
Contents
What is proctalgia fugax
Proctalgia fugax is a medical term to describe the sensation of pain due to rectal muscle spasm. Proctalgia fugax causes episodes of sudden, severe anal pain that last for a few minutes at a time. Proctalgia fugax is a functional recurrent anorectal pain that is part of a spectrum of functional gastrointestinal disorders 1. A functional bowel disorder is diagnosed by characteristic symptoms for at least 12 weeks during the preceding 12 months in the absence of a structural or biochemical explanation 2. Functional gastrointestinal disorders are disorders of gut–brain interaction 3. Functional bowel disorder is a group of disorders classified by gastrointestinal symptoms related to any combination of the following: motility disturbance, visceral hypersensitivity, altered mucosal and immune function, altered gut microbiota, and altered central nervous system (CNS) processing 4.
The term “functional” is generally applied to disorders where the body’s normal activities in terms of the movement of the intestines, the sensitivity of the nerves of the intestines, or the way in which the brain controls some of these functions is impaired. However, there are no structural abnormalities that can be seen by endoscopy, x-ray, or blood tests. Thus it is identified by the characteristics of the symptoms and infrequently, when needed, limited tests.
Proctalgia fugax is defined by the Rome III diagnostic criteria as episodes of sharp fleeting pain that recur over weeks, are localized to the anus or lower rectum, and last from seconds to several minutes with no pain between episodes 5. There is no diurnal variation. There are numerous precipitants including sexual activity, stress, constipation, defecation and menstruation, although proctalgia fugax can occur without a trigger. Proctalgia fugax should be differentiated from chronic proctalgia, a functional anorectal pain disorder with a vague, dull ache or pressure sensation high in the rectum, often worse when sitting than when standing or lying down, and lasts at least 20 minutes 5.
The prevalence of proctalgia fugax in the general population may be as high as 8%–18% 6. Many patients present to primary health care physicians and often do not require further consultation because the symptoms are fleeting 7. This condition is more common among women than among men 7 and usually affects patients between 30 and 60 years of age 8.
Depending on the cause of your anal pain, there are some measures you can try at home to get relief. They include:
- Eating more fruits, vegetables and whole grains, exercising daily, and taking stool softeners, if needed, to facilitate bowel movements, reduce straining and ease pain
- Sitting in a tub of hot water up to your hips — known as a sitz bath — several times a day to ease the pain of hemorrhoids, anal fissures or rectal muscle spasms
- Applying over-the-counter hemorrhoid cream for hemorrhoids or hydrocortisone cream for anal fissures
- Taking an over-the-counter pain reliever such as acetaminophen (Tylenol, others), aspirin or ibuprofen (Advil, Motrin IB, others)
Seek immediate medical attention
Have someone drive you to urgent care or the emergency room if you develop:
- A significant amount of rectal bleeding or rectal bleeding that won’t stop, particularly if accompanied by lightheadedness, dizziness or feeling faint
- Anal pain that gets much worse, spreads, or is accompanied by fever, chills or anal discharge
Schedule a doctor’s visit
Make an appointment with your doctor if your pain lasts more than a few days and self-care remedies aren’t helping. Also make an appointment with your doctor if anal pain is accompanied by a change in bowel habit or rectal bleeding.
A hemorrhoid that develops quickly or is particularly painful may have formed a blood clot inside (thrombosed). Removing the clot within the first 48 hours often gives the most relief, so request a timely appointment with your doctor. The blood clot of a thrombosed hemorrhoid, although painful, can’t break loose and travel, so it won’t cause any of the complications — such as stroke — associated with blood clots that form in other parts of the body.
Proctalgia fugax causes
Although the cause of proctalgia fugax is unclear, spasm of the anal sphincter is commonly implicated 9. The condition may be more likely to occur after sclerotherapy for hemorrhoids and vaginal hysterectomy. There are also associations with other functional pathologies, such as irritable bowel syndrome and anxiety 9.
Other causes of anorectal pain (e.g., hemorrhoids, cryptitis, ischemia, abscess, fissure, rectocele and malignant disease) must be excluded before the diagnosis of proctalgia fugax can be made 10.
Other causes of anal pain include:
- Anal cancer
- Anal fissure (a small tear in the lining of the anal canal)
- Anal itching (pruritus ani)
- Anal sex
- Anorectal fistula (an abnormal channel between the anus or rectum usually to the skin near the anus)
- Coccydynia or coccygodynia (tailbone pain)
- Constipation
- Crohn’s disease
- Diarrhea causing anal irritation
- Fecal impaction (a mass of hardened stool in the rectum due to chronic constipation)
- Hemorrhoids (swollen and inflamed veins in your anus or rectum)
- Levator ani syndrome (spasm in the muscles that surround the anus)
- Perianal abscess (pus in the deep tissue around the anus)
- Perianal hematoma (a collection of blood in the perianal tissue caused by a ruptured vein, sometimes called an external hemorrhoid)
- Proctitis (inflammation of the lining of the rectum)
- Solitary rectal ulcer syndrome (ulcer of the rectum)
- Thrombosed hemorrhoid (blood clot in a hemorrhoid)
- Trauma
- Ulcerative colitis (a type of inflammatory bowel disease)
- Ulcerative proctitis (a type of inflammatory bowel disease)
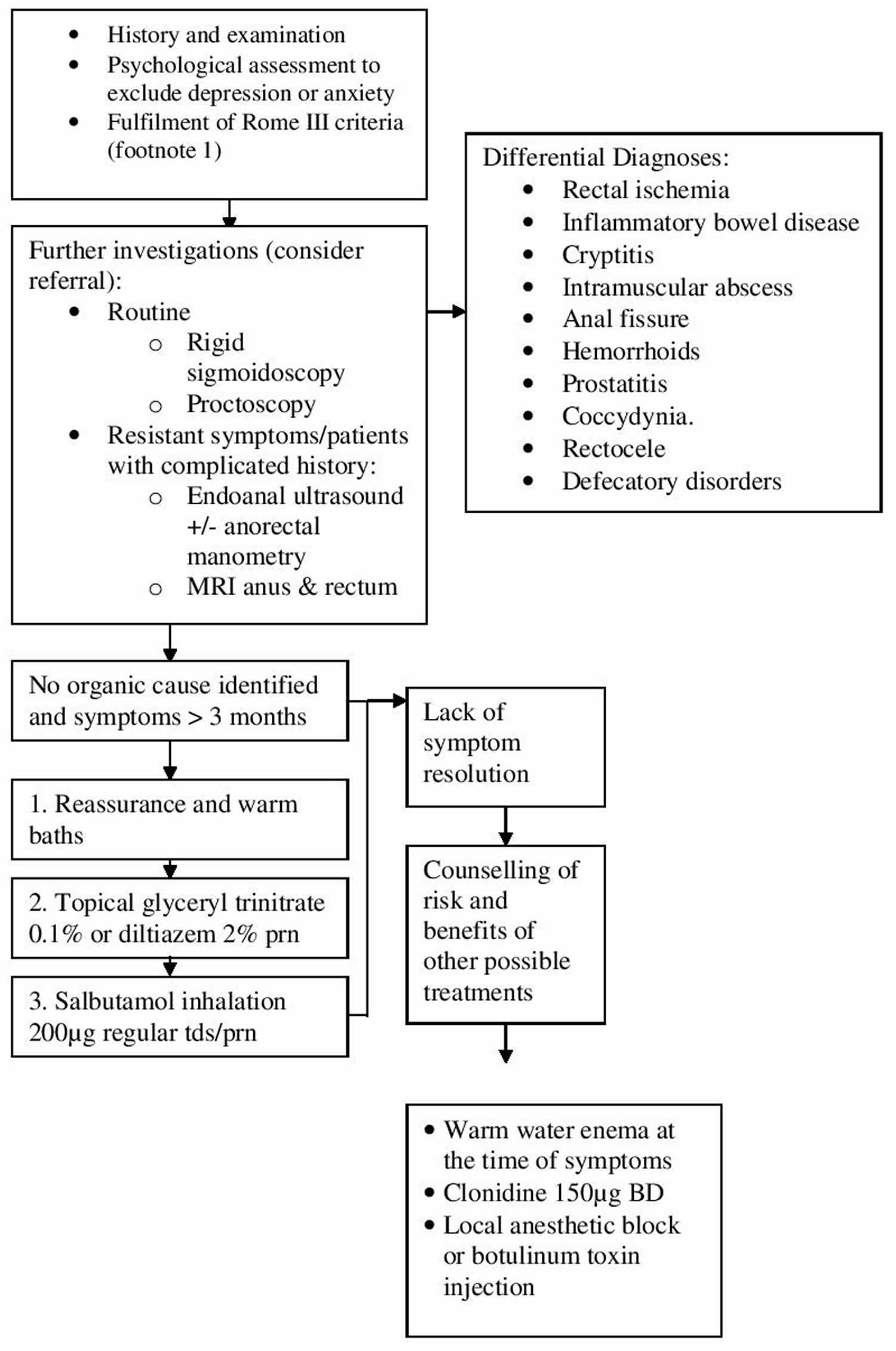
Figure 1. Proctalgia fugax diagnostic pathway
Proctalgia fugax symptoms
Rome III criteria for proctalgia fugax 12:
- Recurrent episodes of pain localized to the anus or lower rectum
- Episodes last from seconds to minutes
- There is no anorectal pain between episodes.
Proctalgia fugax treatment
Most treatments for proctalgia fugax (e.g., oral diltiazem, topical glyceryl nitrate, nerve blocks) act by relaxing the anal sphincter spasm, but the effectiveness of these treatments are supported only by case reports or case series, with the exception of a single randomized controlled trial of salbutamol 13, making the value of most treatment options, including salbutamol, difficult to judge 11.
Summary of recommended treatment modalities for proctalgia fugax 11:
- Tap/hot water enema – there is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial 14
- Hot baths – there is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial 15
- Oral diltiazem – there is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial 16
- Glyceryl trinitrate (nitroglycerin) – there is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial 17
- Clonidine – there is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits 18
- Botulinum toxin injection – there is high certainty that the net benefit is substantial 19
- Salbutamol inhalation – there is high certainty that the net benefit is substantial 20
- Pudendal nerve block – there is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits 21
- Superior hypogastric plexus block – there is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits 22
- Proctalgia fugax. CMAJ. 2013 Mar 19; 185(5): 417. doi: 10.1503/cmaj.101613 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3602260/[↩]
- Thompson WG, Longstreth GF, Drossman DA, et al. Functional bowel disorders and functional abdominal pain. Gut 1999;45:II43-II47.[↩]
- Functional GI Disorders. https://www.iffgd.org/gi-disorders/functional-gi-disorders.html[↩]
- Drossman DA, et al. Rome IV, the functional gastrointestinal disorders. Gastroenterology 2016;150:1262–1279.[↩]
- Functional anorectal disorders. Bharucha AE, Wald A, Enck P, Rao S. Gastroenterology. 2006 Apr; 130(5):1510-8.[↩][↩]
- Whitehead WE, Wald A, Diamant NE, et al. Functional disorders of the anus and rectum. Gut 1999; 45(Suppl 2):II55–9[↩]
- Boyce PM, Talley NJ, Burke C, et al. Epidemiology of the functional gastrointestinal disorders diagnosed according to Rome II criteria: an Australian population-based study. Intern Med J 2006; 36:28–36[↩][↩]
- Bharucha AE, Trabuco E. Functional and chronic anorectal and pelvic pain disorders. Gastroenterol Clin North Am 2008;37:685–96[↩]
- Jeyarajah S, Chow A, Ziprin P, et al. Proctalgia fugax, an evidence-based management pathway. Int J Colorectal Dis 2010;25:1037–46[↩][↩]
- Wesselmann U, Burnett AL, Heinberg LJ. The urogenital and rectal pain syndromes. Pain 1997;73: 269–94[↩]
- Jeyarajah S, Purkayastha S. Proctalgia fugax. CMAJ. 2013;185(5):417. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3602260/[↩][↩][↩]
- Bharucha AE, Wald A, Enck P, Rao S. Functional anorectal disorders. Gastroenterology. 2006 Apr;130(5):1510-8.[↩]
- Eckardt VF, Dodt O, Kanzler G, et al. Treatment of proctalgia fugax with salbutamol inhalation. Am J Gastroenterol 1996;91:686–9[↩]
- Olsen B. Proctalgia fugax–a nightmare drowned in enema. Colorectal Dis. 2008 Jun;10(5):522-3.[↩]
- Potter MA, Bartolo DC. Proctalgia fugax. Eur J Gastroenterol Hepatol. 2001 Nov;13(11):1289-90.[↩]
- Boquet J, Moore N, Lhuintre JP, Boismare F. Diltiazem for proctalgia fugax. Lancet. 1986 Jun 28;1(8496):1493.[↩]
- Lowenstein B, Cataldo PA. Treatment of proctalgia fugax with topical nitroglycerin: report of a case. Dis Colon Rectum. 1998 May;41(5):667-8.[↩]
- Swain R. Oral clonidine for proctalgia fugax. Gut. 1987 Aug;28(8):1039-40.[↩]
- Sanchez Romero AM, Arroyo Sebastian A, Perez Vicente FA, Serrano Paz P, Candela Polo F, Calpena Rico R. [Treatment of proctalgia fugax with botulinum toxin: results in 5 patients]. Rev Clin Esp. 2006 Mar;206(3):137-40.[↩]
- Eckardt VF, Dodt O, Kanzler G, Bernhard G. Treatment of proctalgia fugax with salbutamol inhalation. Am J Gastroenterol. 1996 Apr;91(4):686-9.[↩]
- Bascom JU. Pudendal canal syndrome and proctalgia fugax: a mechanism creating pain. Dis Colon Rectum. 1998 Mar;41(3):406.[↩]
- Waldman SD, Wilson WL, Kreps RD. Superior hypogastric plexus block using a single needle and computed tomography guidance: description of a modified technique. Reg Anesth. 1991 Sep-Oct;16(5):286-7.[↩]





{kind=link}