
Contents
- What is RPR test
- Screening for syphilis infection
- Laboratory diagnosis of syphilis
- Serologic testing algorithms
- RPR test results
- Syphilis Treatment
What is RPR test
RPR test is short for rapid plasma reagin test, is a screening test for syphilis. RPR test measures substances (proteins) called antibodies that are present in the blood of people who may have syphilis. A blood sample is needed for the RPR test.
The RPR test can be used to screen for syphilis. It is used to screen people who have symptoms of sexually transmitted infections and is routinely used to screen pregnant women for the disease.
Several states also require that couples be screened for syphilis before getting a marriage license.
The RPR test is also used to see how treatment for syphilis is working. After treatment with antibiotics, the levels of syphilis antibodies should fall. These levels can be monitored with another RPR test. Unchanged or rising levels can mean a persistent infection.
The RPR test is similar to the venereal disease research laboratory (VDRL) test.
Syphilis is an infection caused by the bacterium Treponema pallidum that is most often spread by sexual contact, such as through direct contact with a syphilis sore (chancre), a firm, raised, painless sore.
Syphilis is easily treated with antibiotics but can cause severe health problems if left untreated. An infected mother can also pass the disease to her unborn child, with serious and potentially fatal consequences for the baby.
There are several possible stages with syphilis:
- Primary syphilis—the primary stage begins about 2-3 weeks after being infected. One or more chancres appear, usually on the part of the body exposed to the sexual partner’s chancre, such as on the penis or vagina. However, the chancre is usually painless and may go unnoticed, especially if it is in the rectum or on the cervix, and disappears within 4-6 weeks, healing regardless of whether the infected person is treated or not.
- Secondary syphilis—if primary syphilis is left untreated, secondary syphilis may occur from 6 weeks to 6 months after the chancre first appears. It is marked by a skin rash that often is rough, red, and spotted, appearing frequently on the palms of the hands and the bottoms of the feet (an unusual place for most other causes of rashes) and that usually does not itch. There may be other symptoms as well, such as fever, fatigue, swollen lymph nodes (“glands”), sore throat, and body aches.
- Late, tertiary syphilis—if untreated, secondary syphilis may continue into a latent stage, during which an infected person has no symptoms but continues to have the infection, and this stage can last for years. If still untreated, about 15% of people will develop the complications of late, or tertiary, syphilis. In these cases, the bacteria can damage the heart, eyes, brain, nervous system, bones, joints, or almost any other part of the body. When the central nervous system is affected, it is called neurosyphilis. Tertiary syphilis can last for years, with the final stage leading to mental illness, blindness, other neurological problems, heart disease, and death.
Syphilis is most infectious during the primary and secondary stages. In 2014, about one-third of over 63,000 new cases of syphilis reported to the Centers for Disease Control and Prevention (CDC) were primary or secondary stage syphilis. Eighty-three percent of these cases were among men who have sex with men.
Syphilis can be treated with antibiotics, preferably penicillin. Newly acquired infections can be cured easily; however, longer treatment may be needed for someone who has been infected for more than a year.
Screening for syphilis infection
In the United States, the most influential recommendations for syphilis screening are from the Centers for Disease Control and Prevention (CDC) 2015 STD Treatment Guidelines 1 and the 2016 US Preventive Services Task Force Recommendation Statement on Screening for Syphilis Infection in Non-pregnant Adults and Adolescents 2. In addition, in 2009 the US Preventive Services Task Force issued screening recommendations for Syphilis Infection in Pregnancy 3. The 2015 STD Treatment Guidelines and the 2016 US Preventive Services Task Force Recommendations both identify men who have sex with men and persons living with HIV as the highest risk groups for acquiring syphilis and therefore high priority groups for syphilis screening 2. In addition, the US Preventive Services Task Force lists four other “risk factors” associated with increased syphilis prevalence rates: history of incarceration, history of exchanging sex for money, certain racial/ethnic groups (highest in blacks), and being a male younger than 29 years of age; certain regional variations may also correlate with risk, such as residence in a local area with a high syphilis rate 2. Routine screening is recommended for several other specific populations, including patients who are pregnant, persons taking preexposure prophylaxis for HIV prevention, and persons who have a sex partner diagnosed with syphilis. The following summarizes recommendations from the CDC 1 and the US Preventive Services Task Force 2.
Summary of Recommendations for Routine Screening for Syphilis
- Women Who Have Sex with Men: The CDC and US Preventive Services Task Force do not recommend routine syphilis screening for nonpregnant women. The US Preventive Services Task Force recommends syphilis screening for nonpregnant women who are at increased risk for syphilis infection. These recommendations are the same for women who have sex with men and women who have sex with women.
- Women Who Have Sex with Women: The CDC recommends that syphilis screening for sexually active women who have sex with women should be based on the same recommendations as for sexually active women who have sex with men 4.
- Men Who Have Sex Only with Women: The CDC and the US Preventive Services Task Force do not recommend routine syphilis screening for men who have sex only with women. The US Preventive Services Task Force recommends syphilis screening men who are at increased risk of infection (see above “risk factors”) 4.
- Men Who Have Sex with Men: For sexually active men who have sex with men, the CDC and the US Preventive Services Task Force recommend syphilis screening at least annually. More frequent screening (every 3 to 6 months) is recommended for men who have sex with men who have ongoing risk for acquiring syphilis 4.
- Transgender Men and Women: The CDC recommends screening for syphilis in transgender men (“trans-men”) and transgender women (“trans-women”) should be based on age, current anatomy, and sexual practices 4.
- Persons with HIV Infection: The CDC and the US Preventive Services Task Force recommend syphilis screening should be performed at the initial HIV evaluation and at least annually thereafter in all sexually active persons with HIV 1. More frequent screening (every 3 to 6 months) is indicated for persons with HIV who have ongoing risk for acquiring syphilis.
- Pregnant Women: The CDC, US Preventive Services Task Force, and the American College of Obstetrics and Gynecology (ACOG) recommend syphilis screening at the first prenatal visit for all pregnant women 2. The recommendation to screen pregnant women for syphilis is mandated by most state laws 5. Women who are at high risk for syphilis or live in areas of high syphilis morbidity should be screened again early in the third trimester (around 28 weeks gestation) and at delivery. Any woman who delivers a stillborn infant after 20 weeks of gestation should be tested for syphilis. Screening for syphilis should occur during each pregnancy.
- Adolescents: The CDC does not recommend routine screening of adolescents for syphilis, but young men who have sex with men and pregnant adolescent females should be screened for syphilis 4.
- Neonates: Neonates should not be discharged from the hospital unless the syphilis serologic status of the mother has been determined at least one time during pregnancy (and again at delivery if there was ongoing risk for acquiring syphilis during pregnancy) 4.
- Correctional Facilities: The CDC recommends routine screening should be performed based the local area and institutional prevalence of early (primary, secondary, and early latent) infectious syphilis. Correctional facilities should stay apprised of syphilis prevalence as it changes over time 1.
Laboratory diagnosis of syphilis
The laboratory diagnosis of syphilis is challenging and requires using a combination of clinical and laboratory criteria to differentiate active infection, prior infection, and absence of infection 6. Treponema pallidum cannot be cultivated on artificial medium, but the organism can be grown using special techniques that involve inoculation in rabbits. In clinical samples, spirochetes can occasionally be visualized in specimens taken from cutaneous lesions using dark-field microscopy techniques. In addition, silver staining and immunohistochemical staining of tissue samples can demonstrate characteristic spirochetes on clinical biopsy specimens. Use of dark-field microscopy or immunohistochemical staining on oral specimens is not recommended due to the extremely poor specificity caused by abundant non-syphilitic oral Treponema species. Serologic testing remains the primary tool for diagnosis in most patients with syphilis and these tests include “nontreponemal” and “treponemal” tests. Although PCR testing is sometimes used for research purposes, there is no FDA-approved PCR test for syphilis at present. Research use of PCR detection of Treponema pallidum DNA has expanded the clinical sites from which Treponema pallidum can be detected.
The most common syphilis tests detect antibodies in the blood that are produced in response to a Treponema pallidum infection. Some methods that are used less commonly directly detect the bacterium or its genetic material (DNA).
Serologic testing for syphilis
In the absence of dark-field microscopy, a probable diagnosis of syphilis is possible with the use of two types of serologic tests: nontreponemal and treponemal. Use of only one type of serologic test is insufficient for diagnosis since each test used alone has major limitations, including false-positive results in persons without syphilis and the inability for treponemal tests to distinguish between recent and distant infection. Both types of tests have several advantages and disadvantages as well as differing test characteristics.
Nontreponemal serologic tests
The nontreponemal tests include Venereal Disease Research Laboratory (VDRL), Rapid Plasma Reagin (RPR), Toluidine Red Unheated Serum Test (TRUST), and Unheated Serum Reagin (USR) 6. These tests measure IgM and IgG antibody and are not specific for Treponema pallidum. Nontreponemal test results are reported with a qualitative result and a quantitative titer, which usually correlates with disease activity 1. A fourfold change in titer, equivalent to a change of two dilutions (e.g., from 1:16 to 1:4 or from 1:8 to 1:32) is considered necessary to demonstrate a clinically significant difference 7. Sequential serologic tests in individual patients should be performed using the same testing method, preferably by the same laboratory. The Venereal Disease Research Laboratory (VDRL) and RPR tests are equally valid assays, but quantitative results from the two tests cannot be compared directly because RPR titers are often slightly higher than Venereal Disease Research Laboratory (VDRL) titers. TRUST is similar to RPR test whereas Unheated Serum Reagin (USR) is similar to VDRL, though in the United States TRUST and Unheated Serum Reagin (USR) are not often used. The nontreponemal tests have several drawbacks, including (1) they are labor intensive to perform, (2) results are typically not available for at least 7 days, (3) the tests have low sensitivity in certain stages, particularly early primary, late latent, and tertiary, and (4) false-positive reactions can occur. Nontreponemal tests usually become nonreactive with time after treatment. In some patients, however, nontreponemal antibodies can persist at a low titer (the definition “low” titer is dependent on laboratory and clinical context, but less than 1:8 is generally consider “low”) for a long period of time, sometimes for the life of the patient. This response is referred to as the “serofast reaction.” In addition, in some patients, nontreponemal tests may, with time, become nonreactive in the absence of therapy.
Treponemal serologic tests
The treponemal serologic tests include Treponema pallidum particle agglutination (TP-PA), fluorescent treponemal antibody absorption (FTA-ABS), and various enzyme immunoassays (EIAs) and chemiluminescence immunoassays 6. These tests measure antibody directed against Treponema pallidum antigens by particle agglutination, immunofluorescence, or enzyme immunoassay; some detect IgG only whereas others detect both IgM and IgG. These qualitative tests most often remain reactive for life, even after adequate treatment, but 15% to 25% of patients treated during the primary stage revert to being serologically nonreactive after two to three years 8. Treponemal antibody titers correlate poorly with disease activity, and they should not be used to assess treatment response.
Patterns of serologic reactivity and sensitivity of tests
The common patterns for serologic reactivity with syphilis tests depend on the specific test used, the stage of syphilis, and whether the patient has received treatment 9. The sensitivity of serologic testing also varies based on the test used and stage of syphilis (Table 1). Serologic testing for syphilis has the highest yield during secondary syphilis. Serologic tests for syphilis may be negative during very early primary syphilis. Thus, when serologic tests do not correspond with clinical findings suggestive of primary syphilis, presumptive treatment is recommended if the patient has known risk factors for syphilis; in this setting, use of other tests, such as dark-field microscopy, biopsy, or PCR, should be considered.
Table 1. Sensitivity and Specificity of common serological tests in Untreated Syphilis
| Sensitivity During Stage of Infection, % (range) | Specificity, % range | |||||
|---|---|---|---|---|---|---|
| Test | Primary | Secondary | Latent | Late | ||
| *FTA-ABS and TP-PA are generally considered equally sensitive in the primary stage of disease. Abbreviations: | ||||||
| VDRL | 78 (74-87) | 100 | 95 (88-100) | 71 (37-94) | 98 (96-99) | |
| RPR | 86 (77-99) | 100 | 98 (95-100) | 73 | 98 (93-99) | |
| FTA-ABS | 84 (70-100) | 100 | 100 | 96 | 97 (94-100) | |
| TP-PA | 88 (86-100) | 100 | 100 | NA | 96 (95-100) | |
| ELISA (IgG) | 100 | 100 | 100 | NA | 100 | |
Prior Serologic Testing for Syphilis
The healthcare professional should determine the date and results of the patient’s most recent serologic test for syphilis, even if the patient reports no history of the disease. Prior results, if available, are particularly helpful when evaluating a patient that has a low titer serologic test for syphilis, no signs or symptoms that suggest a clinical diagnosis of syphilis, and no known contact with an early case of syphilis. Local health departments can often provide information on whether the patient has been reported as having had syphilis in the past, including reported serologic test results and treatment history.
Serologic testing algorithms
Given that treponemal and nontreponemal tests each have significant advantages and disadvantages, these lab tests are used together as part of a screening algorithm in order to maximize sensitivity and specificity for the detection of syphilis infection. Clinicians should be aware of their institution’s chosen method in order to most efficiently use serologic tests to screen for, diagnose, and monitor syphilis disease.
Standard (Traditional) Syphilis Screening Algorithm
Traditionally, the syphilis screening algorithm has consisted of initial screening with a nontreponemal test (VDRL or RPR), with further testing on a positive initial test with a treponemal test (TP-PA or EIA) (Figure 1). Patients with a negative screening test were relegated to periodic repeat screening whereas patients with positive results required a treponemal test to confirm a diagnosis of syphilis. The major limitations with using a nontreponemal test for initial screening include the personnel time required to perform a labor-intensive test, biologic false positives (i.e. pregnancy, medication use, and other conditions) and, as with all diagnostic tests for syphilis, the inability to detect early primary or latent infection.
Figure 1. Standard syphilis screening algorithm
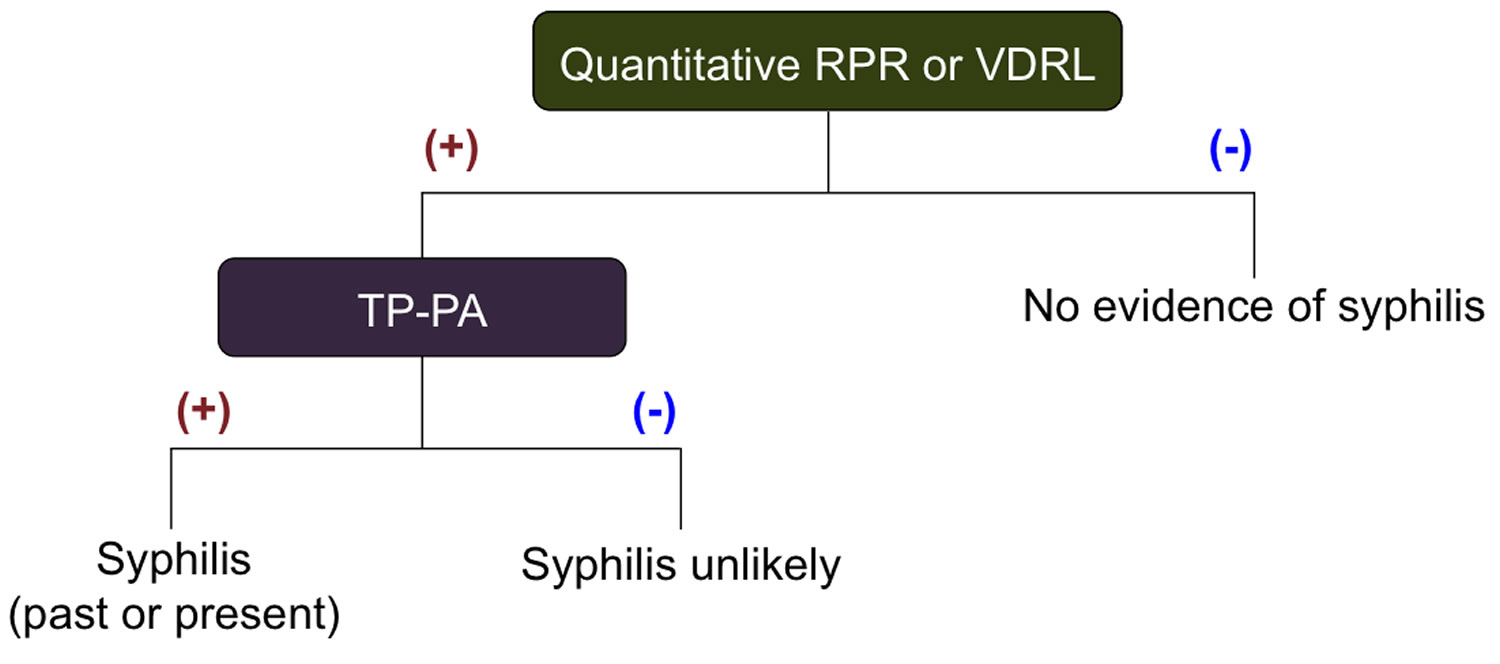
Abbreviation: TP-PA =Treponema pallidum-Particle agglutination
[Source 1 ]Reverse Sequence Syphilis Screening Algorithm
Another option for syphilis screening is to use Treponema pallidum-specific enzyme immunoassays (EIAs) or chemiluminescence immunoassays (CIAs) as an initial screening test. In recent years, increasing numbers of clinical laboratories and blood banks have begun using treponemal EIA or chemiluminescence immunoassays (CIAs) as the initial screening laboratory test for syphilis. With this approach, a positive enzyme immunoassay (EIA) or chemiluminescence immunoassay (CIA) test is followed by further testing with a nontreponemal test—often referred to as reverse screening (Figure 2). In the reverse screening algorithm, negative treponemal results are relegated to follow-up screening as with the standard (traditional) algorithm. Positive treponemal results undergo a confirmatory nontreponemal test (i.e. RPR) to guide management. In the event of a positive EIA and a negative nontreponemal test, a second confirmatory treponemal test (TP-PA) is performed. If either of the confirmatory tests is positive and there is no history of prior, treated syphilis, the patient is diagnosed with syphilis 11. This ‘reverse screening algorithm’ has several advantages and disadvantages distinguishing it from the standard (traditional) screening algorithm. Advantages of the reverse sequence algorithm include improved detection of early primary and treated infection, low cost, and reduced laboratory time and effort (much less pipetting and circumventing the manual dilutions of nontreponemal testing).
Figure 2. Reverse Sequence Syphilis Screening Algorithm
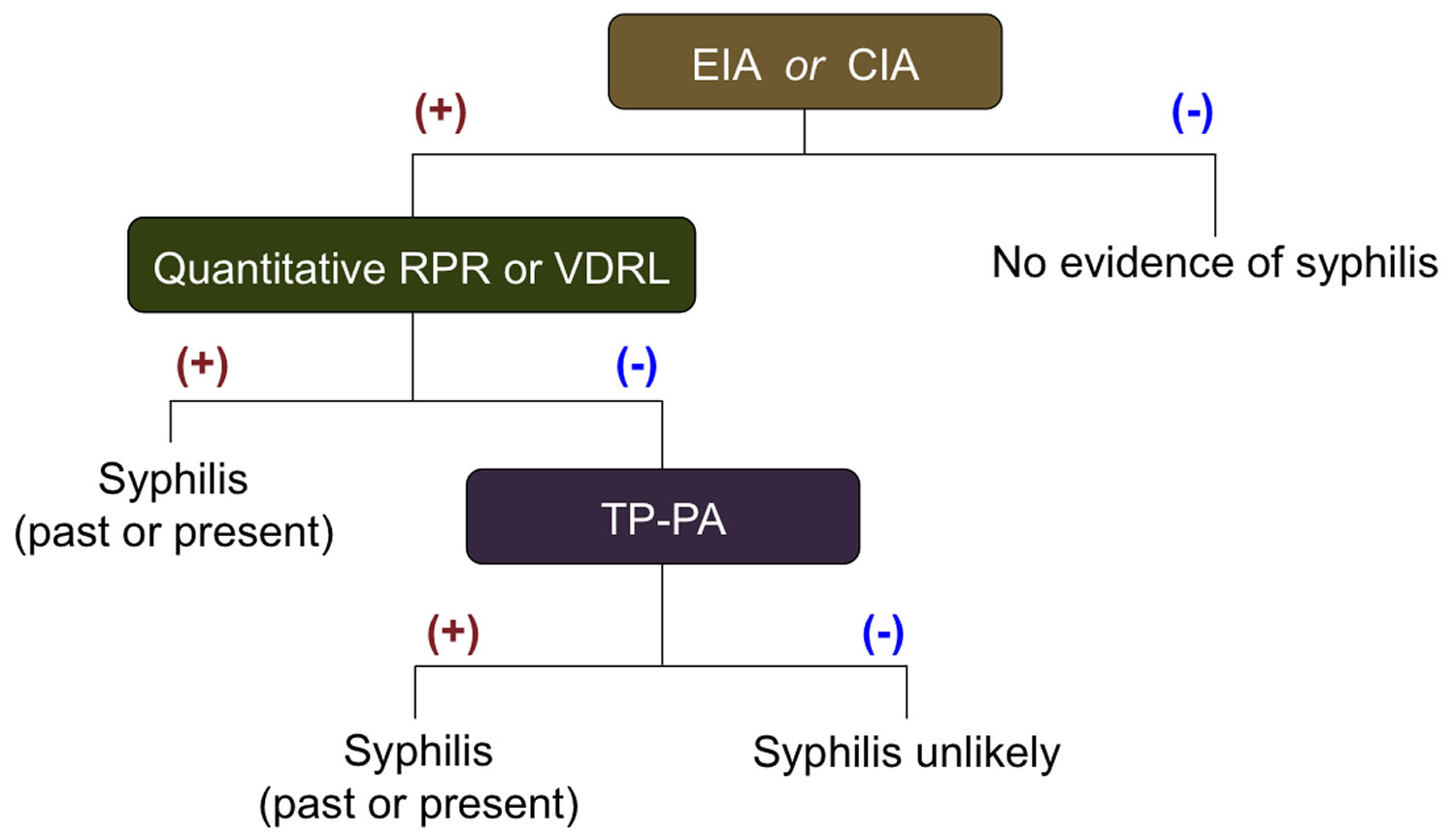
Abbreviations:
- Treponema pallidum-specific enzyme immunoassay (EIA) or chemiluminescence immunoassay (CIA)
- VDRL = Venereal Disease Research Laboratory
- RPR = Rapid Plasma Reagin
- FTA-ABS = Fluorescent Treponemal Antibody Absorbed
- TP-PA =Treponema pallidum-Particle agglutination
- ELISA= Enzyme Linked Immunoassay
Discordant Test Results Using Reverse Screening
In the scenario where a patient has a positive treponemal screening test (EIA), a negative nontreponemal test, and a positive second treponemal test (TP-PA), there are several possible scenarios: prior treated syphilis, early syphilis, untreated latent syphilis, or false-positive test. If the patient has received prior treatment for syphilis and has no evidence by history or examination for recent infection with Treponema pallidum, then the patient does not require further evaluation or management 1. Patients without prior treatment and no evidence for recent infection are considered to have latent syphilis and require further evaluation and treatment. If recent infection possibly occurred, then repeat nontreponemal testing should take place 2 to 3 weeks later; if this repeat testing is positive the patient likely has early syphilis and if the test is negative then further evaluation is usually not needed.
RPR test results
Normal RPR test results
A negative test result is considered normal. However, the body does not always produce antibodies specifically in response to the syphilis bacteria, so the test is not always accurate. False-negatives may occur in people with early- and late-stage syphilis. More testing may be needed before ruling out syphilis.
RPR test positive
A positive RPR test result may mean that you have syphilis. If the screening RPR test is positive, the next step is to confirm the diagnosis with a more specific test for syphilis, such as Fluorescent Treponemal Antibody Absorbed (FTA-ABS). The FTA-ABS (Fluorescent Treponemal Antibody Absorbed) test will help distinguish between syphilis and other infections or conditions.
How well the RPR test can detect syphilis depends on the stage of the infection. The RPR test is most sensitive (almost 100%) during the middle stages of syphilis. It is less sensitive during the earlier and later stages of the infection.
False-positive reactions
With both nontreponemal and treponemal serologic tests for syphilis, false-positive reactions can occur 12. The most common caused of false-positive testings include older age, autoimmune disorders, cardiovascular disease, pregnancy, malaria, leprosy, other spirochete infections, and recent immunizations 1.
Some conditions may cause a false-positive RPR test, including:
- IV drug use
- Lyme disease
- Certain types of pneumonia
- Malaria
- Pregnancy
- Systemic lupus erythematosus and some other autoimmune disorders
- Tuberculosis (TB)
Current syphilis serologic screening algorithms include a nontreponemal titer (VDRL or RPR) to help clarify disease activity. Infections can thus be differentiated based on active disease, prior treatment, and time since prior screening. Symptomatic patients should be classified by stage of syphilis based on clinical findings, including determination of whether they have evidence of neurologic or ophthalmologic disease. Patients without a history of treatment for syphilis should be offered therapy based on clinical findings and the stage of disease. Asymptomatic, previously untreated persons who have not had syphilis testing in the prior year should be considered to have late latent syphilis. All patients who have syphilis should be tested for HIV infection, and those with primary or secondary syphilis who live in areas with a high prevalence of HIV should be retested for HIV after three months (if the first HIV test result was negative). Doctors should consider screening patients with syphilis for other STDs (sexually transmitted diseases), based on risk.
False-Negative Reaction (“Prozone Effect”)
Infrequently, patients may have a false-negative reaction with nontreponemal testing due to the “prozone effect” 13. The prozone effect occurs when very high serum antibodies supersaturate the antigens used in the nontreponemal assay, thereby interfering with the antigen-antibody lattice network needed to visualize a flocculation reaction 14. Overall, this occurs in less than 2% of cases of syphilis 15. This false-negative reaction is most likely to occur in patients with secondary syphilis and HIV infection. If clinical suspicion of secondary syphilis is high and the nontreponemal testing is negative, the clinician should alert the laboratory of a suspected prozone effect and the laboratory should reevaluate the clinical sample after diluting the serum, typically a 1/16 dilution.
Positive titers in patients previously treated for syphilis
Although patients with early syphilis usually have a fourfold or greater decline in nontreponemal titer within 12 months after treatment, some fail to achieve seroreversion at month 12 16. Patients previously treated for syphilis who had a documented adequate reduction in nontreponemal titer after treatment may have a persistent low-positive nontreponemal titer that does not significantly change; this is called a serofast state and they do not require additional therapy. Patients with prior treatment and higher (but unchanged) nontreponemal titer are considered treatment failures unless there is clinical suspicion for reinfection.
Diagnosis of Latent Syphilis
Persons are diagnosed with latent syphilis when they have: (1) serologic evidence of Treponema pallidum infection, (2) no past diagnosis of syphilis, and (3) no active syphilis-related signs or symptoms. It is often difficult to determine the duration of infection in a patient with latent syphilis.
Laboratory evaluation for neurosyphilis
Neurologic involvement can occur during any stage of syphilis. Cerebrospinal fluid (CSF) abnormalities have been noted in 13% of patients with untreated primary syphilis and 25% to 40% of patients with untreated secondary syphilis 17. Although these CSF laboratory abnormalities are common in persons with early syphilis, no evidence exists to support variation from recommended treatment for syphilis at any stage in the absence of clinical neurologic findings, with the exception of tertiary syphilis. In addition to work-up of clinically suspected neurosyphilis, there are a number of additional indications to perform cerebrospinal fluid (CSF) evaluation.
Several studies have shown that among persons with HIV and syphilis, cerebrospinal fluid (CSF) abnormalities (mononuclear pleocytosis and elevated protein) are associated with a CD4 count of 350 cells/mm3 or less and/or a nontreponemal serologic test titer of greater than or equal to 1:32 1. Data are lacking regarding the benefits of a CSF examination in this setting. In general, persons with HIV infection tend to have more frequent CSF abnormalities in the absence of neurologic symptoms, and the presence of 20 or more white blood cells/mm³ might improve the specificity of probable neurosyphilis in this patient population 1. When using a nontreponemal test to evaluate for neurosyphilis, the CSF VDRL is preferred over the CSF RPR test 18. For more detailed information on the diagnosis of neurosyphilis including interpretation of CSF findings, consult the 2015 STD Treatment Guidelines 19.
Diagnosis of syphilis in patients with HIV Coinfection
Syphilis and HIV infection frequently coexist. In general, the clinical course of syphilis in persons with HIV infection is similar to that in persons not infected with HIV. Although not common, unusual serologic responses among persons with HIV infection can occur. If the clinical suspicion of syphilis is high and the serologic tests for syphilis are negative, then use of other tests (e.g., biopsy of the lesion or rash) should be considered. Conventional therapy is usually effective. After appropriate therapy, persons with HIV infection more frequently demonstrate “high serofast” values of nontreponemal serologic tests (often defined as RPR greater than or equal to 1:8) 1.
Diagnosis of syphilis in Infants and Children
The diagnosis of congenital syphilis is often difficult since maternal nontreponemal and treponemal IgG antibodies can be transferred through the placenta to the fetus. The decision to treat a neonate (aged fewer than 30 days) is based on: (1) identification of syphilis in the mother; (2) adequacy of maternal treatment; (3) clinical, laboratory, and radiographic evidence of disease in the neonate; and (4) comparison of maternal and neonatal nontreponemal serologic titer. Based on these factors, neonates are classified as: (1) proven or highly probable congenital syphilis, (2) possible congenital syphilis, (3) congenital syphilis less likely, or 4) congenital syphilis unlikely.
Reporting and Referral to Health Departments
Patients with primary, secondary or early latent syphilis, or syphilis of unknown duration with a high nontreponemal serologic test titer (greater than 1:32), should be referred to the local health department STD program for interview, partner elicitation, and partner follow-up. The follow-up of patients with early syphilis is a public health priority. Laws and regulations in all states require that persons diagnosed with syphilis be reported to public health authorities. Reporting can be provider-based or laboratory-based. Providers unsure of reporting requirements should seek advice from state or local health departments or STD programs. To locate a state health department, see the CDC resource tool Public Health Resources: State or Territorial Health Departments.
Syphilis Treatment
Penicillin G, administered parenterally, is the preferred drug for treating of all stages of syphilis. The preparation(s) of penicillin used (i.e., benzathine, aqueous procaine, or aqueous crystalline), the dosage, and the length of treatment depend on the stage and clinical manifestations of the disease. However, neither benzathine-procaine penicillin co-formulations nor oral penicillin preparations are considered appropriate for the treatment of syphilis 1. Reports have identified the inappropriate use of combination benzathine-procaine penicillin (Bicillin C-R) instead of the standard benzathine penicillin G (Bicillin L-A) product 20. Doctors, pharmacists, and purchasing agents should be aware of the similar names of these two products and avoid use of the inappropriate combination therapy agent for treating syphilis. It is important to understand that benzathine penicillin G is slowly released from the intramuscular site due to extremely low solubility and is also hydrolyzed to penicillin G; the combination of slow absorption and hydrolysis results in prolonged low serum levels of penicillin.
2015 STD Treatment Guidelines: Primary and Secondary Syphilis Treatment of Primary and Secondary Syphilis 19
Recommended for Adults
- Benzathine penicillin G2.4 million units IM in a single dose
- Note: Available data demonstrate that use of additional doses of benzathine penicillin G, amoxicillin, or other antibiotics do not enhance efficacy when used to treat primary and secondary syphilis, regardless of HIV status.
Recommended for Infants and Children
- Benzathine penicillin G50,000 units/kg IM, up to the adult dose of 2.4 million units in a single dose
- Note: Infants and children aged ≥1 month with primary or secondary syphilis should be managed by a pediatric infectious disease specialist and evaluated for sexual abuse (e.g., through consultation with child-protection services)
Jarisch-Herxheimer Reaction
The Jarisch-Herxheimer reaction is a self-limited reaction associated with initiation of anti-treponemal therapy that most often occurs in persons treated for early syphilis, presumably because bacterial burdens are higher during these stages. The Jarisch-Herxheimer reaction is characterized by fever, malaise, nausea, vomiting, and less frequently, chills and exacerbation of a secondary syphilis rash 21. This reaction almost always occurs within 24 hours after initiating antimicrobial therapy and usually resolves within 24 hours. For patients who develop a Jarisch-Herxheimer reaction, the clinician should clarify this reaction is not an allergic reaction to penicillin. It occurs more frequently after treatment with penicillin and treatment of early syphilis, especially at the secondary stage. Antipyretics can be used to manage symptoms associated with the Jarisch-Herxheimer reaction, but they do not prevent this reaction.
Primary and Secondary Syphilis
Parenteral penicillin G is effective in resolving clinical symptoms associated with primary and secondary syphilis and prevents late sequelae in those who receive appropriate treatment. The recommended regimen in the 2015 STD Treatment Guidelines for adults with primary and secondary syphilis is benzathine penicillin G given as 2.4 million units intramuscular (IM) in a single dose; for infants and children, the dose is 50,000 units/kg, with a maximum of 2. 4 million units 1. The few available studies exploring optimal dosing regimens did not find any benefit from additional doses of penicillin or with combination therapy that included other antibiotics 22.
Treatment of primary or secondary syphilis in penicillin-allergic patients
Treatment of primary and secondary syphilis for patients with documented allergy to penicillin is a topic with limited available data. Small studies and clinical experience suggest that regimens of doxycycline (100 mg orally twice daily for 14 days) or tetracycline (500 mg four times daily for 14 days) are acceptable alternatives for nonpregnant, penicillin-allergic persons who have primary or secondary syphilis 23. Doxycycline is preferable to tetracycline because tetracycline can cause gastrointestinal side effects and requires more frequent dosing. In addition, ceftriaxone (1-2 g daily either IM or IV for 10 to 14 days) is considered effective for treating primary and secondary syphilis, but the optimal dose and duration of ceftriaxone in this setting remains unknown 24. Azithromycin as a single 2 g oral dose has been effective for treating primary and secondary syphilis, but concerns for emerging macrolide resistance led the CDC to recommend avoiding azithromycin for first-line syphilis treatment and, if used, it should only be considered when treatment with penicillin or doxycycline is not feasible 25. Further, azithromycin to treat syphilis should not be used in any circumstance to treat MSM, persons with HIV infection, or pregnant women. Any person receiving any of the alternative therapies for the treatment of syphilis should have careful clinical and serologic follow-up. Persons with a penicillin allergy for whom concern exists with adherence or follow-up should undergo penicillin desensitization and then receive treatment with benzathine penicillin G.
Latent Syphilis
The treatment of patients with latent syphilis requires appropriate classification into early latent syphilis (acquired less than 1 year ago as detailed above) or late latent syphilis (acquired longer than 1 year ago), or undetermined duration. The goals of treating patients with latent syphilis are to prevent development of late manifestations of infection (tertiary/neurosyphilis), as well as to prevent transmission to the fetus by infected pregnant women. Early latent syphilis is treated with a single dose of benzathine penicillin G 2.4 million units IM; late latent syphilis is treated with benzathine penicillin G 7.2 million units total split into three weekly IM injections of 2.4 million units 1. There are limited data comparing the efficacy of specific regimens or duration, but available data do not suggest any added benefit of additional antibiotics. Alternative therapies for treatment of latent syphilis have not been well studied.
Treatment of latent syphilis in penicillin-allergic patients
For penicillin-allergic, nonpregnant patients with early latent syphilis, the treatment approach should be the same as penicillin-allergic patients with primary or secondary syphilis. For penicillin-allergic patients with late latent syphilis, the only acceptable treatment alternatives are doxycycline (100 mg orally twice daily) or tetracycline (500 mg orally four times daily), each for 28 days 1. Ceftriaxone may be a reasonable option in this setting, but the optimal number of doses or schedule has not been determined and use of ceftriaxone to treat latent syphilis should involve consultation with a syphilis expert. All patients treated with alternative regimens require close serologic and clinical follow-up, especially in persons with HIV infection. Patients for whom adherence and follow-up is a concern should be desensitized and treated with benzathine penicillin G if possible.
Neurosyphilis
Involvement of the central nervous system (brain and spinal cord) can occur during any stage of syphilis, which makes it essential that any patient receiving treatment for primary, secondary, or latent infection be evaluated for clinical evidence of neurologic involvement. If signs or symptoms of neurologic involvement are noted, a cerebrospinal fluid (CSF) examination should be performed 17. The recommended regimen for both neurosyphilis and ocular syphilis is aqueous crystalline penicillin G 18-24 million units per day, given as 3-4 million units intravenously (IV) every 4 hours (or as continuous infusion), for a total of 10 to 14 days 1. If adherence to therapy can be ensured, an acceptable alternative regimen is procaine penicillin G 2.4 million units IM once daily with probenecid 500 mg orally four times a day. Both agents are given for 10 to 14 days. It is important to note that some experts believe the duration of neurosyphilis therapy is not sufficient for treatment of late latent syphilis. Therefore, benzathine penicillin G 2.4 million units IM once per week for up to 3 weeks can be considered after completion of a neurosyphilis regimen in order to provide a comparable total duration of therapy. In addition, systemic corticosteroids have been used by some experts or specialists as adjunctive therapy for otologic syphilis, but data are insufficient to support the use of systemic corticosteroid therapy for otologic syphilis or any other form of syphilis.
Treatment of neurosyphilis in penicillin-allergic patients
Limited data suggest that ceftriaxone 2 g daily either IM or IV for 10 to 14 days can be used as an alternative treatment for persons with neurosyphilis 1. Other regimens have not been adequately studied for use in patients with neurosyphilis.
Tertiary Syphilis
The recommended regimen for tertiary syphilis (not neurosyphilis) is benzathine penicillin G 7.2 million units total split into three weekly IM injections of 2.4 million units 1. All persons diagnosed with tertiary syphilis should undergo a cerebrospinal fluid (CSF) examination prior to starting therapy. This is done because of the high rates of clinically inapparent neurosyphilis in patients with tertiary syphilis. Patients with tertiary syphilis have potential for a wide variety of sequelae and should be managed in consultation with a syphilis expert. Patients diagnosed with tertiary syphilis who have a documented penicillin allergy also should be treated in consultation with a syphilis expert; for these patients, there is no alternative therapy suggested in the STD Guidelines 1.
Syphilis in persons with HIV infection
Available data suggest that persons with HIV infection who have early syphilis may have an increased risk of developing neurologic complications 26. The extent of this increased risk has not been clarified and current CDC guidelines do no recommend routinely performing cerebrospinal fluid (CSF) examination in persons with HIV infection diagnosed with syphilis, but all persons with HIV infection and syphilis should undergo careful neurologic examination and those with abnormal findings should promptly undergo lumbar puncture for cerebrospinal fluid (CSF) examination 1. There is no evidence that more intensive syphilis treatment improves outcomes or prevents neurosyphilis in persons with HIV infection who have early syphilis 27. The recommended regimens for the treatment of syphilis in persons with HIV infection are the same as for persons without HIV infection 1. Initiation of antiretroviral therapy for HIV infection concurrently with syphilis treatment has been shown to reduce serologic failure rates for syphilis 28.
Syphilis in Pregnancy
All pregnant women diagnosed with syphilis should receive treatment according to stage of infection and whether there is any evidence of neurologic disease. Erythromycin is no longer an acceptable alternative drug for penicillin-allergic patients. Patients who are skin-test-reactive to penicillin should be desensitized in the hospital and treated with penicillin 1. Some experts recommend giving a second dose of benzathine penicillin G 2.4 million units IM 1 week after the initial dose for pregnant women who have primary, secondary, or early latent infection. Treatment of the mother during the last month of pregnancy or with a drug other than penicillin is not considered adequate treatment for the fetus. Pregnant women should be informed that treatment for syphilis may precipitate early labor and that they should notify an obstetrician if problems develop.
Infants and children with syphilis
The regimen for proven or highly probable and possible congenital syphilis is either aqueous crystalline penicillin G 100,000–150,000 units/kg/day, administered as 50,000 units/kg/dose IV every 12 hours during the first 7 days of life and every 8 hours thereafter for a total of 10 days; or procaine penicillin G 50,000 units/kg/dose IM in a single daily dose for 10 days. Neonates classified as possible congenital syphilis have the additional option of receiving treatment with benzathine penicillin G 50,000 units/kg IM in a single dose. The single dose regimen is only acceptable if all elements of the neonate’s lab work-up were performed and unequivocally normal. In addition, follow-up must be assured. Neonates with disease classified as “congenital syphilis less likely” should be given benzathine penicillin G 50,000 units/kg/dose intramuscularly in a single dose. Neonates for whom congenital syphilis is deemed unlikely do not require therapy but should be followed to ensure that their nontreponemal titer returns to nonreactive (as mother’s antibodies are lost). For additional details regarding the diagnosis and management of congenital syphilis, refer to the 2015 STD Treatment Guidelines for information on the management of congenital and acquired syphilis in infants and children or the American Academy of Pediatrics’ Red Book 1. Diagnosis and treatment of congenital syphilis is complex and challenging and should be done in consultation with a congenital syphilis expert. Notably, infants and children with a history of penicillin allergy or who develop signs of allergic reaction during treatment with penicillin present a unique challenge and should be managed with close follow-up and consultation with a syphilis expert.
Follow-Up
The follow-up of patients with syphilis is extremely important to document response to therapy and to reevaluate for reinfection. The following are general recommendations for follow-up after treatment.
- Patients treated for primary or secondary syphilis should be reexamined clinically and serologically 6 months and 12 months following treatment.
- Patients with latent syphilis should be followed up clinically and serologically at 6, 12, and 24 months.
- Persons with HIV infection should be evaluated more frequently; for primary or secondary syphilis at 3, 6, 9, 12, and 24 months and for latent syphilis at 6, 12, 18, and 24 months.
- If cerebrospinal fluid (CSF) pleocytosis was present initially, a CSF examination should be repeated every 6 months until the CSF cell count is normal. If the cell count has not decreased after 6 months, or if the CSF cell count or protein is not normal after 2 years, retreatment should be considered.
- Follow-up titers should be compared to the maximum or baseline nontreponemal titer obtained prior to treatment.
Treatment Failure
A key reason for close follow-up of patients treated for syphilis is to monitor signs, symptoms, or serologic changes that indicate possible treatment failure. There are no well-established, definitive criteria for treatment failure. Treatment failure cannot usually be differentiated from reinfection and thus persons suspected to have treatment failure or reinfection should be retested for HIV and should have a cerebrospinal fluid (CSF) evaluation for neurosyphilis (regardless of symptoms or prior CSF findings). Indications of probable treatment failure or reinfection include the following:
- A patient has persistent or recurring signs or symptoms.
- Patient testing shows sustained fourfold increase in nontreponemal titer. These patients should be retreated and reevaluated for HIV infection. Because treatment failure may be a result of unrecognized central nervous system (CNS) infection, cerebrospinal fluid (CSF) examination should be considered.
- Failure of nontreponemal titers to decline fourfold within twelve months after therapy for primary or secondary syphilis may be indicative of treatment failure. Additional clinical and serological follow-up is necessary since the optimal management is unclear. Examination of cerebrospinal fluid (CSF) can be considered in these instances.[65] If follow-up cannot be ensured, retreatment is recommended.
When patients are retreated for primary, secondary, or latent syphilis (assuming no evidence of neurosyphilis), the recommended regimen is weekly injections of benzathine penicillin G 2.4 million units IM for 3 weeks. If neurosyphilis is diagnosed, aqueous crystalline penicillin G 18-24 million units per day is given as 3 to 4 million units IV every 4 hours (or as continuous infusion), for a total of 10 to 14 days 1. Refer to the 2015 STD Treatment Guidelines 19 for more detailed information on assessment and management of probable treatment failure.
Partner Management and Public Health Measures
In general, the transmission of Treponema pallidum between sex partners only occurs when the person with syphilis has mucocutaneous lesions. In general, all persons who have sexual contact with a person diagnosed with primary, secondary, or early latent syphilis infection should undergo evaluation and testing for syphilis. Potential treatment for syphilis depends on the circumstances, as recommended in the 2015 STD Treatment Guidelines and outlined below 1.
- Persons who have had sexual contact with a person who receives a diagnosis of primary, secondary, or early latent syphilis within 90 days preceding the diagnosis should be treated presumptively for early syphilis, even if serologic test results are negative.
- Persons who have had sexual contact with a person who receives a diagnosis of primary, secondary, or early latent syphilis greater than 90 days before the diagnosis should be treated presumptively for early syphilis if serologic test results are not immediately available and the opportunity for follow-up is uncertain. If serologic tests are negative, no treatment is needed. If serologic tests are positive, treatment should be based on clinical and serologic evaluation and stage of syphilis.
- In some areas or populations with high rates of syphilis, health departments recommend notification and presumptive treatment of sex partners of persons with late latent syphilis who have high nontreponemal serologic test titers (i.e., greater than 1:32), because high titers might be indicative of early syphilis. These partners should be managed as if the index case had early syphilis.
- Long-term sex partners of persons who have late latent syphilis should be evaluated clinically and serologically for syphilis and treated based on these findings.
- Certain sex partners of persons with syphilis are considered at risk for infection and should be confidentially notified of the exposure and the need for evaluation. These include partners who have had sexual contact within 3 months plus the duration of symptoms for persons who receive a diagnosis of primary syphilis, 6 months plus duration of symptoms for those with secondary syphilis, and 1 year for persons with early latent syphilis.
Expedited Partner Therapy
There is insufficient data to support the use of expedited partner therapy in management of syphilis contacts. Accordingly, use of expedited partner therapy is not recommended for sexual contacts of persons diagnosed with syphilis. Transmission of Treponema pallidum is highly unlikely in persons when more than 1 year has elapsed since the time of infection.
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Syphilis. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- US Preventive Services Task Force (USPSTF), Bibbins-Domingo K, Grossman DC, et al. Screening for Syphilis Infection in Nonpregnant Adults and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;315:2321-7.[↩][↩][↩][↩][↩]
- U.S. Preventive Services Task Force. Screening for syphilis infection in pregnancy: U.S. Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med. 2009;150:705-9.[↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Special populations. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩][↩][↩][↩][↩][↩]
- Hollier LM, Hill J, Sheffield JS, Wendel GD Jr. State laws regarding prenatal syphilis screening in the United States. Am J Obstet Gynecol. 2003;189:1178-83.[↩]
- Association of Public Health Laboratories (APHL) and Centers for Disease Control and Prevention (CDC). Laboratory diagnostic testing for Treponema pallidum, Expert Consultation Meeting Summary Report, January 13-15, 2009, Atlanta, GA. https://www.aphl.org/programs/infectious_disease/std/Documents/ID_2009Jan_Laboratory-Guidelines-Treponema-pallidum-Meeting-Report.pdf[↩][↩][↩]
- Syphilis. https://www.std.uw.edu/go/pathogen-based/syphilis/core-concept/all[↩]
- Romanowski B, Sutherland R, Fick GH, Mooney D, Love EJ. Serologic response to treatment of infectious syphilis. Ann Intern Med. 1991;114:1005-9.[↩]
- Peeling RW, Ye H. Diagnostic tools for preventing and managing maternal and congenital syphilis: an overview. Bull World Health Organ. 2004;82:439-46.[↩]
- Seña AC, White BL, Sparling PF. Novel Treponema pallidum serologic tests: a paradigm shift in syphilis screening for the 21st century. Clin Infect Dis. 2010;51:700-8.[↩]
- Centers for Disease Control and Prevention (CDC). Discordant results from reverse sequence syphilis screening–five laboratories, United States, 2006-2010. MMWR Morb Mortal Wkly Rep. 2011;60:133-7.[↩][↩]
- Nandwani R, Evans DT. Are you sure it’s syphilis? A review of false positive serology. Int J STD AIDS. 1995;6:241-8.[↩]
- Geisler WM. The prozone phenomenon in syphilis testing. South Med J. 2004;97:327-8.[↩]
- Jurado RL, Campbell J, Martin PD. Prozone phenomenon in secondary syphilis. Has its time arrived? Arch Intern Med. 1993;153:2496-8.[↩]
- el-Zaatari MM, Martens MG, Anderson GD. Incidence of the prozone phenomenon in syphilis serology. Obstet Gynecol. 1994;84:609-12.[↩]
- Seña AC, Wolff M, Behets F, et al. Rate of Decline in Nontreponemal Antibody Titers and Seroreversion After Treatment of Early Syphilis. Sex Transm Dis. 2017;44:6-10.[↩]
- Marra CM. Update on neurosyphilis. Curr Infect Dis Rep. 2009;11:127-34.[↩][↩]
- Marra CM, Tantalo LC, Maxwell CL, Ho EL, Sahi SK, Jones T. The rapid plasma reagin test cannot replace the venereal disease research laboratory test for neurosyphilis diagnosis. Sex Transm Dis. 2012;39:453-7.[↩]
- 2015 Sexually Transmitted Diseases Treatment Guidelines. https://www.cdc.gov/std/tg2015/default.htm[↩][↩][↩]
- Centers for Disease Control and Prevention (CDC). Inadvertent use of Bicillin C-R to treat syphilis infection–Los Angeles, California, 1999-2004. MMWR Morb Mortal Wkly Rep. 2005;54:217-9.[↩]
- Brown ST. Adverse reactions in syphilis therapy. J Am Vener Dis Assoc. 1976;3:172-6.[↩]
- Cousins DE, Taylor M, Lee V. The outcome of treatment of early syphilis with different benzathine penicillin regimens in HIV-infected and -uninfected patients. Int J STD AIDS. 2012;23:632-4.[↩]
- Wong T, Singh AE, De P. Primary syphilis: serological treatment response to doxycycline/tetracycline versus benzathine penicillin. Am J Med. 2008;121:903-8.[↩]
- Hook EW 3rd, Roddy RE, Handsfield HH. Ceftriaxone therapy for incubating and early syphilis. J Infect Dis. 1988;158:881-4.[↩]
- Mitchell SJ, Engelman J, Kent CK, Lukehart SA, Godornes C, Klausner JD. Azithromycin-resistant syphilis infection: San Francisco, California, 2000-2004. Clin Infect Dis. 2006;42:337-45.[↩]
- Centers for Disease Control and Prevention (CDC). Symptomatic early neurosyphilis among HIV-positive men who have sex with men–four cities, United States, January 2002-June 2004. MMWR Morb Mortal Wkly Rep. 2007;56:625-8.[↩]
- Rolfs RT, Joesoef MR, Hendershot EF, et al. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The Syphilis and HIV Study Group. N Engl J Med. 1997;337:307-14.[↩]
- Ghanem KG, Moore RD, Rompalo AM, Erbelding EJ, Zenilman JM, Gebo KA. Neurosyphilis in a clinical cohort of HIV-1-infected patients. AIDS. 2008;22:1145-51.[↩]





{kind=link}