
Contents
- Rattlesnake bite
- Rattlesnake bite first aid
- Rattlesnake bite symptoms
- Rattlesnake bite diagnosis
- Rattlesnake bite treatment
Rattlesnake bite
Rattlesnakes are venomous snakes found in varying climates in both North and South America 1 and include snakes in the genera Crotalus and Sistrurus. Rattlesnakes are also known as pit vipers, lanceheads, and Asian pit vipers (genus Trimeresurus) 2. Rattlesnakes primary defense mechanism is to hide, and then rattle their tails and hiss which are meant to scare predators away. When they are further challenged, they bite and envenomate with potentially deadly effects. Knowing the common snakes in your area is important in managing a snake bite appropriately.
The death rate is higher with rattlesnake bites compared to all snake bites. In the United States, approximately 9,000 people per year suffer a snake bite, but only five deaths occur. Interestingly, poison center data shows that one in 736 patients who suffer a rattlesnake bite die 2.
Snake bite wounds usually do not get infected due to the relatively inhibitory effect of the venom on microorganisms. Humans often get bit by stepping on snakes mistakenly or by getting extremely close to them when they are in hiding. Usually, the rattle gives away their presence, but there have been rattlesnakes noted to have a dysfunctional tail, possibly a population selected by humans that kill rattling snakes in highly populated areas. Most deaths related to rattlesnake bites are due to immediate anaphylactic reactions or failure to seek medical attention for anti-venom administration 2. Snakebite is a common complication resulting from improper handling or interaction with snakes for leisure. Unfortunately, it is also common in professional snake handlers 3.
The diagnosis and management of rattlesnake bite is best done with a multidisciplianry team that includes the emergency department physician, toxicologist, poison control, surgeon, internist and an intensivist. Appropriate management should begin in the pre-hospital setting. Facilitate immediate and rapid transport of the patient for evaluation by a qualified medical provider. Immobilize the extremity to reduce the potential dissemination of venom through the lymphatic system, but this should not delay transport. Patients presenting with a snake bite should be stabilized by initially assessing their airway, breathing, and circulation just like any other trauma presentation. All patients must be monitored by the nurse until stable. Those who are asymptomatic may be discharged after a period of observation. Those with signs of envenomation need admission to the ICU for close clinical and biochemical monitoring 4.
The prognosis for rattlesnake bite patients treated promptly is good 2.
Rattlesnake bite first aid
If you are bitten by a rattlesnake, , especially if the area changes color, begins to swell or is painful. Many emergency rooms stock antivenom drugs, which may help you.
For all snake bites including rattlesnakes, call your local emergency services number immediately for an ambulance and provide emergency care including cardiopulmonary resuscitation (CPR) if needed. Apply a pressure immobilization bandage and keep the person calm and as still as possible until medical help arrives.
Avoid washing the bite area because any venom left on the skin can help identify the snake.
If possible, take these steps while waiting for medical help:
- Remain calm and move beyond the snake’s striking distance.
- Remove jewelry and tight clothing before you start to swell.
- Position yourself, if possible, so that the bite is at or below the level of your heart.
- Clean the wound, but don’t flush it with water. Cover it with a clean, dry dressing.
Caution
- Don’t use a tourniquet or apply ice.
- Don’t cut the wound or attempt to remove the venom.
- Don’t drink caffeine or alcohol, which could speed your body’s absorption of venom.
- Don’t try to capture the snake. Try to remember its color and shape so that you can describe it, which will help in your treatment.
DO NOT apply a tourniquet, cut the wound or attempt to suck the venom out.
NOTE: If resuscitation is needed it takes precedence over the pressure immobilization bandage. However the resuscitation team should apply pressure immobilization bandage as soon as possible to potentially minimize further venom flow.
- DO NOT cut or excise the bitten area, or attempt to suck venom from the bite site.
- DO NOT wash the bitten area.
- DO NOT apply an arterial tourniquet. (Arterial tourniquets that cut off circulation to the limb, are potentially dangerous
- DO NOT pick up the snake or try to trap it.
- DO NOT wait for symptoms to appear if bitten. Seek immediate medical attention.
- DO NOT allow the person to become over-exerted. If necessary, carry the person to safety.
- DO NOT apply cold compresses to a snake bite.
- DO NOT apply ice or soak the wound in water.
- DO NOT cut into a snake bite with a knife or razor.
- DO NOT try to suck out the venom by mouth.
- DO NOT give the person stimulants or pain medicines unless a doctor tells you to do so.
- DO NOT give the person anything by mouth.
- DO NOT raise the site of the bite above the level of the person’s heart.
Pressure immobilization bandage
A pressure immobilization bandage is recommended for anyone bitten by a venomous snake. This involves firmly bandaging the area of the body involved, such as the arm or leg, and keeping the person calm and still until medical help arrives.
Follow these steps to apply a pressure immobilization bandage:
- First remove any rings or constricting items, because the affected area may swell.
- Secondly put a pressure bandage over the bite itself. If on a limb, apply a broad pressure bandage over the bite site as soon as possible. The bandage should be firm and tight and you should not be able to easily slide a finger between the bandage and the skin. Elasticized bandages (10-15cm wide) are preferred over crepe bandages, if neither are available, clothing or other material should be used 5.
- Then use a heavy crepe or elasticized roller bandage to immobilize the whole limb. In order to further restrict lymphatic flow and to assist in immobilization of the limb. Start at the fingers or toes of the bitten limb and moving upwards on the limb as far as the body, covering as much of the limb as possible 6. Splint the limb including joints on either side of the bite, to restrict limb movement. The bandage should be applied over existing clothing if possible. The purpose of this bandage is to further restrict lymphatic flow and assist immobilization. (Alternatively, a single bandage may be used to achieve both pressure on the bite site and immobilization of the limb. In this method, the bandage is initially applied to the fingers or toes and extended up the limb as far as possible including the bite site) 7.
- Keep the person and the limb completely at rest. If possible, mark the site of the bite on the bandage with a pen.
- Monitor the person’s vital signs — temperature, pulse, rate of breathing, and blood pressure — if possible. If there are signs of shock (such as paleness), lay the person flat, raise the feet about a foot (30 centimeters), and cover the person with a blanket.
If the bite is not on the limb, firm direct pressure on the bite site may be useful. Do not restrict breathing or chest movement and do not apply firm pressure to the neck or head.
Keep the victim and the limb completely at rest. Bring transport to the victim if possible. Transport the victim to medical care, preferably by ambulance. If alone, the victim should apply the pressure immobilization bandage as completely as possible over the bite site and affected limb. They should keep immobile until medical assistance arrives. If they are unable to obtain urgent help to come to them, then apply local pressure if possible, immobilization is contraindicated and they should move themselves to seek urgent help. Do not remove the bandages or splints before evaluation in an appropriate hospital environment.
Figure 1. Snake bite pressure immobilization bandage


Cardiopulmonary resuscitation (CPR)
How to perform a Cardiopulmonary Resuscitation (CPR) for for children over 1 year
- Step 1: If a child is unconscious, the first step is to check his mouth for anything blocking the airway. This could include his tongue, food, vomit or blood.
- Step 2: If you find a blockage, roll him onto his side, keeping his top leg bent. This is the recovery position. Clear blockages with your fingers, then check for breathing.
- Step 3: If you find no blockages, check for breathing and look for chest movements. Listen for breathing sounds, or feel for breath on your cheek.
- Step 4: If the child is breathing, gently roll him onto his side and into the recovery position. Phone your local emergency services number and check regularly for breathing and response until the ambulance arrives. If the child is not breathing and responding, send for help. Phone local emergency services number and start CPR: 30 chest compressions, 2 breaths.
- Step 5: Put the heels of your hands in the center of the child’s chest. Using the heel of your hand, give 30 compressions. Each compression should depress the chest by about one third.
- Step 6: After 30 compressions, take a deep breath, seal your mouth over the child’s mouth, pinch his nose and give two steady breaths. Make sure the child’s head is tilted back to open his airway.
- Step 7: Keep giving 30 compressions then 2 breaths until medical help arrives. If the child starts breathing and responding, turn him into the recovery position. Keep watching his breathing and be ready to start CPR again at any time.
Figure 2. CPR for for children over 1 year

How to perform a Cardiopulmonary Resuscitation (CPR) on Adults
Hands-only CPR
To carry out a chest compression:
- Place the heel of your hand on the breastbone at the centre of the person’s chest. Place your other hand on top of your first hand and interlock your fingers.
- Position yourself with your shoulders above your hands.
- Using your body weight (not just your arms), press straight down by 5-6cm (2-2.5 inches) on their chest.
- Keeping your hands on their chest, release the compression and allow the chest to return to its original position.
- Repeat these compressions at a rate of 100 to 120 times per minute until an ambulance arrives or you become exhausted.
When you call for an ambulance, telephone systems now exist that can give basic life-saving instructions, including advice about CPR. These are now common and are easily accessible with mobile phones.
Cardiopulmonary Resuscitation (CPR) with rescue breaths
If you’ve been trained in CPR, including rescue breaths, and feel confident using your skills, you should give chest compressions with rescue breaths. If you’re not completely confident, attempt hands-only CPR instead (see above).
Adults
- Place the heel of your hand on the center of the person’s chest, then place the other hand on top and press down by 5-6cm (2-2.5 inches) at a steady rate of 100 to 120 compressions per minute.
- After every 30 chest compressions, give two rescue breaths.
- Tilt the casualty’s head gently and lift the chin up with two fingers. Pinch the person’s nose. Seal your mouth over their mouth and blow steadily and firmly into their mouth for about one second. Check that their chest rises. Give two rescue breaths.
- Continue with cycles of 30 chest compressions and two rescue breaths until they begin to recover or emergency help arrives.
Anaphylactic shock
Snake bites can be painful. Occasionally some people have a severe allergic reaction to being bitten. In cases of severe allergic reaction, the whole body can react within minutes to the bite which can lead to anaphylactic shock. Anaphylactic shock is very serious and can be fatal.
Anaphylaxis is a severe and potentially life-threatening reaction to a trigger such as an allergy.
- Anaphylaxis is a medical emergency that requires immediate medical assistance and treatment.
- Anaphylaxis can occur within seconds or minutes of exposure to something you’re allergic to, such as peanuts or bee stings.
Anaphylaxis causes your immune system to release a flood of chemicals that can cause you to go into shock — your blood pressure drops suddenly and your airways narrow, blocking breathing. Signs and symptoms include a rapid, weak pulse; a skin rash; and nausea and vomiting. Common triggers include certain foods, some medications, insect venom and latex.
Anaphylaxis requires an injection of epinephrine and a follow-up trip to an emergency room. If you don’t have epinephrine, you need to go to an emergency room immediately. If anaphylaxis isn’t treated right away, it can be fatal.
Symptoms of anaphylactic shock may include:
- Trouble breathing or noisy breathing
- Difficulty talking more than a few words and/or hoarse voice
- Wheeze
- Cough
- Swelling and tightness of the throat
- Collapse
- Light-headedness or dizziness
- Diarrhea
- Tingling in the hands, feet, lips or scalp
- Swelling of tongue
- Pale and floppy (in young children)
Call your local emergency services number for an ambulance. If the person has a ‘personal action plan’ to manage a known severe allergy, they may need assistance to follow their plan. This may include administering adrenaline to the person via an autoinjector (such as an Epipen®) if one is available.
How to use Adrenaline auto-injectors
People with potentially serious allergies will often be given an adrenaline auto-injector to carry at all times. This can help stop an anaphylactic reaction becoming life threatening.
This should be used as soon as a serious reaction is suspected, either by the person experiencing anaphylaxis or someone helping them.
If you’ve been given an auto-injector, make sure you’re aware how to use it correctly.
There are three main types of adrenaline auto-injector, which are used in slightly different ways.
These are:
- EpiPen – see Figure 1 on how to use Epipen
- Jext
- Emerade
Instructions are also included on the side of each injector if you forget how to use it or someone else needs to give you the injection.
Figure 3. How to use the Epipen
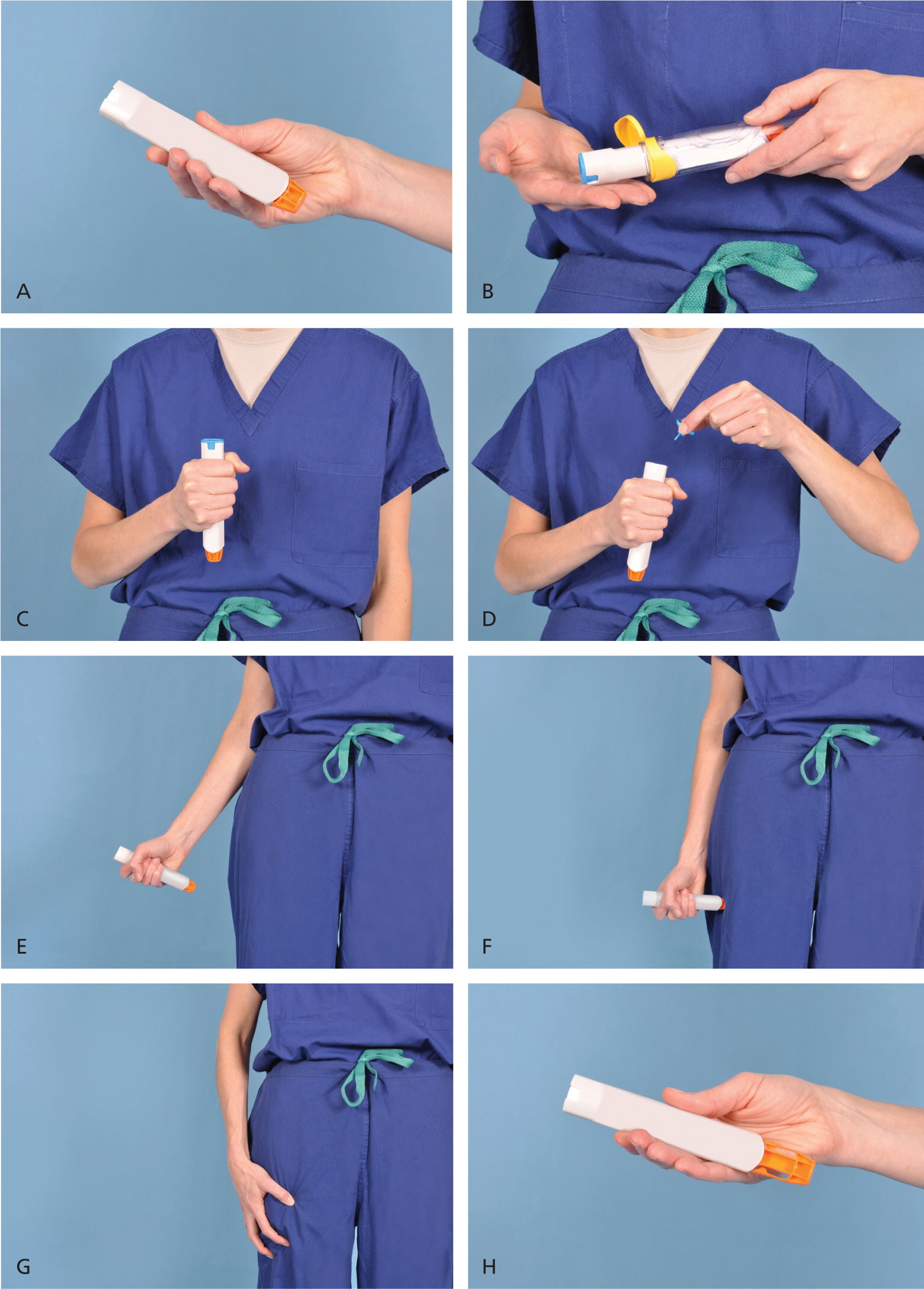
Demonstration of appropriate deployment of the (A) Epipen (released in 2008). For demonstration purposes, a trainer device is being used instead of a live device; however, the coloring of key components is the same as the actual adult device. (B) Open the yellow cap of the carrying case and remove the device from its storage tube (the Epipen Jr. has a green cap). (C) Grasp and form a fist around the unit with the orange tip facing down. (D) With the other hand, remove the blue safety release. (E) Aim the orange tip toward the outer thigh. (F) Swing the arm and jab the device firmly into the outer thigh, at a 90-degree angle, until the device clicks. The needle will deploy at this time into thigh (the autoinjector is designed to work through clothing). Hold the device firmly against the thigh for 10 seconds, so the entire dose will be delivered. (G) Remove the device from the thigh and massage the injection area for 10 seconds. (H) The safety feature of the device, extension of the orange tip that locks into place, will completely cover the needle immediately after use. The used device should be taken to the hospital emergency department with the patient for disposal.
Rattlesnake bite symptoms
The symptoms from a snake bite are related to the envenomation. Rattlesnakes have hollow fangs in the anterior mouth that inject venom into subcutaneous tissue. Rarely, intravenous injection occurs, but when it does, it is usually deadly. Crotalid venom causes necrosis due to toxic tissue enzymes. It also causes increased permeability of the cell membrane, which leads to an increased spread of the venom locally. Crotalid venom has a fibrinolytic and protein C activation effect causing coagulopathy in patients. Certain rattlesnakes, such as timbers, have a higher incidence of angioedema. The mechanism by which angioedema associated with timber rattlesnake envenomation occurs is not understood. The incidence of angioedema in patients suffering from timber rattlesnake bites is high and found to be 66% in one study.
There are two neurotoxins found in rattlesnakes. One is an enzyme phospholipase A2 which decreases the LD50 (lethal dose 50 is the amount of a venom or poison that kills 50 percent of a test sample) of rattlesnake venom by ten to 80 times, and the other is canebrake toxin. Both of these toxins inhibit neuromuscular transmission by blocking Ca2+ (calcium) channels on the presynaptic side of the neuromuscular junction. This may lead to paralysis of a muscle group if it is present in high concentrations. This toxin is also found to induce myokymia, which is an involuntary quivering of muscles or muscle fibers in localized areas.
Rattlesnake bite victims may present with a variety of local and systemic symptoms. Local symptoms include pain and swelling around the bite site, bleeding from the bite site, and local tissue necrosis and ecchymosis. Systemic symptoms include angioedema, bleeding from other orifices including hematemesis and hematochezia, nausea, vomiting, diarrhea, dyspnea, and anaphylaxis 8.
Rattlesnake bite diagnosis
Initial lab tests are necessary for all snake bites and should include coagulation studies, hemoglobin, platelets, and fibrinogen. While an x-ray of the bite wound is not necessary, it may be prudent if there is a suspicion of a foreign body or a fracture that may have occurred while escaping the snake. Upon initial evaluation, the leading edge of the swelling and redness surrounding the bite site should be marked. Grading the envenomation determines the use of antivenin.
Minimal Envenomation (no antivenin)
- Swelling, pain, and ecchymosis limited to the site of the bite
- No systemic signs
- Normal coagulation parameters or isolate mild alterations without clinically relevant bleeding
Moderate Envenomation
- Swelling, pain and ecchymosis involving less than full extremity or extending < 50 cm in adults
- Systemic symptoms present, such as vomiting, mild hypotension, mild tachycardia
- Abnormal coagulation parameters without clinically relevant bleeding
Severe Envenomation
- Swelling, pain, and ecchymosis involving an entire extremity (or more) or threatening airway
- Systemic signs including altered mental status and hemodynamic instability
- Abnormal coagulation parameters with clinically relevant bleeding.
Progression of angioedema is unpredictable as it may progress beyond presentation or may start regressing soon after presentation 9. Elevated protime and/or decreased platelets and fibrinogen levels are also signs of envenomation. Coagulopathy responds to antivenin treatment, but the thrombocytopenia may persist 10. Life-threatening bleeding is rare despite severe coagulopathy and thrombocytopenia. Platelet or fresh frozen plasma (FFP) transfusion should be avoided except when there is life-threatening bleeding because antivenin is the definitive treatment.
If no signs of envenomation are present, the patient should be observed for at least six hours, and labs should be repeated before discharge. If the patient develops signs during the observation period or presents with signs of envenomation, erythema and swelling should be marked, measured, and tracked for progression. Prophylactic antibiotics are not indicated for snake bites as they have an extremely low likelihood of infection owing to the proteolytic properties of snake venom.
Rattlesnake bite treatment
Appropriate management should begin in the pre-hospital setting. Facilitate immediate andrapid transport of the patient for evaluation by a qualified medical provider. Immobilize the extremity to reduce the potential dissemination of venom through the lymphatic system, but this should not delay transport. Patients presenting with a snake bite should be stabilized by initially assessing their airway, breathing, and circulation just like any other trauma presentation. Some patients may be able to identify the snake that bit them, but this may not always be accurate. Knowing the common snakes in the locality of the patient may help elucidate the likely culprit. In any case, the treatment algorithm for snake envenomation does not change drastically depending on the snake.[4][5][6][7]
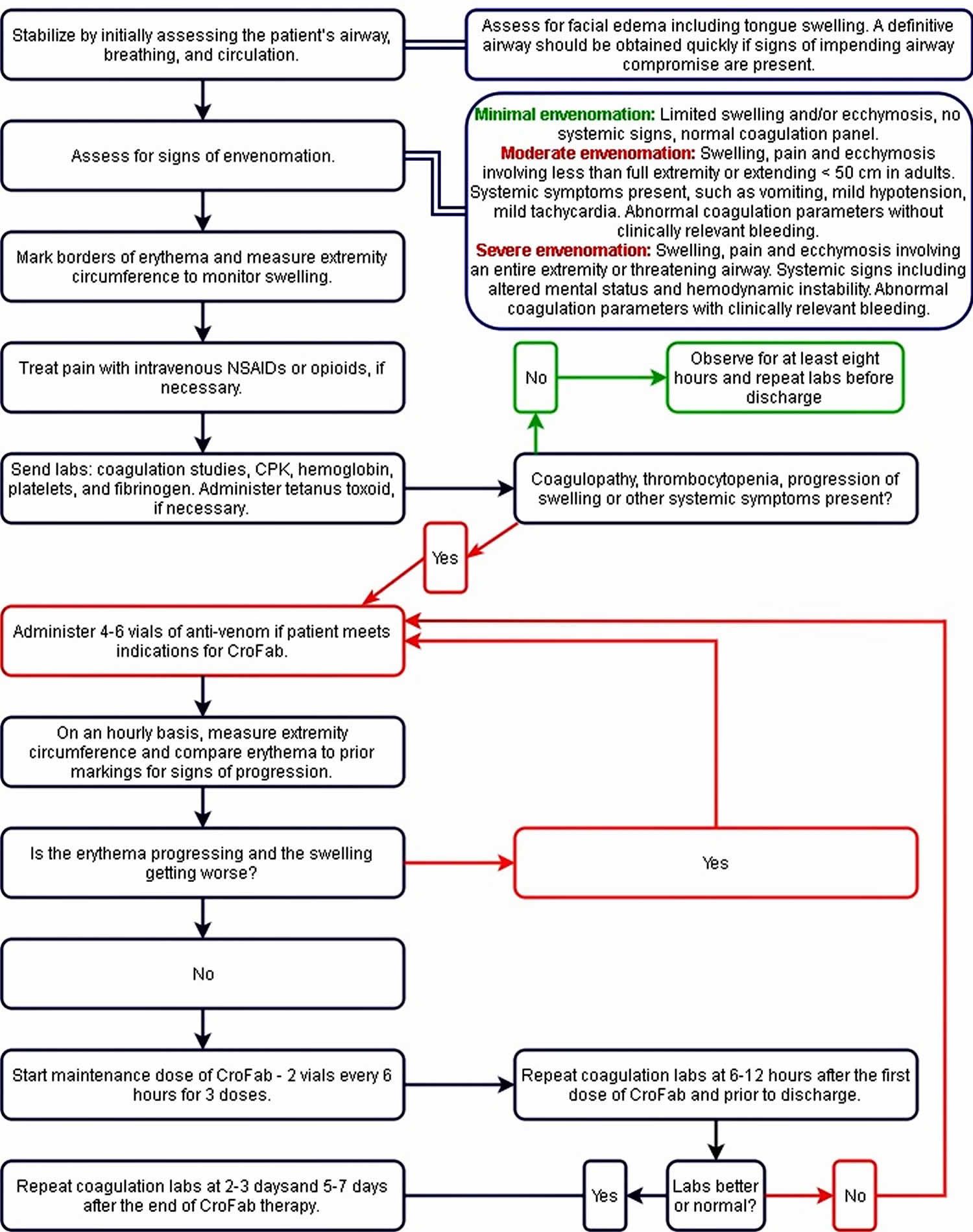
Please refer to the management algorithm attached for a step-by-step approach to crotaline envenomation.
The leading edge of the swelling and redness surrounding the bite site should be marked and tracked every 15 min-30 min. The extremity should be immobilized to reduce motion, and pain should be treated with IV opioids if necessary. Initial labs are necessary for all snake bites and should include coagulation studies, hemoglobin, platelets, and fibrinogen. Tetanus should be updated if necessary, and the local poison center should be notified.
Signs of envenomation may vary between presentations but should be assessed in all snake bite victims. Systemic signs include hypotension, bleeding or oozing from IV sites, vomiting, diarrhea, angioedema and neurotoxicity. Assessment for facial edema including tongue swelling and respiratory distress should be recognized, and a definitive airway should promptly be obtained if there are concerns for airway compromise.
A patient with minimal signs of envenomation should be monitored for at least eight hours and should get a repeat coagulation panel before discharge.
Crotalidae polyvalent immune Fab (CroFab) Dosing
Initial bolus four to six vials mixed in 250 mL normal saline administered over one hour (same number of vials in less fluid for children). Initiate treatment with a bolus of 10 mL/hr observing for adverse effects. If none, then increase every few minutes to achieve complete administration in one hour. Observe patient for local swelling and systemic symptoms. If signs of progression then repeat with four to six vials over one hour. Do not administer to normalize abnormal coagulation markers. Repeat until initial control is achieved (local swelling improves or stops, resolution of systemic signs, and resolution of clinically relevant bleeding. After achieving control, maintenance doses of two vials every six hours for 18 hours are recommended for rattlesnakes, patients with a coagulopathy, and those with severe clinical envenomations. This is not usually required for moderate copperhead envenomations. Remember that if recurrent swelling or coagulopathy occurs during maintenance doses, reduce with bolus protocol.
Recheck coagulation labs prothrombin time (PT), fibrinogen, platelets, and hemoglobin at day two to three and days five to seven. Recurrent coagulopathy without clinically significant bleeding has been observed. Some retreat and others follow parameters to normalization.
Consider contacting a Poison Control Center (https://www.poisonhelp.org/help) to discuss with a medical toxicologist.
Figure 1. Rattlesnake treatment algorithm
Overall Indications for Crotalidae polyvalent immune Fab (CroFab)
- Indicated for moderate or severe envenomations only, not minimal
- Swelling that is progressing and is more than minimal
- Any systemic symptoms
- Any coagulopathy such as increased protime, or decreased platelet count or fibrinogen
CroFab will help local symptoms and coagulopathy, and local symptoms are used to monitor response to therapy. Cessation in the progression of swelling and erythema is reassuring.
Worsening angioedema is not a sign of the failure of treatment with CroFab. CroFab is not expected to reduce or stop the progression of angioedema. Typically, the angioedema resolves with supportive care.
Coagulation studies will improve with CroFab treatment, but persistent thrombocytopenia has been noted despite CroFab treatment and is not considered the failure of treatment. Other systemic signs are expected to improve with treatment as well. Local swelling and pain may persist for weeks to months despite CroFab therapy. CroFab is contraindicated in a patient with known allergy to sheep protein. CroFab use is associated with an 8% incidence of immediate hypersensitivity and a 13% incidence of serum sickness (which is rare and almost always clinically insignificant).
- O’Neil ME, Mack KA, Gilchrist J, Wozniak EJ. Snakebite injuries treated in United States emergency departments, 2001-2004. Wilderness Environ Med. 2007 Winter;18(4):281-7[↩]
- Patel V, Hamilton RJ. Rattle Snake Toxicity. [Updated 2019 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431065[↩][↩][↩][↩][↩]
- Walter FG, Stolz U, Shirazi F, McNally J. Epidemiology of severe and fatal rattlesnake bites published in the American Association of Poison Control Centers’ Annual Reports. Clin Toxicol (Phila). 2009 Aug;47(7):663-9[↩]
- Wigginton JB. Snake, rattle, and roll. J Miss State Med Assoc. 2013 Mar;54(3):64-5.[↩]
- Canale E, Isbister GK, Currie BJ. Investigating pressure bandaging for snakebite in a simulated setting: bandage type, training and the effect of transport. Emergency Medicine Australasia 2009; 21: 184-190.[↩]
- Howarth DM, Southee AE, Whyte IM. Lymphatic flow rates and first-aid in simulated peripheral snake or spider envenomation. Medical Journal of Australia 1994; 161: 695-700.[↩]
- Sutherland SK, Tibballs J. Australian Animal Toxins. Melbourne: Oxford University Press 2001.[↩]
- Lavonas EJ, Ruha AM, Banner W, Bebarta V, Bernstein JN, Bush SP, Kerns WP, Richardson WH, Seifert SA, Tanen DA, Curry SC, Dart RC., Rocky Mountain Poison and Drug Center, Denver Health and Hospital Authority. Unified treatment algorithm for the management of crotaline snakebite in the United States: results of an evidence-informed consensus workshop. BMC Emerg Med. 2011 Feb 03;11:2[↩]
- Rodriguez-Acosta A, Aguilar I. Toxoid preparation from the venom of Crotalus durissus cumanensis (South American rattle snake). J Trop Med Hyg. 1987 Feb;90(1):39-43[↩]
- Brazil OV. Neurotoxins from the South American rattle snake venom. Taiwan Yi Xue Hui Za Zhi. 1972 Jul 28;71(6):394-400[↩]





{kind=link}