and drinking alcohol
- Any previous complaint of high blood pressure
- History of any contact with asbestos
If you have a pleural effusion, you might have the following symptoms:
- difficulty breathing
- cough
- fever
- pain in your chest
To diagnose pleural effusion your doctor will examine your chest and may order tests such as:
- Blood tests
- X-rays
- Ultrasound scan
- Computed tomography (CT) scan
- Diagnostic thoracentesis
Thoracentesis is a procedure in which a needle is inserted into the pleural space between the lungs and the chest wall to remove excess fluid from the pleural space to help you breathe easier. Thoracentesis may be done to determine the cause of your pleural effusion.
In some cases, your doctor may recommend a thoracoscopy, a surgical procedure which involves examining the pleura and lungs with a special camera inserted into your chest via a thin tube.
Pleural effusion treatment depends on the cause and its severity.
- If the pleural effusion is small and not causing any problems, then it might be left alone while the cause, such as heart failure or infection, is treated. Treating the cause will often make the pleural effusion disappear.
- If the pleural effusion is making you short of breath, you might have it drained. That can often be done under local anaesthetic without the need for a stay in hospital.
- If the pleural effusion keeps coming back, there are ways to stop it recurring. Talk to your doctor.
- Malignant pleural effusions may be recurrent. They are treated by drainage, followed by the instillation of certain chemicals into the pleural space which help stick the two layers of pleura together, as to stop further fluid accumulating.
- Other effusions are treated by treating the underlying cause.
Pleural effusion possible complications
Complications of pleural effusion may include:
- Lung damage
- Sometimes the extra fluid gets infected and turns into an abscess. When this happens, it’s called an empyema.
- Air in the chest cavity (pneumothorax) after drainage of the effusion
- Pleural thickening (scarring of the lining of the lung)
The natural history of pleural effusions is largely determined by the cause. Pleural effusions as a result of a transient cause (e.g. pneumonia, infarction, exacerbation of heart failure) will reabsorb. However if the cause is progressive (e.g., mesothelioma or pulmonary metastases), then the pleural effusion, even if drained will re-accumulate.
Large pleural effusions will cause shortness of breath since they prevent the lung on that side from expanding adequately – they are often accompanied by a degree of lung collapse.
Lungs pleural cavity
The pleural cavity is the space between the pleura (thin layer of tissue) that covers the outer surface of each lung and lines the inner wall of the chest cavity. The pleura are thin films of connective tissue, which line both the outer surface of the lungs, and the inside of the chest cavity. The relationship of the pleura to the lungs and chest can be imagined as if the pleura were a balloon blown up inside the chest, into which the lungs have been pushed. Thus, there are in fact two layers of pleura between the outer surface of the lung and the chest wall. One is adherent to the lung, whereas the other layer follows the outline of the chest wall. The two layers press up against one another, and in the healthy chest, there is no air or significant fluid between them. Pleural tissue usually makes a small amount of fluid that helps the lungs move smoothly in the chest while a person is breathing. In a pleural effusion, extra fluid is present in this potential space between the two layers of pleura. The extra fluid presses on the lungs and makes it hard to breathe.
Figure 1. Lungs pleural cavity
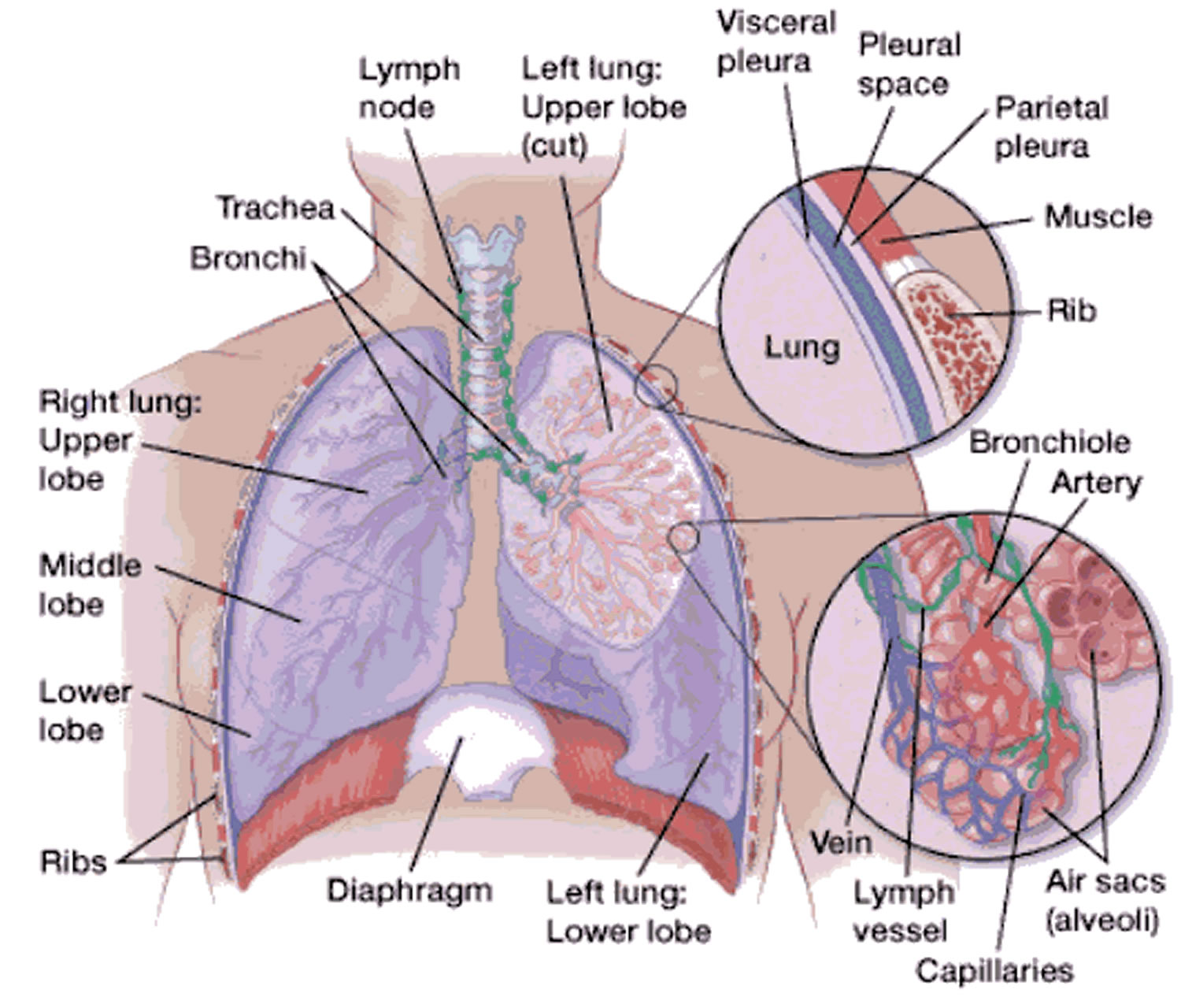 Figure 2. Bronchial tree of the lungs
Figure 2. Bronchial tree of the lungs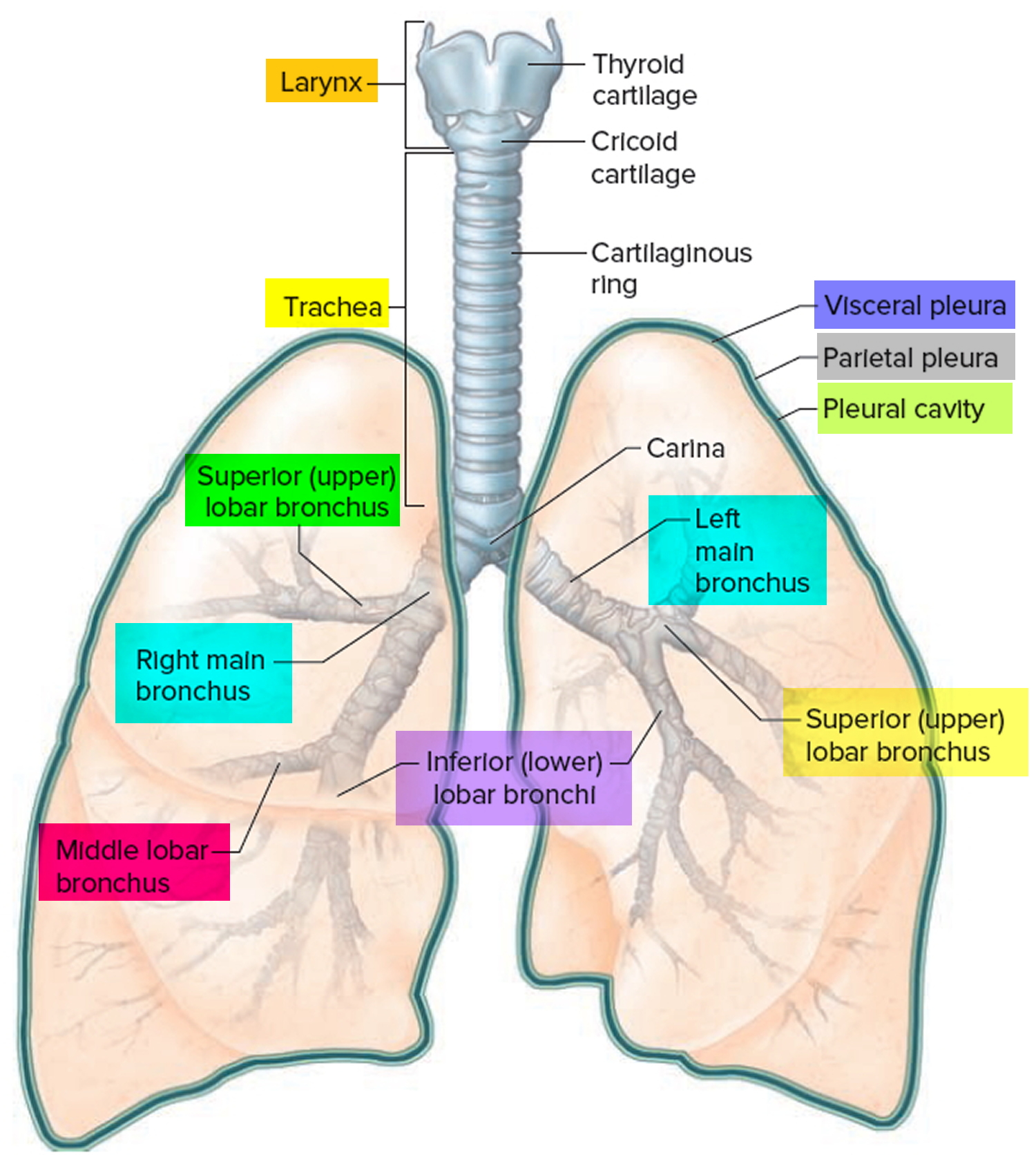
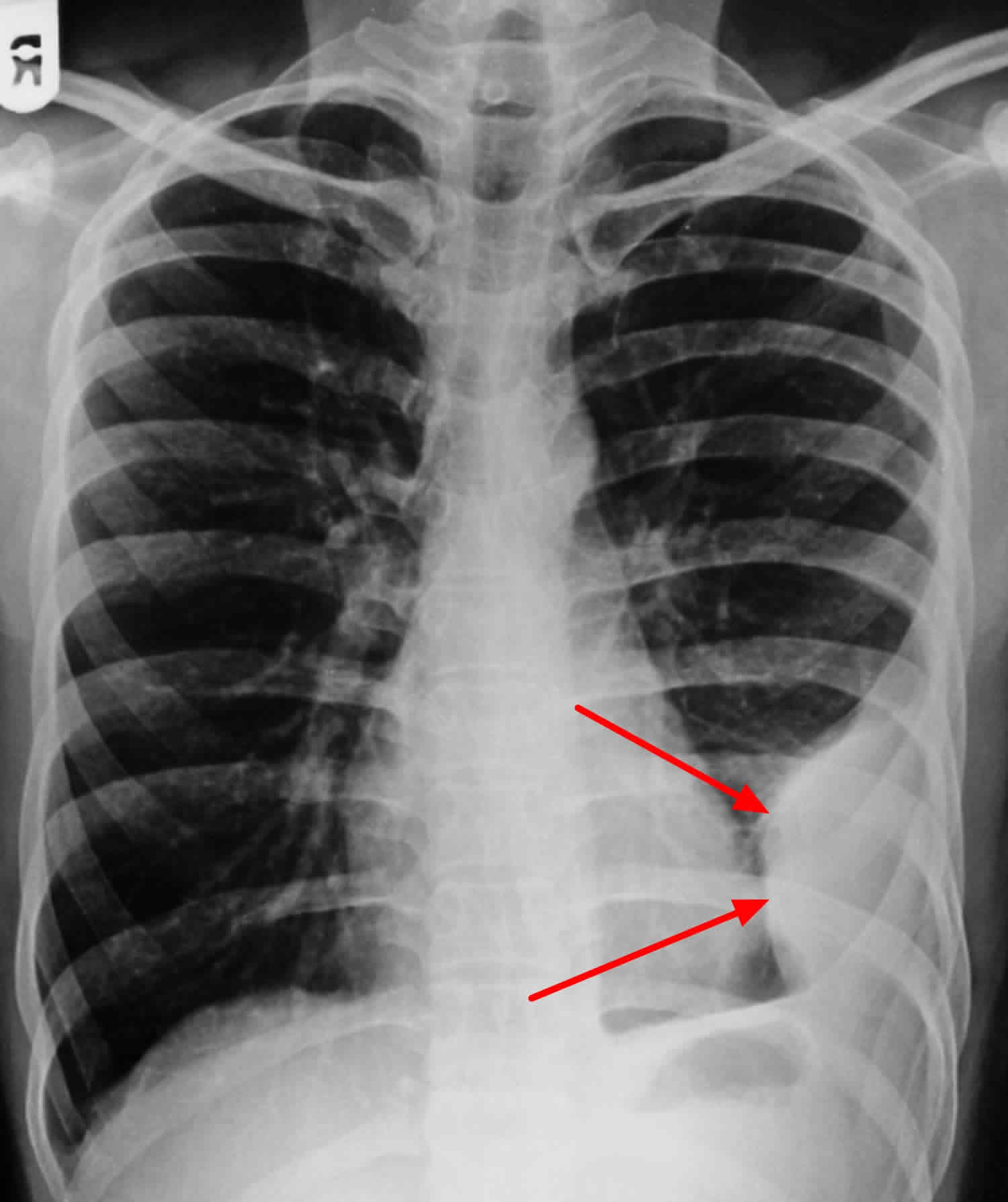
Figure 3. Pleural effusion chest X-ray
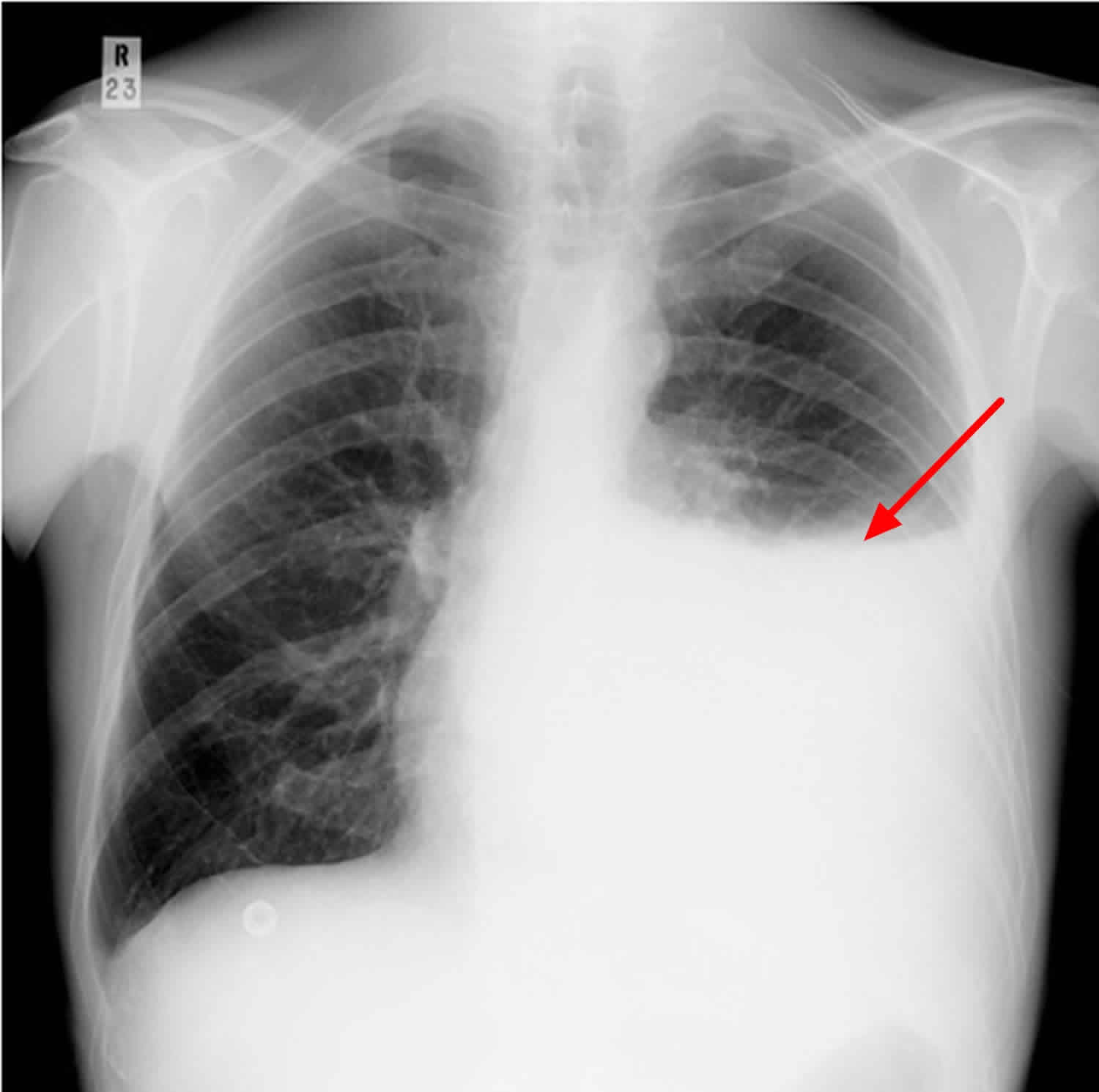
Footnote: The left lower zone is uniformly white. At the top of this white area there is a concave surface – meniscus sign. The left heart border, costophrenic angle and hemidiaphragm are obscured. Slight blunting of the right costophrenic angle indicates a small pleural effusion on that side
[Source 3]Figure 4. Loculated pleural effusion – loculation most commonly occurs with exudative fluid, blood and pus
Footnote: Patient presented with fever and chest pain since last 7 days. Loculation of fluid may occur within the fissures or between the pleural layers (visceral and parietal). Obliteration of left costophrenic angle with a wide pleural based dome shaped opacity projecting into the lung noted tracking along the cardiophrenic angle and lateral chest wall suggestive of loculated pleural effusion, however the possibility of empyema can not be ruled out completely.
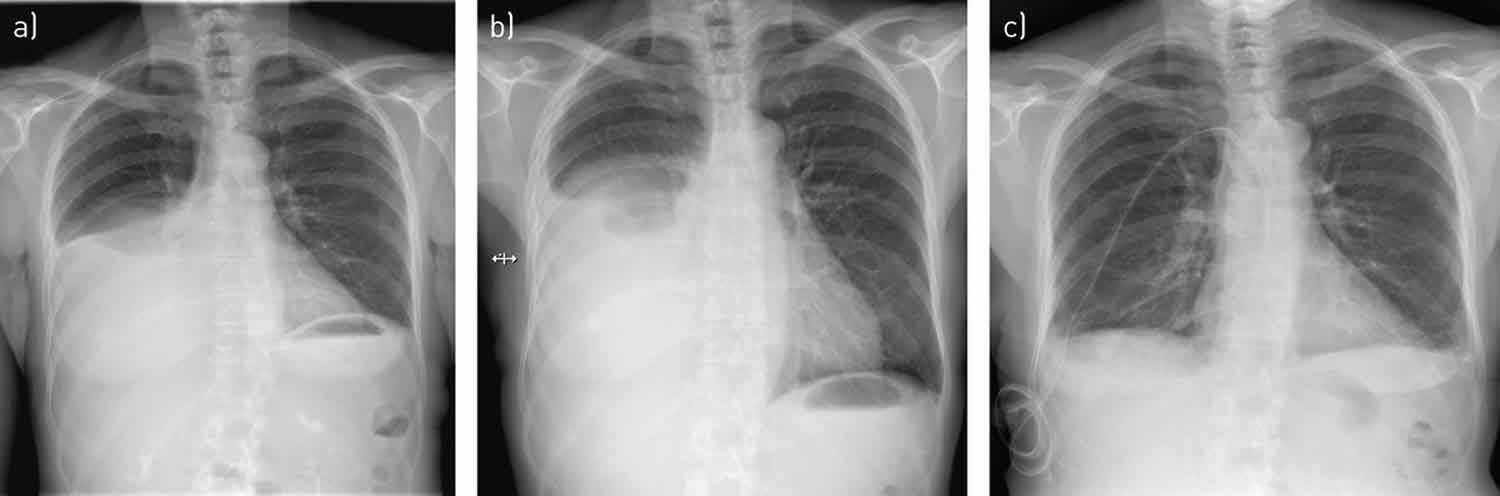
[Source 4]Figure 5. Bilateral pleural effusion with cardiomegaly (enlarged heart)

Footnote: 70 year old man presented with cough, with left chest pain and dyspnea (shortness of breath). Cardiomegaly with bilateral pleural effusions especially left side.
[Source 5]Pleural effusion symptoms
Pleural effusions may not produce any signs or symptoms in some patients. However, if the amount of fluid in the lung lining increases to 500 mL or so, symptoms such as shortness of breath, decreased chest movement, quieter breathing and a dry, non-productive cough, or pleuritic-type chest pain (a sharp pain, usually on breathing in, which worsens with coughing) may start to become noticeable.
See your doctor if you are worried about any of these symptoms. Other patients may complain of symptoms stemming from the cause of their pleural effusion, for example swollen legs or feet in congestive heart failure.
Symptoms of pleural effusion can include any of the following:
- Chest pain, usually a sharp pain that is worse with cough or deep breaths
- Cough
- Fever and chills
- Hiccups
- Rapid breathing
- Shortness of breath
If your doctor suspects you might have a pleural effusion, he or she will ask you a number of questions to try and discover a possible cause for the effusion. This would include details of any drugs you are taking, as some medications can produce pleural effusions. Your doctor would also examine your chest and listen to your lungs with a stethoscope.
Pleural effusion causes
Anything that causes an imbalance between production and reabsorption of pleural fluid can lead to development of a pleural effusion.
The following diseases may cause pleural effusion:
- Heart failure
- Bacterial pneumonia
- Lung cancer and other tumors with lung metastases
- Pulmonary embolism
- Radiation therapy to the chest
- Nephrotic syndrome
- Hypothyroidism
- Ovarian tumors
- Tuberculosis
- Connective tissue disease (for example, rheumatoid arthritis, lupus)
- Rarely: heart attack (myocardial infarction), acute pancreatitis, mesothelioma, sarcoidosis, yellow-nail syndrome, familial Mediterranean fever.
- Medications associated with pleural effusion 6:
- Amiodarone
- Beta blockers
- Ergot alkaloids
- l-tryptophan
- Methotrexate
- Nitrofurantoin (Furadantin)
- Phenytoin (Dilantin)
Transudative pleural effusions (those low in protein) usually form as a result of excess capillary fluid leakage into the pleural space. Common causes of transudative effusions include:
- Congestive heart failure;
- Nephrotic syndrome;
- Cirrhosis of the liver;
- Pulmonary embolism; and
- Hypothyroidism.
Exudative effusions, which are high in protein, are often more serious than transudative effusions. They are formed as a result of inflammation of the pleura, which might happen for example in lung disease. Common causes of exudative effusions include:
- Pneumonia;
- Lung cancer, or other cancers;
- Connective tissue diseases, including rheumatoid arthritis and systemic lupus erythematosus;
- Pulmonary embolism;
- Asbestosis;
- Tuberculosis;
- Radiotherapy.
Table 1. Pleural Effusion: Causes, Types, and Clinical Clues
| Condition | Exudative or transudative | Clinical clues | |
|---|---|---|---|
Most common (by decreasing frequency) | |||
Heart failure | Transudative | Hypoxia, pulmonary/peripheral edema | |
Bacterial pneumonia | Exudative | Chills, cough, fever, infiltrate | |
Pulmonary embolism | Exudative | Dyspnea, immobilization, pleuritic chest pain, recent travel | |
Malignancy | Exudative | History of cancer, lung mass | |
Viral disease | Exudative | Cough, fatigue, fever, muscle aches, rash | |
Post-cardiac surgery | Exudative | Recent surgery | |
Less common (alphabetical order by organ system) | |||
Cardiovascular | |||
Pericarditis | Exudative | Electrocardiographic findings, pericardial effusion on ultrasonography, sharp chest pain | |
Pulmonary vein stenosis | Exudative | Recent heart catheterization | |
Superior vena cava obstruction | Transudative | Facial swelling and ruddy complexion, upper extremity swelling | |
Gastrointestinal | |||
Abdominal abscess | Exudative | Abdominal pain, chills, fever, nausea, vomiting | |
Cirrhosis | Transudative | History of alcohol abuse or viral hepatitis; ascites, caput medusae, palmar erythema | |
Esophageal perforation | Exudative | History of esophageal tumor or reflux; chest or abdominal pain, fever | |
Pancreatitis | Exudative | Abdominal pain, anorexia, elevated amylase and lipase levels, nausea, vomiting | |
Post-abdominal surgery | Exudative | Recent surgery | |
Genitourinary | |||
Endometriosis | Exudative | Dysmenorrhea, infertility, pelvic pain | |
Meigs syndrome | Exudative | History of ovarian tumor | |
Ovarian hyperstimulation syndrome | Exudative | History of infertility treatment, abdominal pain | |
Postpartum effusion | Exudative | Recent childbirth | |
Urinothorax | Transudative | Recent urologic procedure, urinary obstruction | |
Pulmonary | |||
Mesothelioma | Exudative | History of asbestos exposure, pleural mass | |
Other | |||
Chylothorax | Exudative | Chest mass, lipids in pleural fluid, trauma | |
Pseudochylothorax | Exudative | History of tuberculosis or pleural disease, lipids in pleural fluid, rheumatoid disease | |
Medications | Exudative | Medication use | |
Nephrotic syndrome | Transudative | Edema, proteinuria | |
Rheumatoid arthritis | Exudative | Joint pain and swelling | |
Yellow nail syndrome | Exudative | Lymphedema, yellow nails | |
[Source 2]
Table 2. Signs and Symptoms that Suggest a Cause of Pleural Effusion
| Signs and symptoms | Suggested etiology |
|---|---|
Ascites | Cirrhosis |
Distended neck veins | Heart failure, pericarditis |
Dyspnea on exertion | Heart failure |
Fever | Abdominal abscess, empyema, malignancy, pneumonia, tuberculosis |
Hemoptysis | Malignancy, pulmonary embolism, tuberculosis |
Hepatosplenomegaly | Malignancy |
Lymphadenopathy | Malignancy |
Orthopnea | Heart failure, pericarditis |
Peripheral edema | Heart failure |
S3 gallop | Heart failure |
Unilateral lower extremity swelling | Pulmonary embolism |
Weight loss | Malignancy, tuberculosis |
Pleural effusion cancer
Malignant pleural effusion is a common problem for patients who have certain cancers. Lung cancer, breast cancer, lymphoma, and leukemia cause most malignant pleural effusions 7. Pleural effusion also may be caused by cancer treatment, such as radiation therapy or chemotherapy. Some cancer patients have conditions such as congestive heart failure, pneumonia, blood clot in the lung, or poor nutrition that may lead to a pleural effusion.
A diagnosis of the cause of pleural effusion is important in planning treatment.
These and other signs and symptoms may be caused by a pleural effusion. Talk to your doctor if you have any of the following problems:
- Dyspnea (shortness of breath).
- Cough.
- An uncomfortable feeling or pain in the chest.
Treatment for a malignant pleural effusion is different from treatment for a nonmalignant effusion, so the right diagnosis is important.
Diagnostic tests include the following:
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan: A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells. This procedure may be used to reduce pressure on the lungs.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If thoracentesis is not possible, a biopsy may be done during a thoracoscopy. A thoracoscopy is a procedure to look at the organs inside the chest to check for abnormal areas. An incision (cut) is made between two ribs and a thoracoscope (a thin, lighted tube with a lens for viewing) is inserted into the chest. A cutting tool at the end of the thoracoscope is used to remove a sample of tissue.
The type of cancer, previous treatment for cancer, and the patient’s wishes also are important in planning treatment.
Malignant pleural effusion treatment
Treatment may be to control signs and symptoms of pleural effusion and improve quality of life.
A malignant pleural effusion often occurs in cancer that is advanced, cannot be removed by surgery, or continues to grow or spread during treatment. It is also common during the last few weeks of life. The goal of treatment is usually palliative, to relieve signs and symptoms and improve quality of life.
Treatment of the signs and symptoms of malignant pleural effusion includes the following:
Thoracentesis
Thoracentesis is a procedure to remove extra fluid from the pleural cavity using a needle and/or a thin, plastic tube. Removal of the fluid may help to relieve severe symptoms for a short time. A few days after the extra fluid is removed, it is likely it will begin to come back. The risk of a thoracentesis includes bleeding, infection, collapsed lung, fluid in the lungs, and low blood pressure.
Indwelling pleural catheter
An indwelling pleural catheter is a small tube that is inserted and left in place to keep fluid from building up around the lungs. One end of the tube stays inside the chest and the other passes outside the body to allow fluid to drain. This type of catheter may be used for long-term care so that a separate procedure won’t need to be done each time draining is needed. Risks of indwelling pleural catheters include infection and blockage of the catheter.
The PleurX catheter was approved by US Food and Drug Administration in 1997 for the management of malignant pleural effusions 8. Indwelling pleural catheter use in malignant pleural effusions. Increasing evidence is now available supporting the safe use of indwelling pleural catheters in malignant pleural disease, which allows outpatient-based treatment. Use of indwelling pleural catheters in malignant disease is considered to be cost-effective compared with talc pleurodesis (which necessitates an inpatient stay), though this is dependent on expected prognosis 9.
Pleurodesis
This is a procedure to close the pleural space so that fluid cannot collect there. Fluid is first removed by thoracentesis, using a chest tube. A drug that causes the pleural space to close is then inserted into the space through a chest tube. Drugs such as bleomycin or talc may be used. Pleurodesis is a long established, safe and effective technique validated in patients with malignant effusion.
Surgery
Surgery may be done to put in a shunt (tube) to carry the fluid from the pleural cavity to the abdominal cavity, where the fluid is easier to remove. Pleurectomy is another type of surgery that may be used. In this procedure, the part of the pleura that lines the chest cavity is removed.
Pleural effusion diagnosis
Your health care provider will examine you and ask about your symptoms. The provider will also listen to your lungs with a stethoscope and tap (percuss) your chest and upper back.
If a pleural effusion is suspected, a chest X-Ray or chest CT can help to confirm the diagnosis and may be enough for your provider to decide on treatment. The excess accumulation of fluid can usually be seen on these images.
- Abnormal findings can be detected on posteroanterior radiography in the presence of 200 mL of fluid, and on lateral radiography with as little as 50 mL of fluid 10.
- Lateral decubitus radiography may be obtained to help determine the size of the effusion and whether it is free-flowing or loculated.
- Computed tomography (CT scan) can detect effusions not apparent on plain radiography, distinguish between pleural fluid and pleural thickening, and provide clues to the underlying etiology 11.
Thoracentesis
If there is a significant effusion present on X-ray or CT, it may be necessary to take a sample of the fluid for analysis using a procedure called diagnostic thoracentesis. This involves insertion of a small needle through the skin over the pleural and into the pleural space.
Your provider may want to perform tests on the fluid. Tests on the fluid will be done to look for:
- Infection
- Cancer cells
- Protein levels
The fluid can then be analyzed to determine whether it is transudative or exudative, depending on the amount of protein present.
- If the pleural effusion is transudative, no further tests are usually necessary. This is because the cause is likely to be something systemic (affecting the whole body, for example with heart failure) and treatment can be directed towards this.
- If the pleural effusion is thought to be exudative, further tests on the fluid will usually be ordered to try to identify a cause. These may include testing for presence of bacteria and examining the cell types present under a microscope to look for evidence of cancer.
- In approximately 15-20% of cases no cause will be found for the pleural effusion, despite extensive investigation. Most of these cases will resolve with time.
Blood tests that may be done include:
- Complete blood count (CBC), to check for signs of infection or anemia
- Kidney and liver function blood tests
If needed, these other tests may be done:
- Ultrasound of the heart (echocardiogram) to look for heart failure
- Lung biopsy to look for cancer
- Passing a tube through the windpipe to check the airways for problems or cancer (bronchoscopy)
Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. If thoracentesis is not possible, a biopsy may be done during a thoracoscopy. A thoracoscopy is a procedure to look at the organs inside the chest to check for abnormal areas. An incision (cut) is made between two ribs and a thoracoscope (a thin, lighted tube with a lens for viewing) is inserted into the chest. A cutting tool at the end of the thoracoscope is used to remove a sample of tissue.
Pleural effusion – classification
Pleural effusions are traditionally classified as either exudates or transudates but they can also contain blood (hemothorax) or chyle (chylothorax). A chylothorax usually occurs because of disruption of the thoracic duct. A pseudo chylothorax occurs secondary to a long-standing pleural effusion and is characteristered by the accumulation of cholesterol crystals.
An exudative effusion occurs when local factors are altered, such as inflammation of the lung or the pleura leading to capillary leakage of fluid into the pleural space.
A transudative effusion, by contrast, occurs when systemic factors come into play. This includes an elevated portal pressure from cirrhosis, elevated visceral pulmonary capillary pressure from left-sided heart failure, elevated parietal pleural capillary pressure from right-sided heart failure, or low oncotic pressure due to hypoalbuminaemia.
Exudates subsequently have a high protein content (>30g/L) and transudates a low protein content (<30g/L). If the pleural fluid protein is 25-35g/L then Light’s criteria should be applied to differentiate transudates and exudates accurately.
Light’s criteria state that the pleural fluid is an exudate if one or more of the following criteria are met (sensitivity 98%, specificity 83% for exudate):
- Pleural fluid protein : serum protein > 0.5
- Pleural fluid lactate dehydrogenase (LDH) : serum LDH > 0.6
- Pleural fluid lactate dehydrogenase (LDH) > 2/3 upper limit of normal serum LDH
Additional criteria used to confirm exudate if results equivocal:
- Serum albumin – pleural fluid albumin <1.2g/dL
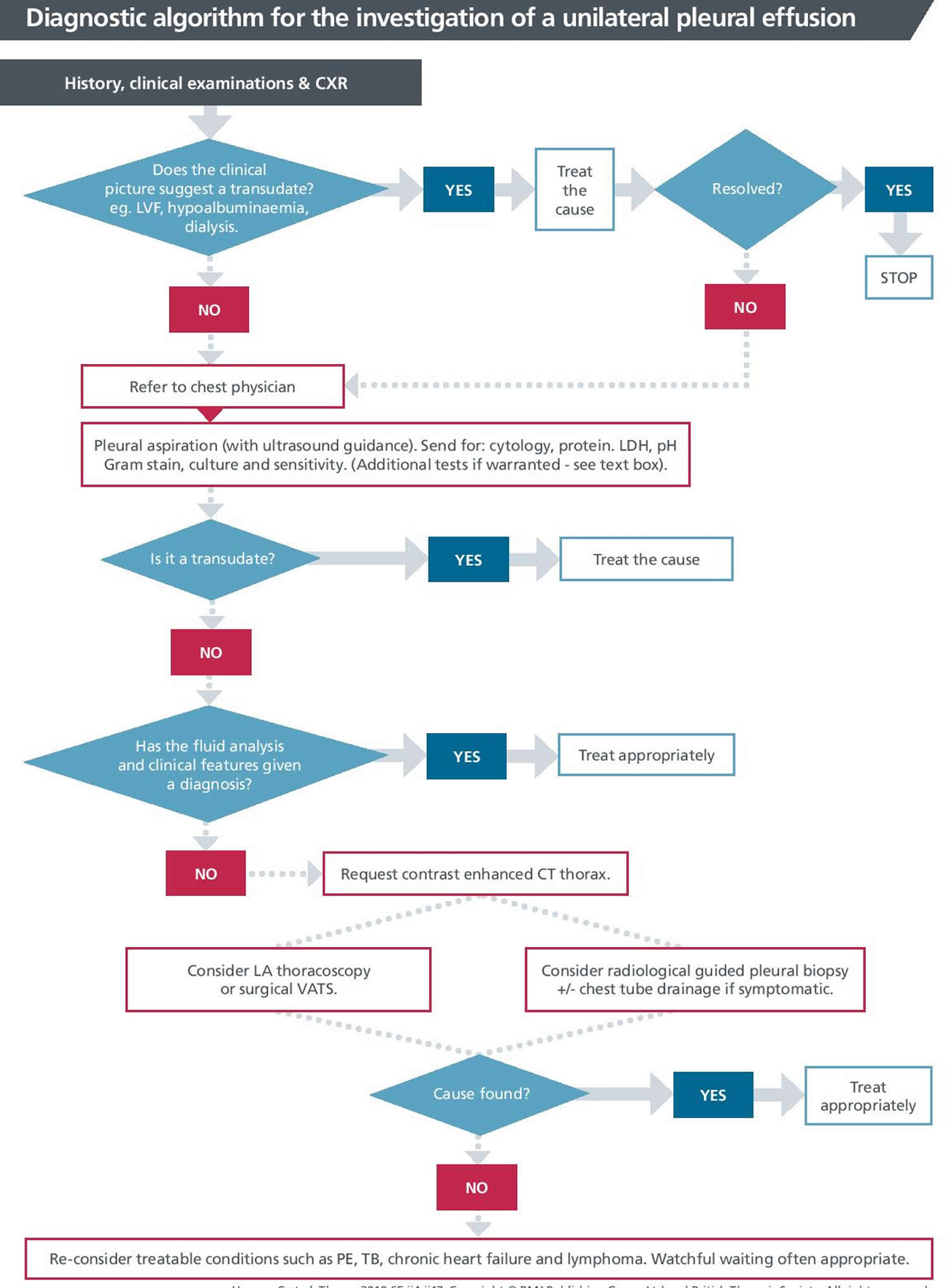
Figure 6. Unilateral pleural effusion diagnostic algorithm
Pleural effusion treatment
The goal of pleural effusion treatment is to:
- Remove the fluid
- Prevent fluid from building up again
- Determine and treat the cause of the fluid buildup
Removing the fluid (thoracentesis) may be done if there is a lot of fluid and it is causing chest pressure, shortness of breath, or a low oxygen level. Removing the fluid allows the lung to expand, making breathing easier. Thoracentesis is performed in a doctor’s office or hospital. The procedure usually takes 10 to 15 minutes, unless you have a lot of fluid in your pleural space. For the procedure, most patients sit quietly on the edge of a chair or bed with their head and arms resting on a table. Your doctor may use ultrasound to determine the best location to insert the needle. After cleaning the skin around the area where the needle will be inserted, your doctor will inject numbing medicine. A needle is inserted between your ribs into the pleural space. You may feel some discomfort or pressure when the needle is inserted. As your doctor draws out excess fluid from around your lungs, you may feel like coughing or have chest pain. The needle will be removed, and a small bandage will be applied to the site.
No more than 1.5L (some advocate 1L) should be removed at a single procedure as fluid shifts can result in re-expansion pulmonary edema.
After the procedure, your blood pressure and breathing will be monitored to make sure you do not have complications. The fluid that was removed from your chest will be sent for laboratory testing to determine the cause of your pleural effusion and to help plan your treatment. Your doctor may order a chest x ray to check for lung problems.
The risks of thoracentesis include a pneumothorax or collapsed lung, pain, bleeding, bruising, or infection. Liver or spleen injuries are rare complications.
- Re-expansion pulmonary edema: with drainage of very large volumes of fluid, there is a small chance that the lungs might react badly to the rapid re-expansion, and the air spaces may fill with fluid. This is a very rare complication, but may be fatal. Patients who have a bleeding disorder, or who are taking anticoagulant medications such as warfarin, may be at increased risk of bleeding during the procedure. Always tell your health provider if this applies to you. There is also a risk that the thoracentesis will be unsuccessful, or that the drained fluid may reaccumulate. This is particularly common in pleural effusions associated with malignancy.
If a very large amount of fluid must be drained, or if drainage needs to be continuous, then a tube can be placed through the chest wall into the pleural space (tube thoracostomy) to allow longer-term symptom relief. Rarely, some patients may require further treatment for pleural effusions which do not resolve, or which recur despite repeated thoracentesis. They may undergo a procedure called pleurodesis (pleural sclerosis), where a chemical is injected into the pleural space to induce scarring. This scarring sticks the two layers of pleura together so that no fluid can accumulate between them.
The cause of the fluid buildup must also be treated:
- If it is due to heart failure, you may receive diuretics (water pills) and other medicines to treat heart failure.
- If it is due to an infection, antibiotics will be given.
In people with cancer or infection, the effusion is often treated by using a chest tube to drain the fluid.
In some cases of malignant pleural effusion, any of the following treatments are done:
- Chemotherapy
- Placing medicine into the chest that prevents fluid from building up again after it is drained
- Radiation therapy
- Surgery
- Light RW. Pleural effusions. Med Clin North Am. 2011;95(6):1055–1070.[↩]
- Diagnostic Approach to Pleural Effusion. Am Fam Physician. 2014 Jul 15;90(2):99-104. https://www.aafp.org/afp/2014/0715/p99.html[↩][↩][↩]
- Chest X-ray Abnormalities. https://www.radiologymasterclass.co.uk/tutorials/chest/chest_pathology/chest_pathology_page4[↩]
- Loculated pleural effusion. https://radiopaedia.org/cases/loculated-pleural-effusion-1[↩]
- Cardiomegaly with bilateral pleural effusion. https://radiopaedia.org/cases/cardiomegaly-with-bilateral-pleural-effusion[↩]
- Pleural effusion. https://www.pneumotox.com/pattern/view/31/V.a/pleural-effusion/[↩]
- Malignant Pleural Effusion. https://www.cancer.gov/about-cancer/treatment/side-effects/cardiopulmonary-pdq#section/_210[↩]
- US Food and Drug Administration. 510(K) Premarket Notification. K971753. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?id=k971753[↩]
- Puri V, Pyrdeck TL, Crabtree TD, et al. Treatment of malignant pleural effusion: a cost-effectiveness analysis. Ann Thorac Surg 2012; 94: 374–379.[↩]
- Hooper C, et al. Investigation of a unilateral pleural effusion in adults: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65(suppl 2):ii4–ii17.[↩]
- Light RW. Pleural Diseases. 4th ed. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2001.[↩]
- The management of benign non-infective pleural effusions. European Respiratory Review 2016 25: 303-316; DOI: 10.1183/16000617.0026-2016[↩]





{kind=link}