Contents
Renal artery stenosis
Renal artery stenosis is a narrowing or blockage of the renal arteries that supply blood to your kidneys. “Renal” means kidney and “stenosis” means narrowing”. The most common cause of renal artery stenosis is a blockage in one or more of the renal arteries. Renal artery stenosis most often occurs when a sticky, fatty substance called plaque builds up on the inner lining of the renal arteries, causing a condition known as atherosclerosis. When the renal arteries that carry blood to your kidneys become narrow, less blood flows to the kidneys. Your kidneys need adequate oxygen-rich blood flow to help filter waste products and remove excess fluids. Reduced blood flow to your kidneys may injure the kidney tissue and increase blood pressure throughout your body. Your kidneys mistakenly respond to the reduced blood flow as if your blood pressure is low. As a result, your kidneys release a hormone called renin that converts angiotensinogen to angiotensin 1. Angiotensin 1 has to be converted to angiotensin 2 with the help of an angiotensin-converting enzyme (ACE) in your lungs. Angiotensin 2 is responsible for the narrowing (constriction) of blood vessels and release of aldosterone which tells the body to hold on to more salt (sodium) and water, thus resulting in secondary hypertension 1.
Renal artery stenosis often doesn’t cause any signs or symptoms until it’s advanced. Renal artery stenosis may be discovered incidentally during testing for something else. In general, people with renal artery stenosis may have a history of very high blood pressure that is hard to bring down with medicines.
Symptoms of renal artery stenosis include:
- High blood pressure at a young age before age 30 or after age 50
- High blood pressure that begins suddenly or worsens without explanation
- High blood pressure that suddenly gets worse or is hard to control
- Kidneys that are not working well (this can start suddenly)
- Elevated protein levels in your urine or other signs of a problem with kidney function
- Worsening kidney function during treatment for high blood pressure
- A whooshing sound as blood flows through a narrowed vessel (bruit), which your doctor hears through a stethoscope placed over your kidneys
- Narrowing of other arteries in the body, such as to the legs, the brain, the eyes and elsewhere
- Fluid overload and swelling in your body’s tissues
- Sudden buildup of fluid in the air sacs of your lungs (pulmonary edema)
- Treatment-resistant heart failure
If you have a dangerous form of high blood pressure called malignant hypertension, symptoms can include:
- Bad headache
- Nausea or vomiting
- Confusion
- Changes in vision
- Nosebleeds
To diagnose renal artery stenosis, your doctor may hear a “whooshing” noise, called a bruit, when placing a stethoscope over your belly area.
The following blood tests may be done:
- Cholesterol levels
- Renin and aldosterone levels
- Blood urea nitrogen (BUN)
- Creatinine
- Potassium
- Creatinine clearance
Imaging tests may be done to see if the kidney arteries have narrowed. They include:
- Angiotensin converting enzyme (ACE) inhibition renography
- Doppler ultrasound of the renal arteries
- Magnetic resonance angiography (MRA)
- Renal artery angiography.
High blood pressure caused by renal artery stenosis is often hard to control. If your blood pressure is moderately or severely elevated, a healthy lifestyle such as limiting salt in your diet, eating healthy foods and getting regular physical activity — can help control your blood pressure.
Your doctor may also recommend that you:
- Maintain a healthy weight. When your weight increases, so does your blood pressure. If you’re overweight, losing weight may help to lower your blood pressure.
- Restrict salt in your diet. Salt and salty foods cause your body to retain fluid. This may increase the volume of your blood and, in turn, increase your blood pressure.
- Be physically active. Being physically active on a regular basis may help you lose weight, lower your risk of heart disease, lower your cholesterol and lower your blood pressure. Check with your doctor before beginning an exercise program, especially if you have high blood pressure and haven’t been active in the past.
- Reduce stress. Lowering stress levels may decrease your blood pressure.
- Drink alcohol in moderation, if at all. Too much alcohol may increase your blood pressure.
- Don’t smoke. Tobacco injures blood vessel walls and speeds up the process of hardening of the arteries. If you smoke, ask your doctor to help you quit.
High blood pressure even when mainly related to renal artery stenosis can often be successfully treated with medications. One or more medicines are needed to help control blood pressure. There are many types available. Finding the right medication or combination of medications may require time and patience.
Some medications commonly used to treat high blood pressure associated with renal artery stenosis include:
- Angiotensin-converting enzyme (ACE) inhibitors and angiotensin 2 receptor blockers (ARBs), which help relax your blood vessels and block the formation or effects of a natural body chemical called angiotensin 2, which narrows blood vessels
- Diuretics also known as water pills, which help your body eliminate excess sodium and water
Beta blockers and alpha-beta blockers, which may have the effect of making your heart beat slowly and less forcefully or widening (dilating) your blood vessels, depending on which medication you use - Calcium channel blockers, which help relax blood vessels
If atherosclerosis is the underlying cause of renal artery stenosis, your doctor may also recommend aspirin and a cholesterol-lowering medication. Which medications are best for you depends on your individual situation.
Further treatment depends on what causes the narrowing of the kidney arteries. Your doctor may recommend a procedure called angioplasty with stenting. These procedures may be an option if you have:
- Severe narrowing of the renal artery
- Blood pressure that cannot be controlled with medicines
- Kidneys that are not working well and are becoming worse
However, the decision about which people should have these procedures is complex, and depends on many of the factors.
Figure 1. Kidney anatomy
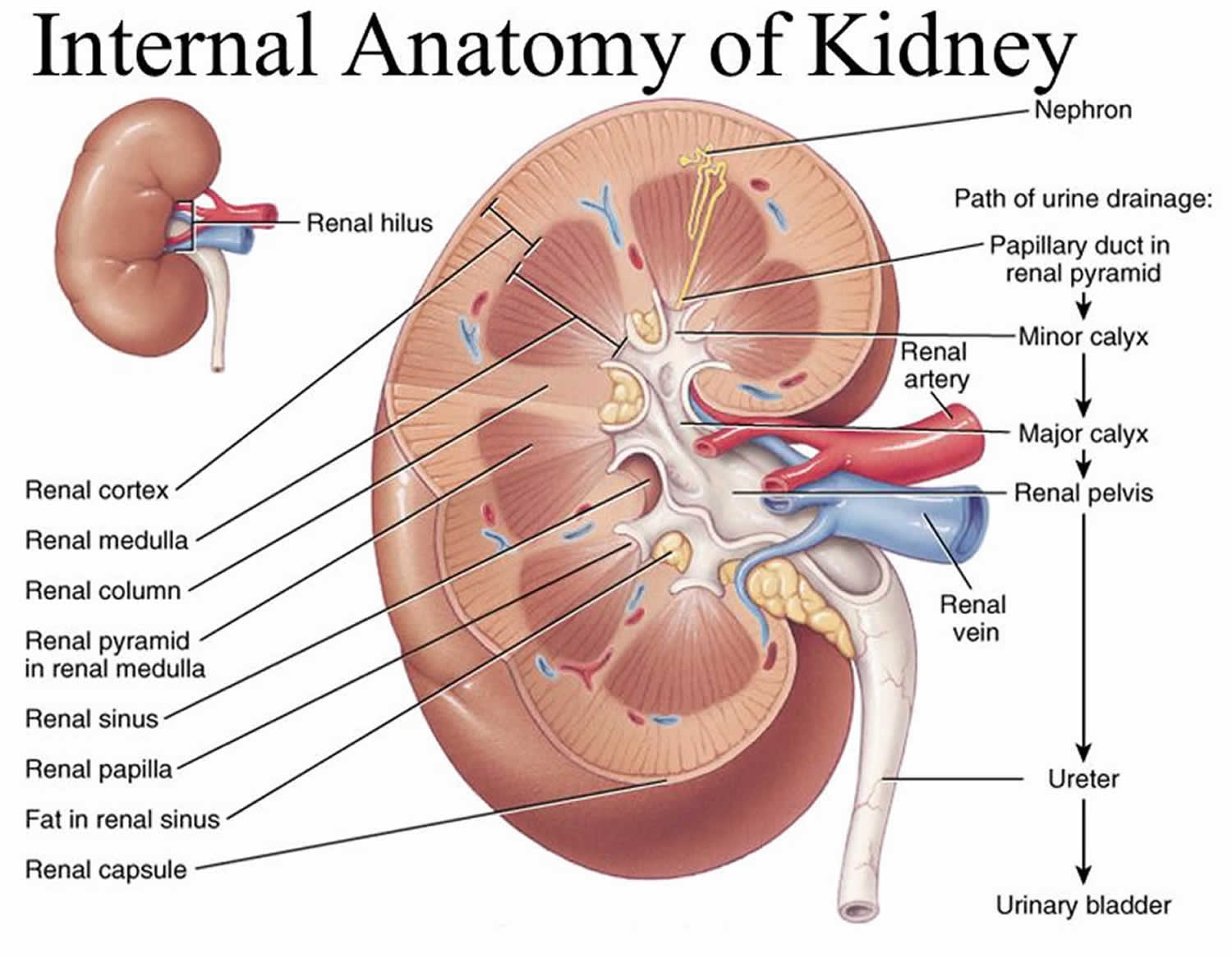
Figure 2. Renal artery anatomy
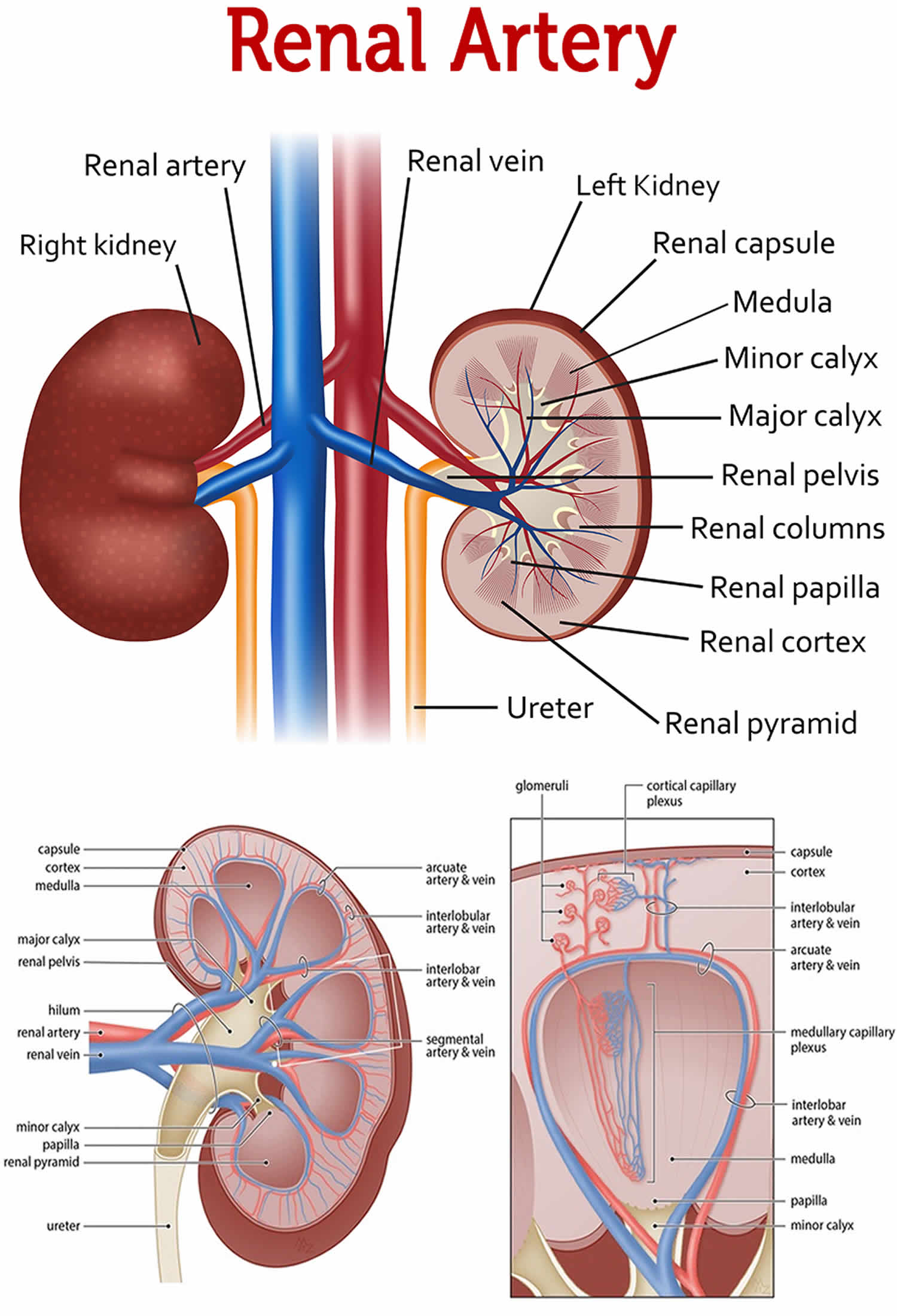
Figure 3. Renal artery stenosis
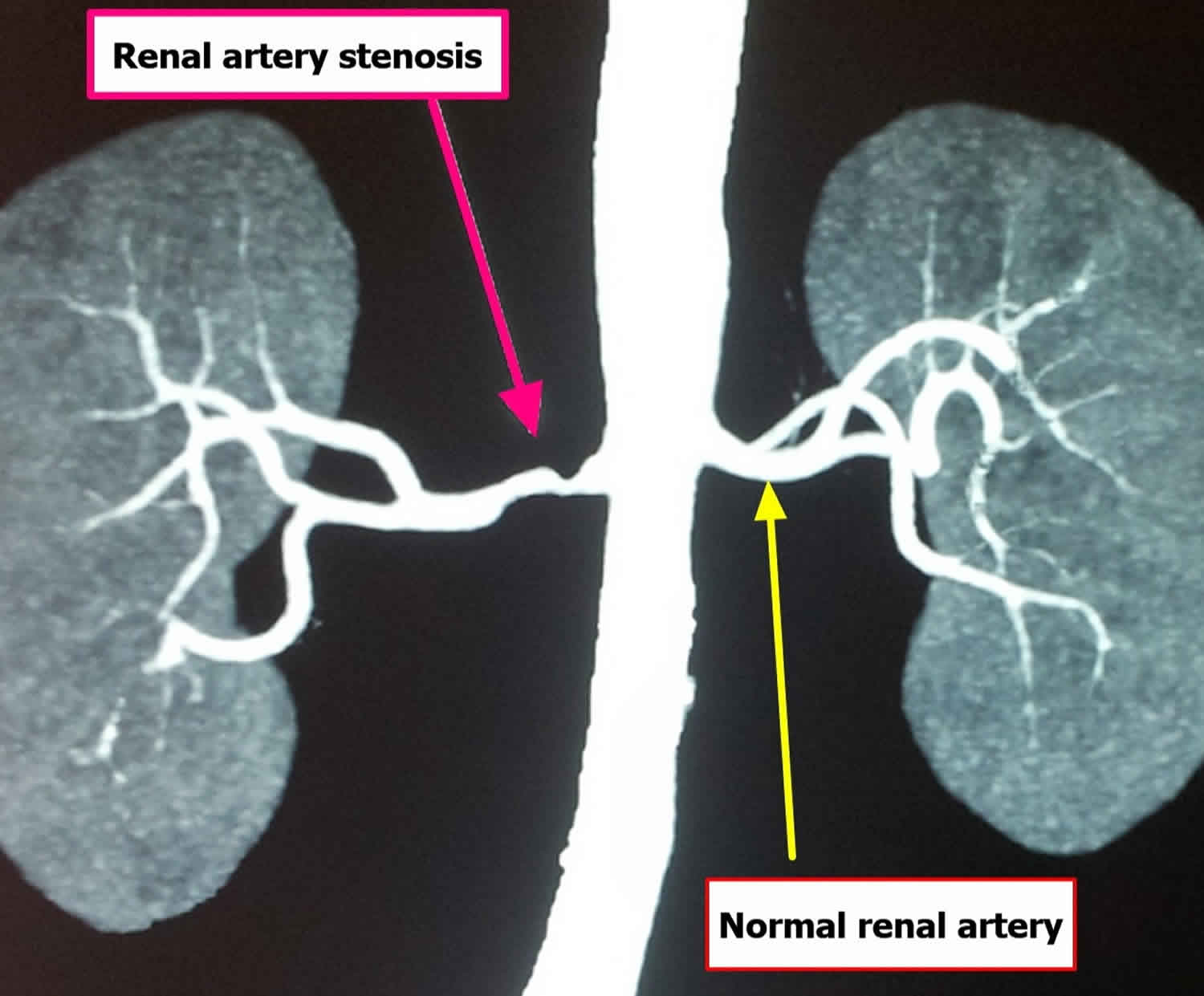
Figure 4. Fibromuscular dysplasia renal artery stenosis
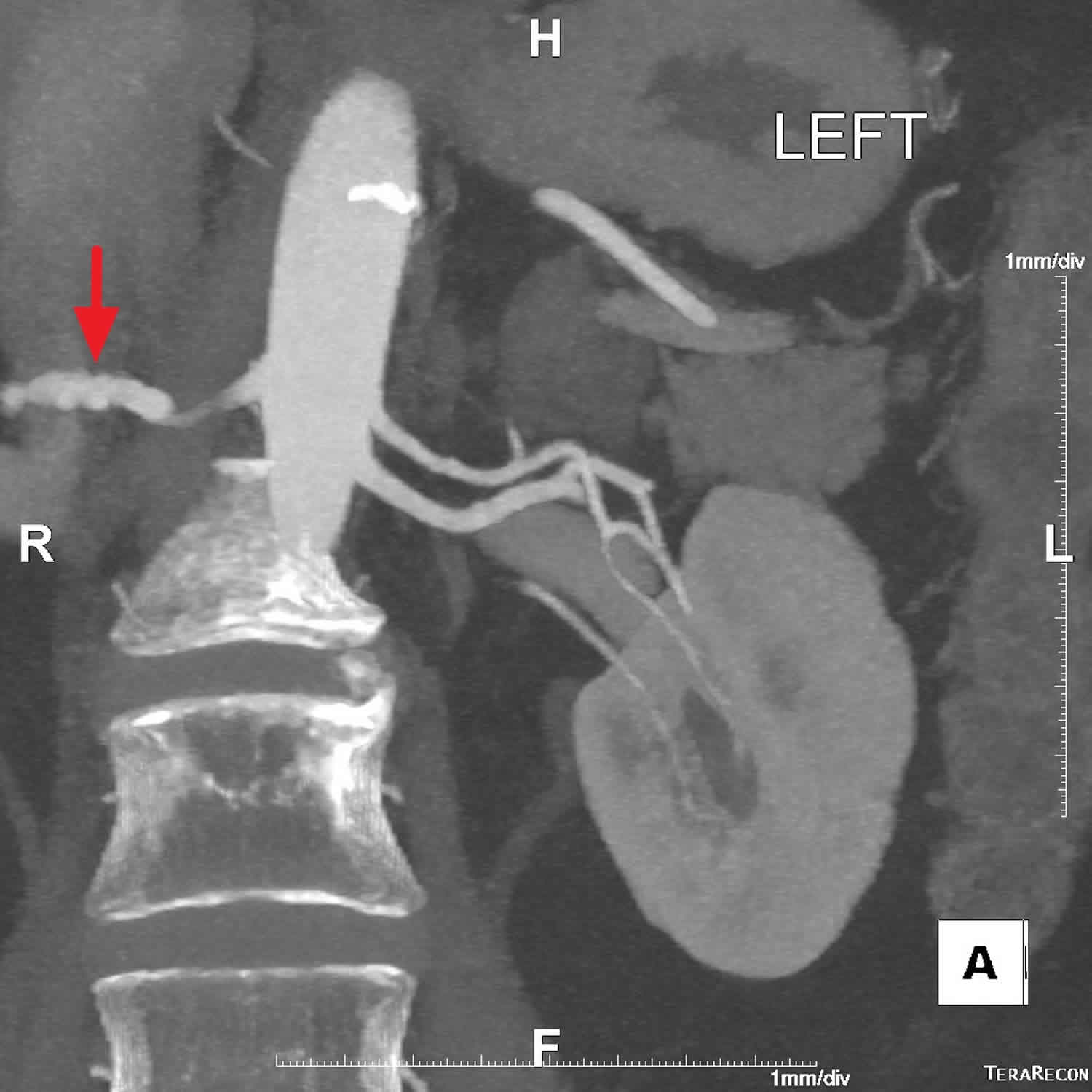
Footnote: Extensive beading or undulation of the entire main right renal artery. Probable tiny saccular aneurysm projecting posteriorly from a segmental branch in the interpolar region. Less pronounced, mildly beaded appearance of the main and accessory left renal arteries. No dissection or aneurysm. Possible mild ectasia of the celiac trunk. Normal adrenals. It is appropriate to recommend cervical and intracranial angiography after this examination, as a complication related to disease in the head and neck could result in the most devastating consequences for this patient and would direct more aggressive therapy if indicated.
[Source 2 ]Figure 5. Renal artery fibromuscular dysplasia progression
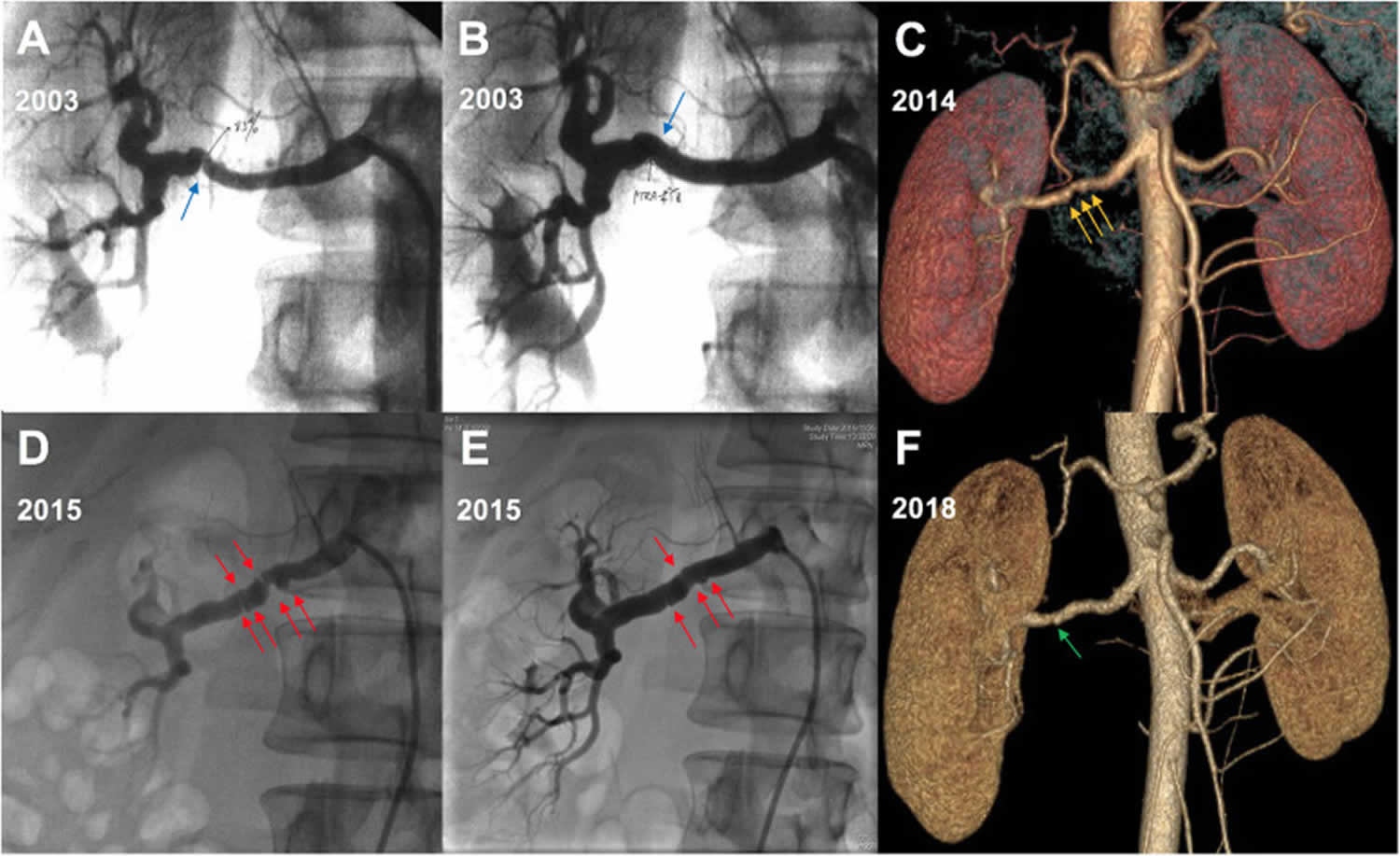
Footnote: Renal artery fibromuscular dysplasia progression in a 24-year-old female patient with refractory hypertension. (A) The first catheter angiography revealed distal unifocal stenosis of the right renal artery. (B) The renal artery stenosis was relieved after percutaneous transluminal angioplasty. (C) Computed tomographic angiography showed new middle multiple stenoses of the same renal artery. (D) The second catheter angiography confirmed a middle typical string-of-beads appearance of the right renal artery without the distal unifocal stenosis. (E) The renal artery stenosis was relieved after percutaneous transluminal angioplasty again. (F) Computed tomographic angiography at the last follow-up showed the normal right renal artery.
[Source 3 ]Who is at risk for renal artery stenosis?
People at risk for atherosclerosis are also at risk for renal artery stenosis. Risk factors for renal artery stenosis caused by atherosclerosis include:
- high blood cholesterol levels
- high blood pressure
- smoking
- insulin resistance
- diabetes
- being overweight or having obesity
- lack of physical activity
- a diet high in fat, cholesterol, sodium, and sugar
- being a man older than 45 or a woman older than 55
- a family history of early heart disease
The risk factors for renal artery stenosis caused by fibromuscular dysplasia are unknown, but fibromuscular dysplasia is most common in women and people 25 to 50 years of age 4. Fibromuscular dysplasia can affect more than one person in a family, indicating that it may be caused by an inherited gene.
Renal artery stenosis causes
The two main causes of renal artery stenosis include 5, 6:
- Atherosclerosis (~75 to 90% of cases) involving the proximal renal artery 7. Atherosclerosis is the buildup of fats, cholesterol, calcium and other substances (plaque) in and on your kidney artery walls (renal arteries). Plaque buildup is what makes the artery wall hard and narrow. As these deposits get larger, they can harden, reduce blood flow, cause kidney scarring and eventually narrow the renal artery. Atherosclerosis occurs in many areas of your body and is the most common cause of renal artery stenosis. Risk factors for atherosclerosis include:
- High blood pressure
- Smoking and other tobacco use
- Diabetes
- High cholesterol
- Heavy alcohol use
- Cocaine abuse
- Increasing age
- Fibromuscular dysplasia (~20%) involving the distal renal artery in children. Fibromuscular dysplasia as an idiopathic (unknown), nonatherosclerotic and noninflammatory disease that can affect all layers of small and medium caliber arteries 8. Experts don’t know what causes fibromuscular dysplasia, but the condition is more common in women and may be something that’s present at birth (congenital). In fibromuscular dysplasia, the muscle in the artery wall doesn’t grow as it should. This often begins in childhood. Fibromuscular dysplasia most frequently affects the renal (one or both kidneys), carotid, and vertebral arteries, but it can affect any arteries in your body and cause complications. The renal artery can have narrow sections alternating with wider sections, giving a bead-like appearance (“string of beads” sign) in images of the artery. Other less common imaging findings include vascular loops, ectasia, arterial dissection, and aneurysm. The renal artery can narrow so much that the kidney doesn’t get enough blood. This can lead to high blood pressure at a young age (Figure 5). Fibromuscular dysplasia in the renal arteries is found in about 1% of hypertensive patients, with strong female prevalence (90%), and occurs in premenopausal Caucasian women from 15 to 50 years of age 9, 10. Fibromuscular dysplasia is more common on the right 2.
Rarely, renal artery stenosis results from other conditions such as inflammation of the blood vessels or a growth that develops in your abdomen and presses on your kidneys’ arteries 5, 6:
- Vasculitis: especially polyarteritis nodosa (PAN) (causes multiple microaneurysms), Takayasu arteritis, radiation
- Neurofibromatosis type 1: most commonly involves the ostium
- Abdominal aortic coarctation
- Aortic dissection
- Segmental arterial mediolysis
- Compression by diaphragmatic crura 11, 12
- Williams syndrome
Renal artery stenosis is also common following a renal transplant.
Risk factors for developing renal artery stenosis
Most cases of renal artery stenosis result from narrowed kidney arteries. Risk factors that make narrowed arteries more likely in your kidneys and other parts of your body include:
- Aging
- High blood pressure
- High cholesterol
- Diabetes
- Obesity
- Smoking and other tobacco use
- A family history of early heart disease
- Lack of exercise.
Renal artery stenosis pathophysiology
Pathogenesis of high blood pressure
In atherosclerosis, the initiator of endothelial injury although not well understood can be, high cholesterol, cigarette smoking, viral infection, immune injury, or increased homocysteine levels 13. At the lesion site, permeability to low-density lipoprotein (LDL) and macrophage migration increases with subsequent proliferation of endothelial and smooth muscle cells and ultimate formation of atherosclerotic plaque. Renal blood flow, which is significantly greater than the perfusion to other organs, along with glomerular capillary hydrostatic pressure is an important determinant of the glomerular filtration rate (GFR). In patients with renal artery stenosis, the chronic ischemia produced by the obstruction of renal blood flow leads to adaptive changes in the kidney which include the formation of collateral blood vessels and secretion of renin by juxtaglomerular apparatus. The renin enzyme has an important role in maintaining homeostasis in that it converts angiotensinogen to angiotensin 1. Angiotensin 1 has to be converted to angiotensin 2 with the help of an angiotensin-converting enzyme (ACE) in the lungs. Angiotensin 2 is responsible for vasoconstriction and release of aldosterone which causes sodium and water retention, thus resulting in secondary hypertension or renovascular hypertension 14, 15.
Pathogenesis of chronic kidney disease
Glomerular filtration rate (GFR) is autoregulated by angiotensin 2 and other modulators between the afferent and efferent arteries. The maintenance of GFR fails when renal perfusion pressure falls below 70 mmHg to -85 mmHg. Therefore significant functional impairment of autoregulation, leading to a decrease in the GFR, is only likely to be observed until arterial luminal narrowing exceeds 50%. Studies demonstrate that a moderate reduction in renal perfusion pressure (up to 40%) and renal blood flow (mean 30%) cause reduction in glomerular filtration, however, tissue oxygenation within the kidney cortex and medulla can adapt without the development of severe hypoxia. As an inference patients at an early stage can be treated with medical therapy without progressive loss of function or irreversible fibrosis in many cases, sometimes for many years.
It is reported that more advanced stenosis corresponding to a 70% to 80% of vascular occlusion leads to demonstrable cortical hypoxia, and it is proposed that this hypoxia produce rarefaction of microvessels, as well as activation of inflammatory and oxidative pathways that cause interstitial fibrosis 16. Therefore loss of renal function in renovascular disease in addition to being a usually reversible consequence of antihypertensive therapy can reflect a progressive narrowing of the renal arteries and/or progressive intrinsic renal disease. Eventually, long-standing parenchymal injury becomes an irreversible process. At this point, restoring renal blood flow provides no recovery of renal function or clinical benefit 1.
Renal artery stenosis prevention
Preventing atherosclerosis may prevent renal artery stenosis. Taking the following steps can help:
- Lose weight if you are overweight.
- Ask your doctor about your smoking and alcohol use.
- Control your blood sugar if you have diabetes.
- Make sure your doctor is monitoring your blood cholesterol levels.
- Eat a heart-healthy diet.
- Get regular exercise.
Renal artery stenosis symptoms
In many cases, renal artery stenosis doesn’t cause any signs or symptoms until it’s advanced. Renal artery stenosis may be discovered incidentally during testing for something else. In general, people with renal artery stenosis may have a history of very high blood pressure that is hard to bring down with medicines.
Signs and symptoms of renal artery stenosis include:
- High blood pressure at a young age before age 30 or after age 50
- High blood pressure that begins suddenly or worsens without explanation
- High blood pressure that suddenly gets worse or is hard to control with at least three or more different types of blood pressure medications
- Kidneys that are not working well, this can start suddenly (decreased kidney function)
- Elevated protein levels in your urine or other signs of a problem with kidney function
- Worsening kidney function during treatment for high blood pressure
- A whooshing sound as blood flows through a narrowed vessel (bruit), which your doctor hears through a stethoscope placed over your kidneys
- Narrowing of other arteries in the body, such as to the legs, the brain, the eyes and elsewhere
- Fluid overload and swelling in your body’s tissues
- Sudden buildup of fluid in the air sacs of your lungs (pulmonary edema)
- Treatment-resistant heart failure
Symptoms of a significant decrease in kidney function include:
- increase or decrease in urination
- edema—swelling, usually in the legs, feet, or ankles and less often in the hands or face
- drowsiness or tiredness
- generalized itching or numbness
- dry skin
- headaches
- weight loss
- appetite loss
- nausea
- vomiting
- sleep problems
- trouble concentrating
- darkened skin
- muscle cramps
If you have a dangerous form of high blood pressure called malignant hypertension, symptoms can include:
- Bad headache
- Nausea or vomiting
- Confusion
- Changes in vision
- Nosebleeds
Renal artery stenosis complications
People with renal artery stenosis are at increased risk for complications resulting from loss of kidney function or atherosclerosis occurring in other blood vessels, such as:
- High blood pressure
- Chronic kidney disease (CKD) — reduced kidney function over a period of time
- Kidney failure, requiring treatment with dialysis or a kidney transplant
- Aortic aneurysm
- Coronary artery disease, narrowing and hardening of coronary arteries that supply blood to your heart
- Heart attack
- Heart failure
- Peripheral vascular disease — blockage of blood vessels that restricts flow of blood from the heart to other parts of the body, particularly the legs
- Fluid retention in your legs, causing swollen ankles or feet
- Shortness of breath due to a sudden buildup of fluid in the lungs (pulmonary edema)
- Stroke —brain damage caused by lack of blood flow to the brain
- Vision problems
Renal artery stenosis can lead to kidney failure, described as end-stage renal disease when treated with blood-filtering treatments called dialysis or a kidney transplant, though this is uncommon in people who receive ongoing treatment for renal artery stenosis 17.
Renal artery stenosis diagnosis
For diagnosis of renal artery stenosis, your doctor may start with:
- A review of your medical history
- A physical exam that includes your doctor listening through a stethoscope over your kidney areas for sounds that may mean the renal artery to your kidney is narrowed
- Blood and urine tests to check your kidney function i.e., blood urea nitrogen (BUN), creatinine, creatinine clearance, potassium, sodium, cholesterol levels
- Blood and urine tests to measure the levels of hormones, renin and aldosterone, that regulate blood pressure.
The following imaging tests are used to diagnose renal artery stenosis:
- Duplex ultrasound. Duplex ultrasound combines traditional ultrasound with Doppler ultrasonography. Traditional ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. Doppler ultrasonography records sound waves reflected off of moving objects, such as blood, to measure their speed and other aspects of how they flow. Duplex ultrasound is performed in a doctor’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging. Anesthesia is not needed. Duplex ultrasound help your doctor see the arteries and kidneys and check their function. This procedure also helps your doctor find blockages in the blood vessels and measure their severity.
- Computerized tomographic angiography (CTA) scan. CTA scans use a combination of x-rays and computer technology to create detailed images that show cross-sectional images of the renal arteries. The procedure is performed in an outpatient center or hospital by an x-ray technician, and the images are interpreted by a radiologist. Anesthesia is not needed. Contrast medium is injected into a vein in the person’s arm to better see the structure of the arteries. CTA scans require the person to lie on a table that slides into a tunnel-shaped device where the x-rays are taken. CTA scans are less invasive than catheter angiograms and take less time. However, the risks from the x-ray radiation still exist, and the test often requires more contrast medium than a catheter angiogram, so it may not be recommended for a person with poor kidney function.
- Magnetic resonance angiography (MRA). Magnetic resonance angiography (MRA) uses radio waves and strong magnetic fields to produce detailed 3D images of the renal arteries and kidneys. A dye injection into the arteries outlines blood vessels during imaging. The procedure is performed in an outpatient center or hospital by an x-ray technician, and the images are interpreted by a radiologist. Anesthesia is not needed though light sedation may be used for people with a fear of confined spaces. Contrast medium may be injected into a vein in the person’s arm to better see the structure of the arteries. With most MRA scans, the person lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines are designed to allow the person to lie in a more open space. In addition to providing high-quality images noninvasively, MRA can provide a functional assessment of blood flow and organ function. However, the use of contrast medium for an MRA is not advised for people with poor kidney function because of the risk of complications to the skin and other organs if the kidneys do not remove the contrast medium well enough.
- Renal artery angiography. A catheter angiogram also called a traditional angiogram, is a special kind of X-ray in which a thin, flexible tube called a catheter is threaded through the large arteries, often from the groin, to the artery of interest—in this case, the renal artery. The procedure is performed in a hospital or outpatient center by a radiologist. Anesthesia is not needed though a sedative may be given to lessen anxiety during the procedure. Contrast medium is injected through the catheter so the renal artery shows up more clearly on the x-ray. Catheter angiogram is the “gold standard” for diagnosing renal artery stenosis due to the high quality of the image produced. In addition, severe renal artery stenosis can be treated with a balloon or a small tube (stent) placed in your blood vessel to widen it during the same visit. However, a catheter angiogram is an invasive procedure, and a person may have side effects from the sedative or contrast medium or may have bleeding or injury to the artery from the catheter. The procedure is also more expensive than other imaging tests.
- Angiotensin Converting Enzyme (ACE) inhibitor scintigraphy. A kidney with renovascular hypertension particularly renal artery stenosis exhibits impaired function during Angiotensin Converting Enzyme (ACE) inhibition. This phenomenon is believed to be a manifestation of disruption of the autoregulation system of the glomerular filtration rate (GFR), which becomes dependent on angiotensin 2 under circumstances of low perfusion. Although a decline in the GFR can be induced by ACE inhibition in the affected kidney of patients with unilateral renal artery stenosis, the contralateral kidney preserves the overall renal function. This change in renal function in unilateral renal artery stenosis-induced by ACE inhibition can be revealed with scintigraphy. In these patients, ACE inhibitor scintigraphy induces significant changes in the time-activity curves of the affected kidney in contrast to the baseline curves. ACE inhibitor scintigraphy is performed 1 hour after an oral dose of 25 mg of captopril or 15 minutes after an intravenous dose of 0.04 mg/kg of enalapril maleate. Any pre-existing ACE inhibitor therapy should be ceased 2 to 5 days before the study according to the half-life of the drug, and adequate hydration must be ensured. Blood pressure should be monitored during the procedure. Baseline and ACE inhibitor scintigraphy is performed after intravenous injection of technetium-99m mercaptoacetyltriglycine (MAG), iodine-131 ortho iodohippurate (OIH), or Tc-99m diethylenetriaminepentaacetic acid (DTPA). Sequential images and scintigraphic curves are acquired for 30 minutes after injection of the radiotracer. Time-activity curves are generated from the renal cortex and pelvis. Renal uptake is measured every 1-min to 2-min intervals after injection. Tc-99m MAG and I-131 OIH are excreted through tubular secretion while Tc-99m DTPA is excreted through glomerular filtration. In patients with renal artery stenosis, ACE inhibitors prompt renal retention of the radiotracer due to decreased urinary output secondary to reduced GFR.
- ACE Inhibitor Scintigraphy general interpretive criteria are 1:
- A normal ACE inhibitor scintigram is indicative of low probability (less than 10%) of renovascular hypertension
- A small, poorly functioning kidney (less than 30% uptake with a time of maximum activity [T] 2 minutes or less) that shows no change on the ACE inhibitor scintigram and bilateral symmetric abnormalities such as cortical retention of tubular agents signal an intermediate probability of RVH
- Criteria associated with a high probability of renal artery stenosis include worsening of the scintigraphic curve, decrease in the relative uptake, prolongation of the renal and parenchymal transit time, increase in the 20-minute/peak uptake ratio of 0.15 or greater, and prolongation of time of maximum activity [T] .
- Specific interpretive criteria for Tc-99m MAG and I-131 OIH scintigrams are following:
- Unilateral parenchymal retention after ACE inhibition (demonstrated as a change in the 20-minute/peak uptake ratio of 0.15 or greater, a significantly prolonged transit time, delay in excretion of the tracer into the renal pelvis) is the most important criterion for Tc-99m MAG and I-131 OIH scintigraphy and represents a high probability (greater than 90%) of renovascular hypertension.
- ACE Inhibitor Scintigraphy general interpretive criteria are 1:
Renal artery stenosis treatment
Treatment for renal artery stenosis may involve lifestyle changes, medication and a procedure to restore blood flow to the kidneys. Sometimes a combination of treatments is the best approach. Depending on your overall health and symptoms, you may not need any specific treatment.
Renal artery stenosis that has not led to renovascular hypertension (high blood pressure caused by renal artery stenosis) or caused a significant blockage of the renal artery may not need treatment. Renal artery stenosis that needs to be treated, also called critical renal artery stenosis, is defined by the American Heart Association as a reduction by more than 60 percent in the diameter of the renal artery 18. However, health care providers are not exactly sure what degree of blockage will cause significant problems.
Lifestyle changes
The first step in treating renal artery stenosis is making lifestyle changes that promote healthy blood vessels throughout the body, including the renal arteries. If your blood pressure is moderately or severely elevated, a healthy lifestyle such as limiting salt in your diet, eating healthy foods and getting regular physical activity — can help control your blood pressure.
Your doctor may also recommend that you:
- Maintain a healthy weight. When your weight increases, so does your blood pressure. If you’re overweight, losing weight may help to lower your blood pressure.
- Restrict salt in your diet. Salt and salty foods cause your body to retain fluid. This may increase the volume of your blood and, in turn, increase your blood pressure.
- Be physically active. Being physically active on a regular basis may help you lose weight, lower your risk of heart disease, lower your cholesterol and lower your blood pressure. Check with your doctor before beginning an exercise program, especially if you have high blood pressure and haven’t been active in the past.
- Reduce stress. Lowering stress levels may decrease your blood pressure.
- Drink alcohol in moderation, if at all. Too much alcohol may increase your blood pressure.
- Don’t smoke. Tobacco injures blood vessel walls and speeds up the process of hardening of the arteries. If you smoke, ask your doctor to help you quit.
Medication
High blood pressure even when mainly related to renal artery stenosis can often be successfully treated with medications. One or more medicines are needed to help control blood pressure. There are many types available. Finding the right medication or combination of medications may require time and patience.
Some medications commonly used to treat high blood pressure associated with renal artery stenosis include 19, 20:
- Angiotensin-converting enzyme (ACE) inhibitors and angiotensin 2 receptor blockers (ARBs), which help relax your blood vessels and block the formation or effects of a natural body chemical called angiotensin 2, which narrows blood vessels
- Diuretics also known as water pills, which help your body eliminate excess sodium and water
Beta blockers and alpha-beta blockers, which may have the effect of making your heart beat slowly and less forcefully or widening (dilating) your blood vessels, depending on which medication you use - Calcium channel blockers, which help relax blood vessels
If atherosclerosis is the underlying cause of renal artery stenosis, your doctor may also recommend aspirin and a cholesterol-lowering medication. Which medications are best for you depends on your individual situation.
Surgical procedures
For some people a surgical procedure may be recommended to restore blood flow through the renal artery to improve blood flow to the kidney. Results from recent studies comparing medication with renal angioplasty and stenting didn’t show a difference between the two treatment approaches on reducing high blood pressure and improving kidney function for people with moderate renal artery stenosis. Procedures to open the vessel should be considered for people who don’t do well on medicine alone, who can’t tolerate medications, who often retain fluids and who have treatment-resistant heart failure. Furthermore, surgery may be recommended for people with renal artery stenosis caused by fibromuscular dysplasia or renal artery stenosis that does not improve with medication. Different types of surgery for renal artery stenosis include the following. The procedures are performed in a hospital by a vascular surgeon—a doctor who specializes in repairing blood vessels. Anesthesia is needed.
Procedures to treat renal artery stenosis may include:
- Renal angioplasty and stenting. Angioplasty is a procedure in which a catheter is put into your renal artery, usually through your groin, just as in a catheter angiogram. In addition, for angioplasty, a tiny balloon at the end of the catheter can be inflated to flatten the plaque against the artery wall. A small mesh tube, called a stent, may then be positioned inside the artery to keep plaque flattened and the artery open. People with renal artery stenosis caused by fibromuscular dysplasia may be successfully treated with angioplasty alone, while angioplasty with stenting has a better outcome for people with renal artery stenosis caused by atherosclerosis.
- Renal artery bypass surgery or endarterectomy. In an endarterectomy, the plaque is cleaned out of the renal artery, leaving the inside lining smooth and clear. To create a bypass, a vein or synthetic tube is used to connect (graft) the kidney to the aorta. This new path serves as an alternate route for blood to flow around the blocked artery into the kidney. Sometimes this means connecting the renal artery to a vessel from somewhere else, such as the liver or spleen. These operations are most often done if angioplasty isn’t successful, or when there’s a need for additional surgical procedures. However, these procedures are not performed as often as in the past due to a high risk of complications during and after the procedure.
- Bokhari MR, Bokhari SRA. Renal Artery Stenosis. [Updated 2022 Sep 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430718[↩][↩][↩]
- Hartung M, Fibromuscular dysplasia – renal arteries. Case study, Radiopaedia.org https://doi.org/10.53347/rID-59558[↩][↩]
- Chen Y, Dong H, Jiang X, Zou YB. Unifocal progressed to multifocal renal artery fibromuscular dysplasia. Eur Heart J Case Rep. 2021 Dec 24;6(1):ytab522. doi: 10.1093/ehjcr/ytab522[↩]
- Fibromuscular Dysplasia. https://www.ninds.nih.gov/health-information/disorders/fibromuscular-dysplasia[↩]
- D’Souza D, Knipe H, Yap J, et al. Renal artery stenosis. Reference article, Radiopaedia.org https://doi.org/10.53347/rID-3871[↩][↩]
- Renal artery stenosis. https://www.mayoclinic.org/diseases-conditions/renal-artery-stenosis/symptoms-causes/syc-20352777[↩][↩]
- Plouin PF, Bax L. Diagnosis and treatment of renal artery stenosis. Nat Rev Nephrol. 2010 Mar;6(3):151-9. doi: 10.1038/nrneph.2009.230[↩]
- Olin JW, Sealove BA. Diagnosis, management, and future developments of fibromuscular dysplasia. J Vasc Surg. 2011 Mar;53(3):826-36.e1. doi: 10.1016/j.jvs.2010.10.066[↩]
- Olin JW, Froehlich J, Gu X, Bacharach JM, Eagle K, Gray BH, Jaff MR, Kim ES, Mace P, Matsumoto AH, McBane RD, Kline-Rogers E, White CJ, Gornik HL. The United States Registry for Fibromuscular Dysplasia: results in the first 447 patients. Circulation. 2012 Jun 26;125(25):3182-90. doi: 10.1161/CIRCULATIONAHA.112.091223[↩]
- Chrysant SG, Chrysant GS. Treatment of hypertension in patients with renal artery stenosis due to fibromuscular dysplasia of the renal arteries. Cardiovasc Diagn Ther. 2014 Feb;4(1):36-43. doi: 10.3978/j.issn.2223-3652.2014.02.01[↩]
- Gaebel G, Hinterseher I, Saeger HD, Bergert H. Compression of the left renal artery and celiac trunk by diaphragmatic crura. J Vasc Surg. 2009 Oct;50(4):910-4. doi: 10.1016/j.jvs.2009.05.004[↩]
- Mirza AK, Kendrick ML, Bower TC, DeMartino RR. Renovascular hypertension secondary to renal artery compression by diaphragmatic crura. J Vasc Surg Cases Innov Tech. 2020 May 28;6(2):239-242. doi: 10.1016/j.jvscit.2020.03.002[↩]
- Park KH, Park WJ. Endothelial Dysfunction: Clinical Implications in Cardiovascular Disease and Therapeutic Approaches. J Korean Med Sci. 2015 Sep;30(9):1213-25. doi: 10.3346/jkms.2015.30.9.1213[↩]
- Ma N, Wang SY, Sun YJ, Ren JH, Guo FJ. [Diagnostic value of contrast-enhanced ultrasound for accessory renal artery among patients suspected of renal artery stenosis]. Zhonghua Yi Xue Za Zhi. 2019 Mar 19;99(11):838-840. Chinese. doi: 10.3760/cma.j.issn.0376-2491.2019.11.008[↩]
- Tetteh PW, Antwi-Boasiako C, Gyan B, Antwi D, Adzaku F, Adu-Bonsaffoh K, Obed S. Impaired renal function and increased urinary isoprostane excretion in Ghanaian women with pre-eclampsia. Res Rep Trop Med. 2013 Jun 18;4:7-13. doi: 10.2147/RRTM.S40450[↩]
- Gloviczki ML, Glockner JF, Crane JA, McKusick MA, Misra S, Grande JP, Lerman LO, Textor SC. Blood oxygen level-dependent magnetic resonance imaging identifies cortical hypoxia in severe renovascular disease. Hypertension. 2011 Dec;58(6):1066-72. doi: 10.1161/HYPERTENSIONAHA.111.171405[↩]
- Renal Artery Stenosis. https://www.niddk.nih.gov/health-information/kidney-disease/renal-artery-stenosis[↩]
- James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 5;311(5):507-20. doi: 10.1001/jama.2013.284427. Erratum in: JAMA. 2014 May 7;311(17):1809.[↩]
- Fournier T, Sens F, Rouvière O, Millon A, Juillard L. Prise en charge de la sténose athéromateuse d’artère rénale en 2016 [Management of atherosclerotic renal-artery stenosis in 2016]. Nephrol Ther. 2017 Feb;13(1):1-8. French. doi: 10.1016/j.nephro.2016.07.450[↩]
- Ricco JB, Belmonte R, Illuminati G, Barral X, Schneider F, Chavent B. How to manage hypertension with atherosclerotic renal artery stenosis? J Cardiovasc Surg (Torino). 2017 Apr;58(2):329-338. doi: 10.23736/S0021-9509.16.09827-X[↩]





{kind=link}