Contents
What is premature atrial contraction
Premature atrial contractions also known as atrial premature complexes or atrial premature beats, are a common cardiac arrhythmia characterized by premature heartbeats originating in the atria. While the sinoatrial node typically regulates the heartbeat during normal sinus rhythm, premature atrial contractions occur when another region of the atria depolarizes before the sinoatrial node and thus triggers a premature heartbeat. Premature atrial contractions are observed frequently in normal subjects and patients with a variety of diseases. The exact cause of premature atrial contractions is unclear; while several predisposing conditions exist, premature atrial contractions commonly occur in healthy young and elderly people without heart disease, and by themselves are not considered an abnormal finding. Premature atrial contractions found in healthy young are more likely to lead to other heart conditions or even death. Elderly people that get premature atrial contractions usually don’t need any further attention besides follow ups due to unclear evidence. Premature atrial contractions are often completely asymptomatic and may be noted only with Holter monitoring, but occasionally they can be perceived as a skipped beat or a jolt in the chest. In most cases, no treatment other than reassurance is needed for premature atrial contractions, although medications such as beta blockers can reduce the frequency of symptomatic premature atrial contractions.
Premature atrial contractions are manifested as an interruption in the heart rhythm with a premature beat having a narrow QRS complex. Because the origin of the atrial impulse is ectopic, the appearance of the P wave is abnormal, denoting its abnormal early origin. There is quite a wide spectrum in the incidence and frequency of premature atrial contractions. Their nature is classified as follows: If the premature atrial contractions occur singly, they are classified according to their incidence per period of time. Therefore, an ambulatory ECG report commonly describes how many premature atrial contractions were observed in a given time, such as an hour, a minute, or 24 hours, according to how common they are. When premature atrial contractions are frequent, it is customary to further describe their nature (cyclic or noncyclic) and rate. For example, when premature atrial contractions occur cyclically, they may show a bigeminal pattern.
On an electrocardiogram (ECG), premature atrial contractions are characterized by an abnormally shaped P wave. Since the premature beat initiates outside the sinoatrial node, the associated P wave appears different from those seen in normal sinus rhythm (see Figures 1 and 2). Typically, the atrial impulse propagates normally through the atrioventricular node and into the cardiac ventricles, resulting in a normal, narrow QRS complex. However, if the atrial beat is premature enough, it may reach the atrioventricular node during its refractory period, in which case it will not be conducted to the ventricle and there will be no QRS complex following the P wave.
When you have single or occasional premature atrial contractions, there’s usually no need to seek medical treatment.
But if you have premature atrial contractions often or if they really bother you, see a doctor. Based on your symptoms, your doctor may order one or more of these tests:
Figure 1. Premature atrial contraction electrocardiogram (EKG) (as you can see, the cardiac cycle looks basically normal, sometimes the P wave is not the same shape as other P waves and these can be hard to pick out of a normal ECG. The identifying feature: The R-R interval between the premature atrial contraction and the preceeding beat is shorter than any of the other R-R intervals)
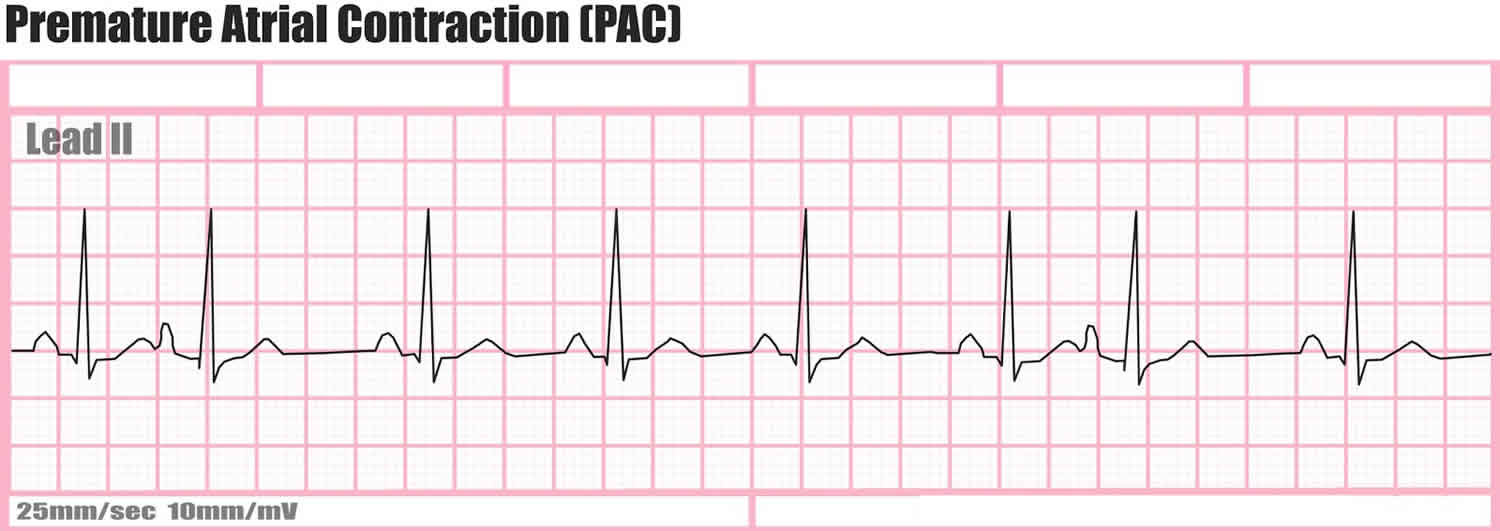
Footnote: A premature atrial contraction is characterized by:
- a normal progression from P to QRS to T wave
- the P wave may or may not look the same as other P waves in the recording (this is dependent on where the ectopic focus is in the atria)
- the PR interval is normal
- the RR interval between the PAC and the preceeding beat is shorter than normal.
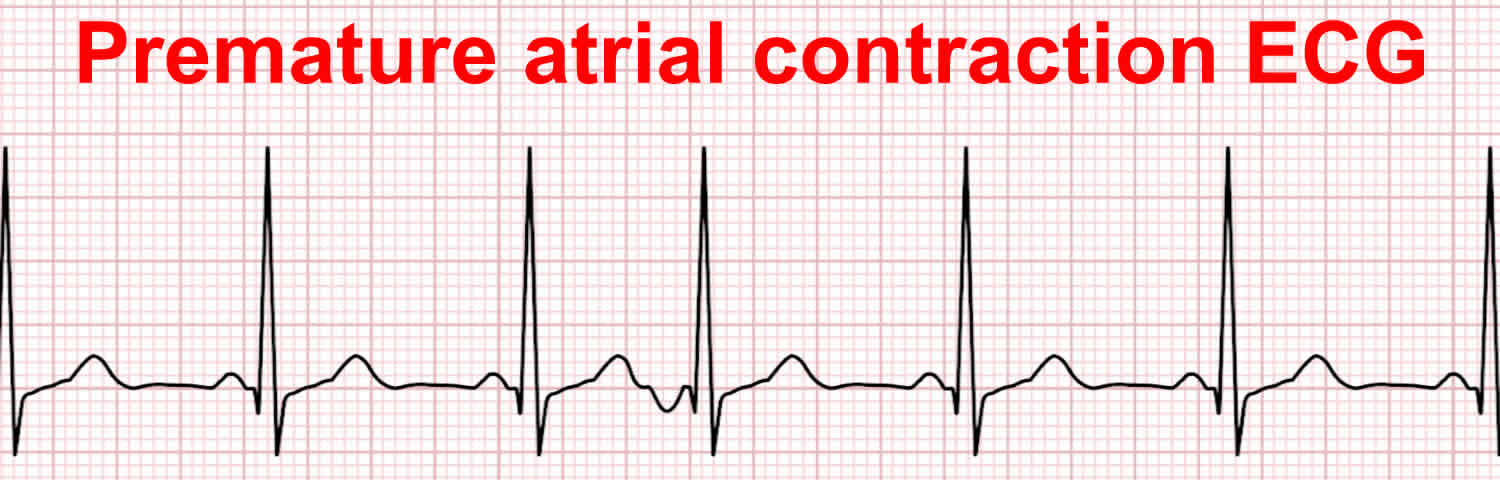
Figure 2. Premature atrial contraction ECG (with inverted P wave)
Premature atrial contraction causes
The exact cause of premature atrial contractions is unclear; premature atrial contractions commonly occur in healthy young and elderly people without heart disease, and by themselves are not considered an abnormal finding. However, patients with structural heart disease and coronary heart disease are at increased risk of premature atrial contraction.
These things can make premature atrial contractions more likely:
- Pregnancy
- High blood pressure, heart disease, or hyperthyroidism
- Stress, anxiety or nervousness
- Fatigue
- Caffeine
- Alcohol
- Smoking
- Recreational drugs
- Cold or hay fever medicine
- Asthma medicine
- Dehydration
Usually, premature atrial contractions have no clear cause and no health risks. In most cases, premature atrial contractions aren’t a sign of heart disease and just happen naturally.
But some people who have premature atrial contractions turn out to have related heart conditions, such as:
- Cardiomyopathy (a weakened heart muscle)
- Coronary heart disease (fatty deposits in your blood vessels)
If your doctor finds that you have a condition related to the premature heartbeats, you’ll work together to make a treatment plan.
Premature atrial contraction symptoms
When you have a premature atrial contraction, you might notice:
- A flutter in your chest
- Fatigue after exercise
- Shortness of breath or chest pain
- Lightheadedness or dizziness
Premature atrial contraction diagnosis
Electrocardiogram or EKG . This test will show if you have arrhythmia.
- Holter monitor. This is a portable version of an EKG that you’ll wear for 1 or 2 days. It tracks all the electric activity of your heart for your doctor to study.
- Exercise stress test. This test has you attached to an EKG while doing physical activity like running or walking on a treadmill or riding a stationary bike.
- Echocardiogram. This test uses sound waves to measure how well your heart valves and muscles work.
The presence of premature atrial contractions is diagnosed based upon either an EKG, Holter, or cardiac event monitor.
- By definition the P waves are premature.
- Morphology of the P’ wave is different than the P wave in normal sinus rhythm. If its origin is close to that of the sinus node, then the P’ morphology is hard to distinguish from the native sinus P wave.
- A premature atrial contraction differs from a premature junctional contraction in that the PR interval is > 0.12 second in a premature atrial contraction.
- The PR interval may be shorter than that in normal sinus rhythm if it is located closer to the AV node.
- The PR interval tends to lengthen when the coupling time to the premature atrial contraction is short.
- A premature atrial contraction may not be conducted to the ventricles and this is called a blocked premature atrial contraction.
- The differential diagnosis in this scenario includes second degree AV block. In second degree AV block, the PP intervals remain constant.
- Usually the QRS is of normal duration, but occasionally there is aberrant conduction, most frequently of right bundle branch block (RBBB) morphology.
- Aberrancy is more likely to occur when the coupling time is shorter.
- Usually there is no compensatory pause. The premature atrial contraction resets the sinus node.
- Most of these patients do not have organic heart disease.
- 64% of healthy subjects will have premature atrial contractions on 24 hour Holter monitoring
- Frequency higher in the elderly
- The QRS complex is normal.
- There is normal T wave repolarization (not inverted to the other T waves).
Premature atrial contraction treatment
If your test results show that you have other heart-related problems, your doctor will recommend a treatment plan for you. Most of the time, though, premature atrial contractions don’t need treatment.
Your doctor may recommend that you adopt the following lifelong heart-healthy lifestyle changes to help lower your risk for conditions such as high blood pressure and heart disease, which can lead to premature atrial contraction.
- Aiming for a healthy weight
- Being physically active
- Heart-healthy eating
- Managing stress
- Quitting smoking
- Lifestyle changes. Cut back on caffeine, and treat other health issues like sleep apnea and high blood pressure.
If you have severe symptoms or find them bothersome, treatments can include:
Medicines for arrhythmia. Take medications that are used to cut down on or end premature heartbeats.
Some medicines are used in combination with each other or together with a procedure or a pacemaker. If the dose is too high, medicines to treat arrhythmia can cause an irregular rhythm. This happens more often in women.
- Adenosine to slow a racing heart. Adenosine acts quickly to slow electrical signals. It can cause some chest pain, flushing, and shortness of breath, but any discomfort typically passes soon.
- Atropine to treat a slow heart rate. This medicine may cause difficulty swallowing.
- Beta blockers to treat high blood pressure or a fast heart rate or to prevent repeat episodes of arrhythmia. Beta blockers can cause digestive trouble, sleep problems, and sexual dysfunction and can make some conduction disorders worse.
- Blood thinners to reduce the risk of blood clots forming. This helps prevent stroke. With blood-thinning medicines, there is a risk of bleeding.
- Calcium channel blockers to slow a rapid heart rate or the speed at which signals travel. Typically, they are used to control arrhythmias of the upper chambers. In some cases, calcium channel blockers can trigger ventricular fibrillation. They can also cause digestive trouble, swollen feet, or low blood pressure.
- Digitalis, or digoxin, to treat a fast heart rate. This medicine can cause nausea and may trigger arrhythmias.
- Potassium channel blockers to slow the heart rate. They work by lengthening the time it takes for heart cells to recover after firing, so that they do not fire and squeeze as often. Potassium channel blockers can cause low blood pressure or another arrhythmia.
- Sodium channel blockers to block transmission of electrical signals, lengthen cell recovery periods, and make cells less excitable. However, these drugs can increase risks of sudden cardiac arrest in people who have heart disease.
Beta blockers may be prescribed to control your heart rate and rhythm.





{kind=link}