
Contents
- What is restrictive lung disease
What is restrictive lung disease
Restrictive lung disease is a group of conditions characterized by reduced lung volume, either because of an intrinsic cause, such as an alteration in lung parenchyma, or because of an extrinsic cause, such as a disease of the pleura, chest wall, or neuromuscular apparatus 1. Unlike obstructive lung diseases, such as asthma and chronic obstructive pulmonary disease (COPD), which show a normal or increased total lung capacity (TLC), restrictive lung disease are associated with a decreased total lung capacity (TLC). Measures of expiratory airflow are preserved and airway resistance is normal and the forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio is increased. If both the FEV1/FVC ratio and the FVC are low, the patient has a mixed defect 2. If caused by parenchymal lung disease, restrictive lung disorders are accompanied by reduced gas transfer (DLCO test), which may be marked clinically by desaturation after exercise 3. DLCO (diffusing capacity of lung for carbon monoxide) test is a quantitative measurement of gas transfer in your lungs. Diseases that decrease blood flow to the lungs or damage alveoli will cause less efficient gas exchange, resulting in a lower DLCO measurement. During the DLCO test, patients inhale a mixture of helium (10%), carbon monoxide (0.3%), oxygen (21%), and nitrogen (68.7%) then hold their breath for 10 seconds before exhaling 4. The amounts of exhaled helium and carbon monoxide are used to calculate the DLCO. Carbon monoxide is used to estimate gas transfer instead of oxygen due to its much higher affinity for hemoglobin. A baseline hemoglobin level should be obtained before DLCO testing because results are adjusted for the hemoglobin level.
Obstructive vs Restrictive lung disease
Obstructive lung disease is a category of respiratory disease characterized by airway obstruction. Many obstructive diseases of the lung result from narrowing (obstruction) of the smaller bronchi and larger bronchioles, often because of excessive contraction of the smooth muscle itself. It is generally characterized by inflamed and easily collapsible airways, obstruction to airflow, problems exhaling and frequent medical clinic visits and hospitalizations. Types of obstructive lung disease include; asthma, bronchiectasis, bronchitis and chronic obstructive pulmonary disease (COPD). Although COPD shares similar characteristics with all other obstructive lung diseases, such as the signs of coughing and wheezing, they are distinct conditions in terms of disease onset, frequency of symptoms and reversibility of airway obstruction. Cystic fibrosis is also sometimes included in obstructive pulmonary disease.
Common causes of obstructive lung disease:
- Alpha-1 antitrypsin deficiency (α1-antitrypsin deficiency)
- Asthma
- Bronchiectasis
- Bronchiolitis obliterans
- Chronic obstructive pulmonary disease
- Cystic fibrosis
- Silicosis (early)
Types of restrictive lung disease
The many disorders that cause reduction or restriction of lung volumes may be divided into two groups based on anatomical structures 5.
- Intrinsic lung diseases or diseases of the lung parenchyma. The diseases cause inflammation or scarring of the lung tissue (interstitial lung disease) or result in filling of the air spaces with exudate and debris (pneumonitis). These diseases can be characterized according to etiological factors. They include idiopathic fibrotic diseases, connective-tissue diseases, drug-induced lung disease, environmental exposures (inorganic and organic dusts), and primary diseases of the lungs (including sarcoidosis).
- Extrinsic disorders or extrapulmonary diseases. The chest wall, pleura, and respiratory muscles are the components of the respiratory pump, and they need to function normally for effective ventilation. Diseases of these structures result in lung restriction, impaired ventilatory function, and respiratory failure (eg, nonmuscular diseases of the chest wall, neuromuscular disorders).
Intrinsic lung diseases
Collagen-vascular diseases, including scleroderma, polymyositis, dermatomyositis, systemic lupus erythematosus, rheumatoid arthritis, and ankylosing spondylitis, are potential causes of restrictive lung disease.
Other causes may include drugs and other treatments (eg, nitrofurantoin, amiodarone, gold, phenytoin, thiazides, hydralazine, bleomycin, bischloroethylnitrosourea [BCNU or carmustine], cyclophosphamide, methotrexate, radiation). More than 600 drugs are known to cause pulmonary toxicity, and illicit drugs are well-known to result in pulmonary toxicities.
Causes related to primary or unclassified diseases may include sarcoidosis, pulmonary Langerhans cell histiocytosis, lymphangioleiomyomatosis (LAM), pulmonary vasculitis, alveolar proteinosis, eosinophilic pneumonia, and cryptogenic organizing pneumonia (COP).
Inorganic dust exposure (eg, silicosis, asbestosis, talc, pneumoconiosis, berylliosis, hard metal fibrosis, coal worker’s pneumoconiosis, chemical worker’s lung) may cause restrictive lung disease.
Organic dust exposure can lead to hypersensitivity pneumonitis (eg, farmer’s lung, bird fancier’s lung, bagassosis, and mushroom worker’s lung, humidifier lung, hot tub pneumonitis).
Extrinsic disorders
Nonmuscular diseases of the chest wall, in which kyphosis can be idiopathic or secondary, may cause restrictive lung disease. The most common cause of secondary kyphoscoliosis is neuromuscular disease (eg, polio, muscular dystrophy). Fibrothorax, massive pleural effusion, morbid obesity, ankylosing spondylitis, and thoracoplasty are other causes.
Neuromuscular diseases manifest as respiratory muscle weakness and are due to myopathy or myositis, quadriplegia, or phrenic neuropathy from infectious or metabolic causes.
Pleural diseases, including trapped lung or asbestos-related pleural plaques, are an underrecognized, and potentially treatable, cause of restrictive lung disease.
Idiopathic fibrotic disorders
These may include acute interstitial pneumonia, idiopathic pulmonary fibrosis (usually interstitial pneumonitis), lymphocytic interstitial pneumonitis, desquamative interstitial pneumonitis, and nonspecific interstitial pneumonitis.
Causes of restrictive lung disease
The mnemonic “PAINT” has been used to divide the causes of restrictive lung disease into pleural, alveolar, interstitial, neuromuscular, and thoracic cage abnormalities.
Common causes of restrictive lung disease:
Chest wall
- Ankylosing spondylitis
- Kyphosis
- Morbid obesity
- Scoliosis
Drugs (adverse reaction)
- Amiodarone
- Methotrexate
- Nitrofurantoin (Furadantin)
Interstitial lung disease
- Asbestosis
- Berylliosis
- Eosinophilic pneumonia
- Hypersensitivity pneumonitis
- Idiopathic pulmonary fibrosis
- Sarcoidosis
- Silicosis (late)
Neuromuscular disorders
- Amyotrophic lateral sclerosis
- Guillain-Barré syndrome
- Muscular dystrophy
- Myasthenia gravis
Table 1. Causes of Restrictive Lung Disease
| Causes | Examples | Diagnosis | PFT Findings |
|---|---|---|---|
| Pleural | Trapped lung, pleural scarring, large pleural effusions, chronic empyema, asbestosis | Radiography, CT scanning, pleural manometry, pleural biopsy | Low RVa, low TLC, low FVC |
| Alveolar | Edema, hemorrhage | Radiography, CT scanning, physical examination | Increased DLCOb in hemorrhage (Intrapulmonary hemoglobin absorbs the carbon monoxide, thus increasing the DLCO reading.) |
| Interstitial | Interstitial lung disease including IPFc, NSIPd, COPe | Radiography, CT scanning, physical examination, echo often shows pulmonary hypertension | Low RV, low FVC, low TLC, decreased DLCO, poor lung compliance |
| Neuromuscular | Myasthenia gravis, ALSf, myopathy | Physical examination, EMGsg, serology | Low RV, low TLC, low NIFh, low MMVi |
| Thoracic/extrathoracic | Obesity, kyphoscoliosis, ascites | Physical examination | Low ERVj and FRC in obesity, low VCk, TLC, FRCl in kyphoscoliosis |
Footnotes:
- a) Residual volume.
- b) Diffusion capacity of the lungs for carbon monoxide.
- c) Idiopathic pulmonary fibrosis.
- d) Nonspecific interstitial pneumonitis.
- e) Cryptogenic organizing pneumonia.
- f) Amyotrophic lateral sclerosis.
- g) Electromyography.
- h) Negative inspiratory force.
- i) Maximal voluntary ventilation.
- j) Expiratory reserve volume.
- k) Vital capacity.
- l) Functional residual capacity.
Restrictive lung disease symptoms
Symptoms of intrinsic diseases
Progressive exertional dyspnea is the predominant symptom. Grading the level of dyspnea is useful as a method to gauge the severity of the disease and to follow its course. It is helpful to use an objective quantification of the degree of dyspnea, such as the number of steps walked before becoming dyspneic.
A dry cough is common and may be a disturbing sign. A productive cough is an unusual sign in most patients with diffuse parenchymal lung disorders.
Hemoptysis or grossly bloody sputum occurs in patients with diffuse alveolar hemorrhage syndromes and vasculitis 6.
Wheezing is an uncommon manifestation but can occur in patients with an airway-centered process, such as lymphangitic carcinomatosis, chronic eosinophilic pneumonia, and respiratory bronchiolitis or sarcoidosis 7.
Chest pain is uncommon in most instances of the disease, but pleuritic chest pain can occur in patients and presents as serositis. This can occur with rheumatoid arthritis, systemic lupus erythematosus, and some drug-induced disorders 8. Substernal chest pain is also commonly described in sarcoidosis 9.
Symptoms of extrinsic disorders
Nonmuscular diseases of the chest wall affect patients with kyphoscoliosis. Patients younger than 35 years tend to be asymptomatic, whereas middle-aged patients develop dyspnea, decreased exercise tolerance, and respiratory infections 10.
The cause of respiratory failure is often multifactorial and is secondary to spinal deformity, muscle weakness, disordered ventilatory control, sleep-disordered breathing, and airway disease 11.
Neuromuscular disorders occur as the respiratory muscle weakness progresses. Patients develop dyspnea upon exertion, followed by dyspnea at rest, and their condition ultimately advances to respiratory failure.
Patients with neuromuscular diseases develop significant respiratory muscle weakness and may demonstrate fatigue, dyspnea, impaired control of secretions, and recurrent lower respiratory tract infections. In these patients, the central drive is not decreased 12. Acute and chronic respiratory failure, pulmonary hypertension, and cor pulmonale eventually ensue.
Restrictive lung disease complications
Acute exacerbation in patients with idiopathic pulmonary fibrosis is a recognized complication that occurs unpredictably and presents as worsening dyspnea 13. Chest radiography demonstrates bilateral mixed alveolar-interstitial infiltrates, and CT scanning reveals ground-glass opacities and consolidation. Treatment includes high-dose systemic corticosteroids, although these are likely not effective, and the worsening disease portends an extremely poor prognosis. Series of patients with acute exacerbation of idiopathic pulmonary fibrosis reported in-hospital mortality rates between 78% and 96% 14.
Restrictive lung disease diagnosis
Restrictive lung disease can be difficult to diagnose since many lung diseases can cause breathlessness and cough, and some of these other diseases can have similar symptoms and X-ray results. You may have to see more than one specialist, including a respirologist, to help with the diagnosis.
- Your doctor will ask you questions about your home and work environments, your smoking history and your medical history. This will help them determine whether there were any environmental, occupational, genetic, or other factors that could be linked to the development of pulmonary fibrosis.
- Your doctor will do a physical examination of your lungs and will also examine other parts of your body including your heart, joints, fingernails, skin and muscles.
Although no single test can diagnose restrictive lung disease, your doctor may recommend a number of different tests including:
- Pulmonary function test: A pulmonary function test, or breathing test, is a simple test to measure how much air you can blow in and out of your lungs and how well your lungs can absorb oxygen.
- Six-minute walk test: This test helps determine your physical fitness, as well as the amount of oxygen in your blood at rest and with physical activity.
- Chest x-ray: Chest X-rays are simple images that can screen for interstitial lung disease and can sometimes be useful to help monitor progression.
- Blood tests: A number of blood tests can be requested to help identify other causes of interstitial lung disease.
- Computed tomography (CT scan): These radiology images will determine whether there is scarring in your lungs and will help identify the subtype of interstitial lung disease.
- Bronchoscopy: Bronchoscopy is a procedure that involves inserting a small flexible tube, called bronchoscope, through your mouth or nose and into your lungs. This is not necessary for diagnosis but some patients with possible restrictive lung disease undergo this procedure to help identify the presence of infection or to suggest other subtypes of interstitial lung disease.
- Surgical lung biopsy: Patients with an unclear diagnosis will sometimes undergo a surgical lung biopsy performed by a surgeon under general anesthetic. This test involves small incisions in the side of the chest, which allows removal of lung tissue and its examination under a microscope.
Medical history
The initial evaluation of patients should consist of a complete history, including a total review of past systemic conditions. A careful history of occupation, travel, habits, hobbies, exposures, and HIV risk factors is critical to help identify any etiologic agent or trigger.
Duration of illness
Acute disorders last days to weeks and include acute interstitial pneumonitis, eosinophilic pneumonia, and diffuse alveolar hemorrhage 15.
Subacute disorders lasting weeks to months include sarcoidosis, drug-induced interstitial lung disease, alveolar hemorrhage syndrome, cryptogenic organizing pneumonia and connective-tissue diseases 16.
Chronic cases lasting months to years include idiopathic pulmonary fibrosis (IPF), sarcoidosis, and pulmonary Langerhans cell histiocytosis 16.
Hypersensitivity pneumonitis and cryptogenic organizing pneumonia may manifest as acute, subacute, or chronic disease 15.
Smoking history
Pulmonary Langerhans cell histiocytosis, desquamative interstitial pneumonitis, idiopathic pulmonary fibrosis (IPF) and respiratory bronchiolitis occur with increased frequency among persons who smoke or those who previously smoked 17.
Prior medication use
A detailed history of previously used medications is needed to exclude the possibility of drug-induced lung disease. These commonly used drugs are nitrofurantoin, amiodarone, gold, sulfonamides, thiazides, isoniazid, chemotherapeutic agents (eg, bleomycin, busulfan, cyclophosphamide, methotrexate), procainamide, and hydralazine.
Radiation may also cause pneumonitis and fibrosis.
Family history
Familial associations include idiopathic pulmonary fibrosis (IPF), sarcoidosis, and lymphangioleiomyomatosis (LAM).
Occupational history
Seek a strict chronological listing of the patient’s lifelong employment, including specific duties and known exposures.
Inhaled inorganic dust from substances (eg, silica, asbestos, beryllium, hard metals, cobalt) can cause pneumoconiosis 18.
Inhaled organic dust may cause hypersensitivity pneumonitis 19.
Environmental exposure
A review of the domestic and work environment of the patient and spouse is invaluable.
Physical Examination
Intrinsic disorders
The physical examination in patients with intrinsic lung disorders may yield distinguishing physical findings.
Velcro crackles are common in most patients with interstitial lung disorders.
Inspiratory squeaks or scattered, late, inspiratory high-pitched rhonchi are frequently heard in patients with bronchiolitis.
Cyanosis at rest is uncommon in persons with interstitial lung diseases, and this is usually a late manifestation of advanced disease.
Digital clubbing is common in those with idiopathic pulmonary fibrosis and is rare in others (eg, those with sarcoidosis or hypersensitivity pneumonitis).
Extrapulmonary findings, including erythema nodosum, suggest sarcoidosis. A maculopapular rash can occur in those with connective-tissue diseases or drug-induced lung diseases. Raynaud phenomenon may be present in patients with connective-tissue diseases, and telangiectasia is present in those with scleroderma. Peripheral lymphadenopathy, salivary gland enlargement, and hepatosplenomegaly are signs of systemic sarcoidosis. Uveitis may be observed in those with sarcoidosis and ankylosing spondylitis. Other signs of systemic vasculitis may include palpable purpura, signifying a leukocytoclastic vasculitis. In addition, renal involvement may be heralded by hematuria and anasarca.
Cor pulmonale occurs in the late stages of pulmonary fibrosis or advanced kyphoscoliosis. Pulmonary hypertension and cor pulmonale become evident when signs include a loud P2, right-sided precordial lift, jugulovenous distension with a prominent A wave, and right-sided gallop.
Extrinsic disorders
By their very nature, severe kyphoscoliosis and massive obesity are easily recognizable. The pleural disorders are associated with decreased tactile fremitus, dullness upon percussion, and decreased intensity of breath sounds.
In cases of neuromuscular diseases, the physical examination findings may indicate accessory muscles usage, rapid shallow breathing, paradoxical breathing, and other features of systemic involvement.
Laboratory Studies
Intrinsic lung diseases
Routine laboratory evaluations often fail to reveal positive findings. However, anemia can indicate vasculitis, polycythemia can indicate hypoxemia in advanced disease, and leukocytosis can suggest acute hypersensitivity pneumonitis.
The decision to perform additional tests should be directed by the findings of the clinical assessment. Antinuclear antibodies and rheumatoid factor should be measured to screen for collagen-vascular disorders, creatine kinase for polymyositis, antineutrophilic cytoplasmic antibodies for vasculitis, and antiglomerular basement membrane antibody for Goodpasture syndrome.
The presence of precipitating antibodies to an antigen may help in diagnosing hypersensitivity pneumonitis. Serum angiotensin-converting enzyme levels are often elevated in patients with sarcoidosis, but this finding has poor specificity.
Extrinsic disorders
An elevated creatine kinase level may indicate myositis, which may cause muscle weakness with resultant restrictive lung disease.
Imaging Studies
Chest radiography for intrinsic lung disorders
The diagnosis of an interstitial lung disorder is often initially based on abnormal chest radiograph findings, although they can be normal in as many as 10% of patients. All previous chest films should be reviewed.
The most common radiographic abnormality is a reticular pattern. Nodular, reticulonodular, or mixed patterns, such as alveolar filling (ie, ground-glass appearance), and increased interstitial markings are not unusual; however, these are not predictive of a specific pathological picture. High-resolution CT scanning can be helpful in such cases by providing an accurate assessment and is recommended before lung biopsy 20.
Air-space opacities suggest pulmonary hemorrhage, eosinophilic pneumonia, and cryptogenic organizing pneumonia.
Upper-zone predominance on chest radiographs is observed in patients with sarcoidosis, pulmonary Langerhans cell histiocytosis, chronic hypersensitivity pneumonitis, pneumoconiosis, or ankylosing spondylitis. Lower-zone predominance is seen in patients with idiopathic pulmonary fibrosis (idiopathic pulmonary fibrosis), asbestosis, or collagen-vascular diseases.
The finding of honeycombing correlates with advanced fibrosis and indicates a poor prognosis. Bilateral hilar lymphadenopathy, with or without mediastinal adenopathy, suggests sarcoidosis.
CT scanning of the chest
High-resolution CT scanning of the chest can be helpful, but the expense and high dose of radiation makes it inappropriate for every patient 21. idiopathic pulmonary fibrosis can be diagnosed clinically based on the typical clinical features and CT scan findings without the need for lung biopsy 22. Bibasilar peripheral lung zone involvement is seen in patients with idiopathic pulmonary fibrosis, asbestosis, connective-tissue disease, or eosinophilic pneumonia.
Central disease along bronchovascular bundles is indicative of sarcoidosis or lymphangitic carcinoma.
Upper-zone predominance is observed in patients with sarcoidosis, eosinophilic granuloma, silicosis, or chronic hypersensitivity pneumonitis. Lower-zone predominance is seen in patients with idiopathic pulmonary fibrosis, asbestosis, or rheumatoid arthritis.
Lower-zone and peripheral infiltration is ordinarily seen in patients with idiopathic pulmonary fibrosis or asbestosis.
The presence of bilateral cysts and nodules, with preservation of lung volumes, may suggest a diagnosis of lymphangioleiomyomatosis (LAM) or pulmonary Langerhans cell histiocytosis.
Bibasilar reticular fibrosis with coexisting retraction bronchiectasis indicates end-stage irreversible disease, and ground-glass attenuation may result from changes in the interstitium, air spaces, or redistribution of capillary blood flow 23.
Lung Ultrasonography
Lung ultrasonography has a limited diagnostic role in the evaluation of pulmonary fibrosis. However, it may provide some information. A 3.5- to 7.5-MHz probe is placed on the chest wall, using the intercostal spaces as an acoustic window. A high-frequency (5-7.5MHz) “vascular” probe or a low-frequency (2.5-5Mhz) “cardiac” probe can be used. Use of a higher-frequency probe may yield more resolution at the pleural line.
Pulmonary fibrosis is associated with pleural thickening, especially in the lower posterior lobes. Notable lung sonographic findings include subpleural cysts and nodules, thickening of the pleural line, reductions in lung sliding, and the presence of sonographic B-lines. In a study of 52 patients with diffuse interstitial lung disease and 50 control patients, pleural-line abnormalities (irregularity, blurring, thickening, and fragmentation), B-lines, and subpleural consolidations (< 5 mm) are found to be characteristics of pulmonary fibrosis on lung sonography 24.
Tests for extrinsic disorders
Evidence of nonmuscular diseases of the chest wall and associated deformities of the spinal column and ribs are readily appreciated on chest radiographs. The severity of kyphoscoliosis is determined by the Cobb angle, which, when greater than 100°, indicates severe deformity. Neuromuscular diseases are also diagnosed based on chest radiograph findings showing low volumes and basal atelectasis.
Fluoroscopy is used to assess for diaphragm paralysis. A pleural sonogram of the diaphragm can also be use to assess for diaphragm paralysis.
A positive result from a sniff test may demonstrate paradoxical upward movement of the affected diaphragm.
Pulmonary function testing
Complete lung function testing includes spirometry, lung volume, diffusing capacity, and arterial blood gas measurements. Pulmonary function test findings do not indicate a specific diagnosis or help distinguish alveolitis from fibrosis. Findings from sequential tests are invaluable for monitoring the course of the disease and assessing the response to therapy.
All disorders are associated with a restrictive defect with a reduction in total lung capacity (TLC), functional reserve capacity (FRC), and residual volume (RV).
While a reduction in the forced expiratory volume in one second (FEV1) and the forced vital capacity (FVC) with a normal or increased FEV1 -to-FVC ratio suggests a restrictive pattern, the diagnosis of restriction is based on a decreased TLC. The assessment of the severity of restriction is also based on TLC.
A normal diffusion capacity of the lungs for carbon monoxide (DLCO) in the setting of restrictive lung parameters suggests a chest wall or neuromuscular disorder. Conversely, a low carbon monoxide (DLCO) in the setting of restrictive lung parameters would support interstitial lung disease or one of the pneumonitides.
An obstructive airflow limitation may be observed in patients with sarcoidosis, lymphangioleiomyomatosis (LAM), hypersensitivity pneumonitis, or pulmonary fibrosis with concomitant chronic obstructive pulmonary disease (COPD).
Tests for extrinsic lung disorders
In nonmuscular diseases of the chest wall, severe kyphoscoliosis produces a restrictive pattern. The total lung capacity (TLC) is markedly reduced, with relative preservation of the residual volume (RV). The vital capacity is reduced, and the RV-to-TLC ratio is elevated. Chest wall components are reduced, and inspiratory muscle weakness may also contribute to the restrictive process. Maximal inspiratory and expiratory pressures are modestly decreased in patients with mild disease but are severely reduced in patients with advanced disease.
Hypoxemia is due to a ventilation-perfusion mismatch caused by the underlying atelectasis and shunt.
In neuromuscular diseases, the maximal inspiratory and expiratory mouth pressures vary from normal to severely reduced. When maximal inspiratory pressure falls below 30 cm of water, ventilatory failure commonly ensues.
Patients with chronic muscular diseases have a decreased vital capacity and functional reserve capacity (FRC), but the RV is preserved. TLC is also moderately reduced. Breathing during sleep is often abnormal in these patients, resulting in nocturnal desaturation during rapid eye movement sleep, secondary to hypoventilation.
The diffusing capacity of lung for carbon monoxide (DLCO) is reduced in all patients with intrinsic lung disorders; however, the severity of this reduction does not correlate well with the stage of the disease. The DLCO is the most sensitive parameter, and findings may be abnormal even when the lung volumes are preserved. A normal DLCO value excludes intrinsic lung disease and indicates a chest wall, pleural, or neuromuscular cause of restrictive lung disease.
Arterial blood gas values at rest may reveal hypoxemia. Arterial oxygen desaturation occurs with exercise, along with an excessive increase in the respiratory rate and a high ratio of dead-space gas volume to tidal gas volume.
Cardiopulmonary exercise testing with measurements of gas exchange and oxygenation is more sensitive, and findings correlate better with lung biopsy but do not help predict the prognosis. A 6-minute walk test with oximetry provides a measure of oxygen requirement and a quantifiable measure of disease progression.
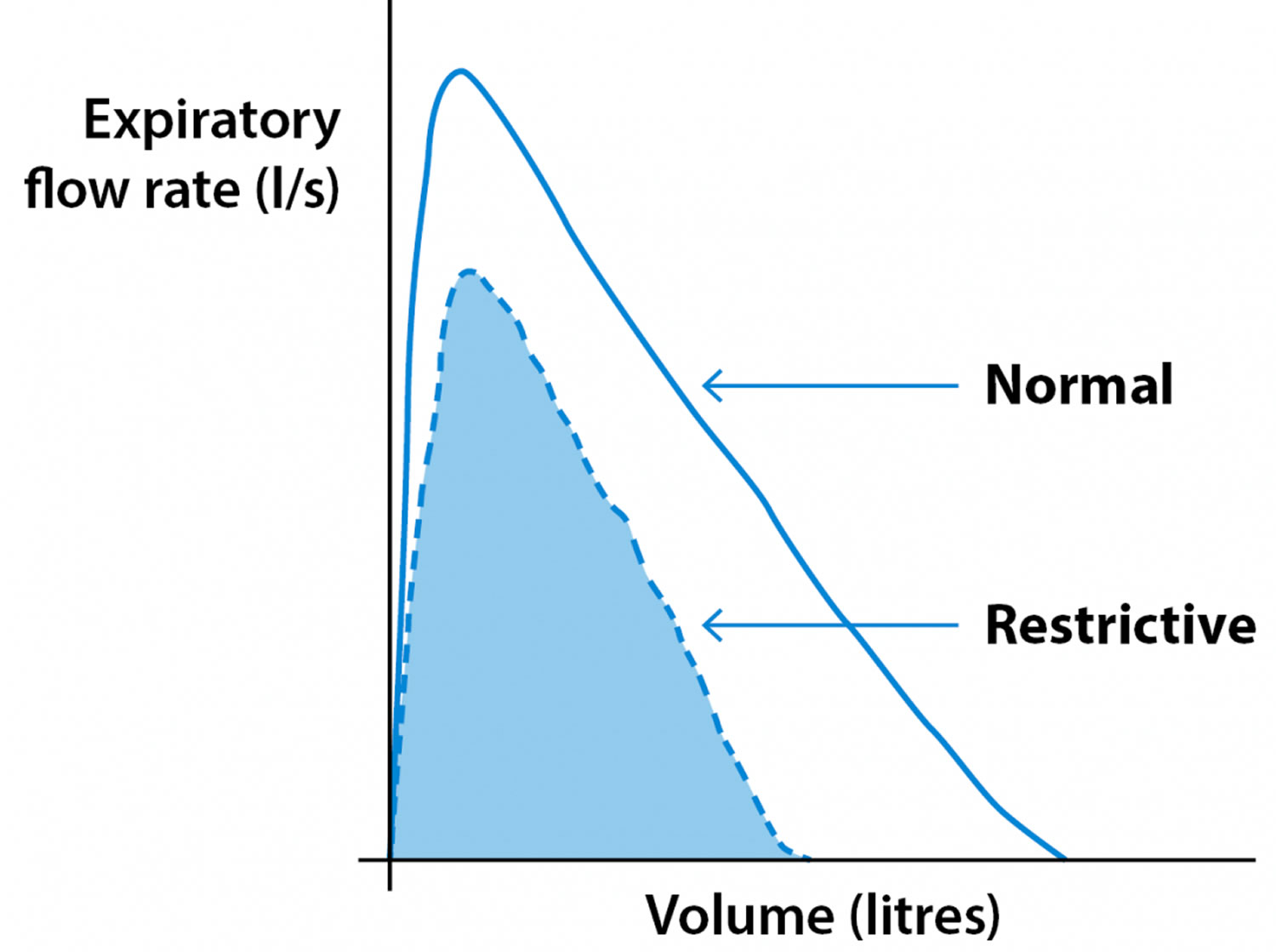
Restrictive lung disease spirometry
With a restrictive pattern, the total amount of air you can breathe in is reduced but the speed you can breathe out is preserved. In this situation, both the FEV1 and FVC will be lower than predicted, but the ratio between the two will not be reduced.
This is caused by various conditions that affect the tissue of your lungs or affect the capacity of your lungs to expand and hold a normal amount of air, such as pulmonary fibrosis. This pattern can also be seen in people who are significantly overweight, have an abnormal curvature of the spine or weak breathing muscles.
Figure 1. Spirometry Restrictive pattern – measuring FEV1 and FVC
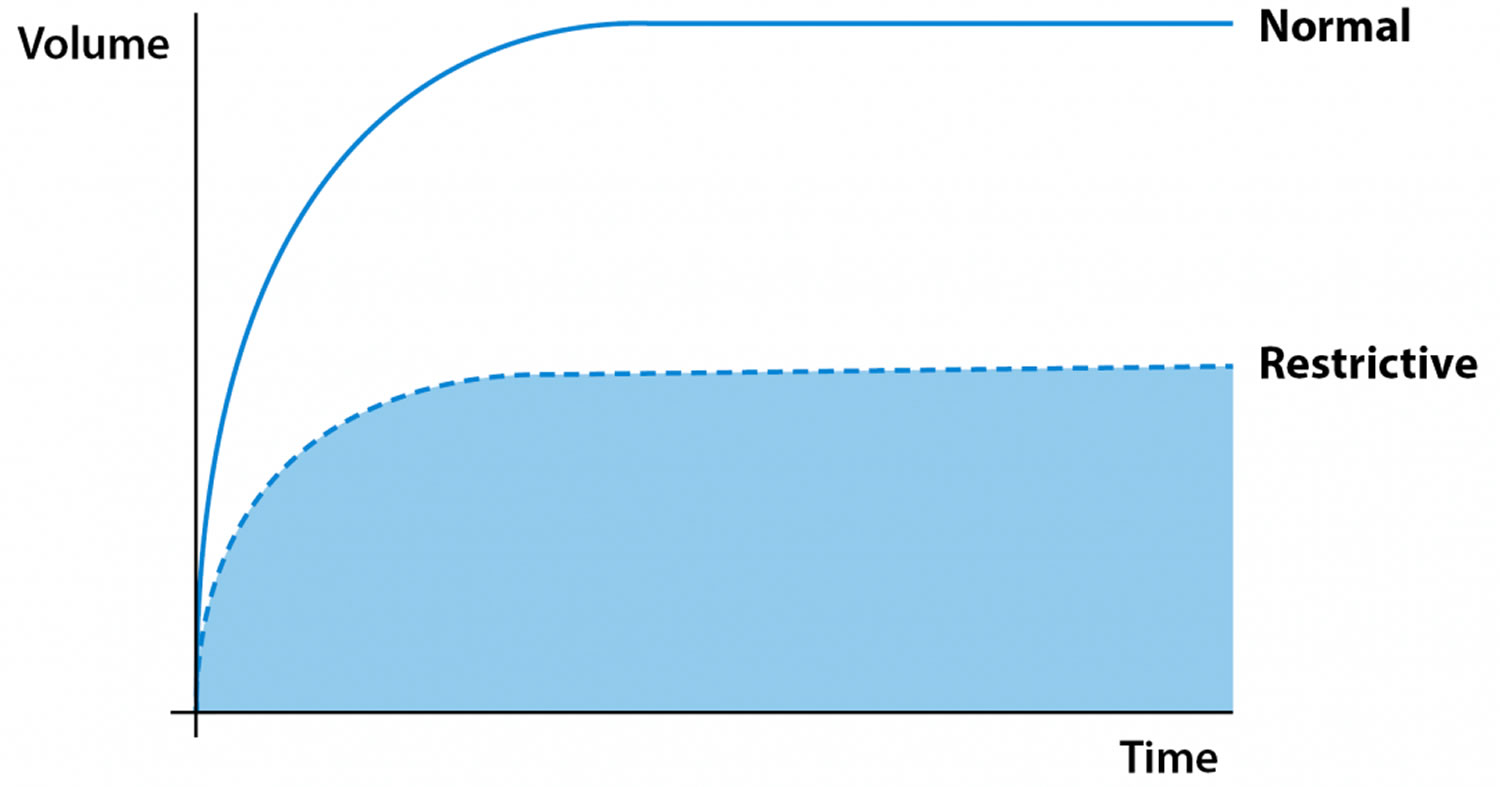
Figure 2. Spirometry Restrictive pattern
Procedures
Bronchoalveolar lavage
In selected cases, bronchoalveolar lavage (BAL) cellular analysis may be helpful to narrow the differential diagnosis. However, the utility of bronchoalveolar lavage in the clinical assessment and management of interstitial lung diseases remains to be established.
Performing bronchoalveolar lavage lymphocytosis in patients with idiopathic pulmonary fibrosis may help predict steroid responsiveness. A predominance of T lymphocytes with an elevated CD4-to-CD8 ratio is characteristic but not diagnostic of sarcoidosis. Significant bronchoalveolar lavage lymphocytosis suggests the presence of a granulomatous interstitial lung disease, suggestive of hypersensitivity pneumonitis, a drug reaction ,or cellular nonspecific interstitial pneumonitis.
Bronchoalveolar lavage fluid may contain malignant cells, asbestos bodies, eosinophils, and hemosiderin macrophages, which assist in making a diagnosis. A progressively bloody lavage specimen would support a diagnosis of diffuse alveolar hemorrhage.
A primary role of bronchoalveolar lavage in the management of interstitial lung disease is to rule out infection. Bronchoalveolar lavage fluid is highly sensitive for bacterial, viral, fungal, and mycobacterial diseases.
Lung biopsy
A lung biopsy is not always required to make a diagnosis in patients suggestive of having iingnterstitial lung diseases. A lung biopsy can provide information that may help lead to a specific diagnosis, help assess for disease activity, exclude neoplastic and infectious processes, establish a definitive diagnosis, and predict the prognosis.Open lung biopsy can be as valuable in selected patients 25 as high-resolution CT scanning, and the American Thoracic Society/European Respiratory Society clinical criteria may misdiagnose patients with interstitial lung disease 26. This is a bit confusing.
Fiberoptic bronchoscopy with transbronchial lung biopsy is often the initial procedure of choice, especially when sarcoidosis, lymphangitic carcinomatosis, eosinophilic pneumonia, Goodpasture syndrome, pulmonary Langerhans cell histiocytosis, hypersensitivity pneumonitis, or infection is suggested based on clinical evidence.
Despite the utility of transbronchial biopsy, certain forms of idiopathic interstitial pneumonias (ie, idiopathic pulmonary fibrosis, nonspecific interstitial pneumonia, lymphocytic interstitial pneumonitis ) require surgical biopsy to make an accurate diagnosis.
Surgical lung biopsy
Video-assisted thoracoscopic lung biopsy is the preferred method for obtaining lung tissue samples for analysis.
Histologic patterns may be helpful in narrowing the differential diagnosis 27. Honeycombing is seen in end-stage disease, in which the original disease process often cannot be differentiated.
The common histologic patterns include interstitial pneumonitis (ie, idiopathic pulmonary fibrosis). Subpleural and paraseptal inflammation is present, with an appearance of temporal heterogeneity. Patchy scarring of the lung parenchyma and normal, or nearly normal, alveoli interspersed between fibrotic areas is the hallmark of this disease. Also, the lung architecture is completely destroyed.
Desquamative interstitial pneumonitis is characterized by diffuse and temporally uniform involvement of the lung parenchyma. The alveoli are filled with macrophages and hyperplastic type II pneumocytes.
Cryptogenic organizing pneumonia (also called proliferative bronchiolitis) is often patchy and peribronchiolar. The proliferation of granulation tissue within small airways and alveolar ducts is excessive and is associated with chronic inflammation of surrounding alveoli.
Diffuse alveolar damage is marked by a nonspecific reaction with diffuse temporally uniform involvement and marked thickening of the alveolar septa; inflammatory cell infiltration and type II cell hyperplasia and fibroblast proliferation are present.
For acute interstitial pneumonia, the pathological appearance is identical to that of diffuse alveolar damage.
In eosinophilic pneumonia, eosinophils and macrophages are the predominant alveolar inflammatory cells, and they also extend into the interstitium.
Lymphocytic interstitial pneumonitis marked by a lymphoid infiltrate that involves both the interstitium and alveolar spaces is the prominent finding.
In nonspecific interstitial pneumonia, the lesions are characterized by a relatively uniform appearance consisting of mononuclear interstitial infiltrates associated with varying degrees of interstitial fibrosis.
Granulomatous lung diseases are marked by granulomas characterized by the accumulation of T lymphocytes, macrophages, and epithelioid cells. These may progress to pulmonary fibrosis.
Restrictive lung disease treatment
Treatment depends on the specific diagnosis, which is based on findings from the clinical evaluation, imaging studies, and lung biopsy.
Corticosteroids, immunosuppressive agents, and cytotoxic agents are the mainstay of therapy for many of the interstitial lung diseases. Objective data assessing the risks and benefits of immunosuppressive and cytotoxic agents to treat diverse interstitial lung disorders are sparse. Direct comparisons among these agents are lacking.
Ancillary therapies include supplemental oxygen therapy, which alleviates exercise-induced hypoxemia and improves performance.
Idiopathic pulmonary fibrosis
The rate of progression of idiopathic pulmonary fibrosis is highly variable, and controversy exists regarding the timing of treatment. The disease may be responsive to treatment in the early, so-called inflammatory stage. idiopathic pulmonary fibrosis always progresses insidiously, and documenting the changes over short periods is difficult. Initiate a trial of therapy for 6-12 weeks, starting as early as possible, with the hope of slowing disease progression. Discontinue therapy if no benefit is observed or if adverse effects develop.
The prognosis for patients with idiopathic pulmonary fibrosis who do not respond to medical therapy is poor. They usually die within 2-3 years. These and other patients with severe functional impairment, oxygen dependency, and a deteriorating course should be listed for lung transplantation.
Conventional therapies (corticosteroids, azathioprine, cyclophosphamide) provide only marginal benefit to patients with idiopathic pulmonary fibrosis 28. Corticosteroids have never been studied against placebo. Retrospective studies have not demonstrated any benefit from steroid monotherapy 29. Acute exacerbations may not respond to high-dose corticosteroid therapy 30.
Intermittent intravenous cyclophosphamide given to idiopathic pulmonary fibrosis patients surviving 6 months improved pulmonary function and reduced prednisone dosage in one study 31. However, current guidelines recommend against the use of combination immunosuppressant therapy, owing to limited efficacy data 32.
Thalidomide has been shown to attenuate pulmonary fibrosis after a bleomycin challenge in animal models 33. A randomized crossover design study has demonstrated a significant reduction in cough and improved quality of life in patients with idiopathic pulmonary fibrosis 34.
Pulmonary rehabilitation has been demonstrated to improve overall quality of life and can provide education and psychosocial support for patients with idiopathic pulmonary fibrosis 35.
A retrospective cohort study found that treatment of gastroesophageal reflux disease was associated with an increased length of survival and reduced radiographic evidence of fibrosis 36.
Supplemental oxygen can be provided for patients with hypoxemia (PaO2< 55 mm Hg or oxygen saturation [SaO2] < 88%) at rest or during exertion. However, rigorous studies of benefit or improvement in quality of life have not been demonstrated, as it has been in the COPD population.
Lung transplantation should be considered for patients with idiopathic pulmonary fibrosis refractory to medical therapy 37. Transplantation has been reserved for patients at advanced stages of idiopathic pulmonary fibrosis. The 5-year mortality rate remains around 50%. However, bronchiolitis obliterans syndrome, a process of progressive fibrosis of the bronchioles, can occur post transplantation and has high mortality.
Because of a lack of response to available anti-inflammatory therapy, alternative approaches to therapy are being pursued 38. Emerging strategies to treat patients with idiopathic pulmonary fibrosis include agents that inhibit epithelial injury or enhance repair, anticytokine approaches, agents that inhibit fibroblast proliferation or induce fibroblast apoptosis, and other novel approaches 39.
Corticosteroids
Corticosteroids are a first-line therapy but are associated with myriad adverse effects. Corticosteroids, the most commonly used drugs, halt or slow the progression of pulmonary parenchymal fibrosis with variable success.
Questions about which patients should be treated, when therapy should be started 40 and what constitutes the best therapy receive uncertain answers at present.
Although subjectively most patients with idiopathic pulmonary fibrosis feel better, an objective improvement occurs in 20-30% patients. A favorable response is a reduction in symptoms; the clearing of radiographs; and improvements in forced vital capacity (FVC), total lung capacity (TLC), and diffusion capacity of the lungs for carbon monoxide (DLCO). The optimal duration of therapy is not known, but treatment for 1-2 years is suggested.
Cytotoxic therapy
Immunosuppressive cytotoxic agents may be considered for patients who do not respond to steroids, experience adverse effects, or have contraindications to high-dose corticosteroid therapy. The failure of steroid therapy is defined as a fall in FVC or TLC by 10%, a worsened radiographic appearance, and a decreased gas exchange at rest or with exercise.
Azathioprine is less toxic than methotrexate or cyclophosphamide and may be preferred as a corticosteroid-sparing agent for disorders that are not life threatening. A response to therapy may not occur for 3-6 months.
Because of potentially serious toxicities, cyclophosphamide is reserved for fulminant or severe inflammatory disorders refractory to alternate therapy.
Antifibrotic therapies
These therapies, including colchicine, are suggested for a variety of fibrotic disorders, including idiopathic pulmonary fibrosis.
idiopathic pulmonary fibrosis subjects given high-dose prednisone had an increased incidence of serious adverse effects and shortened survival compared with those given colchicine in a prospective randomized study 41; therefore, a trial of therapy with colchicine is reasonable in less symptomatic patients or those who are experiencing adverse effects with steroid therapy.
One study showed that in patients with idiopathic pulmonary fibrosis, interferon gamma-1b did not affect progression-free survival, pulmonary function, or quality of life. No survival benefit was demonstrated in this trial 42.
Nintedanib, a triple tyrosine kinase inhibitor of fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF), and platelet-derived growth factor (PDGF), has been demonstrated to lead to a reduction in the decline of FVC, led to improved quality of life, and yielded a reduction in acute exacerbations of idiopathic pulmonary fibrosis 43. In 2014, the INPULSIS studies, two randomized, double-blind, phase 3 trials, were able to demonstrate that nintedanib led to a reduced rate of progression of disease in patients with idiopathic pulmonary fibrosis 44.
Pirfenidone an oral medication that reduces fibroblast proliferation and collagen deposition, via down-regulation of transforming growth factor (TGF)–β and tumor necrosis factor (TNF)–α, was investigated in 2010 in two phase 3 trials 45. Results suggested that pirfenidone may reduce the FVC decline associated with idiopathic pulmonary fibrosis. Some conflicting data necessitated an additional phase 3 study. In 2014, the ASCEND trial, a multicenter, randomized control trial, demonstrated a reduction in the composite outcome of FVC decline and all-cause mortality 44. Additional secondary outcomes demonstrated no significant decrease in all-cause mortality decline in the treatment arm. However, there was a significant improvement in progression-free survival.
Collagen-vascular disease
Therapy for pulmonary fibrosis associated with collagen-vascular disease is controversial because the course may be indolent. Because these diseases begin as an alveolitis, an aggressive approach may be warranted.
Patients with severe disease or those who have a deteriorating course must be treated with corticosteroids, cytotoxic therapy, or both.
Sarcoidosis
Because the disease remits spontaneously, patients with respiratory symptoms and radiographic or pulmonary function evidence of extensive disease may benefit from corticosteroids. Patients with hypercalcemia or extrapulmonary involvement generally require treatment. Therapy should be continued for 6 months or longer; however, even after prolonged treatment, up to 50% of patients relapse after therapy is discontinued.
For patients who do not respond to corticosteroids, alternate therapies (eg, chloroquine, methotrexate, azathioprine) may be used; however, data are limited.
Treatment of extrinsic lung disorders
Patients with nonmuscular chest wall disorders and neuromuscular disease may develop problems with ventilation and gas exchange during sleep. The effect of decreased chest wall and lung compliance or decreased muscle strength is hypercapnia and hypoxemia, which occurs initially during sleep. Identify and treat the cause of muscle weakness.
Treatment of neuromuscular diseases includes preventive therapies to minimize the impact of impaired secretion clearance and the prevention and prompt treatment of respiratory infections.
Patients who develop respiratory failure or have severe gas exchange abnormalities during sleep may be treated with noninvasive positive-pressure ventilation via a nasal or oronasal mask. Patients in whom these devices fail may require a permanent tracheotomy and ventilator assistance with a portable ventilator 46.
Noninvasive ventilation with body-wrap ventilators or positive-pressure ventilation has been proven beneficial because it helps relieve dyspnea and pulmonary hypertension and helps improve RV and gas exchange. Also, hospitalization rates are markedly reduced and the activities of daily living are enhanced 47.
Treatment for massive obesity consists of weight loss, which causes dramatic improvement in pulmonary function test findings but is harder to achieve. These patients require polysomnographic study because of the high incidence of nocturnal hypoventilation or upper airway obstructions. Either continuous positive airway pressure or noninvasive pressure ventilation helps correct hypoventilation and upper airway obstruction.
In advanced disease, when respiratory failure develops, these patients are treated with mechanical ventilation. If they have copious secretions, cannot control their upper airway, or are not cooperative, then invasive ventilation with a tracheotomy tube is indicated. In other patients, eg, those who have good airway control and minimal secretions, use noninvasive ventilation, initially nocturnal, and then intermittently.
Surgical Care
If a pleural disorder is the cause of the restriction, surgery can occasionally be curative. Trapped lung and chronic empyema may be cured with decortication. FVC and FEV1 improve after decortication for chronic empyema, and chest wall deformity may improve after surgery as well 48.
Restrictive lung disease life expectancy
Restrictive lung disease life expectancy depends on the causes of restrictive lung disease and is dependent on the underlying cause of the disease process.
The natural history of interstitial lung diseases is variable. It depends on the specific diagnosis and the extent and severity of lung involvement based on high-resolution CT scanning and lung biopsy 49. Idiopathic pulmonary fibrosis is typically a relentless progressive disorder, and patients have a mean survival of 3-6 years after diagnosis 50. Early recognition of idiopathic pulmonary fibrosis is important for directing patient management and predicting prognosis 15.
Pulmonary sarcoidosis has a relatively benign self-limiting course, with spontaneous recovery or stabilization in most cases 16. However, up to 20% of patients develop pulmonary fibrosis and disability 17.
Prognosis for collagen-vascular diseases, eosinophilic pneumonia, cryptogenic organizing pneumonia and drug-induced lung disease is generally favorable with treatment 51.
Patients with chest wall diseases and neuromuscular disorders develop progressive respiratory failure and often succumb during an intercurrent pulmonary infection 8.
The median survival time for patients with idiopathic pulmonary fibrosis is less than 3 years. Factors that predict poor outcome include older age, male sex, severe dyspnea, history of cigarette smoking, severe loss of lung function, appearance and severity of fibrosis on radiologic studies, lack of response to therapy, and prominent fibroblastic foci on histopathologic evaluation 50.
- Ginde S, Bartz PJ, Hill GD, et al. Restrictive lung disease is an independent predictor of exercise intolerance in the adult with congenital heart disease. Congenit Heart Dis. 2013;8(3):246–254. doi:10.1111/chd.12010 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4832600[↩]
- A Stepwise Approach to the Interpretation of Pulmonary Function Tests. Am Fam Physician. 2014 Mar 1;89(5):359-366. https://www.aafp.org/afp/2014/0301/p359.html[↩]
- Seif NE, ELbadawy AM. Comparative study of mid-thoracic spinal versus epidural anesthesia for open nephrectomy in patients with obstructive/restrictive lung disease: A randomized controlled study. Saudi J Anaesth. 2019 Jan-Mar. 13 (1):52-59.[↩]
- Weinberger SE, Johnson TS, Weiss ST. Clinical significance of pulmonary function tests. Use and interpretation of the single-breath diffusing capacity. Chest. 1980;78(3):483–488.[↩]
- Restrictive Lung Disease. https://emedicine.medscape.com/article/301760-overview[↩][↩]
- Lara AR, Schwarz MI. Diffuse alveolar hemorrhage. Chest. 2010 May. 137 (5):1164-71.[↩]
- Schwarz MI, King TE, eds. Approach to the evaluation and diagnosis of interstitial lung disease. Interstitial Lung Disease. 4th ed. London: BC Decker Inc; 2003. 1-30.[↩]
- Gheita TA, Azkalany GS, El-Fishawy HS, Nour Eldin AM. Shrinking lung syndrome in systemic lupus erythematosus patients; clinical characteristics, disease activity and damage. Int J Rheum Dis. 2011 Oct. 14(4):361-8.[↩][↩]
- James D. Sarcoidosis of the Respiratory System. 1986;8:1-111. Semin Respir Med. 1986. 8:1-111.[↩]
- Leech JA, Ernst P, Rogala EJ, Gurr J, Gordon I, Becklake MR. Cardiorespiratory status in relation to mild deformity in adolescent idiopathic scoliosis. J Pediatr. 1985 Jan. 106 (1):143-9.[↩]
- Pehrsson K, Bake B, Larsson S, Nachemson A. Lung function in adult idiopathic scoliosis: a 20 year follow up. Thorax. 1991 Jul. 46 (7):474-8.[↩]
- Baydur A. Respiratory muscle strength and control of ventilation in patients with neuromuscular disease. Chest. 1991 Feb. 99(2):330-8.[↩]
- Kondoh Y, Taniguchi H, Kawabata Y, Yokoi T, Suzuki K, Takagi K. Acute exacerbation in idiopathic pulmonary fibrosis. Analysis of clinical and pathologic findings in three cases. Chest. 1993 Jun. 103 (6):1808-12.[↩]
- Rice AJ, Wells AU, Bouros D, du Bois RM, Hansell DM, Polychronopoulos V, et al. Terminal diffuse alveolar damage in relation to interstitial pneumonias. An autopsy study. Am J Clin Pathol. 2003 May. 119 (5):709-14.[↩]
- du Bois RM. Evolving concepts in the early and accurate diagnosis of idiopathic pulmonary fibrosis. Clin Chest Med. 2006 Mar. 27 (1 Suppl 1):S17-25, v-vi.[↩][↩][↩]
- Morgenthau AS, Teirstein AS. Sarcoidosis of the upper and lower airways. Expert Rev Respir Med. 2011 Dec. 5(6):823-33.[↩][↩][↩]
- Margaritopoulos GA, Vasarmidi E, Jacob J, Wells AU, Antoniou KM. Smoking and interstitial lung diseases. Eur Respir Rev. 2015 Sep. 24 (137):428-35.[↩][↩]
- Neghab M, Mohraz MH, Hassanzadeh J. Symptoms of respiratory disease and lung functional impairment associated with occupational inhalation exposure to carbon black dust. J Occup Health. 2011 Dec 9. 53(6):432-8.[↩]
- Baur X, Fischer A, Budnik LT. Spotlight on the diagnosis of extrinsic allergic alveolitis (hypersensitivity pneumonitis). J Occup Med Toxicol. 2015. 10:15.[↩]
- Shin JM, Kim TH, Haam S, Han K, Byun MK, Chang YS, et al. The repeatability of computed tomography lung volume measurements: Comparisons in healthy subjects, patients with obstructive lung disease, and patients with restrictive lung disease. PLoS One. 2017. 12 (8):e0182849[↩]
- Müller NL. Clinical value of high-resolution CT in chronic diffuse lung disease. AJR Am J Roentgenol. 1991 Dec. 157(6):1163-70.[↩]
- Fishbein MC. Diagnosis: to biopsy or not to biopsy: assessing the role of surgical lung biopsy in the diagnosis of idiopathic pulmonary fibrosis. Chest. 2005 Nov. 128 (5 Suppl 1):520S-525S.[↩]
- Remy-Jardin M, Remy J, Giraud F, Wattinne L, Gosselin B. Computed tomography assessment of ground-glass opacity: semiology and significance. J Thorac Imaging. 1993 Fall. 8(4):249-64.[↩]
- Buda N, Piskunowicz M, Porzezińska M, Kosiak W, Zdrojewski Z. Lung Ultrasonography in the Evaluation of Interstitial Lung Disease in Systemic Connective Tissue Diseases: Criteria and Severity of Pulmonary Fibrosis – Analysis of 52 Patients. Ultraschall Med. 2016 Aug. 37 (4):379-85.[↩]
- Wagner JD, Stahler C, Knox S, Brinton M, Knecht B. Clinical utility of open lung biopsy for undiagnosed pulmonary infiltrates. Am J Surg. 1992 Aug. 164(2):104-7; discussion 108.[↩]
- Peckham RM, Shorr AF, Helman DL Jr. Potential limitations of clinical criteria for the diagnosis of idiopathic pulmonary fibrosis/cryptogenic fibrosing alveolitis. Respiration. 2004 Mar-Apr. 71(2):165-9.[↩]
- Flaherty KR, Toews GB, Travis WD, et al. Clinical significance of histological classification of idiopathic interstitial pneumonia. Eur Respir J. 2002 Feb. 19(2):275-83.[↩]
- Winterbauer RH, Hammar SP, Hallman KO, et al. Diffuse interstitial pneumonitis. Clinicopathologic correlations in 20 patients treated with prednisone/azathioprine. Am J Med. 1978 Oct. 65(4):661-72.[↩]
- Richeldi L, Davies HR, Ferrara G, Franco F. Corticosteroids for idiopathic pulmonary fibrosis. Cochrane Database Syst Rev. 2003. CD002880[↩]
- Parambil JG, Myers JL, Ryu JH. Histopathologic features and outcome of patients with acute exacerbation of idiopathic pulmonary fibrosis undergoing surgical lung biopsy. Chest. 2005 Nov. 128(5):3310-5[↩]
- Baughman RP, Lower EE. Use of intermittent, intravenous cyclophosphamide for idiopathic pulmonary fibrosis. Chest. 1992 Oct. 102(4):1090-4[↩]
- Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011 Mar 15. 183 (6):788-824[↩]
- Tabata C, Tabata R, Kadokawa Y, Hisamori S, Takahashi M, Mishima M, et al. Thalidomide prevents bleomycin-induced pulmonary fibrosis in mice. J Immunol. 2007 Jul 1. 179 (1):708-14.[↩]
- Horton MR, Santopietro V, Mathew L, Horton KM, Polito AJ, Liu MC, et al. Thalidomide for the treatment of cough in idiopathic pulmonary fibrosis: a randomized trial. Ann Intern Med. 2012 Sep 18. 157 (6):398-406.[↩]
- De Vries J, Kessels BL, Drent M. Quality of life of idiopathic pulmonary fibrosis patients. Eur Respir J. 2001 May. 17 (5):954-61.[↩]
- Lee JS, Ryu JH, Elicker BM, Lydell CP, Jones KD, Wolters PJ, et al. Gastroesophageal reflux therapy is associated with longer survival in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011 Dec 15. 184 (12):1390-4.[↩]
- Shah NR, Noble P, Jackson RM, et al. A critical assessment of treatment options for idiopathic pulmonary fibrosis. Sarcoidosis Vasc Diffuse Lung Dis. 2005 Oct. 22(3):167-74.[↩]
- Hunninghake GW, Kalica AR. Approaches to the treatment of pulmonary fibrosis. Am J Respir Crit Care Med. 1995 Mar. 151(3 Pt 1):915-8.[↩]
- Goldstein RH, Fine A. Potential therapeutic initiatives for fibrogenic lung diseases. Chest. 1995 Sep. 108(3):848-55.[↩]
- Turner-Warwick M, Burrows B, Johnson A. Cryptogenic fibrosing alveolitis: response to corticosteroid treatment and its effect on survival. Thorax. 1980 Aug. 35(8):593-9.[↩]
- Douglas WW, Ryu JH, Swensen SJ, et al. Colchicine versus prednisone in the treatment of idiopathic pulmonary fibrosis. A randomized prospective study. Members of the Lung Study Group. Am J Respir Crit Care Med. 1998 Jul. 158(1):220-5.[↩]
- Raghu G, Brown KK, Bradford WZ, et al. A placebo-controlled trial of interferon gamma-1b in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2004 Jan 8. 350(2):125-33.[↩]
- Richeldi L, Costabel U, Selman M, Kim DS, Hansell DM, Nicholson AG, et al. Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N Engl J Med. 2011 Sep 22. 365 (12):1079-87.[↩]
- King TE Jr, Bradford WZ, Castro-Bernardini S, Fagan EA, Glaspole I, Glassberg MK, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014 May 29. 370 (22):2083-92.[↩][↩]
- Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (CAPACITY): two randomised trials. Lancet. 2011 May 21. 377 (9779):1760-9.[↩]
- Bach JR, Chaudhry SS. Standards of care in MDA clinics. Muscular Dystrophy Association. Am J Phys Med Rehabil. 2000 Mar-Apr. 79 (2):193-6.[↩]
- Bach JR, Alba AS. Intermittent abdominal pressure ventilator in a regimen of noninvasive ventilatory support. Chest. 1991 Mar. 99 (3):630-6.[↩]
- Gokce M, Okur E, Baysungur V, Ergene G, Sevilgen G, Halezeroglu S. Lung decortication for chronic empyaema: effects on pulmonary function and thoracic asymmetry in the late period. Eur J Cardiothorac Surg. 2009 Oct. 36 (4):754-8.[↩]
- Gay SE, Kazerooni EA, Toews GB, et al. Idiopathic pulmonary fibrosis: predicting response to therapy and survival. Am J Respir Crit Care Med. 1998 Apr. 157(4 Pt 1):1063-72.[↩]
- Bjoraker JA, Ryu JH, Edwin MK, et al. Prognostic significance of histopathologic subsets in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 1998 Jan. 157(1):199-203.[↩][↩]
- Patterson KC, Strek ME. Pulmonary fibrosis in sarcoidosis. Clinical features and outcomes. Ann Am Thorac Soc. 2013 Aug. 10 (4):362-70.[↩]





{kind=link}