Contents
What is pterygium
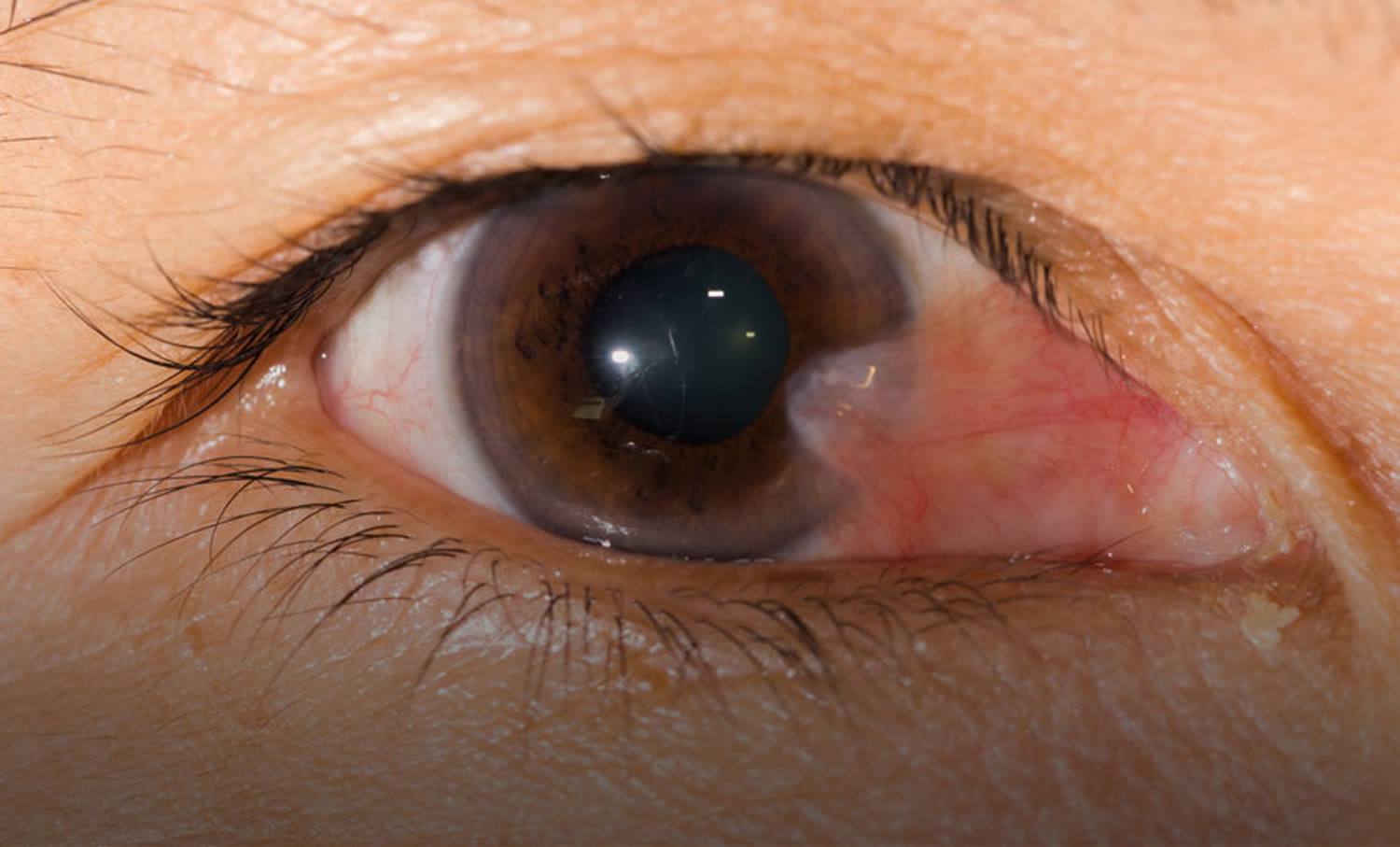
A pterygium is also known as Surfer’s Eye, is a benign (non-cancerous) growth that starts in the clear, thin tissue (conjunctiva) of the eye. This growth covers the white part of the eye (sclera) and extends onto the cornea. A pterygium is often slightly raised and contains visible blood vessels. A pterygium may occur in one or both eyes and it’s more common in people between 20 and 40 years. Men are usually more likely to develop a pterygium than women. When extensive, pterygium can result in corneal astigmatism or occlusion of the visual axis.
A pterygium is a visible growth on the superficial corneal layers on the surface of the eye. It typically emerges as a triangular,fibrovascular tissue growth from the corner of the eye, with a pink and fleshy appearance. A pterygium is your body’s way of trying to protect your eye from intense environments, such as high levels of sunlight, dust, sand or wind. Surfers are one group of people who are prone to developing pterygium, which is also known as Surfer’s Eye. Other at-risk groups include farmers, welders and people living in sunnier areas.
In general, pterygia (plural) are not dangerous. During the early stages of pterygium development, the main concern is cosmetic – they change the eye’s appearance – but there is no effect on vision. Symptoms in the early stages may include irritation, itching or burning. These can generally be managed with eye drops. Avoid further exposure to sunlight and wind to reduce the stimulus for it to grow larger. A small pterygium that has stopped growing is relatively harmless and may not need any further treatment.
However, in some cases, the pterygium may continue growing across the eye and either directly block vision or distort the shape of the cornea and cause blurred vision (astigmatism). In these cases, surgery is recommended. Surgery is also an option if you are worried about the cosmetic appearance of your eye.
Importantly, pterygia are not cancerous – they are benign growths. That means that while they may grow locally (and possibly affect your sight), they won’t spread to other parts of your body. Nevertheless, it’s important that you have an ophthalmologist evaluate any growth on your eye to rule out more serious conditions, such as a conjunctival or iris tumour.
And while pterygia themselves are not cancerous, new findings published by Australian researchers 1 suggest that people who have a pterygium are nearly 25% more likely to develop malignant melanoma – a fatal form of skin cancer. Tell your doctor or dermatologist if you have (or have had) a pterygium, make sure that you protect your skin from the sun/UV exposure (i.e. sunscreen, long-sleeved tops, shade) and always have regular skin checks.
A number of potential therapeutic options exist for the management of pterygium ranging from conservative management with lubrication to surgical excision with conjunctival autografts. Due to the potential for recurrence of a more aggressive lesion, as well as other surgical risks, the surgical removal of pterygium should not be undertaken casually. Using modern micro-surgical techniques, the surgeon will carefully remove the pterygium and replace it with a graft of healthy tissue taken from the same eye, which is fixed into place. There is a chance that the condition may recur following surgery, but the process of grafting helps to prevent this.
Inflamed pterygium may cause irritation, foreign body sensation, and tearing which, in many cases, can be alleviated with over the counter vasoconstrictor drops, lubricating drops and ointments.
Figure 1. Pterygium eye
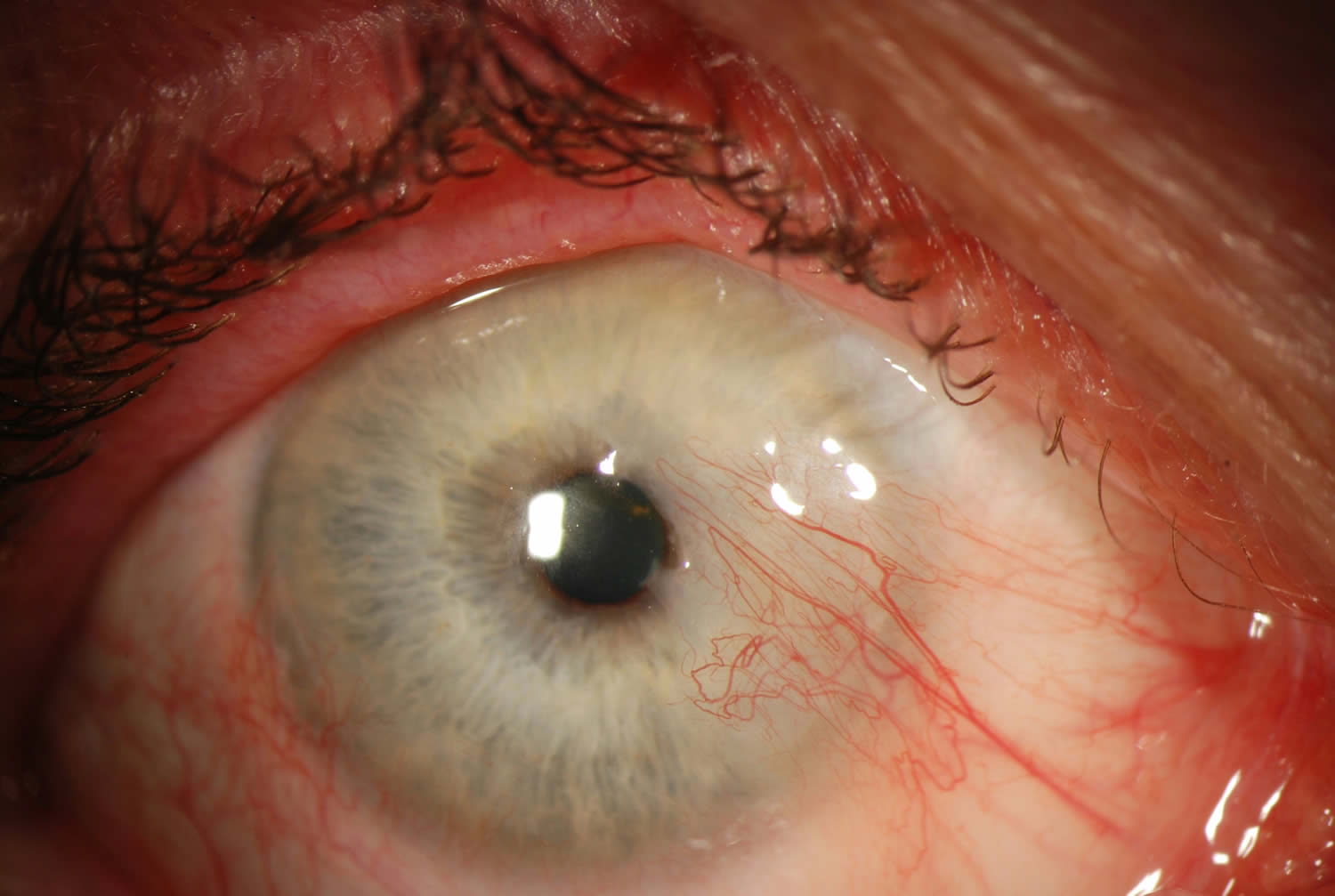
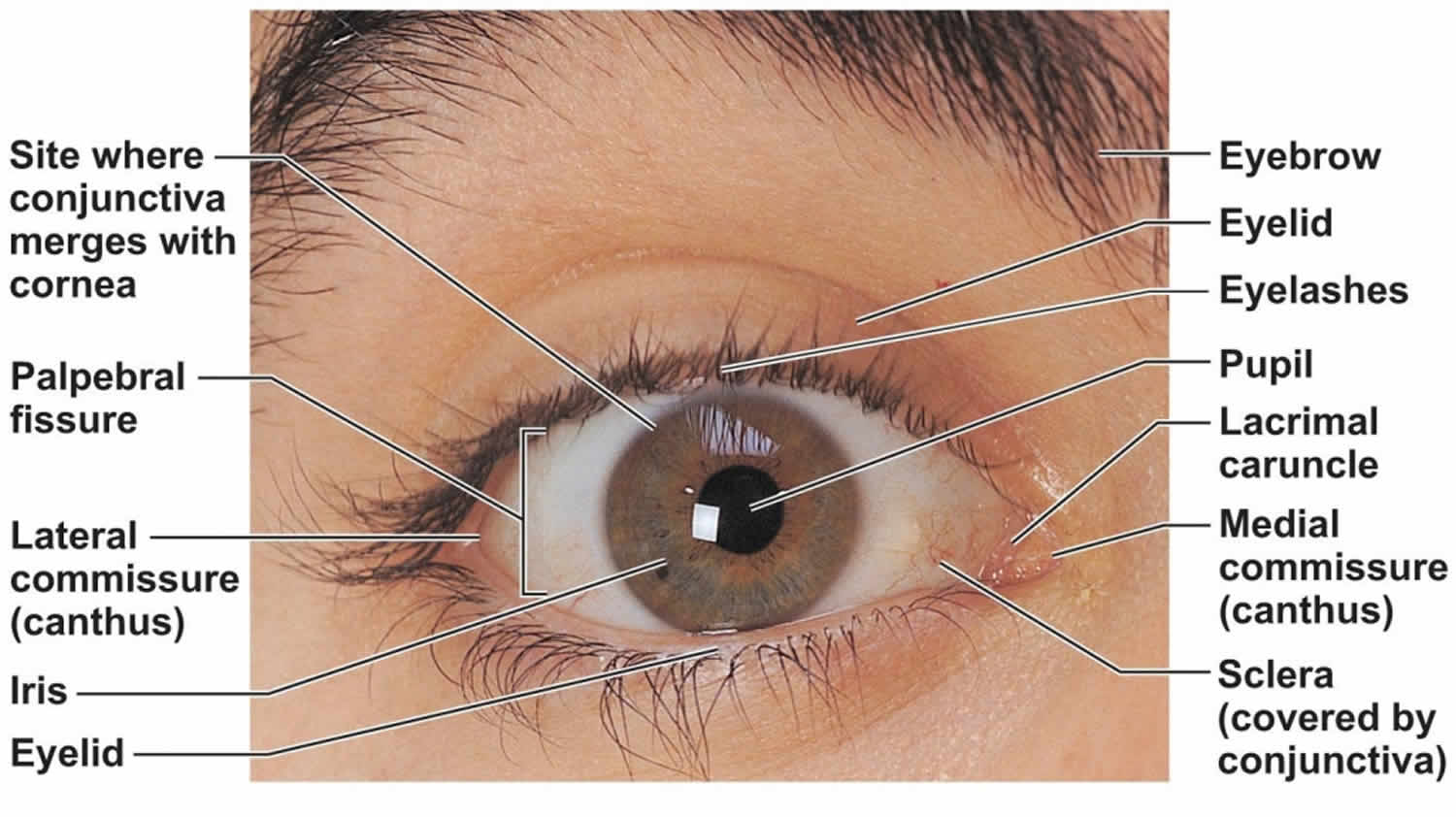
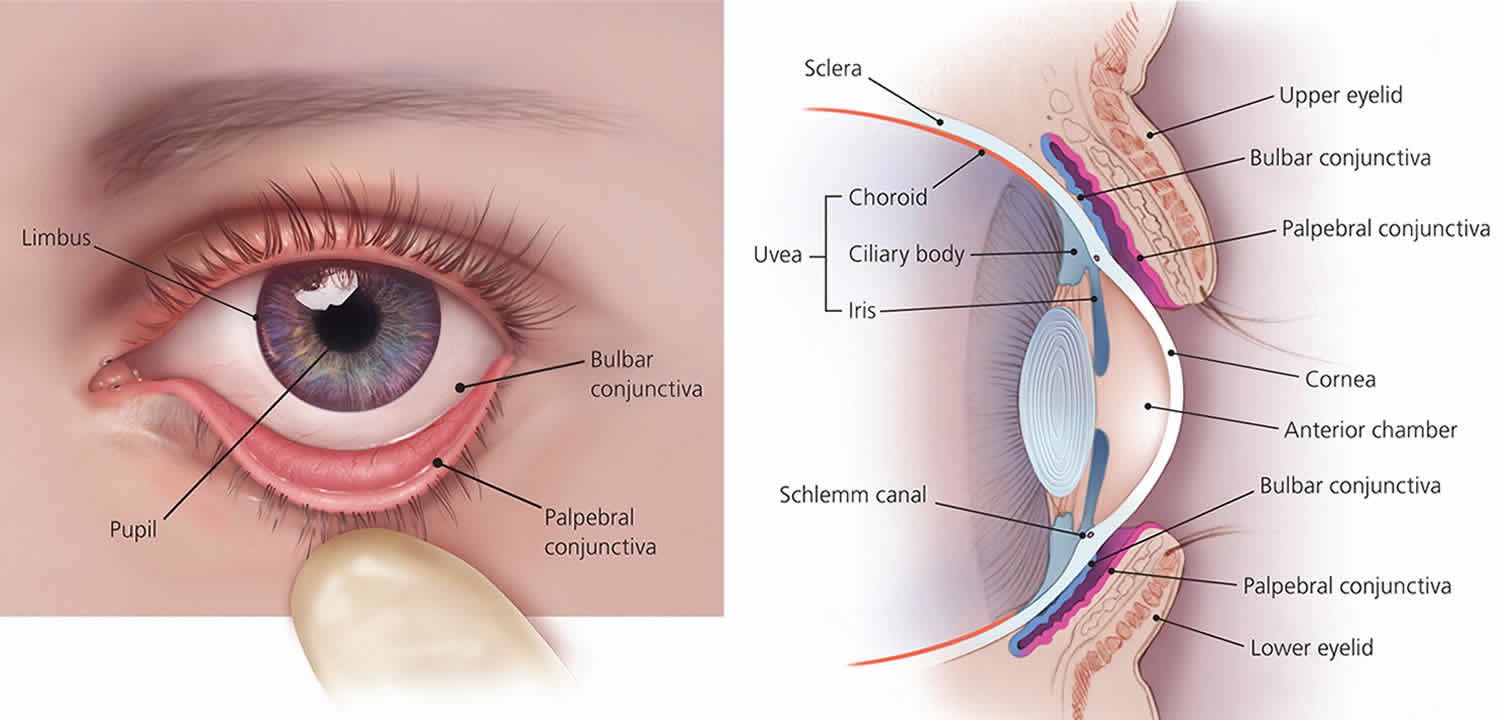
Figure 2. Human eye anatomy
Is pterygium cancerous?
No, a pterygium is a benign growth and usually harmless. However, in some cases it may harbor cancerous cells.
Histologically, pterygia are an accumulation of degenerated subepithelial tissue which is basophilic with a characteristic slate gray appearance on H&E staining. Vermiform or elastotic degeneration refers to the wavy worm-like appearance of the degenerate fibers. Destruction of Bowman’s layer by fibrovascular ingrowth is typical. The overlying epithelium is usually normal, but may be acanthotic, hyperkeratotic, or even dysplastic and often exhibits areas of goblet cell hyperplasia 2.
Pterygium causes
It is not known exactly what causes a pterygium to develop, but dusty, sandy and sunny environments (with high UV exposure) are contributing factors. An increased incidence is noted in latitudes nearer the equator and in individuals with a history of increased UV exposure. Some studies have shown a slightly higher incidence in males than females, which may only reflect a higher rate of UV radiation.
The increased prevalence in hot dry climates and regions nearer to the equator suggest a role of environmental factors such as UV radiation and dryness. Actinic changes seen on histopathology similar to actinic keratoses on the skin also supports the role of UV radiation. It has been suggested that radiation activated fibroblasts may result in excessive production of material resulting in pterygia. Other proposed theories include choline deficiency, an inflammatory disorder, disregulation of angiogenesis, immune system abnormalities, tear film abnormalities, as well as the possible role of a viral stimulus.
Recurrent pterygia appear to be more related to surgical trauma than UV radiation as avoidance of UV radiation has not been shown to affect the incidence of recurrence. The actinic damage noted histologically on primary pterygia is characteristically absent from recurrent pterygia, supporting this theory.
Risk factors for developing pterygium
UV radiation, proximity to the equator, dry climates, outdoor lifestyle.
Pterygium prevention
As UV radiation is believed to play an important role in the pathophysiology, avoidance of UV exposure is probably important to primary prevention. Ocular surface lubrication may also help.
- When outdoors, wear good-quality, wrap-around sunglasses as recommended by an optometrist. Choose sunglasses that meet the American Standard and have an Eye Protection Factor (EPF) UV rating of either 9 or 10. The single most important thing to look for when buying sunglasses to protect your eyes is a sticker or tag indicating that they block 100 percent of UV rays. Less expensive pairs marked as 100 percent UV-blocking can be just as effective as pricier options.
- The more coverage from sunglasses, the less sun damage inflicted on the eyes. Consider buying oversized glasses or wraparound-style glasses, which help cut down on UV entering the eye from the side.
- Polarization reduces glare coming off reflective surfaces like water or pavement. This does not offer more protection from the sun, but can make activities like driving or being on the water safer or more enjoyable.
- Surfers and others involved in water sports should always wear sunglasses during these activities.
- A wide-brimmed hat will also protect your eyes from sun and wind exposure.
- Keep your eyes protected in dry, dusty conditions with wraparound glasses, goggles or other protective eyewear.
- Lubricate your eyes as often as possible in dry conditions by using artificial tears.
Pterygium symptoms
A pterygium can go unnoticed for many years, or it may be dismissed as a general irritation of the eye. As pterygium progresses, it can start to spread across the cornea. A pterygium can become inflamed and cause ocular surface irritation. Many patients will disclose their dislike of the appearance of the pterygium when questioned directly. As the lesion progresses vision may be affected by induction of astigmatism or obscuration of the visual axis.
Common symptoms include:
- Localized redness
- Irritation
- Itching
- Foreign-body sensation
- Corneal scarring
Some people with a pterygium may find it difficult to wear contact lenses, while others dislike the look of the growth on their eye and may seek surgical treatment to have it removed.
Pterygium diagnosis
The diagnosis is made by slit-lamp examination of the typical limbal growth at the characteristic location within the palpebral fissure. The diagnosis is most often clear clinically, but histopathologic confirmation is performed routinely.
The diagnosis of pterygium is based on the clinical appearance of the lesion. Typical findings include:
- Fibrovascular conjunctival growth within the palpebral fissure extending onto the corneal surface
- Triangular shape with the apex, or head, extending onto the cornea
- Vascular straightening in the direction of the advancing head of the pterygium on the corneal surface.
- May be a thin translucent membrane or significantly thickened with an elevated mound of gelatinous material.
- It may affect the nasal and temporal limbus of both eyes or only a single location.
- Raised lesion, white to pink in color depending on vascularity
- Ranges from a fine transparent area with very mild elevation, few vessels, and minimal corneal involvement in the early stages to a thick opaque vascular growth extending to the visual axis in later stages
- Pinguecula are often present in the ipsilateral or contralateral eye
- A pigmented epithelial iron line (Stocker’s line) adjacent to a pterygium is evidence of chronicity.
It is unusual for pterygia to deviate from the characteristic locations of three and nine o’clock within the palpebral fissure. Pterygioid lesions in other locations should elevate suspicion for alternate diagnoses.
A complete eye exam should be performed on all patients with apparent pterygia focusing on assessment of visual and refractive impact as well as the exclusion of less common alternate diagnoses.
- Visual acuity with current correction and manifest refraction
- External examination (lids, lashes, lacrimal apparatus)
- Examination of bulbar and palpebral conjunctiva as well as fornices
- Slit lamp biomicroscopy of the ocular surface and anterior segment
- Keratometry
- Corneal Topography
- Motility Exam
- The remainder of a comprehensive eye exam to include pupil exam, visual fields, intraocular pressure, and dilated funduscopic exam
Pterygium treatment
Initially, the corneal extension of the pterygium should be measured and followed every 1 to 2 years to determine the rate of growth toward the visual axis. In many cases, simple eye drops can be used to treat symptoms, such as inflammation, mild pain, itching or a feeling of having grit in the eye. Treatment for a minor irritation includes eye drops or ointments that help to lubricate and soothe the cornea. For severe inflammation, you may be prescribed a short course of steroid eye drops. These medications only ease the symptoms and are not a cure.
Pterygium surgery
If the pterygium growth is significant and continues to spread across the cornea or causes other problems, surgery is usually recommended to eliminate associated symptoms and avoid adverse effects on vision. Some people choose to have surgery for cosmetic reasons.
Excision: simple excision or simple conjunctival closure will result in a recurrence rate as high as 80% and is now considered unacceptable.
Excision together with adjunctive therapies such as radiotherapy, mitomycin and 5FU: the use of these adjunctive agents will reduce the 80% recurrence of simple excision to about 10% but bring with them some visually threatening complications. The only real advantage of these methods is the simplicity and speed of the surgery.
Conjunctival Flap/Graft : this is considered the Gold Standard of care and carries an approximate rate of recurrence of 5-10% with minimal complications. However, it is a lengthier procedure and technically slightly more complicated than those methods above. Recently a major modification of a routine autograft, known as P.E.R.F.E.C.T. for PTERYGIUM, has reduced the recurrence rate to 1/1000 and results in a cosmetic result where the appearance of the eye after this procedure is indistinguishable from that of a normal eye.
Pterygium surgical follow up
Intensive postoperative topical steroids may be required. Patients need to be followed for one year if a recurrence is to be identified. 97% of all recurrences occur in the first year after surgery.
Pterygium complications
- Recurrence
- Corneal scarring
- Corneal perforation
- Strabismus
- Non-healing epithelial defect (esp with mitomycin C)
- Scleral melt (esp with mitomycin C)
Pterygium prognosis
Recurrence rate can be as low as 1/1000 with complications being very uncommon.





{kind=link}