Contents
What is quadriplegia
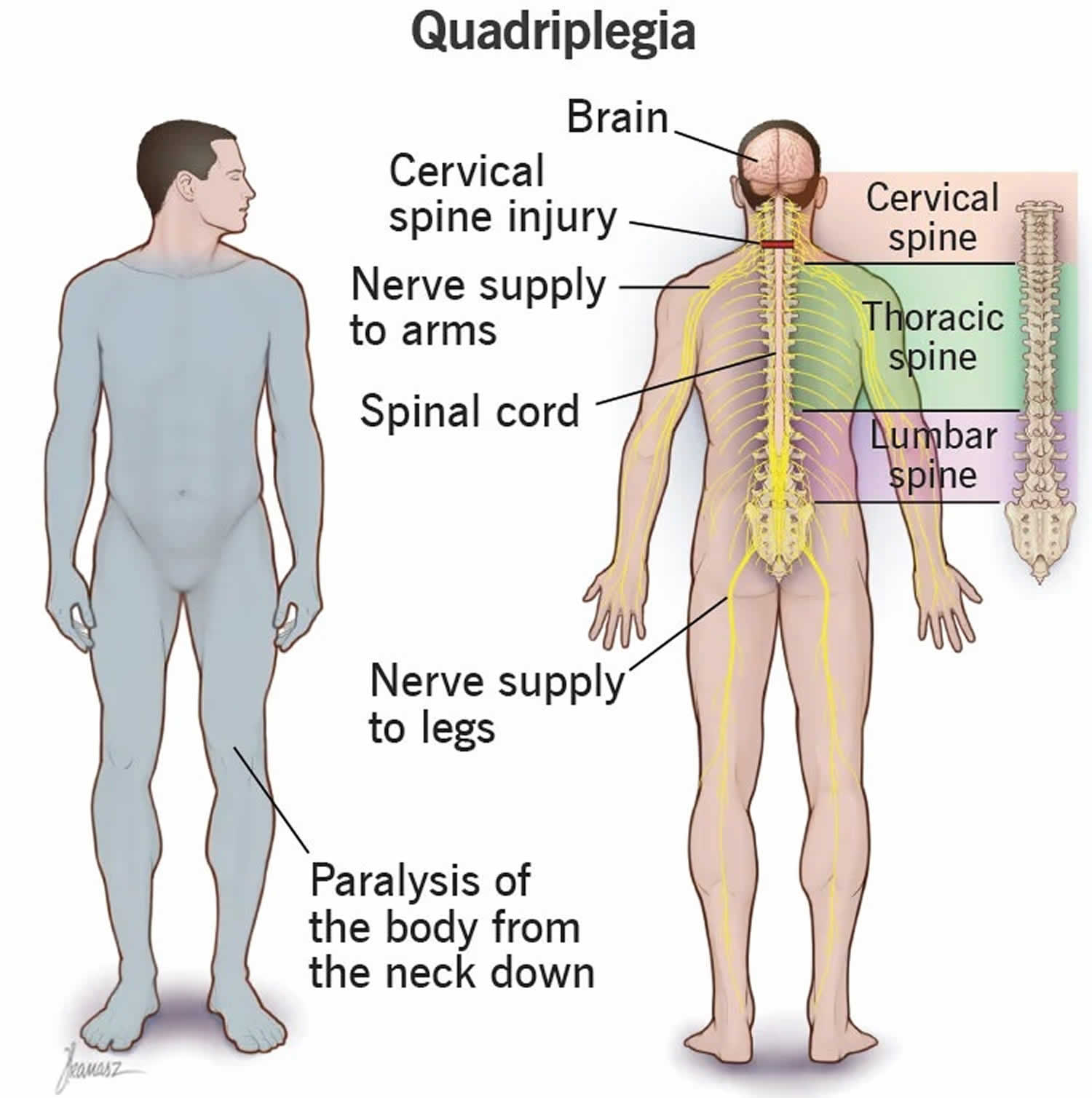
Quadriplegia also known as tetraplegia means paralysis below your neck that affects your arms, hands, trunk, legs and pelvic organs are all affected by your spinal cord injury. “Quadri” is Latin word for “four” and “Tetra” is Greek for “four” and “plegia” in Greek means “paralysis”. Quadriplegia refers to impairment or loss of motor (total or partial paralysis) and/or sensory function in the cervical segments of the spinal cord due to damage of neural elements within the spinal canal 1. Quadriplegia can happen when there’s a complete or incomplete spinal cord injury anywhere between cervical spine C1 to T1 (Figures 1 to 3). The higher the injury, the more dangerous the effects. A spinal cord injury is damage to the tight bundle of cells and nerves that sends and receives signals from your brain to and from the rest of your body. The spinal cord extends from the lower part of your brain down through the lower back (Figure 1). The spinal cord does not have to be severed in order for a loss of function to occur. It can be bruised, stretched, or crushed. Tetraplegia results in impairment of function in the arms as well as typically in the trunk, legs, and pelvic organs (i.e., including your arms and legs). Brain damage (e.g., cerebral palsy, stroke) or spinal cord damage (e.g., motor vehicle accidents, falls, shallow diving, acts of violence, and sports injuries) causes quadriplegia and usually occurs when there is damage to the spinal cord in the cervical region of the vertebral column. Nerve fiber injury degree is also a determinant of complete or partial damage to the spinal cord. If an injury is incomplete, sensational and movement abnormalities may result, but permanent paralysis occurs if the injury is complete. What this means is that there is total discontinuation of flow of information. Quadriplegia does not include brachial plexus lesions or injury to peripheral nerves outside the neural canal 1.
Your spinal cord is a bundle of nerves and other tissue which extends from your brain at the top of your neck down the length of your back. It’s protected by the bones or vertebrae that make up the spine, and by spinal fluid (Figure 1). Your brain and spinal cord are vital for controlling your bodily functions. The spinal cord is responsible for communicating two-way messages to and from the brain to all parts of the body – your muscles, organs and your skin. You are able to feel pain and move your arms or legs because of these messages or impulses. If you spinal cord is damaged or injured, some of the messages or impulses may be ‘interrupted’. This can lead to partial or total loss of feeling or movement in parts of your body – including your limbs and your internal organs.
Your ability to control your arms and legs after a spinal cord injury depends on two factors 2:
- Where the injury occurred on your spinal cord and
- The severity of the spinal cord injury.
The lowest part of your spinal cord that remains undamaged after an injury is referred to as the neurological level of injury (NLI) 1. The neurological level of injury (NLI) refers to the lowest segment of your spinal cord with normal sensory and antigravity motor function on both sides of your body, provided that there is normal (intact) sensory and motor function rostrally. The segments at which normal function is found often differ by side of the body and in terms of sensory and motor testing. Therefore, up to four different segments may be identified in determining the neurological level, i.e., Right-sensory, Left-sensory, Right-motor, Left-motor.
The severity of the spinal cord injury is often called “the completeness” and is classified as either of the following:
- Complete injury: If all feeling (sensory) and all ability to control movement (motor function) are lost below the spinal cord injury, your injury is called complete.
- Incomplete injury: If you have some motor or sensory function below the neurological level, your injury is called incomplete. There are varying degrees of incomplete injury.
There are also two main ways that quadriplegia can happen 3:
- Incomplete quadriplegia. This means that the quadriplegia blocks some — but not all — signals from getting through. That means a person might still have some ability to move, feel sensations or control automatic body processes (such as bowel and bladder function). This happens with about one-third of traumatic spinal cord injuries.
- Complete quadriplegia. This means whatever causes the quadriplegia blocks all signals from getting through. That means a person loses muscle control, the ability to feel sensations and their brain can’t manage any automatic processes that rely on brain signaling to work. This happens with about 20% of spinal cord injuries.
There are also two main ways that paralyzed muscles act in quadriplegia 3:
- Flaccid quadriplegia: This means that muscles don’t work at all and remain flaccid or limp.
- Spastic quadriplegia: This type of quadriplegia results in muscles that don’t work by themselves and contract uncontrollably.
Spinal cord injuries can cause one or more of the following signs and symptoms 2:
- Loss of movement
- Loss of or altered sensation, including the ability to feel heat, cold and touch
- Loss of bowel or bladder control
- Exaggerated reflex activities or spasms
- Changes in sexual function, sexual sensitivity and fertility
- Pain or an intense stinging sensation caused by damage to the nerve fibers in your spinal cord
- Difficulty breathing, coughing or clearing secretions from your lungs
Emergency signs and symptoms of a spinal cord injury after an accident include 2:
- Extreme back pain or pressure in your neck, head or back
- Weakness, incoordination or paralysis in any part of your body
- Numbness, tingling or loss of sensation in your hands, fingers, feet or toes
- Loss of bladder or bowel control
- Difficulty with balance and walking
- Impaired breathing after injury
- An oddly positioned or twisted neck or back
A medical doctor should ALWAYS examine and treat quadriplegia.
Depending on how and why it happens, quadriplegia is often permanent (no cure). Modern treatments and medical advances such as prostheses and medications can offer some hope of recovery, but these vary widely from case to case. Spinal cord injury treatment focuses on preventing further injury and empowering people with a spinal cord injury to return to an active and productive life. For those who face long-term or permanent effects, many assistive technologies and devices are now available, which can help those individuals with quadriplegia adapt and live more comfortably.
Figure 1. Spinal cord anatomy
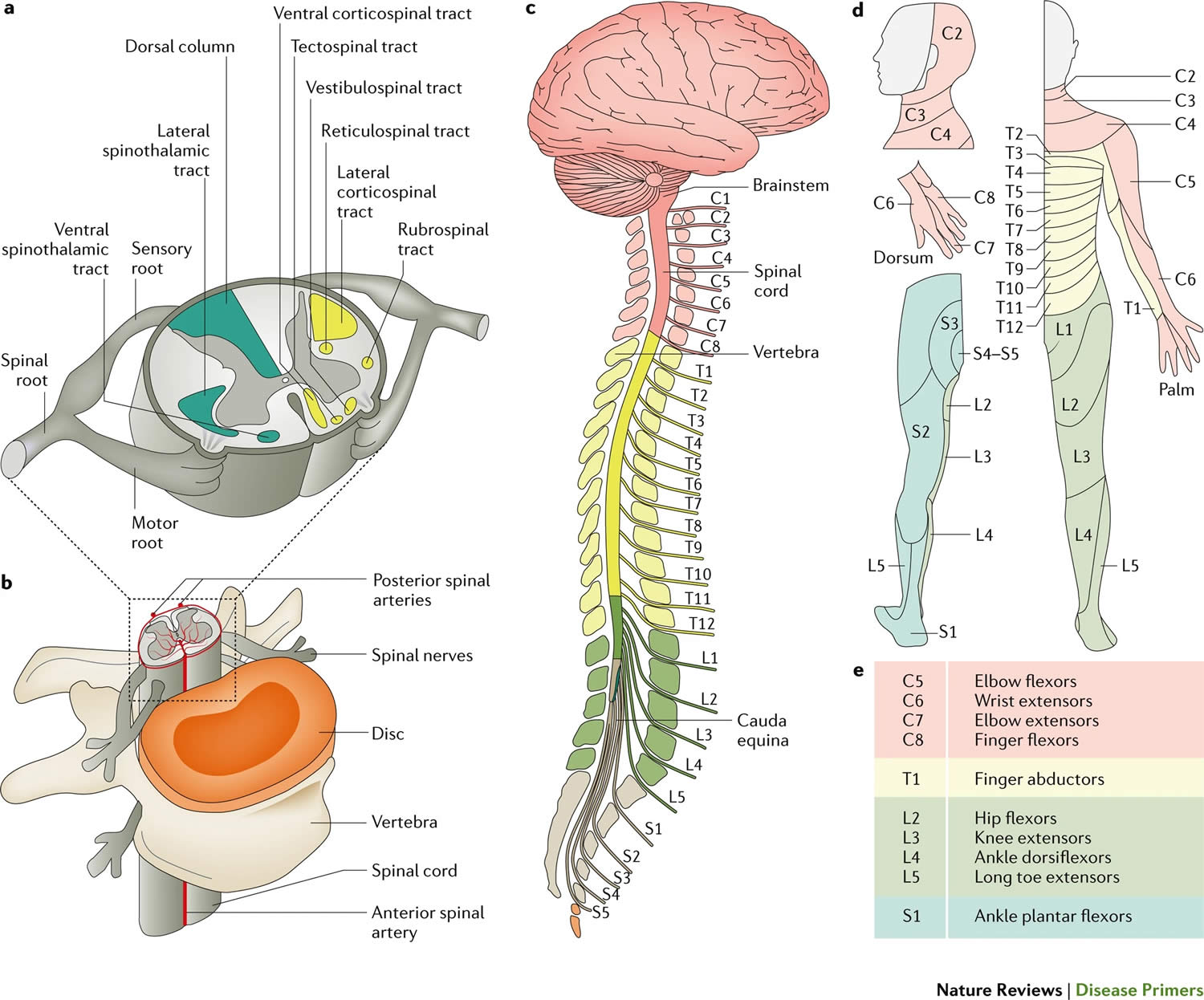
Footnotes: (a) The spinal cord itself is organized into grey matter (which contains neuronal cell bodies) and white matter (which contains myelinated axons). The white matter can be further subdivided into several ascending or descending tracts, which are composed of bundles of axons that originate from and project to specific regions in the brain and periphery. These tracts transmit specific information, such as sensory information (for example, temperature or itch) or motor information. Spinal nerve roots enter the spinal cord and either convey sensory information to the spinal cord (through the sensory or dorsal root) or convey motor information to the periphery (through the motor or ventral root). (b) The vertebral column encircles the spinal cord in protective bone and ligament, which, in humans, is segmented into 7 cervical, 12 thoracic, 5 lumbar and 5 sacral vertebrae. Blood is supplied to the spinal cord by the spinal arteries, which are located anteriorly and posteriorly and branch to perfuse the spinal cord parenchyma. The spinal cord is also surrounded by a protective layer of cerebrospinal fluid contained within the pachymeninges. (c–e) Each segmental region of the spinal cord (part c) innervates a specific region of the skin (part d), muscle (part e) or organ group. Damage to the spinal cord can result in partial or complete loss of function below the level of the injury. Note that part e describes the ‘key muscles’ as described in the International Standards for Neurological Classification of Spinal Cord Injury.
[Source 4 ]Figure 2. Spinal cord injury
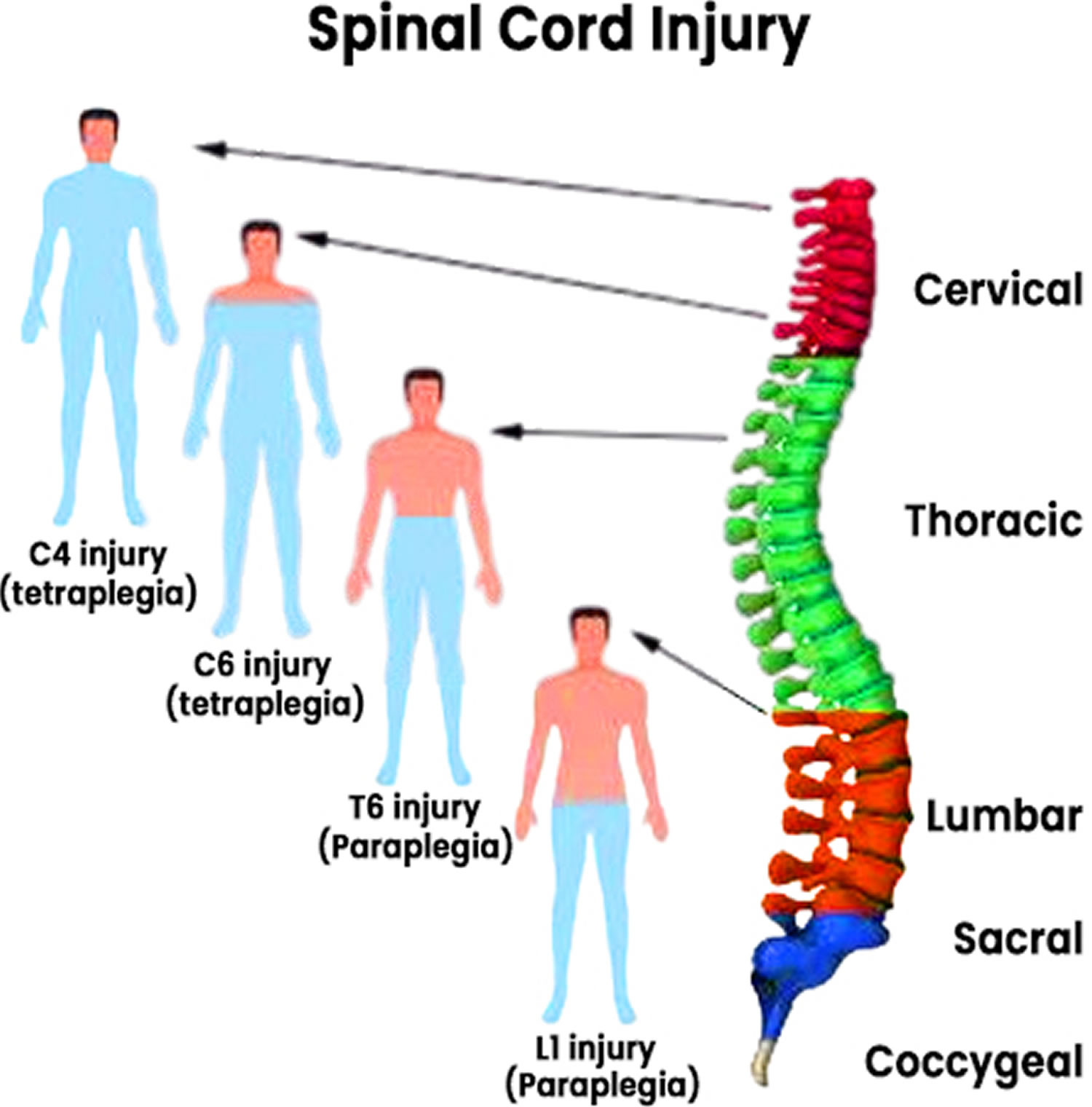
Figure 3. Quadriplegia
Anyone who has significant trauma to their head or neck needs immediate medical evaluation for a spinal injury. In fact, it’s safest to assume that trauma victims have a spinal injury until proved otherwise because:
- A serious spinal injury isn’t always immediately obvious. If it isn’t known, a more severe injury may occur.
- Numbness or paralysis can be immediate or come on gradually.
- The time between injury and treatment can be critical in determining the extent and severity of complications and the possible extent of expected recovery.
If you suspect that someone has a back or neck injury:
- Don’t move the injured person — permanent paralysis and other serious complications can result
- Call your local emergency services number immediately
- Keep the person still and avoid doing anything that could make the injury worse
- Place heavy towels on both sides of the neck or hold the head and neck to prevent them from moving until emergency care arrives
- Provide basic first aid, such as stopping bleeding and making the person comfortable, without moving the head or neck
Quadriplegia is a symptom of a problem that happens with many conditions and problems that affect your brain or spinal cord. Many of these problems and conditions are dangerous or deadly. Because of that, you shouldn’t try to self-diagnose or self-treat quadriplegia.
Even small movements or shifts in vertebrae and tissue around your spinal cord can lead to permanent damage. Only trained medical professionals or first responders should attempt to move someone with a possible spinal cord injury. The ONLY exception to this guidance is if the injured person is at risk for immediate injury or death if you don’t move them (such as in the event of a motor vehicle crash where the person is in a vehicle that may catch fire).
Can quadriplegia be cured?
In some cases — though these are usually rare — quadriplegia is temporary or even curable. This is most likely when the problem involves disruptions in how the spinal cord works that don’t permanently damage or affect your spinal cord’s structure. Examples of these include infections or benign tumors. In general, a healthcare provider is the best person to tell you if quadriplegia is curable, as they can consider all the factors involved before telling you what you can and should expect.
What is spastic quadriplegia?
Spastic quadriplegia is a form of paralysis (muscle weakness) that happens because the affected muscles aren’t receiving signals from your brain. Without those signals, muscles can sometimes move on their own. Because these muscle movements are uncontrollable, this is still a form of paralysis.
What is spastic quadriplegic cerebral palsy?
Cerebral palsy (CP) is a group of neurological disorders that appear in infancy or early childhood and permanently affect body movement and muscle coordination that cause problems with movement, balance, and posture 5. Cerebral palsy (CP) affects the cerebral motor cortex. This is the part of the brain that directs muscle movement. In fact, the first part of the name, cerebral, means having to do with the brain. The second part, palsy, means weakness or problems with using the muscles.
Cerebral palsy (CP) is caused by damage to or abnormalities inside the developing brain that disrupt the brain’s ability to control movement and maintain posture and balance. In some cases, the areas of the brain involved in muscle movement do not develop as expected during fetal growth. In others, the damage is a result of injury to the brain either before, during, or after birth. In either case, the damage is not reversible and the disabilities that result are permanent. Cerebral palsy (CP) isn’t progressive, meaning it doesn’t get worse over time and some symptoms may even change as the child gets older. If a child is continuously losing motor skills, the problem more likely is a condition other than cerebral palsy (CP) such as a genetic or muscle disease, metabolism disorder, or tumors in the nervous system 5.
Cerebral palsy (CP) is the leading cause of childhood disabilities in the U.S., but it doesn’t always cause profound disabilities. Someone with mild cerebral palsy (CP) may not need any assistance or may have slight problems, such as difficulty walking, while a person with severe cerebral palsy (CP) might need special equipment or lifelong care.
There are different types of cerebral palsy (CP) 5:
- Spastic cerebral palsy is the most common type of cerebral palsy caused by damage to the motor cortex. Individuals with spastic cerebral palsy experience spasticity (high muscle tone) and awkward movements in their arms, trunk, and legs. It can even affect the muscles in the face and impact an individual’s ability to eat and speak. However, spasticity is most severe in the arms and legs. This typically results in stiff muscles which cause jerky or repeated movements through the entire body.
- There are different forms of spastic cerebral palsy, depending on the body parts affected. Forms of spastic cerebral palsy include 5:
- Spastic hemiplegia or spastic hemiparesis typically affects the arm and hand on one side of the body, but it can also include the leg. Children with spastic hemiplegia generally walk later and on tip-toe because of tight heel tendons. The arm and leg of the affected side are frequently shorter and thinner. Some children will develop scoliosis, an abnormal curvature of the spine. Speech is delayed and, at best, may be competent, but intelligence is usually normal.
- Spastic diplegia or spastic diparesis involves muscle stiffness that is mainly in the legs and less severely affects the arms and face, although the hands may be clumsy. Tendon reflexes in the legs are hyperactive. Tightness in certain leg muscles makes the legs move like the arms of a scissor. Children may require a walker or leg braces. Intelligence and language skills are usually normal.
- Spastic quadriplegia or spastic quadriparesis is the most severe form of cerebral palsy and is often associated with moderate-to-severe intellectual and developmental disabilities. It is caused by widespread damage to the brain or significant brain malformations. Children will often have severe stiffness in their limbs but a floppy or weak neck. People with spastic quadriplegia are usually unable to walk and often have trouble speaking. Seizures can be frequent and hard to control.
- There are different forms of spastic cerebral palsy, depending on the body parts affected. Forms of spastic cerebral palsy include 5:
- Ataxic cerebral palsy is a type of cerebral palsy caused by damage to the cerebellum. As a result, individuals with ataxic cerebral palsy typically experience poor coordination and balance as well as low muscle tone throughout their entire bodies, which causes problems with balance and coordination. Children with ataxic cerebral palsy will often have poor coordination and walk unsteadily with a wide-based gait. They have difficulty with quick or precise movements, such as writing or buttoning a shirt, or a hard time controlling voluntary movement such as reaching for a book.
- Dyskinetic cerebral palsy (also includes athetoid, choreoathetoid, and dystonic cerebral palsies) is a type of cerebral palsy caused by damage to the basal ganglia and/or thalamus. Individuals with dyskinetic cerebral palsy experience fluctuations of high and low muscle tone throughout their entire bodies, which causes problems controlling the movement of the hands, arms, feet, and legs. Dyskinetic cerebral palsy is characterized by slow and uncontrollable writhing or jerky movements of the hands, feet, arms, or legs. This can make it hard to sit straight or walk. Hyperactivity in the muscles of the face and tongue makes some children grimace or drool. Some children have problems hearing, controlling their breathing, and/or coordinating the muscle movements required for speaking. Intelligence is rarely affected.
- Mixed cerebral palsy means that you have symptoms of more than one type of cerebral palsy (CP). For example, a child with mixed cerebral palsy may have some muscles that are too tight and others that are too relaxed, creating a mix of stiffness and floppiness.
Most children with cerebral palsy are diagnosed during the first two years of life. But if a child’s symptoms are mild, it can be difficult for a doctor to make a reliable diagnosis before the age of 4 or 5.
Infants with cerebral palsy (CP) frequently have developmental delays, in which they are slow in learning to roll over, sit, crawl, or walk. Decreased muscle tone (hypotonia) can make them appear relaxed, even floppy. Increased muscle tone (hypertonia) can make their bodies seem stiff or rigid. Children with cerebral palsy (CP) may also have unusual posture or favor one side of the body when they reach, crawl, or move.
Younger than 6 months of age:
- The head lags when you pick them up while they’re lying on their back
- They feel stiff
- They feel floppy
- Their legs get stiff and cross or scissor when you pick them up
Older than 6 months of age:
- They don’t roll over in either direction
- They cannot bring their hands together
- They have difficulty bringing their hands to their mouth
- They reach out with only one hand while keeping the other fisted
Older than 10 months of age:
- They crawl in a lopsided manner, pushing off with one hand and leg while dragging the opposite hand and leg
- They cannot stand even while holding on to support
Lab tests can identify other conditions that may cause symptoms similar to those associated with cerebral palsy (CP). Neuroimaging techniques can detect abnormalities that indicate a potentially treatable movement disorder.
- Cranial ultrasound uses high-frequency sound waves to produce pictures of the brain. It is used for high-risk premature infants because it is the least intrusive of the imaging techniques.
- Magnetic resonance imaging (MRI) uses a computer, a magnetic field, and radio waves to create an anatomical picture of the brain’s tissues and structures. MRI can show the location and type of damage, such as subtle changes in the white matter—the type of brain tissue that is damaged in cerebral palsy (CP). MRI can also show characteristic brain abnormalities or malformations in metabolic disorders that can masquerade as cerebral palsy (CP).
- Electroencephalogram (EEG), uses a series of electrodes that are either taped or temporarily pasted to the scalp to detect electrical activity in the brain. Changes in the normal electrical pattern may help to detect seizures.
There is no cure for cerebral palsy (CP), but treatment can improve the lives of those who have it. It is important to begin a treatment program as early as possible.
Many children are able to manage their disabilities; the earlier treatment begins, the better chance children have of overcoming developmental disabilities.
A team of health professionals will work with you and your child to develop a treatment plan. Common treatments include:
- Medicines
- Oral medications such as diazepam, baclofen, dantrolene sodium, and tizanidine are usually used as the first line of treatment to relax stiff, contracted, or overactive muscles. Some drugs have side effects such as drowsiness, changes in blood pressure, and risk of liver damage that require continuous monitoring. Oral medications are most appropriate for children who need only mild reduction in muscle tone or who have widespread spasticity.
- Botulinum toxin (BT-A), injected locally into muscles, has become a standard treatment for overactive muscles in children with spastic cerebral palsy (CP). Botulinum toxin relaxes contracted muscles by keeping nerve cells from over-activating muscle. The relaxing effects last approximately three months. Side effects include pain upon injection and occasionally mild flu-like symptoms. Botulinum toxin injections are most effective when followed by physical therapy and splinting. Botulinum toxin injections work best for children who have some control over their motor movements and have a limited number of muscles to treat, none of which is fixed or rigid.
- Intrathecal baclofen therapy uses an implantable pump to deliver baclofen, a muscle relaxant, into the fluid surrounding the spinal cord. Baclofen decreases the excitability of nerve cells in the spinal cord, which then reduces muscle spasticity throughout the body. The pump can be adjusted if muscle tone is worse at certain times of the day or night. The baclofen pump is most appropriate for individuals with chronic, severe stiffness or uncontrolled muscle movement throughout the body.
- Surgery
- Orthopedic surgery is often recommended when spasticity and stiffness are severe enough to make walking and moving about difficult or painful. Surgeons can lengthen muscles and tendons that are proportionately too short, which can improve mobility and lessen pain. Tendon surgery may help the symptoms for some children with cerebral palsy (CP) but could also have negative long-term consequences. Orthopedic surgeries may be staggered at times appropriate to a child’s age and level of motor development. Surgery can also correct or greatly improve spinal deformities.
- Surgery to cut nerves or selective dorsal rhizotomy (SDR), is a surgical procedure recommended for cases of severe spasticity when all of the more conservative treatments haven’t helped. A surgeon locates and selectively severs overactivated nerves at the base of the spinal column. Selective dorsal rhizotomy is most commonly used to relax muscles and decrease chronic pain in limbs. Potential side effects include sensory loss, numbness, or uncomfortable sensations.
- Assistive devices. Assistive devices such devices such as computers, computer software, voice synthesizers, and picture books can greatly help some individuals with cerebral palsy (CP) improve communications skills. Other devices make it easier for people with cerebral palsy (CP) to adapt to activities of daily living.
- Orthotic devices help to compensate for muscle imbalance and increase independent mobility.
- Braces and splints use external force to correct muscle abnormalities and improve function such as sitting or walking. Other orthotics help stretch muscles or the positioning of a joint.
- Braces, wedges, special chairs, and other devices can help people sit more comfortably.
- Wheelchairs, rolling walkers, and powered scooters can help individuals who are not independently mobile.
- Vision aids include glasses, magnifiers, and large-print books and computer typeface. Some individuals with cerebral palsy (CP) may need surgery to correct vision problems.
- Hearing aids and telephone amplifiers may help people hear more clearly.
- Physical, occupational, recreational, and speech therapy
- Physical therapy, usually in the first few years of life, is a cornerstone of cerebral palsy (CP) treatment. Specific sets of exercises like stretching, resistive, or strength training programs and activities can maintain or improve muscle strength, balance, and motor skills, and prevent contractures. Special braces (orthotic devices) may be used to improve mobility and stretch spastic muscles.
- Occupational therapy focuses on optimizing upper body function, improving posture, and making the most of a child’s mobility. Occupational therapists help individuals address new ways to meet everyday activities and routines at home, school, and in the community.
- Recreation therapy encourages participation in art and cultural programs, sports, and other events that help an individual expand physical and cognitive skills and abilities. Parents of children who participate in recreational therapies usually notice an improvement in their child’s speech, self-esteem, and emotional well-being.
- Speech and language therapy can improve a child’s ability to speak, help with swallowing disorders, and learn new ways to communicate, such as using sign language and/or special communication devices such as a computer with a voice synthesizer.
- Treatments for problems with eating and drooling are often necessary when children with cerebral palsy (CP) have difficulty eating and drinking because they have little control over the muscles that move their mouth, jaw, and tongue.
Treatments for other conditions associated with cerebral palsy:
- Epilepsy: Many children with intellectual disability and cerebral palsy (CP) also have epilepsy. Drugs are prescribed based on the type of seizures an individual experiences. Some people may need a combination of two or more drugs to achieve good seizure control.
- Incontinence: Medical treatments for incontinence include special exercises, biofeedback, prescription drugs, surgery, or surgically implanted devices to replace or aid muscles.
- Osteopenia: Children with cerebral palsy (CP) who are unable to walk risk developing poor bone density (osteopenia), which makes them more likely to break bones. Vitamin D can help promote bone health.
- Pain: Pain can be a problem for people with cerebral palsy (CP) due to spastic muscles and the stress and strain on parts of the body that are compensating for muscle abnormalities. Some individuals may also have frequent and irregular painful muscle spasms. Drug treatments such as diazepam, gabapentin, botulinum toxin injections, and intrathecal baclofen have been shown to ease pain. Some people with cerebral palsy (CP) use noninvasive and drug-free interventions such as distraction, relaxation training, biofeedback, and therapeutic massage to treat pain.
What is transient quadriplegia?
One of the most common forms of temporary quadriplegia is a type of spinal compression that occasionally happens in athletes, especially football players. This is “transient quadriplegia,” and athletes often call this a “stinger” or “burner.” Those names come from the intense stinging or burning, especially in one or both hands, that a person feels, along with an inability to move their limbs. The effects of transient quadriplegia usually go away in 10 to 15 minutes but can take up to two days. Athletes who experience this also need immediate medical attention from qualified personnel (such as certified athletic trainers) to make sure they don’t have an injury to their spine or spinal cord that could cause permanent damage and paralysis.
IMPORTANT: When transient quadriplegia affects more than one limb, it should be treated like a medical emergency, and trained personnel should immediately respond as if the affected person has a spinal injury. That means the injured person needs immobilization to prevent further injury, and they need to go to a hospital right away so a healthcare professional can assess if they have an injury and begin treatment if necessary.
Can people with quadriplegia move their hands?
People with incomplete quadriplegia can sometimes move or use their arms and hands. Whether or not they can do so depends on the level and severity of the injury. The higher up the spine an injury happens, the less likely that hand or arm use is possible. A healthcare provider can tell you more about what to expect in specific situations.
Quadriplegia causes
There are many possible causes of quadriplegia. The most common reason people have quadriplegia in the United States is trauma (injury) to their spinal cord. The most common causes of trauma include:
- Motor vehicle crashes (especially without the use of seat belts or when the crash causes a person to be ejected from a vehicle). Auto and motorcycle accidents are the leading cause of spinal cord injuries, accounting for almost half of new spinal cord injuries each year.
- Falls (especially those that involve older adults who have bone density-related issues like osteoporosis or osteopenia). A spinal cord injury after age 65 is most often caused by a fall.
- Violence-related injuries (gunshot wounds, stab wounds, blunt impact, etc.). About 12% of spinal cord injuries result from violent encounters, usually from gunshot wounds. Knife wounds also are common.
- Sports-related injuries. Athletic activities, such as impact sports and diving in shallow water, cause about 10% of spinal cord injuries.
Other problems that can cause quadriplegia include the following:
- Spine tumors, including cancers. This can involve cancer that develops on or around your spinal cord, or that starts elsewhere in your body and spreads to your spine.
- Cysts or fluid-filled cavities within your spinal cord (syringomyelia).
- Infections that attack or compress your spinal cord.
- Lack of blood flow (ischemia) due to a blocked blood vessel or blood vessel rupture.
- Congenital conditions (that you have when you’re born) where you have a problem with your spine or spinal cord structure, such as myelomeningocele or spina bifida.
- Injuries that happen during birth or very early childhood, causing conditions like cerebral palsy.
- Autoimmune or inflammatory conditions like Guillain-Barré syndrome, multiple sclerosis or transverse myelitis.
Risk factors for quadriplegia
Although a spinal cord injury is usually the result of an accident and can happen to anyone, certain factors can predispose you to being at higher risk of having a spinal cord injury, including:
- Being male. Spinal cord injuries affect a disproportionate number of men. In fact, females account for only about 20% of traumatic spinal cord injuries in the United States.
- Being between the ages of 16 and 30. More than half of spinal cord injuries occur in people in this age range.
- Being 65 and older. Another spike in spinal cord injuries occurs at age 65. Falls cause most injuries in older adults.
- Alcohol use. Alcohol use is involved in about 25 % of traumatic spinal cord injuries.
- Engaging in risky behavior. Diving into too-shallow water or playing sports without wearing the proper safety gear or taking proper precautions can lead to spinal cord injuries. Motor vehicle crashes are the leading cause of spinal cord injuries for people under 65.
- Having certain diseases. A relatively minor injury can cause a spinal cord injury if you have another disorder that affects your joints or bones, such as osteoporosis.
Quadriplegia prevention
The most common cause of quadriplegia (i.e., trauma) is often preventable. The best things you can do to prevent spinal injuries and trauma are:
- Wear safety equipment. Car crashes are one of the most common causes of spinal cord injuries. Wear a seat belt every time you’re in a moving vehicle. Seat belts and other restraints can help avoid injuries that could lead to quadriplegia. Make sure that your children wear a seat belt or use an age- and weight-appropriate child safety seat. To protect them from air bag injuries, children under age 12 should always ride in the back seat. People playing sports should always use recommended safety gear, too. Helmets and padding are essential, as are playing conscientiously and safely. That means avoiding tackling/hitting from behind in contact sports like football, hockey, etc.
- Take precautions when playing sports. Always wear recommended safety gear. Avoid leading with your head in sports. For example, don’t slide headfirst in baseball, and don’t tackle using the top of your helmet in football. Use a spotter for new moves in gymnastics.
- Don’t drink and drive. Don’t drive while intoxicated or under the influence of drugs. Don’t ride with a driver who’s been drinking.
- Check water depth before diving. Don’t dive into a pool unless it’s 12 feet (about 3.7 meters) or deeper, don’t dive into an above-ground pool and don’t dive into water if you don’t know how deep it is.
- Take precautions to avoid falls. Use safety equipment, especially safety harnesses, when working on a roof or another elevated environment. You should also take steps to avoid falls in the home, especially with stairs or in bathrooms. This can include installing handrails, using non-slip footwear and put nonslip mats on tile floors and in the tub or shower, keeping stairs clear of tripping hazards. Use a step stool with a grab bar to reach high-up objects. For young children, use safety gates to block stairs and consider installing window guards.
- Be careful when using firearms. Gunshot wounds are one of the most common causes of spinal cord injuries that lead to paraplegia. You should ALWAYS treat firearms with extreme caution, no matter the circumstance. Act as if they’re loaded even if you’re absolutely certain they aren’t. You should also store firearms unloaded, secured with a trigger lock and out of reach of children. It’s also wise to store ammunition separately under lock and key.
- Avoid misusing prescription medications, recreational drugs and alcohol. These can affect your immune system’s ability to fight infection. They can also increase your risk of injury from falls, car crashes, etc.
Quadriplegia signs and symptoms
Your spine has several sections (see Figure 1). The cervical spine (often shortened to C-spine) is the section in your neck. There are seven vertebrae (the word for one of these is “vertebrum”), interlocking bone segments, which make up your cervical spine (C-spine). Your cervical spine (C-spine) also includes eight spinal nerves, which run in-between vertebrae and lead to different areas of your body.
The effects of a problem with a spinal cord can vary widely depending on where exactly it happens. There are also varying definitions of “paralysis.” Some experts define it as a total loss of muscle control, while others include muscle weakness under the definition. Because of that, some definitions of quadriplegia include limited movement ability in your arms or hands.
Healthcare providers use a letter-number combination to talk about sections of the spine and related spinal nerves. For example, the fifth cervical spinal nerve is known as C5. Quadriplegia can happen when there’s a complete or incomplete spinal cord injury anywhere between C1 and C8. The higher the injury, the more dangerous the effects.
The effects, depending on location, are as follows:
- C1 to C2: Complete paralysis of all four limbs and the muscles that control your breathing. These injuries are almost always deadly without immediate care, especially breathing support (ventilation). Injuries at this level can also cut off your brain’s connection to other parts of your autonomic nervous system, which manages automatic functions like sweating, blood pressure control, digestion, and the muscles in your bladder and bowels you deliberately relax so you can pee or poop.
- C3 to C4: Same as above, but damage that’s closer to C4 may not block your brain’s control of breathing muscles. Some breathing problems are still possible, and coughing is severely affected, which increases the risk of developing pneumonia as a complication.
- C4 to C8: Varying levels of paralysis in your arms and hands. The further down your spinal cord, the less widespread the effects of the paralysis.
There are also two main ways that quadriplegia can happen 3:
- Incomplete quadriplegia. This means that the quadriplegia blocks some — but not all — signals from getting through. That means a person might still have some ability to move, feel sensations or control automatic body processes (such as bowel and bladder function). This happens with about one-third of traumatic spinal cord injuries.
- Complete quadriplegia. This means whatever causes the quadriplegia blocks all signals from getting through. That means a person loses muscle control, the ability to feel sensations and their brain can’t manage any automatic processes that rely on brain signaling to work. This happens with about 20% of spinal cord injuries.
There are also two main ways that paralyzed muscles act in quadriplegia 3:
- Flaccid quadriplegia: This means that muscles don’t work at all and remain flaccid or limp.
- Spastic quadriplegia: This type of quadriplegia results in muscles that don’t work by themselves and contract uncontrollably.
Signs and symptoms of quadriplegia include:
- Weakness or paralysis of the arms and legs
- Loss of sensation
- Incontinence of bladder or bowel
- Sexual dysfunction—male or female
- Breathing difficulties
- Poor trunk control (which may influence posture and balance). Difficulty sitting upright depending on the level of the damage
- Pain, numbness, or tingling below the level of injury
- Spasticity (involuntary muscle contractions)
Inactivity due to quadriplegia can cause additional problems, like:
- Bed sores
- Spastic limbs
- Pneumonia
- Urinary tract infection
- Weakened bones
- Chronic pain
People with quadriplegia may also become depressed because of:
- Social isolation
- Lack of emotional support
- Increased dependence on others
Because quadriplegia affects the majority of the body, individuals may require the help of a caregiver to perform everyday activities such as grooming and feeding.
Additionally, many individuals with quadriplegia need assistive mobility devices such as wheelchairs to increase mobility. Those with more severe weakness or paralysis may find a power wheelchair more helpful while those with milder motor impairments may be able to utilize a manual wheelchair.
Quadriplegia complications
Depending upon the spinal cord injury levels, quadriplegia complications may vary. Obviously, apart from wounds and infections, any injury higher in the spinal cord leads to more severe complications.
At first, changes in the way your body functions can be overwhelming. However, your rehabilitation team will help you develop tools to address the changes caused by the spinal cord injury, in addition to recommending equipment and resources to promote quality of life and independence. Areas often affected include:
- Bladder control. Your bladder will continue to store urine from your kidneys. However, your brain might not control your bladder as well because the message carrier (the spinal cord) has been injured. The changes in bladder control increase your risk of urinary tract infections (UTIs). The changes may also cause kidney infections and kidney or bladder stones. During rehabilitation, you’ll learn ways to help empty your bladder. You may need to use a catheter to empty your bladder.
- Bowel control. Although your stomach and intestines work much like they did before your injury, control of your bowel movements is often altered. A high-fiber diet might help regulate your bowels, and you’ll learn ways to help control your bowel during rehabilitation.
- Pressure sores also known as pressure ulcers. Pressure sores are areas of skin that have broken down because of continuous pressure on the skin and reduced blood flow to the area. Below the neurological level of your injury, you might have lost some or all skin sensations. Therefore, your skin can’t send a message to your brain when it’s injured by certain things such as prolonged pressure. This can make you more susceptible to pressure sores, but changing positions frequently — with help, if needed — can help prevent these sores. You’ll learn proper skin care during rehabilitation, which can help you avoid these problems.
- Circulatory control. A spinal cord injury can cause circulatory problems ranging from low blood pressure when you rise (orthostatic hypotension) to swelling of your extremities (edema). These circulation changes can also increase your risk of developing blood clots, such as deep vein thrombosis or a pulmonary embolus. Another problem with circulatory control is a potentially life-threatening rise in blood pressure (autonomic dysreflexia) and abnormal heart rhythms (arrhythmias). Blood pressure needs to be closely monitored. Because the brain’s control of the cardiac nerves can be cut off, your heart can beat at a dangerously slow pace, or it can pound rapidly and irregularly. Changes in the control of blood vessels can cause them to widen and allow blood to pool in the small arteries far away from the heart. People with spinal cord injuries are at increased risk for blood clots due to stagnation of blood flow in the large veins in the legs. Treatment includes anticoagulant drugs and compression stockings to increase blood flow in the lower legs and feet.
- Breathing problems. Your injury might make it more difficult to breathe and cough if your abdominal and chest muscles are affected. Your neurological level of injury will determine what kind of breathing problems you have. If you have a cervical and thoracic spinal cord injury, you might have an increased risk of pneumonia or other lung problems. Medications and therapy can help prevent and treat these problems.
- About one-third of people with a neck injury will need temporary or permanent help with breathing and may require an inserted artificial breathing tube. Any injury to the spinal cord between the C1-C4 segments can stop breathing as the nerves in this region cause the diaphragm to move and the lungs to expand. Special training regarding breathing and swallowing may be needed.
- Pneumonia: Respiratory complications are the leading cause of death in people with spinal cord injury, commonly as a result of pneumonia. If you are placed on a ventilator to assist with breathing (intubation), you are at increased risk of developing pneumonia. You must be carefully monitored and treated with antibiotics if symptoms of pneumonia appear. Clearing secretions from the throat and preventing food and liquids from being sucked into the lungs (aspiration) can prevent pneumonia.
- Bone density. After spinal cord injury, there’s an increased risk of osteoporosis and fractures below the level of injury.
- Muscle spasticity and decreased muscle tone. Some people with spinal cord injuries have one of two types of muscle tone problems: uncontrolled tightening or motion in the muscles (spasticity) or soft and limp muscles lacking muscle tone (flaccidity) that may require special treatment. Muscles may deteriorate due to underuse.
- Autonomic dysreflexia. Autonomic dysreflexia is a life-threatening reflex action that primarily affects those with injuries to the neck or upper back. Symptoms may include flushing or sweating, a pounding headache, anxiety, sudden increase in blood pressure, vision changes, or goose bumps on the arms and legs. If possible, you should be kept in a sitting position to keep blood flowing to the legs and feet and help reduce blood pressure.
- Fitness and wellness. Weight loss and muscle atrophy are common soon after a spinal cord injury. Limited mobility can lead to a more sedentary lifestyle, placing you at risk of obesity, cardiovascular disease and diabetes. A dietitian can help you eat a nutritious diet to sustain an adequate weight. Physical and occupational therapists can help you develop a fitness and exercise program.
- Sexual function. Depending on the level of injury and recovery from the trauma, sexual function and fertility may be affected. Men might notice changes in erection and ejaculation; women might notice changes in lubrication after a spinal cord injury. Physicians specializing in urology (urologist) or fertility can offer options for sexual functioning and fertility.
- Pain. Some people have pain, such as muscle or joint pain, from overuse of particular muscle groups. Nerve pain can occur after a spinal cord injury, especially in someone with an incomplete injury.
- Some people who have spinal cord nerve damage develop neurogenic pain, which is pain or an intense burning or stinging sensation that may be constant due to extreme physical sensitivity (hypersensitivity) in some parts of the body. It can either be spontaneous or triggered by a variety of factors and can occur even in parts of the body that have lost sensation. Treatments for chronic pain include medications, acupuncture, spinal or brain electrical stimulation, and surgery. However, none of these treatments are completely effective at relieving neurogenic pain.
- Depression. Coping with the changes a spinal cord injury brings and living with pain causes depression in some people. Therapy and medicine may help treat depression and other mental health conditions.
Quadriplegia diagnosis
In the emergency room, a doctor may be able to rule out a spinal cord injury by examination, testing for sensory function and movement, and by asking some questions about the accident. But if the injured person complains of neck pain, isn’t fully awake, or has obvious signs of weakness or neurological injury, emergency diagnostic tests may be needed. These tests can include:
Imaging studies
Plain X-rays
Plain X-rays is a useful screening tool to demonstrate associated bone fractures or degenerative changes in the spine, vertebral (spinal column) problems and tumors. Although disc space reduction is seen in chronic disc degeneration, plain films may not necessarily demonstrate reduced disc space secondary to acute disc injury.
Plain films have a role for assessment of cervical spinal stenosis, as this is associated with a higher incidence of cervical cord injury. The Torg ratio is used to assess cervical spinal stenosis 6. The Torg ratio is the sagittal canal/vertebral body ratios measured on cervical spine lateral radiographs. The normal value is 1.0. A ratio of 0.8 and below has been considered indicative of cervical spinal stenosis 6.
Plain radiography helps diagnose spear tackler spine, which is an entity seen in a subset of football players. Permanent neurologic injury is higher in this population due to axial loading of a relatively straight spine 7. Spear tackler spine is characterized by the following 8:
- Developmental narrowing (stenosis) of the cervical canal
- Persistent straightening or reversal of the normal cervical lordotic curve on erect lateral radiographs obtained in the neutral position
- Concomitant preexisting posttraumatic radiographic abnormalities of the cervical spine
- Documentation of having employed spear tackling techniques
CT scan
Computerized tomography (CT) scan can provide a clearer image of abnormalities seen on X-ray (images of organs, bones, and tissues). CT scan uses computers to form a series of cross-sectional images that can define bone, disk and other problems. CT can detect bone fractures, bleeding, and spinal stenosis (narrowing of the spinal canal).
Magnetic resonance imaging (MRI)
Magnetic resonance imaging (MRI) uses a strong magnetic field and radio waves to produce computer-generated three-dimensional images of body structures, including tissues, organs, bones, and nerves. MRI is helpful for looking at the spinal cord and identifying herniated discs (cartilage located between the vertebrae), vascular (blood vessel) irregularities, bleeding, blood clots, inflammation or other masses that might compress the spinal cord and injury to the ligaments that support the cervical spine.
MRI is more important to evaluate spinal cord or nerve root compression secondary to the disc herniation.
Interpretation of MRIs is important, as many abnormal MRI findings are noted in individuals who are asymptomatic. A cross-sectional study designed to determine the prevalence and distribution of abnormal findings on cervical spine MRI concluded that disc bulging was frequently observed in asymptomatic subjects, even including those in their 20s 9.
Other tests
A few days after your injury, when some of the swelling might have subsided, your doctor will conduct a more comprehensive neurological exam to determine the level and completeness of your spinal cord injury. This involves testing your muscle strength and your ability to sense light touch and pinprick sensations.
Your nerve function may be tested with:
- Nerve conduction study
- Somatosensory evoked potentials (SSEPs) (rarely used)
Your bodily fluids may be tested. This can be done with a lumbar puncture if some specific neurologic diseases are suspected.
Quadriplegia treatment
At the accident scene, if a spinal cord injury is suspected, emergency personnel will place a rigid collar around your neck and carefully place you on a backboard to prevent further damage to your spinal cord. They may use sedatives to relax and prevent movement. A breathing tube may be inserted if you have problems breathing and your body isn’t receiving enough oxygen from the lungs.
The treatments for quadriplegia can vary widely depending on the cause and where in your spine the problem happens. The potential to recover from quadriplegia can also vary.
With trauma, the first priority is to limit the damage as much as possible and prevent more from happening. That usually involves immobilizing a person using specialized backboards, collars or braces to keep their spinal cord stable and prevent anything from pressing into or damaging it.
Other ways to prevent damage to the spinal cord from injuries and trauma include:
- Early surgery to relieve pressure around the spinal cord.
- Early surgery to stabilize or fuse vertebrae together to keep them from damaging the spinal cord.
Because of these factors, your doctor is the best person to explain the situation. He or she can offer you guidance and relevant information for your specific situation, including the possible treatments and the side effects or complications that can happen with those treatments.
Emergency actions
Urgent medical attention is critical to minimize the effects of head or neck trauma. Therefore, treatment for a spinal cord injury often begins at the accident scene. Emergency personnel typically immobilize the spine as gently and quickly as possible using a rigid neck collar and a rigid carrying board, which they use during transport to the hospital.
Early (acute) stages of treatment
In the emergency room, doctors focus on:
- Maintaining your ability to breathe
- Preventing shock
- Immobilizing your neck to prevent further spinal cord damage
- Avoiding possible complications, such as stool or urine retention, respiratory or cardiovascular difficulty, and formation of deep vein blood clots in the extremities
If you have a spinal cord injury, you’ll usually be admitted to the intensive care unit (ICU) for treatment. You might be transferred to a regional spine injury center that has a team of neurosurgeons, orthopedic surgeons, spinal cord medicine specialists, psychologists, nurses, therapists and social workers with expertise in spinal cord injury.
- Medications. Methylprednisolone (Solu-Medrol) given through a vein in the arm (IV) has been used as a treatment option for an acute spinal cord injury in the past. But recent research has shown that the potential side effects, such as blood clots and pneumonia, from using this medication outweigh the benefits. Because of this, methylprednisolone is no longer recommended for routine use after a spinal cord injury.
- Immobilization. You might need traction to stabilize or align your spine. Options include soft neck collars and various braces.
- Surgery. Often surgery is necessary to remove fragments of bones, foreign objects, herniated disks or fractured vertebrae that appear to be compressing the spine. Surgery might also be needed to stabilize the spine to prevent future pain or deformity.
- Experimental treatments. Scientists are trying to figure out ways to stop cell death, control inflammation and promote nerve regeneration. For example, lowering body temperature significantly — a condition known as hypothermia — for 24 to 48 hours might help prevent damaging inflammation. More study is needed.
Ongoing care
After the initial injury or condition stabilizes, doctors turn their attention to preventing secondary problems that may arise, such as deconditioning, muscle contractures, pressure ulcers, bowel and bladder issues, respiratory infections, and blood clots.
The length of your hospital stay will depend on your condition and the medical issues you face. Once you’re well enough to participate in therapies and treatment, you might transfer to a rehabilitation facility.
Rehabilitation
Rehabilitation team members will begin to work with you while you’re in the early stages of recovery. Rehabilitation programs combine physical therapies with skill-building activities and counseling to provide social and emotional support, as well as to increase independence and quality of life. Your rehabilitation team might include a physical therapist, an occupational therapist, a rehabilitation nurse, a rehabilitation psychologist, a social worker, a dietitian, a recreation therapist, and a doctor who specializes in physical medicine (physiatrist) or spinal cord injuries.
- Physical therapy includes exercise programs geared toward strengthening muscles. Physical therapy for quadriplegia focuses on helping individuals strengthen weakened or underused muscles and maintain full range of motion through targeted exercises. A physical therapist will teach individuals the most effective exercises to stimulate neuroplasticity in the central nervous system. A physical therapist may also recommend orthotics such as braces and splints to promote correct musculoskeletal alignment and assist with mobility.
- Occupational therapy helps redevelop fine motor skills, particularly those needed to perform activities of daily living (ADLs) such as getting in and out of a bed, self-grooming, eating, and using the toilet. An occupational therapist will work with individuals with quadriplegia and their caregivers to teach them the most effective ways to perform everyday activities such as transferring, bathing, and grooming. This may involve learning how to use adaptive tools, such as a universal cuff, or adaptive techniques like tenodesis. Tenodesis is a natural movement that all of your body make. When you bend your wrist forward, the hand should open up. Likewise, when you extend the wrist (bend it backward), the fingers should curl in. Learning to utilize a tenodesis grasp can help individuals with quadriplegia become more independent. You may learn how to cope with spasticity, autonomic dysreflexia, and neurogenic pain.
- Vocational rehabilitation includes identifying basic work skills and physical and cognitive capabilities to determine the likelihood for employment; identifying potential workplaces and any assistive equipment that will be needed; and arranging a user-friendly workplace.
- Speech therapy. Individuals with quadriplegia often experience oral motor impairments that affect their ability to chew, swallow, and speak. Additionally, individuals with spinal cord injuries at the C5 level or above may experience breathing difficulties due to impaired innervation of the diaphragm. A speech therapist can help individuals with quadriplegia improve their oral motor functions, communication skills, and breathing.
- Educational training can help you develop skills for a new line of work that may be less dependent upon physical abilities and more dependent upon computer or communication skills. People with spinal cord injury or other disabilities are encouraged to participate in activities that provide a sense of satisfaction and self-esteem, such as educational classes, hobbies, special interest groups, and participating in family and community events.
- Recreation therapy encourages people with spinal cord injury to participate in sports or activities at their level of mobility, as well as achieve a more balanced lifestyle that provides opportunities for socialization and self-expression.
- Psychotherapy. Individuals with quadriplegia may develop mental health problems such as depression or anxiety due to feelings of isolation, lack of support, or difficulties adjusting to life with paralysis. Working with a psychotherapist can help individuals with quadriplegia better understand their negative feelings and find more effective ways to cope.
During the initial stages of your rehabilitation, therapists usually emphasize maintaining and strengthening muscle function, redeveloping fine motor skills, and learning ways to adapt to do day-to-day tasks. For some individuals, mobility will only be possible with assistive or adaptive devices such as a walker, leg braces, or a wheelchair. Communication skills such as writing, typing, and using the telephone may also require adaptive devices for those with tetraplegia.
You’ll be educated on the effects of a spinal cord injury and how to prevent complications, and you’ll be given advice on rebuilding your life and increasing your quality of life and independence.
You’ll be taught many new skills, and you’ll use equipment and technologies that can help you live on your own as much as possible. You’ll be encouraged to resume your favorite hobbies, participate in social and fitness activities, and return to school or the workplace.
Medications
Medications might be used to manage some of the effects of spinal cord injury. These include medications to control pain and muscle spasticity, as well as medications that can improve bladder control, bowel control and sexual functioning.
To reduce spasticity, therapists may recommend Botox injections or muscle relaxants to temporarily relieve high muscle tone. This creates a window of opportunity for individuals to practice therapeutic activities and exercises without the interference of spasticity. Often, some of the improvements made while spasticity is controlled are maintained even after the effects of the medication wear off due to neuroplasticity.
Surgery
Individuals with severe spasticity that does not respond to other forms of treatment may benefit from surgery. Surgery for spasticity typically involves manually lengthening of the muscles and tendons, the implantation of an intrathecal baclofen pump, or selective incisions of nerves that cause hyperactive muscle contractions.
Assistive medical devices
Assistive medical devices can help people with a spinal cord injury become more independent and more mobile, thereby promoting their well-being. Depending on the severity of the injury, people may need a wheelchair, electronic stimulators, assisted training with walking, neural prosthetics (assistive devices that may stimulate the nerves to restore lost functions), computer adaptations, and other computer-assisted technology.
- Modern wheelchairs. Improved, lighter weight wheelchairs are making people with spinal cord injuries more mobile and more comfortable. Some people need an electric wheelchair. Some wheelchairs can even climb stairs, travel over rough ground and elevate a user to reach high places without help.
- Computer adaptations. For someone who has limited hand function, computers can be difficult to operate. Computer adaptations range from simple to complex, such as key guards and voice recognition.
- Electronic aids to daily living. Essentially any device that uses electricity can be controlled with an electronic aid to daily living. Devices can be turned on or off by switch or voice-controlled and computer-based remotes.
- Electrical stimulation devices. Often called functional electrical stimulation systems, these sophisticated devices use electrical stimulators to control arm and leg muscles to allow people with spinal cord injuries to stand, walk, reach and grip.
Quadriplegia prognosis
Your doctor might not be able to give you a prognosis right away. Recovery, if it occurs, usually relates to the severity and level of the injury. Generally, the milder your injury, the better the recovery outlook. The fastest rate of recovery is often seen in the first six months, but some people make small improvements for up to 1 to 2 years.
Damaged neurons in the brain and spinal cord are unable to regenerate. However, areas of the central nervous system (brain and spinal cord) unaffected by injury have the ability to recover affected functions by utilizing neuroplasticity. Neuroplasticity is the central nervous system’s ability to make adaptive changes to its neural circuitry based on the behaviors we repetitively practice. Therefore, the more you practice a function weakened by injury, the more you stimulate the central nervous system and reinforce demand for those functions. This encourages the brain and/or spinal cord to rewire functions affected by injury to unaffected regions and strengthen them.
As long as individuals have spared neural pathways, there is potential to recover or at least improve functions affected by quadriplegia.
Although those with complete spinal cord injuries resulting in quadriplegia are unable to utilize neuroplasticity to improve their motor and sensory functions, they can still learn various adaptive techniques to become as independent as possible. The following section will discuss various treatment interventions that utilize neuroplasticity to help individuals with quadriplegia improve their mobility and functional independence.
Quadriplegia prognosis life expectancy
The life expectancy for people with quadriplegia can vary widely depending on many factors. These factors include a person’s age, the location and severity of the injury, whether or not it affects their ability to breathe on their own and more. Life expectancy in quadriplegia is reduced by 20% to 30% overall compared with the general population; however, much of this reduction is due to peri-injury mortality, and if people survive the first year after injury, life expectancy is impacted less 10, 11. As such, any prevalent secondary complication will be with a younger person for most of their life and will add to the comorbidities of ageing alongside the quadriplegia per se in an older person.
Furthermore, thanks to advances in modern medicine, treatment techniques, and assistive devices and therapies, people with quadriplegia can live for years or even decades. However, because life expectancy can vary widely, a healthcare provider is the best person to tell you what’s most likely to happen in your case.
- Rupp R, Biering-Sørensen F, Burns SP, Graves DE, Guest J, Jones L, Read MS, Rodriguez GM, Schuld C, Tansey-Md KE, Walden K, Kirshblum S. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top Spinal Cord Inj Rehabil. 2021 Spring;27(2):1-22. doi: 10.46292/sci2702-1[↩][↩][↩]
- Spinal cord injury. https://www.mayoclinic.org/diseases-conditions/spinal-cord-injury/symptoms-causes/syc-20377890[↩][↩][↩]
- Quadriplegia. https://my.clevelandclinic.org/health/symptoms/23974-quadriplegia-tetraplegia[↩][↩][↩][↩][↩]
- Ahuja, C., Wilson, J., Nori, S. et al. Traumatic spinal cord injury. Nat Rev Dis Primers 3, 17018 (2017). https://doi.org/10.1038/nrdp.2017.18[↩]
- Cerebral Palsy. https://www.ninds.nih.gov/health-information/disorders/cerebral-palsy[↩][↩][↩][↩]
- Torg JS, Corcoran TA, Thibault LE, Pavlov H, Sennett BJ, Naranja RJ Jr, Priano S. Cervical cord neurapraxia: classification, pathomechanics, morbidity, and management guidelines. J Neurosurg. 1997 Dec;87(6):843-50. https://doi.org/10.3171/jns.1997.87.6.0843[↩][↩]
- Torg JS, Sennett B, Pavlov H, Leventhal MR, Glasgow SG. Spear tackler’s spine. An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med. 1993 Sep-Oct;21(5):640-9. doi: 10.1177/036354659302100502[↩]
- Cervical Disc Injuries Workup. https://emedicine.medscape.com/article/93635-workup[↩]
- Nakashima H, Yukawa Y, Suda K, Yamagata M, Ueta T, Kato F. Abnormal findings on magnetic resonance images of the cervical spines in 1211 asymptomatic subjects. Spine (Phila Pa 1976). 2015 Mar 15;40(6):392-8. doi: 10.1097/BRS.0000000000000775[↩]
- Middleton JW, Dayton A, Walsh J, et al.. Life expectancy after spinal cord injury: a 50-year study. Spinal Cord 2012;50:803–11. 10.1038/sc.2012.55[↩]
- Berlowitz DJ, Schembri R, Graco M, Ross JM, Ayas N, Gordon I, Lee B, Graham A, Cross SV, McClelland M, Kennedy P, Thumbikat P, Bennett C, Townson A, Geraghty TJ, Pieri-Davies S, Singhal R, Marshall K, Short D, Nunn A, Mortimer D, Brown D, Pierce RJ, Cistulli PA; COSAQ Collaborative. Positive airway pressure for sleep-disordered breathing in acute quadriplegia: a randomised controlled trial. Thorax. 2019 Mar;74(3):282-290. doi: 10.1136/thoraxjnl-2018-212319[↩]





{kind=link}