Contents
- What is postmenopausal
- Postmenopausal health problems
- Postmenopausal vaginal bleeding
- Postmenopausal osteoporosis
- Postmenopausal hot flashes
- Risk factors of hot flashes
- Hot flashes treatment
- Non-Hormone Options for Treating Hot Flashes
- Medications For Treating Hot Flashes and Night Sweats with Hormones
- Hormone therapy
- Types of hormone replacement therapy
- Hormone replacement therapy hormones
- Ways of taking hormone replacement therapy
- Hormone replacement therapy treatment regimens
- Side effects of hormone replacement therapy
- More serious risks of HRT
- Bioidentical or “natural” hormones
- Unproven, Nonscientific “Treatments” for Hot Flashes
- Nerve block procedure
- Other postmenopausal symptoms and treatment
What is postmenopausal
Post menopause means the period of life after the menopause. Menopause is the time when your menstrual periods stop permanently and you can no longer get pregnant. You have reached menopause only after it has been a full year since your last period. This means you have not had any vaginal bleeding, including spotting, for 12 months in a row. Menopause is a normal part of a woman’s life. It is sometimes called “the change of life.” Menopause does not happen all at once. As your body transitions to menopause over several years, you may have menopause symptoms and irregular periods. The average age for menopause in the United States is 52.
Some people call the time leading up to a woman’s last period menopause. This time actually is the transition to menopause, better known as perimenopause. Perimenopause means “around menopause.” After menopause, your body makes much less of the hormones estrogen and progesterone. Very low estrogen levels after menopause can affect your health and cause symptoms such as hot flashes. You can take steps to protect your health and relieve your symptoms.
Menopause happens when you have gone 12 months in a row without a period. The average age of menopause in the United States is 52. The range for women is usually between 45 and 58 1. One way to tell when you might go through menopause is the age your mother went through it 2.
Menopause may happen earlier if you:
- Never had children. Pregnancy, especially more than one pregnancy, may delay menopause 3
- Smoke. Studies show smoking can cause you to start menopause up to two years earlier than women who don’t smoke 4
Certain health problems can also cause you to start menopause earlier.
Menopause usually happens on its own. However, you may enter menopause earlier than you normally would if you have had chemotherapy or surgery to remove both ovaries.
Symptoms of menopause may begin suddenly and be very noticeable, or they may be very mild at first. Symptoms may happen most of the time once they begin, or they may happen only once in a while. Some women notice changes in many areas. Some menopausal symptoms, such as moodiness, are similar to symptoms of premenstrual syndrome (PMS). Others may be new to you. For example:
- Your menstrual periods may not come as regularly as before. They also might last longer or be shorter. You might skip some months. Periods might stop for a few months and then start up again.
- Your periods might be heavier or lighter than before.
- You might have hot flashes and problems sleeping.
- You might experience mood swings or be irritable.
- You might experience vaginal dryness. Sex may be uncomfortable or painful.
- You may have less interest in sex. It may take longer for you to get aroused.
Other possible changes are not as noticeable. For example, you might begin to lose bone density because you have less estrogen. This can lead to osteoporosis, a condition that causes bones to become weak and break easily. Changing estrogen levels can also raise cholesterol levels and increase your risk for heart disease and stroke.
Talk to your doctor about possible treatment for your menopause symptoms if they bother you.
What happens after menopause?
After menopause you will no longer be able to get pregnant and you will no longer get a period. If you have any type of vaginal bleeding after menopause, you should see a doctor as soon as possible. Vaginal bleeding after menopause is not normal and can mean that you have a serious health problem.
You may experience any of the following after menopause:
- Low hormone levels. With menopause, your ovaries make very little of the hormones estrogen and progesterone. Because of changing hormone levels, you may develop certain health risks, including osteoporosis, heart disease, and stroke.
- Menopause symptoms instead of period problems. After menopause, most women get relief from period problems or menopause symptoms. However, you may still experience symptoms such as hot flashes because of changing estrogen levels. One recent study found that hot flashes can continue for up to 14 years after menopause 5
- Vaginal dryness. Vaginal dryness may be more common post-menopause. Learn more about treatments for vaginal dryness.
Postmenopausal health problems
After menopause, your ovaries make very little estrogen. Women who have gone through menopause have very low estrogen levels. Low levels of estrogen and progesterone raise your risk for certain health problems after menopause. Other health problems may happen naturally as you age.
Examples of common health problems in the years after menopause include:
- Heart disease. Before age 55, women have a lower risk of heart disease than men. Estrogen helps keep blood vessels relaxed and open and helps the body maintain a healthy balance of good and bad cholesterol. Without estrogen, cholesterol may start building up on artery walls leading to the heart. By age 70, women have about the same risk for heart disease as men of the same age.
- Stroke. Your risk for stroke doubles every decade after age 55 6. The lower levels of estrogen in your body may play a role in cholesterol build-up on artery walls leading to the brain.
- Osteoporosis. Having less estrogen after menopause causes you to lose bone mass much more quickly than you did before, which puts you at risk for osteoporosis. Osteoporosis is a condition that causes your bones to become brittle and weak and break easily. A recent large study found that women who have severe hot flashes and night sweats during the years around menopause usually have more bone loss and are at higher risk for hip fractures than women who do not have severe symptoms 7
- Lead poisoning. Lead that you are exposed to over your lifetime gets stored in your bones. Because bone begins to break down much more quickly after menopause, that lead is more likely to be released into the blood. Older women can have blood lead levels 30% higher than before they reached menopause. This lead increases your risk for high blood pressure and atherosclerosis (sometimes called hardening of the arteries). This lead in your blood can also cause your kidneys to not work as well. It can also cause symptoms similar to dementia, affecting your memory and ability to think 8
- Urinary incontinence. About half of postmenopausal women have trouble holding in their urine 1. Lower estrogen levels may weaken the urethra. Learn about treatment options for incontinence.
- Oral issues. Dry mouth and an increased risk for cavities are more common after menopause. Learn more about oral health.
Please speak to your doctor if you are concerned.
Does hormone therapy during menopause prevent these health problems?
No. Menopausal hormone therapy is medicine to help relieve your menopause symptoms, such as hot flashes and vaginal dryness. Menopausal hormone therapy may actually raise your risk for blood clots, stroke, and some cancers and does not help prevent heart disease or dementia.
What screenings do I need after menopause?
All women need regular checkups and screening tests throughout their lives. Most women can help take care of their health with:
- Regular mammograms after age 50 through age 75
- Regular Pap tests, even after menopause. You should get a Pap test and HPV test together every five years if you have a cervix, until you are 65 and have had three clear tests in a row.
- Regular height measurements to detect loss of height due to bone loss
- Blood, urine, and other tests to screen for risk of diabetes and heart disease
- Blood pressure, cholesterol, and other tests your doctor recommends
Ask your doctor or nurse about flu shots and other vaccines. Besides the flu shot, vaccinations are available for pneumonia, shingles, and other diseases.
Your doctor or nurse might also recommend other tests, depending on your health. For example, you might need to see a specialist for some specific problems, like urinary incontinence.
How can I stay healthy during and after menopause?
There are many important steps you can take to build your health in the years around menopause.
- Quit smoking. Quitting smoking is the most important step you can take to be healthier. Smoking hurts your health in many ways, including by damaging your bones and causing heart disease and as many as 12 types of cancer in women.5,6 Stay away from secondhand smoke and get help quitting if you need it.
- Be active. Getting at least 30 minutes of physical activity on most days of the week is one of the best ways you can be healthier. Physical activity can help your bones, heart, and mood. Exercise doesn’t have to be complicated. Brisk walking and regular household chores are good for your health. Ask your doctor about what activities are right for you. Aim to do:
- At least 2 hours and 30 minutes a week of moderate aerobic physical activity or 1 hour and 15 minutes of vigorous aerobic activity or some combination of the two
- Exercises that build muscle strength on two days each week
- Eat well. Getting vitamins, minerals, fiber, and other essential nutrients is just as important as when you were younger. But older women usually need fewer calories for energy.
- Talk to your doctor or nurse about dietary supplements.
- Women older than 50 need 2.4 micrograms of vitamin B12 and 1.5 milligrams of vitamin B6 each day. Ask your doctor or nurse if you need a vitamin supplement.
- After menopause, calcium needs go up to maintain bone health. Doctors recommend that women 51 and older get 1,200 milligrams of calcium each day. Vitamin D also is important to bone health. Doctors also recommend that women 51 to 70 get 600 international units (IU) of vitamin D each day and women ages 71 and older get 800 IU of vitamin D each day. Ask your doctor or nurse if you need a calcium supplement or if you need more vitamin D.
- Practice safe sex. After menopause, you can’t get pregnant. But you can still get a sexually transmitted infection (STI, or STD). Condoms are the best way to prevent STIs when you have sex. After menopause the vagina may be drier and thinner, leading to small cuts or tears during sex. Vaginal cuts or tears put you at higher risk for STIs.
Will I gain weight after menopause?
Maybe. Many women gain an average of 5 pounds after menopause. Lower estrogen levels may play a role in weight gain after menopause. But weight gain may be caused by your metabolism slowing down as you age. You may also not eat as healthy or be as active as when you were younger. You also lose muscle mass as you age (muscle burns more calories at rest than other types of tissue in the body).
Weight gain can raise your risk for high blood pressure, cholesterol, diabetes, heart attack, and stroke. The risk is greater if you are already overweight or are not active or eating healthy.
The best way to lose weight, if you are overweight or obese, is to eat fewer calories each day. Exercise or physical activity is also important for good health, but works better to keep weight off than it does to help you lose weight. Researchers think this might be because people who are physically active are usually hungrier. Eating healthy and getting at least 30 minutes of exercise on most days is the best way to keep a healthy weight.
Postmenopausal vaginal bleeding
Menopause is usually diagnosed in women over 45 who haven’t had a period for more than a year. Any bleeding from the vagina after this needs to be checked by a doctor.
See a doctor if you have postmenopausal bleeding, even if:
- it’s only happened once
- there’s only a small amount of blood, spotting, or pink or brown discharge
- you don’t have any other symptoms
- you’re not sure if it’s blood
Postmenopausal bleeding isn’t usually serious, but can be a sign of cancer. Cancer is easier to treat if it’s found early.
A doctor, will offer you tests to help find out what’s causing postmenopausal bleeding and plan any necessary treatment.
The tests may include:
- a small device being placed in your vagina to scan for any problems (vaginal ultrasound scan)
- an examination of your pelvis and vagina
- a thin, telescope-like camera being passed up your vagina and into your womb to look for any problems (a hysteroscopy) and to take a tissue sample (biopsy) for testing – under local or general anaesthetic
Causes of postmenopausal bleeding
There can be several causes of postmenopausal bleeding.
The most common causes postmenopausal bleeding or spotting are:
- inflammation and thinning of the vaginal lining (atrophic vaginitis) or womb lining (endometrial atrophy) – caused by lower estrogen levels
- cervical or womb polyps – growths that are usually non-cancerous
- a thickened womb lining (endometrial hyperplasia) – this can be caused by hormone replacement therapy (HRT), high levels of estrogen or being overweight, and can lead to womb cancer (cancer of the uterus)
Less commonly, postmenopausal bleeding is caused by cancer.
Treatment for postmenopausal bleeding
Treatment depends on what’s causing your bleeding.
Postmenopausal osteoporosis
Osteoporosis is a disease of the bones that causes bones to become weak and break easily. Osteoporosis affects mostly older women, but prevention starts when you are younger. No matter your age, you can take steps to build bone mass and prevent bone loss. Broken bones from osteoporosis cause serious health problems and disability in older women.
The most common injuries in people with osteoporosis are:
- wrist fractures
- hip fractures
- fractures of the spinal bones (vertebrae)
However, they can also occur in other bones, such as in the arm or pelvis. Sometimes a cough or sneeze can cause a rib fracture or the partial collapse of one of the bones of the spine.
Osteoporosis isn’t usually painful until a fracture occurs, but spinal fractures are a common cause of long-term (chronic) pain.
Although a fracture is the first sign of osteoporosis, some older people develop the characteristic stooped (bent forward) posture. It happens when the bones in the spine have fractured, making it difficult to support the weight of the body.
Signs and Symptoms of Osteoporosis
Patients with osteoporosis are asymptomatic unless a fracture has occurred. Sometimes there are obvious signs that a person has osteoporosis – for example they may ”shrink” a little and develop a stooped posture. But often the first sign that someone has osteoporosis is when they break a bone, sometimes without knowing how or why it happened. This kind of break is called a “spontaneous fracture.” When bone mass is lost the risk of breaking a bone (fractures) is higher. Osteoporosis that has already caused a fracture is referred to as “established” osteoporosis.
The bones of the spinal column (vertebrae) are the most likely to break or “collapse” in someone who has osteoporosis. Sometimes this will cause back pain, but most people do not notice anything.
Broken vertebrae are one reason why many older people stoop over and develop what is often called a “dowager’s hump” at the top of their spine.
Osteoporosis also commonly affects the wrist, the upper arm and the femur (thigh bone).
Nonvertebral fractures are typically symptomatic, but about two thirds of vertebral compression fractures are asymptomatic (although patients may have underlying chronic back pain due to other causes such as osteoarthritis). A vertebral compression fracture that is symptomatic begins with acute onset of pain that usually does not radiate, is aggravated by weight bearing, may be accompanied by point spinal tenderness, and typically begins to subside in 1 wk. However, residual pain may last for months or be constant.
Multiple thoracic compression fractures eventually cause dorsal kyphosis, with exaggerated cervical lordosis (dowager’s hump). Abnormal stress on the spinal muscles and ligaments may cause chronic, dull, aching pain, particularly in the lower back. Patients may have shortness of breath due to the reduced intrathoracic volume and/or abdominal discomfort due to the compression of the abdominal cavity as the rib cage approaches the pelvis.
Causes of osteoporosis
Losing bone is a normal part of the ageing process, but some people lose bone density much faster than normal. This can lead to osteoporosis and an increased risk of fractures.
Women also lose bone rapidly in the first few years after the menopause (when monthly periods stop and the ovaries stop producing an egg). Women are more at risk of osteoporosis than men, particularly if the menopause begins early (before the age of 45).
Many other factors can also increase the risk of developing osteoporosis, including:
- long-term use of high-dose oral corticosteroids
- other medical conditions – such as inflammatory conditions, hormone-related conditions, or malabsorption problems
- a family history of osteoporosis – particularly history of a hip fracture in a parent
- long-term use of certain medications which can affect bone strength or hormone levels
- having a low body mass index (BMI)
- heavy drinking and smoking
Preventing osteoporosis
Your genes are responsible for determining your height and the strength of your skeleton, but lifestyle factors such as diet and exercise influence how healthy your bones are.
If you’re at risk of developing osteoporosis, you should take steps to help keep your bones healthy. This may include:
- taking regular exercise
- healthy eating – including foods rich in calcium and vitamin D
- taking a daily supplement containing 10 micrograms (mcg) of vitamin D
- making lifestyle changes – such as:
- quitting smoking – smoking is associated with an increased risk of osteoporosis
- limiting your alcohol intake – it’s also important to avoid binge drinking
Regular exercise
Regular exercise is essential. Adults aged 19 to 64 should do at least 150 minutes (2 hours and 30 minutes) of moderate-intensity aerobic activity, such as cycling or fast walking, every week.
Weight-bearing exercise and resistance exercise are particularly important for improving bone density and helping to prevent osteoporosis.
As well as aerobic exercise, adults aged 19 to 64 should also do muscle-strengthening activities on two or more days a week by working all the major muscle groups, including the legs, hips, back, abdomen, chest, arms and shoulders.
If you’ve been diagnosed with osteoporosis, it’s a good idea to talk to your doctor or health specialist before starting a new exercise programme to make sure it’s right for you.
Physical activity guidelines for older adults aged 65 and over
Adults aged 65 or older who are generally fit and have no health conditions that limit their mobility should try to be active daily.
You should do:
- at least 150 minutes of moderate aerobic activity such as cycling or walking every week and
- strength exercises on 2 or more days a week that work all the major muscles (legs, hips, back, abdomen, chest, shoulders and arms)
Or
- 75 minutes of vigorous aerobic activity such as running or a game of singles tennis every week and
- strength exercises on 2 or more days a week that work all the major muscles (legs, hips, back, abdomen, chest, shoulders and arms)
Or
- a mix of moderate and vigorous aerobic activity every week (for example, two 30-minute runs plus 30 minutes of brisk walking equates to 150 minutes of moderate aerobic activity) and
- strength exercises on 2 or more days a week that work all the major muscles (legs, hips, back, abdomen, chest, shoulders and arms)
A general rule of thumb is that 1 minute of vigorous activity provides the same health benefits as 2 minutes of moderate activity.
You should also try to break up long periods of sitting with light activity, as sedentary behaviour is now considered an independent risk factor for ill health, no matter how much exercise you do.
Older adults at risk of falls, such as people with weak legs, poor balance and some medical conditions, should do exercises to improve balance and co-ordination on at least 2 days a week. Examples include yoga, tai chi and dancing.
What counts as moderate aerobic activity?
Examples of activities that require moderate effort for most people include:
- walking
- water aerobics
- ballroom and line dancing
- riding a bike on level ground or with few hills
- playing doubles tennis
- pushing a lawn mower
- canoeing
- volleyball
Moderate activity will raise your heart rate and make you breathe faster and feel warmer.
One way to tell if you’re exercising at a moderate level is if you can still talk but can’t sing the words to a song.
Daily chores such as shopping, cooking or housework don’t count towards your 150 minutes because the effort isn’t enough to raise your heart rate.
But this type of activity is still important, as it breaks up periods of sitting.
Weight-bearing exercises
Weight-bearing exercises are exercises where your feet and legs support your weight. High-impact weight-bearing exercises, such as running, skipping, dancing, aerobics, and even jumping up and down on the spot, are all useful ways to strengthen your muscles, ligaments and joints.
When exercising, wear footwear that provides your ankles and feet with adequate support, such as trainers or walking boots.
People over the age of 60 can also benefit from regular weight-bearing exercise. This can include brisk walking, keep-fit classes or a game of tennis. Swimming and cycling aren’t weight-bearing exercises.
Resistance exercises
Resistance exercises use muscle strength, where the action of the tendons pulling on the bones boosts bone strength. Examples include press-ups, weightlifting or using weight equipment at a gym.
If you’ve recently joined a gym or haven’t been for a while, your gym will probably offer you an induction. This involves being shown how to use the equipment and having exercise techniques recommended to you.
Always ask an instructor for help if you’re not sure how to use a piece of gym equipment or how to do a particular exercise.
Healthy eating and vitamin D supplements
Eating a healthy, balanced diet is recommended for everyone. It can help prevent many serious health conditions, including heart disease, diabetes and many forms of cancer, as well as osteoporosis.
Calcium is important for maintaining strong bones. Adults need 700mg a day, which you should be able to get from your daily diet. Calcium-rich foods include:
- leafy green vegetables
- dried fruit
- tofu
- yogurt
Vitamin D is also important for healthy bones and teeth because it helps your body absorb calcium. All adults should consume 10 micrograms (mcg) of vitamin D a day. Good dietary sources are:
- oily fish – such as salmon, sardines, herring and mackerel
- red meat
- liver
- egg yolks
- fortified foods such as most fat spreads and some breakfast cereals
- dietary supplements.
However, it can be difficult to get enough vitamin D from foods alone. So, all adults should consider taking a daily supplement containing 10mcg of vitamin D.
Get some sunlight
From late March/April to the end of September, sunlight triggers the production of vitamin D, which helps your body absorb calcium.
This process helps strengthen teeth and bones, which in turn helps prevent conditions such as osteoporosis.
Your body creates vitamin D from direct sunlight on your skin when we’re outdoors. From about late March/early April to the end of September, most people should be able to get all the vitamin D they need from sunlight.
You also get some vitamin D from a small number of foods, including oily fish such as salmon, mackerel, herring and sardines, as well as red meat and eggs.
Another source of vitamin D is dietary supplements.
How long should you spend in the sun?
Most people can make enough vitamin D from being out in the sun daily for short periods with their forearms, hands or lower legs uncovered and without sunscreen from late March or early April to the end of September, especially from 11am to 3pm.
It’s not known exactly how much time is needed in the sun to make enough vitamin D to meet the body’s requirements.
This is because there are a number of factors that can affect how vitamin D is made, such as your skin color or how much skin you have exposed.
But you should be careful not to burn in the sun, so take care to cover up or protect your skin with sunscreen before your skin starts to turn red or burn.
People with dark skin, such as those of African, African-Caribbean or south Asian origin, will need to spend longer in the sun to produce the same amount of vitamin D as someone with lighter skin.
How long it takes for your skin to go red or burn varies from person to person.
Your body can’t make vitamin D if you’re sitting indoors by a sunny window because ultraviolet B (UVB) rays (the ones your body needs to make vitamin D) can’t get through the glass.
The longer you stay in the sun, especially for prolonged periods without sun protection, the greater your risk of skin cancer.
If you plan to be out in the sun for long, cover up with suitable clothing, wrap-around sunglasses, seeking shade and applying at least SPF30+ sunscreen.
Winter sunlight
In the US, sunlight doesn’t contain enough UVB radiation in winter (October to early March) for our skin to be able to make vitamin D.
During these months, we rely on getting our vitamin D from food sources (including fortified foods) and supplements.
Using sunbeds isn’t a recommended way of making vitamin D.
How you can find out if you have Osteoporosis
There are tests you can get to find out your bone density. This is related to how strong or fragile your bones are. One test is called dual-energy X-ray absorptiometry (DXA or DEXA). A DXA scan takes X-rays of your bones. Screening tools also can be used to predict the risk of having low bone density or breaking a bone. Talk with your doctor or nurse about this test or tools to assess risk.
- DXA Scan
Bone density should be measured using dual-energy X-ray absorptiometry (DXA) to screen people at risk, to provide a quantitative measure of bone loss, and to monitor those undergoing treatment 9.
A DXA scan is recommended for the following patients:
- All women ≥ 65 yr
- Women between menopause and age 65 who have risk factors, including a family history of osteoporosis, a low body mass index (eg, previously defined as body weight < 127 lb), and use of tobacco and/or drugs with a high risk of bone loss (eg, glucocorticoids)
- Patients (men and women) of any age who have had fragility fractures
- Patients with evidence on imaging studies of decreased bone density or asymptomatic vertebral compression fractures incidentally noted on imaging studies
- Patients at risk of secondary osteoporosis
Although low bone density (and the associated increased risk of fracture) can be suggested by plain x-rays, it should be confirmed by a bone density measurement.
Dual-energy X-ray absorptiometry (DXA) is used to measure bone mineral density (g/cm2); it defines osteopenia or osteoporosis (in the absence of osteomalacia), predicts the risk of fracture, and can be used to follow treatment response. Bone density of the lumbar spine, hip, distal radius, or the entire body can be measured. (Quantitative CT scanning can produce similar measurements of the spine or hip but is currently not widely available.) Bone density is ideally measured at two sites, including the lumbar spine and one hip; however, at some centers, measurements are taken of the spine and both hips.
If the spine or a hip is not available for scanning (eg, because of hardware from prior total hip arthroplasty), the distal radius can be scanned (called “1/3 radius” on the DXA scan report). The distal radius should also be scanned in a patient with hyperparathyroidism because this is the most common site of bone loss in hyperparathyroidism.
DXA results are reported as T-scores and Z-scores. The T-score corresponds to the number of standard deviations that the patient’s bone density differs from the peak bone mass of a healthy, young person of the same sex and ethnicity. The WHO establishes cutoff values for T-scores that define osteopenia and osteoporosis. A T-score < -1.0 and > -2.5 defines osteopenia. A T-score ≤ -2.5 defines osteoporosis.
The Z-score corresponds to the number of standard deviations that the patient’s bone mineral density differs from that of a person of the same age and sex and should be used for children, premenopausal women, or men < 50 yr. If the Z-score is ≤ -2.0, bone density is low for the patient’s age and secondary causes of bone loss should be considered.
Current central DXA systems can also assess vertebral deformities in the lower thoracic and lumbar spine, a procedure termed vertebral fracture analysis (VFA). Vertebral deformities, even those clinically silent, are diagnostic of osteoporosis and are predictive of an increased risk of future fractures. VFA is more likely to be useful in patients with height loss ≥ 3 cm.
The need for drug therapy is based on the probability of fracture, which depends on DXA results as well as other factors. The fracture risk assessment (FRAX) score (WHO Fracture Risk Assessment Tool 10) predicts the 10-yr probability of a major osteoporotic (hip, spine, forearm, or humerus) or hip fracture in untreated patients. The score accounts for significant risk factors for bone loss and fracture. If the FRAX score is above certain thresholds (in the US, a ≥ 20% probability of major osteoporotic fracture or 3% probability of hip fracture), drug therapy should be recommended.
- For access to the free Fracture Risk Assessment Tool (FRAX tool) go here 10.
Monitoring for ongoing bone loss or the response to treatment with serial DXA scans should be done using the same DXA machine, and the comparison should use actual bone mineral density (g/cm2) rather than T-score. In patients with osteopenia, DXA should be repeated periodically to determine whether there is ongoing bone loss or development of frank osteoporosis requiring treatment. The frequency for follow-up DXA varies from patient to patient. DXA is often done every 2 to 3 yr but can sometimes be done less frequently, for example, if bone density is normal and fracture risk is low. In patients being treated for osteoporosis, DXA should be repeated, usually about every 2 to 3 yr, but sometimes more frequently in patients taking glucocorticoids. A stable or improved bone mineral density predicts a lower fracture risk. Monitoring bone density with a repeat DXA scan may help identify patients at higher risk of fractures due to a suboptimal response to osteoporosis treatment 9. Patients being treated for osteoporosis who have a significantly decreased bone mineral density on serial DXA examinations should be evaluated for drug adherence and secondary causes of bone loss.
When you should get a bone density (DXA) test
If you are age 65 or older, you should get a bone density test to screen for osteoporosis. If you are younger than 65 and have risk factors for osteoporosis, ask your doctor or nurse if you need a bone density test before age 65. Bone density testing is recommended for older women whose risk of breaking a bone is the same or greater than that of a 65‑year‑old white woman with no risk factors other than age. To find out your fracture risk and whether you need early bone density testing, your doctor will consider factors such as:
- Your age and whether you have reached menopause
- Your height and weight
- Whether you smoke
- Your daily alcohol use
- Whether your mother or father has broken a hip
- Medicines you use
- Whether you have a disorder that increases your risk of getting osteoporosis
Plain x-rays
Bones show decreased radiodensity and loss of trabecular structure, but not until about 30% of bone has been lost. However, plain x-rays are important for documenting fractures resulting from bone loss. Loss of vertebral body height and increased biconcavity characterize vertebral compression fractures. Thoracic vertebral fractures may cause anterior wedging of the bone. In long bones, although the cortices may be thin, the periosteal surface remains smooth. Vertebral fractures at T4 or above raise concern of cancer rather than osteoporosis. Plain x-rays of the spine should be considered in older patients with severe back pain and localized vertebral spinous tenderness 11.
Glucocorticoid-induced osteoporosis is likely to cause rib fractures as well as fractures at other sites where osteoporotic fractures are common. Hyperparathyroidism can be differentiated when it causes subperiosteal resorption or cystic bone lesions (rarely). Osteomalacia may cause abnormalities on imaging tests similar to those of osteoporosis (see What is Osteopenia vs Osteoporosis : Differentiating Osteopenia, Osteoporosis and Osteomalacia).
Other testing
An evaluation for secondary causes of bone loss should be considered in a patient with a Z-score ≤ -2.0 or if a cause of secondary bone loss is clinically suspected. Laboratory testing 11 should usually include the following:
- Serum calcium, magnesium, and phosphorus
- 25-Hydroxy vitamin D level
- Liver function tests, including an alkaline phosphatase (hypophosphatasia)
- Intact PTH level (hyperparathyroidism)
- 24-h urine for calcium and creatinine (hypercalciuria)
Other tests such as thyroid-stimulating hormone or free thyroxine to check for hyperthyroidism, measurements of urinary free cortisol, and blood counts and other tests to rule out cancer, especially myeloma (eg, serum and urine protein electrophoresis), should be considered depending on the clinical presentation.
Patients with weight loss should be screened for GI disorders (eg, malabsorption, celiac disease, inflammatory bowel disease) as well as cancer. Bone biopsy is reserved for unusual cases (eg, young patients with fragility fractures and no apparent cause, patients with chronic kidney disease who may have other bone disorders, patients with persistently very low vitamin D levels suspected of having osteomalacia).
Levels of fasting serum C-telopeptide cross-links (CTX) or urine N-telopeptide cross-links reflect increased bone resorption 11. Although reliability varies for routine clinical use, C-telopeptide cross-links and N-telopeptide cross-links may be helpful in monitoring response to therapy or with the timing of a drug holiday.
Osteoporosis treatment
Treating osteoporosis involves treating and preventing fractures, and using medication to strengthen bones.
An important objective for health services across England is to try to prevent falls and fractures, particularly in people with osteoporosis and those with risk factors for osteoporosis.
The key messages for older people and their family and carers are:
- falls are a risk as you get older but aren’t inevitable – there are measures you can take to prevent falls or reduce the harm that might be caused by falling
- staying active and healthy – for example, through exercise and diet – is likely to keep you independent and reduce your risk of falling
- if you’re unsteady on your feet or you fall, speak to your doctor so that possible causes of falls, such as poor eyesight, certain medications, and poor muscle strength and balance, can be identified and treated
Although a diagnosis of osteoporosis is based on the results of your bone mineral density scan (DEXA or DXA scan), the decision about what treatment you need, if any, is also based on a number of other factors. These include your:
- age
- sex
- risk of fracture
- previous injury history
If you’ve been diagnosed with osteoporosis because you’ve had a fracture, you should still receive treatment to try to reduce your risk of further fractures.
You may not need or want to take medication to treat osteoporosis. However, you should ensure you’re maintaining sufficient levels of calcium and vitamin D. To achieve this, your healthcare team will ask you about your diet and may recommend making changes or taking supplements.
Medication for osteoporosis
A number of different medications are used to treat osteoporosis. Your doctor will discuss the treatments available and make sure the medicines are right for you.
A number of factors are taken into consideration before deciding which medication to use. These include your:
- age
- bone mineral density (measured by your T score)
- risk factors for fracture
Bisphosphonates
Bisphosphonates slow the rate that bone is broken down in your body. This maintains bone density and reduces the risk of fracture.
There are a number of different bisphosphonates, including:
- alendronate
- ibandronate
- risedronate
- zoledronic acid
They’re given as a tablet or injection.
You should always take bisphosphonates on an empty stomach with a full glass of water. Stand or sit upright for 30 minutes after taking them. You’ll also need to wait between 30 minutes and 2 hours before eating food or drinking any other fluids.
Bisphosphonates usually take 6 to 12 months to work, and you may need to take them for 5 years or longer. You may also be prescribed calcium and vitamin D supplements to take at a different time to the bisphosphonate.
The main side effects associated with bisphosphonates include:
- irritation to the esophagus (the tube that food passes through from the mouth to the stomach)
- swallowing problems (dysphagia)
- stomach pain
Not everyone will experience these side effects.
Osteonecrosis of the jaw is a rare side effect linked with the use of bisphosphonates, although most frequently with high-dose intravenous bisphosphonate treatment for cancer and not for osteoporosis.
In osteonecrosis, the cells in the jaw bone die, which can lead to problems with healing. If you have a history of dental problems, you may need a check-up before you start treatment with bisphosphonates. Speak to your doctor if you have any concerns.
Selective oestrogen receptor modulators (SERMs)
SERMs are medications that have a similar effect on bone as the hormone oestrogen. They help to maintain bone density and reduce the risk of fracture, particularly of the spine.
Raloxifene is the only type of SERM available for treating osteoporosis. It’s taken as a daily tablet.
Side effects associated with raloxifene include:
- hot flushes
- leg cramps
- a potential increased risk of blood clots
Parathyroid hormone (teriparatide)
Parathyroid hormone is produced naturally in the body. It regulates the amount of calcium in bone.
Parathyroid hormone treatments (human recombinant parathyroid hormone or teriparatide) are used to stimulate cells that create new bone (osteoblasts). They’re given by injection.
While other medication can only slow down the rate of bone thinning, parathyroid hormone can increase bone density. However, it’s only used in a small number of people whose bone density is very low and when other treatments aren’t working.
Nausea and vomiting are common side effects of the treatment. Parathyroid hormone treatments should only be prescribed by a specialist.
Calcium and vitamin D supplements
Calcium is the major mineral found in bone, and having enough calcium as part of a healthy, balanced diet is important for maintaining healthy bones.
For most healthy adults, the recommended amount of calcium is 700 milligrams (mg) of calcium a day, which most people should be able to get from a varied diet that contains good sources of calcium.
However, if you have osteoporosis, you may need more calcium, which will usually be in the form of supplements. Ask your GP for advice about taking calcium supplements.
Vitamin D is needed to help the body absorb calcium. All adults should consume 10 micrograms (mcg) of vitamin D a day from October to March.
Because vitamin D is found in only a small number of foods, it might be difficult to get enough from your diet alone – so all adults should consider taking a daily supplement containing 10mcg of vitamin D.
Hormone replacement therapy (HRT)
HRT is sometimes recommended for women who are experiencing the menopause, as it can help control symptoms.
HRT has also been shown to maintain bone density and reduce the risk of fracture during treatment.
However, HRT isn’t specifically recommended for treating osteoporosis and isn’t often used for this purpose.
This is because HRT slightly increases the risk of developing certain conditions – such as breast cancer, endometrial cancer, ovarian cancer, stroke and venous thromboembolism – more than it lowers the risk of osteoporosis.
Discuss the benefits and risks of HRT with your doctor.
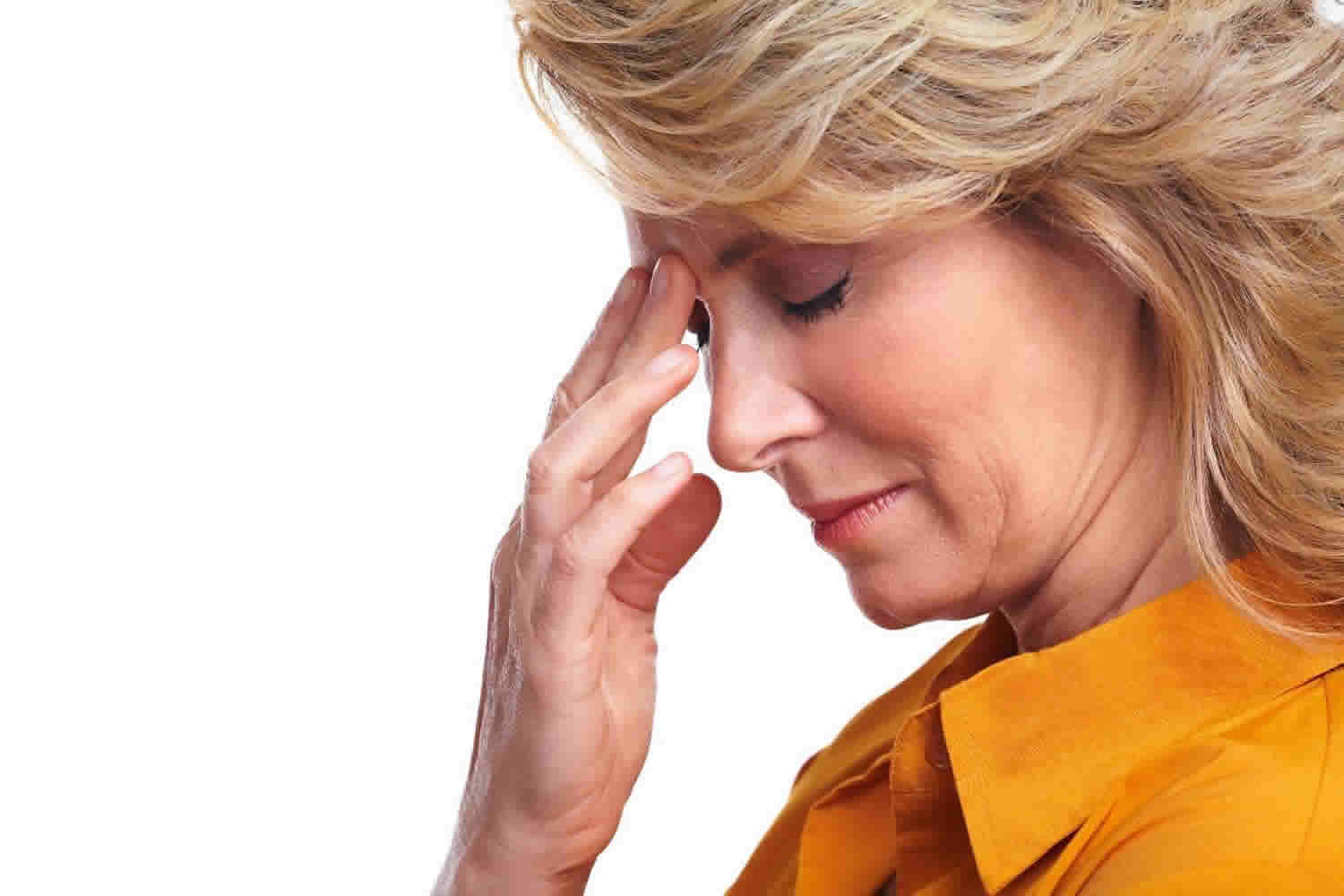
Postmenopausal hot flashes
Hot flashes, also called hot flushes, are the most common menopause symptom. As many as three out of four women experience hot flashes. Some women begin having hot flashes before menopause, when they are still getting a period 1.
Hot flashes are a sudden feeling of heat in the upper part of your body. Your face and neck may become red. Red blotches may appear on your chest, back, and arms. You may also get heavy sweating during hot flashes or cold chills after the hot flashes. Some women get more cold chills (also called cold flashes) than hot flashes.
During a hot flash, you might have:
- A sudden feeling of warmth spreading through your upper body and face
- A flushed appearance with red, blotchy skin
- Rapid heartbeat
- Perspiration, mostly on your upper body
- A chilled feeling as the hot flash lets up
Hot flashes can vary in frequency and intensity. How long symptoms last varies greatly. On average, symptoms persist for more than seven years. Some women have them for more than 10 years.
Hot flashes are most common in women in the year before their period stops and in the year after their period stops. However, recent studies show that hot flashes can continue for up to 14 years after menopause 5. Doctors and researchers do not know why hot flashes are so common during menopause. There are medicines that can prevent some hot flashes, and there are ways you can try to manage hot flashes when they do happen.
Risk factors of hot flashes
Not all women who go through menopause have hot flashes, and it’s not clear why some women do have them. Factors that may increase your risk include:
- Smoking. Women who smoke are more likely to get hot flashes.
- Obesity. A high body mass index (BMI) is associated with a higher frequency of hot flashes.
- Ethnicity. More African-American women report menopausal hot flashes than do women of European descent. Hot flashes are less common in women of Japanese and Chinese descent than in white European women.
Hot flashes treatment
Deciding whether and how to treat the symptoms of the menopause can be complicated and personal. Discuss your symptoms, family and medical history, and preferences with your doctor.
No matter what you decide, see your doctor every year to talk about your treatment plan and discuss any changes you want to make.
However, the most effective way to relieve the discomfort of hot flashes is to take estrogen, but taking this hormone carries risks. If estrogen is appropriate for you and you start it within 10 years of your last menstrual period or before age 60, the benefits can be greater than the risks.
Medications such as antidepressants and anti-seizure drugs also might help reduce hot flashes, although they’re less effective than hormones.
Discuss the pros and cons of various treatments with your doctor. If hot flashes don’t interfere with your life, you probably don’t need treatment. Hot flashes subside gradually for most women, even without treatment, but it can take several years for them to stop.
- Consider using hormones. If you still have menstrual periods, ask your doctor about low-dose hormonal birth control. This may help your symptoms. For women who have gone through menopause, menopausal hormone therapy helps relieve hot flashes and night sweats. There are risks to menopausal hormone therapy. Ask your doctor whether it may help you. If you decide to use menopausal hormone therapy, take it for the shortest amount of time possible in the lowest dose that helps your symptoms.
- Consider other medicines. If hormone treatments are not an option for you, ask your doctor about prescription medicines used for other health problems. Certain antidepressants, epilepsy medicine, and blood pressure medicines may help with hot flashes, even if you don’t have these specific health problems.
- Track your hot flashes. Write down what triggers your hot flashes and try to avoid those things. Possible triggers might include spicy foods, alcohol, caffeine, stress, or being in a hot place.
- Drink cold water. Keep ice water close by to drink when you feel a hot flash coming on.
- Take off a layer of clothing. Dress in layers as much as possible.
- Use a fan. Turn on a fan at night by your bed and keep one at work if possible.
- Take deep breaths. Try taking slow, deep breaths when a hot flash starts. Slow, deep breaths tell your body that it is time to relax and be calm. This might make hot flashes shorter.
- Lose weight. Hot flashes may be worse in women who have overweight or obesity. A recent study found that losing weight may help improve hot flashes.4
Non-Hormone Options for Treating Hot Flashes
If lifestyle changes are not enough to improve your symptoms, non-hormone options for managing hot flashes may work for you. They may be a good choice if you are unable to take hormones or if you are worried about their potential risks.
The U.S. Food and Drug Administration (FDA) has approved the use of paroxetine, a low-dose selective serotonin reuptake inhibitor (SSRI) antidepressant, to treat hot flashes. Researchers are studying the effectiveness of other antidepressants in this class.
Women who use an antidepressant to help manage hot flashes generally take a lower dose than people who use the medication to treat depression. Side effects depend on the type of antidepressant you take and can include dizziness, headache, nausea, jitteriness, or drowsiness. As with any medication, talk with your doctor about whether this is the right medication for you and how you can manage any possible side effects.
Antidepressants
A low-dose form of paroxetine (Brisdelle) is the only nonhormone treatment for hot flashes approved by the Food and Drug Administration. Other antidepressants that have been used to treat hot flashes include:
- Venlafaxine (Effexor XR, Pristiq)
- Paroxetine (Paxil, Pexeva)
- Fluoxetine (Prozac, Sarafem, others)
These medications aren’t as effective as hormone therapy for severe hot flashes, but they can be helpful to women who can’t use hormones. Possible side effects include nausea, dizziness, weight gain, dry mouth or sexual dysfunction.
Other prescription medications
Other medications that might offer relief for some women include:
- Gabapentin (Neurontin, Gralise, others). Gabapentin is an anti-seizure medication that’s moderately effective in reducing hot flashes. Side effects can include drowsiness, dizziness and headaches.
- Clonidine (Catapres, Kapvay, others). Clonidine, a pill or patch typically used to treat high blood pressure, might provide some relief from hot flashes. Side effects include dizziness, drowsiness, dry mouth and constipation.
- Tibolone. Tibolone (brand name Livial) is a prescription medication that is similar to taking combined hormone replacement therapy (oestrogen and progestogen). It’s taken as a tablet once a day.It can help relieve symptoms such as hot flushes, low mood and reduced sex drive, although some studies have suggested it may not be as effective as combined hormone replacement therapy.It’s only suitable for women who had their last period more than a year ago (known as the post-menopause).
Side effects of tibolone can include tummy (abdominal) pain, pelvic pain, breast tenderness, itching and vaginal discharge.
Risks of tibolone are similar to the risks of hormone replacement therapy, and include an increased risk of breast cancer and strokes. Talk to your doctor about the risks and benefits of tibolone if you’re considering taking it.
- Clonidine. Clonidine is a prescription medicine that can help reduce hot flushes and night sweats in some menopausal women. It’s taken as tablets two or three times a day. It doesn’t affect hormone levels, so unlike hormone replacement therapy (HRT) it doesn’t carry an increased risk of problems such as breast cancer. But research suggests it only has a very small effect on menopausal symptoms.Clonidine can also cause some unpleasant side effects, including dry mouth, drowsiness, depression and constipation.It may take two to four weeks to notice the effects of clonidine. Speak to your doctor if your symptoms don’t improve or you experience any troublesome side effects.
Medications For Treating Hot Flashes and Night Sweats with Hormones
Some women may choose to take hormones to treat their hot flashes. A hormone is a chemical substance made by an organ like the thyroid gland or ovary. During the menopausal transition, the ovaries begin to work less and less well, and the production of hormones like estrogen and progesterone declines over time. It is believed that such changes cause hot flashes and other menopausal symptoms.
Hormone therapy steadies the levels of estrogen and progesterone in the body. It is a very effective treatment for hot flashes in women who are able to use it. There are risks associated with taking hormones, including increased risk of heart attack, stroke, blood clots, breast cancer, gallbladder disease, and dementia. The risks vary by a woman’s age and whether she has had a hysterectomy. Women are encouraged to discuss the risks with their healthcare provider.
Women who still have a uterus should take estrogen combined with progesterone or another therapy to protect the uterus. Progesterone is added to estrogen to protect the uterus against cancer, but it also seems to increase the risk of blood clots and stroke. Hormones should be used at the lowest dose that is effective for the shortest period of time possible.
- Talk with your doctor before using hormones to treat menopause symptoms. Hormones should be used at the lowest dose and for the shortest period of time they are effective.
Hormones can be very effective at reducing the number and severity of hot flashes. They are also effective in reducing vaginal dryness and bone loss.
Hormone treatments (sometimes called menopausal hormone therapy) can take the form of pills, patches, rings, implants, gels, or creams. Patches, which stick to the skin, may be best for women with cardiac risk factors, such as a family history of heart disease.
There are many types of hormones available for women to treat hot flashes. These include estradiol, conjugated estrogen, selective estrogen receptor modulators (SERMs), and compounded or synthetic hormones. It is a common misconception that synthetic (“bioidentical”) hormones mixed by a compounding pharmacist are safer and less risky than other hormone therapies. This is not the case. We must assume they have the same risks as any hormone therapy.
Some of the relatively mild side effects of hormone use include breast tenderness, spotting or return of monthly periods, cramping, or bloating. By changing the type or amount of the hormones, the way they are taken, or the timing of the doses, your doctor may be able to help control these side effects or, over time, they may go away on their own.
Hormone therapy
Estrogen is the primary hormone used to reduce hot flashes. Women who have had a hysterectomy can take estrogen alone. But if you still have a uterus, you should take progesterone with estrogen to protect against cancer of the lining of the uterus (endometrial cancer).
With either regimen, the therapy needs to be tailored to your needs. Guidelines suggest using the smallest effective dose for symptom control. How long you use the treatment depends on the balance of your risks and benefits from hormone therapy. The goal is to optimize your quality of life.
A combination drug of bazedoxifene with conjugated estrogens (Duavee) has been approved for treating menopausal symptoms. This drug might not increase your risk of uterine cancer and might protect your bones.
Estrogen therapy isn’t a good option if you’ve had a blood clot or breast cancer.
The main benefit of hormone replacement therapy (HRT) is that it can help relieve most of the menopausal symptoms, such as:
- hot flushes
- night sweats
- mood swings
- vaginal dryness
- reduced sex drive
Many of these symptoms pass in a few years, but they can be very unpleasant and taking hormone replacement therapy can offer relief for many women.
It can also help prevent weakening of the bones (osteoporosis), which is more common after the menopause.
Some women should not use hormones for their hot flashes.
You should not take hormones for menopausal symptoms if:
- You have had certain kinds of cancers, like breast cancer or uterine cancer
- You have had a stroke or heart attack, or you have a strong family history of stroke or heart disease
- You have had blood clots
- You have had problems with vaginal bleeding or have a bleeding disorder
- You have liver disease
- You have untreated high blood pressure – your blood pressure will need to be controlled before you can start hormone replacement therapy
- You think you are pregnant or may become pregnant. It’s still possible to get pregnant while on hormone replacement therapy, so you should use contraception until two years after your last period if you’re under 50 or for one year after the age of 50
- You have had allergic reactions to hormone medications
Talk with your doctor to find out if taking hormones to treat your symptoms is right for you.
Types of hormone replacement therapy
There are many different types of hormone replacement therapy and finding the right one for you can be tricky.
If you’re considering hormone replacement therapy, talk to your doctor about the options suitable for you, as well as possible alternatives to hormone replacement therapy.
There are different:
- hormone replacement therapy hormones – most women take a combination of the hormones estrogen and progestogen, although women who don’t have a womb can take estrogen on its own
- ways of taking hormone replacement therapy – including tablets, skin patches, gels and vaginal creams, pessaries or rings
- hormone replacement therapy treatment regimens – hormone replacement therapy medication may be taken continuously without a break, or in cycles where you take estrogen continuously and only take progestogen every few weeks
Your doctor can give you advice to help you choose which type is best for you. You may need to try more than one type before you find one that works best.
Hormone replacement therapy hormones
Hormone replacement therapy replaces the hormones that a woman’s body no longer produces because of the menopause.
The two main hormones used in hormone replacement therapy are:
- Estrogen – types used include estradiol, estrone and estriol
- progestogen – a synthetic version of the hormone progesterone, such as dydrogesterone, medroxyprogesterone, norethisterone and levonorgestrel
Hormone replacement therapy involves either taking both of these hormones (combined hormone replacement therapy) or just taking estrogen (estrogen-only hormone replacement therapy).
Most women take combined hormone replacement therapy because taking oestrogen on its own can increase your risk of developing womb (endometrial) cancer. Taking progestogen alongside oestrogen minimises this risk.
Estrogen-only hormone replacement therapy is usually only recommended for women who have had their womb removed during a hysterectomy.
Ways of taking hormone replacement therapy
Hormone replacement therapy is available in several preparations that are taken in different ways. Talk to your doctor about the pros and cons of each option.
Tablets
Tablets, which are usually taken once a day, are one of the most common ways of taking hormone replacement therapy.
Estrogen-only and combined hormone replacement therapy tablets are available. For some women this may be the simplest way of having treatment.
However, it’s important to be aware that some of the risks of hormone replacement therapy, such as blood clots, are higher with tablets than with other forms of hormone replacement therapy (although the overall risk is still small).
Skin patches
Skin patches are also a common way of taking hormone replacement therapy. You stick them to your skin and replace them every few days. Oestrogen-only and combined hormone replacement therapy patches are available.
Patches may be a better option than tablets if you think you might find it inconvenient to take a tablet every day.
Using patches can also help avoid some side effects of hormone replacement therapy, such as indigestion, and unlike tablets they don’t increase your risk of blood clots.
Estrogen gel
Estrogen gel is an increasingly popular form of hormone replacement therapy. It’s applied to the skin once a day and is absorbed by the body.
Like skin patches, this can be a convenient way of taking hormone replacement therapy while avoiding an increased risk of blood clots.
But if you still have your womb, you’ll need to take some form of progestogen separately too, to reduce your risk of womb cancer.
Implants
Hormone replacement therapy can be given using small pellet-like implants inserted under your skin (usually in the tummy area) while your skin is numbed with local anaesthetic, although these aren’t widely available and aren’t used very often.
The implants release estrogen gradually over time and can stay in place for several months before needing to be replaced.
This may be a convenient option if you don’t want to worry about taking your treatment every day or every few days. But if you still have your womb, you’ll need to take progestogen separately too.
If you’re taking a different form of estrogen and need to take progestogen alongside it, another implant option is the intrauterine system (IUS). An IUS releases a progestogen hormone into the womb. It can remain in place for a few years and also acts as a contraceptive.
Vaginal estrogen
Estrogen is also available in the form of a cream, pessary or ring that is placed inside your vagina.
This can help relieve vaginal dryness, but won’t help with other symptoms such as hot flushes.
It doesn’t carry the usual risks of hormone replacement therapy and can be used without taking progestogen even if you still have a womb.
Hormone replacement therapy treatment regimens
Different treatment courses of hormone replacement therapy are also available, depending on whether you’re still in the early stages of the menopause or have had menopausal symptoms for some time.
The two types are cyclical (or sequential) hormone replacement therapy and continuous hormone replacement therapy.
Cyclical hormone replacement therapy
Cyclical hormone replacement therapy, also known as sequential hormone replacement therapy, is often recommended for women taking combined hormone replacement therapy who have menopausal symptoms but still have their periods.
There are two types of cyclical hormone replacement therapy:
- monthly hormone replacement therapy – you take estrogen every day, and take progestogen alongside it for the last 14 days of your menstrual cycle
- three-monthly hormone replacement therapy – you take estrogen every day, and take progestogen alongside it for around 14 days every three months
Monthly hormone replacement therapy is usually recommended for women having regular periods.
Three-monthly hormone replacement therapy is usually recommended for women experiencing irregular periods. You should have a period every three months.
It’s useful to maintain regular periods so you know when your periods naturally stop and when you’re likely to progress to the last stage of the menopause.
Continuous combined hormone replacement therapy
Continuous combined hormone replacement therapy is usually recommended for women who are post-menopausal. A woman is usually said to be post-menopausal if she has not had a period for a year.
As the name suggests, continuous hormone replacement therapy involves taking estrogen and progestogen every day without a break.
Estrogen-only hormone replacement therapy is also usually taken continuously.
Side effects of hormone replacement therapy
Like any medication, the hormones used in hormone replacement therapy (hormone replacement therapy) can sometimes have side effects.
Any side effects usually improve over time, so it’s a good idea to persevere with treatment for at least three months if possible.
Speak to your doctor if you experience severe side effects or they continue for longer than three months.
Side effects of estrogen
The main side effects associated with taking estrogen include:
- bloating
- breast tenderness or swelling
- swelling in other parts of the body
- nausea
- leg cramps
- headaches
- indigestion
- vaginal bleeding
These side effects will often pass in a few weeks, but the following measures may help relieve some of them in the meantime:
- taking your estrogen dose with food may help to reduce nausea and indigestion
- eating a low-fat, high-carbohydrate diet may reduce breast tenderness
- regular exercise and stretching may help reduce leg cramps
If side effects persist, your doctor may recommend switching to a different way of taking estrogen (for example, changing from a tablet to a patch), changing the specific medication you’re taking, or lowering your dose.
Side effects of progestogen
The main side effects associated with taking progestogen include:
- breast tenderness
- swelling
- headaches or migraines
- mood swings
- depression
- acne
- tummy (abdominal) pain
- back pain
- vaginal bleeding
As with side effects of estrogen, these will usually pass in a few weeks.
If they persist, your doctor may recommend switching to a different way of taking progestogen, changing the specific medication you’re taking, or lowering your dose.
Weight gain and hormone replacement therapy
Many women believe that taking hormone replacement therapy will make them put on weight, but there’s no evidence to support this claim.
You may gain some weight during the menopause, but this often happens regardless of whether you take hormone replacement therapy.
Exercising regularly and eating a healthy diet should help you to lose any unwanted weight.
More serious risks of HRT
Hormone replacement therapy has also been associated with some more serious risks, such as an increased risk of blood clots and certain types of cancer.
Breast cancer
The National Institute for Health and Care Excellence 12 says:
- taking combined hormone replacement therapy (estrogen and progestogen) is associated with a small increased risk of breast cancer – some studies have suggested that for every 1,000 women taking combined hormone replacement therapy, there will be around five extra cases of breast cancer (from a normal risk of 22 cases of breast cancer per 1,000 menopausal women to 27)
- the risk of breast cancer decreases when you stop taking hormone replacement therapy – estimates suggest the level of risk returns to normal after about five years
- estrogen-only hormone replacement therapy is associated with little or no change in the risk of breast cancer
Because of the risk of breast cancer, it’s especially important to attend all your breast cancer screening appointments if you’re taking combined hormone replacement therapy.
Ovarian cancer
Studies looking at whether hormone replacement therapy can increase your risk of ovarian cancer have so far had conflicting results.
It’s thought that if there is any increase in cases of ovarian cancer in women taking hormone replacement therapy, the risk is very small.
A recent study found that for every 1,000 women taking hormone replacement therapy for five years, there will be one extra case of ovarian cancer.
Any risk of ovarian cancer is thought to decrease once you stop taking hormone replacement therapy.
Womb cancer (uterine cancer)
Estrogen-only hormone replacement therapy can increase the risk of womb cancer (also called endometrial cancer), which is why it’s only used in women who don’t have a womb (for example, because they’ve had a hysterectomy).
Taking combined hormone replacement therapy, particularly a course of continuous hormone replacement therapy (where you take both medications without a regular break), largely eliminates this risk.
If you still have a womb and you’re taking hormone replacement therapy, it’s important to take both medications as advised by your doctor to avoid increasing your risk of womb cancer.
Blood clots
Blood clots can be serious if they become lodged in a blood vessel and block the flow of blood.
The National Institute for Health and Care Excellence 12 says:
- taking hormone replacement therapy tablets can increase your risk of blood clots
- there’s no increased risk of blood clots from hormone replacement therapy patches or gels
- It’s thought the risk of developing a blood clot is about two to four times higher than normal for women taking hormone replacement therapy tablets. But as the risk of menopausal women developing blood clots is normally very low, the overall risk from hormone replacement therapy tablets is still small.
It’s estimated that for every 1,000 women taking hormone replacement therapy tablets for 7.5 years, less than two will develop a blood clot.
Heart disease and strokes
The National Institute for Health and Care Excellence 12 says:
- hormone replacement therapy doesn’t significantly increase the risk of cardiovascular disease (including heart disease and strokes) when started before 60 years of age
- estrogen-only hormone replacement therapy is associated with no, or reduced, risk of heart disease
- combined hormone replacement therapy is associated with little or no increase in the risk of heart disease
- taking estrogen tablets is associated with a small increase in the risk of stroke, although the normal risk of women under 60 having a stroke is very low, so the overall risk is small
Speak to your doctor if you’re taking hormone replacement therapy or are considering taking it and are worried about the risk of stroke or heart disease.
Bioidentical or “natural” hormones
Bioidentical hormones are hormone preparations made from plant sources that are promoted as being similar or identical to human hormones.
Practitioners claim these hormones are a “natural” and safer alternative to standard hormone replacement therapy preparations.
However, bioidentical preparations aren’t recommended because:
- they aren’t regulated and it’s not clear how safe they are – there’s no good evidence to suggest they’re safer than standard HRT
- it’s not known how effective they are in reducing menopausal symptoms
- the balance of hormones used in bioidentical preparations is usually based on the hormone levels in your saliva, but there’s no evidence that these levels are related to your symptoms
Many standard hormone replacement therapy hormones are made from natural sources, but unlike bioidentical hormones they’re closely regulated and have been well researched to ensure they’re as effective and safe as possible.
Unproven, Nonscientific “Treatments” for Hot Flashes
People often assume that “natural” or “herbal” products cause no harm. However, all supplements may have potentially harmful side effects, and supplements can also interact with medications you’re taking for other medical conditions. Always review what you’re taking with your doctor.
You may have heard about black cohosh, DHEA, or soy isoflavones from friends who are using them to try to treat their hot flashes. These products are not proven to be effective and some carry risks like liver damage.
Phytoestrogens are estrogen-like substances found in some cereals, vegetables, and legumes (like soy), and herbs. They might work in the body like a weak form of estrogen, but they have not been consistently shown to be effective in research studies, and their long-term safety is unclear.
At this time, it is unknown whether herbs or other “natural” products are helpful or safe. The benefits and risks are still being studied. Always talk with your doctor before taking any herb or supplement to treat your hot flashes or other menopausal symptoms.
Dietary supplements commonly used for menopause symptoms include:
- Plant estrogens. Asian women, who consume soy regularly, are less likely to report hot flashes and other menopausal symptoms than are women in other parts of the world. One reason might be related to the estrogen-like compounds in soy. However, studies have generally found little or no benefit with soy, although research is ongoing to determine whether specific components of soy, such as genistein, help hot flashes.
- Black cohosh. Black cohosh has been popular among many women with menopausal symptoms. Studies of black cohosh’s effectiveness have had mixed results, and the supplement might be harmful to the liver in rare circumstances.
- Ginseng. While ginseng may help with mood symptoms and insomnia, it doesn’t appear to reduce hot flashes.
- Dong quai. Study results indicate that dong quai isn’t effective for hot flashes. The supplement can increase the effectiveness of blood-thinning medications, which can cause bleeding problems.
- Vitamin E. Taking a vitamin E supplement might offer some relief from mild hot flashes. In high doses, it can increase your risk of bleeding.
Nerve block procedure
A procedure known as stellate ganglian block has shown promise for treating moderate to severe hot flashes, but more research is needed. It involves injecting an anesthetic into a nerve cluster in the neck. The treatment has been used for pain management. Side effects include pain and bruising at the injection site.
Other postmenopausal symptoms and treatment
Vaginal problems and infections
Vaginal problems, such as vaginal dryness, may start or get worse in the time around menopause. Low levels of the hormone estrogen may cause your vaginal tissue to get drier and thinner. This can cause itching, burning and pain or discomfort. It also can make sex painful and cause small cuts and tears in your vagina during sex 13. Vaginal cuts or tears put you at higher risk for sexually transmitted infections (STIs, or STDs).
What you can do:
- Vaginal moisturizer. An over-the-counter vaginal moisturizer can help keep your vagina lubricated and can make sex more comfortable. You use this every few days.
- Vaginal lubricant. A water-based, over-the-counter vaginal lubricant can help make sex more comfortable. You use this before or during sex.
- Prescription medicine. You can also talk to your doctor about other ways to treat your vaginal dryness, including hormonal birth control, menopausal hormone therapy, or a prescription estrogen cream, gel, or ring that is inserted into your vagina.
Problems sleeping
Many women in menopause find it hard to sleep through the night. Low levels of progesterone can make it hard to fall and stay asleep. Low estrogen levels can also cause hot flashes that make you sweat while you sleep 14. This is sometimes called night sweats. Many menopausal women get urinary symptoms that make them get up several times during sleep to urinate. You may also feel more tired than usual during the day.
What you can do
- Exercise. One of the best ways to get a good night’s sleep is to get regular physical activity. But you may need to work out earlier in the day. Too much activity close to bedtime can make you more awake. Even if you have not exercised regularly in the past, starting to exercise during menopause may help you feel better. Studies show that certain exercises, such as yoga and stretching, may help improve hot flashes 15
- Do not eat, drink alcohol, or smoke before bed. Avoid large meals, smoking, and drinking alcohol right before bedtime. Avoid caffeine after noon.
- Drink warm drinks. Try drinking something warm before bedtime, such as caffeine-free tea or warm milk.
- Limit screen-time near bedtime. Limit TV, phone, or computer use near bedtime, especially in your bedroom. The bright light of the screens tell your brain to wake up instead of sleep 16
- Practice good sleep habits. Keep your bedroom dark, quiet, and cool. Use your bedroom only for sleep and sex, if you can.
- Don’t nap during the day. Try to go to bed and get up at the same times every day.
- Train your brain. If you wake during the night and can’t get back to sleep, get up and do something relaxing until you’re sleepy again.
- Talk to your doctor or nurse. Talk to your doctor or nurse about your sleep problems, as it could be something serious. Many women develop sleep apnea or insomnia 17. Treating sleep problems can also help improve chronic pain.
- Consider treatment for hot flashes. Talk to your doctor or nurse about treatment for your hot flashes if they are causing your sleep problems. This will usually improve your sleep.
- Treat bladder problems. Talk to your doctor or nurse about treatment for urinary problems. Urinary or bladder incontinence is not a normal part of the aging process. There are treatments that work.
Memory problems
You might become forgetful or have trouble focusing. As many as two-thirds of women going through perimenopause say they have problems with memory or trouble focusing 18. Menopausal hormone therapy does not treat or prevent memory loss or brain diseases, including dementia and Alzheimer’s disease. In a recent study, memory problems were linked to depression and loss of sleep but not to levels of the hormone estrogen 18.
What you can do
- Get enough sleep and physical activity, eat healthy and don’t smoke. This may improve memory 19
- Stay socially active. Join a group or club that focuses on activities you enjoy, such as a hiking club or a quilting bee. Social interaction may help delay memory loss and prevent diseases such as dementia and Alzheimer’s disease 20
- Stay mentally active. You may be able to boost your memory and focus by doing mental activities like crossword puzzles, taking a class, or learning a new skill like a foreign language.
- Talk to your doctor if forgetfulness or other mental problems affect your daily life.
Urinary problems
Many women develop bladder or urinary problems during menopause. Lower estrogen levels may weaken the urethra. Some women find it hard to hold their urine long enough to get to the bathroom. This is called urinary urge incontinence. Urine might also leak out when you sneeze, cough, or laugh. This is called urinary stress incontinence. Some women have disrupted sleep during menopause because of the need to urinate during sleep. Urinary problems after menopause are not a normal part of aging and can be treated.
What you can do
- Treatment for urinary incontinence can include limiting or avoiding caffeine, taking medicine, using special medical devices, physical therapy, or having surgery, depending on the cause of the condition.
- If you have urine leakage, you can try urinary incontinence products such as pads, a urethra cap, or a pessary. A urethra cap fits over your urinary opening. It is reusable. A pessary is a round disk that is inserted into your vagina to support your bladder. Your doctor or nurse will fit you for your pessary, but you can remove, wash, and reinsert it yourself.
- Talk to your doctor or nurse about things you can do at home to help treat urinary incontinence. These may include a special kind of exercise for your pelvic floor muscles called Kegel exercises. Your doctor or nurse may also suggest losing weight, since extra weight puts more pressure on your bladder and nearby muscles.
Mood changes
You might feel irritable or have crying spells. If you had mood changes with your monthly periods or depression after giving birth, you may be more likely to have mood changes with menopause, too 21. Even if you never experienced mood changes during your monthly periods or after giving birth, you may still get mood changes during menopause. Mood changes at this time also could be from stress, family changes, or feeling tired. Mood changes are not the same as depression.
What you can do
- Try to get seven to eight hours of sleep.
- Get active to help you feel your best. Find ways to get active.
- Avoid taking on too many duties as much as possible. Look for positive ways to ease your stress.
- Join a support group online or in your community with women who are also going through menopause.
- Talk to your doctor or nurse about menopausal hormone therapy, which can help with mild mood changes. All medicines have risks, including menopausal hormone therapy. Mood changes that happen during menopause are usually not the same as depression, which is a different, serious illness that also needs treatment.
Depression and anxiety
Your risk for depression and anxiety is higher during the time around menopause. This may be caused by changing hormones, menopausal symptoms, or both. You may experience sadness or depression over the loss of fertility or the changes in your body. If you have symptoms of depression or anxiety, see your doctor. Your doctor may recommend therapy or medicine or both to treat depression or anxiety.
What you can do
- Sleep. Try to get enough sleep. Most adults need between seven and eight hours of sleep each night. Lack of sleep is linked to depression 17
- Exercise. Get at least 30 minutes of physical activity on most days of the week. Exercise is proven to help with depression. See our Fitness section for tips on how to get active.
- Limit alcohol. Limit how much alcohol you drink, if any. A moderate amount of alcohol for women is one drink a day, and no more than seven drinks in a week. More than four drinks at a time is considered binge drinking.
- Lower stress. Set limits for how much you take on. Look for positive ways to unwind and ease daily stress. Try relaxation techniques, reading a book, spending some quiet time outdoors, or other healthy ways to unwind.
Changing feelings about sex
Some women feel more comfortable with their sexuality after menopause. Others may feel less aroused. You may feel less interested in sex if it is uncomfortable or painful. This can happen because of drier or thinner vaginal tissue.
Menopause may cause changes in your sex life, or you may not notice any changes at all. Here are some possible changes:
- Lower hormone levels can make your vaginal tissue drier and thinner. This condition, called vaginal atrophy, can make sex uncomfortable or painful.
- Lower hormones may lower your sex drive. It may take you longer to get aroused.
- Night sweats can disturb your sleep and make you tired.
- Emotional changes can make you feel stressed or irritable.
Being less interested in sex as you get older is not a medical condition that requires treatment. But if changes in your sexual health bother you, talk to your doctor or nurse about ways to help, such as treatments to relieve vaginal dryness.
What you can do
- If you are bothered by vaginal dryness, there are safe over-the-counter and prescription treatments to improve vaginal lubrication.
- Some women are less interested in sex during menopause because of other menopause symptoms such as depression, anxiety, or lack of sleep. Talk with your doctor or nurse about possible treatments if your menopause symptoms bother you.
- Be active. Physical activity can boost your energy levels, lift your mood, and improve your body image. All of these can help increase your interest in sex.
- Don’t smoke. Cigarette smoking can reduce blood flow to the vagina and lower the effects of estrogen. This can make it more difficult to get aroused.
Avoid drugs and alcohol. They can slow down how your body responds. - Have sex more often. If you choose to have sex, it can increase blood flow to your vagina and help keep tissues healthy.
- Allow time to become aroused during sex. Moisture from being aroused protects tissues and makes sex more comfortable.
- Practice pelvic floor exercises. These can increase blood flow to the vagina and strengthen the muscles involved in orgasm. Learn more about pelvic floor exercises.
- Avoid products that irritate your vagina. Bubble bath and strong soaps might cause irritation. See your doctor or nurse if you have vaginal itching or irritation as it may be a sign of infection.
- Talk to your doctor or nurse about products to increase your sex drive if you are bothered by a low level of interest in sex. Some women try products like pills or creams with the male hormone testosterone or similar products. The Food and Drug Administration (FDA) has not approved these products for treating low female sex drive. But, the FDA has approved flibanserin, a medicine to treat low sexual desire. If you take flibanserin, you cannot drink alcohol because of its risks for serious low blood pressure problems and loss of consciousness. Flibanserin can increase the number of times you have a satisfying sexual experience by once a month or once every two months. Talk to your doctor about the benefits and other risks of taking any medicine.
For vaginal dryness that causes mild discomfort during sex:
- Use an over-the-counter, water-based vaginal lubricant when you have sex.
- Try an over-the-counter vaginal moisturizer to help increase moisture. You may need to use it every few days.
For more severe vaginal dryness, your doctor might prescribe medicines that you put into your vagina to increase moisture and sensation. These may include 22:
- Vaginal estrogen creams
- Estrogen tablets or rings for insertion into the vagina
- A non-hormonal medicine called ospemifene 23
Discuss your symptoms and personal health issues with your doctor or nurse to decide whether one or more treatment options are right for you.
- Shifren, J.L., Gass, M.L.S., for the NAMS Recommendations for Clinical Care of Midlife Women Working Group. (2014). The North American Menopause Society Recommendations for Clinical Care of Midlife Women. Menopause; 21(10): 1038–1062.[↩][↩][↩]
- Mishra, G.D., Cooper, R., Tom, S.E., Kuh, D. (2009). Early life circumstances and their impact on menarche and menopause. Womens Health; 5: 175–190.[↩]
- Avis, N.E., McKinlay, S.M. (1991). A longitudinal analysis of women’s attitudes toward the menopause: Results from the Massachusetts Women’s Health Study (link is external). Maturitas; 13: 65–79.[↩]
- Smoking’s Impact on Women’s Health. https://women.smokefree.gov/quit-smoking/what-women-should-know/smokings-impact-on-women[↩]
- Tepper, P.G., Brooks, M.M., Randolph, J.F., Crawford, S.L., Khoudary, E., Gold, E.B., et al. (2016). Characterizing the trajectories of vasomotor symptoms across the menopausal transition. Menopause; 23(10): 1067–1074.[↩][↩]
- Becker, R.C. (2005). Heart attack and stroke prevention in women (link is external). Circulation; 112: e273–e275.[↩]
- Crandall, C., Aragaki, A., Cauley, J., Manson, J., LeBlanc, E., Wallace, R., et al. (2015). Associations of Menopausal Vasomotor Symptoms with Fracture Incidence (link is external). Journal of Clinical Endocrinology and Metabolism; 100(2): 524–534.[↩]
- Jackson, L.W., Cromer, B.A., Panneerselvamm, A. (2010). Association between bone turnover, micronutrient intake, and blood lead levels in pre-and postmenopausal women, NHANES 1999–2002. Environmental Health Perspectives; 118(11): 1590–1596.[↩]
- Leslie WD, Majumdar SR, Morin SN, Lix LM: Change in bone mineral density is an indicator of treatment-related antifracture effect in routine clinical practice: A registry-based cohort study. Ann Intern Med 165(7):465–472, 2016. doi: 10.7326/M15-2937. http://annals.org/aim/article/2534408/change-bone-mineral-density-indicator-treatment-related-antifracture-effect-routine[↩][↩]
- Centre for Metabolic Bone Diseases, University of Sheffield, UK. Fracture Risk Assessment Tool. https://www.sheffield.ac.uk/FRAX/tool.jsp[↩][↩]
- Merck Sharp & Dohme Corp., Merck Manual. Osteoporosis. https://www.merckmanuals.com/professional/musculoskeletal-and-connective-tissue-disorders/osteoporosis/osteoporosis[↩][↩][↩]
- The National Institute for Health and Care Excellence. https://www.nice.org.uk/[↩][↩][↩]
- Muhleisen, A. L., Herbst-Kralovetz, M. M. (2016). Menopause and the vaginal microbiome. Maturitas; 91:42-50.[↩]
- Kravitz, H. M., Ganz, P. A., Bromberger, J., Powell, L. H., Sutton-Tyrrell, K., Meyer, P. M. (2003). Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause; 10, 19–28.[↩]
- Innes, K.E., Selfe, T.K., Vishnu, A. (2010). Mind-body Therapies for Menopausal Symptoms: A Systematic Review. Maturitas; 66(2): 135-149.[↩]
- Lights Out for a Good Night’s Sleep. https://www.sleepfoundation.org/sleep-news/lights-out-good-nights-sleep[↩]
- Eichling, P.S., Sahni, J. (2005). Menopause Related Sleep Disorders (link is external). Journal of Clinical Sleep Medicine; 1(3): 291–300.[↩][↩]
- Weber, M., Mapstone, M., Staskiewicz, J., Maki, P.M. (2012). Reconciling subjective memory complaints with objective memory performance in the menopausal transition. Menopause; 19: 735–741.[↩][↩]
- Gardener, H., Wright, C. B., Dong, C., Cheung, K., DeRosa, J., Nannery, M., … Sacco, R. L. (2016). Ideal Cardiovascular Health and Cognitive Aging in the Northern Manhattan Study. Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease, 5(3), e002731.[↩]
- Ertel, K.A., Glymour, M.M., Berkman, L.F. (2008). Effects of Social Integration on Preserving Memory Function in a Nationally Representative US Elderly Population. American Journal of Public Health; 98(7): 1215–1220.[↩]
- Roberts, H., Hickey, M. (2016). Managing the menopause: An update. Maturitas. 201;86:53-8.[↩]
- North American Menopause Society Position Statement. (2013). Management of symptomatic vulvovaginal atrophy: 2013 position statement of the North American Menopause Society. Menopause; 20: 888–902.[↩]
- https://www.accessdata.fda.gov/scripts/cder/ob/results_product.cfm?Appl_Type=N&Appl_No=203505[↩]



{kind=link}