Contents
What is radiofrequency ablation
Radiofrequency ablation is also known as rhizotomy, is one of the newest pain control techniques. In this non-surgical procedure, radio waves are used to heat and destroy certain nerves, with the goal of interrupting pain signals to the brain. The radio waves travel through electrodes (small devices that carry electricity). Radiofrequency ablation uses imaging techniques such as ultrasound, computed tomography (CT) or magnetic resonance imaging (MRI) to help guide a needle electrode into the target area. High-frequency electrical currents are then passed through the electrode to ground pads placed on the body, creating focal heat that destroys certain nerves or cancer cells surrounding the electrode.
Radiofrequency ablation is done using fluoroscopic (x-ray) guidance and should NOT be performed on people who have an infection, are pregnant, or have bleeding problems.
The types of physicians who perform radiofrequency ablation include physiatrists, pain specialists, radiologists, anesthesiologists, neurologists, and surgeons.
Radiofrequency ablation typically targets pain from the facet joints, which can contribute to chronic pain in the neck or lower back, and the sacroiliac joints, which can contribute to chronic low back pain. However, the efficacy of radiofrequency ablation for discogenic back pain remains unclear 1.
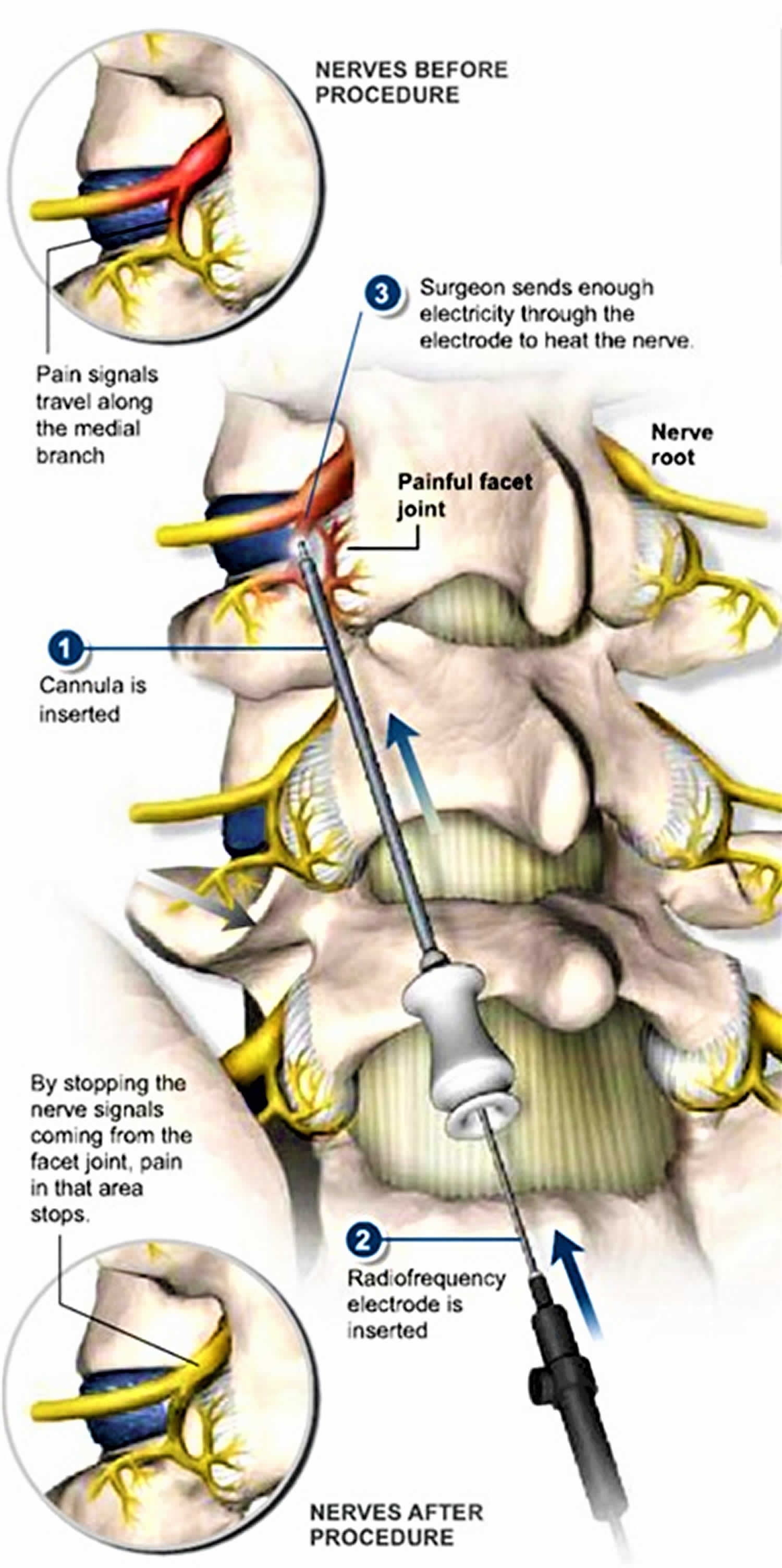
Facet joints are pairs of small joints located at each vertebral level of the spine. Each facet joint is connected to two medial branch nerves that carry signals, including pain signals, away from the joints to the spine and brain. The sacroiliac joints are located at the lowest part of the spine, between the sacrum and ilium in the pelvis, and are also connected to nerves that carry signals to other parts of the body.
Radiofrequency ablation is usually done by a doctor who specializes in treating pain. The goal is to reduce chronic back, neck, hip or knee pain that hasn’t improved with medications or physical therapy, or when surgery isn’t an option.
For example, your doctor may suggest the procedure if you have back pain that:
- Occurs on one or both sides of your lower back
- Spreads to the buttocks and thighs (but not below the knee)
- Feels worse if you twist or lift something
- Feels better when you’re lying down
Radiofrequency neurotomy might also be recommended to treat neck pain associated with whiplash.
Radiofrequency ablation can also be used to treat stomach pain caused by pancreatic cancer or pelvic pain caused by ovarian cancer.
Radiofrequency ablation is sometimes used to treat cancers in the:
- Adrenal gland
- Breast
- Bone
- Kidney
- Liver
- Lung
- Pancreas
- Thyroid
Radiofrequency ablation is typically considered a treatment option only if you’re not a good candidate for surgery for some reason — such as your overall health or the presence of many small tumors in an organ.
Radiofrequency ablation is most commonly used to treat a spot of cancer that is causing problems such as pain or other discomfort, and is generally not used as the primary treatment for most cancers.
Radiofrequency ablation may also be an option for treating precancerous cells in the esophagus that are associated with Barrett’s esophagus. Radiofrequency ablation is one of several types of ablation therapy used to treat a wide range of conditions.
Radiofrequency ablation is commonly used to treat many types of liver cancer. The two most common types are:
- hepatocellular carcinoma, which is a primary liver cancer (meaning it begins in the liver).
- colon cancer that metastasizes or spreads from the colon to the liver.
Radiofrequency ablation can be an effective treatment for primary liver cancer and for cancers that have spread to the liver in select patients whose liver tumors are unsuitable for surgical resection. In general, radiofrequency ablation is most effective treating tumors that are less than one and a half inches in diameter. It may be used in addition to chemotherapy or radiation therapy or as an alternative to surgical treatment. In cancer treatment a radiofrequency ablation needle is inserted into the tumor either percutaneously or surgically (via the laparoscopic or open approach). Alternating current is generated using radio waves and, through radiofrequency ablation needle, create local tissue temperatures of 50-100˚C temperature for at least 4-6 minutes 2, that causes “coagulation” 3 and tumor necrosis 4; usually the duration of radiofrequency ablation is 10-30 minutes for the slow conduction from the radiofrequency ablation needle electrode through the tumor 2. To reduce the incidence of local tumor recurrence after radiofrequency ablation, a 1-cm-thick tumor-free margin along each tumor is necessary, which can be achieved by multiple overlapping ablations or modified radiofrequency ablation devices 2. At present, new modified radiofrequency ablation devices are available: a multi-pled expandable electrode with multiple retractable prongs on the tip (AngioDynamics/RITA Medical Systems) and an internally cooled electrode (Radionics, Tyco Healthcare Group, Burlington, MA) 3. Tumor size and localization are important factors for successfully ablation treatment, such as smaller colorectal derived oligometastasis isolated to the liver less than 3 cm in diameter 2, surrounded by liver parenchyma, 1 cm or more deep to the liver glissonian, and ≥ 2 cm from large liver veins 5. Data on long-term survival (5-year overall survival), after different methods of radiofrequency ablation, have been reported with a range between 22-30% 6. There is a 5-year overall survival increasing (40%) in small (≤4 cm) solitary liver metastases from colorectal cancer 7. A well conducted 2012 Cochrane Systematic study 8 showed that progression-free survival (the length of time during and after the treatment of a disease, such as cancer, that a patient lives with the disease but it does not get worse) was significantly higher in the group that received radiofrequency ablation. However, the review was not able to provide information on overall survival. In conclusion, evidence from the included studies are insufficient to recommend radiofrequency ablation for a radical oncological treatment of liver metastases from colorectal cancer.
Radiofrequency ablation is a viable and effective treatment option if you:
- are not a good candidate for surgery because your tumor is difficult to reach.
- have other medical conditions that make surgery especially risky.
- would not have enough liver tissue left for the organ to function adequately following the surgical removal of a tumor.
- have liver tumors that have not responded to chemotherapy or that have recurred after being removed surgically.
- you have several small liver tumors that are too spread out to be removed surgically.
How does radiofrequency ablation work?
Radiofrequency ablation works by passing electrical currents in the range of radiofrequency waves between the needle electrode and the grounding pads placed on the patient’s skin. These currents create heat around the electrode, which when directed into the nerve or tumor, heats and destroys the nerve or cancer cells. At the same time, heat from radiofrequency energy closes small blood vessels and lessens the risk of bleeding. The dead nerve or tumor cells are gradually replaced by scar tissue that shrinks over time.
Radiofrequency ablation preparation
- Arrange to have someone drive you home after the procedure, as you will not be able to drive or operate machinery for at least 24 hours after the radiofrequency ablation procedure.
- Do not eat or drink anything after midnight the night before the procedure, except for a small amount of water if needed to take medications on the day of the radiofrequency ablation procedure.
- If you have diabetes and use insulin, you must adjust the dosage of insulin the day of the procedure. Consult the doctor who manages your insulin or diabetes medication for any necessary adjustments. Bring your diabetes medication with you so you can take it after the radiofrequency ablation procedure.
- If you take any blood thinning medications or antiplatelet medications, these must be stopped with the permission of your doctor who manages these medications.
- Continue to take all other medications with a small sip of water. Bring all medications with you so you can take them after the procedure. It is important to note that you must not stop taking any medication without first consulting with your primary or referring doctor.
Radiofrequency ablation procedure
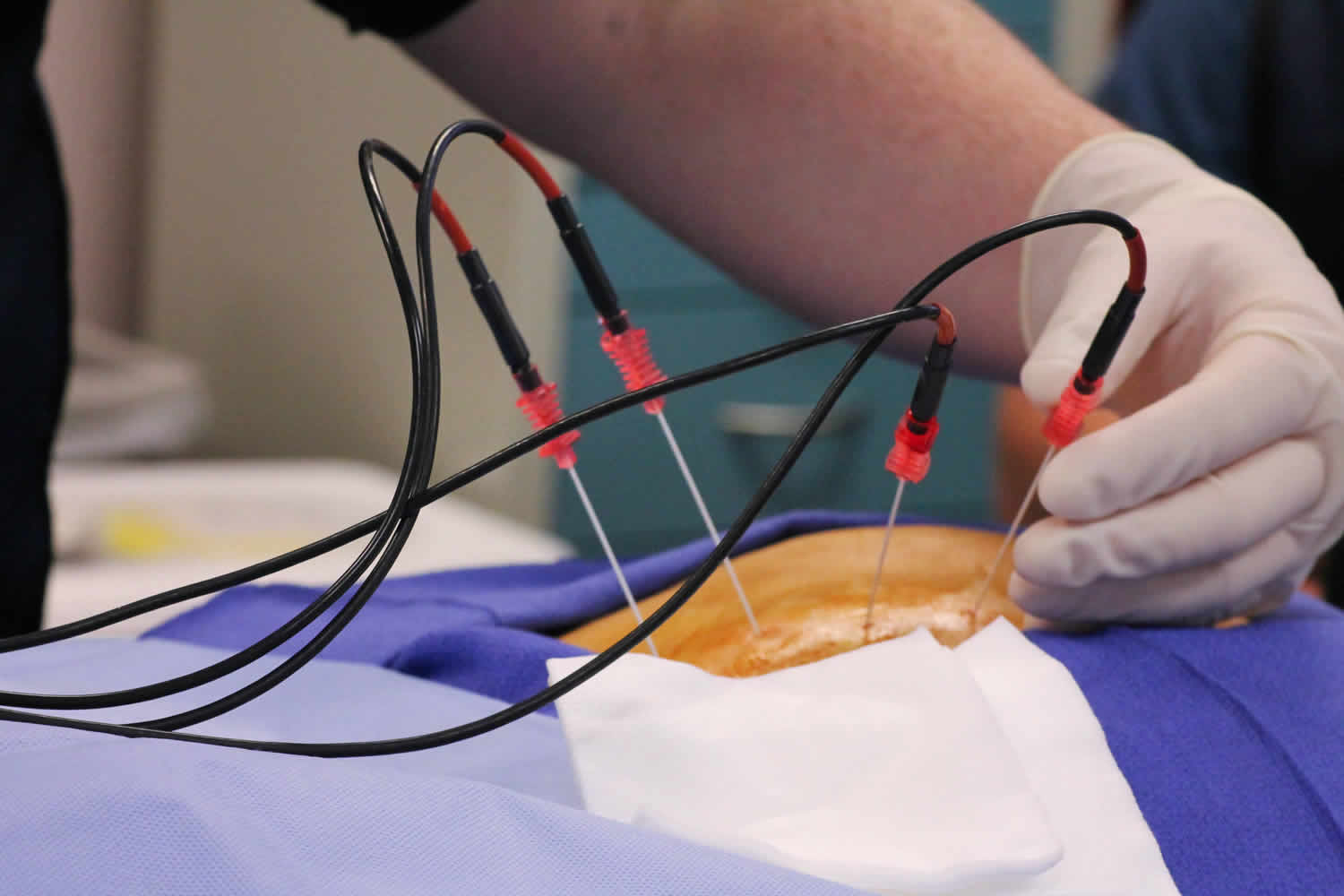
Radiofrequency ablation is a minimally invasive procedure that does not require anesthesia. During the procedure, you will lie on your stomach, or for some neck procedures, on your side. You may have an intravenous (IV) line so we can administer a sedative to relax you.
Your doctor will numb a small area of skin around your spine with an anesthetic. The doctor will then use X-ray guidance to direct a special radiofrequency needle alongside the targeted nerves. There are two types of needle electrodes: simple straight needles and a straight, hollow needle that contains several retractable electrodes that extend when needed. The radiofrequency generator produces electrical currents in the range of radiofrequency waves. It is connected by insulated wires to the needle electrodes and to grounding pads that are placed on the patient’s back or thigh. To confirm proper position, a small amount of electrical current is passed through a probe placed in the needle to the targeted nerve. At this point, you may experience brief pain or a muscle twitch, which the doctor will discuss with you at the time.
Once proper position is confirmed, more local anesthetic is given to the area where the radiofrequency ablation will be performed. During the procedure, most patients feel either nothing or a mild warm sensation.
Radiofrequency ablation procedure may take one to two hours, depending on the treatment site and number of treatments performed.
What will I experience during and after the radiofrequency ablation procedure?
Devices to monitor your heart rate and blood pressure will be attached to your body.
You will feel a slight pin prick when the needle is inserted into your vein for the intravenous line (IV) and when the local anesthetic is injected. Most of the sensation is at the skin incision site, which is numbed using local anesthetic. You may feel pressure when the catheter is inserted into the vein or artery.
If the procedure is done with sedation, the intravenous (IV) sedative will make you feel relaxed, sleepy and comfortable for the procedure. You may or may not remain awake, depending on how deeply you are sedated.
If you are put under general anesthesia, your throat may be sore after you wake up. This is caused by the breathing tube that was placed in your throat while you were asleep.
Pain immediately following ablation can be controlled by pain medication given through your IV or by injection. Afterward any mild discomfort you experience can be controlled by oral pain medications. Patients may feel nauseous, but this can also be relieved by medication.
You will remain in the recovery room until you are completely awake and ready to return home.
You should be able to resume your usual activities within a few days.
Only about ten percent of patients will still have pain a week following radiofrequency ablation.
Radiofrequency ablation for back pain
Radiofrequency ablation or radiofrequency neurotomy uses heat generated by radio waves to target specific nerves and temporarily turn off their ability to send pain signals. Needles inserted through your skin near the painful area deliver the radio waves to the targeted nerves. Your doctor will use imaging scans during radiofrequency neurotomy to make sure the needles are positioned properly. Radiofrequency ablation is most commonly used for pain in the back, neck and buttocks (sacroiliac joint). It may also be helpful for long-term knee or hip joint pain.
Radiofrequency ablation isn’t a permanent fix for back or neck pain. Studies on the success of treatment have been conflicting. Some people may have modest, short-term pain relief, while others might feel better for several months. Sometimes, the treatment does not improve pain or function at all. For the treatment to work and for you to feel better, it’s important that the nerves targeted by the procedure are the same nerves responsible for your pain.
More than 80% of the global population will experience low back pain at least once in their life 9. At any one time, low back pain is prevalent in 4% to 33% of the population 10. One-half of the adult population in the United States report having experienced low back pain within the previous year, and one-quarter report experiencing low back pain in the previous three months 11. Low back pain is responsible for significant resource utilization; it has been estimated that this condition costs more than $100 billion per year in the United States, primarily due to lost productivity and wages 12.
Low back pain can originate from the lumbar facet joints, the sacroiliac joint, the intervertebral discs (discogenic low back pain) and the coccyx. While there is no standardized definition 13, chronic low back pain is typically defined as pain in the low back that persists for ≥3 months, while acute low back pain is typically defined as pain lasting for <3 months 14. Of the population with acute low back pain, approximately 2% to 34% will eventually experience chronic low back pain 15.
Conservative treatment options for chronic low back pain may include pharmaceuticals, manual therapy (eg, massage, physiotherapy, spinal manipulation), exercise therapy (eg, aerobic activity, muscle strengthening), and educational or psychological therapies (eg, cognitive behavioural therapy, support groups, educational sessions) 16. A systematic review of randomized controlled trials, which assessed conservative treatment options for low back pain, found strong evidence for the use of muscle relaxants, manipulation, education (‘back school’) and exercise therapy 17. If conservative treatments are unsuccessful, more invasive methods, such as steroid injections, nerve blocks, cryoablation, radiofrequency ablation (radiofrequency ablation) or surgery, can be attempted 17.
First used to treat low back pain by Shealy 18 in 1975, radiofrequency ablation is a procedure that may offer low back pain relief for patients without a known pathology (infection, tumor, fracture or osteoporosis). During the procedure, a high-frequency electrical current runs through an insulated needle. At the tip of the needle, the electric field causes molecule movement which, in turn, produces thermal energy. The heat from the tip of the radiofrequency ablation device is targeted to create a small lesion within a nerve, which disrupts the pain signal. Numerous randomized controlled trials and observational studies have been completed assessing the ability of radiofrequency ablation to treat low back pain.
Discogenic back pain
Three studies assessed the use of radiofrequency ablation for treating discogenic back pain using a variety of methods. Two of the included studies used conventional radiofrequency ablation 19, 20 and one used cooled radiofrequency ablation 21. The study using cooled radiofrequency ablation, used a bipolar configuration which was then followed by the standard monopolar configuration 21.
All three studies used diagnostic discography to confirm diagnosis of discogenic low back pain, and only participants with a positive response to this procedure were included in the studies.
Studies used radiofrequency ablation at a temperature between 50°C and 70°C to create the lesion. The three studies reported that the characteristics of patients were not significantly different between the control and intervention groups, with the exception of Barendse et al 19, who reported that those in the intervention group had higher pain and had a longer duration of pain than the control group. Although all three studies used different outcome measures to assess change in pain, all used a 0 to 10 scale.
The two studies, Barendse et al 19 and Kvarstein et al 20, that assessed the efficacy of conventional radiofrequency ablation found no evidence of statistically significant benefit when the intervention group was compared with the control group. A study conducted by Kapural et al 21, which assessed the efficacy of cooled radiofrequency ablation, found evidence of a statistically significant benefit. This study reported a 2.19-point reduction in pain within the intervention group and a 0.6-point reduction in pain in the control group six months postprocedure 21.
Lumbar facet joint pain
Six studies included in the present systematic review assessed the efficacy of radiofrequency ablation in reducing chronic lumbar facet back pain 22, 23, 24, 25, 26, 27. Five studies used continuous radiofrequency ablation 22, 23, 24, 26, 27, and one used a combination of pulsed and continuous radiofrequency ablation (22). All six included studies used conventional radiofrequency ablation, and used diagnostic blocks to confirm diagnosis of lumbar facet joint pain 22, 23, 24, 25, 26, 27. Five of the six studies used 22-gauge cannulas 23, 24, 25, 26, 27 and one study did not report these data 22,. All six studies assessed pain reduction using a visual analogue scale; three used a 0 to 10 scale 26, 27, two used a 0 to 100 scale (16,19) and one study did not report the scale used 25. Five studies reported that there were no statistically significant differences in patient characteristics between the intervention and control groups at baseline 22, 23, 24, 26, 27. Nath et al 24 reported that those who received radiofrequency ablation had more general pain, low back pain and referred pain than those in the control group.
Results from the included studies were mixed as to the efficacy of radiofrequency ablation. Five of the included studies found evidence of statistically significant reductions in pain when comparing radiofrequency ablation with sham 22, 24, 26, 27. One of these studies found a significant effect only in participants who experienced a positive response to diagnostic block; for participants who experienced equivocal response to diagnostic blocks, statistically significant benefit was not found 22. One of the six included studies did not find any evidence of statistically significant improvement; this study found a 0.5 point reduction in pain within the intervention group and a 0.6 point reduction in pain in the control group 23.
Sacroiliac joint pain
Two studies assessed the efficacy of radiofrequency ablation for treating sacroiliac pain 28, 29. Both used continuous, cooled radiofrequency ablation procedures 28, 29. These studies used a 17-gauge cannula and a 4 mm tip length. Cohen et al 28 heated the device to 80°C for 90 seconds, while Patel et al 29 used 60°C heat for 150 seconds. Both studies used a numerical rating scale, with a range of 0 to 10 to assess change in pain. Cohen et al 28 followed participants for six months. Patel et al 29 followed participants for nine months postprocedure, but only presented data for the control group up to three months. Both of these studies reported that there were no statistically significant differences in patient characteristics at baseline between the intervention and controls groups.
These two studies assessing the efficacy of radiofrequency ablation for treating sacroiliac joint pain studies found statistically significant reduction in pain for the intervention group, when compared with the control group 28, 29. Three months post procedure, Cohen et al 28 found a 3.7-point reduction in pain within the intervention group, while the control group experienced only a 0.5-point reduction in pain. Three months postprocedure, Patel et al 29 found a 2.4-point pain reduction in the intervention group, and a 0.8-point pain reduction in the control group.
Lumbar radiofrequency ablation success rate
Eleven sham-controlled randomized controlled trials were found, assessing the efficacy of radiofrequency ablation for discogenic back pain 19, 21, 30, lumbar facet joint pain 23, 29 and sacroiliac joint pain 28, 29. There were no randomized controlled trials investigating the use of radiofrequency ablation for pain in the coccyx region found in the literature. The efficacy of radiofrequency ablation for discogenic back pain remains unclear.
The evidence supports radiofrequency ablation as an efficacious treatment for lumbar facet joint and sacroiliac joint pain with five of six and both of the randomized controlled trials demonstrating statistically significant pain reductions, respectively. The evidence supporting radiofrequency ablation for treatment for discogenic pain is mixed and no randomized controlled trial evidence exists for treatment of the coccyx. However, all the randomized controlled trial data are short-term (<1 year) and do not report clinically meaningful pain reduction or outcomes such as ability to complete daily tasks or return to work. Further evidence should be generated before radiofrequency ablation is widely integrated into evidence-based clinical guidelines.
How you prepare for a lumbar radiofrequency ablation
To determine if you’re a good candidate for radiofrequency neurotomy, your doctor may refer you to a pain specialist or order more tests.
For example, a test may be done to see if the nerves commonly targeted by the procedure are the same nerves responsible for your pain. A small amount of numbing medication is injected into the precise spots where the radiofrequency needles will go. If your pain significantly lessens, radiofrequency treatment at those spots may help you.
However, the doctor may determine a different procedure is needed to help your specific symptoms.
Before the lumbar radiofrequency ablation
Let your doctor know if you take blood-thinning medications. You may need to stop taking them for a period of time before the procedure.
Follow these steps:
- Arrange for someone to drive you home.
- Swallow any necessary medications with clear liquids only and take them as early in the day as possible. Don’t take medications within two hours of your surgery.
- Don’t smoke or use any tobacco products the day of your procedure.
During the lumbar radiofrequency ablation
Radiofrequency neurotomy is an outpatient procedure, so you’ll go home later that same day.
You’ll wear a hospital gown and lie on your stomach on an X-ray table. An intravenous (IV) line will be placed in your arm or hand to deliver medication that will keep you comfortable during the procedure. Numbing medication will be injected into your skin before the radiofrequency needles are inserted.
The doctor will the use a special X-ray machine (fluoroscope) to guide the radiofrequency needles to the precise area — so only the targeted nerve tissue will be treated.
After lumbar radiofrequency ablation
You’ll be taken to another room to rest until you feel ready to go home. You might notice some soreness in the area where the needles were inserted, but this usually goes away in a day or two.
When you get home:
- Use an ice pack on the injection sites if you have discomfort. Place the pack on the sore spot for 20 minutes, three or four times a day, during the first day of your recovery.
- Don’t use a heating pad on the injection sites.
- Avoid baths for two days. You may take a warm shower 24 hours after your procedure.
Radiofrequency ablation recovery time
Most patients can walk around immediately after the procedure. After being monitored for a short time, you can usually leave the office or suite. Someone must drive you home.
After the radiofrequency ablation procedure, you may experience soreness in the targeted area for a few days, which may be relieved by oral medications. Some swelling or bruising may occur where the needle was inserted and this may be reduced by applying a cold pack.
You may experience pain from the procedure for up to 14 days, but this is generally due to the residual effects of the nerve ablation or muscle spasm. Some patients are often up and around and back to work 24 to 72 hours after the procedure. Pain relief is typically experienced within 10 days, although relief may be immediate for some patients and it may take up to three weeks for others for the full effects of radiofrequency ablation to be felt.
Although results vary from patient to patient, the effectiveness of radiofrequency ablation may last from three to 12 months. Often the nerve will eventually regenerate and in some cases, the joint pain may return and radiofrequency ablation may need to be repeated.
Radiofrequency ablation side effects
Common side effects of lumbar radiofrequency ablation include:
- Temporary numbness
- Temporary pain at the procedure site
Rarely, more-serious complications may occur, including:
- Bleeding
- Infection
- Nerve damage
- Leggett LE, Soril LJ, Lorenzetti DL, et al. Radiofrequency ablation for chronic low back pain: A systematic review of randomized controlled trials. Pain Research & Management : The Journal of the Canadian Pain Society. 2014;19(5):e146-e153. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4197759/[↩]
- Lencioni R, Crocetti L, Cioni D. Loco-regional ablative therapies for colorectal metastases. In: Dionigi R editor(s). Recent advances in liver surgery. Austin (USA): Landes Bioscience, 2009:234-41.[↩][↩][↩][↩]
- Lencioni R, Cioni D, Lera J, Rocchi E, Della Pina C, Crocetti L. Radiofrequency ablation: principles and techniques. In: Lencioni R, Cioni D, Bartolozzi C editor(s). Focal liver lesions. Heidelberg (Germany): Springer-Verlag, 2005:307-316.[↩][↩]
- Decadt B, Siriwardena AK. Radiofrequency ablation of liver tumours: systematic review. Lancet Oncology 2004;5(9):550-60.[↩]
- Goode JA, Sabharwal T, Adam A. Percutaneous ablation of hepatic metastases. In: Lencioni R, Cioni D, Bartolozzi C editor(s). Focal liver lesions. Heidelberg: Springer-Verlag, 2005:337-48.[↩]
- Veltri A, Sacchetto P, Tosetti I, Pagano E, Fava C, Gandini G. Radiofrequency ablation of colorectal liver metastases:small size favourably predicts technique effectiveness and survival. Cardiovascular Interventional Radiolology 2008;31:948–56.[↩]
- Gillams AR, Lees WR. Five-year survival following radiofrequency ablation of small, solitary, hepatic colorectal metastases. Journal of Vascular and Interventional Radiology 2008;19:712-7.[↩]
- Cirocchi R, Trastulli S, Boselli C, Montedori A, Cavaliere D, Parisi A, Noya G, Abraha I. Radiofrequency ablation in the treatment of liver metastases from colorectal cancer. Cochrane Database of Systematic Reviews 2012, Issue 6. Art. No.: CD006317. DOI: 10.1002/14651858.CD006317.pub3. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD006317.pub3/full[↩]
- World Health Organization WHO Technical Report Series: The Burden of Musculoskeletal Conditions at the Start of the New Millenium. World Health Organization. 2003[↩]
- World Health Organization Chronic Diseases and Health Promotion. World Health Organization. 2013. http://www.who.int/chp/topics/rheumatic/en/[↩]
- Lawrence R, Felson D, Helmick C, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum. 2008;58:26–35 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3266664/[↩]
- Katz JN. Lumbar disc disorders and low-back pain: Socioeconomic factors and consequences. J Bone Joint Surg Am. 2006;88(Suppl 2):21–4. https://www.ncbi.nlm.nih.gov/pubmed/16595438[↩]
- Andersson GB. Epidemiological features of chronic low-back pain. Lancet. 1999 Aug 14;354:581–5. https://www.ncbi.nlm.nih.gov/pubmed/10470716[↩]
- Office of Communication and Public Liaison. Low Back Pain Fact Sheet. National Institute of Neurological Disorders and Stroke. 2013. https://www.ninds.nih.gov/Disorders/All-Disorders/Back-Pain-Information-Page[↩]
- Steenstra IA, Verbeek JH, Heymans MW, et al. Prognostic factors for duration of sick leave in patients sick listed with acute low back pain: A systematic review of the literature. Occup Environ Med. 2005;62:851–60. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1740930/[↩]
- Savigny P, Watson P, Underwood M. Early management of persistent non-specific low back pain: Summary of NICE guidance. BMJ. 2009;338:61805[↩]
- Towards Optimized Practice Program. Guideline for the Evidence-Informed Primary Care Management of Low Back Pain. Toward Optimized Practice Program. 2011 http://nationalpaincentre.mcmaster.ca/documents/LowerBackPainGuidelineNov2011.pdf[↩][↩]
- Shealy CN. Percutaneous radiofrequency denervation of spinal facets: Treatment for chronic back pain and sciatica. J Neurosurg. 1975;43:448–51. https://www.ncbi.nlm.nih.gov/pubmed/125787[↩]
- Barendse GA, van Den Berg SG, Kessels AH, et al. Randomized controlled trial of percutaneous intradiscal radiofrequency thermocoagulation for chronic discogenic back pain: Lack of effect from a 90-second 70 C lesion. Spine. 2001;26:287–92.[↩][↩][↩][↩]
- Kvarstein G, Mawe L, Indahl A, et al. A randomized double-blind controlled trial of intra-annular radiofrequency thermal disc therapy – a 12-month follow-up. Pain. 2009;145:279–86[↩][↩]
- Kapural L, Vrooman B, Sarwar S, et al. A randomized, placebo-controlled trial of transdiscal radiofrequency, biacuplasty for treatment of discogenic lower back pain. Pain Med. 2013;14:362–73.[↩][↩][↩][↩][↩]
- Gallagher J, Petriccione DVPL, Wedley JR, et al. Radiofrequency facet joint denervation in the treatment of low back pain: A prospective controlled double-blind study to assess its efficacy. Pain Clin. 1994;7:193–8.[↩][↩][↩][↩][↩][↩][↩]
- Leclaire R, Fortin L, Lambert R, et al. Radiofrequency facet joint denervation in the treatment of low back pain: A placebo-controlled clinical trial to assess efficacy. Spine. 2001;26:1411–6.[↩][↩][↩][↩][↩][↩][↩]
- Nath S, Nath CA, Pettersson K. Percutaneous lumbar zygapophysial (Facet) joint neurotomy using radiofrequency current, in the management of chronic low back pain: A randomized double-blind trial. Spine. 2008;33:1291–7.[↩][↩][↩][↩][↩][↩][↩]
- Tekin I, Mirzai H, Ok G, et al. A comparison of conventional and pulsed radiofrequency denervation in the treatment of chronic facet joint pain. Clin J Pain. 2007;23:524–9.[↩][↩][↩][↩]
- van Wijk R, Geurts JWM, Wynne HJ, et al. Radiofrequency denervation of lumbar facet joints in the treatment of chronic low back pain: A randomized, double-blind, sham lesion-controlled trial. Clin J Pain. 2005;21:335–44.[↩][↩][↩][↩][↩][↩][↩]
- van Kleef M, Barendse GA, Kessels A, et al. Randomized trial of radiofrequency lumbar facet denervation for chronic low back pain. Spine. 1999;24:1937–42.[↩][↩][↩][↩][↩][↩][↩]
- Cohen SP, Hurley RW, Buckenmaier CC, et al. Randomized placebo-controlled study evaluating lateral branch radiofrequency denervation for sacroiliac joint pain. Anesthesiology. 2008;109:279–88.[↩][↩][↩][↩][↩][↩][↩]
- Patel N, Gross A, Brown L, et al. A randomized, placebo-controlled study to assess the efficacy of lateral branch neurotomy for chronic sacroiliac joint pain. Pain Med. 2012;13:383–98.[↩][↩][↩][↩][↩][↩][↩][↩]
- Kvarstein G, Mawe L, Indahl A, et al. A randomized double-blind controlled trial of intra-annular radiofrequency thermal disc therapy – a 12-month follow-up. Pain. 2009;145:279–86.[↩]





{kind=link}